Nebraska 103rd Unicameral 1st Session Rule Book Legislative Rules 2013

Journal of Pediatric Orthopedics2:71-79 © 1982Raven Press, New York
Unicameral Bone Cyst with Epiphyseal Involvement:Clinicoanatomic Analysis
*Martin M. Malawer and tBruce Markle
Departments of "'Orthopedic Surgery and tRadiology, Children's Hospital National Medical Center and GeorgeWashingfOl7 University School of Medicine, washington, D.C.
Summary: Epiphyseal involvement of a unicameral bone cyst (UBC) is rare.This anatomic setting represents a distinct clinical and radiographic entity. Thisstudy reports a new case and analyzes the clinical and biological behavior ofseven additional UBCs with epiphyseal involvement from the literature. Wereport the first successful treatment of this variant with methylprednisoloneacetate. The average age was 20.1 years with a male to female ratio of 1.3: 1.Anatomic location: proximal femur (4), proximal humerus (2), and proximaltibia (2). Both age and location were atypical when compared to the classicmetaphyseal location. Radiographically, all lesions presented a characteristicinvolvement of the epiphysis and metaphysis in various proportions. Theepiphyseal plates were judged closed versus open in 50%, respectively.Follow-up ranged from 9 months to 3 years. Six cases healed following a singlecurettage (three with and three without bone graft). There were no late compli-cation of fracture, deformity, shortening, or avascular necrosis. Recurrencewas 0%. No secondary procedures were required. We conclude the age, loca-tion, and radiographic appearance is atypical and diagnosis is difficult, but thebiological behavior is less agressive and the prognosis more favorable than thetypical, metaphyseal UBC. Curettage with or without bone graft has a highsuccess rate. We recommend aspiration and intralesional methylprednisoloneas the initial management. We hypothesize that epiphyseal UBCs have a betterprognosis than metaphyseal location alone due to the older age, atypical loca-tion, and the potential of the epiphysis to reossify. Key Words: Epiphysis-Unicameral bone cyst-Methylprednisolone acetate-Proximal humerus-Proximal femur-Benign bone tumor (childhood).
Unicameral bone cyst (UBC) is a benign lesionfound in the long tubular bones of children and ad-olescents. Classically, they originate in themetaphysis, abut the growth plate, and later mayinvolve the diaphysis. This results from the con-tinued longitudinal bone growth of the epiphysisbeyond the site ofthe cyst (11). UBCs rarely involvethe epiphysis. Jaffee first decribed UBC, noting a
Dr. Malawer is Consultant at the Surgery Branch, NationalCancer Institute, N.I.H., Bethesda, Maryland.
Address correspondence and reprint requests to Dr. MaJawerat Department of Orthopedics/Oncology Section, Children'sHospital National Medical Center, III Michigan Avenue, .W.,Washington, D.C. 20010.
single example of epiphyseal involvement in a 42-year-old man (11). Cohn reported three cases ofUBC that had evidence of penetration of the physisat surgery (6). Other reports of epiphyseal involve-ment by UBC, including treatment and results, havebeen described (2,3,7,10,18,22). We have recentlytreated a solitary bone cyst with extensive epiph-yseal involvement in the proximal femur of a 14-year-old boy. Treatment consisted of biopsy, aspi-ration, and injection of methylprednisolone acetate.Curettage or bone grafting was not performed. Thepurpose of this paper is to report this case and toreview the literature.
A review of the literature has revealed a total of
71

72 M. M. MALAWER AND B. MARKLE
seven cases of UBC with epiphyseal involvement(Table I) (2,3,7,10,11,18,22). All of these reportshave been of isolated cases (1942-1980). To ourknowledge, this study is the first report to analyzethe overall manifestation and behavior of unicam-eral bone cysts with epiphyseal involvement (EUBC).This paper presents a retrospective analysis of theabove cases in order to answer the following ques-tions:
I. What are the clinical and radiographic char-acteristics of UBCs with epiphyseal extension?
2. What is the clinical significance (biological be-havior) regarding growth disturbance, deformity,recurrence, and avascular necrosis?
3. What is the appropriate clinical managementof this rare variant?
CASE REPORT
A 14-year-old male complained of exercise-related pain in the right hip for 3 months not re-sponsive to salicylates. There were no other mus-culoskeletal or constitutional complaints. Therewere no cutaneous abnormalities. Physical exami-nation showed that both legs were of equal leglengths without atrophy. The gait was normal; theTrendelenburg test was negative. The range ofinternal and external rotation on the right hip waslimited by 30°. The remainder of the musculo-skeletal examination was normal. Laboratory
studies, including CBC, serum electrolytes, calciumphosphorus, and serum alkaline phosphatase werewithin normal limits.
