

Unguided e-therapy for adults with depressive symptoms: IPT vs. CBT Tara Donker a, Kathleen M....
58
Unguided e-therapy for adults with depressive symptoms: IPT vs. CBT Tara Donker a , Kathleen M. Griffiths b , Helen Christensen b , Kylie Bennett b , Anthony Bennett b , Annemieke van Straten a , Pim Cuijpers a a VU University, Amsterdam b Australian National University, Canberra
-
Upload
damon-sherman -
Category
Documents
-
view
230 -
download
0
Transcript of Unguided e-therapy for adults with depressive symptoms: IPT vs. CBT Tara Donker a, Kathleen M....

Unguided e-therapy for adults with depressive symptoms:
IPT vs. CBT
Tara Donkera, Kathleen M. Griffithsb, Helen Christensenb, Kylie Bennettb , Anthony
Bennettb, Annemieke van Stratena , Pim Cuijpersa
a VU University, Amsterdamb Australian National University, Canberra
Introduction
Life time prevalence: 19% (Bijl et al., 1998)
Introduction
Top four leading causes of burden of disease worldwide (Lopez & Murray, 1998)
Introduction
Costs per capita for mood disorders: € 5,009 (Smit et al., 2006)
Low-intensity treatment for depression and anxiety
Obstacles
Long waitlists
Obstacles
2 hrs of travelling to the clinic

Obstacles
Take leave from work
Obstacles
Arrange a babysit
Obstacles
Costs of babysit
Obstacles
+.. Costs of travelling, babysit..
Low-intensity treatment for depression and anxiety
Psychological self-help:
•|Standardized •Independent•Homework/tasks•Via book, audio, internet..•Guidance by email, chat, telephone
Advantages
No wait lists
Advantages
Working from home
Advantages
24/7

Advantages
Cost-effective

Advantages
Anonymous

Low-intensity treatment for depression and anxiety
Intensive face-to face treatment
Obstacles
• Wait lists• Costs of therapy etc.• Time of travelling• Leave/babysit
Low-intensity treatment
Advantages
• Directly accessable• Cost-effective• Working from home• 24/7

Introduction

Introduction
Introduction
Introduction
E-CBT = effective (e.g. Carlbring et al., 2009; Christensen et al., 2004;Kaldo et al., 2008; Ruwaard et al., 2009; Spek et al., 2008; Warmerdam et al., 2008)
Introduction
Introduction
Introduction
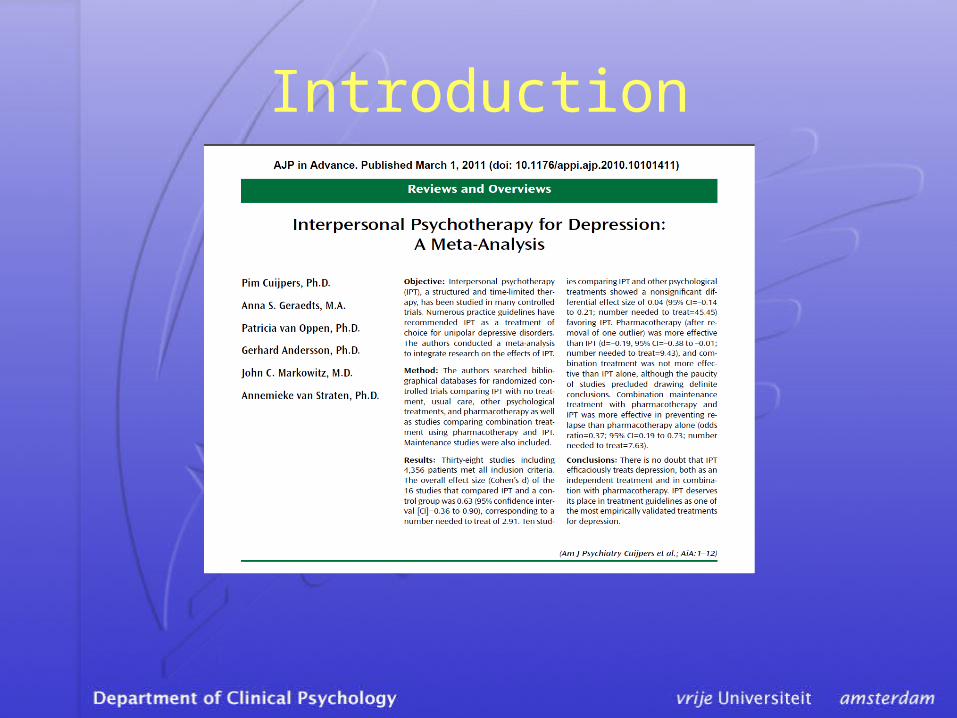
Depression: IPT = CBT (Cuijpers et al., 2011) Effect size: 0.04 (95% CI 0.14-0.21)

