UNIVERSAL HEALTH COVERAGE - gov.uk · universal health coverage p sy g i responsive stems h cess...
3
R A V L S SU U S I EN REV O V N N ANCIA E N EVEN N U A S E RESPONSIVE SYSTEM RESPONSIVE SYSTEM R NF RING THE INFORMAL SEC NFORMAL S N F NI UNIVERSAL AL H INSURANC R C N A DUCIN C UIT Y T QUIT IT C PURC GIC PU TH INSU S TH IN V H IN ICE V S L SE H N NIV IN CESS ALT SER AYMEN ANCING MECHAN IV SU A S SU SMS CE T STR TR ERIN FORDA F R EAL E EA RVIC O O O OL V V V E V V V E E A U S U R RA VID UNIVERSAL HEALTH COVERAGE S P SY G I Y RESPONSIVE SYSTEMS H CESS STRATEGIC PURCHASING COVE AC EQUITY DESIGN ER PAYMENT N COLL HEALTH RDABLE HEALTH SERVICES G . VE FINAN OOLING R AFFORDABLE HEALTH SERVICE AFFORDABLE SE STRATEGIC PURCHA PROVIDER VATIVE FINAN EN URANCE COVERING THE INFORMAL SECTOR ACCESS INCENTIVES UNIVERSAL FUNDING . HEALTH INSURANCE . NEFIT PACKAGE DESIG A FFORDABLE HEALTH SERVICE S P LING RE NUE . COVER ING THE INFOR MAL SECTOR WORKERS . UBSIDIES STR ATEGIC PUR CHASING INNO VATIVE FINANCING MECHANIS MS INNO VATIVE FINANCING MECHANIS MS HEALTH INSURANCE . HEA LTH INS URANCE HE LTH INS URANCE . STRATEGIC PURCHSING PROVIDER PAYMENT . R T IN ATE I TEG N SEC C SE THE ES T TION H S H OR O O R ES CES K CE I E G C G C G CE T C T M CC T AC T CE N M T NT ACC A T S H M H M M E S STEM S. S S E L H U S E H TH H E TH D A A SID EA H TOR UALI IDIES T A T L V N I E T V A I L D D I E N E CT ILI N LI L T D C I C N T SILIE N I D D E N RESIL R V R EC V R T D T S E IT PACKAGE D . P Y S PACK S F R ST C TO SER NIVERSAL HEALTH COVERAGE H CO C FU NS E S EG ACCES C E CENTIVE Q INEQ NG N AN U G D R D E E RA H A V R P P P R PU PU PU P C C C S S R R H R R E S SU S C U P RIN RI A RA HE EA RV PO O EV E R P R F E FF EA F E C FO AL V R V EA S U R S U RA T ES E UNIVERSAL V ERV TO SERVI N HE INF THE INF OR R Y C P P C U ST VERIN ACCE ER PA NANC THE IN CR YMENT . NG MECHA RMAL ICES ROS ANISM N AY UN VER TH IN ERVICE U ES TH V INFO V RDA H C OR ALTH VICE O O U RAT HSI VID CE OL ALTH L S S C O OLI V EN EA L U DA ER A IN ST P A EGIC G MECHANISM INC R R NG MECHANISM W L RDAB P URCHS TA PURCH H U T T RAT RATEGIC M ER K PON ING T ESPON N E N E N R N RKERS L M S L RAT CHSI OVID R G S LE E R R LT R TE U RATE HEALTH BLE S TEGIC L C LT V DE N M A CH A N ID L EV R R R N NA A E H V H N L L R T G U G NS UNI ALTH E SER N T H IN C U N U N E I IV U N N N L N E S S S C S I C C C AGE AGE E ED E E GE BL G DA C PURCHAS ES G T S WO RAGE NT H ACCESS PACKAGE D PROVIDER INNOVATIV HEALTH INSU ORK A H A V C W R HE SYST TO IDIES UITY GE SID EQUI ES . LLECTION CES E NTIVES . EFIT PACKAG S N S UBS S. E RMAL SEC OSS-SUBSID SM K SECT P P O I U U Y C O A O I