Radiographic Evaluation
Radiographs of the right hip (Fig. l) demonstratedan extensive radiolucent defect of the femoral neckand capital femoral epiphysis, partly circumscribedby a narrow margin of sclerosis. The cortex showedthinning but no expansion, cortical breakthrough,periosteal reaction or fracture. The femoral neckwas of normal length without deformity. Theacetabulum, pelvis, and joint space were normal.
A 99'J'c-MDP bone scan (Fig. 2) revealed no in-creased uptake in the lesion, but a subtle decreasein the femoral neck. There was normal activity inthe growth plates (signifying an open, active growthplate) without evidence or hyperemia or soft tissueextension.
Computed tomography (Fig. 3) showed a lucent,nonexpansile lesion of the femoral head and neckwithout extraosseous extension or matrix forma-tion, with an internal absorption coefficient of fluid.The combined radiographic studies suggested anonagressive lesion. The preoperative differentialdiagnoses included atypical UBC, atypical chon-droblastoma, giant cell tumor, unusual aneurysmalbone cyst, or eosinophilic granuloma.
TABLE 1. Epiphvse al unicamera! bone C.I'SI: literature review
Location Rx Status CommentReference Age/sex
Relationshipto epiphyseal Status of
plate plate
Closed
Metaphyseal!epiphyseal
Closed
MetaphyseaJ/ Openepiphyseal
Metaphyseal! Closedepiphyseal (tomograms)
Metaphyseall Closedepiphyseal
Epiphyseal Open
II 42/M Distal femur
10 6.5/F Proximal tibia
221F Proximal femur
22 Proximal tibial(entire ~)
15.3/F Proximal humerus(entire VI)
241M Proximal humerus
18
7 171M Proximal femur
Malawer and 141M Proximal femurMarkley (1982)
Metaphyseal! Openepiphyseal
Curettage:bone graft
Curettage:no graft
Curettage:bone graft
Curettage:no graft
Curettage;no graft
Curettage;bone graft
Healed 3 years, No shortening,FROM" no deformity
Healed 18 rnos,no Fx·
FROM 9 mos,healed
Healed (80%),2 years
Healing 6 mos, Initially presentedasymptomatic with articular collapse and
early degenerative change
2 em shortening
Intralesionalmethylprednisolonealone; no curettageor graft
FROMhealed (80%)2 years
Pressure, 16 em H20(pulsatile)
a FROM. full range of motion.• Fx. fracture.
J Pe-Iiatr Orthop, v'ol. 2. No. I. /982

UNICAMERAL BONE CYST WITH EPIPHYSEAL INVOLVEMENT
,B
Operative Procedure and Histology
The femoral neck was approached through ananterolateral incision. An I8-gauge needle was in-serted into the lesion, and clear, yellow fluid wasaspirated. Manometric measurements showed 16cm H20 pressure. Pulsation of the column syn-chronized with the patient's pulse. A Valsalva ma-neuver was performed, and a direct variation of thepressure was noted. Biopsy of the wall through alimited 0.5 x 0.5 em window in the anterior cortexconfirmed a cystic cavity with no underlying pri-mary neoplasm.
Histologically, the lining showed islands of acel-lular eosinophilic material, interspersed by a thinfibrous stroma containing a few vessels (Fig. 4).There were no giant cells, histiocytes, or hernosid-
R
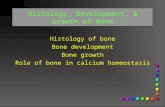
FIG. 2. Coned down, pinhole collimator views of 99mTc-MDPbone scan of the hips, in frontal projection, show normallinear areas of increased activity at the open growth platesof the femoral heads (straight arrow). greater trochanters(small arrowhead), and at the triradiate cartilates (largearrowhead). Despite the uncertain status of the growth plateby radiography, this scan demonstrates an active physealmechanism within the lesion. Note the subtle photon defi-cient area of the right femoral neck corresponding to the cyst(curved arrow).
