T.R.N.C NEAR EAST UNIVERSITY INSTITUTE OF HEALTH SCIENCES
57
T.R.N.C NEAR EAST UNIVERSITY INSTITUTE OF HEALTH SCIENCES CRITICAL CARE NURSES’ KNOWLEDGE ON PREVENTION OF VENTILATOR ASSOCIATED PNEUMONIA AND BARRIERS OF ADHERENCE TO PREVENTIVE MEASURES MOATH ALKHAZALI In Partial Fulfillment of the Requirements for the Degree of Master of Nursing (Emergency Nursing) NICOSIA 2017
Transcript of T.R.N.C NEAR EAST UNIVERSITY INSTITUTE OF HEALTH SCIENCES

T.R.N.C
NEAR EAST UNIVERSITY
INSTITUTE OF HEALTH SCIENCES
CRITICAL CARE NURSES’ KNOWLEDGE ON
PREVENTION OF VENTILATOR ASSOCIATED
PNEUMONIA AND BARRIERS OF ADHERENCE TO
PREVENTIVE MEASURES
MOATH ALKHAZALI
In Partial Fulfillment of the Requirements for the
Degree of
Master of Nursing (Emergency Nursing)
NICOSIA 2017

T.R.N.C
NEAR EAST UNIVERSITY
INSTITUTE OF HEALTH SCIENCES T.R.N.C
CRITICAL CARE NURSES’ KNOWLEDGE ON
PREVENTION OF VENTILATOR ASSOCIATED
PNEUMONIA AND BARRIERS OF ADHERENCE TO
PREVENTIVE MEASURES
MOATH ALKHAZALI
Master of Nursing (Emergency Nursing)
Advisor:
Prof. Dr. Nurhan Bayraktar
NICOSIA 2017

I
APPROVAL
The Directorate of Graduate School of Health Sciences, This study has been
accepted by the thesis committee in nursing program as a master of
emergency nursing thesis.
Thesis Committee:
Chairman: Assoc. Prof. Ümran DAL YILMAZ (Near East University).
Member: Professor, Nurhan BAYRAKTAR (Near East University).
Member: Assist. Prof. Gülten SUCU DAĞ (Eastern Mediterranean University).
Approval:
According to the relevant article of the Near East University Postgraduate
Study-Education and Examination Regulation, this thesis has been approved
by the above-Mentioned members of the thesis committee and the decision of
the board of Directors of the Institute.
Professor, K. Hüsnü Can BAŞER
Director of Graduate Institute of Health Sciences

II
DECLARATION
I hereby declare that the work in this thesis entitled “Critical Care Nurses’ Knowledge
on Prevention of Ventilator Associated Pneumonia and Barriers of Adherence to
Preventive Measures.” is the study of my own research efforts undertaken under the
supervision of Prof. Dr. Nurhan Bayraktar.
My deepest thanks to Prof. Dr. Nurhan Bayraktar, my supervisor, for her expertise,
on-going support and mentorship during my research.
A special thank you to my committee members, Assoc. Prof. Ümran DAL YILMAZ,
Assist. Prof. Gülten SUCU DAĞ and Assist. Prof. Burcu TOTUR DİKMEN for
their invaluable feedback and support with this thesis.
I express my profound gratitude to my parents for their support, constant
encouragement through all my years of study and through the process of researching
and writing the thesis.
Thank you as well to my colleagues and dearest friends for all your encouragement and
guidance.

III
Critical Care Nurses’ Knowledge on Prevention of Ventilator
Associated Pneumonia and Barriers of Adherence to Preventive
Measures
ABSTRACT
Introduction: Ventilator associated pneumonia (VAP) is the most prevalent infection
in intensive care units (ICUs), with the highest mortality rate among nosocomial
infections. There is a need to increase knowledge and awareness of nurses on VAP risks
and prevention to avoid complications.
Objectives: The aim of the study is determination of the knowledge on prevention of
ventilator associated pneumonia and barriers of adherence to preventive measures of
the critical care nurses.
Methods: The study was performed as descriptive design on critical care nurses (n =
193) in two hospitals of Jordan. A questionnaire that was developed by the researchers
was used as data collection tool. Data were collected in June-July 2017. Descriptive
statistics and Pearson Chi-Square tests were used in analysis of the data.
Results: Results of the present study showed high level of knowledge on general VAP
knowledge and VAP prevention. Regarding to barriers of nurses to adherence to VAP
prevention guidelines, there were high rates of “sometimes” and “always” and low rates
of the “never” answers. The main self-reported barriers towards evidence-based
guidelines were Shortage of staff in the ICU, Lack of time and educational programs
on VAP.
Conclusions: Continuous educational programs in order to enhance the knowledge and
practices of the nurses on VAP, and national and institutional regulations to prevent
barriers of VAP prevention were recommended.
Keywords: Critical care nurses, VAP, Prevention, Knowledge, Barriers.

IV
List of content
APPROVAL .............................................................................................................. I
DECLARATION ...................................................................................................... II
ABSTRACT ..............................................................................................................3
List of Abbreviations ..................................................................................................7
1. INTRODUCTION ..................................................................................................1
1.1 Problem Definition ..........................................................................................1
1.2 Aim of the Study..............................................................................................4
2. BACKGROUND ....................................................................................................4
2.1. Definition ........................................................................................................4
2.2. Risk Factors for VAP .....................................................................................5
2.3. Prevention of VAP .........................................................................................6
2.4. Nurses’ Roles and Barriers in VAP Prevention ............................................8
3. METHODOLOGY ............................................................................................... 10
3.1 Study Design: ................................................................................................ 10
3.2 Study Setting: ................................................................................................ 10
3.3 Sample Selection: .......................................................................................... 10
3.4 Study Tools:................................................................................................... 10
3.5 Pilot Study: .................................................................................................... 11
3.6 Data Collection: ............................................................................................. 11
3.7 Ethical Aspect: .............................................................................................. 11
3.8 Analysis of Data: ........................................................................................... 11
4. RESULTS ............................................................................................................ 12
5. DISCUSSION ...................................................................................................... 25
6. CONCLUSION .................................................................................................... 29
7. FINDINGS AND RECOMMENDATIONS.......................................................... 30
7.1. Findings ........................................................................................................ 30
7.2 Recommendations ........................................................................................ 31
8. REFERENCES ..................................................................................................... 32

V
List of Tables
Table 4.1 Descriptive Characteristics of the Nurses (N= 193) .................................12
Table 4. 2 Characteristics of the Nurses on VAP Education (N= 193) ......................13
Table 4. 3 Nurses General Knowledge on VAP (N=193).........................................15
Table 4.4 Nurses’ Knowledge on Prevention of VAP (N=193) ...............................16
Table 4. 5 Barriers of Nurses to Adherence to VAP Prevention Guidelines (N=193)
.................................................................................................................................18
Table 4. 6 Comparison of Nurses` Educational Degree, Years of ICU Experience and
Previous VAP Education with General Knowledge on VAP (N=193) .......................19
Table 4.7 Comparison of Nurses` Educational Degree, Years of ICU Experience and
Previous VAP Education with Knowledge on prevention of VAP (N=193) ..............20
Table 4. 8 Comparison of Nurses` Educational Degree, Years of ICU Experience and
Previous VAP Education with Nurses ` Barriers to Adherence to VAP Prevention
Guidelines (N=193) ..................................................................................................24

VI
List of Appendix
APPENDIX 1 Critical Care Nurses’ Knowledge on Prevention of Ventilator
Associated Pneumonia (VAP) and Barriers of Adherence to Preventive Measures
.................................................................................................................................41
APPENDIX 2 King Abdullah University Hospital Ethical Approval Form .......45
APPENDIX 3 Islamic Hospital Ethical Approval Form ......................................46
APPENDIX 4 Ethical Approval Near East institutional Reviews Board ............47
APPENDIX 5 Informed Consent Form For Adults .............................................48

VII
List of Abbreviations
Hospital Acquired Infections HAI
Centers For Disease Control And Prevention CDC
Ventilator Associated Pneumonia VAP
Intensive Care Units ICUs
Endotracheal Tube ETT
Mechanical Ventilator MV
Acute Respiratory Distress Syndrome ARDS
Institute For Healthcare Improvement IHI
Noninvasive Positive Pressure Ventilation NIPPV
Ventilator Associated Event VAE
Deep Vein Thrombosis DVT
Spontaneous Awakening Trials SATs
Spontaneous Breathing Trials SBTs
Head Of Bed HOB
Polyvinyl Chloride PVC
Nurse Assistants RAs
Registered Nurses RNs

