Tumours of oral cavity
22
TUMOURS OF ORAL CAVITY DR ROOHIA
Transcript of Tumours of oral cavity

TUMOURS OF ORAL CAVITY
DR ROOHIA

EPIDEMIOLOGY
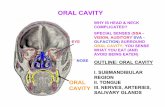
Oral cavity: extends from vermillion border of lips to plane between junction of hard palate and soft palate.
Include : buccal mucosa, tongue, gingiva, retromolar trigone, floor of mouth, hard palate
High incidence in India, France.
40% of HN cancer Age of onset 6-7th decade,

Classification The tumours of oral cavity can be
classified as follows: I. Benign tumours (a) Solid (b) Cystic II. Premalignant lesions III. Malignant lesions

I. BENIGN TUMOURS
Solid Tumours Fibroma
(fibroepithelial polyp)
Haemangioma

Pyogenic granuloma
trauma or chronic irritation
anterior gingivae

Cystic Lesions Mucocele soft and cystic mass of bluish
colour lower lip retention cyst of minor salivary
glands of the lip Ranula cystic translucent floor of mouth on one side of the
frenulum and pushing the tongue up
sublingual salivary gland due to obstruction of its ducts
ranulae extend into the neck (plunging type).


Pre-Malignant Lesions
Leukoplakia - chronic, white, verrucous plaque with histologic atypia Severity linked to the
duration and quantity of tobacco and alcohol use
Occur anywhere in the oral cavity
Lip, tongue, or floor of the mouth lesions are prone for progression to SCC
Erythroplakia - non-inflammatory
erythematous plaque Decrased keratinisation

Pre-Malignant Lesions…
Submucous fibrosis generalized white
discoloration of oral mucosa with progressive fibrosis, painful mucosal atrophy and restrictive fibrotic bands
individuals who chew betel quid, tobacco, lime, and betel leaves
Ultimately leads to trismus, dysphagia and severe xerostomia
5 - 10 % progress to SCC

Cancerous lesion of Lips& Oral cavity Lips –SCC, Melanoma, BCC(rare) Oral cavity: -- scc: 9/10 incidence --verrucous ca: <5% low grade, slow growing rarely metastasizes with tendency to invade deep tissue.

Cancerous lesion of Lips& Oral cavity Minor salivary gland
tumor: -in the glands lining the oral cavity -adenoidcystic ca, mucoepidermoid ca, adenocarcinoma.-Sarcoma

etiology
a)smoking (b) Tobacco chewing.. (c) Alcohol .. (d) Dietary deficiencies. (e) Dental sepsis, jagged sharp
teeth and ill fitting dentures

subsites
1. Mucosal lip 2. Buccal mucosa 3. Anterior two thirds
of tongue (oral tongue)
4. Hard palate 5. Lower alveolar
ridge 6. Upper alveolar
ridge 7. Floor of mouth 8. Retromolar trigone.

Ca tongue
(i) An exophytic lesion
(ii) A non-healing ulcer with rolled edges, greyish white shaggy base and induration
(iii) A submucous nodule with induration of the surrounding tissue

C/f
(i) asymptomatic for a long time. (ii) Pain in the tongue locally at the site
of ulcer. (iii) Pain in the ipsilateral ear; (iv) A lump in the mouth. (v) Enlarged lymph node mass in the
neck. (vi) Dysphagia, difficulty to protrude the
tongue, slurred speech and bleeding from the mouth are late
features

STAGING OF THE DISEASE
American joint committee on cancer: T , N , M Tx- primary tumour cannot be assessed T0- No evidence of primary tumour T1- ≤ 2cm in greatest dimension T2- 4cm < 2cm> in greatest dimension T3- > 4cm in greatest dimension

STAGING OF THE DISEASE
T4a- Oral cavity: tumour invades through cortical bone, into deep(extrinsic) muscle of tongue, maxillary sinus or skin. Lips: cortical bone, inferior alveolar nerve, floor of mouth, skin i.e. chin or nose.
T4b- involves masticator space, pterygoid plates, skull base and/or encases internal carotid artery

STAGING OF THE DISEASE
N stage: Nx- regional lymph nodes can not be assessed. N0- no regional lymph node metastasis. N1- metastasis in a single ipsilateral lymph node ≤ 3cm in greatest dimension. N2a- metastasis in a single ipsilateral LN > 3cm but < 6cm in greatest dimension.

STAGING OF THE DISEASE
N2b- metastasis in multiple ipsilateral LNs, none > 6cm in greatest dimension. N2c- metastasis in B/L or C/L LNs, none > 6 cm. N3- metastasis in a LN > 6 cm in greatest dimension
M stage: Mx- cannot be assessed, M0- no distant metastasis, M1- distant metastasisi.

TREATMENT
Small tumours (T1N0) treated with radiotherapy or surgery.
T2N0 tumours can also be treated by radiotherapy including the neck nodes, . They can also be treated by surgical excision with prophylactic neck dissection.
Stage III or IV tumours require combined treatment with surgery and post-operative radiotherapy.
hemiglossectomy including a portion of the floor of mouth, segmental or hemimandibulectomy and block dissection of neck "commando operation".


THANK YOU