Tulane – PPE Assessment · PDF file11F-OEHS /Tulane (Rev 8/03) PPE PERSONAL PROTECTIVE...
4
11F-OEHS /Tulane (Rev 8/03) PPE PERSONAL PROTECTIVE EQUIPMENT ASSESSMENT This assessment form shall be used to assess the hazards to which employees may be exposed to determine whether there are hazards in the environment that necessitate the use of personal protective equipment. Departments and Administrative Units are responsible for completing and submitting this form to the Office of Environmental Health and Safety. (A separate assessment form must be completed for each work area). Person(s) Conducting the Assessment:__________________________________________________________ Department: ________________________________ Phone No/Ext: ___________________________________ e-Mail: _____________________________________________________ Mail Code:_____________________ Location of Area to Be Assessed: Campus: _______________________ Building:____________________________ Room No: ______________ (Campus: e.g., Uptown, TUHSC, Primate, etc.) Date of Assessment: _____/_____/_____ CHEMICAL OR INFECTIOUS HAZARDS 1. Are hazardous chemicals or infectious materials used in this work area? ___Yes___No 2. What types of hazardous chemicals or materials are used? (Check all that apply.) ___ Corrosives ___ Flammables ___ Toxics ___ Oxidizers ___ Biohazards ___ Carcinogens (please list)____________________________________________________ ___ Explosives ___ Radioactive Materials ___ Infectious Agents ___ Other(s) (please list)__________________________________________________ 3. What personal protective equipment is recommended for use with these materials? (See Material Safety Data Sheets or other sources of information) (Check all that apply.) ___ Gloves ___ Chemical Apron ___ Respirator ___ Goggles ___ Lab coat ___ Safety Glasses ___ Face Shield ___ Shoe Covers ___ Other(s) ____________________________________________ HARMFUL DUST 1. Are there sources of harmful dust to which employees may be exposed (such as from blasting, buffing, woodworking, mixing of concrete and/or glazes for art, etc.) in this work area? ___ Yes ___ No 2. What personal protective equipment is recommended (see Material Safety Data Sheets or other sources of information)? (Check all that apply.) ___ Gloves ___ Dust/Mist Respirator ___Safety Glasses ___Goggles ___ Face Shield ___ Other(s) ____________________________________________________ COMPRESSION 1. Are there activities in which employees may encounter compression hazards such as from hydraulic jacks, tools, presses, or compactors in this work area? ___Yes___No 2. Are forklifts used in this work area? ___Yes___No 3. Do employees install or work with heavy pipes in this work area? ___ Yes___No 4. Are there objects in the work area that may roll over an employee's feet? ___Yes___No 5. What personal protective equipment is recommended? ___ Gloves ___Foot Protection ___ Hard Hat ___ Other(s) _____________________________ Fill out the form online and print, then mail to OEHS - TW16.
-
Upload
truongdung -
Category
Documents
-
view
218 -
