TUMOURS OF
7
275 TUMOURS OF RENAL PELVIS By I. H. GRIFFITHS, F.R.C.S. From the Urological Department, Middlesex Hospital At the Annual Meeting of the British Association of Urological Surgeons in June 195I a survey was made of 2314 renal and ureteric tumours collected from 67 Centres in the British Isles (Riches, Griffiths and Thackray (I95I)). In this series 315 (12.5 per cent.) were tumours of the renal pelvis, an incidence of about i in I200 of malignant tumours admitted to General Hospitals. This long series of an interesting, though com- paratively rare, condition presented an opportunity to study the clinical and pathological behaviour and to determine what factors influence the prog- nosis. Many of the conclusions of this series serve only to confirm those of J. B. Macalpine (I947) to whom credit is given for much valuable and original work on this subject. Aetiology Like most other tumours of the urinary tract, very little is known of the aetiology. A most interesting fact arising from the collective report was that no cases of bilateral papillary tumours of the pelvis were recorded. This does suggest that the noxious agent responsible for tumour production is not excreted in the urine. In the case of papillary tumours of the pelvis it is un- common to find any local condition which may be presumed to be a cause. The urine is usually found to be sterile, and stone, which was recorded as being present in association with papillary tumours in only 5 per cent., probably develops as a result of tumour obstruction. In the aetiology of squamous-cell carcinoma chronic inflammation undoubtedly plays an impor- tant part. Prolonged continuous renal infection is a common finding and often gives rise to squamous metaplasia, although leukoplakia, a precarcinoma- tous condition, is not often observed. Associated calculous disease of the kidney was found in approximately a third of the cases, a much lower incidence than is recorded by some authorities but high enough to be significant as a predisposing cause of epitheliomata of the pelvis. .0 *14 j- Il FIG. i.-Obstruction by simple papilliferous tumours of the renal pelvis causing gross hydronephrosis with destruction of the renal parenchyma. Pathology Transitional-cell and squamous-cell tumours arising within the renal pelvis are similar in appear- ance and structure to those developing within the urinary bladder, but the prognosis of the renal tumours is distinctly worse than comparable tumours of the bladder. This gloomy outlook for renal growth is, in all probability, due to the thin copyright. on December 15, 2021 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.28.319.275 on 1 May 1952. Downloaded from
Transcript of TUMOURS OF
275
TUMOURS OF RENAL PELVISBy I. H. GRIFFITHS, F.R.C.S.
From the Urological Department, Middlesex Hospital
At the Annual Meeting of the British Associationof Urological Surgeons in June 195I a survey wasmade of 2314 renal and ureteric tumours collectedfrom 67 Centres in the British Isles (Riches,Griffiths and Thackray (I95I)).
In this series 315 (12.5 per cent.) were tumoursof the renal pelvis, an incidence of about i inI200 of malignant tumours admitted to GeneralHospitals.This long series of an interesting, though com-
paratively rare, condition presented an opportunityto study the clinical and pathological behaviourand to determine what factors influence the prog-nosis. Many of the conclusions of this seriesserve only to confirm those of J. B. Macalpine(I947) to whom credit is given for much valuableand original work on this subject.
AetiologyLike most other tumours of the urinary tract,
very little is known of the aetiology. A mostinteresting fact arising from the collective reportwas that no cases of bilateral papillary tumoursof the pelvis were recorded. This does suggestthat the noxious agent responsible for tumourproduction is not excreted in the urine. In thecase of papillary tumours of the pelvis it is un-common to find any local condition which may bepresumed to be a cause. The urine is usually foundto be sterile, and stone, which was recorded as beingpresent in association with papillary tumours inonly 5 per cent., probably develops as a result oftumour obstruction.
In the aetiology of squamous-cell carcinomachronic inflammation undoubtedly plays an impor-tant part. Prolonged continuous renal infection isa common finding and often gives rise to squamousmetaplasia, although leukoplakia, a precarcinoma-tous condition, is not often observed. Associatedcalculous disease of the kidney was found inapproximately a third of the cases, a much lowerincidence than is recorded by some authoritiesbut high enough to be significant as a predisposingcause of epitheliomata of the pelvis.
