Ueda2016 symposium - glp-1 story,a closer look -yehia ghanem
43
-
Upload
ueda2015 -
Category
Health & Medicine
-
view
424 -
download
0
Transcript of Ueda2016 symposium - glp-1 story,a closer look -yehia ghanem


GLP-1 RA story: A closer look
Prof Yehia Ghanem
Head of Internal Medicine, Diabetes Unit
Alexandria University

Agenda
• The Incretin effect
• GLP-1 RA position in guidelines
• What’s Liraglutide
• Difference between Incretin-based therapies

Pathophysiology of type 2 diabetes
Cernea S & Raz I. Diabetes Care 2011;34(suppl 2):S264–S271
CNS, central nervous system; GI, gastrointestinal; T2DM, type 2 diabetes mellitus
Adipocyte
CNS
Incretin deficiency
GI tract
Altered fat metabolism
INSULIN RESISTANCE
INADEQUATE INSULIN
SECRETION
↑ HEPATIC GLUCOSE
PRODUCTION
↑ BLOOD GLUCOSE
Hyperglucagonaemia↑ hepatic sensitivity
to glucagon
cellsα cells
SkeletalMuscle
Pancreas
Muscle
Kidney
Enhanced glucose reabsorption
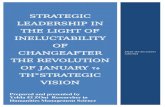
Role of incretin effect in healthy insulin response
• Insulin response is greater following oral glucose than IV glucose, despite similar plasma glucose concentration
1. Nauck M et al. Diabetologia 1986;29:46–52; 2. Wick A & Newlin K. J Am Acad Nurse Pract 2009;21(suppl 1):623–360
Oral glucose load (50 g) IV glucose infusion
Pla
sm
a G
lucose (
mm
ol/
L)
–10 –5 60 120 180
10
Time (min)
5
0
15
Plasma Glucose1 Insulin Response2
Insulin (
mU
/L)
80
60
40
20
–10 –5 60 120 1800
Time (min)
Incretineffect

The incretin hormones
1. Glucagon-like Peptide-1 (GLP-1)• secreted by cells in the distal ileum and colon, in
response to food intake – nerve and hormonal stimulation
• more potent than GIP in stimulating insulin secretion
2. Glucose-dependent insulinotropic Peptide (GIP)• secreted by cells in duodenum when food enters the area
• circulating levels up to 10x higher than GLP-1
Insulin (
pm
ol/
L)
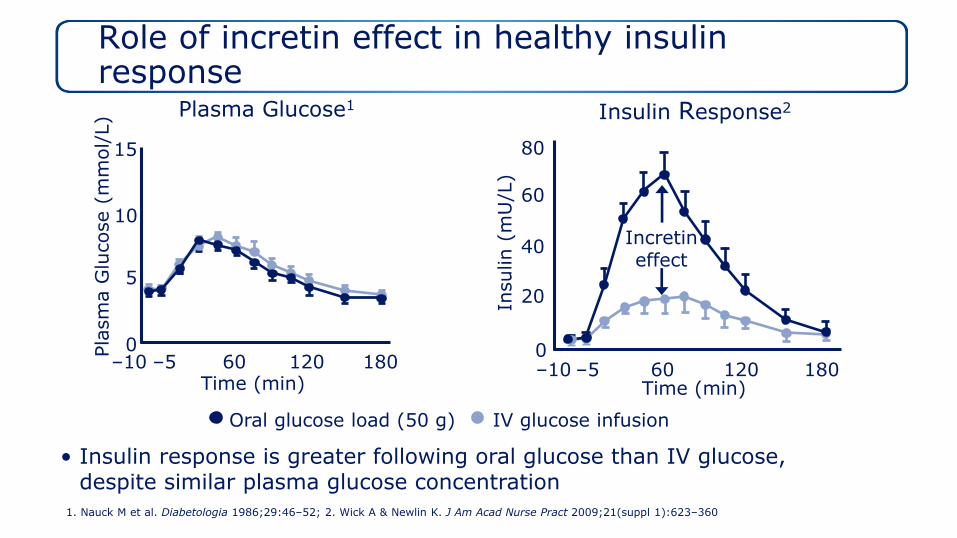
Continuous IV infusion during hyperglycaemic clamp (15 mmol/L)
Time (min)
GLP-1 (1 pmol)
GIP (16 pmol)
0
500
1000
1500
2000
2500
–20 30 80 120
3000
0
GLP-1 (but not GIP) increases both early- and late-stage insulin secretion
Vilsbøll T et al. Diabetologia 2002;45:1111–1119
Mean±SEMGIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1; IV, intravenous; SEM, standard error of the mean