download
2
Transcript of Tulane – PPE Assessment · PDF file11F-OEHS /Tulane (Rev 8/03) PPE PERSONAL PROTECTIVE...
11F-OEHS /Tulane (Rev 8/03) PPE
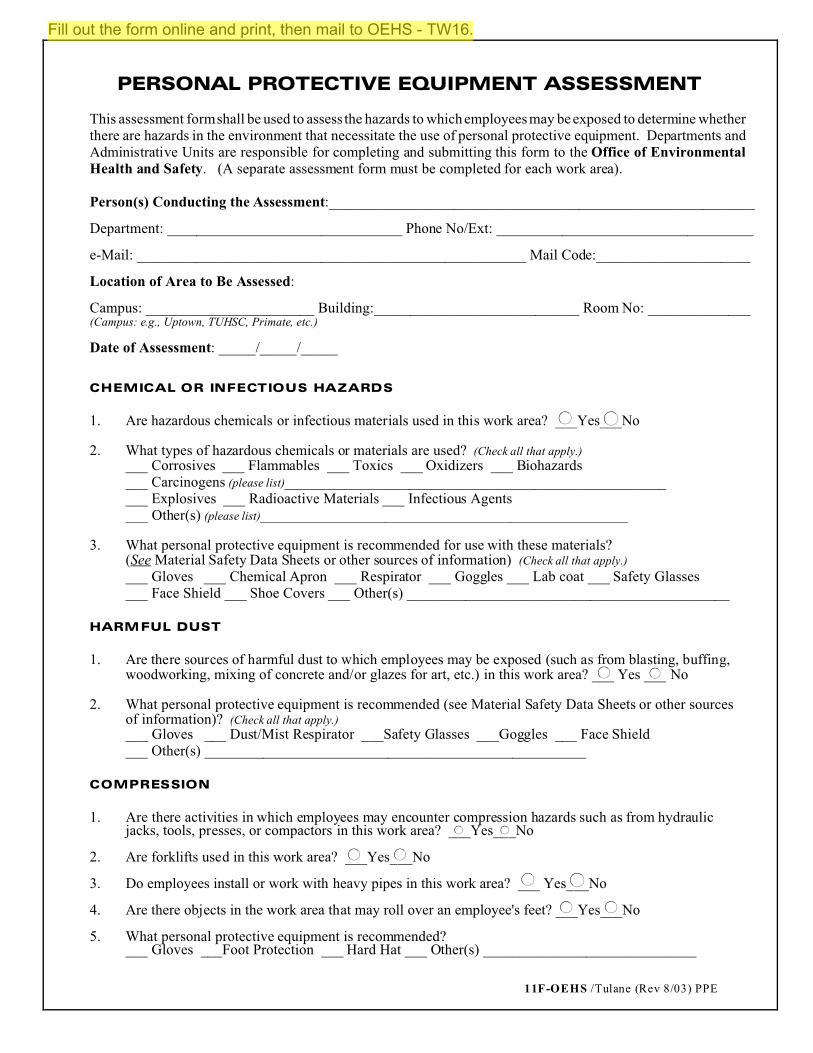
PERSONAL PROTECTIVE EQUIPMENT ASSESSMENT
This assessment form shall be used to assess the hazards to which employees may be exposed to determine whetherthere are hazards in the environment that necessitate the use of personal protective equipment. Departments andAdministrative Units are responsible for completing and submitting this form to the Office of EnvironmentalHealth and Safety. (A separate assessment form must be completed for each work area).
Person(s) Conducting the Assessment:__________________________________________________________
Department: ________________________________ Phone No/Ext: ___________________________________
e-Mail: _____________________________________________________ Mail Code:_____________________
Location of Area to Be Assessed:
Campus: _______________________ Building:____________________________ Room No: ______________(Campus: e.g., Uptown, TUHSC, Primate, etc.)
Date of Assessment: _____/_____/_____
CHEMICAL OR INFECTIOUS HAZARDS
1. Are hazardous chemicals or infectious materials used in this work area? ___Yes___No
2. What types of hazardous chemicals or materials are used? (Check all that apply.)
___ Corrosives ___ Flammables ___ Toxics ___ Oxidizers ___ Biohazards ___ Carcinogens (please list)_______________________________________________________ Explosives ___ Radioactive Materials ___ Infectious Agents ___ Other(s) (please list)__________________________________________________
3. What personal protective equipment is recommended for use with these materials?(See Material Safety Data Sheets or other sources of information) (Check all that apply.)
___ Gloves ___ Chemical Apron ___ Respirator ___ Goggles ___ Lab coat ___ Safety Glasses___ Face Shield ___ Shoe Covers ___ Other(s) ____________________________________________
HARMFUL DUST
1. Are there sources of harmful dust to which employees may be exposed (such as from blasting, buffing,woodworking, mixing of concrete and/or glazes for art, etc.) in this work area? ___ Yes ___ No
2. What personal protective equipment is recommended (see Material Safety Data Sheets or other sourcesof information)? (Check all that apply.)
___ Gloves ___ Dust/Mist Respirator ___Safety Glasses ___Goggles ___ Face Shield___ Other(s) ____________________________________________________
COMPRESSION
1. Are there activities in which employees may encounter compression hazards such as from hydraulicjacks, tools, presses, or compactors in this work area? ___Yes___No
2. Are forklifts used in this work area? ___Yes___No
3. Do employees install or work with heavy pipes in this work area? ___ Yes___No
4. Are there objects in the work area that may roll over an employee's feet? ___Yes___No
5. What personal protective equipment is recommended?___ Gloves ___Foot Protection ___ Hard Hat ___ Other(s) _____________________________
Fill out the form online and print, then mail to OEHS - TW16.