.0
*14
j-
Il
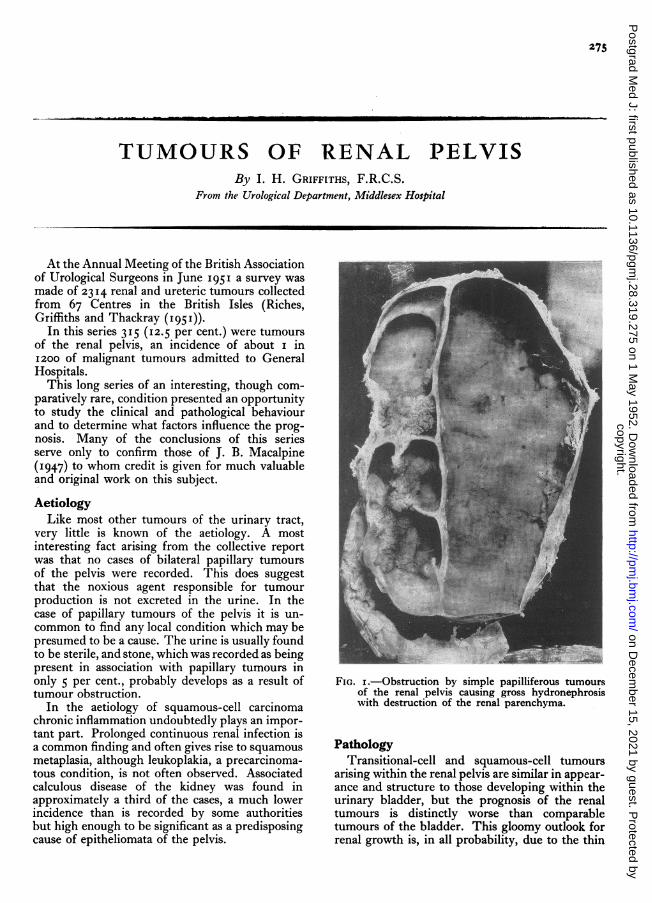
FIG. i.-Obstruction by simple papilliferous tumoursof the renal pelvis causing gross hydronephrosiswith destruction of the renal parenchyma.
PathologyTransitional-cell and squamous-cell tumours
arising within the renal pelvis are similar in appear-ance and structure to those developing within theurinary bladder, but the prognosis of the renaltumours is distinctly worse than comparabletumours of the bladder. This gloomy outlook forrenal growth is, in all probability, due to the thin
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from
276 POSTGRADUATE MEDICAL JOURNAI, May I952
walled pelvis being penetrated more rapidly bymalignant invasion.
Elaborate classification of pelvic tumours leadsto confusion and a simple grouping into threeprimary types has much greater practical value:
(a) Transitional cell papilloma.(b) Transitional cell carcinoma.(c) Squamous cell carcinoma.
Transitional cell PapillomaSimple papillomata account for about 25 per
cent.. of tumours .of the renal pelvis and are moreoften multiple than single. A single tumour isoccasionally found near the pelvi-ureteric junctioncausing obstruction, pain and haematuria early inits development. In less fortunate cases thesetumours may arise within the pelvis or a calyx anddevelop silently into large and multiple papillarytumours before revealing themselves (Fig. i).The simple nature of these tumours is doubted
by many pathologists, and with good reason, sincesimple papillomata of the pelvis may be found inassociation with papillary carcinoma in the ureteror bladder. However, from the clinical aspect, itis wise to make a distinction between benign andmalignant tumours since the prognosis in eachcase is quite different.
Transitional cell CarcinomaThese tumours constitute about 50 per cent. of
growths of the kidney pelvis. They are usuallybulkier tumours than the simple papillomata andare more apt to give rise to hydronephrosis orhydrocalycosis, and in each cases the distendedorgan may be found indurated by multiple tumoursstudding the wall. The villi may be long and thepedicles narrow, but, as malignancy advances, thevilli become short and stumpy and the pediclesbecome wider, giving rise to a nodular type ofgrowth showing a higher degree of malignancyand greater invasion of the pelvic wall.Squamous metaplasia to a varying degree occurs
frequently, but tumours showing this transitionshould n'ot be regarded as epitheliomata2 whichshow a significant difference in mode of spreadand in prognosis.
