
PTSD in Children and Adolescents - UCSF CME · PTSD in Children and Adolescents Presented by Lynn...
67
PTSD in Children PTSD in Children and Adolescents and Adolescents Presented by Lynn Ponton, M.D. Presented by Lynn Ponton, M.D. Professor of Clinical Psychiatry Professor of Clinical Psychiatry UCSF UCSF
-
Upload
vuongthuan -
Category
Documents
-
view
214 -
download
0
Transcript of PTSD in Children and Adolescents - UCSF CME · PTSD in Children and Adolescents Presented by Lynn...
PTSD in Children PTSD in Children and Adolescentsand Adolescents
Presented by Lynn Ponton, M.D. Presented by Lynn Ponton, M.D. Professor of Clinical PsychiatryProfessor of Clinical Psychiatry
UCSFUCSF


IntroductionIntroduction Traumatic events often happen to Traumatic events often happen to children living in families and children living in families and communities. These events are neither communities. These events are neither isolated nor infrequent occurrences.isolated nor infrequent occurrences.
Key points• Traumatic events are a part of every child’s
life• Trauma happens to children living in
families and communities• ¼ of all children experience a significant
traumatic event before adulthood(Costello et al., 2002)
HISTORYHISTORY Severe emotional trauma has Severe emotional trauma has long been known to have long been known to have widespread effects on childrenwidespread effects on childrenEarly studies of trauma in children focused on disasters.
• 1943 Anna Freud, WWII, London Blitz• 1956 Block, Mississippi tornado• 1976 Newman, Buffalo Creek Flood• 1979 Terr, bus kidnapping

HISTORYHISTORY• Winnicott, a pediatrician and child psychoanalyst
who worked with Anna Freud, argued that trauma catastrophically destroys both the illusion of omnipotence in children and the idea that their parents could protect them. (1971)
• Following the development of PTSD as a diagnosis, child researchers, such as Van Der Kolk (1984), began to conceptualize PTSD as a neurophysiologic disorder with significant impact on brain function.
• There is also suggestion of genetic predispositions for PTSD, linking it to a child’s temperament and reactivity of the hypothalamic axis. (Perry 2001)


Diagnostic TimelineDiagnostic Timeline
• 1980 DSM first summarizes PTSD in adults
• 1987 DSM mentions PTSD in children and adolescents

Diagnostic Criteria for Diagnostic Criteria for 309.81 PTSD, DSM309.81 PTSD, DSM--IVIV
A.A. The child has been exposed to a traumatic The child has been exposed to a traumatic event in which both of the following were event in which both of the following were present:present:
1. The child experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others
2. The child’s response involved intense fear, helplessness, or horror. Note: In children, this Note: In children, this may be expressed instead by disorganized or may be expressed instead by disorganized or agitated behavioragitated behavior

Diagnostic Criteria for Diagnostic Criteria for 309.81 PTSD, DSM309.81 PTSD, DSM--IVIV
B.B. The traumatic event is persistently reexperienced in The traumatic event is persistently reexperienced in one (or more) of the following ways:one (or more) of the following ways:
1. Recurrent and intrusive distressing recollections of the event, including images, thoughts, or perceptions. Note: In young Note: In young children, repetitive play may occur in which themes or aspects ochildren, repetitive play may occur in which themes or aspects of f the trauma are expressed.the trauma are expressed.
2. Recurrent distressing dreams of the event. Note: In children, there Note: In children, there may be frightening dreams without recognizable content.may be frightening dreams without recognizable content.
3. Acting or feeling as if the traumatic event were recurring (includes a sense of reliving the experience, illusions, hallucinations, and dissociative flashback episodes, including those that occur on awakening or when intoxicated). Note: In young children, traumaNote: In young children, trauma-- specific reenactment may occur.specific reenactment may occur.
4. Intense psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event
5. Physiological reactivity on exposure to internal and external cues that symbolize or resemble an aspect of the traumatic event.

Diagnostic Criteria for Diagnostic Criteria for 309.81 PTSD, DSM309.81 PTSD, DSM--IVIV
C.C. Persistent avoidance of stimuli associated with the Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not trauma and numbing of general responsiveness (not present before the trauma), as indicated by three (or present before the trauma), as indicated by three (or more) of the following:more) of the following:
1. Efforts to avoid thoughts, feelings, or conversations associated with the trauma
2. Efforts to avoid activities, places, or people that arouse recollections of the trauma
3. Inability to recall an important aspect of the trauma4. Markedly diminished interest or participation in significant activities5. Feeling of detachment or estrangement from others6. Restricted range of affect (e.g., unable to have loving feelings)7. Sense of a foreshortened future (e.g., does not expect to have a
career, marriage, children, or a normal life span). In children and In children and adolescents, omens may be experienced.adolescents, omens may be experienced.