I I I I I I I T N N N RA U R R R R H RA H H A T A A A C H H H H H H H H H H H H C A S N H H H C NI TH R A A A R S MS S E O O I N NAN CH EA A S U RESILIE A BEN Y . AC H LIE N L T E EAL T STE RESIL HEA R CTO DI CT D IE NT FIT P D S HE C OR V L TH STEM DESIG H MS ACCE EQUITY H SIGN COVE NFO V U C EC HE C OR ALTH COVER RESILI T R BENEFIT PA ALITY FU . CIN AN N AN LT C I E K I R R G KAG AGE CKAGE D OVID TIO ES UB S N ON . AGE S . NT NF N NF N C R OS RSA CE RS RSAL H RVICES VER ER NIV TO O CRO A I S N SER TR PAYM CIN THE O NT . C T P NC U CE NG TH ESS T YME U A AT AT T A H L U U E S C C N V E N C V U U O O RO V V V EC N S ST CES NI T R SER TEG INS CES RSA O SE TO S TH T S C E EN UN CESS G ATEG LTH ERV V FOR ERVI E IN VI IN F CR FOR DUCIN QU SURA L SEC AL FUN RANCE C VE SYS FORMA NIVERSAL H INSUR N V INF UNI E IN UN ES NU PO UE CIN UIT Y T E VIC SS SU SYST RS . IAL PRO TAX CO LTH SERV CROS C TAX CO INCEN BENE R RE R REV R TRAT PURCHS ORDAB NG M STR PU TE M C N N . A V IE H TR PUR INN FIN ES RIN RE ER P P H AF SP N U RE LTH W EVEN ORD PU HEAL REVE AFFO YST AL S TEM SECTO MS ION O UBSID SIVE S NCIA NSI NA E IN ONS R FINA E . AL AL AL IT ACCESS ENTIVE EALTH ES INEQ AC INCE CING T Y T T ES NCE TEGIC HSING L RED INEQ ALTH INS QUI CENT VE NG AN HS H WORK F UE ABLE H ING IV RKERS ANCI HEAL TEMS ROTECTION SS-SU U G C C A RV PO REV HE S RA R R HE ES CH AL HEALTH COVERAGE EGIC PURCHASIN SECTO S . QUA NSURANCE . AFFORDABL UNIVERSAL FUNDING . ES . S O N H TH SEC O O UNIVERSAL HEALTH COVERAGE RESEARCH FOR
Transcript of UNIVERSAL HEALTH COVERAGE - gov.uk · universal health coverage p sy g i responsive stems h cess...

O
RA
VLLS SUWORKERS USH
IL
ENUREVENU OVENUEEVENUEEVENUE ANCIAE NEVEN NU ASO
SRESPONSIVE SYSTRESPONSIVE SYSTEMRESPONSIVE SYSTEMTRING THE INFORMAL SRING THE INFRING THE INFORMAL SECNFORMAL SNF
NIUNIVERSALSAL
H INSURANCSUURC
SC N
ADUCINNQ
CUITTYTQUITIT
C PURCGIC PUTH INSU
STH IN
VH INICE
VSL SEH
N
NIVINCESS
ALTSER
AYMENANCING MECHAN
IVSUA
SSU
SMSCETSTRTR
PERIN
FORDAF REALAEEARVICC
OOOOLVEVVEVVVVEEAA
USURRAT
HSVID
UNIVERSAL HEALTH COVERAGE
SP
SY
GI Y
RESPONSIVE SYSTEMSH
CESS
STRATEGIC PURCHASING
COVEAC
EQUITY
DESIGNER PAYMENT
N
COLL
HEALTH RDABLE HEALTH SERVICESG .
VE FINANCING MECHA--
POOLING R
AFFORDABLE HEALTH SERVICE
AFFORDABLE SE STRATEGIC PURCHASING
PROVIDERINNNOVATIVE FINAN
ENURANCE .
COVERING THE INFORMAL SECTOR
ACCESSINCENTIVES
UNIVERSAL FUNDING .HEALTH INSURANCE .
NEFIT PACKAGE DESIG
AFFORDABLE HEALTHSERVICES
P LINGRE NUE.
COVERING THE INFORMAL SECTOR
WORKERS .
UBSIDIES
STRATEGIC PURCHASINGINNOVATIVE FINANCING MECHANISMS
INNOVATIVE FINANCING MECHANISMS
HEALTH INSURANCE .
HEALTH INSURANCE .
