UCSF Clinical Enterprise Strategic Plan
82
UCSF Clinical Enterprise Strategic Plan Retreat 1 May 6, 2013 1
description
UCSF Clinical Enterprise Strategic Plan . Retreat 1 May 6, 2013. Retreat Agenda. UCSFCE Strategic Planning Process – Project Overview. February - April. August - October. May - July. 4. Clinical Enterprise Group & Steering Committee Meetings . - PowerPoint PPT Presentation
Transcript of UCSF Clinical Enterprise Strategic Plan

1
UCSF Clinical Enterprise Strategic Plan Retreat 1
May 6, 2013

2
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

3
UCSFCE Strategic Planning Process – Project Overview
May - July August - OctoberFebruary - April
4. Clinical Enterprise Group & Steering Committee Meetings
1. Engage USCF Leadership to
Define UCSFCE’s Vision & Strategic
Imperatives
2. Engage UCSF Community to
Develop Strategies & Tactics
3. Create Implementation Plan for Success

4
Leadership of the CE Strategic Planning Process
Executive Sponsors (M Laret, S Hawgood)
Clinical Enterprise Group (CEG)
Clinical Enterprise Strategic Planning (CESP) Steering Committee
Strategic Initiative Workgroups 1. Grow Complex Care Referrals Via Innovation &
Distinction2. Lead a High Value System of Care 3. Build a Culture of Continuous Process
Improvement 4. Strengthen Fiscal Position & Resource the Plan
• Teams of 15 – 20 faculty and clinical enterprise leaders that will recommend strategies, tactics and requirements to the CESP Steering Committee
• Teams will meet 5 times, between May – late July

5
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

A Health Plan View of the California Market
UCSF Clinical EnterpriseStrategic Planning Retreat
May 6, 2013
1

My Perspectives 8 Years of Consulting, Physician Practice Management
14 Years at Blue Shield of California• Strategic Planning• Network Contracting• Employer Sales and Account Management
Hill Physicians• 3 Weeks as Chief Operating Officer
2

What’s Important
Three most important priorities for health plans (and should be for the rest of the healthcare delivery system)…
1) Affordability2) Affordability3) Affordability
We’ve been discussing this for years, but now it is much, much more serious…
3

Drivers of Change
Social/Political Tipping Point• Health reform put healthcare front and center• Visibility/transparency of prices in the exchange• Sticker shock driven by health reform impacts• Premium rate setting legislation is being proposed
Employers are Struggling• Health insurance costs are equal or greater than the profit
margins of many companies• Health insurance costs = fully loaded salary of a software
programmer in India• Companies that compete in global industries can’t afford it
4

Drivers of Change (cont’d.)
The value proposition is not compelling• Prices of health insurance rise ~10% per year the last 15 years…
• About the same networks• About the same outcomes (that the system can show)• Similar member experience
One organization is providing a differentiated product: Kaiser
• More affordable• More integrated• More standardized• Attracting superior (healthier) risk
5

Erosion of Employer Based Coverage
6
AveragePremiums
2002 vs. 2012+169.7%
Inflation2002 vs. 2012
+32%
Political View: Health insurance inflation is the health plan’s fault
Reality: Health insurance inflation is due to health care cost inflation
71%
60%
2002 2012
% of
employersofferinghealth
coverage

Why will there be Sticker Shock?
Individual policies in the exchange will be expensive due to…• Risk selection (a big unknown)• 3:1 Age Rating• Benefit levels (“essential” benefits) Employer premium may also rise due to…• Age rating limitations• Essential benefits Few people today understand what health
insurance costs – the exchange will make it much more visible and politicians will react
7

The Challenge
How can our system achieve dramatically lower cost/trend and demonstrate quality and outcomes, while maintaining the vitality and innovation of individual provider organizations working together?
If we do not solve it, the government may try to solve it for us.
8

Implications
Plans/Hospitals/Physician Organizations must find ways to work together in an integrated manner…• Aligning incentives• Integrating data and using data to improve care• Building systems of care• Breaking down silos• Avoiding waste• Moving from reactive to proactive• Focusing on total cost of care for populations
9