Diagnostic Criteria for Diagnostic Criteria for 309.81 PTSD, DSM309.81 PTSD, DSM--IVIV
D.D. Persistent symptoms of increased arousal (not present before Persistent symptoms of increased arousal (not present before the trauma), as indicated by two (or more) of the following:the trauma), as indicated by two (or more) of the following:
1. Difficulty falling asleep or staying asleep2. Irritability or outbursts of anger3. Difficulty concentrating4. Hypervigilance5. Exaggerated startle response
E.E. Duration of the disturbance (symptoms in Criteria B, C and D) isDuration of the disturbance (symptoms in Criteria B, C and D) is more than 1 month.more than 1 month.
F.F. The disturbance causes clinically significant distress or The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of impairment in social, occupational, or other important areas of functioning.functioning.
Specify if:• Acute: if duration of symptoms is less than 3 months old• Chronic: If duration of symptoms is 3 months or more• With Delayed Onset: If onset of symptoms is at least 6 months
after the stressor

Diagnostic Criteria for 308.3 Diagnostic Criteria for 308.3 Acute Stress Disorder, DSMAcute Stress Disorder, DSM--IVIV
A.A. The child has been exposed to a traumatic event in which both ofThe child has been exposed to a traumatic event in which both of the the following were present:following were present:
1. The child experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others
2. The person’s response involved intense fear, helplessness, or horror
B.B. Either while experiencing or after experiencing the distressing Either while experiencing or after experiencing the distressing event, event, the child has three (or more) of the following dissociative sympthe child has three (or more) of the following dissociative symptoms:toms:
1. A subjective sense of numbing, detachment, or absence of emotional responsiveness
2. A reduction in awareness of his or her surroundings (e.g., “being in a daze”)
3. Derealization4. Depersonalization5. Dissociative amnesia (i.e., inability to recall an important aspect
of the trauma)

Diagnostic Criteria for 308.3 Diagnostic Criteria for 308.3 Acute Stress Disorder, DSMAcute Stress Disorder, DSM--IVIVC.C. The traumatic event is persistently experienced in at least one The traumatic event is persistently experienced in at least one of the of the
following ways: recurrent images, thoughts, dreams, illusions, following ways: recurrent images, thoughts, dreams, illusions, flashback episodes, or a sense of reliving the experience; or diflashback episodes, or a sense of reliving the experience; or distress stress on exposure to reminders of the traumatic event.on exposure to reminders of the traumatic event.
D.D. Marked avoidance of stimuli that arouse recollections of the traMarked avoidance of stimuli that arouse recollections of the trauma uma (e.g., thoughts, feelings, conversations, activities, places, pe(e.g., thoughts, feelings, conversations, activities, places, people).ople).
E.E. Marked symptoms of anxiety or increased arousal (e.g., difficultMarked symptoms of anxiety or increased arousal (e.g., difficulty y sleeping, irritability, poor concentration, hypervigilance, exagsleeping, irritability, poor concentration, hypervigilance, exaggerated gerated startle response, motor restlessnessstartle response, motor restlessness
F.F. The disturbance causes clinically significant distress or impairThe disturbance causes clinically significant distress or impairment in ment in social, occupational, or other important areas of functioning orsocial, occupational, or other important areas of functioning or impairs impairs the individualthe individual’’s ability to pursue some necessary task, such as s ability to pursue some necessary task, such as obtaining necessary assistance or mobilizing personal resources obtaining necessary assistance or mobilizing personal resources by by telling family members about the traumatic experiencetelling family members about the traumatic experience
G.G. The disturbance lasts for a minimum of 2 days and a maximum of 4The disturbance lasts for a minimum of 2 days and a maximum of 4 weeks and occurs within 4 weeks of the traumatic eventweeks and occurs within 4 weeks of the traumatic event
H.H. The disturbance is not due to the direct physiological effects oThe disturbance is not due to the direct physiological effects of a f a substance (e.g., a drug abuse, a medication) or a general medicasubstance (e.g., a drug abuse, a medication) or a general medical l condition, is not better accounted for by Brief Psychotic Disordcondition, is not better accounted for by Brief Psychotic Disorder, and er, and is not merely an exacerbation of a preexisting Axis I or Axis IIis not merely an exacerbation of a preexisting Axis I or Axis II disorderdisorder

Symptoms of PTSD more common Symptoms of PTSD more common in children, Highlighted in DSMin children, Highlighted in DSM--IVIV• Their initial response may be expressed by
disorganized or agitated behavior instead of intense fear or helplessness
• Repetitions in children may occur in the form of repetitive play with traumatic themes
• Trauma-specific reenactments are more likely to occur
• Frightening dreams without recognition of their content
• Omens are more frequently experienced

Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: Diagnostic IntervalsDiagnostic Intervals• Acute Stress
Disorder (ASD)• Acute PTSD• Chronic PTSD• Complex PTSD*
• Within 4 weeks
• 1-3 months• More than 3 months• More than 3 months
-AACAP Practice Parameters, 2007
*Complex PTSD is Chronic PTSD with co-morbid conditions

Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: Other Diagnoses to ConsiderOther Diagnoses to Consider
• ADHD• Oppositional Defiant
Disorder (ODD)• Panic Disorder• Social Anxiety
Disorder• Obsessive
Compulsive Disorder
• Phobias• General Anxiety
Disorder (GAS)• Depression• Psychotic Disorders• Medical conditions
– Hyperthyroidism– Asthma– Seizure Disorders
Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: Ongoing DebatesOngoing Debates
• There is ongoing discussion about the validity of DSM-IV-TR diagnosis criteria for children and adolescents, particularly the requirement for three avoidance/numbing symptoms in younger children (Criterion C)
• PTSD symptoms require the child to report on complex internal states, conditions difficult for children to report and for parents to observe
(Scheeringa et al., 2006)

Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: GuidelinesGuidelines
• The diagnosis of PTSD requires a child or adolescent to describe a traumatic event and specific symptoms or the presence of other compelling evidence. Compelling evidence might include the presence of a sexually transmitted disease in a young child, a reliable eye witness, or forensic support.
• In the absence of a child report or other compelling evidence, the diagnosis should not be made.
• Instead, the child’s symptoms should be well- described
-AACAP Practice Parameters, 2007
Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: GuidelinesGuidelines• Any psychiatric assessment of children and
adolescents should routinely include questions about traumatic experiences and PTSD symptoms
• Developmentally appropriate language• DSM-IV criteria highlighting child factors with
attention to a child’s developmental age• Questioning both parents and children• Scales can assist in diagnosis, but interviews are
key• A search for confirmatory evidence• Consideration of co-morbid diagnoses

Diagnosis of Child PTSDDiagnosis of Child PTSD• Many PTSD symptoms are highly internalized,
abstract and not easily observable in contrast to the symptoms of depression and ADHD.
• In one study, 88% of PTSD symptoms were not observable from non-focused clinical examination of young children. (Costello et al., 2002)
• It is important to interview child and parents separately and jointly.
• Ask questions tailored to the traumatic event(s) and in words that they can understand – “When you went by the house where the event occurred, did you get upset?”
• For younger children use happy-sad faces or a fear thermometer

Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD:PTSD: Scales that can assist in screeningScales that can assist in screening
• UCLA PTSD index(Steinberg et al., 2004)
• Child PTSD Symptom Scale(Foa et al., 2001)
*The diagnosis is made by clinical interview of the child and the parents.

1.1. I get upset, afraid or sad when something makes me I get upset, afraid or sad when something makes me think about what happened.think about what happened.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
2.2. I have upsetting thoughts or pictures of what happened I have upsetting thoughts or pictures of what happened come into my mind when I do not want them to.come into my mind when I do not want them to.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
3.3. I feel grouchy, or I am easily angered.I feel grouchy, or I am easily angered.None Little Some Much MostNone Little Some Much Most
0 0 1 1 2 2 3 3 44
4.4. I try not to talk about, think about, or have feelings I try not to talk about, think about, or have feelings about what happened.about what happened.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
5.5. I have trouble going to sleep, or wake up often during I have trouble going to sleep, or wake up often during the night.the night.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
6.6. I have trouble concentrating or paying attention.I have trouble concentrating or paying attention.None Little Some Much MostNone Little Some Much Most
0 0 1 1 2 2 3 3 44
7.7. I try to stay away from people, places, or things that I try to stay away from people, places, or things that make me remembers what happened.make me remembers what happened.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
8.8. I have bad dreams, including dreams about what I have bad dreams, including dreams about what happened.happened.
None Little Some Much MostNone Little Some Much Most0 0 1 1 2 2 3 3 44
9.9. I feel alone inside and not close to other people.I feel alone inside and not close to other people.None Little Some Much MostNone Little Some Much Most
0 0 1 1 2 2 3 3 44
Abbreviated UCLA PTSD Reaction Index for DSMAbbreviated UCLA PTSD Reaction Index for DSM--IVIV

EPIDEMIOLOGYEPIDEMIOLOGY

EpidemiologyEpidemiology• Different studies report varying rates of PTSD in
childhood• Examples indicating range:
Lifetime prevalence for PTSD in adolescence: 9.2% (Breslau et al., 1991)1.6% (Essau et al., 2000)
• Studies (McFarlane, 1987 and Scheeringa, et al. 2005) show that PTSD, once diagnosed, is still present at 18-24 months, if untreated.
• In the U.S. alone 5 million children each year are victims or witnesses to violent trauma. (Perry, 2001)
• ¼ of all children experience a significant traumatic event before adulthood (Costello et al., 2002)

Risk factors for PTSDRisk factors for PTSD• Female gender• Past trauma exposure• Greater exposure to the index trauma (amount,
proximity)• The presence of a pre-existing psychiatric disorder,
particularly an anxiety disorder• Parental psychopathology• Parental lack of support
(Pine and Cohen, 2002)• Witnessing threat to caregiver
(Scheeringa et al., 2006)• Following a disaster:
a) Increased television viewing of the disasterb) Delayed evacuation of the disaster-areac) Life or family member’s life in danger
(Pfefferbaum et al., 1991)

Diagnosis of Child and Adolescent Diagnosis of Child and Adolescent PTSD confers increased risk for:PTSD confers increased risk for:• Smaller cerebral volume and corpus
colossi (Debellis et al., 1996)
• Lower academic scores(Saigh et al., 1997)
• Child sexual abuse is associated with increased rates of sexual risk-taking, substance abuse, conduct disorder, depression and suicide
(Fergusson et al., 1996)

THEORYTHEORY

TheoryTheoryA theoretical understanding of PTSD in children and adolescents is aided by a developmentally-informed integrational approach. Neurobiological information, cognitive-behavioral knowledge, an openness to philosophical perspectives and a dynamic relational understanding of a child’s life in their family and cultural community combine to promote understanding of treatment.
PTSD: Combinations of PTSD: Combinations of Hyperarousal and DissociationHyperarousal and Dissociation• Arousal Alarm Fear• Frontal cortex shuts down and non-
verbal cues are the focus• Dissociation may involve the child
curling up into a ball, preparing the body for possible injury. The heart rate may be decreased and opioids released
(Perry and Szalavitz, 2006)

Revised theories of PTSD integrate an understanding of the abnormal processing of traumatic memories and poor organization of autobiographical memories. The memories are triggered as if they are happening in the present and not in the past. From this perspective, therapy focuses on re-organizing these memories.
(Ehlers and Clark, 2000)

TREATMENTTREATMENT

Treatment of Children and Treatment of Children and Adolescents with PTSDAdolescents with PTSD
• First-step management
• Psychotherapy
• Medications
• Eye Movement Desensitization and Reprocessing (EMDR)

FirstFirst--step: Identification and step: Identification and Management of SymptomsManagement of SymptomsWhen a child or adolescent has been exposed to a traumatic incident, (i.e. in an emergency room or a disaster relief situation) healthcare professionals should inform the parents about the risk for PTSD. This should be accompanied by a brief description of the most likely symptoms and an information sheet about what to expect.