ksimon
Highlight
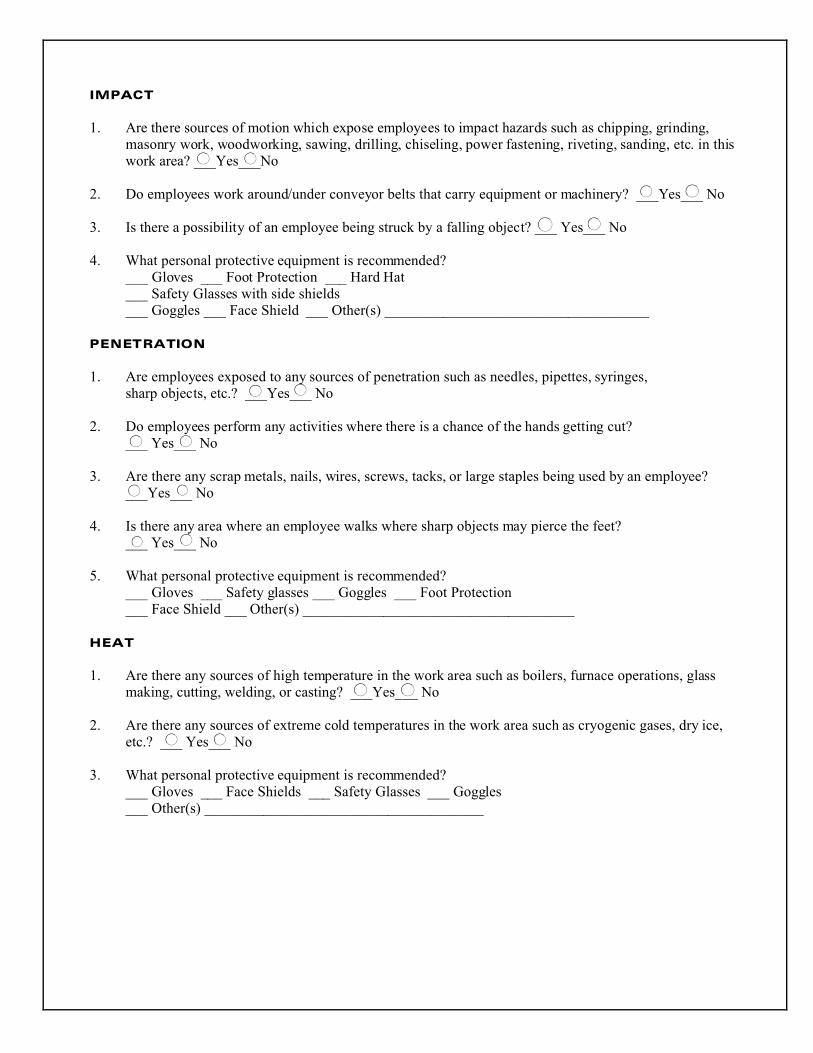
IMPACT
1. Are there sources of motion which expose employees to impact hazards such as chipping, grinding,masonry work, woodworking, sawing, drilling, chiseling, power fastening, riveting, sanding, etc. in thiswork area? ___Yes___No
2. Do employees work around/under conveyor belts that carry equipment or machinery? ___Yes___ No
3. Is there a possibility of an employee being struck by a falling object? ___ Yes___ No
4. What personal protective equipment is recommended?___ Gloves ___ Foot Protection ___ Hard Hat ___ Safety Glasses with side shields___ Goggles ___ Face Shield ___ Other(s) ____________________________________
PENETRATION
1. Are employees exposed to any sources of penetration such as needles, pipettes, syringes,sharp objects, etc.? ___Yes___ No
2. Do employees perform any activities where there is a chance of the hands getting cut?___ Yes___ No
3. Are there any scrap metals, nails, wires, screws, tacks, or large staples being used by an employee? ___Yes___ No
4. Is there any area where an employee walks where sharp objects may pierce the feet? ___ Yes___ No
5. What personal protective equipment is recommended?___ Gloves ___ Safety glasses ___ Goggles ___ Foot Protection ___ Face Shield ___ Other(s) _____________________________________
HEAT
1. Are there any sources of high temperature in the work area such as boilers, furnace operations, glassmaking, cutting, welding, or casting? ___Yes___ No