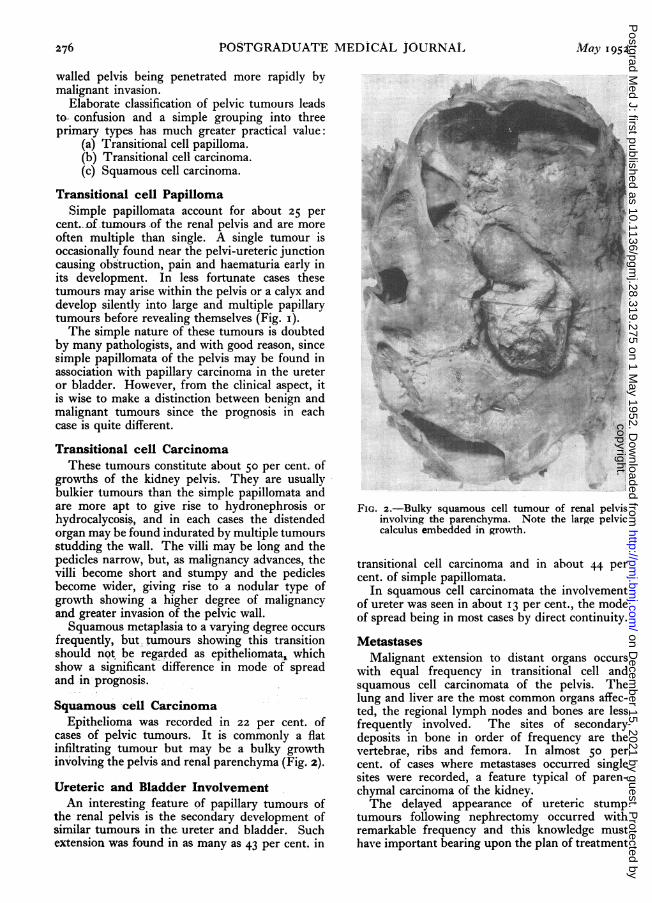
Squamous cell CarcinomaEpithelioma was recorded in 22 per cent. of
cases of pelvic tumours. It is commonly a flatinfiltrating tumour but may be a bulky growthinvolving the pelvis and renal parenchyma (Fig. 2).
Ureteric and Bladder InvolvementAn interesting feature of papillary tumours of
the renal pelvis is the secondary development ofsimilar tumours in the ureter and bladder. Suchextension was found in as many as 43 per cent. in
v.
FIG. 2.-Bulky squamous cell tumour of renal pelvisinvolving the parenchyma. Note the large pelviccalculus embedded in growth.
transitional cell carcinoma and in about 44 percent. of simple papillomata.
In squamous cell carcinomata the involvementof ureter was seen in about 13 per cent., the modeof spread being in most cases by direct continuity.
MetastasesMalignant extension to distant organs occurs
with equal frequency in transitional cell andsquamous cell carcinomata of the pelvis. Thelung and liver are the most common organs affec-ted, the regional lymph nodes and bones are lessfrequently involved. The sites of secondarydeposits in bone in order of frequency are thevertebrae, ribs and femora. In almost 50 percent. of cases where metastases occurred singlesites were recorded, a feature typical of paren-chymal carcinoma of the kidney.The delayed appearance of ureteric stump
tumours following nephrectomy occurred withremarkable frequency and this knowledge musthave important bearing upon the plan of treatment
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from

May I952 GRIFFITHS: Tumours of Renal Pelvis 277
of this renal disease. In 8 per cent. of simplepapillary tumours of the pelvis the uretericstump was involved, and for transitional cellcarcinoma of the pelvis the incidence was 9 percent., whilst for squamous call carcinoma it wasonly 3.6 per cent. Thus, it appeared that thepapillary tumours showed a greater tendency todelayed appearance, and in the majority of casesthis took place -vithin a year.
'Theories of Tumour DisseminationThe secondary appearance of tumours in the
subpelvic regions of the urinary tract is a patho-logical feature which has many theories to accountfor it. Two most attractive possibilities are (a)implantation of seedlings and (b) origin frommulticentric foci in the urinary tract.