FirstFirst--step: Identification and step: Identification and Management of SymptomsManagement of Symptoms
The “Facts for Families”, “Helping Your Child After a Disaster” and “Post-Traumatic Stress Disorder” prepared by the American Academy of Child and Adolescent Psychiatry offer this information and can be disseminated. (Available in several languages – used worldwide)

StageStage--Based Treatment of PTSD Based Treatment of PTSD for Children and Adolescentsfor Children and Adolescents
First HoursFirst Hours
DaysDays
Months/YearsMonths/Years
•• FirstFirst--Step Management: Evaluation and traumaStep Management: Evaluation and trauma-- focused support for children and parentsfocused support for children and parents
•• FrontFront--Line Education: Hotlines, media, one:one Line Education: Hotlines, media, one:one consultationconsultation
•• Consider SSRIConsider SSRI’’s and alphas and alpha--adrenergic blockers adrenergic blockers for adolescents and parents following early for adolescents and parents following early screeningscreening
•• Trauma diaries and drawing picturesTrauma diaries and drawing pictures---------------------------------------------------------------------------------•• Evaluation and traumaEvaluation and trauma--focused support for parents focused support for parents
and children and children •• Ongoing education for parents and childrenOngoing education for parents and children•• TraumaTrauma--focused CBT for children, adolescents and focused CBT for children, adolescents and
parentsparents•• Psychiatric Evaluations for Children and ParentsPsychiatric Evaluations for Children and Parents---------------------------------------------------------------------------------•• TraumaTrauma--focused group, individual and family focused group, individual and family
therapytherapy•• Complex medication evaluations consideringComplex medication evaluations considering•• (SSRI(SSRI’’s and other medications including support for s and other medications including support for
sleep disturbances) sleep disturbances) •• LongLong--term education efforts regarding longterm education efforts regarding long--term term
problemsproblems•• Continue to look for coContinue to look for co--morbid diagnosesmorbid diagnoses•• Individual, family and group psychotherapyIndividual, family and group psychotherapy
Traumatic Event: TreatmentTraumatic Event: Treatment

TraumaTrauma--focused Cognitive focused Cognitive Behavioral Therapy (a version)Behavioral Therapy (a version)
1. Collaboration between parents and therapist and child therapist – a trusting relationship must be established
2. Psychoeducation: the therapist explains both to child and parents, in a developmentally appropriate manner, the etiology, symptoms and treatment
3. Exposure, both imaginal and in vivo, gradually decreasing a child’s fears
4. Anxiety is graded by a fear thermometer (0-10)5. Relaxation techniques may be used to decrease anxiety6. The therapist helps the child to tell and re-organize their
trauma narrative, modifying negative thoughts and reducing avoidance
7. The meaning that the traumatic memory has for them is understood and dysfunctional beliefs are modified
(Vickers B et al., 2005)

An Integrated Treatment ModelAn Integrated Treatment Model
Child-Parent Psychotherapy with Young Children Exposed to Violence
(Liberman A, 2006)
Violence in domestic situations with younger children results in loss of security for the child and the parent alike, doubles the rate of psychiatric problems and negatively changes the parent-child relationship. Following violence, the parent and child may act as traumatic reminders to each other with mutual negative attributions and impaired affect regulation

MultiMulti--Theoretical/IntegrationalTheoretical/Integrational
• Developmentally Informed• Attachment• Psychoanalytic• Social Learning• Cognitive-Behavioral
(Lieberman A, 2006)

ChildChild--parent Psychotherapy parent Psychotherapy Intervention ModalitiesIntervention Modalities
1. Promote developmental progress through play, physical contact, and language
2. Unstructured/reflective developmental guidance
3. Modeling protective behaviors4. Interpretation: linking past and present5. Emotional support6. Concrete assistance, case management,
crisis intervention(Lieberman A, 2006)

ChildChild--Parent Psychotherapy GoalsParent Psychotherapy Goals• Encouraging normal development:
engagement with present activities and future goals
• Maintaining regular levels of affective arousal
• Establishing a trust in bodily sensations
• Achieving reciprocity in intimate relationships
(Lieberman A, 2006)

ChildChild--Parent Psychotherapy Parent Psychotherapy TraumaTrauma--Related GoalsRelated Goals
• Increased capacity to respond to threat• Differentiation between reliving and
remembering• Normalization of the traumatic
response• Placing the traumatic experience in
perspective(Lieberman A, 2006)

Treatment of Child and Adolescent Treatment of Child and Adolescent PTSD with MedicationsPTSD with Medications
Key PointsKey Points1. There are few randomized controlled trials, but several clinical trials have
been completed2. Early treatment of anxious arousal with Beta-blockers (10-100 mg PO
daily) may decrease acute symptoms of anxiety and/or prevent the development of the disorder (Off-label-prescribing)
3. Treatment of symptoms at any point with Selective Serotonin Reuptake Inhibitors (low-full dose). These medications also treat associated depression, panic attacks and sleep disturbance. (Sertraline (12.5-200 mg) and paroxetine (5-50 mg) are FDA-approved with adults for treating PTSD and other symptoms).
If children and adolescents are treated with SSRIIf children and adolescents are treated with SSRI’’s it is important to be aware of:s it is important to be aware of:Black Box Data:Black Box Data: A recent meta-analysis of suicidal ideation and behavior in placebo-controlled clinical trials of paroxetine in adult patients with Major Depressive Disorder and other psychiatric disorders showed a higher frequency of suicidal behavior in young adults treated with paroxetine as compared with placebo. It is vital to carefully monitor young adult patients treated with paroxetine and other SSRI’s. “Start low and go slow” in both directions to avoid increased arousal and unwanted side effects.