1
1. INTRODUCTION
1.1 Problem Definition
Hospital acquired infections (HAI), also known as nosocomial infections
are important problem all over the world. This term is used for any disease acquired by
patient under medical care (Krishna, 2014). Recently, a new term, “healthcare
associated infections” is used for the type of infections caused by prolonged hospital
stay and it accounts for a major risk factor for serious health issues leading to
death (Brusaferro et al, 2015). About 75% of the burden of these infections is present
in developing countries (Obiero et al, 2015). The U.S.A Centers for Disease Control
and Prevention (CDC, 2015) estimates that HAIs in American hospitals account for
approximately 1.7 million infections and 99,000 associated deaths each year. Based on
a study of a large sample of the U.S.A. acute care hospitals, on any given day,
approximately 1 in 25 hospital patients has at least one healthcare-associated infection
(CDC, 2015). In the U.S.A. the direct costs associated with HAIs have been estimated
at >$30 billion annually (Cusumano-Towner et al, 2013). In some countries of the
Eastern Mediterranean Region (Morocco, Jordan and Tunisia), prevalence studies on
the rates of health care-associated infections conducted between 2004 and 2008 have
found them to be between 12% and 18% ( Allegranzi, 2010). There are many type of
hospital acquired infections, but the most common health care associated infections are
ventilator associated pneumonia (VAP), urinary tract infection (catheter associated),
bloodstream infection (associated with the use of intravascular device) and surgical-site
infection.
VAP is the most prevalent infection in intensive care units (ICUs), with the
highest mortality rate among nosocomial infections (Albertos et al, 2011). It accounts
for 25 % of all types of intensive care unit acquired infections (Balkhy, 2014). In the
United States, the incidence is 3-5 cases per 1,000 ventilator-days (Spalding et al,
2017). A recent prospective surveillance study found that VAP prevalence was 15.6%
globally (13.5% in the USA, 19.4% in Europe, 13.8% in Latin America and 16.0% in
Asia Pacific) (Kollef, 2014).
2
VAP results in a significant increase in the cost of care (van Oort et al 2017),
prolonged hospitalization (Kandeel et al 2012), an extended number of days in need of
the mechanical ventilator (Khan et al 2017), and a significant increase in the rate of
mortality (Porhomayon et al 2017). The mortality rate of this infection ranges from 20
to 70% (Azab et al 2013, Kandeel et al 2012).
VAP is an infection of the lung that occurs 48 hours after insertion of an
endotracheal tube (Rodrigues et al, 2017). The principal factor for the development of
VAP is the presence of an endotracheal tube (Zolfaghari et al, 2011). A ventilator is a
device that is used to improve patient breathe by giving oxygen via tube placed in the
nose or mouth, or through a hole in the front of the neck (tracheostomy). An infection
occur when the germs enter via tube and reach to patient`s lung and caused lung
infection (alveoli infection). These tubes interfere with the normal protective upper
airway reflexes, prevent effective coughing, and encourage micro aspiration of
contaminated pharyngeal contents (He et al, 2014).
Many risk factors cause to ventilator associated pneumonia (VAP). The risk
factors for VAP can be divided into 3 categories: host related (such as acute respiratory
distress syndrome) device related (such as the ventilator circuit) and personnel related
(such asfailure to wash hands) (Casado et al, 2011). In a study, re-intubation was found
as a risk factor for VAP in patients who had ever undergone cardiac surgery (He et al,
2014). It is important to control modifiable factors.
There is no single method to prevent VAP, but multiple non-pharmacological
and pharmacological interventions exist that could reduce the incidence and severity of
VAP (Lim et al, 2015; Shitrit et al, 2015). CDC ( 2012) provides guidelines and tools
to the healthcare community to help end ventilator-associated pneumonia and resources
to help the public understand these infections and take measures to safeguard their own
health when possible (CDC, Health Healthcare-associated Infections Update Guideline
2012). There are a lot of recommendations to prevent VAP like head elevated 30-45
and good oral hygiene, selective oral or digestive decontamination (Liberati et al, 2009),
and facilitate early mobility (Lord et al, 2013; Needham et al, 2010). According to the
previously published studies, the implementation of a VAP prevention bundle had been
proven to be efficacious in reduction of VAP rates (Lim et al, 2015; Shitrit et al, 2015).

3
Quality nursing care based on evidence-based strategies is efficient ways of
preventing VAP in intensive care units (ICUs) (Akın, 2014). Nurses play an important
role to prevent VAP and improve the patient`s outcome if they are well-educated. The
application of knowledge to the care of critically ill patients is a hallmark of
professional nursing practice. Many non-pharmacological evidence-based strategies
aimed at preventing VAP can be seen as part of basic and routine nursing care, a direct
responsibility of the bedside intensive care nurse and can easily be instituted at minimal
costs; neglecting any of these could put the patient at risk of infection (Llauradó et al,
2011).
There are many barriers to ventilator associated pneumonia (VAP) prevention
and practice among nurses. The most of these barriers is including shortage of
resources, insufficient compliance with infection-control standards (AL-Rawajfah et al,
2014) and inadequate knowledge about VAP among health care providers (Hassan et
al, 2016). Insufficient knowledge of the nurses ‘about the guidelines results in a lack of
competence, and is considered a barrier to adherence (Yeganeh et al, 2016; Ha et al,
2016).
Determination of the knowledge on prevention of ventilator associated
pneumonia and barriers of adherence to preventive measures of the critical care nurses
may be useful in improving their awareness, practices and preventing this important
problem. However a study was not found in the Jordan about this subject and studies.

4
1.2 Aim of the Study
The aim of the study is determination of the knowledge on prevention of ventilator
associated pneumonia and barriers of adherence to preventive measures of the critical
care nurses. Study questions include followings:
What is the knowledge on prevention of ventilator associated pneumonia of
critical care nurses?
What are the barriers of adherence to preventive measures of ventilator
associated pneumonia of the critical care nurses?
Is there any difference between descriptive characteristics, and knowledge on
prevention of ventilator associated pneumonia and barriers of adherence to
preventive measures of the critical care nurses?
2. BACKGROUND
2.1. Definition
Ventilator associated pneumonia (VAP) is defined as a type of pneumonia that
is an acquired from the hospital in a patient who connected to mechanical ventilator
support via tracheostomy or endotracheal tube for more than 48 hours with signs and
symptoms indicate to pneumonia. VAP is considered the most common hospital
acquired infection. VAP characterized by new or progressive pulmonary infiltrate and
one or more of the following findings: decrease in oxygen saturation and tidal volume;
increase in respiratory rate, white blood cells (leukocytosis) and body temperature
(fever); and purulent tracheobronchial secretions. The studies have reported that 27%
of intubated patients develop VAP during hospitalization (Spalding et al 2017).
Intubation is an invasive procedure, and puts patients at risk in developing a HAI
(Mietto et al, 2013). The process of intubation decreases the body’s natural response to
infection by disrupting the ability to initiate a cough or gag reflex that assists in
expelling secretions, as a result, secretions settle around the posterior portion of the
pharynx and can eventually lead to micro-aspiration (Sedwick et al, 2012). Proper
inflation of the endotracheal tube (ETT) cuff does not prevent micro-aspiration, because
there is a small opening that allows leakage of the secretions to travel (Mietto et al,
2013).

5
2.2. Risk Factors for VAP
There are many risk factors for VAP. Although any patient connected to
mechanical ventilator (MV) for more than 48 hours is at risk for VAP; host related,
device related, and personnel related factors are considered as categories of VAP risk
factors (Casado et al, 2011).
Host related factors include the problems which previously exist such as:
immune deficiency, acute respiratory distress syndrome (ARDS), and chronic
obstructive lung disease. There are other host-related factors including patients’ body
positioning, level of consciousness, number of intubations, and medications, including
sedative agents and antibiotics (Fathy et al, 2013).
Device related risk factors include, use the nasal route to place endotracheal
tubes, un-clean ventilator circuit, and un-cuffed endotracheal tubes. Insufficient cuff
pressure leads to aspiration of oropharyngeal contents (Sole et al, 2011).
Lack of stuff hand washing due to cross-contamination from patient to another
and it is the most personnel-related risk factor for VAP. Failure to wash hands and
change gloves between contaminated patients has been associated with an increased
incidence of VAP (Labeau et al, 2007).
The risk factors for VAP differ between adults and children. The duration of
mechanical ventilation is a risk for both groups, but the results of studies in children
have differed somewhat from the results of studies in adults (Casado et al, 2011).
Primarily, unlike adults, children have developmental and physiological differences for
a wide range of ages. Age is also a factor in immunity, so younger or preterm infants
are more likely than older children or adults to experience infection and to have more
frequent episodes of infection (Casado et al, 2011).

6
2.3. Prevention of VAP
VAP prevention is performed through pharmacological and non-
pharmacological measures that mainly focus on modifiable risk factors. The Center for
Disease Control and Prevention (CDC) and Institute for Healthcare Improvement (IHI)
have introduced recommendations (Andrews et al, 2013; Munro et al, 2014). There are
many recommendations to prevent VAP:
Avoiding intubation if possible and use noninvasive positive pressure
ventilation (NIPPV) whenever feasible is recommended. NIPPV can be
beneficial for patients with acute hypercarbic or hypoxemic respiratory failure
secondary to chronic obstructive pulmonary disease or cardiogenic congestive
heart failure. NIPPV for these indications may decrease VAP risk, shorten the
duration of mechanical ventilation, decrease length of stay, and lower mortality
rates compared with invasive ventilation (Klompas et al, 2014).
Managing ventilated patients without sedatives whenever possible.
Preferentially use agents and strategies other than benzodiazepines to manage
agitation, such as analgesics for patients in pain, reassurance, antipsychotics,
dexmedetomidine and propofol is recommended. Sedation should be interrupted
once a day (spontaneous awakening trials) for patients without
contraindications. Assessing readiness to extubate once a day (spontaneous
breathing trials) in patients without contraindications is recommended. Pairing
spontaneous breathing trials with spontaneous awakening trials is necessary
(Klompas et al, 2014).
Minimizing pooling of secretions above the endotracheal tube cuff is
recommended (Klompas et al, 2014).
Changing the ventilator circuit only if visibly soiled or malfunctioning is
recommended. Changing the ventilator circuit as needed rather than on a fixed
schedule has no impact on VAP rates or patient outcomes but decreases costs
(Klompas et al, 2014).