2. Are there any sources of extreme cold temperatures in the work area such as cryogenic gases, dry ice,etc.? ___ Yes___ No
3. What personal protective equipment is recommended?___ Gloves ___ Face Shields ___ Safety Glasses ___ Goggles ___ Other(s) ______________________________________
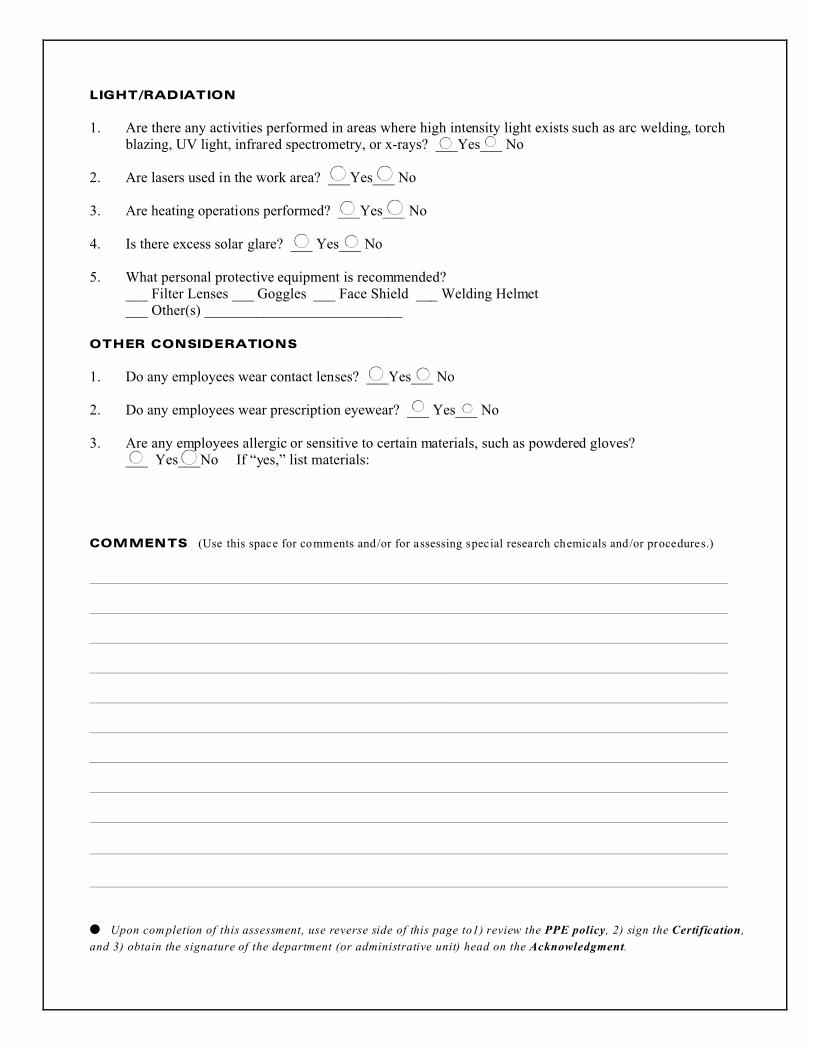
LIGHT/RADIATION
1. Are there any activities performed in areas where high intensity light exists such as arc welding, torchblazing, UV light, infrared spectrometry, or x-rays? ___Yes___ No
2. Are lasers used in the work area? ___Yes___ No
3. Are heating operations performed? ___Yes___ No
4. Is there excess solar glare? ___ Yes___ No
5. What personal protective equipment is recommended?___ Filter Lenses ___ Goggles ___ Face Shield ___ Welding Helmet___ Other(s) ___________________________
OTHER CONSIDERATIONS
1. Do any employees wear contact lenses? ___Yes___ No
2. Do any employees wear prescription eyewear? ___ Yes___ No
3. Are any employees allergic or sensitive to certain materials, such as powdered gloves?___ Yes___No If “yes,” list materials:
COMMENTS (Use this space for comments and /or for assessing special research chemicals and/or procedures.)
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
� Upon completion of this assessment, use reverse side of this page to1) review the PPE policy, 2) sign the Certification,
and 3) obtain the signature of the department (or administrative unit) head on the Acknowledgment.