Treatment of Child and Adolescent Treatment of Child and Adolescent PTSD with MedicationsPTSD with Medications
4. Antiseizure medications such as carbamazepine (200-800 mg daily) may be used to treat anger and behavioral problems associated with PTSD.
5. Benzodiazepines such as clonazepam (.25-2 mg daily) can be used on a temporary basis to treat associated anxiety, but pose several problems. Withdrawal and aggravation of symptoms in adolescents are serious concerns.
6. Major tranquilizers such as risperidone (.25-1 mg daily) can be used to reduce associated anxiety, disorganization and psychotic features
7. Buspirone (a 5-HT receptor agonist) has successfully treated anxiety in adolescents (5-60 mg). There are no trials with PTSD.

8. Clinical Studies of PTSD Symptoms in Children and Adolescents with Atypical Antipsychotics (off-label uses)• Stathis et al, 2005 – 6 week open label study of
quetiapine (50-200 mg). Six adolescents with PTSD showed decreased symptoms of dissociation, anxiety, depression and anger. No side effects noted.
• Kant et al, 2004. Nineteen adolescents with refractory PTSD were treated with clozapine (mean dose 102 mg/day). Symptom reduction but many side effects among them weight gain, agranulocytosis, neutropenia and sedation.
• Harrigan and Barnhill (1999) – 15 of 18 children with PTSD and co-morbid bipolar disease or ADHD showed large decreases in symptoms with risperidone (mean dose 1.37 mg/day) No side effects noted.
Treatment of Child and Adolescent Treatment of Child and Adolescent PTSD with MedicationsPTSD with Medications

Treatment of PTSD in children and Treatment of PTSD in children and adolescents:adolescents: Eye Movement Desensitization and Eye Movement Desensitization and Reprocessing (EMDR)Reprocessing (EMDR)• Based on theoretical model – dysfunctional
intrusions, emotions and physical sensations are due to improper storage of traumatic events in implicit memory.
• Treatment consists of eliciting specific targets to represent the traumatic events, triggers and future templates for better function.
(Shapiro, 2001)Question: Is it the cognitive therapy component Question: Is it the cognitive therapy component that is helpful?that is helpful?

MetaMeta--analysis of Psychotherapy analysis of Psychotherapy with PTSD in Adultswith PTSD in Adults
• Brief psychotherapies for PTSD produce substantial improvement. Of patients who complete treatment, 67% no longer meet criteria for PTSD.
• Of those who enter treatment (whether or not they complete), the recovery rate is 56%.
• Most studies do follow-up only through 6 months. Studies are planned with children and adolescents.
(Bradley et al., 2005)

High Risk Situations for High Risk Situations for Child and Adolescent PTSDChild and Adolescent PTSD
1. Pediatric Intensive Care Unit and serious medical illnesses
2. Having a Developmental Disability3. Physical and sexual abuse plus
witnessing violence at home and in communities
4. Exposure to man-made and natural disasters
5. War, terrorism and refugee status

PTSD in the Pediatric ICUPTSD in the Pediatric ICU• Children, adolescents and their
parents in ICU settings are at increased risk for PTSD during and after their stay
• Injury, illness, treatment and separation from family all contribute to PTSD in the ICU setting
(Ward-Begnoche, 2007)

PTSD in the Pediatric ICUPTSD in the Pediatric ICU Symptoms persist after dischargeSymptoms persist after discharge
• In one study, 75% of children and adolescents presented with PTSD symptoms on admission
• 50% had depressive or anxiety disorders
• 17% had symptoms three months later
(Ward-Begnoche et al., 2007)

PTSD in the Pediatric ICUPTSD in the Pediatric ICU• Treatment for parents and minimizing exposure
to other children’s trauma is key.(Ward-Begnoche et al., 2007)
• Moderate dose risperidone has been used to treat preschool children in clinical trials
(Meighen et al., 2007)
• Treat pain adequately(Mizra et al., 1998)

Summary: Key Points in Summary: Key Points in Child and Adolescent PTSDChild and Adolescent PTSD
1. Traumatic events happen to children living in families and communities. They are not isolated events.
2. Children develop in relationships. They use relationships to regulate stress. When children’s relationships are affected by traumatic events (either from outside or within) they lose their ability to regulate their affects and their behaviors, and physiological responses.

Summary: Key Points in Child Summary: Key Points in Child and Adolescent PTSDand Adolescent PTSD
3. Although the same diagnostic criteria (DSM-IV- TR) are used for children and adults, there are differences in symptom presentation. Disorganized, agitated behavior, repetitive play and re-enactments, time skew and omens are more frequent in children.
4. The strict “avoidance” criteria (Category C) are less frequently reported in children, but may be manifested differently.
5. PTSD in adolescents is more likely revealed by traumatic re-enactments and dangerous risk- taking.