Reasons for Optimism
Sacramento ACO for CalPERS• Blue Shield, Dignity Health, Hill Physicians• 0% trend year 1, dramatically lower trends years 2 and 3• Aligned incentives, focused attention• Leadership engaged at the highest level• Focusing on outcomes of system as a whole• Membership migration to the ACO
Before the ACO• 8-10% trends every year• Loss of members to Kaiser.
10

Reasons for Optimism (cont’d.)
ACO in San Francisco with Health Net, UCSF, Dignity Health and Hill Physicians• Started 1/1/13• Promising engagement• Sharing data• Aligned incentives• Focusing on improving care while managing costs
• UCSF has been a great partner !• Too early for results, but encouraging signs
11

Implications for Plans and Providers
Work closely together with aligned incentives – make decisions that drive a better overall outcome not maximize the result for one party/department/facility/group
Share and use data to move from fee-for-service fragmented care to population health management
Use new technologies and approaches to improve care, such as team-based care, use of secure messaging, in-home technologies
Change organizational structure and decision making to break down barriers and silos
Work with plans to design benefits with meaningful incentives for members to improve health status
12

Thoughts on UCSF
Incredible reputation and brand for high quality (and expensive) healthcare
A magnet for higher risk patients (e.g. in The Exchange), and very important to purchasers who are less price sensitive (e.g. high-tech companies)
Need to find a way to partner with others to combine broad-based and cost effective care in the community with high quality tertiary and quaternary care delivered by UCSF
Requires a difficult shift away from “heads in beds” and expensive clinical programs to finding ways to keep people healthy (and get paid for it)
Need to move away from cost shifting: compensating for inadequate Medicare and MediCal reimbursements by increasing margins on commercial insurance is killing the golden goose

Questions?

20
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

Academic Medicine for the Future
May 6, 2013UCSF Clinical Enterprise Retreat
Tom Enders, Managing DirectorManatt Health Solutions

22
NIH Doubling
HealthReform
Managed Care and Capitation
Despite dire predictions, the last two decades have been excellent for academic medicine
NIHStimulus
Innovation in Medicine — Aging of the Population — Specialty Services Boom
1990 1995 2000 2005 2010 2015
Gro
wth
of t
he A
MC
Mis
sion
s
Stoc
k M
arke
t B
ubbl
e20
03 –
200
8
Excellent Clinical Margins
Philanthropy Boom

23Erosion!
AMC
Relentless Forces
Defenses

24The AMC Business Model….
Talent2 x Pricing Power x (Enterprise
Costs)
AMC Sustainability
∫(Δ)(Technology Introduction - Diffusion) (Regulation)

25

26The Challenge of Change
Risk of change perceived as greatConnection to people who succeeded in the
old modelFear of lacking the competence to succeedOverloadHealthy skepticism about new ideasThe fear of hidden agendasFeeling of personal threat from the changesGenuine belief that “next generation” models
are a bad idea

27
Strategy

28Options for AMCs
Population Health Manager
Merge / Affiliate with Mega-System
Specialized Complex Care
Leader
High Performance Regional System
Regionally distributed health care system Risk bearing “population manager” Health Plan or payer partnership to supportClinically integrated network of faculty and community based physicians $ Multi-Billion Scale
Merge or establish primary preferred affiliation with large health system and become the “academic brand” for the system
Renown regional, national, international for a selected comprehensive specialty service (e.g. Cancer) Contractor to large systems Expert at Complex Care management Very strong Brand promise
Independent AMC with tightly controlled system of care in attractive geography Market share leader in an attractive “sub-regional” geography with “must-have” status Strong brand promise

29Clinical Strategies of Research Intensive AMCs
NIH RANK INSTITUTION1 JOHNS HOPKINS2 UCSF3 U MICHIGAN4 U PENNSYLVANIA5 U WASHINGTON6 U PITTSBURGH7 UCSD8 WASHINGTON UNIVERSITY9 YALE UNIVERSITY10 UNC CHAPEL HILL