7
Elevating the head of the bed to 30–45 degree (Keeley, 2007); Head of bed
elevated between 30 to 45 degree is a simple nursing measure to reduce VAP;
Keeping the head of bed elevated has been shown to help prevent aspiration of
gastric contents and secretions (Klompas et al, 2014; Schallom et al, 2015).
Providing early exercise and mobilization: Early exercise and mobilization
speed extubation, decrease length of stay, and increase the rate of return to
independent function (Klompas et al, 2014).
Prophylactic probiotics: Four meta-analyses of randomized controlled trials
have found an association between probiotics and lower VAP rates (Barraud et
al, 2013; Siempos et al, 2010).
Good oral hygiene: Oral care may seem to be a simple task, but it can be
challenging to implement. Swabbing a patient’s mouth with an antiseptic mouth
wash has been recommended for comfort, but recent studies have demonstrated
that oral care with an antiseptic has also reduced the risk for Ventilator
Associated Event (Garcia et al, 2009). Chlorhexidine is a broad spectrum
antiseptic agent (gram-positive, gram-negative, and yeast) which is easy to use,
safe, and cost-effective. Additionally, chlorhexidine's slow release properties
maintain antimicrobial activity up to 12h (Osman, 2014; Williams al, 2012).
Use of mechanical tooth brushing (Alhazzani et al, 2013; Yao et al, 2011).
Saline instillation before tracheal suctioning (Caruso et al, 2009) is
recommended. One randomized trial in oncology patients found that saline
instillation before tracheal suctioning lowered the rate of microbiologically
confirmed VAP but had no impact on clinical VAP rates or patient outcomes
(Klompas et al, 2014).
Automated control of endotracheal tube cuff pressure between (20 to 30 cm) is
recommended (Nseir et al, 2011; Valencia et al, 2007).
Endotracheal tubes with ultrathin polyurethane cuff membranes of 7 mm only
have been introduced to prevent the formation of folds within the cuff and fluid
and air leakage. These devices have shown to reduce the frequency of early
postoperative pneumonia in cardiac surgical patients (Poelaert et al, 2014).

8
The development by the Institute of Healthcare Improvement (IHI) of VAP
“bundles”—a series of performance measures associated with reducing the incidence
of VAP—was an important step in the overall evolution of process measures and
accountability for changing clinical behavior and improving the quality of care for
critically ill patients (Resar et al, 2012). The VAP prevention bundle includes: head-of-
bed elevation to 30 to 45 degrees, oral care with chlorhexidine at 0.12 percent, peptic
ulcer disease prophylaxis, deep vein thrombosis (DVT) prophylaxis and ABCDEF
bundle elements (i.e. assess, prevent and manage pain — both spontaneous awakening
trials and breathing trials, choice of analgesia and sedation, delirium assessment,
prevention and management, exercise and early progressive mobility and family
engagement and empowerment) (Frimppong et al, 2014; Institute for Healthcare
Improvement, 2012).
2.4. Nurses’ Roles and Barriers in VAP Prevention
Nurses are the most contact with patients and they playing a main role to prevent
VAP and increase the positive patient`s outcome if the nurse receive well-educated.
The nurses’ main practice roles to prevent VAP include:
Assessing readiness to extubate daily through combined spontaneous awakening
trials (SATs: sedation interruption/minimization) and spontaneous breathing trials
(SBTs), unless clinically contraindicated (Balas et al, 2014; Yang et al, 2014).
Elevating the head of bed (HOB) to 30 to 45 degree unless clinically contraindicated
in patients receiving mechanical ventilation, as well as patients at high risk for
aspiration (Alexiou et al, 2009).
Utilizing endotracheal tubes with subglottic secretion drainage ports for patients
expected to require greater than 48 or 72 hours of mechanical ventilation (Muscedere
et al, 2011).
Collaborating to identify patients where implementation of noninvasive positive
pressure ventilation (NIPPV) may be appropriate to prevent the need for intubation
(Burns et al, 2013).
Good hand hygiene and oral care and change gloves between the patients.
Changing the ventilator circuit only if visibly soiled or malfunctioning (Lorente et
al, 2004).
Using sterilize equipment and aseptic technique.

9
Adherence the nurses to prevention measures is playing important role to reduce
probability of VAP because the nurses is most connected with the patients. However,
there are a lot of nursing practice barriers among VAP prevention. In the same line the
study conducted by (Jordan et al., 2014) that notices the main barriers to using VAP
guidelines are lack of VAP courses and nursing shortages and lack of time was
identified as another barrier. In another hand, a survey study revealed poor information
provided to nurses regarding current guidelines and the lack of instruction in VAP
prevention methods in nursing schools (Jansson et al., 2013). The lack of knowledge
may be a barrier towards adherence to evidence-based guidelines (El-Khatib et al.,
2010). Study that published in (Aloush, 2017) revealed Jordanian nursing students had
poor knowledge.
Several studies implicated that education, guidelines as well as ventilator
bundles and instruments should be developed and updated to improve infection control
(Jansson et al. 2013). A study that held at Jordan's nursing schools with (Al-Hussami et
al 2013) recommended that the nursing curriculum should include additional emphasis
on practice as a means to help translate theory into clinical behavior. There are many
educational programs that were linked to significant improvements in the overall
adherence to VAP evidence-based strategies and a significant decrease in VAP rates.
Educational programs consisted of self-study modules (Abbot, 2006), repeated lectures
(Bloos, 2009), teaching materials (Morris, 2011), multidisciplinary education meetings
(Morris, 2011) and reminders, such as e-mails (Abbot, 2006), posters (Morris, 2011)
and visual aids, Also reported that the clinical outcomes of educational programs was
decreasing in the incidence of VAP (Morris, 2011).

11
3. METHODOLOGY
3.1 Study Design:
The study was planned as descriptive design.
3.2 Study Setting:
The study was conducted at the King Abdullah University Hospital and Islamic
Hospital Jordan. The King Abdullah University Hospital is the largest and leading
university of Jordan which is located in northern part of Jordan in Irbid city. The
hospital consists of 15 floors and 683 beds,12 operating theatres, 78-bed Intensive Care
Unit (divided into medical, surgical, pediatric, neonatal, cardiac and burn) and has
hospital protocol for prevention the VAP is (bundle VAP protocol). Islamic hospital
has 300 beds, 8 operating theatres and 25 intensive care bed, and hospital protocol for
prevention the VAP.
3.3 Sample Selection:
The study was performed on the registered nurses who work in ICU departments
of the King Abdullah University Hospital and Islamic Hospital. A total of 132 nurses
work in ICU in the King Abdullah University Hospital and 61 nurses in ICU in Islamic
Hospital (Total 193 nurses). There was no sample selection method. Total 193
voluntary nurses who work in ICU clinics was composed the sample of the study.
3.4 Study Tools: A questionnaire that was developed by the researchers on the basis of
the literature was used as data collection tool in this study (Yaseen et al
2015); (Jansson, et al 2013) (Appendix 1). The first section was regarding to
demographics characteristics of the nurses and included 10 questions. The
second section consisted 30 questions regarding knowledge of nurses on
VAP prevention with “True / False / I don’t know” choices. The last section
consisted 8 questions regarding the barriers to adherence to VAP prevention
measures with “Always / Sometimes / Never” choices. Since all of the nurses
in the hospital can speak English, the questionnaire was prepared as English.

11
3.5 Pilot Study:
A pilot study was performed on ten nurses after approval from the Near East
Institutional Reviews Board (IRB) and King Abdullah University Hospital and Islamic
Hospital. After the pilot study, revision was not necessary and the nurses who included
in pilot study were added to main sample.
3.6 Data Collection:
Data was collected using a questionnaire from 20th of June to 10th of July 2017.
The questionnaires were administered by researchers on nurses while they are on the
wards or clinics during duty shift with self-completion method. Completion of the
questionnaire took almost 20 minutes.
3.7 Ethical Aspect:
Ethical approval was obtained from the Near East Institutional Reviews Board
(IRB) of King Abdullah University Hospital and Islamic Hospital of Jordon (Appendix
2& Appendix 3). In addition, informed consent from the nurses and organizational
permission were obtained (Appendix 4).
3.8 Analysis of Data:
Statistical Package of Social Sciences (SPSS) software version 20.0 was used
to analyze the collected data. The methods used to analyze the data include an analysis
of descriptive statistic variables such as frequency and percentages for the categorical
variables. “True / False’’ variables were used in evaluations of knowledge questions,
the comparison were between only always scale and educational degree, years of nurses
experience and previous VAP education of the nurses barriers. The person chi-squire
test was used in comparisons. When finding statistic was significant, the chosen level
of significance is p < 0.05.