Summary: Key Points in Summary: Key Points in Child and Adolescent PTSDChild and Adolescent PTSD
6. In children under 3, PTSD symptoms are less frequently seen, in part, because they have to be verbalized. Traumatic play and separation or stranger anxiety are more common. Parental report modified scales and compelling evidence are key in diagnosis. Interviewers experienced in working with younger children are key.
7. Untreated PTSD has serious consequences for children. Early diagnosis and treatment is key.

Summary: Key Points in Summary: Key Points in Child and Adolescent PTSDChild and Adolescent PTSD
8. Comorbid Diagnoses are common with PTSD and must also be addressed and treated.
9. Research-controlled trials on treatment and prevention continue to be conducted and are yielding important information
10.Treatment of PTSD in children and adolescents is aided by a developmentally-informed integrational approach. Neurobiological information, cognitive behavioral knowledge, an openness to philosophical perspectives and a dynamic relational understanding of a child’s life in their family and community must be considered.

BenjieBenjie: A Case in the ICU: A Case in the ICUCC: Mute, eight year-old boy following a car accident where several members of his family were killed, including two siblings. His parents are alive, but seriously injured and in another hospital. Benjie has several fractures that are healing, but is unable to talk.
Consult questions:Consult questions:•• Is he depressed? Is he depressed? •• Does he need medications?Does he need medications?•• Can you help him talk?Can you help him talk?

Assessment and DiagnosisAssessment and Diagnosis• Phone interview with parents who reveal details
about the car accident and earlier history of Benjie’s life.
• In-person interview with aunt, uncle and a 14 year- old sister who were not in the accident.
• Check adequacy of pain medications.• Review diagnostic criteria for ASD, PTSD,
bereavement, selective mutism, separation anxiety disorder, communication disorders and major depressive disorder.
• Symptom checklist filled out by Benjie’s primary nurse
• Medical tests have ruled out medical etiologies for Benjie’s silence.

Early Interventions and Early Interventions and Continued AssessmentContinued Assessment
• An initial phone call is arranged with Benjie and his mother. Their primary nurses and Benjie’s therapist are present. Benjie cries, but does not speak. Daily calls are begun.
• Benjie’s symptoms fit selective mutism and major depressive disorder and he is also grieving, although has not yet been told about his two siblings.

In addition, In addition, BenjieBenjie meets the meets the following criteria for PTSD:following criteria for PTSD:
A. Witnessed the death of his two siblings and experienced fear and helplessness, verified by parents.
B. Re-experiencing symptomsIntense psychological distress at cues that remind him of trauma.
C. Avoidance1. Efforts to avoid thoughts, feelings and conversations about
trauma2. Inability to recall events related to trauma3. Decreased interest in significant activities4. Restricted range of affect
D. Symptoms of Arousal1. Difficulty falling asleep2. Difficulty concentrating3. Hypervigilence4. Exaggerated startle response

Continued InterventionsContinued Interventions1. Low doses of an SSRI are added and within 4-5 days
his hypervigilence and exaggerated startle are decreased.
2. Benjie develops sign language with his therapist and begins to hum in sessions.
3. Following a session where he draws a picture of the accident, he says a few words.
4. Several days later, his parents are able to visit him for the first time. They tell him his two siblings are dead.
5. Family sessions are held with Benjie, his grieving parents and their parist priest.
6. Benjie leaves the hospital with two casts, but speaking and continues treatment outside of the hospital.

PREVENTIONPREVENTION
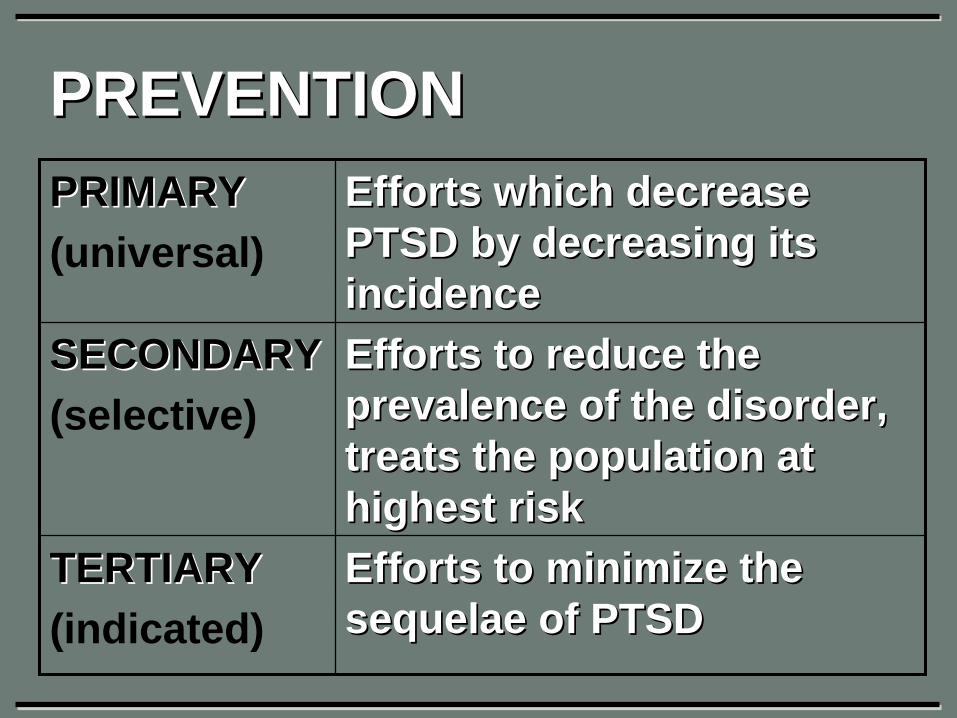
PREVENTIONPREVENTIONPRIMARYPRIMARY(universal)
Efforts which decrease Efforts which decrease PTSD by decreasing its PTSD by decreasing its incidenceincidence
SECONDARYSECONDARY(selective)
Efforts to reduce the Efforts to reduce the prevalence of the disorder, prevalence of the disorder, treats the population at treats the population at highest riskhighest risk
TERTIARYTERTIARY(indicated)
Efforts to minimize the Efforts to minimize the sequelaesequelae of PTSDof PTSD