30
Sufficient scale to build a regional system of care Highly differentiated programs of excellence
with well integrated basic & clinical research Economic alignment with physician, academic
and hospital partnersIncreasing integration of clinical servicesPrimary care & ambulatory care expansionSophisticated analytics and IT infrastructureMaximizing brand valueQuality: Measurable, Demonstrable, Superior
Some Consistent Themes

31
AMCSystem

32
Strategy
Organization Execution

33
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

34
Vision Questions
• What mission will our clinical enterprise meet?
• What will distinguish our clinical services and operating model from Kaiser? From Sutter? From Stanford?
• If the distinctiveness is innovation, what does that mean?
• Who will be part of the clinical enterprise? At what scale will we operate?
• Will we be independent or part of a system?
• What settings of care will be invested in?
• What payment model will we operate under and how will we succeed with it?

Clinical Enterprise SWOT
• Regional leader in select tertiary/quaternary services
• Research innovator• Talent and commitment• Capital investment in plant, IT• Nascent network development
Strength Weakness
Opportunity Threat35

• Regional leader in select tertiary/quaternary services
• Research innovator• Talent and commitment• Capital investment in plant, IT• Nascent network development
• Cost structure• Limited regional primary care• Hard to access specialists• Limited access to capital• Limited population health
experience or infrastructure• Highly federated governance
Strength Weakness
Opportunity Threat
Clinical Enterprise SWOT
36

• Regional leader in select tertiary/quaternary services
• Research innovator• Talent and commitment• Capital investment in plant, IT• Nascent network development
• Cost structure• Limited regional primary care• Hard to access specialists• Limited access to capital• Limited population health
experience or infrastructure• Highly federated governance
• Provider consolidation and competition
• Changing insurance models• New world challenging to our
‘core’ identity & competencies
Strength Weakness
Opportunity Threat
Clinical Enterprise SWOT
37

• Regional leader in select tertiary/quaternary services
• Research innovator• Talent and commitment• Capital investment in plant, IT• Nascent network development
• Cost structure• Limited regional primary care• Hard to access specialists• Limited access to capital• Limited population health
experience or infrastructure• Highly federated governance
• UCSF brand development• Trainer of the workforce• Nascent ACO experience• Regional relationships – getting to
scale
• Provider consolidation and competition
• Changing insurance models• New world challenging to our
‘core’ identity & competencies
Strength Weakness
Opportunity Threat
Clinical Enterprise SWOT
38

Proposed Vision as Developed by the Clinical Enterprise Group & Clinical Enterprise Strategic Planning Committee
UCSF will be Northern California’s preeminent high
value health system as defined by our success in
providing innovative, high-quality, cost-competitive
clinical services, and delivering an unparalleled
patient experience across the entire care continuum.
39

40
Vision: UCSF as the Preeminent High-Value System in Northern California
Wor
ld C
lass
Ed
ucati
on
Specialist Network
Home & Sub-Acute Care
Long-Term Care
UCSF
Cutti
ng E
dge
Rese
arch
High
-Val
ue, Q
ualit
y Cl
inic
al C
are
Strong Primary Care Teams
Clinical Research Implementation
Leading Acute Facilities
Regional T/Q Partnerships
Strategic Regional Expansion
Northern California System of Care

41
Strategic Priority 1:Grow Complex Care Referrals Via Innovation & Distinction
Patient Outcomes & Breakthrough
Research
System of Care with Referring Providers
Excellent Patient Experience

42
Strategic Priority 2: Lead A High Value System of Care
UCSF
Hospitals / Systems
(Marin General, UCSF oncology affiliates etc.)
Existing UCSF Distributed
Services
SCCIPAPediatric System
Kaiser? Other?
Physician Groups(Hill, One
Medical, etc.)
Existing Relationships On Which To Build
Relationships Under Development
Potential Transformation of Existing Relationship

43
Strategic Priority 3:Build a Culture of Continuous Process Improvement
Today:Organization in silos….
Tomorrow: Integrated organization that is high-quality and efficient