12
4. Results
Table 4.1 Descriptive Characteristics of the Nurses (N= 193)
Description of characteristics of the nurses is shown in Table 4.1. A total of the nurses
of participants in this study 193, the mean of ages of the participants were 28.4 and the
26-30 group of age was the most frequent (56.5%). Females were the majority of the
Participants (60.1%). Most of the participants have bachelor's degree (89.7%). Majority
of the nurses have experience less than five years as a registered nurses (60.1%). The
number of beds were approximately the same for the groups where the percent of
participants working in ICU beds <=12 beds was 50.3%.
% N Descriptive characteristics
Age (Mean :28.4)
22.8 44 <=25 years
56.5 109 26-30 years
20.7 40 >=31
Gender
39.9 77 Male
60.1 116 Female
Educational degree
89.7 173 Bachelor`s
10.3 20 Master degree
Working experience in the ICU
60.1 116 <=5 years
34.7 67 6-10 years
5.2 10 >=11
Number of beds in ICU
50.3 97 <=12 beds
49.7 96 >=13 beds
13
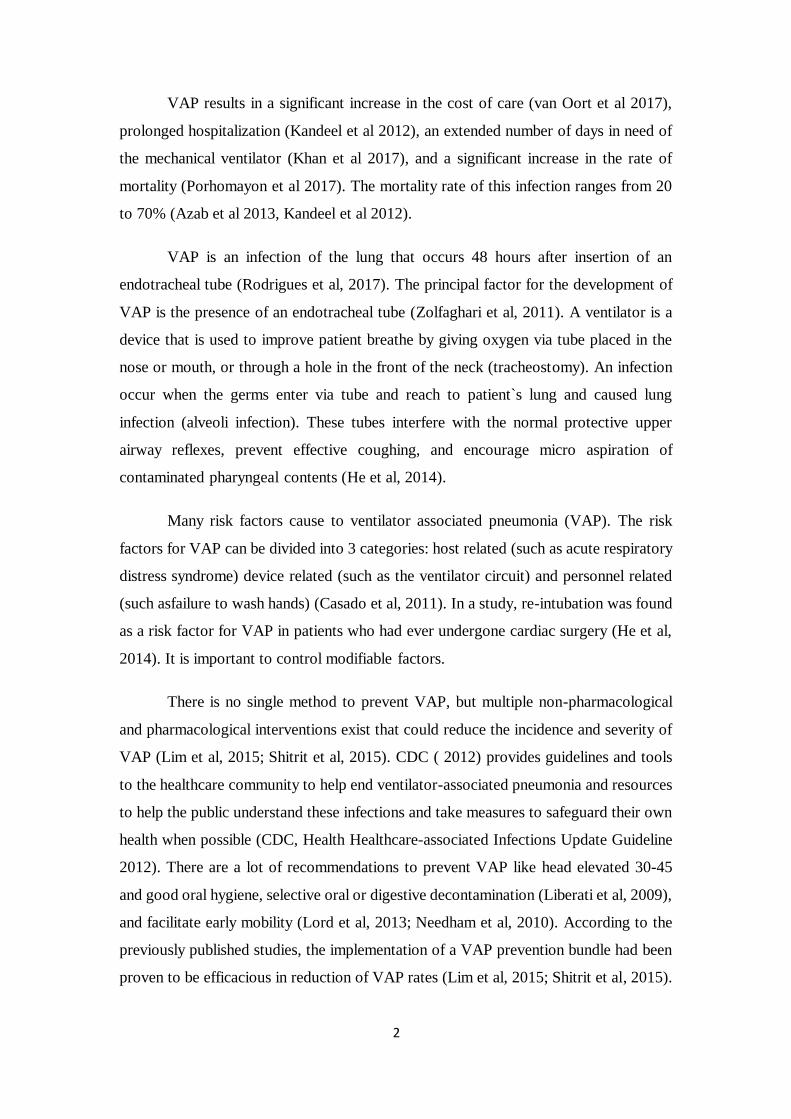
Table 4. 2 Characteristics of the Nurses on VAP Education (N= 193)
*Percentage were calculated based on N=137
% N Characteristics on VAP Education
Previous VAP education
71.0 137 Yes
29.0 56 No
Educational resource (N=137)*
15.4 21 School
34.3 47 Courses
13.1 18 Web resources
23.4 32 In-service education
2.9 4 Congress\Conferences
10.9 15 Other
Opinions about quality of the VAP Education (N=137)*
10.2 14 Excellent
19.0 26 Very good
57.7 79 Good
10.9 15 Fair
2.2 3 Poor
Need for education on VAP
79.8 154 Yes
20.2 39 No
Using Hospital protocol on prevention of VAP
90.7 175 Yes
9.3 18 No

14
The description of characteristics of the nurses on VAP education is shown in Table
4.2. The majority of the nurses had received VAP education (71.0%). There are six
categories of educational recourse which the participants had received VAP education.
The highest percent was the courses as educational resource (34.3%). Most frequently
stated opinion by the nurses on quality of VAP education was “good” (57.7%). The
majority of nurses need for education on VAP (79.8%) and there are hospital protocols
on prevention of VAP (90.7%).
15
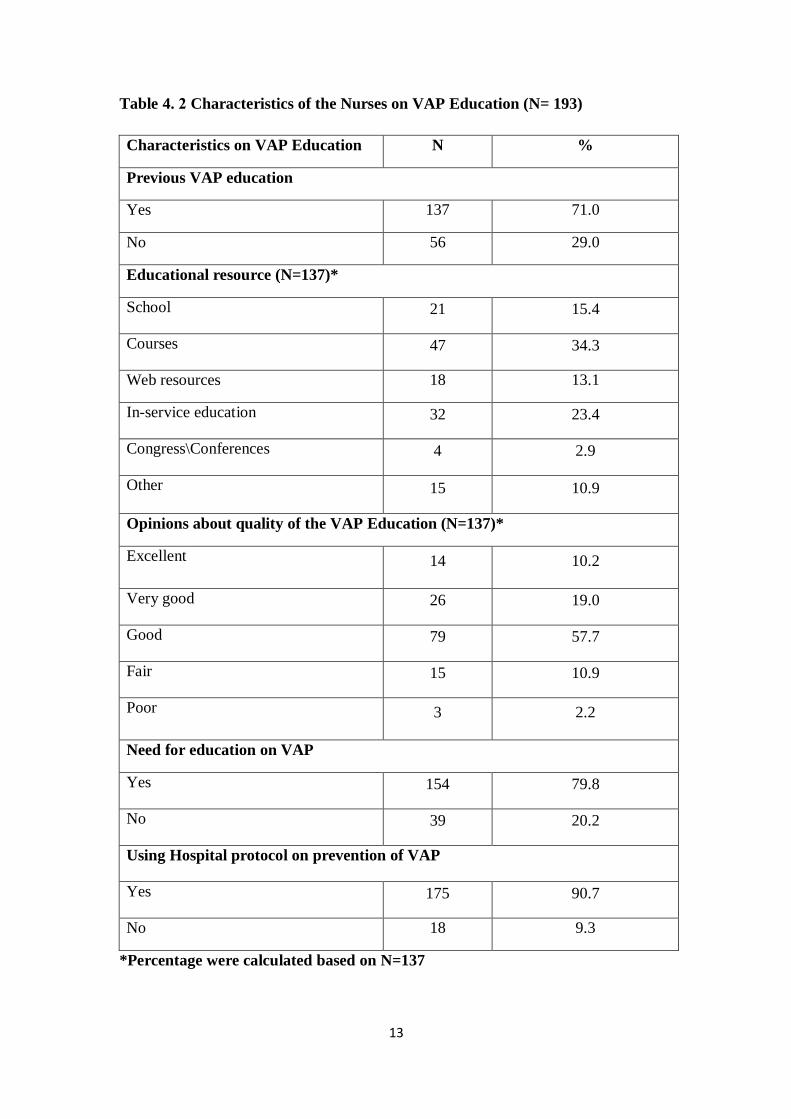
Table 4. 3 Nurses General Knowledge on VAP (N=193)
*(T) = True statement, (F) = False statement
Table 4.3 shows nurses` general knowledge on VAP. It was found that; majority of the nurses
had correct answers in majority of the items (5 of 6 items). The most frequently known items
were "Continuous education to ICU nurses on prevention of nosocomial infection is
associated with decreased rates of VAP" (T) (88.6%), "VAP is cause of highest mortality rate
among nosocomial infections" (T) (86.5%) and “The Ventilator Associated Pneumonia
(VAP) is pneumonia that occurs > or equal 48 hours after endotracheal intubation” (81.3%)
respectively. Percentages of the correct answers of the nurses were close in item "Automated
control of endotracheal tube cuff pressure is important because it decrease the risk for VAP"
(T) (The correct answers: 53.4% and the wrong\ I don`t know answers: 46.6%).
Statements on VAP
T\F
Correct answer Wrong \I don’t
know answer
N % N %
The Ventilator Associated Pneumonia (VAP) is
pneumonia that occurs > or equal 48 hours after
endotracheal intubation.
T 157 81.3 36 18.7
VAP is cause of highest mortality rate among
nosocomial infections. T 167 86.5 26 13.5
VAP is the most prevalent infection in intensive care
units. T 145 75.1 48 24.8
Automated control of endotracheal tube cuff
pressure is important because it decreases the risk
for VAP.
T 103 53.4 90 46.6
Over feeding a ventilated patient is associated with
increased the risk for VAP. T 150 77.7 43 22.3
Continuous education to ICU nurses on prevention
of nosocomial infection is associated with decreased
rates of VAP.
T 171 88.6 22 11.4