Prevention Efforts with PTSD Prevention Efforts with PTSD and Childrenand ChildrenPRIMARYPRIMARY(universal)
GunGun--control efforts, postcontrol efforts, post-- disaster media effort, seat disaster media effort, seat beltsbelts
SECONDARYSECONDARY(selective)
School and community School and community based intervention based intervention programs, postprograms, post--disaster disaster intervention effortsintervention efforts
TERTIARYTERTIARY(indicated)
Most treatment effortsMost treatment efforts
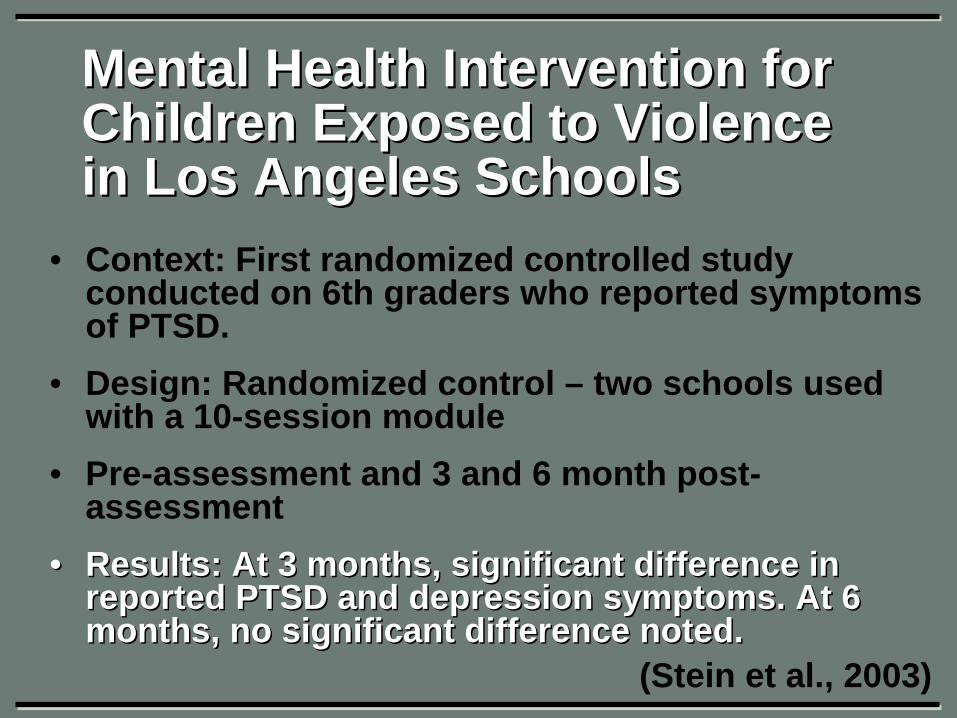
Mental Health Intervention for Mental Health Intervention for Children Exposed to Violence Children Exposed to Violence in Los Angeles Schoolsin Los Angeles Schools
• Context: First randomized controlled study conducted on 6th graders who reported symptoms of PTSD.
• Design: Randomized control – two schools used with a 10-session module
• Pre-assessment and 3 and 6 month post- assessment
•• Results: At 3 months, significant difference in Results: At 3 months, significant difference in reported PTSD and depression symptoms. At 6 reported PTSD and depression symptoms. At 6 months, no significant difference noted.months, no significant difference noted.
(Stein et al., 2003)

Cognitive BehavioralCognitive Behavioral Intervention in Intervention in Los Angeles Schools (10 sessions)Los Angeles Schools (10 sessions)
SESSION PROGRESSIONPROGRESSION1 Introduction, explanation of trauma and treatmentIntroduction, explanation of trauma and treatment
2 Relaxation training, education about common reactions Relaxation training, education about common reactions to traumato trauma
3,4 Fear thermometer, combat negative thoughts, links Fear thermometer, combat negative thoughts, links between thoughts and feelings.between thoughts and feelings.
5 Alternative coping strategiesAlternative coping strategies6,7 Exposure to trauma memories through drawing.Exposure to trauma memories through drawing.8 Introduction to social problemIntroduction to social problem--solvingsolving9 Practice with problemPractice with problem--solving and hotsolving and hot--seatseat10 GraduationGraduation
(Stein et al., 2003)