73
FIG. 1. Initial anteroposterior (A) andlateral (B) radiographs demonstrate anextensive, well marginated, lytic de-fect of the femoral head and neck.The cortices of the femoral neck arethinned. The joint space and acetabu-lum are normal. The overall shape andsize of the femoral head are normal.There is no pathological fracture. Notethe extensive metaphyseal and epiph-yseal involvement without deformity.
erin. The clinical and histological diagnosis of UBCwas based on the finding of a cavity containing yel-low fluid lined by a thin fibrous membrane. Curet-tage and bone graft were not performed. Methyl-prednisolone acetate, 240 mg, was instilled underdirect vision via the cortical window, and thewound was closed. The dose was determined by theamount required to fill the cyst cavity.
RESULTS AND FOLLOW-UP
Postoperatively, the patient was maintainednonweight bearing for 6 weeks. Full weight bearingwas begun at 2 months. Twenty-four months fol-lowing surgery, he was fully ambulatory and par-ticipating in all activity. Examination of the hipshowed a full range of motion and a normal gait.
Radiographic Evaluation
Radiographs were obtained at 2 months, 6months, 8 months, 12 months (Fig. 5), and 18months (Fig. 6) after surgery. Serial radiographsshowed rapid thickening of the bony cortex andsecondarily progressive centripedal ossification.Heterotopic bone formation in the abductor mus-cles was noted and considered secondary to thesurgery. Twelve months after surgery, 80% of thedefect had reossified. There was complete reossifi-cation of the epiphysis and remodeling of the calcar,with premature obliteration of the epiphyseal plateand subsequent femoral neck shortening (decreasearticular trochanteric distance) but without defor-mity or avascular necrosis and with maintenance ofa normal joint space (Fig. 6A).
.I Pediatr Orthop , Vol. 2, No. I, 1982

74 M. M. MALA WER AND B. MARKLE
3A,8
FIG. 3. Computed tomography scans at the level of the capital epiphysis (A) and at the level of the femoral neck (8). Apart from asolitary central calcification, no osseous or cartilaginous matrix is present. There is no soft tissue mass. The cortex of the femuris thinned but intact. The joint space and acetabulum are normal. Note the surrounding zone of reactive sclerosis indicating abenign lesion.
Comment
In planning the treatment of this lesion, thepreoperative radiographic evaluation was importantin demonstrating the limits of the lesion and its
,• #
...-- , ,fit,
-,
I
II , .
FIG. 4. Histologic section of the bone cyst lining shows anamorphous, eosinophilic extracellular material and a cellularcomponent composed of mature fibrocytes. No osseous orcartilaginous matrix is present. There is no evidence of giantcells, chondroblasts, or inflammation.
J Pediatr Or/hop, Vol. 2. No. I, 1982
nonaggressive character. The unusual, extensiveinvolvement of the epiphysis made a specific diag-nosis difficult, even though many of the lesion'scharacteristics suggested a bone cyst. Additionalpossible diagnoses included chondroblastoma, giantcell tumor, eosinophilic granuloma, aneurysmalbone cysts, or a well healed infection (21). The"cold" character on radionuclide bone scan arguedagainst fibrous dysplasia (9). An intraosseouslipoma should have shown a typical low attenuationvalue by computed tomography. A bone cyst wasultimately diagnosed by the finding of a cystic cav-ity, containing clear yellow fluid, and Linedby a thinfibrous membrane.
CLINICOANATOMIC ANALYSIS ANDLITERATURE REVIEW
An extensive review of the literature noted sevencases in addition to the present case of UBC withepiphyseal involvement (Table 1). We analyzed theage, sex, location, treatment, rate of recurrence,and deformity in order to determine the clinicalbehavior and the appropriate management of thivariant.
Age and Sex Distribution
Age at the time of diagnosis ranged from 6.5 to 42years with an average of 20.1 years. Males outnum-bered females 4:3. The average age was notablyhigher than those reported of classic metaphy eallesions (1,2,4,10,14-16,19).

UNICAMERAL BONE CYST WITH EPIPHYSEAL INVOLVEMENT
Location of Lesion
There were four (50%) femoral, two (25%) proxi-mal humeral, and two (25%) proximal tibial lesions.This is an unusual distribution. Neer reported a re-verse ration of 2: 1, proximal humerus:proximalfemur, in a review of250 simple bone cysts (17). Hefound the tibia to be a rare site (less than 4%). Twoof eight cases of EUBCs involved the tibia.
Radiological Relationship and Status of Physis
All lesions (except Case 7) involved the metaphy-sis and epiphysis. The degree of involvement variedfrom predominantly metaphyseal to equivalent de-grees of epiphyseal and metaphyseal involvement.