In the former theory, papillomatous materialfrom the primary lesion in the pelvis is alleged tobe transferred down the ureter in the urinarystream and becomes held up at some constrictedpart, most commonly at the juxta-vesical segment,and, after a period of close contact with the ureteralmucosa, develops a blood supply from it. Thiswould account for multiple and unilateral distri-bution of the disease but does not explain theassociation of malignant tumours in the lowerurinary tract with simple tumours of the pelvis.A most enigmatic feature of the disease is theoccurrence of ureteric stump tumours, for inmore than 8o per cent. of these cases the tumourswere revealed within one year after nephrectomy.It is suggested that in such cases ureteric implantswere present at the time of nephrectomy but wentunobserved by the surgeon.The origin of tumours from multicentric foci is
a conception that considers the epithelium of theurinary tract to have an inherent propensity totumour formation. This property is thought tobe a regional feature which explains the unilateraldevelopment of multiple tumours. That thesetumours show differences in character is due to
different degrees of advancement. Thus, it be-comes possible to have simple and malignantpapilliferous tumours in close or distant associa-tion with each other.
Age, Sex and Side IncidenceMore than 8o per cent. of the more common
tumours of the renal pelvis occur in the 5th, 6thand 7th decades. An exceptional case, in theB.A.U.S. series was of a transitional cell carcinomadeveloping in a child of 9.
Males are affected three to four times more oftenthan females except in the case of squamous celltumours, where male incidence only slightlyexceeds female. There appears to be no preferencefor side, for in all tumours of the renal pelvis theincidence of right and left is almost identical.
Symptoms and SignsPain, Haematuria and Tumour is a symptomatic
triad found in varying proportions and severity inall tumours of the urinary tract. Haematuriais the leading symptom and occurs in about 90per cent. oi cases of transitional cell carcinomaand simple papilloma, whilst pain is present inabout 45 per cent. The high incidence of pain inthese cases must be due to associated urinaryinfection, passage of blood clots, and distensionof the renal pelvis. In cases of squamous cellcarcinoma the incidence is about 6o per cent. Thefrequent association of stone with renal epithelio-mata must be mainly responsible for the increasedincidence of pain.
TumourTumours of the renal pelvis may cause gross
dilatation of the pelvis and calyceal system, butthey are seldom clinically palpable. In contrastto tumours of the renal parenchyma, which arepalpable in 6o per cent. of cases, only 2 per cent.of renal pelvis tumours are revealed on abdominalexamination. Dilatation of the ureter. or the-
....... ...
..... ..... .........
FIG. 3.-A blood cast of ureter from a case of papilliferous tumour of the renal pelvis.
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from
278 POSTGRADUATE MEDICAL JOURNAL May I952
pelvis, or the calyceal system may occur dependingon the site of tumour development, but it is notusually appreciated before radiological examination.
InvestigationsHaematuria demands an early and full urological
investigation. The urine must be examined toestablish the presence of blood, which sometimesmay be only microscopic and at other times maybe profuse and clotted. Vermiform blood clot, acast of the ureter, is a reliable sign of profusehaemorrhage from the upper part of the urinarytract (Fig. 3).
In this disease of the upper urinary tract diag-nosis is often difficult and one can sympathizewith the clinician who fails to detect a tumour toosmall to be seen radiographically. But, so fre-quently, transient episodes of haematuria arespaced by long periods of silence during whichtime both doctor and patient are willing to forgetthe ominous and colourful warning so providentlyarranged by nature.
CystoscopyCystoscopy has the greatest value in the presence
of haematuria, when the source of haemorrhagemay be determined; if it is of renal origin, abloody efflux from a ureteric orifice will'reveal theoffending side. If cystoscopy during a quiescentperiod does not produce a diagnosis with certaintythen it is wiser to re-examine during the period ofhaemorrhage than to make a doubtful diagnosisof such a condition as varicose veins of the bladder.