REFERENCESREFERENCES1. American Academy of Child and Adolescent Psychiatry (2007). Practice Parameter for the
Assessment and Treatment of Children and Adolescents with Posttraumatic Stress Disorder, Washington, D.C., Author
2. American Psychiatric Association, (1994) Diagnostic and Statistical Manual of Mental Disorders (4th ed.) Washington, D.C. Author
3. Block D, Siber E, Perry S (1956). Some factors in the emotional reaction of children to disaster, Am J. Psychiatry 113:416-422
4. Breslau, N Davis C6 Audeski P, Peterson (1991). Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry. 48: 216-222
5. Costello EJ, Erkanli A, Fairbank JA, Angold A (2002). The prevalence of potentially traumatic events in childhood and adolescence. J Trauma Stress 15:99-112
6. DeBellis MD, Keshevan MS, Clark DB, et al. (1996). Developmental traumatology, part II: brain development. Biol Psychiatry 45:1271-1284
7. Ehlers, A & Clark, DM (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319-45.
8. Essau CA, Conradt J, Petermann F (2000). Frequency, comorbidity, and psychosocial impairment of anxiety disorders in German adolescents. J Anxiety Disorders. 14(3), 263- 79.
9. Fergusson DM, Horwood J, Lynskey MT (1996). Childhood sexual abuse and psychiatric disorder in young adulthood; II: Psychiatric outcomes of childhood sexual abuse. J Am Acad Child Adolesc Psychiatry 34:1365-1374
10. Foa EB, Treadwell K, Johnson K, Feeny NC (2001). The Child PTSD Symptom Scale: a preliminary examination of its psychometric properties. J Clin Child Psychol 30:376-384
11. Freud, A, Burlingham DT (1943). War and Children, Medical War Books, London12. Horrigan JP, Barnhill LJ (1999). Risperidone and PTSD in boys. J Neuropsychiatry Clin
Neurosci 11:126-127

REFERENCESREFERENCES
13. Kant R, Chalansani R, Chengappa KN, Dieringer MF (2004). The off-label use of clozapine in adolescents with bipolar disorder, intermittent explosive disorder, or posttraumatic stress disorder. J Child Adolesc Psychopharmacol 14:57-63
14. Lieberman, A (2006). Child-Parent Psychotherapy with young children exposed to violence, Presented at UCSF
15. McFarlane, AC (1987). Posttraumatic phenomena in a longitudinal study of children following natural disaster, J Am Acad. Child Adol. Psychiatry 26:764-69
16. Meighen, KG, Hines, LA, Lagges, AM (2007). Risperidone treatment of preschool children with thermal burns and acute stress disorder. J Child Adolesc Psychopharmacol, 17(2), 223-32.
17. Mirza KAJ, Bhadrinath BR, Goodyer IM, Gilmour C. (1998). Post-traumatic stress disorder in children and adolescents following road traffic accidents. British Journal of Psychiatry, 172, 443-447.
18. Newnan, CJ (1976). Children of Disaster: Clinical Observations at Buffalo Creek, Am J. Psychiatriy, 133: 306-312
19. Perry B, Szalavitz M (2006) The boy who was raised as a dog: And other stories from a child psychiatrist’s notebook. New York: Basic Books.
20. Perry B (2001). Incubated in Terror: Neurodevelopmental Factors in the Cycle of Violence, Presented at UCSF
21. Pfefferbaum B, Nixon SJ, Krug RS, et al.(1999). Clinical needs assessment of middle and high school students following the 1995 Oklahoma City bombing. Am J Psychiatry 156:1069-1074
22. Pine DS, Cohen JA (2002). Trauma in children and adolescents: risk and treatment of psychiatric sequelae. Biological Psychiatry, 51(7), 519-31.
23. Saigh PA, Mroveh M, Bremner JD (1997). Scholastic impairments among traumatized adolescents. Behav Res Ther, 35:429-436
REFERENCESREFERENCES24. Scheeringa MS, Wright MJ, Hunt JP, Zeanah CH (2006). Factors affecting the diagnosis and
prediction of PTSD symptoms in children and adolescents. Am J Psychiatry 163:644-65125. Scheeringa MS, Zeanah C, Myers L, Putnam F (2005). Predictive validity in a prospective
follow up of PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 44:899-90626. Shapiro F (2001). Eye-movement desensitization and reprocessing, basic principles,
protocols and procedures, 2nd edition. New York: Guilford Press. 27. Stein B, Jaycox L, Kataoka S, Wong M, Tu W, Elliot M, Fink A (2003). A Mental Health
Intervention for Schoolchildren Exposed to Violence: A Randomized Controlled Trial. Journal of the American Medical Association, 290(5), 603-611)
28. Steinberg A, Brymer M, Decker K, Pynoos R (2004). The UCLA PTSD Reaction Index. Curr Psychiatry Rep 6:69-100
29. Terr L, (1979). Children of Chowchilla: a study of psychic trauma. The Psychoanalytic study of the child, 34: 547-623
30. Stathis S, Martin, G, McKenna, JG. (2005). A preliminary case series on the use of quetiapine for posttraumatic stress disorder in juveniles within a youth detention center. J Clin Psychopharmacol, 25(6), 539-44.
31. Van der Kolk, BA (1984). Post-Traumatic Stress Disorders: Psychological and Biological Sequelae. Washington D.C.: American Psychiatric Press
32. Vickers B (2005). Cognitive model of the maintenance and treatment of post-traumatic stress disorder applied to children and adolescents. Clinical Child Psychology and Psychiatry 10: 217-234
33. Ward-Begnoche W (2007). Posttraumatic stress symptoms in the pediatric intensive care unit. Journal for specialists in pediatric nursing, 12(2), 84-92.
34. Winnicott D (1971) Playing and Reality. London: Tavistock Publications.


