HE LTH INSURANCE .
STRATEGICPURCHSING
PROVIDER PAYMENT .
R
T INATEITEGIC
N
SECCSECTHEES T
TIONHS H
OROORWSESA CESK CESI EG CG CG CET CET M CCTT ACT CEN M.EST TNT ACCAT S HTEM HMS MES STEMS .S L
SUI E LS E HHUUS
E HE THHE THD AU ABSID EA HSTOR
UALI
IDIES TA THL VN
I EA T VALTIESIL
DDIENI ENLCTO SILIEC NLILT DCT ICT ENT SILIENLI DLCT DRR
YE NRESILI IR VREC VR TE DTS E
N IT PACKAGE D. PYS PACKS FR PS T CATO SERNIVERSAL HEALTH COVERAGEH COC
FUNS
ESEG
ACCESCCESECENTIVEQINEQ
NGNAN
U
GD
RDE
E
RAHA
VR
C PPP RPUPUPUPCCC
S
S
RRH
RR
E
SSU
S
CCC
U
P
RINRI
ARAHE
EARVPOO
EVE
RP
R
FEFFEAFE
CFOALV
R
VEASUR
SURA
T
ESEUNIVERSAL HV
EERVTO SERVINHE INFTHE INFORCRYM CPP
C
U
ST
VERINACCE
ER PANANC
THE INCRYMENT .
NG MECHA
RMAL ICES
ROSANISM
NAY
UN VERTH IN
ERVICEU
ESTH
V
INFORV
RDAH
RCOR
ALTHVICEOO
URAT
HSIVID
CEOL
ALTHLS
S
COOLI
VENEAL
U
DAERA
SINSTP
AEGIC
G MECHANISMINCRR
NG MECHANISM
EW
LRDABPURCHS TAPURCHSHURCH
TTRATRATEGICM
ER
RK
PONING T
ESPONNE NAE FINRNRKERS
L
MS
L
RATCHSI
OVID
R
G
S
LEE
R
R
LTR TE
U
RATEHEALTH
BLE S
TEGIC
L
CLT
VDE
N M
ACHA
N
ID
L
EVR
RR
NNAAE
HV
H
NLL
RT
GUG
NS
UNIALTH
E SERN
TH IN
CU
N
UNE
IIVUN
NNL
NE
SSS
C
S
ICCC
AGEAGEEE D
EE
GEBL
GDA
C PURCHAS
ESG T
S
WO
RAGENTH
ACCESS
PACKAGE DPROVIDERINNOVATIVHEALTH INSU
ORK
AHA
V
CW
RHESYST
TOIDIESUITY
GE
SIDEQUI
ES .
LLECTIONCES
ENTIVES .EFIT PACKAG
SNSUBS
S . E
RMAL SECOSS-SUBSID
SM
K
SECT
PP
OI UUY
COA O
IIIIIIIITNNN
RAURRRRH
RAHH
ATA
AA
CHHHHHHHHHHHH
CAS
NHHHC NI
THRAAAR
SMS
SSE
OOI
NNANCH
EAASU
RESILIEA
BENY .
ACH
LIENLTE
EALTSTE
RESILHEA
RCTODI
CTD
IENTFIT P
D
SHE
C
OR
V
LTHSTEM
DESIG
HMSACCE
EQUITY
H
SIGN
COVENFO
VU
CECHE
C
OR
ALTH COVERRESILI TR
BENEFIT PAALITY
FU
.
CINAN
NANLT
C
I
EK
I
RR
GKAG
AGECKAGE D
OVID
TIOESUB
SN
ON .AGE
S .NT
NFNNFNC
ROS
RSACE
RSRSAL HRVICES
VERER
NIVTO
OCROA
I SNSER
TRPAYMCIN
THE O
NT .C
TP
NC
UCENG TH
ESS T
YME
U
AATATTAHL
UU ES CC
NV
ENC
VUUOORO
VVV
EC N
SS T
CESNI
TR
SER
TEG INS
CESRSA
O SETO STH
T
S
CEEN
UNCESS
G
ATEGLTH
ERVV
FORERVI
E INS VI
INFCR
FOR
DUCINQU
SURA
L SECAL FUN
RANCEC
VE SYSFORMA
NIVERSALH INSUR
N
VINF
UNIE INUN
ESNU
POUE
CINUITYT
E
VICSS SU
SYSTRS .