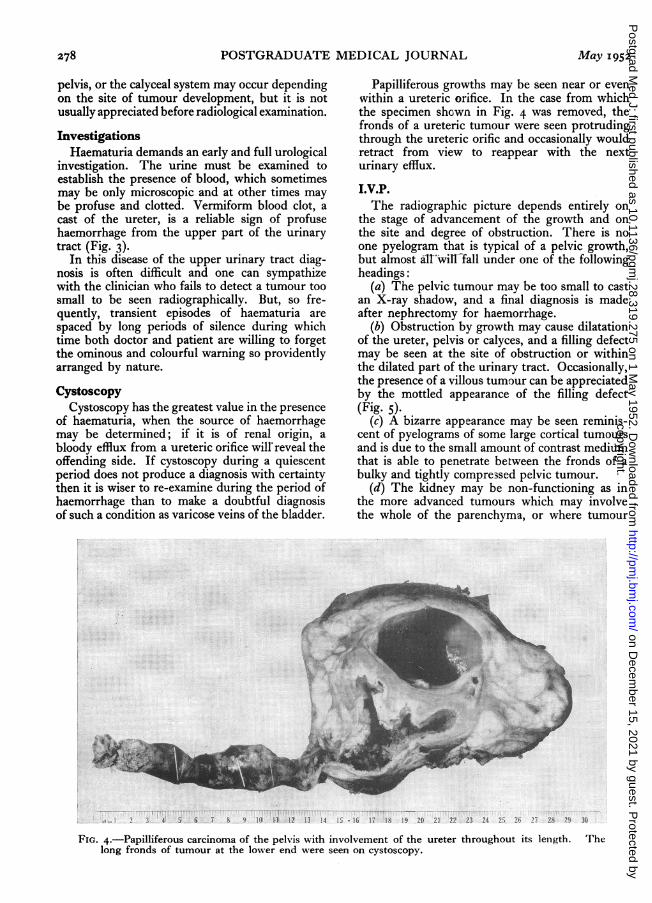
Papilliferous growths may be seen near or evenwithin a ureteric orifice. In the case from whichthe specimen shown in Fig. 4 was removed, thefronds of a ureteric tumour were seen protrudingthrough the ureteric orific and occasionally wouldretract from view to reappear with the nexturinary efflux.
I.V.P.The radiographic picture depends entirely on
the stage of advancement of the growth and onthe site and degree of obstruction. There is noone pyelogram that is typical of a pelvic growth,but almost allwill Tall under one of the followingheadings:
(a) The pelvic tumour may be too small to castan X-ray shadow, and a final diagnosis is madeafter nephrectomy for haemorrhage.
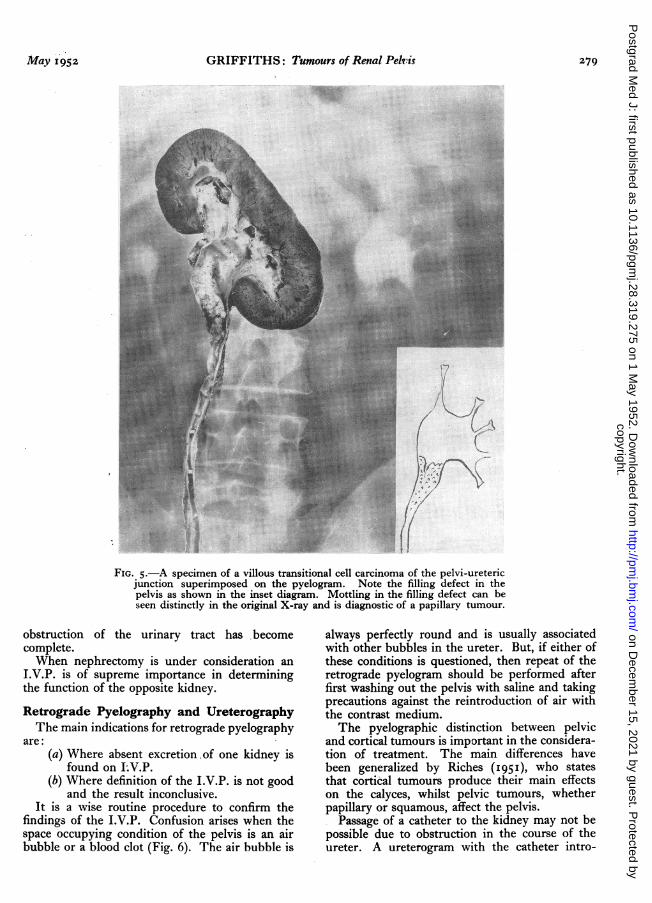
(b) Obstruction by growth may cause dilatationof the ureter, pelvis or calyces, and a filling defectmay be seen at the site of obstruction or withinthe dilated part of the urinary tract. Occasionally,the presence of a villous tumour can be appreciatedby the mottled appearance of the filling defect(Fig. 5).