Four of the seven cases (Cases 1,3,5, and 6) werein older individuals whose epiphyseal plates wereclosed. Three reported cases (Cases 2, 4, and 7) inaddition to our case (Case 8) had an open physis. Inone case, the epiphyseal plate was obliterated bythe lesion and the effects of old trauma.
Treatment and Results
Follow-up ranged from 9 months to 3 years. Re-sults of the earliest case (Case I) were not reported.
Six of the remaining cases reviewed were treatedwith curettage, three with and three without bonegrafting. All lesions healed. Bone grafting did notoffer any apparent advantage. There were no differ-ences between those with open or closed epiphysesregarding final outcome, irrespective of treatment.There were no recurrences, late fractures, defor-mity, avascu lar necrosis, or secondary proceduresrequired. No patient developed leg-length discrep-ancy. Humeral shortening in Case 5 was attributedto old trauma. Case 7, a femoral head lesion, pre-senting with subarticular collapse and early de-generative changes, was cured with curettage andbone graft. This was the only case of articular col-lapse. Thus, open epiphyseal plates did not appearto increase the incidence of late complications.
DISCUSSION
Unicameral bone cysts are classically metaph-y eal and adjacent to the physis in origin but maylater involve the diaphysis. Seventy percent willremain juxta-epiphyseal (17). The epiphysis israrely involved. This study reports one new case of
75
a UBC with epiphyseal involvement and retrospec-tively analyzed seven cases from the literature.
Clinical Considerations
The average age of patients with UBC in tubularbones is 9 to 15 years (1,3,4,10,14,16,19,20) with amale to female ratio of2 to 3: 1. In the present series,the average was older, 20 years, and the male to fe-male ratio was decreased to 1.3:1. The proximalhumerus and proximal femur (2: 1) are the mostcommon sites representing 75% of most large series. Incontrast, the present series showed four femoraland two proximal humeral lesions, a reverse of theexpected ratio. In addition, two patients (Cases 3and 4) had proximal tibia lesions, whereas tibial le-sions were much less common in other series. Neernoted that less frequent locations were characteris-tically found in adults (19). Boeseker et al. foundno proximal tibia lesion in 145simple UBC reviewed(3). He noted only one UBC with epiphyseal involve-ment in a review of the 145 UBCs seen at the MayoClinic during a 47 year period. Therefore, we con-cluded that the age, sex, and anatomic location ofEUBCs are atypical and do not lead to a correctdiagnosis from clinical or radiographic criteria alone.Surgery is necessary to establish the correct diag-nosis. Aspiration is a simple diagnostic technique.
Biological Activity and HemodynamicConsiderations
Biological and hemodynamic correlates of "ac-tivity" in addition to radiological location have beendescribed by Enneking (8) (1977). Latent cysts werecharacterized by a pressure on manometric mea-surement equal to venous pressure (6-10 cm H20)with a nonpulsatile column. Our hemodynamicmeasurements correspond to an active cyst (16 emH20 and pulsatile). This is the first reported pres-sure determination of a EUBC. Cohen (6) (1977)briefly reported three proximal femoral lesions withapparent perforation of the physis at surgery, but nofurther clinical or hemodynamic data were given.While one can speculate that increased cyst pres-sure may cause local erosion of the epiphyseal platewith subsequent epiphyseal extension, we suspectthis is not the main determinant, since most activecysts (therefore increased pressure) (8) do not clini-cally involve the epiphysis. Epiphyseal involvementhas been postulated to result from trauma to the
J Pediatr Or/hop. Vol. 2, No. I, /982

76 M. M. MALAWER AND B. MARKLE
SA,B
SC,D
SE,F
J Pediatr Or/hop, Vol. 2, No. /, /982

UNICAMERAL BONE CYST WITH EPIPHYSEAL lNVOLVEMENT
5G,H
77
FIG. 5. Serial postoperative radiographs at 2, 3, 6, and 10 months following cyst aspiration and steroid injection demonstrate thepattern of centripedal reossification. The initial stage shows amorphous ossification, which faintly outlines the radiolucent cystlining (open arrow, 3 months). Progressive ossification of this matrix provides substantial thickening of the bony cortex in bothfemoral neck and in the epiphysis (arrows). This continues centrally, slowly obliterating the cavity, i.e., endosteal new boneformation and not central ossification of the lesion.
growth plate with secondary extension (18). Thiscannot be substantiated by this review. The pul-satile, elevated pressure measurement we obtainedmay suggest a vascular etiology. Previously venousobstruction had been proposed by Cohen (5,6).Johnson suggested an etiology related to a smallangiomyxofibrillar lipoma (12).