IAL PRO
TAX COLTH SERV
CROS
CTAX CO
INCENBENE
RRERREV
R
TRATPURCHS
ORDAB
NG MSTRPU
TEM
C
NN .
AV
IE
H
TRPURINNFIN
ESRIN
REER
P
PHAF
SPN
U
RELTH W
EVEN
ORDPU
HEALREVE
AFFO
YSTAL S
TEMSECTO
MSION
O
UBSID
SIVE SNCIA
NSINA
E INONS
RFINAE .
ALALAL
ITACCESS
ENTIVE
EALTHES
INEQAC
INCE
CINGTYTT
ES
NCE
TEGICHSING
L
G
REDINEQ
ALTH INS
QUICENT VE
NGAN
HSH WORK
FUE
ABLE HING
IVRKERS
ANCI
HEAL
TEMSROTECTION
SS-SUUG
CCA
RVPOREV
HESURAR
R
HEE S
CH
AL HEALTH COVERAGE
EGIC PURCHASIN
SECTOS . QUA
NSURANCE .AFFORDABLUNIVERSAL FUNDING .ES . S
ONH
THSEC
O
O
UNIVERSAL HEALTH COVERAGE
RESEARCH FOR

POOLING AND FINANCIAL RISK PROTECTIONCovering the informal sector The informal sector is highly diverse and its composition varies across and within countries. Health care coverage is particularly low among the near-poor who do not benefit from targeted interventions but constitute the bulk of the informal sector. For these groups, out-of-pocket payments persist as a way of funding services despite being grossly inequitable and contributing towards household poverty.
RESYST research in this area comprises reviewing the evidence and compiling country experiences of extending health coverage to the informal sector. Our review has identified significant challenges to using contributory schemes to cover the informal sector: low membership means small risk pools, schemes are only able to offer a limited package of services, and they often require additional payments at point of use. Even for mandatory schemes,
1
2
REVENUE COLLECTION
Increasing domestic resources for health The experience of Thailand has demonstrated that Universal Health Coverage can be achieved at low cost; however, insufficient funding impedes progress towards UHC in many countries. More money for health is needed from domestic resources rather than donor funding, which can be both unstable and unsustainable.
RESYST has generated new evidence showing that governments in three settings (Lagos State in Nigeria, South Africa, and Kenya) have increased domestic tax revenue without raising rates by expanding the tax base and improving the efficiency of tax collection systems. However, in these three countries, the share of revenue allocated towards health has not increased.
UNIVERSAL HEALTH COVERAGE
“The rallying call to pursue universal health coverage presents a unique opportunity to build health systems that are responsive to the needs of the population. But this dream will not be realised unless each government creates the fiscal space to fund health services adequately and develops the strategic purchasing capacity required to ensure equitable access to quality services. None of this is feasible without strong governance.”
RESEARCH ON FINANCING FOR
Whilst Universal Health Coverage is high on national and international agendas, many low and middle-income countries face significant challenges in expanding access to health services and financial protection to all people. Adequately addressing these challenges requires evidence, generated through research, which takes into account the complexity of countries’ diverse health systems and addresses the needs of their populations.
RESYST is conducting a programme of research for UHC across several low and middle-income countries in Africa and Asia. The research focuses on three key components of a health financing system for UHC: revenue collection, pooling and financial risk protection, and strategic purchasing.
A critical challenge for Ministries of Health is to find ways to make a better case for health during budget negotiations so as to expand the share of government spending on health. This includes demonstrating the economic and social benefits of health investments, improvements and achievements in health service delivery, and efficient use of money.
International actors, including WHO and donor organisations, have a role in helping Ministries of Health to develop the technical and analytical capacity to effectively advocate for health and demonstrate the benefits of UHC.