Effect of GLP-1 is glucose-dependent
• Effects of 4-hour GLP-1 infusion (1.2 pmol/kg/min) in 10 patients with type 2 diabetes
GLP-1, glucagon-like peptide-1; SE, standard error
Nauck M et al. Diabetologia 1993;36:741–744
Mean (SE); n=10*p<0.05
Placebo Native human GLP-1
300
200
100
0
Insulin (pmol/L)
Time (min)-30 0 60 120 180 240
*** **
**
*
Glucagon (pmol/L)
-30 0 60 120 180 240
20
10
0
Time (min)
***
*
Glucose (mmol/L)15
10
5
0
-30 0 60 120 180 240
Time (min)
*
*
*
**
*
*

Liraglutide
GLP-1R
Insulin exocytosis
ATP
Glut2Potassium Channel
Calcium Channel
Glucose
K+
TCA
Amplifying
Pyruvate
EpacTriggering
AC
GsαGsα
ATPcAMP
Ca2+
Ca2+
GLP-1 Receptor agonist Liraglutide mode of action in the β cell
Hinke SA et al. J Physiol 2004;558:369–380; Henquin JC. Diabetes 2000;49:1751–1760; Henquin JC. Diabetes 2004;53:S48–S58; Drucker D. Cell Metab 2006;3:153–165

The incretin effect is diminished in patients with type 2 diabetes
*p<0.05, healthy volunteers (n=8)
Nauck M et al. Diabetologia 1986;29:46–52
Type 2 Diabetes
Insulin (
mU
/L)
80
60
40
20
0 30 60 120 1800
Time (min)15090
**
*
Insulin (
mU
/L)
0 30 60 120 180
40
Time (min)
20
0
80
Healthy Controls
60
90 150
***
****
Incretineffect
Oral glucose IV glucose

Diminished insulin response to physiological levels of GLP-1impaired in T2DM
Physiological levels of GLP-11
(15 mM hyperglycaemic clamp)
GLP-1, glucagon-like peptide 1, T2DM, type 2 diabetes mellitus
1. Højberg PV et al. Diabetologia 2009;52:199–207; 2. Vilsbøll T et al. Diabetologia 2002;45:1111–1119
00 30 60 90 120
Time (min)
1000
2000
3000
4000
5000
6000
Insulin (
pm
ol/
L)
GLP-1 infusion period
(0.5 pmol/kg/min)
Plasma GLP-1:46 pmol/L
Healthy
Plasma GLP-1:41 pmol/L
T2DM
Pharmacological levels of GLP-12
(15 mM hyperglycaemic clamp)
0
1000
2000
3000
4000
0 45 90 135 180
Time (min)
Insulin (
pm
ol/
L)
5000
6000GLP-1 infusion period
(1.0 pmol/kg/min)
Plasma GLP-1:126 pmol/L
T2DM

n=8GLP-1, glucagon-like peptide-1
Larsen J et al. Diabetes Care 2001;24:1416–1421
24-hour GLP-1 presence required for 24-hour glucose control
Time (h)Before native human GLP-1 treatmentBlood glucose profiles:
After 7 days’ native human GLP-1 treatment
24-h GLP-1 infusion
12 00 0408 16 2004
5
10
20
15
25
Pla
sm
a G
lucose (
mm
ol/
L)
5
10
20
25
15
04 12 00 0408 16 20
16-h GLP-1 infusion