(c) A bizarre appearance may be seen reminis-cent of pyelograms of some large cortical tumoursand is due to the small amount of contrast mediumthat is able to penetrate between the fronds of abulky and tightly compre3sed pelvic tumour.
(d) The kidney may be non-functioning as inthe more advanced tumours which may involvethe whole of the parenchyma, or where tumour
........ ........
.....
... ... .....
...
............
.........
............
....
...
.....
.... ..
Pr-.-... ..
.....
......
-1%:, A Ig 19 ..,I] 23 ..24 26' '27 ?A" WJ
FIG. 4.-Papilliferous carcinoma of the pelvis with involvement of the ureter throughout its lenigth. Thelong fronds of tumour at the lower end were seen on cystoscopy.
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from
May I952 GRIFFITHS: Tumours of Renal Pelvis 279
--f-
Ls
^}N: .. :: :'ij..:
:i:.].:t=--
-.: S.
|:i-||--
.. B
FIG. 5.-A specimen of a villous transitional cell carcinoma of the pelvi-uretericjunction superimposed on the pyelogram. Note the filling defect in thepelvis as shown in the inset diagram. Mottling in the filling defect can beseen distinctly in the original X-ray and is diagnostic of a papillarv tumour.
obstruction of the urinary tract has becomecomplete.When nephrectomy is under consideration an
I.V.P. is of supreme importance in determiningthe function of the opposite kidney.
Retrograde Pyelography and UreterographyThe main indications for retrograde pyelography
are:(a) Where absent excretion of one kidney is
found on LV.P.(b) Where definition of the I.V.P. is not good
and the result inconclusive.It is a wise routine procedure to confirm the
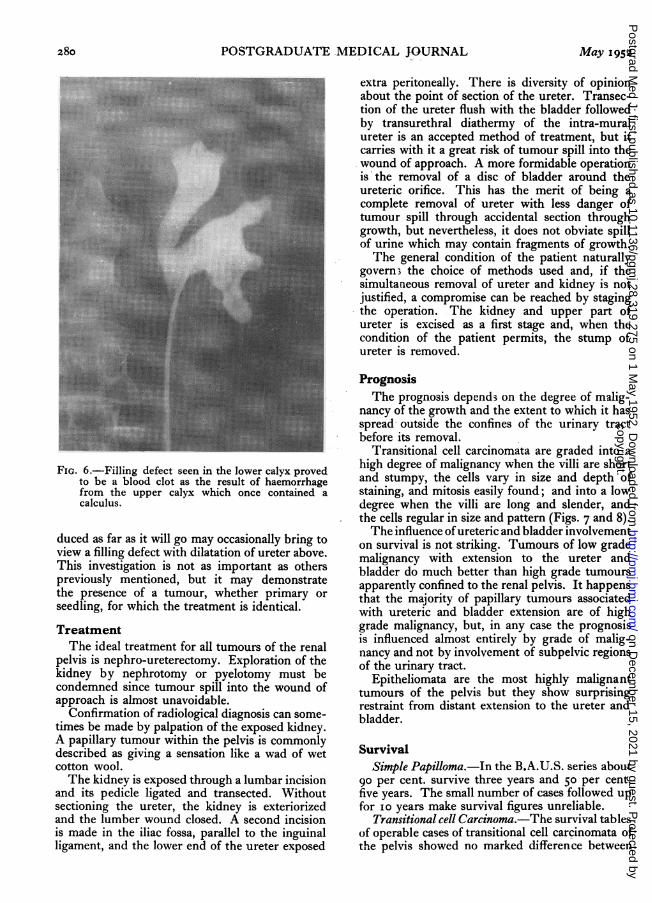
findings of the I.V.P. Confusion arises when thespace occupying condition of the pelvis is an airbubble or a blood clot (Fig. 6). The air bubble is
always perfectly round and is usually associatedwith other bubbles in the ureter. But, if either ofthese conditions is questioned, then repeat of theretrograde pyelogram should be performed afterfirst washing out the pelvis with saline and takingprecautions against the reintroduction of air withthe contrast medium.The pyelographic distinction between pelvic
and cortical tumours is important in the considera-tion of treatment. The main differences havebeen generalized by Riches (I95I), who statesthat cortical tumours produce their main effectson the calyces, whilst pelvic tumours, whetherpapillary or squamous, affect the pelvis.