11F-OEHS /Tulane (Rev 8/03) PPE
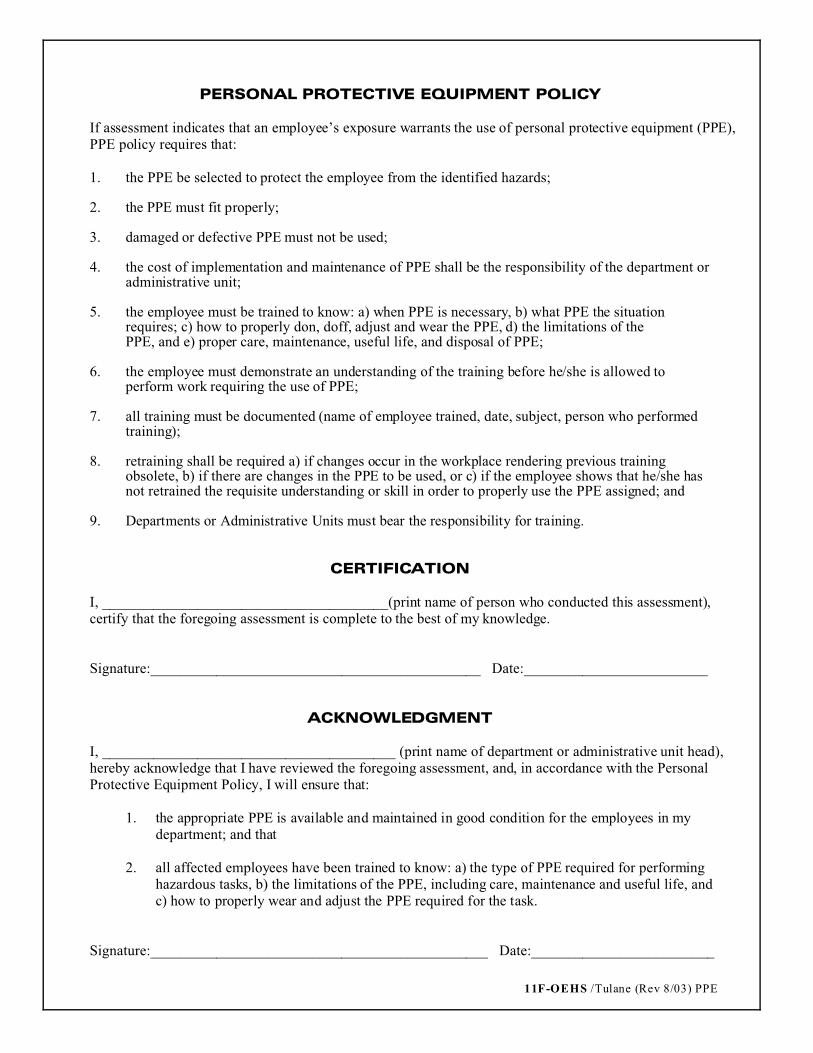
PERSONAL PROTECTIVE EQUIPMENT POLICY
If assessment indicates that an employee’s exposure warrants the use of personal protective equipment (PPE),PPE policy requires that:
1. the PPE be selected to protect the employee from the identified hazards;
2. the PPE must fit properly;
3. damaged or defective PPE must not be used;
4. the cost of implementation and maintenance of PPE shall be the responsibility of the department oradministrative unit;
5. the employee must be trained to know: a) when PPE is necessary, b) what PPE the situationrequires; c) how to properly don, doff, adjust and wear the PPE, d) the limitations of thePPE, and e) proper care, maintenance, useful life, and disposal of PPE;
6. the employee must demonstrate an understanding of the training before he/she is allowed toperform work requiring the use of PPE;
7. all training must be documented (name of employee trained, date, subject, person who performedtraining);
8. retraining shall be required a) if changes occur in the workplace rendering previous trainingobsolete, b) if there are changes in the PPE to be used, or c) if the employee shows that he/she hasnot retrained the requisite understanding or skill in order to properly use the PPE assigned; and
9. Departments or Administrative Units must bear the responsibility for training.
CERTIFICATION
I, _______________________________________(print name of person who conducted this assessment),certify that the foregoing assessment is complete to the best of my knowledge.
Signature:_____________________________________________ Date:_________________________
ACKNOWLEDGMENT
I, ________________________________________ (print name of department or administrative unit head),hereby acknowledge that I have reviewed the foregoing assessment, and, in accordance with the PersonalProtective Equipment Policy, I will ensure that:
1. the appropriate PPE is available and maintained in good condition for the employees in mydepartment; and that
2. all affected employees have been trained to know: a) the type of PPE required for performinghazardous tasks, b) the limitations of the PPE, including care, maintenance and useful life, andc) how to properly wear and adjust the PPE required for the task.
Signature:______________________________________________ Date:_________________________