44
Enablers of UCSF’s Strategic Priorities and Vision
Build UCSF Brand
Lead in Precision Medicine
Align Financial and Administrative Operations
Establish Risk Management Capability
Apply Research to Clinical Care
Train and Recruit The Next Generation
Develop Physician Services

45
UCSFCE Vision
Grow Complex Care Referrals Via Innovation &
Distinction
Lead A High Value System of Care
Build a Culture of Continuous Process
Improvement
Build the UCSF Brand Lead in Precision Medicine Align Financial &
Administrative Operations Establish Risk Management
Capability
Apply Research to Clinical Care
Train & Recruit the Next Generation
Develop Physician Services
The preeminent high-value health system in Northern California
ENAB
LERS
S
TRAT
EGIC
PRI
ORI
TIES

46
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

47
UCSFCE Vision
Grow Complex Care Referrals Via Innovation
& Distinction
Lead A High Value System of Care
Build a Culture of Continuous Process
Improvement
Develop Physician Services Build the UCSF Brand Lead in Precision Medicine Establish Risk Management
Capability
Apply Research to Clinical Care Train & Recruit the Next
Generation Align Financial & Administrative
Operations
The Preeminent High-Value Health System in Northern California
ENAB
LERS
S
TRAT
EGIC
PRI
ORI
TIES

48
Imperatives
Transition from FFS to Risk-Based Contracting
Develop Population
Health Management Capabilities
Grow Bay Area Market
Share
Establish an Integrated Physician Platform
Deliver a World Class
Patient Experience

49
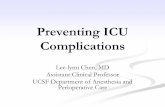
UCSF Market Position: Overall Bay Area Market Share - Adults
Adult IP Market Share – Bay AreaCY 2011; Market Discharges = 524,170
UCSF3% Stanford
4%
Kaiser Hospitals25%
Sutter19%
Dignity3%
Others45%
Source: UCSF Data Reports and OSHPD; Excludes MS-DRG 795Note: Counties included: San Francisco, Marin, Napa, Solano, Sonoma, San Mateo, Santa Clara, Alameda, Contra Costa
?

50
UCSF Overall Adult Market Share by County
Kaiser dominates the Bay area
markets and parts of Sacramento
Sutter is the second major player in SF County, and is very strong in the East
Bay and Sacramento
Stanford’s overall modest market strength
remains mostly in the South Bay and Central
Coast, but is aggressively moving into the East Bay
Dignity Health’s positioning is strongest in the Far North, Sacramento &
pockets of South Bay & Central Valley marketsUCSF’s Strongest
Overall Market Share
Filed Knox-Keene license to become a
full service health plan
Brown & Toland has an approved
Knox Keene license to manage
global risk
UCSF Overall Market Share
by County

51
Building on UCSF Regional Outreach
UCSF’s current outreach is strongest in the SF, North & East Bay markets and coastal areas of Far Northern CA. There may be opportunity to expand specialty
outreach to the south and east in order to build T/Q referrals
UCSF Overall Tertiary/Quaternary Market Share by
County

52
Establishing a Robust, Clinically Integrated Physician Network
South Bay – SCCIPA• Develop medical group
and establish a strong provider presence in the South Bay
• Enhance MSO capability
North Bay• Marin General/PRIMA
and Marin IPA are good partners and represent significant opportunities to build stronger ties
• Other regional relationships (Queen of the Valley and Santa Rosa Memorial) could be expanded further
East Bay• Children’s Oakland enhances
pediatric presence• Additional adult physician
partners are needed – Alta Bates and John Muir are well established options
SacramentoClose Coordination with UC Davis (and potentially Dignity) could help establish more integrated system in Sacramento, and across far North and Central Valley
UCSF Overall Market Share
by County

53
Ingredients of a High-Value System of Care
UCSF ACO
Analytics and Reporting
Governance and
PartnershipsPatient
Centered Care
Population Health
Management
Health Information Technology
Risk Contracts

54
Strategies to Promote Clinical Integration
1. Rapidly developing primary care physician practices employed by UCSFCE
2. Increasing the ability of the faculty practices to function in a highly effective group practice mode
3. Enhancing the scope and scale of clinical affiliates that are aligned and clinically integrated with the faculty practice and other employed UCSF physicians.
4. Building the relationship with SCCIPA so that it flourishes and provides UCSF a major position in the South Bay. Build stronger relationships with other IPAs.
5. Integrating Children’s Oakland physicians, enhancing the ability of the pediatric strategy to succeed