Introduction
==
??
Design
Internet-assisted
Cognitive Behavior Therapy (CBT) Cognitive Behavior Therapy (CBT)
&
Interpersonal Psychotherapy (IPT):Interpersonal Psychotherapy (IPT):
Design
Internet-assisted
Cognitive Behavior Therapy (CBT) Cognitive Behavior Therapy (CBT)
&
Interpersonal Psychotherapy (IPT):Interpersonal Psychotherapy (IPT):
Compared to
Internet-assisted
CBT MoodGYM (control group)
Design
• Non-inferiority trial
• H0: (IPT ≠ CBT) ≠ MoodGYM
• H1: (IPT= CBT) = MoodGYM
Design
MoodGYM
• Within effect size: 0.56 (95% CI: 0.33-0.79) (MacKinnon et al., 2008)
• Determined sample size: N=450 on post-test

Design
MoodGYM
• Between effect size: 0.33 (95% CI: 0.11-0.55)• Within effect size: 0.56 (95% CI: 0.33-0.79) (MacKinnon et al., 2008)
• Determined sample size: N=450 on post-test
Design
• Non-inferiority trial • 3 e-conditions (IPT, New CBT, CBT
MoodGYM)• Fully automated trial, 4 weeks • Online recruitment and screening

Design
• Inclusion: 18 years or older• Exclusion: currently under treatment by
mental health specialist • 3 measurements (baseline, after 4 weeks
and after 6-months)• Primary outcome: depressive symptoms
Interpersonal Psychotherapy
• Developed by Klerman and Weissman (1984)
• Relationship between depression and experiences
• IPT aims at improvement of interpersonal functioning and (inherent) depression
Internet-assisted IPT - overview
Internet-assisted IPT -week 1
Role disputes
• Identification of the dispute (with whom?)
• Modification of communication patterns
Internet-assisted IPT -week 2
Problems making relationships
• Realistic evaluation of can do`s/ can`t do`s
• Increase social contacts

Internet-assisted IPT -week 2 Problems making relationships
Internet-assisted IPT – week 2
Internet-assisted IPT - week 3 Role Changes
• Investigate which old role is given up
• Validate the loss
• Support letting go of old role
Internet-assisted IPT - week 3 Role Changes
• Develop new skills for the new role
• Develop new relationships and social support