Role of Methylprednisolone
Recurrence following curettage of UBC haveranged from 17 to 50% (17). Specifically, UBCs of
the proximal femur are difficult to treat and oftenresult in growth disturbance and pathologic frac-tures with subsequent coxa vara and ischemic ne-crosis (J 3). Boeseker (1968) noted a 28% recurrencerate of proximal femoral UBCs (3). Thus, we choseto treat our patient with aspiration and methylpred-nisolone as described by Scaglietti et al, (19) in orderto avoid this anticipated high rate of morbidity andrecurrence.
Scaglietti et aJ. (1979) reported 72 bone cyststreated by topical injection of methylprednisolone(19). Seventy-two percent of the lesions involved
6A,B
FIG. 6. Postoperative result at 18 months. Finalpostoperative anteroposterior (A) and lateral (B)radiographs demonstrate a small residual centralradiolucency, but significant reconsitution of thenormal bony architecture of the femoral head,neck, and calcar has been achieved without defor-mity, shortening, or avascular necrosis. Note thepremature obliteration of the physis and the resul-tant decrease in articular trochanteric distancesecondary to the healing (reossification) of thephysis.
J Pediatr Orthop, Vol. 2, No.1, 1982

78 M. M. MALA WER AND B. MARKLE
the humerus or proximal femur. Radiographic find-ings showed reconstitution of the cortical bone ofthe cyst wall (similar to our patient). Progressiveformation of new bone was noted at 6 months withopacification of the cyst cavity. Complete oblitera-tion of the cavity took 3 years. The epiphysis, un-like in our patient, usually continued normal growth,and Scaglietti stressed that no damage to the epiph-yseal cartilage resulted from injection of steroids.We hypothesize the premature closure of the epiph-yseal plate in the present case was due to the heal-ing process, i.e., reossification of the involved phy-sis and epiphysis (Fig. 6).
Scaglietti noted in all cases with a positiveradiological response that no fracture occurred. Nopatient required surgical treatment. Our patient sim-ilarly showed a good response, with early thicken-ing of the cortical walls and opacification of thecavity with resultant early ambulation and mainte-nance of a good range of motion (Fig. 5).
CONCLUSIONS
Unexpectedly, all six reported cases in the pres-ent series healed with a single curettage (with orwithout bone graft). More importantly, there wereno late sequelae offracture, deformity (except Case7), or avascular necrosis. Joint destruction and re-currence was not a problem. Interestingly, thestatus of the physis (open or closed) did not influ-ence the final outcome.
EUBC is a rare lesion and may be difficult todiagnose. The differential diagnosis should includechondroblastoma, giant cell tumor, eosinophilicgranuloma, intraosseous lipoma, and aneurysmalbone cyst (21). We believe that the clinical behaviorof a EUBC is to heal with simple curettage. Theexpected tendency for recurrence, deformity, andavascular necrosis is less than we anticipated. Wehypothesize that these lesions have a better prog-nosis than metaphyseal location alone due to theolder age of these patients (a good prognosticator insimple UBC), their atypical locations, and the in-creased potential of the epiphysis to reossify. Webelieve EUBCs represent a distinct clinicoanatomicentity with a less aggressive behavior and a morefavorable prognosis than the classic, metaphysealUBC, although its etiology is unknown. Furtherhemodynamic evaluation of both the metaphysealand epiphyseal variant is warranted and may eluci-date an underlying mechanism of epiphyseal exten-IOn.
SUMMARY
This paper reports a new case of a unicameralbone cyst with epiphyseal involvement and reviewsseven cases from the literature. The clinical andbiological behavior were analyzed.
1. An exact radiologic diagnosis is difficult.Radiologic imaging aids by demonstrating a nonag-gressive, solitary osseous lesion confined to bone.Aspiration is recommended as a simple confirma-tory diagnostic technique.
2. UBC (epiphyseal valiant) presents in an olderage group, often after epiphyseal closure, withoutexpansion or cortical destruction and involves boththe metaphysis and epiphysis.
3. These lesions are less aggressive than themetaphyseal UBC and can be expected to heal withsimple curettage, with or without bone graft.
4. There is a low morbidity following curettage.Postoperative fracture, deformity, and avascularnecrosis did not occur.
5. We recommend intralesional methylpred-nisolone acetate following aspiration with protec-tive bracing as the initial management and wouldreserve curettage for recurrent lesions or for diag-nosis when aspiration is nonconfirmatory.