55
Measures of Success
Adapted from The Commonwealth Fund, Framework for a High Performance Health System for the United States, August 2006
High Quality- Medical Home
- Patient-Centered- Evidence-Based
Accessible- Timely
- Convenient- Affordable
Innovative- Continuous Improvement
- Translating Discovery
Efficient- Information Driven
- Right Care in the Right Environment
High-Value System of Care

56
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

Clinical Enterprise Financial View
UNDERSTAND & PROJECT THE FINANCIAL PERFORMANCE OF THE UCSF CLINICAL ENTERPRISE IN ITS ENTIRETY
Integrate Finance with StrategyLeverage scale of our EnterpriseAlign assumptions, planning, and decision
makingCreate new financial resources that will be
needed for investment in the strategy and our missions of research and education
57

UCSF Clinical Enterprise Financial View
Clinical Operating Margin
Expenses
Institutional & Technical
Revenue
Pro-Fee Revenue
58

UCSF Clinical Enterprise Financial View
Debt
Clinical Operating Margin
Clinical Departments Medical Center
Research and Education
Operating Expenses/Program
Investments and Reserves
Non-Operating Revenue/Philanthropy
Program and Capital
InvestmentsReserves
59

UCSF Clinical Enterprise Key AssumptionsFY 2013-FY22
(Medical Center and Medical Group)
VolumeInpatientOutpatient
0%-1.5% annually2.3-3.7% annually
Payor Mix FY 2013 Budgeted Payor Mix: 0.5% shift from Commercial to Government; additional 1% shift to Government in FY 2020 (1)
Net RevenueGovernmentCommercial
0%-2.5% annually4.0%-5.0% annually
Salaries (2) 3.0% annually (UCSF MG)3.0-%-4.7% annually (UCSF MC)
UCRP Benefits (Covered Comp Only)
12.8% in FY 201414.8% in FY 2015 and beyond
Net New Clinical Faculty 89 for FY 2013-FY 2023Increase to 3.6M from 3M wRVUs
Notes:(1) Base to be updated to the UCSF Medical Group historical payor mix(2) Variance in salary rate increases are reasonable due to the difference in staffing mix between the
UCSF Medical Group and the Medical Center
60

61
UCSF Clinical EnterpriseFY 2012 Actuals
Dollars (000's)UCSF Med
GroupMedical Center
Eliminating Entries
Consolidated Clinical
EnterpriseNon Medical
Group
Total Operating Revenue 575,338 1,581,631 (126,726) 2,030,243 1,327,037
Labor Expense 312,164 846,429 0 1,158,593 822,135Non Labor Expense 205,216 671,172 (89,788) 786,600 531,519Total Operating Expenses 517,380 1,517,601 (89,788) 1,945,193 1,353,654
Nonoperating Revenue 0 42,451 0 42,451 0
Excess of Revenue over Expenses 57,958 106,481 (36,938) 127,501 (26,617)
Changes in Net AssetsStrategic Support - School of Medicine 0 (27,870) 27,870 0 0Strategic Support - Cancer Center 0 (9,068) 9,068 0 0Other Strategic Support 0 (22,546) 0 (22,546) 0Total Changes in Net Assets 0 (59,484) 36,938 (22,546) 0
Excess Revenue after change in Net Assets 57,958 46,997 - 104,955 (26,617)
Margin % 10% 7% 6% - 2%

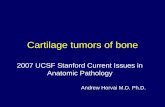
UCSF Clinical EnterpriseConsolidated Income Statement
*Projections based on FY 2013 Budget*Note: Medical Center margin is negative only in FY 2016; FY16-FY18 combined negative margin takes into account strategic support to Medical Group.
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 $(100,000.00)
$(50,000.00)
$-
$50,000.00
$100,000.00
$150,000.00
$87,234.00
$104,660.00
$4,380.00
$(75,916.00)
$(26,019.00)
$(3,457.00)
$18,170.00 $25,469.00
$52,274.00
$77,535.00
Revenue Minus ExpensesFY 2013 - FY2022
Reve
nue
Min
us E
xpen
ses
(000
’s)
62