16
Table 4 .4 Nurses’ Knowledge on Prevention of VAP (N=193)
Statements on Prevention of VAP
T\F Correct answer
Wrong /I don’t
know answer
N % N %
If possible, intubation should be avoided to prevent
VAP. T 141 73.1 52 26.9
Whenever feasible, noninvasive positive pressure
ventilation should be used to prevent VAP T 102 52.8 91 47.1
It is necessary to manage patients without sedation
whenever possible to prevent VAP T 121 62.7 72 37.3
Benzodiazepines should always be preferred to
manage agitation F 83 43.0 110 57.0
Sedation should be interrupted daily to prevent
VAP T 124 64.2 69 35.8
It is necessary to assess readiness to extubate of the
patient daily to prevent VAP T 164 85.0 29 15
Pairing spontaneous breathing trials with
spontaneous awakening trials is not necessary F 69 35.8 124 64.3
Minimizing pooling of secretions above the
endotracheal tube cuff is necessary to prevent VAP T 133 68.9 60 31.1
Changing the ventilator circuit regularly is
necessary to prevent VAP F 146 75.6 47 24.3
Elevating the head of the bed to 30–45 is important
in prevention of VAP T 173 89.6 20 10.4
Early exercise and mobilization may increase the
possibility of VAP F 103 53.4 90 46.7
Regular oral care with chlorhexidine is necessary
to prevent VAP T 170 88.1 23 11.9
Proper sterilization and disinfection of respiratory
care equipment is important to prevent VAP T 169 87.6 24 12.4
Oral route is recommended for endotracheal
intubation to prevent VAP T 125 64.8 68 35.2
Prophylactic probiotics may be useful to prevent
VAP T 139 72.0 54 27.9
Ultrathin polyurethane endotracheal tube cuffs
may lower VAP rates T 71 36.8 122 63.2
Saline instillation before tracheal suctioning may
cause to VAP F 120 62.2 73 37.8
Mechanical tooth brushing may be useful in
prevention of VAP T 115 59.6 78 40.4
Closed/in-line endotracheal suctioning reduce the
risk of VAP F 143 74.1 50 25.9
Kinetic beds reduce the risk of VAP and
recommended F 126 65.3 67 34.8
Adequate hand hygiene between patients and
change gloves is important to prevent the VAP T 170 88.1 23 11.9

17
Prone positioning intermittently may prevent VAP
and recommended F 84 43.5 109 56.5
Using selective oral or digestive decontamination
to reduce risk VAP T 136 70.5 57 29.5
Care bundles may be useful in reducing VAP T 155 80.3 38 19.7
*(T) = True statement, (F) = False statement
Nurses` knowledge on prevention of VAP is shown in table 4.4 (53.6%) the percentage of total
frequency of correct answers and (46.4%) the total of wrong or "I don`t know" answers. The
highest correct answers were in “Elevating the head of the bed to 30–45 degree is important in
prevention of VAP” (89.6%), “Regular oral care with chlorhexidine is necessary to prevent VAP”
(88.1%), “Adequate hand hygiene between patients and change gloves is important to prevent the
VAP” (88.1%), "Proper sterilization and disinfection of respiratory care equipment is important
to prevent VAP " (T) (87.6%), " It is necessary to assess readiness to extubate of the patient daily
to prevent VAP " (T) (85.0%) and “Care bundles may be useful in reducing VAP” (80.3%) items
respectively. Most frequent wrong /I don’t know answers were in “Pairing spontaneous breathing
trials with spontaneous awakening trials is not necessary (64.3%). “Ultrathin polyurethane
endotracheal tube cuffs may lower VAP rates” (63.2%) with wrong answer, and "Prone
positioning intermittently may prevent VAP and recommended" (56.5%) items.

18
Table 4. 5 Barriers of Nurses to Adherence to VAP Prevention Guidelines (N=193)
Table 4.5 shows barriers of nurses to adherence to VAP Prevention Guidelines. It was
determined that, majority of nurse had "sometimes" answer for the barriers nurses to adherence
to VAP prevention guideline. Most frequent "always" answer was "Shortage of staff in the ICU"
(55.4%). Highest “sometimes” answers were “Lack of educational programs on VAP such as in-
service education or courses”, “Lack of time to deliver proper infection control” (55.4%),
“Forgetting to practice the sterile technique” (54.4%) and “Lack of VAP prevention knowledge”
(53.9%) respectively. Low frequencies in majority of the "never" answers were determined and
most frequent "never" answer was "Lack of equipment such as gloves and face masks"(43.5%).
Statements About Barriers
Always
Sometimes
Never
N % N % N %
Lack of VAP prevention knowledge 73 37.8 104 53.9 16 8.3
Lack of educational programs on VAP such as
in-service education or courses 74 38.3 107 55.4 12 6.2
Shortage of staff in the ICU 107 55.4 72 37.3 14 7.3
Lack of equipment such as gloves and face
masks 34 17.6 75 38.9 84 43.5
Lack of written VAP protocol in the hospital 44 22.8 87 45.1 62 32.1
Forgetting to practice the sterile technique 44 22.8 107 55.4 42 21.8
Lack of time to deliver proper infection control 44 22.8 105 54.4 44 22.8
Hospital system insufficiencies 54 28.0 87 45.1 52 26.9

19
General Knowledge on VAP
(Statements)
Educational Degree
P value
Years of ICU Experience
P value
Previous VAP Education
P
value
Bachelor Master <=5 6-10 >=11 Yes No
Correct answer Correct answer Correct answer
N % N % N % N % N % N % N %
The Ventilator Associated Pneumonia
(VAP) is pneumonia that occurs > or equal 48 hours after endotracheal
intubation
142 82.1 15 75.0 0.441 93 80.2 55 82.1 9 90.0 0.732 111 81.0 46 82.1 0.856
VAP is cause of highest mortality rate
among nosocomial infections 148 85.5 19 95.0 0.241 100 86.2 59 88.1 8 80.0 0.775 120 87.6 47 83.9 0.499
VAP is the most prevalent infection in
intensive care units 130 75.1 15 75.0 0.989 83 71.6 52 77.6 10 100. 0.115 111 81.0 34 60.7 0.003
Automated control of endotracheal tube cuff pressure is important because it
decreases the risk for VAP
96 55.5 7 35.0 0.082 67 57.8 36 53.7 0 0.0 0.002 84 61.3 19 33.9 0.001
Over feeding a ventilated patient is
associated with increased the risk for VAP
134 77.5 16 80.0 0.796 90 77.6 55 82.1 5 50 0.75 103 75.2 47 83.9 0.185
Continuous education to ICU nurses on
prevention of nosocomial infection is
associated with decreased rates of VAP
152 87.9 19 95.0 0.342 102 87.9 59 88.1 10 100. 0.507 126 92.0 45 80.4 0.021
Table 4. 6 Comparison of Nurses` Educational Degree, Years of ICU Experience and Previous VAP Education with General Knowledge on VAP
(N=193)
Table 4.6 shows that there were statistically significant differences between correct answers of some items on general knowledge on VAP and years of ICU experience
and previous VAP education. Nurses with <=5 (57.8%) and 6-10 (53.7%) years of experience had higher correct knowledge rates than the >=11 group (0.0) in terms
of “Automated control of endotracheal tube cuff pressure is important because it decreases the risk for VAP” item (P< 0.05). Nurses who had previous VAP education
had higher correct knowledge rates than the other group in terms of “VAP is the most prevalent infection in intensive care units” (81.0%), “Automated control of
endotracheal tube cuff pressure is important because it decreases the risk for VAP” (61.3%) and “Continuous education to ICU nurses on prevention of nosocomial
infection is associated with decreased rates of VAP” (92.0%) items (P< 0.05). However, there wasn’t statistically significant differences in terms of majority of the
items on general knowledge on VAP and educational degree, years of nursing experience and previous VAP education (P>0.05).