13

Agenda
• The Incretin effect
• GLP-1 RA position in guidelines
• What’s Liraglutide
• Difference between Incretin-based therapies
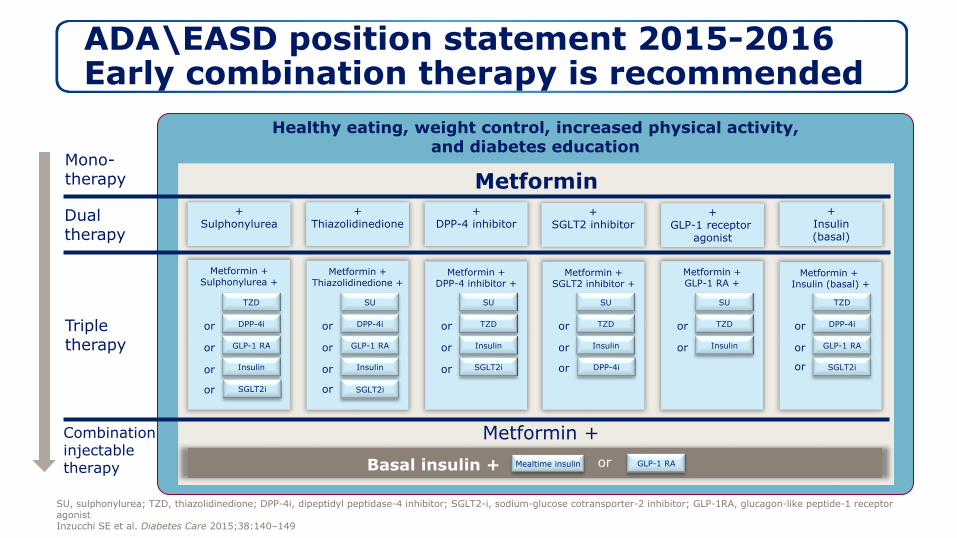
ADA\EASD position statement 2015-2016Early combination therapy is recommended
Healthy eating, weight control, increased physical activity, and diabetes education
MetforminMono-therapy
Dual therapy
Triple therapy
Combination injectable therapy
Metformin + Sulphonylurea +
TZD
DPP-4i
GLP-1 RA
Insulin
or
or
or
Metformin +Thiazolidinedione +
SU
DPP-4i
GLP-1 RA
Insulin
or
or
or
Metformin +DPP-4 inhibitor +
SU
TZD
Insulin
or
or
Metformin +GLP-1 RA +
SU
TZD
Insulin
or
or
Metformin + Insulin (basal) +
TZD
DPP-4i
GLP-1 RA
or
or
+Sulphonylurea
+Thiazolidinedione
+DPP-4 inhibitor
+GLP-1 receptor
agonist
+Insulin(basal)
Metformin + SGLT2 inhibitor +
SU
TZD
Insulin
or
or
SGLT2i SGLT2i
SGLT2i DPP-4i SGLT2i
Metformin +
Mealtime insulinBasal insulin +
or or or
or or
+SGLT2 inhibitor
or GLP-1 RA
SU, sulphonylurea; TZD, thiazolidinedione; DPP-4i, dipeptidyl peptidase-4 inhibitor; SGLT2-i, sodium-glucose cotransporter-2 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonistInzucchi SE et al. Diabetes Care 2015;38:140–149

ADA\EASD position statement 2015:Choice of therapy after metformin.
DPP-4i, dipeptidyl peptidase-4 inhibitor; GI, gastrointestinal; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin; SU, sulphonylurea; TZD, thiazolidinedione; ↑, weight gain; ↓, weight loss; ↔, weight neutral
SU TZD DPP-4i SGLT-2i GLP-1RAInsulin (basal)
Efficacy (↓HbA1c)
High High Intermediate Intermediate High Highest
Hypoglycaemia risk
Moderate Low Low Low Low High
Weight effect ↑ ↑ ↔ ↓ ↓ ↑
Major side effects
Hypo-glycaemia
OedemaHeart failure
Bone fracturesRare
GenitourinaryDehydration
GIHypo-
glycaemia
Inzucchi SE et al. Diabetes Care 2015;38:140–149


Strictly Confidential. Proprietary
information of Novartis. For internal
use ONLY. March 2010. GAL10.497. 19

Agenda
• The Incretin effect
• GLP-1 RA position in guidelines
• What’s Liraglutide
• Difference between Incretin-based therapies

Liraglutide is a once-daily, human GLP-1 analogue
glutamoyl spacer
3426
Knudsen et al. J Med Chem 2000;43:1664–9; Degn et al. Diabetes 2004;53:1187–94