Balance Sheet DetailsUCSF Medical Center
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Net Income Margin % (1) 5% 6% 1% - 2% 0% 1% 2% 2% 3% 3%
Debt Service Coverage (2) 3.6 3.9 3.3 3.3 4.0 4.2 4.7 4.8 4.4 4.6
Days Cash on Hand (2) 74 65 38 28 29 30 36 40 44 49
Notes: (1) Clinical Enterprise Net Income Margin (2) Medical Center Balance Sheet Indicators
63

UCSF Clinical EnterpriseMedical Center Net Income - Mitigation Strategies
($150,000)
($100,000)
($50,000)
$0
$50,000
$100,000
$150,000
FY 2013 FY 2014 FY 2015 FY 2016 FY 2017
Net Operating Income ($000's)
Net Income with Mitigation Net Income without Mitigation
FY 2013 FY 2014 FY 2015 FY 2016 FY 2017Revenue Enhancements 8,000 16,700 18,300 20,400 22,900 Expense Reductions 11,300 44,300 52,200 60,300 68,500
19,300 61,000 70,500 80,700 91,400
64

Dollars (000's) FY 2013 -
FY 2014 FY 2015 -
FY 2018 FY 2019 - FY 2022 (4)
Mission Bay Project (1) 734,626 327,132 APeX Electronic Medical Record (2) 21,815 - Strategic Investments 10,000 160,531
Renewals and ReplacementsInformation Technology 25,299 55,050 Equipment 29,695 69,087 Construction (3) 72,912 126,415 Sub- Total 127,906 250,552
Total 894,347 738,215 650,000
Notes:(1) Total Mission Bay Project $1.5B(2) Total APeX project $165M(3) Includes Backfill projects(4) Allocation among categories to be determined
UCSF Clinical EnterpriseMedical Center Capital Allocation Proposal
UCSFCE IS CERTAIN TO NEED MORE!!
65

UCSF Clinical Enterprise
A. Forecast Challenges B. Needs
• Downward pressure on reimbursement rates (Medi-Cal, Medicare, DSH, IME, insurance exchange)
• Pressure on professional fee margin to support sponsored research and education
• High pension and retiree health insurance rates
• Expanded fixed costs (i.e.. Mission Bay)
• State Budget impact (specifically on education and research)
• Philanthropy targets not met
• Strategic & Program Investment
• Capital demands for IT and routine replacement and infrastructure (i.e. non-clinical facilities needs)
• Capital investment issues• Limited or no debt capacity
66

67
UCSF Clinical EnterpriseBalancing Sources and Uses
How should these tradeoffs be optimizedwithin an appropriate credit and risk context?
Cash Debt
Capital Operations
How much cash?
How much capital?
How much debt?
How much profitability?Philanthropy and
Other Sources?
Source: Kaufman, Hall & Associates
67

Clinical Enterprise Financial View
Must anticipate significant investment requirements our current economics will be hard pressed to meet
We will need to increase the yield from operations….
….while developing new & creative sources of capital
Take-Aways:
68

69
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

70
Leadership of the CE Strategic Planning Process
Executive Sponsors (M Laret, S Hawgood)
Clinical Enterprise Group (CEG)
Clinical Enterprise Strategic Planning (CESP) Steering Committee
Strategic Initiative Workgroups 1. Grow Complex Care Referrals Via Innovation &
Distinction2. Lead a High Value System of Care 3. Build a Culture of Continuous Process
Improvement 4. Strengthen Fiscal Position & Resource the Plan
• Teams of 15 – 20 faculty and clinical enterprise leaders that will recommend strategies, tactics and requirements to the CESP Steering Committee
• Teams will meet 5 times, between May – late July