Internet-assisted IPT – week 3

Internet-assisted IPT - week 4 Grief
• Activate grief proces– Psychoeducation– Learn to express emotions
• Finding new meaningful activities and social contacts replacing those which were lost
Internet-assisted IPT – week 4
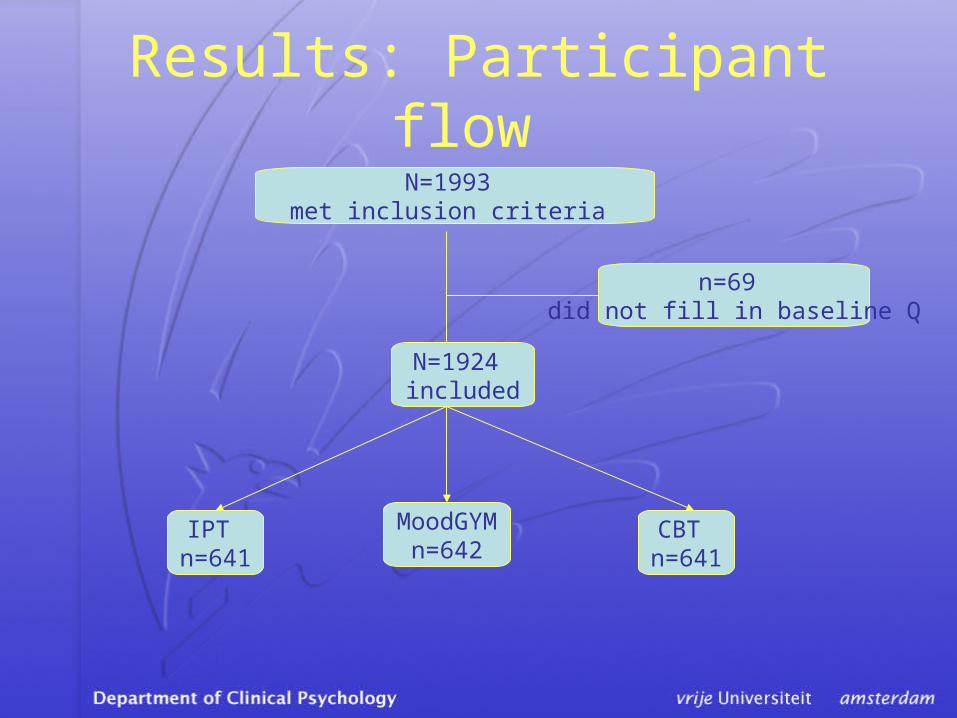
Results: Participant flow N=1993
met inclusion criteria
CBT n=641
IPT n=641
MoodGYMn=642
N=1924 included
n=69 did not fill in baseline Q
Results: demographics
• Gender: 71% female • Age category: 25-29 years (15.1%) • Country: 1: Australia (38%)• 2: United Kingdom (25%)• 3: United States (19%) • Education: higher degree (26%)• Previous treatment by professional: 80% • Been depressed before: 90%

Results: depressive symptoms
Mean CES-D at baseline (n.s.):
• Moodgym: 35 (sd: 11.7) n=622
• IPT: 36 (sd: 11.9) n=623
• CBT: 36 (sd: 11.) n=615

Results: depressive symptomscompleters only
15
20
25
30
35
40
0 4weeks since randomization
CE
S-D
depre
ssio
n s
core
CBTI PTMG
Results: depressive symptomscompleters only
Pre-post test:
• No significant differences across the condition (F=2.018; P=.13)
• Effect sizes:MoodGYM: 0.81
CBT: 0.87IPT: 0.77
Results: drop out
• CES-D: p=.02* (higher CES-D)
• Sexe: p =.<0.1* (more men)
• Age: p =.<0.1* (25-29 years)
• Education: p =.04* (lower education)
• Condition: p = .02* (MoodGYM)
• Been depressed: p = .80

Conclusions
Pre-post test for completers: • H1: (CBT = IPT) = MoodGYM• Effect sizes between 0.77-0.81• E-IPT: more treatment choice• 70% “drop out” • Significant differences in drop out for
demographics, treatment allocation, baseline CES-D score
Discussion
• ‘Gold standard’ MoodGYM:
Equivalence margin: 0.33
• Follow up data not yet available
• Drop out rate: 70% →» Missing data approaches» high symptoms: seek your GP » Unguided self-help » Characteristic of population

Disadvantages
Anonymous
Disadvantages
Guided self-help
Disadvantages
High drop out rate
Discussion
Unguided self-help….
• Ethical..?
• Under which conditions?


