Liraglutide: Mechanisms of protraction
• Self-association to form heptamers: slow absorption.
• Reversible albumin binding: protection against cleavage.
• Higher enzymatic stability to DPP-4: Longer half life.
• Half life is 13 hours and suitable for once daily injection.
Knudsen et al. J Med Chem 2000;43:1664–9; Degn et al. Diabetes 2004;53:1187–94

Percentage of patients with increase in antibodies
Liraglutide10
20
40
60
80
100
Exenatide + metformin2
43%8.6%
Liraglutide: greater homology to native human GLP-1, less antibody formation
97% amino acid homology
to human GLP-1
53% amino acid homology to human GLP-1 • There was no blunting
of efficacy by liraglutide antibodies
Study duration: Liraglutide 26 weeks; exenatide 30 weeks.1LEAD1,2,3,4,5 meta-analysis of antibody formation; Data on file; 2DeFronzo et al. Diabetes Care 2005;28:1092
Native human GLP-1
Liraglutide
Exenatide

H2H incretins
Liraglutide clinical trial program covers different treatment modalities
BID, twice daily; Met, metformin; OAD, oral antidiabetes drug; SU, sulphonylurea; TZD, thiazolidinedioneSource: ClinicalTrials.gov
Drug naive Special populations
LIRA-RENAL™ (n=279)vs placebo
Add-on to SOC
≥1 OAD Insulin users
LIRA-DETEMIR (n=323)vs liraglutide plus IDet
Add-on to met
LIRA-ADD2BASAL™ (n=446)vs placebo
Add-on to basal insulin ± met
ellipse™ (paediatric; n=172)vs placebo
Add-on to metTo be finished in 2020
LIRA-LIXI™ (n=400)vs lixisenatideAdd-on to met
LIRA-SWITCH™ (n=396)vs sitagliptin
Add-on to met, switch from sitagliptin
To be published in ADA-16
LIRA-Ramadan™ (n=320)vs SU
Add-on to met, switch from SU
LEAD-3 (n=746)vs SU
LEAD-4 (n=533)vs placebo
Add-on to met + TZD
LEAD-2 (n=1091)vs SU or placeboAdd-on to met
LEAD-1 (n=1041)vs TZD or placebo
Add-on to SU
LEAD-5 (n=581)vs insulin glargine or placebo
Add-on to met + SU
LEAD-6 (n=564)vs exenatide BID
Add-on to met ± SU
LIRA-DPP-4 (n=665)vs sitagliptin
Add-on to met
Completed
Ongoing
LEADER® (cardiovascular outcomes trial) SOC plus liraglutide 0.6 mg–1.8 mg vs SOC plus placebo (n=9,340)
Drug-naïve or add-on to ≥1 OAD or add-on to basal or premix insulin (alone or in combination with OADs)
To be published in ADA-16

Significant HbA1c reduction up to 1.6% from 8.6% baseline
Significant *vs. comparator; #change in HbA1c from baseline for overall population (LEAD-4) add-on to diet and exercise failure (LEAD-3); or add-on to previous OAD monotherapy (LEAD-2,-1)
Marre M et al. Diabet Med 2009;26:268–278 (LEAD-1); Nauck M et al. Diabetes Care 2009;32:84–90 (LEAD-2); Garber A et al. Lancet 2009;373:473–481 (LEAD-3); Zinman B et al. Diabetes Care 2009;32:1224–1230 (LEAD-4); Russell-Jones D et al. Diabetologia 2009;52:2046–2055 (LEAD-5);
n= 702Duration= 52 w Previous : Diet
(272)
n= 1026Duration= 26 wPrevious: 1 OAD
(385)
n= 1026Duration= 26 w
Previous: 1 or more
OAD
n= 492Duration= 26 w
Previous: 1 or more
OAD
n= 570Duration= 26 wPrevious: 94% on
OAD combination

Liraglutide is effective early and late in the treatment but early is better than late
Early use defined as liraglutide add-on to ≤1 OAD; late use defined as add-on to 2 oral OADs
Analysis includes data from the liraglutide vs. sitagliptin study
HbA1c, glycosylated haemoglobin; OAD, oral antidiabetic drug; T2DM, type 2 diabetes mellitus
Garber et al. Diabetes 2011;60(Suppl. 1):967-P`