71
Retreat Break-Out Groups
• Break-out groups’ findings will be used to provide content to the CESP Work Groups
• Each break-out group will focus on one of 3 topics:1. Grow Complex Care Referrals Via Innovation & Distinction2. Lead a High Value System of Care3. Build a Culture of Continuous Process Improvement
• Break-out groups will have approximately 60 minutes to engage in discussion on an assigned set of questions.
• Group leaders have been assigned to each break-out group to facilitate and share the group’s findings

72
Breakout Group Assignments
Topic Tables Facilitators Support Location
1 A: Grow Complex Care Referrals Via Innovation & Distinction 3, 6 Mark Laret &
Talmadge King Tom Enders Conference Room 1
1 B: Grow Complex Care Referrals Via Innovation & Distinction 9, 10 Mike Hindery &
Peter Carroll Alex Morin Conference Room 2
2 A: Lead a High Value System of Care 4, 5 Kevin Grumbach &
Bruce Wintroub Jan NorrisMain Conference Room
2 B: Lead a High Value System of Care 1, 2 Sam Hawgood &
Ron Arenson Jonah FrohlichMain Conference Room
3 A: Build a Culture of Continuous Process Improvement 7, 8 Ken Jones & Jay
Harris Min Zhu Conference Room 3
3 B: Build a Culture of Continuous Process Improvement 11, 12 Barrie Strickland &
Tad Vail Megan IngrahamMain Conference Room

73
Retreat AgendaTime Activity Speaker
8:00am – 8:30
Welcome Overview of Opportunities & Challenges Facing UCSFCEBrief Summary of Planning ProcessPerspectives on the Clinical Strategy
Mark LaretJack Stobo
8:30 – 9:20 A Health Plan View of the California MarketDavid Joyner, Hill COO, formerly of Blue Shield
9:20 – 9:45 Academic Medicine for the Future Tom Enders, Manatt9:45 – 10:00 Break --10:00 – 10:30 Emerging UCSFCE Vision & Draft Strategic Priorities Sam Hawgood
10:30 – 11:10 Building a High Value System of Care in Northern California
Jonah Frohlich, Manatt----Mark Laret & Jay Harris (Q&A)
11:10 – 11:40 Clinical Enterprise Economics: Challenges & Opportunities
Barrie Strickland & Mike Hindery----Sam Hawgood (Q&A)
11:40 – 11:55BreakBoxed LunchesBreak to Tables
Tom Enders
11:55 – 1:15pm Retreat Participant Breakout Group Sessions Participants
1:15 – 2:00 Groups Report Out; Q&AClosing Discussion
M Laret, S Hawgood, T Enders

74
Retreat Breakout Groups # 1 A & B: Grow Complex Care Referrals Via Innovation & Distinction
For the next 5 years, specify the critical issues & solutions the Complex Care Work Group should address to advance innovation and build our complex care referrals
• What are the critical issues to be addressed?
• What break-through solutions should be put on the table for further exploration?

75
A “high value system of care” rests on the foundation of clinical and financial integration between physicians and health service providers across the community. With this in mind:
• How can we establish a strong foundation of clinical integration between UCSFCE and community-based physicians & other health care providers?
• What needs to change at UCSFCE in order to achieve a “high value system of care” that can manage the health of a population?
Retreat Breakout Group # 2 A: Lead a High Value System of Care

76
How could the UCSF Medical Center and clinical practices work together to accomplish building a true regional system of care?
• What strategic opportunities should be prioritized and pursued?
• What needs to change at UCSFCE in order to address the prioritized opportunities and successfully achieve a regional system of care?
Retreat Breakout Group # 2 B: Lead a High Value System of Care

77
Retreat Breakout Groups # 3 A & B: Build a Culture of Continuous Process Improvement
How can UCSFCE migrate to a culture where every single person in UCSF shares the imperative to achieve and deliver world class quality, cost, safety & patient experiences?
• How do we achieve the magnitude of change that will be required across the enterprise in order for us to be successful?