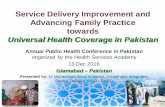
REGULATION: setting policy frameworks, setting standards a
nd monito
ring p
rogr
ess t
owar
ds u
nive
rsal
hea
lth co
vera
ge
R
EVEN
UE CO
LLECTION
1
2
3
RISK PROTECTION
POOLING & FINANCIAL
STRATEGIC PU RCHASING
e.g. Single pool covering whole population or other mechanism for promoting cross-subsidies across pools
e.g. Different insurance schemes covering different socio-economic groups with very different benefits
4
UNIVERSAL HEALTH
COVERAGE
Sour
ces o
f
reve
nue
How funds flow to different levels, services, geographic areas and interventions
Services that the population are
entitled to from the pooled funds
Methods that promote
equity, efficiency and quality e.g. salary, fee-for-
service, capitation
e.g. User fees to public sector, informal payments, fees paid to private providers
e.g. Taxes (general revenue,
earmarked tax), health insurance contributions
(mandated or voluntary)
Provider payment methods Benefi t package R
esource allocatio
n
Universal systems
Tiered systems
Dire
ct pa
ymen
ts
Pre-payments
countries face challenges in collecting contributions from the informal sector.
Countries that have had significant success in extending coverage, such as Rwanda (through its Community Based Health Insurance Scheme) and Thailand (through its tax-funded Universal Coverage Scheme) have demonstrated strong political support for the concept of UHC which is backed up by legislative, technical and regulatory frameworks, and accompanied by focused efforts on reaching poor and vulnerable groups.
More information:http://resyst.lshtm.ac.uk/research-projects/covering-informal-sector
More information:http://resyst.lshtm.ac.uk/research-projects/case-studies-improving-tax-collection
Professor Di McIntyreRESYST financing theme co-leader
Director, Health Economics Unit, University of Cape Town.

3STRATEGIC PURCHASINGMulti-country purchasing studyPurchasing is the critical link between resources mobilised for UHC and the effective delivery of quality services: strategic purchasing involves a number of key steps: determining which services will be provided, taking into account factors such as national health priorities as well as cost-effectiveness; choosing service providers, giving consideration to quality, efficiency and equity; and determining how services will be purchased, including contractual arrangements and provider payment mechanisms.
Through the multi-country RESYST Purchasing Study we are gathering information about the nature of purchasing arrangements in a range of settings in Africa and Asia, covering purchasers that include government ministries, social health insurance funds, and voluntary insurance funds. Through this research we intend to inform discussions about how purchasing arrangements can be structured to better support progress to UHC.
More information: http://resyst.lshtm.ac.uk/research-projects/multi-country-purchasing-study
RESYST is an international research consortium which aims to enhance the resilience and responsiveness of health systems to promote health and health equity and reduce poverty.
RESYST is funded by UK aid from the UK Government, however the views expressed do not necessarily reflect the UK Government’s official policies.
Dr Viroj TangcharoensathienRESYST financing theme co-leader
Senior Advisor, International Health Policy Program, Thailand
“Several Asian countries including Vietnam, the Philippines and China, have invested large amounts of funding for UHC into social health insurance schemes. Yet, despite some achievements, many people are still being pushed into poverty by the high cost of health care, and it is the relatively wealthy populations who are benefiting the most from public health spending.
The design of purchasing arrangements (such as benefit packages, or the way that providers are paid) has a substantial effect on how effectively and equitably health funds are used. Health financing organisations need to strengthen their governance and capacity to design and implement strategic purchasing to achieve UHC goals.”
http://resyst.lshtm.ac.uk@RESYSTresearch
COVERAGE OF SERVICES
UHC is not only about funding; a vital element of UHC is ensuring that there are enough trained health workers to provide services to everybody. Currently, many countries face a severe and persistent shortage of qualified health workers, especially in rural areas.
Attracting and retaining nurses in rural areasIn South Africa, RESYST researchers have sought to address the challenge of how to attract health workers to rural areas by tracking a cohort of nursing graduates and monitoring their employment decisions over several years. Evidence suggests that nurses who are exposed to rural life, either through training or as part of their upbringing, are more likely to work in rural posts.
New research has found that decisions about job location are also affected by a characteristic intrinsic to each individual - the dedication of nurses towards their patients. The more dedicated nurses are, as measured by their generosity towards patients in an economic experiment, the more likely they are to choose a rural job.
To ensure a higher proportion of nurses choose rural posts, the recruitment processes of nursing students could try and ascertain the extent to which potential candidates show signs of dedication towards patients. Also nurses’ curricula and experience during their studies could be adapted to cultivate positive attitudes towards patients.
More information: http://resyst.lshtm.ac.uk/research-projects/monitoring-nurses-job-choices