21
Knowledge on prevention of VAP
(Statements)
Educational Degree
P value
Years of ICU Experience
P
value
Previous VAP Education
P
value
Bachelor Master <=5 6-10 >=11 Yes No
Correct answer Correct answer Correct answer
N % N % N % N % N % N % N %
If possible, intubation should be
avoided to prevent VAP
124 71.7 17 85.0 0.204 84 72.7 53 79.1 4 40.0 0.033 97 70.8 44 78.6 0.270
Whenever feasible, noninvasive positive pressure ventilation should be
used to prevent VAP
90 52.0 12 60.0 0.499 55 47.4 42 62.7 5 50.0 0.135 73 53.3 29 51.8 0.850
It is necessary to manage patients
without sedation whenever possible to prevent VAP
109 63.0 12 60.0 0.792 73 62.9 42 62.7 6 60.0 0.983 86 62.8 35 62.5 0.972
Benzodiazepines should always be
preferred to manage agitation
79 45.7 4 20.0 0.028 48 41.4 30 44.8 5 50.0 0.814 63 46.0 20 35.7 0.191
Sedation should be interrupted daily
to prevent VAP
111 64.2 13 65.0 0.941 58.1 62.1 46 68.7 6 60 0.642 92 67.2 32 57.1 0.188
It is necessary to assess readiness to
extubate of the patient daily to prevent
VAP
145 83.8 19 95.0 0.185 96 82.8 60 89.6 8 80.0 0.419 119 86.9 27 80.4 0.251
Pairing spontaneous breathing trials
with spontaneous awakening trials is
not necessary
66 38.2 3 15.0 0.041 39 33.6 27 40.3 3 30.0 0.614 52 38.0 17 30.4 0.317
Minimizing pooling of secretions above the endotracheal
tube cuff is necessary to prevent VAP
121 69.9 12 60.0 0.363 74 63.8 52 77.6 7 70.0 0.150 100 73.0 33 58.9 0.055
Table 4.7 Comparison of Nurses` Educational Degree, Years of ICU Experience and Previous VAP Education with Knowledge on prevention of VAP (N=193)

21
Knowledge on prevention of VAP
(Statements)
Educational Degree
P
value
Years of ICU Experience
P
value
Previous VAP Education
P
value
Bachelor Master <=5 6-10 >=11 Yes No
Correct answer Correct answer Correct answer
N % N % N % N % N % N % N %
Changing the ventilator circuit
regularly is necessary to prevent VAP
132 76.3 14 70.0 0.534 83 71.6 57 85.1 6 60.0 0.060 109 79.6 37 66.1 0.048
Elevating the head of the bed to 30–
45 is important in prevention of VAP
155 89.6 18 90.0 0.955 98 84.5 65 97.0 10 100.0 0.015 124 90.5 49 87.5 0.533
Early exercise and mobilization may
increase the possibility of VAP 97 56.1 6 30.0 0.027 68 58.6 30 44.8 5 50.0 0.190 71 51.8 32 57.1 0.502
Regular oral care with chlorhexidine is necessary to prevent VAP
152 87.9 18 90.0 0.780 102 87.9 59 88.1 9 90.0 0.981 126 92.0 44 78.6 0.009
Proper sterilization and disinfection
of respiratory care equipment is
important to prevent VAP
151 87.3 18 90.0 0.727 104 89.7 55 82.1 10 100.0 0.155 120 87.6 49 87.5 0.986
Oral route is recommended for endotracheal intubation to prevent
VAP
113 65.3 12 60.0 0.637 75 64.7 46 68.7 4 40.0 0.209 88 64.2 37 66.1 0.808
Prophylactic probiotics may be useful to prevent VAP
128 74.0 11 55.0 0.073 84 72.4 48 71.6 7 70.0 0.983 100 73.0 39 69.6 0.638
Ultrathin polyurethane endotracheal
tube cuffs may lower VAP rates 59 34.1 12 60.0 0.023 37 31.9 34 50.7 0 0.0 0.02 59 43.1 12 21.4 0.005
4.7 Conti, Comparison of Nurses` Educational Degree, Years of ICU Experience and Previous VAP Education with Knowledge on prevention of
VAP (N=193).

22
Knowledge on prevention of VAP
(Statements)
Educational Degree
P value
Years of ICU Experience
P
value
Previous VAP Education
P
value
Bachelor Master <=5 6-10 >=11 Yes No
Correct answer Correct answer Correct answer
N % N % N % N % N % N % N %
Saline instillation before tracheal
suctioning may cause to VAP
107 61.8 13 65.0 0.783 74 63.8 41 61.2 5 50.0 0.675 88 64.2 32 57.1 0.357
Mechanical tooth brushing may be useful in prevention of VAP
105 60.7 10 50.0 0.356 65 56.0 42 62.7 8 80.0 0.272 87 63.3 28 50.0 0.083
Closed in-line endotracheal suctioning
reduce the risk of VAP
133 76.9 10 50.0 0.009 85 73.3 52 77.6 6 60.0 0.471 108 78.8 35 62.5 0.019
Kinetic beds reduce the risk of VAP
and recommended
111 64.2 15 75.0 0.335 78 67.2 47 70.1 1 10.0 0.001 92 67.2 34 60.7 0.394
Adequate hand hygiene between patients and change gloves is important
to prevent the VAP
151 87.3 19 95.0 0.313 99 85.3 62 92.5 9 90.0 .345 123 89.9 47 83.9 0.255
Prone positioning intermittently may
prevent VAP and recommended
78 45.1 6 30.0 0.198 45 38.8 36 53.7 3 30.0 0.098 66 48.2 18 32.1 0.041
Using selective oral or digestive
decontamination to reduce risk VAP
125 72.3 11 55.0 0.109 79 68.1 51 76.1 6 60.0 0.393 99 72.3 37 66.1 0.392
Care bundles may be useful in reducing
VAP
137 79.2 18 90 0.250 92 79.3 57 85.1 6 60.0 0.162 113 82.5 42 75.0 0.236
4.7 Conti, Comparison of Nurses` Educational Degree, Years of ICU Experience and Previous VAP Education with Knowledge on prevention of
VAP (N=193)

23
Comparison of nurses` educational degree, years of ICU experience and previous VAP education with knowledge on prevention of VAP is
shown in is table 4.7. There were statically insignificant differences in majority of the items (P>0.05). In the present study, results that reveled
two there were statistically significant differences only in a few items. Regarding the educational levels; nurses with bachelor degree education
had higher knowledge rates on prevention of VAP in terms of “Benzodiazepines should always be preferred to manage agitation” (45.7%),
“Pairing spontaneous breathing trials with spontaneous awakening trials is not necessary” (38.2%) and “Closed/in-line endotracheal suctioning
reduce the risk of VAP” (76.9%) items than the master degree group (P< 0.05). However in “Ultrathin polyurethane endotracheal tube cuffs
may lower VAP rates” item, master degree group had higher knowledge rates (60.0%) than the nurses with bachelor degree (34.1%) (P< 0.05).
It was determined that, there were statistically significant differences between nurses who had <=5 years and 6-10 years of ICU experience,
and the nurses who had >=11 years of ICU experience in a few items (P< 0.05). Nurses with <=5 and 6-10 years of experience had higher
correct knowledge rates than the >=11 group in terms of “If possible, intubation should be avoided to prevent VAP”, “Ultrathin polyurethane
endotracheal tube cuffs may lower VAP rates” and “Kinetic beds reduce the risk of VAP and recommended” items (P< 0.05). However in
“Elevating the head of the bed to 30–45 is important in prevention of VAP” item, >=11 group had higher knowledge rates (100 %) than the
other groups (P< 0.05). There were also statistically significant differences in terms of previous VAP education (P< 0.05). Nurses who had
previous VAP education had higher correct knowledge rates than the other group in terms of “Regular oral care with chlorhexidine is necessary
to prevent VAP” (92.0%), “Ultrathin polyurethane endotracheal tube cuffs may lower VAP rates” (43.1%), “Closed/in-line endotracheal
suctioning reduce the risk of VAP” (78.8%) and “Prone positioning intermittently may prevent VAP and recommended” (48.2%) items.

24
Nurses ` Barriers to Adherence to
VAP Prevention Guidelines
(Statements)
Educational Degree
P value
Years of ICU Experience
P
value
Previous VAP Education
P
value
Bachelor Master <=5 6-10 >=11 Yes No
Always Always Always
N % N % N % N % N % N % N %
Lack of VAP prevention knowledge 65 37.6 8 40.0 0.832 45 38.8 26 38.8 2 20.0 0.490 47 34.3 26 46.4 0.115
Lack of educational programs on VAP
such as in-service education or courses 65 37.6 9 45.0 0.518 41 35.0 30 44.8 3 30.0 0.385 55 40.1 19 33.9 0.420
Shortage of staff in the ICU 94 54.3 13 65.0 0.364 63 54.3 41 61.2 3 30.0 0.167 77 56.2 30 53.6 0.738
Lack of equipment such as gloves and
face masks 30 17.3 4 20.0 0.768 17 14.7 15 22.4 2 20.0 0.408 28 20.4 6 10.7 0.108
Lack of written VAP protocol in the hospital
39 22.5 5 25.0 .804 25 21.6 17 25.4 2 20.0 0.819 31 22.6 13 23.2 0.930
Forgetting to practice the sterile
technique 40 23.1 4 20.0 0.753 25 21.1 17 25.4 2 20.0 0.819 30 21.9 14 25.0 0.641
Lack of time to deliver proper infection
control 37 21.4 7 35.0 .169 25 21.6 17 25.4 2 20.0 0.819 32 23.4 12 21.4 0.772
Hospital system insufficiencies 49 28.3 5 25.0 0.754 26 22.4 24 35.8 4 40.0 0.103 39 28.5 15 26.8 0.813
Comparison of nurses` educational degree, years of ICU experience and previous VAP education with nurses’ barriers to adherence to VAP
prevention guidelines is shown in table 4.8. It was determined that there were no statically significant differences between items and descriptive
characteristics (P >0.05).
Table 4. 8 Comparison of Nurses` Educational Degree, Years of ICU Experience and Previous VAP Education with Nurses ` Barriers to Adherence to VAP
Prevention Guidelines (N=193)