Passage of a catheter to the kidney may not bepossible due to obstruction in the course of theureter. A ureterogram with the catheter intro-
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from
280 POSTGRADUATE MEDICAL JOURNAL May i952
~~~~~~~~~~~..
.:. !:..: °?ciKX;2;AZxos-3e....t<:S?~k
::::i:::.: :i::.''? 'IS......... #?e' ti;........ .. ...: x3l<dA??x,8........ .. .. .:a s<>m>. >. .>; .; .:;4..:..::.:.:; 2i¢o!?SX?...
.. ...i}i< ...s B ?es:s.i::i:.. '..:.:...:: .. :. :.<; > <:::::.::::. ::: .!:.y} :.y :i?..r...... ..::} ..: xw
....:: }: }:.s4}|s4:: },...:.;9.Xt.. ses.s .:: ::.:.:: 3<
S.j.- jiij.,, W-.............--.; -..... e3y. . ..
FIG. 6.-Filling defect seen in the lower calyx provedto be a blood clot as the result of haemorrhagefrom the upper calyx which once contained acalculus.
duced as far as it will go may occasionally bring toview a filling defect with dilatation of ureter above.This investigation is not as important as otherspreviously mentioned, but it may demonstratethe presence of a tumour, whether primary orseedling, for which the treatment is identical.
TreatmentThe ideal treatment for all tumours of the renal
pelvis is nephro-ureterectomy. Exploration of thekidney by nephrotomy or pyelotomy must becondemned since tumour spill into the wound ofapproach is almost unavoidable.
Confirmation of radiological diagnosis can some-times be made by palpation of the exposed kidney.A papillary tumour within the pelvis is commonlydescribed as giving a sensation like a wad of wetcotton wool.The kidney is exposed through a lumbar incision
and its pedicle ligated and transected. Withoutsectioning the ureter, the kidney is exteriorizedand the lumber wound closed. A second incisionis made in the iliac fossa, parallel to the inguinalligament, and the lower end of the ureter exposed
extra peritoneally. There is diversity of opinionabout the point of section of the ureter. Transec-tion of the ureter flush with the bladder followedby transurethral diathermy of the intra-muralureter is an accepted method of treatment, but itcarries with it a great risk of tumour spill into thewound of approach. A more formidable operationis the removal of a disc of bladder around theureteric orifice. This has the merit of being acomplete removal of ureter with less danger oftumour spill through accidental section throughgrowth, but nevertheless, it does not obviate spillof urine which may contain fragments of growth.The general condition of the patient naturally
govern-3 the choice of methods used and, if thesimultaneous removal of ureter and kidney is notjustified, a compromise can be reached by stagingthe operation. The kidney and upper part ofureter is excised as a first stage and, when thecondition of the patient permits, the stump ofureter is removed.
PrognosisThe prognosis depend3 on the degree of malig-
nancy of the growth and the extent to which it hasspread* outside the confines of the urinary tractbefore its removal.
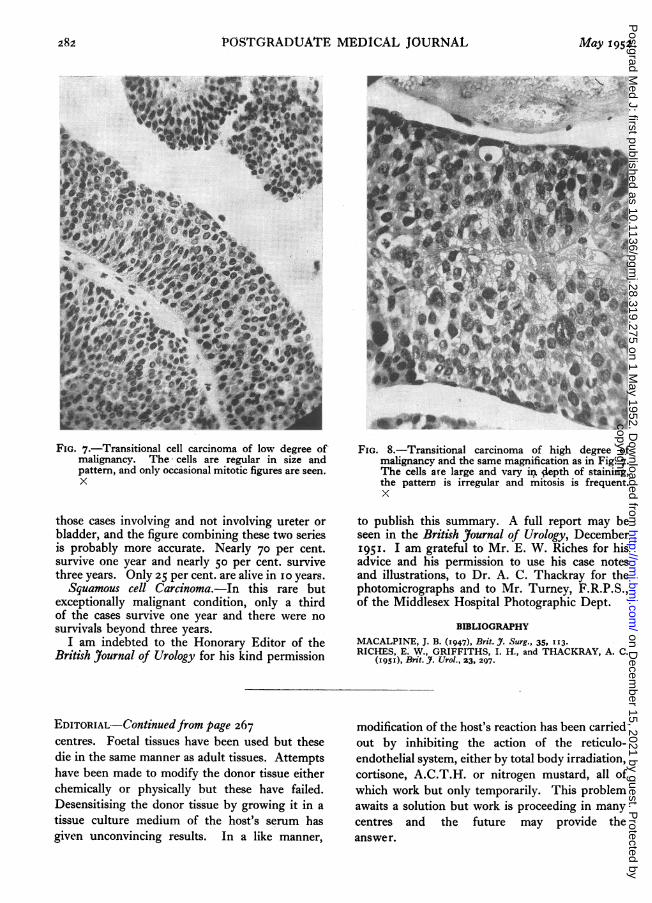
Transitional cell carcinomata are graded into ahigh degree of malignancy when the villi are shortand stumpy, the cells vary in size and depth ofstaining, and mitosis easily found; and into a lowdegree when the villi are long and slender, andthe cells regular in size and pattern (Figs. 7 and 8).The influence of ureteric and bladder involvement
on survival is not striking. Tumours of low grademalignancy with extension to the ureter andbladder do much better than high grade tumoursapparently confined to the renal pelvis. It happensthat the majority of papillary tumours associatedwith ureteric and bladder extension are of highgrade malignancy, but, in any case the prognosisis influenced almost entirely by grade of malig-nancy and not by involvement of subpelvic regionsof the urinary tract.