A quartile of patients have an average weight loss of 7.7 Kg.
(Metformin + liraglutide 1.8 mg/day) Mean±2SE
Nauck MA, et al. Diabetes Care 2009; 32; 84–90 (LEAD-2)
More than 80% of patients lost weight

28

Agenda
• The Incretin effect
• GLP-1 RA position in guidelines
• What’s Liraglutide
• Difference between Incretin-based therapies

Family of Incretin-based therapies

Summary of mode of action of GLP-1 receptor agonists and DPP-4 inhibitors
1. Degn et al. Diabetes 2004;53:1187–94; 2. Mari et al. J Clin Endocrinol Metab 2005;90:4888–94
Subcutaneous injection
Resist degradation by DPP-4
Active GLP-1 level ~80 pmol/L1
High pharmacological level of GLP-1 receptor activity
Oral ingestion
Inhibit DPP-4 enzyme
Active GLP-1 level ~20 pmol/L2
Increased physiological activity of GLP-1 receptor
(mainly after meals)
GLP-1 receptor agonists DPP-4 inhibitors
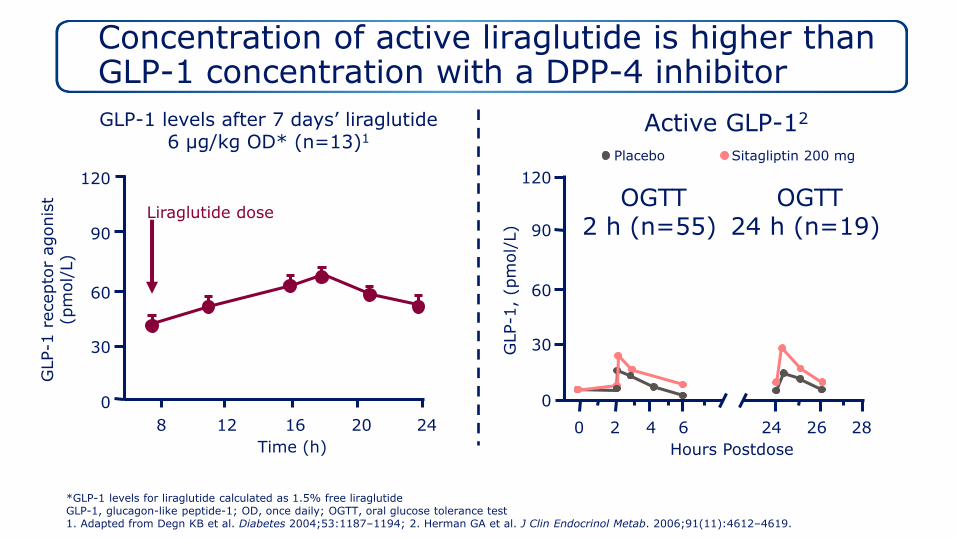
Concentration of active liraglutide is higher than GLP-1 concentration with a DPP-4 inhibitor
*GLP-1 levels for liraglutide calculated as 1.5% free liraglutideGLP-1, glucagon-like peptide-1; OD, once daily; OGTT, oral glucose tolerance test1. Adapted from Degn KB et al. Diabetes 2004;53:1187–1194; 2. Herman GA et al. J Clin Endocrinol Metab. 2006;91(11):4612–4619.
OGTT2 h (n=55)
Active GLP-12
Hours Postdose
GLP-1
, (p
mol/
L)
GLP-1 levels after 7 days’ liraglutide6 µg/kg OD* (n=13)1
120
90
60
30
0
0 2 4 6 24 26 288 12 16 20 24
GLP-1
recepto
r agonis
t(p
mol/
L)
Time (h)
Liraglutide dose
Placebo Sitagliptin 200 mg
OGTT24 h (n=19) 90
60
30
120
0