25
5. DISCUSSION
The aim of this study was determination of critical care nurses’ knowledge on
prevention of ventilator associated pneumonia and barriers of adherence to preventive
measures.193 volunteer nurses with different age, educational level and experience
participated in this study.
Regarding to descriptive characteristics of the nurses on VAP education, it was
determined that, the majority of the nurses had received VAP education and more than one
third of them received the VAP education by courses. Participants rated the quality of the
VAP as excellent, very good, good, fair and poor and the most frequent answer was good.
However, majority of participants mentioned that they need education on VAP to improve
nursing skills and enhance patient's outcomes. This result is satisfying in terms of showing
their willingness to improve themselves. Training activities and evidence-based guidelines
and protocols in the ICUs improve the quality of nursing care and narrow the gap between
scientific knowledge and actual performance and form basis for nurses to make the right
decision. In the same line, in our survey more than two third of the participants reported
that there are guidelines and or protocols on prevention of VAP in hospital during their
work experience.
Examination of general knowledge of the nurses on VAP showed that, a majority of
the nurses had correct answers in majority of the items (5 of 6 items). The majority of the
nurses had correct answers for "Continuous education to ICU nurses on prevention of
nosocomial infection is associated with decreased rates of VAP" (T), "VAP is cause of
highest mortality rate among nosocomial infections" (T) and “The Ventilator Associated
Pneumonia (VAP) is pneumonia that occurs > or equal 48 hours after endotracheal
intubation” items. Percentages of the correct answers and wrong/I don’t know answers of
the nurses were close together in "Automated control of endotracheal tube cuff pressure is
important because it decrease the risk for VAP" (T) item. There are same line studies in the
relevant literature; VAP is described in the literature as an infection of the lung that occurs
48 hours after insertion of an endotracheal tube (Rodrigues et al, 2017). There is significant
increase in the rate of VAP resulted with mortality (Porhomayon et al, 2017). In Jordan, a
rate of 29 cases per 1,000 ventilator-days, and the rate of mortality related to VAP as 53%
was determined (Samrah et al, 2016).

26
Another study reported that continuous control of pressure cuff is associated with a
decrease of micro aspiration and VAP (Nseir et al, 2011). Zeinab Hassan et al
recommended continuous education programs about ventilator-associated pneumonia for
nurses in Jordan (Hassan et al, 2016).
In the current study, regarding to nurses` knowledge on prevention of VAP results
showed that, majority of the nurses had correct answers in majority of the items (19 of 24
items) and this is satisfying result. The highest correct answers were “Changing the
ventilator circuit regularly is necessary to prevent VAP”, “Early exercise and mobilization
may increase the possibility of VAP”, “Adequate hand hygiene between patients and
change gloves is important to prevent the VAP”, "Proper sterilization and disinfection of
respiratory care equipment is important to prevent VAP" (T), "Sedation should be
interrupted daily to prevent VAP" (T) and “Care bundles may be useful in reducing VAP”
items. There are studies in the relevant literature supporting our results. A descriptive,
cross-sectional study conducted with 205 ICU nurses to investigate knowledge, attitudes
and practices of nurses about oral care of intubated patients found that, higher scores on
oral care knowledge were associated with performing oral care (Lin et al. 2011). Improved
oral care is necessary and contributes to reduce the incidence of VAP. An observational
study by Llaurado-Serra et al (2014) concluded that, patients connected with endotracheal
tube and without head-of-bed elevation had increased incidence of complications. The
Spanish ‘‘Zero-VAP’’ bundle emphasize that the use of gloves does not preclude the
obligation of hand-washing before and after management of the artificial airway (Lerma et
al. 2013). National Infection Control Guidelines (2016, Singapore) emphasize that patients
undergo mechanically ventilated for >48 hours, a daily sedation vacation and assessment
for readiness-to-extubate is undertaken, early extubation decreases the time spent on
mechanical ventilation and directly reduces the risk of VAP. A study conducted by
Mogyoródi et al (2016) showed a reduction in the incidence and risk of VAP after the
implementation of the bundle that similar to our results. In the present study, most frequent
wrong /I don’t know answers were in “It is necessary to assess readiness to extubate of the
patient daily to prevent VAP”, “Ultrathin polyurethane endotracheal tube cuffs may lower
VAP rates” and “It is necessary to manage patients without sedation whenever possible to
prevent VAP”. However, CDC recommends assessing readiness to extubate once a day
(spontaneous breathing trials) in patients without contraindications (CDC, 2014).

27
Using the endotracheal tube with polyurethane material results in reducing ventilator-
associated pneumonia compared to ETT with Polyvinyl Chloride (PVC) cuff
(Mahmoodpoor et al 2013). Regarding the barriers of the nurses on adherence to VAP
prevention guidelines, present study showed that majority of the nurses had "sometimes"
answers for the barriers to adherence to VAP prevention guideline.
Highest “sometimes” answers were “Lack of educational programs on VAP such as
in-service education or courses”, “Lack of time to deliver proper infection control”,
“Forgetting to practice the sterile technique” and “Lack of VAP prevention knowledge”
respectively. Most frequent "always" answer was "Shortage of staff in the ICU". These
results show similarity results of the study of Jordan et al (2014). The authors notice lack
of time, probably because of the small number of staff at the ICU, the main barrier.
Enough number of nurses in ICUs and professional teamwork reflect nursing
performance. Jansson et al (2013) emphasized that, educational programs and guidelines
as well as ventilator bundles and instruments should be developed and updated to improve
practice and reduce barriers.
Low frequencies in majority of the "never" answers were determined and this result
is unsatisfying. Most frequent "never" answer was "Lack of equipment such as gloves
and face masks” This result shows similarty with the results of the study conducted in
Saudi Arabia. They determined that "Not wearing personal protective equipment" was
not considered as a barrier by majority of the nurses (62.4%) (Yaseen et al 2015).
In comparison of nurse's educational degree, years of nursing experience and
previous VAP education with general knowledge and VAP prevention, results showed
statistically significant differences only in a few items (P< 0.05). There wasn’t
statistically significant differences between descriptive characteristics and items on
barriers to adherence to VAP prevention guidelines statements (P>0.05). Results of the
current study showed statistically significant differences in terms of educational levels
and experiences of the nurses. Nurses who had previous VAP education had higher
correct knowledge rates than the other group in terms of “VAP is the most prevalent
infection in intensive care units”, “Automated control of endotracheal tube cuff pressure
is important because it decreases the risk for VAP” and “Continuous education to ICU
nurses on prevention of nosocomial infection is associated with decreased rates of VAP”
items (P< 0.05).

28
Same line study conducted in Jordan nurses showed significant improvements in
mean knowledge scores on ventilator-associated pneumonia and preventive measures after
an educational program (p<0.05) (Hassan et al, 2016). Samra et al. (2017) recommend
education and periodic training remain a fundamental process of improving health services.
In comparison of knowledge on prevention of VAP with nurses’
educational degree that shown bachelor degree nurses’ correct knowledge rates
were higher than nurses graduated from master degree in items
“Benzodiazepines should always be preferred to manage agitation”, “Pairing
spontaneous breathing trials with spontaneous awakening trials is not
necessary”, “Ultrathin polyurethane endotracheal tube cuffs may lower VAP
rates” and “Closed/in-line endotracheal suctioning reduce the risk of VAP” (P<
0.05). This was an unexpected result. In contrast to other study was conducted to
objective of evaluation of knowledge, attitude, and adherence of healthcare
workers to evidence-based guidelines for prevention of VAP and exploration of
the barriers of their implementation in clinical practice that report significantly
different between nurse assistants (RAs), nurses (RNs), and shown register
nurses higher than assistant nurses with (P=0.001) Mardani et al (2016).
Regarding to experiences of the nurses, results showed that, nurses with <=5 and
6-10 years of experience had higher correct knowledge rates than the >=11
group in terms of “Automated control of endotracheal tube cuff pressure is
important because it decreases the risk for VAP” items of general knowledge;
“If possible, intubation should be avoided to prevent VAP”, “Ultrathin
polyurethane endotracheal tube cuffs may lower VAP rates” and “Kinetic beds
reduce the risk of VAP and recommended” items of prevention knowledge (P<
0.05). Nurses with less experience showed higher knowledge rates than the
nurses who had more experienced. This result may be resulted from being newly
graduated and to remember the knowledge easily. Conversely, Yaseen et al
showed that more experienced nurses performed significantly better rates of
VAP prevention knowledge than their less experienced colleagues (p<0.05)
(Yaseen et al 2015).

29
6. CONCLUSION
Results of the present study showed that, the majority of the nurses had received VAP
education and perceived the quality of the education as “good”; however they have stated
that they need education on VAP to improve nursing skills and enhance patient's outcomes.
This result may be resulted from weakness of quality of the VAP education and is important
in terms of showing the willingness of the nurses for education and development.
Results of the present study showed high level of knowledge on general VAP
knowledge and VAP prevention and this is a satisfying result. Regarding to barriers of
nurses to adherence to VAP prevention guidelines, there were high rates of “sometimes”
and “always” and low rates of the “never” answers. Frequent rated barriers were “Lack of
educational programs on VAP such as in-service education or courses”, “Lack of time to
deliver proper infection control”, “Forgetting to practice the sterile technique” and “Lack
of VAP prevention knowledge” and "Shortage of staff in the ICU". This condition may
inhibit for stuff improvement and development; also may prevent from motivations and
increase incidences of VAP complications. Both national and institutional regulations are
necessary to prevent barriers of VAP prevention.
Results of the current study showed statistically significant differences in terms of
previous VAP education, educational levels and experiences of the nurses. Education
remains as a vital process of improving health services. Professional training programs can
affect for well outcome and reflect for inpatients services. It is necessary to give the chance
of education to the nurses with higher opportunity to achieve and exposure to professional
new in-service education related VAP (Akın et al, 2014). Recommend implementing
multifaceted educational programmers comprising information on recent VAP prevention
guidelines in the general intensive care unit and promoting nurses’ participation to
maximize awareness of infection control.