Epitheliomata are the most highly malignanttumours of the pelvis but they show surprisingrestraint from distant extension to the ureter andbladder.
SurvivalSimple Papilloma.-In the B.A.U.S. series about
go per cent. survive three years and 50 per cent.five years. The small number of cases followed upfor io years make survival figures unreliable.
Transitional cell Carcinoma.-The survival tablesof operable cases of transitional cell carcinomata ofthe pelvis showed no marked difference between
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from
282 POSTGRADUATE MEDICAL JOURNAL May 1952
6)
-i*
;pj.7.1.8·-L.PB...i
i:iirjlL.i.Jj.B.I I)i!i·i. ·.C1...E.'.IIPL.r:hlhl .· r
..*:.*..IJ' "' j
"E..*'; ""'
·*ri. 1
....I,.i.i.bkY r,-.lITPd .r··i·.· ,·,,.u.i ·" L.
.g.i....*.
FIG. 7.-Transitional cell carcinoma of low degree ofmalignancy. The cells are regular in size andpattern, and only occasional mitotic figures are seen.X
those cases involving and not involving ureter orbladder, and the figure combining these two seriesis probably more accurate. Nearly 70 per cent.survive one year and nearly 50 per cent. survivethree years. Only 25 per cent. are alive in o1 years.Squamous cell Carcinoma.-In this rare but
exceptionally malignant condition, only a thirdof the cases survive one year and there were nosurvivals beyond three years.
I am indebted to the Honorary Editor of theBritish Journal of Urology for his kind permission
-r-~
FIG. 8.-Transitional carcinoma of high degree ofmalignancy and the same magnification as in Fig. 7.The cells are large and vary ii 4epth of staining,the pattern is irregular and mitosis is frequent.X
to publish this summary. A full report may beseen in the British Journal of Urology, December195I. I am grateful to Mr. E. W. Riches for hisadvice and his permission to use his case notesand illustrations, to Dr. A. C. Thackray for thephotomicrographs and to Mr. Turney, F.R.P.S.,of the Middlesex Hospital Photographic Dept.
BIBLIOGRAPHY
MACALPINE, J. B. (1947), Brit. J. Surg., 35, II3.RICHES, E. W., GRIFFITHS, I. H., and THACKRAY, A. C.
(I95I), Brit. J. Urol., 23, 297.
EDITORIAL-Continuedfrom page 267centres. Foetal tissues have been used but thesedie in the same manner as adult tissues. Attemptshave been made to modify the donor tissue eitherchemically or physically but these have failed.Desensitising the donor tissue by growing it in atissue culture medium of the host's serum hasgiven unconvincing results. In a like manner,
modification of the host's reaction has been carriedout by inhibiting the action of the reticulo-endothelial system, either by total body irradiation,cortisone, A.C.T.H. or nitrogen mustard, all ofwhich work but only temporarily. This problemawaits a solution but work is proceeding in manycentres and the future may provide theanswer.
copyright. on D
ecember 15, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.319.275 on 1 May 1952. D
ownloaded from