Gastric emptying
Additional physiological benefits are observed at pharmacological levels of GLP-1
Adapted from Holst et al.1
1. Holst JJ et al. Trends Mol Med 2008;14:161–168; 2. Flint A et al. Adv Ther 2011;28:213–226
Physiological GLP-1 levels
Pharmacological GLP-1 levels
GLP-1 effects
Incre
asin
g P
lasm
a G
LP-1
Concentr
ations
GLP-1RAs
DPP-4is
DPP-4is, dipeptidyl peptidase-4 inhibitors; GLP-1, glucagon-like peptide 1; GLP-1RAs, glucagon-like peptide 1 receptor agonists
Insulin Glucagon= Plasma glucose2
Appetite Food intake= Weight loss2

Sustained better HbA1c reduction vs. Sitagliptin – 52 weeks
Estimated treatment difference (ANCOVA): liraglutide 1.2 mg vs. sitagliptin 0.40; liraglutide 1.8 mg vs. sitagliptin 0.63 (both p<0.0001). Data are mean (1.96 SE) from FAS, LOCF
Pratley et al. Int J Clin Pract 2011;65:397–407
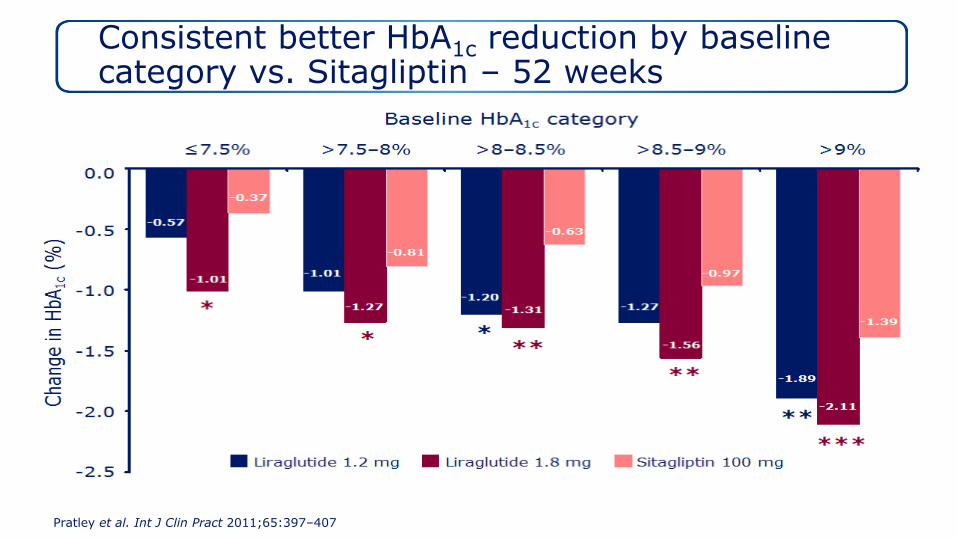
Consistent better HbA1c reduction by baseline category vs. Sitagliptin – 52 weeks
Pratley et al. Int J Clin Pract 2011;65:397–407

Higher percentage of patients reaching ADA/EASD target vs. Sitagliptin
ADA, American Diabetes Association
Pratley et al. Int J Clin Pract 2011;65:397–407

Similar very low rate of minor hypoglycaemia weeks 0-52 vs. Sitagliptin
Pratley et al. Int J Clin Pract 2011;65:397–407
Event/
patient/
year
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Liraglutide 1.2 mg Liraglutide 1.8 mg Sitagliptin 100 mg

Significant reduction in body weight vs. sitagliptin
Mean (1.96 SE); data are from the FAS, LOCF
Pratley et al. Lancet 2010:375;1447–56; Pratley et al. Int J Clin Pract 2011;65:397–407