Acknowledgment. We wish to acknowledge the con-tribution of Karen Harris in preparation of the manu-script and Dr. Lee Haacker in patient contribution.
REFERENCES
I. Baker OM: Benign unicameral bone cyst. A study of fortyfive cases with long-term follow up. Clin Orthop 71: 140-151.1970
2. Bernhang AM, Dua NK: Solitary bone cyst with epiphysealinvolvement. Or/hop ReI' 8:81-83, 1979
3. Boeseker EH, Bickel WH, Dahlin DC: A clinicopathologicstudy of simple unicameral bone cysts. Surg Gynecol Obsiet127:550-560, 1968
4. Campanacci M, Desessa L, Bellando Randone P: Solitarybone cyst: Results of surgical treatment and early results oftreatment by methylprednisolone acetate injection. Chir Or-gani Mall 62:471-482, 1975
5. Cohen J: Etiology of simple bone cyst. J Balle Joint Surg[AM] 52: 1493-1497, 1970
6. Cohen J: Unicameral bone cysts. A current synthesis ofreported cases. Orthop Clin North Alii 8:715-736, 1977
7. Czitrom AA, Pritzker KPH: Simple bone cyst cau ing col-lapse of the articular surface of the femoral head and incon-gruity of the hip joint. A case report. J Bone Join! Surg [AM]62:842-845, 1980
8. Enneking WF: Benign Skeletal Diseases ill Clinical Mus-culoskelet al Pathology, Gainesville, Storter Printing, 1977,pp 203-234
9. Gilday DL, Ash JM: Benign bone tumors. Semin Nucl Med6:33-46, 1976
10. Hutter CG: Unicameral bone cyst J BOlle Joint Surg [AM]32:430-432, 1950

UNICAMERAL BONE CYST WITH EPIPHYSEAL INVOLVEMENT
II. Jaffe HL, Lichtenstein L: Solitary unicameral bone cystwith emphasis on the roentgen picture, the pathologic ap-pearance and the pathogenesis. Arch Surg 44: 1004-1025,1942
12. Johnson LC, Kindred RG: The anatomy of bone cysts. Pro-ceedings of the Joint Meeting of the Orthopedic Associa-tions of the English Speaking world. J Balle Joint Surg [AM]40: 1440, 1958
13. Khermosh O. Weissman SL: Coxa vara. avascular necrosiand osteochondritis dissecan complicating bone cysts ofthe proximal femur. Clin Orthop 126: 143-146, 1977
14. McDougall A: Fracture of the neck of the femur in child-hood. J BOlle Joint Surg [Br] 43: 16- 28, 1961
15. McKay OW, Nason SS: Treatment of unicameral bone cystsby subtotal resection without grafts. J BOlle Joint Surg [Alii]59:515-519, 1977
16. Necr CS, Francis KC, Marcove RC, Terz J. Carbonara PN:Treatment of unicameral bone cyst. A follow-up study ofone hundred seventy five cases. J BOlle Joint Surg [Am]48:731-745,1966
79
17. Neer CS, Francis KC, Johnston AD, Kiernan HA Jr: Cur-rent concepts on the treatment of solitary unicameral bonecyst. cu» Orthop 97:40- 51, 1973
18. Nelson JP, Foster RJ: Solitary bone cyst with epiphysealinvolvement. A case report. Clin Orthop ll8: 147-150, 1976
19. Scaglietti 0, Marchetti PG, Bartolozzi P: The effects ofmethylprednisolone acetate in the treatment of bone cysts.Results of three years follow-up. 1. BOlle Joint Surg [Br]61:200-204,1979
20. Spence KF, Bright RW, Fitzgerald SP, SeU KW: SoLitaryunicameral bone cyst: Treatment with freeze-dried crushedcortical-bone allograft. J BOlle Joint Surg [Am] 58:636-641,1976
21. Spjut HL, Dorfman HD, Fechner RE, Ackerman LV:Tumors and tumor-like lesions simulating primary tumors ofbone. In: TUlI10rs of BOlle and Cartilage, Washington, D.C.,Armed Forces Institute of Pathology, 1970, pp 347-352
22. Tachdjian MO: Bone tumors and tumorlike conditions. Uni-cameral bone cyst. In Pediatric Orthopedics, Philadelphia,Saunders, 1972, pp 509-517
J Pedia!!' Or/hop, Vol. 2. No. I. 1982