78
Appendix

79
UCSF Clinical EnterpriseConsolidated Income Statement
Projections based on FY 2013 Budget
Dollars (000's) 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Total Operating Revenue 2,121,245 2,180,007 2,255,421 2,371,033 2,487,320 2,597,608 2,706,395 2,801,507 2,919,776 3,041,681
Labor Expense 1,227,878 1,246,167 1,343,528 1,415,589 1,454,522 1,503,343 1,550,529 1,598,576 1,647,654 1,716,619Non Labor Expense 812,153 838,151 911,936 1,032,080 1,057,421 1,093,899 1,133,924 1,173,870 1,216,352 1,244,177Total Operating Expenses 2,040,031 2,084,318 2,255,464 2,447,669 2,511,943 2,597,242 2,684,453 2,772,446 2,864,006 2,960,795
Nonoperating Revenue 31,661 30,663 26,769 23,470 21,777 19,794 20,311 20,979 21,586 22,268
Excess of Revenue over Expenses 112,875 126,352 26,725 (53,166) (2,846) 20,160 42,254 50,040 77,355 103,153
Changes in Net AssetsStrategic Support - School of Medicine (3,634) (3,815) (4,006) (4,206) (4,417) (4,637) (4,869) (5,113) (5,368) (5,637)Strategic Support - Cancer Center 0 0 0 0 0 0 0 0 0 0Other Strategic Support (22,008) (17,876) (18,340) (18,544) (18,757) (18,979) (19,213) (19,458) (19,714) (19,983)Total Changes in Net Assets (25,641) (21,692) (22,346) (22,750) (23,173) (23,617) (24,083) (24,571) (25,082) (25,619)
87,233 104,660 4,379 (75,915) (26,019) (3,456) 18,171 25,469 52,273 77,534
Margin % 5% 6% 1% - 2% 0% 1% 2% 2% 3% 3%
Excess Revenue after change in Net Assets

80
Strategic Priority: Expand market position as a referral center for tertiary/ quaternary services* by achieving superior patient outcomes and efficiencies and continuously introducing innovation in the delivery of complex care throughout the UCSF health system
Objectives: • Consider the future state market dynamics regarding T/Q care in Northern California
and beyond• Define an approach that enables UCSF to deliver leading-edge, consistently
distinctive T/Q care to referral and network patients on an episode of care basis for specific services, with the necessary care management and outpatient care to achieve superior outcomes
• Consider how to succeed with bundles• Define an approach to demonstrate services’ outcomes and cost-effectiveness to
purchasers and patients • Consider how this model may align with an advanced partnership with Kaiser
Permanente
*Q/T services are defined based on the UC Health Tertiary / Quaternary Strategy, March 2013.
Workgroup 1: Grow Complex Care Referrals Via Innovation & Distinction

81
Workgroup 2: Lead a High Value System of Care
Strategic Priority: Transform health care delivery and partner with a network of Northern Californian hospitals and providers to create a comprehensive health care system accountable for a defined population’s health and providing a seamless continuum of coordinated, patient-centered, cost-effective care
Objectives: • Establish health care principles for the UCSF Health System, defining what it will stand for
and its value proposition to potential purchasers, leveraging external perspective as appropriate
• Define operating principles, the change management process, and accountability standards for a redesigned care model, including transformation of primary care into patient-centered medical homes, integration of care into service lines, and coordination across primary/secondary/TQ services and between inpatient, ambulatory, and community sectors.
• Define a regional network through partnership and outreach strategies, identifying specific types of target physician, hospital and sub-acute care partners in each region, the primary care capacity needed to care for the size of the targeted enrolled population for the health system, and the organizational models for an expanded physician network.
• Establish clinical integration among UCSF affiliated physicians – faculty and community physicians – for purposes of supporting value-based clinical practice, a lower-cost system of care and common payer contracting

82
Workgroup 3: Build a Culture of Continuous Process Improvement
Strategic Priority: Rigorously and unrelentingly apply data-driven process improvement principles to reduce waste and improve safety and quality
Objectives: • Define enterprise-wide principles to transform UCSFCE culture into one
committed to continuous process improvement and related accountability
• Develop approach to identifying and rolling out efficient practices across the enterprise
• Identify 2-3 process improvements to launch enterprise-wide as a pilot over the next 18 months