-2.0
-1.8
-1.6
-1.4
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
Liraglutide has unsurpassed efficacy in GLP-1 RA comparative studies
*Treatment difference (nominal 95% CI)=-0.06 (-0.19, 0.07), p<0.0001 for non inferiority vs liraglutideBID, twice a day; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin Buse JB et al. Lancet 2009;374:39–47 (LEAD-6); Buse JB et al. Lancet 2013;381:117–24 (DURATION-6); Pratley RE et al. Lancet Diabetes Endocrinol 2014;2:289–97 (Harmony-7); Dungan KM et al. Lancet 2014; 384(9951):1349–1357 (AWARD-6); Nauck MA et al. European Association for the Study of Diabetes 2015 Annual Meeting, Abstract #75 (LIRA-LIXI) www.easdvirtualmeeting.org/resources/once-daily-liraglutide-vs-lixisenatide-as-add-on-to-metformin-in-type-2-diabetes-a-26-week-randomised-controlled-clinical-trial--2 Accessed August 2015.
Ch
an
ge in
Hb
A1
c(%
)
p<0.0001
Baseline HbA1c (%):
LEAD-6
8.2 8.1
HARMONY-7
8.2 8.2
DURATION-6
8.58.4
AWARD-6
8.1 8.1
-1.12
-0.79
-1.28
-0.98
-0.79
-1.42
p=0.0001
-1.36
-1.48
LIRA-LIXI
8.4 8.4
p<0.0001
-1.83
-1.21
Liraglutide 1.8 mg Exenatide 10 µg BID
Dulaglutide 1.5 mgAlbiglutide 50 mg
Exenatide 2 mg
Lixisenatide 20 µg
95% CI [0.08,0.34]
95% CI [-0.19,0.07]

-5.0
-4.5
-4.0
-3.5
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Liraglutide has unsurpassed weight reduction in GLP-1 RA comparative studies
*BID, twice a day; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin Buse JB et al. Lancet 2009;374:39–47 (LEAD-6); Buse JB et al. Lancet 2013;381:117–24 (DURATION-6); Pratley RE et al. Lancet Diabetes Endocrinol 2014;2:289–97 (Harmony-7); Dungan KM et al. Lancet 2014; 384(9951):1349–1357 (AWARD-6); Nauck MA et al. European Association for the Study of Diabetes 2015 Annual Meeting, Abstract #75 (LIRA-LIXI) www.easdvirtualmeeting.org/resources/once-daily-liraglutide-vs-lixisenatide-as-add-on-to-metformin-in-type-2-diabetes-a-26-week-randomised-controlled-clinical-trial--2 Accessed August 2015.
Ch
an
ge in
bo
dy w
eig
ht
(K
g)
Baseline weight (Kg):
LEAD-6
93.1 93.0
HARMONY-7
92.8 91.7
DURATION-6
90.991.1
AWARD-6
93.8 94.4
LIRA-LIXI
101.9 100.6
Liraglutide 1.8 mg Exenatide 10 µg BID
Dulaglutide 1.5 mgAlbiglutide 50 mg
Exenatide 2 mg
Lixisenatide 20 µg
p=0.22
-2.87
-3.24
p<0.001
-2.68
-3.57
-0.60
-2.20
p<0.0001
p<0.01
-2.90
-3.60-3.67
-4.26
p=0.2347

Odds ratio of achieving composite end point with liraglutide 1.8 mg is superior, with *p<0.001; †p<0.01; ‡p<0.0001Odds ratio of achieving composite end point with liraglutide 1.2 mg is superior, with § p<0.0001HbA1c, glycosylated haemoglobin; SU, sulphonylurea; TZD, thiazolidinedione, LEAD: Liraglutide effect and action in diabetes.Zinman B et al. Diabetes Obes Metab 2012;14:77–82
Meta-analysis of LEAD program :Composite end point: HbA1c <7.0%, no weight gain, no hypoglycaemia
40
32
25
11
86
15
0
5
10
15
20
25
30
35
40
45
Liraglutide 1.8mg
Liraglutide 1.2mg
Exenatide Insulin glargine Sitagliptin SU TZD
Patients
Reachin
g
Com
posite E
nd P
oin
t (%
)
(n=1513) (n=1077)(n=186) (n=210) (n=447) (n=226)(n=225)
5.2‡3.7§
7.4 ‡5.2 § 10.5 ‡
7.4 §
3.7 ‡
2.0†


Summary
• Incretin-based therapies are considered early in the treatment in different guidelines
• Liraglutide is a human GLP-1 analogue with 97% homology to the native hormone
• Liraglutide is effective on glycaemic control without increasing risk of Hypoglycaemia and weight benefit.
• Compared with DPP-4I, GLP-1 receptor agonists are associated with greater reduction in HbA1c and weight loss and same vey low rate of Hypoglycaemia

45
THANK YOU