31
7. FINDINGS AND RECOMMENDATIONS
7.1. Findings
Main findings of the study that was performed with the aim of determination
of the knowledge on prevention of ventilator associated pneumonia and
barriers of adherence to preventive measures of the critical care nurses were
listed as followings:
A total of the nurses of participants in this study 193, the mean of ages of the
participants were 28.4 and the 26-30 group of age was the most frequent (56.5%).
Females were the majority of the participants (60.1%). Most of the participants have
bachelor's degree (89.7%). Majority of the nurses have experience less than five years
as a registered nurses (60.1%). (Table 4.1)
Regarding to general knowledge of the nurses on VAP it was found that; majority of
the nurses had correct answers in majority of the items (5 of 6 items). The most
frequently known items were "Continuous education to ICU nurses on prevention of
nosocomial infection is associated with decreased rates of VAP" (T) (88.6%), "VAP
is cause of highest mortality rate among nosocomial infections" (T) (86.5%) and “The
Ventilator Associated Pneumonia (VAP) is pneumonia that occurs > or equal 48 hours
after endotracheal intubation” (81.3%) respectively. (Table 4.3)
About nurses` knowledge on prevention of VAP; the highest correct answers were in
“Elevating the head of the bed to 30–45 degree is important in prevention of VAP”
(89.6%), “Regular oral care with chlorhexidine is necessary to prevent VAP” (88.1%),
“Adequate hand hygiene between patients and change gloves is important to prevent
the VAP” (88.1%), "Proper sterilization and disinfection of respiratory care equipment
is important to prevent VAP " (T) (87.6%), " It is necessary to assess readiness to
extubate of the patient daily to prevent VAP " (T) (85.0%) and “Care bundles may be
useful in reducing VAP” (80.3%) items respectively. (Table 4.4)
It was determined that, majority of nurse had "sometimes" answer for the barriers
nurses to adherence to VAP prevention guideline. Most frequent "always" answer was
"Shortage of staff in the ICU" (55.4%). Highest “sometimes” answers were “Lack of
educational programs on VAP such as in-service education or courses”, “Lack of time
to deliver proper infection control” (55.4%),“Forgetting to practice the sterile

31
technique” (54.4%) and “Lack of VAP prevention knowledge” (53.9%) respectively.
(Table 4.5)
There were statistically significant differences between correct answers of some items
on general knowledge on VAP and years of ICU experience and previous VAP
education. (Table 4.6)
Regarding the educational levels; there were statically insignificant differences in
majority of the items (P>0.05). In the present study, results that reveled two there
were statistically significant differences only in a few items. (Table 4.7)
Comparison of nurses` educational degree, years of ICU experience and previous VAP
education with nurses’ barriers to adherence to VAP prevention guidelines is shown
in table 4.8. It was determined that there were no statically significant differences
between items and descriptive characteristics (P >0.05).
7.2 Recommendations
Based on the result of this study following recommendations were made:
Continues education programs are necessary to improve nurses’ knowledge
on VAP prevention.
Following and implementation the new guidelines and protocols on VAP
prevention.
National and institutional regulations are necessary to prevent barriers of
VAP prevention.
Further experimental studies related to educational interventions for nurses
may be useful for evidence-based practices.

32
8. REFERENCES
Abbott, C. A., Dremsa, T., Stewart, D. W., Mark, D. D., & Swift, C. C. (2006). Adoption
of a Ventilator‐Associated Pneumonia Clinical Practice Guideline. Worldviews on
Evidence‐Based Nursing, 3(4), 139-152.
Akın Korhan, E., Hakverdioğlu Yönt, G., Parlar Kılıç, S., & Uzelli, D. (2014). Knowledge
levels of intensive care nurses on prevention of ventilator‐associated pneumonia. Nursing
in critical care, 19(1), 26-33.
Albertos, R., Caralt, B., & Rello, J. (2011). Ventilator-associated pneumonia.
Management in critical illness. Current opinion in gastroenterology, 27(2), 160-166.
Alexiou, V. G., Ierodiakonou, V., Dimopoulos, G., & Falagas, M. E. (2009). Impact of
patient position on the incidence of ventilator-associated pneumonia: a meta-analysis of
randomized controlled trials. Journal of critical care, 24(4), 515-522.
Alhazzani, W., Alenezi, F., Jaeschke, R. Z., Moayyedi, P., & Cook, D. J. (2013). Proton
pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in
critically ill patients: a systematic review and meta-analysis. Critical care medicine, 41(3),
693-705.
Al-Hussami, M., & Darawad, M. (2013). Compliance of nursing students with infection
prevention precautions: effectiveness of a teaching program. American journal of
infection control, 41(4), 332-336.
Allegranzi, B. (2010). The global burden of health care-associated infection. WHO
Inaugural infection control webinar series. 19 January 2010.
Aloush, S. M. (2017). Nursing students' knowledge about ventilator-associated pneumonia
prevention guidelines: Effectiveness of a teaching program. American journal of infection
control, 45(5), 544-546.
AL‐Rawajfah, O. M. (2016). Infection control practices among intensive care unit
registered nurses: a Jordanian national study. Nursing in critical care, 21. (2)

33
Andrews, T., & Steen, C. (2013). A review of oral preventative strategies to reduce
ventilator‐associated pneumonia. Nursing in critical care, 18(3), 116-122.
Balas, M. C., Vasilevskis, E. E., Olsen, K. M., Schmid, K. K., Shostrom, V., Cohen, M.
Z.& Stothert, J. C. (2014). Effectiveness and safety of the awakening and breathing
coordination, delirium monitoring/management, and early exercise/mobility (ABCDE)
bundle. Critical care medicine, 42(5), 1024.
Balkhy, H. H., El-Saed, A., Maghraby, R., Al-Dorzi, H. M., Khan, R., Rishu, A. H., &
Arabi, Y. M. (2014). Drug-resistant ventilator associated pneumonia in a tertiary care
hospital in Saudi Arabia. Annals of thoracic medicine, 9(2), 104.
Barraud, D., Bollaert, P. E., & Gibot, S. (2013). Impact of the administration of probiotics
on mortality in critically ill adult patients: a meta-analysis of randomized controlled trials.
CHEST Journal, 143(3), 646-655.
Bloos, F., Müller, S., Harz, A., Gugel, M., Geil, D., Egerland, K. & Marx, G. (2009).
Effects of staff training on the care of mechanically ventilated patients: a prospective
cohort study. British journal of anaesthesia, 103(2), 232-237.
Brusaferro, S., Arnoldo, L., Cattani, G., Fabbro, E., Cookson, B., Gallagher, R. &
Privitera, G. (2015). Harmonizing and supporting infection control training in Europe.
Journal of Hospital Infection, 89(4), 351-356.
Burns, K. E., Meade, M. O., Premji, A., & Adhikari, N. K. (2013). Noninvasive positive‐
pressure ventilation as a weaning strategy for intubated adults with respiratory failure. The
Cochrane Library.
Cambridge, MA. (2012).How-to Guide: Prevent Ventilator-Associated Pneumonia:
Institute for Healthcare Improvement
Caruso, P., Denari, S., Ruiz, S. A., Demarzo, S. E., & Deheinzelin, D. (2009). Saline
instillation before tracheal suctioning decreases the incidence of ventilator-associated
pneumonia. Critical care medicine, 37(1), 32-38.
Casado, R. J., de Mello, M. J. G., de Aragão, R. C., Maria de Fátima, P. M., & Correia, J.
B. (2011). Incidence and risk factors for health care-associated pneumonia in a pediatric
intensive care unit. Critical care medicine, 39(8), 1968-1973.

34
CDC, health associated Infections (HAI), Ventilator-associated Pneumonia (VAP),
Update guideline (2012), available online: https://www.cdc.gov/hai/vap/vap.html.
Centers for Disease Control and Prevention. Healthcare-associated Infections (HAIs).
CDC; 2015; Available from: http://www.cdc.gov/HAI/surveillance. (Accessed May 8,
2017.)
Cusumano-Towner, M., Li, D. Y., Tuo, S., Krishnan, G., & Maslove, D. M. (2013). A
social network of hospital acquired infection built from electronic medical record data.
Journal of the American Medical Informatics Association, 20(3), 427-434.
D'Amico, R., Pifferi, S., Torri, V., Brazzi, L., Parmelli, E., & Liberati, A. (2009).
Antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults
receiving intensive care. The Cochrane Library.
El Azab, S. R., El Sayed, A. E., Abdelkarim, M., Al Mutairi, K. B., Al Saqabi, A., & El
Demerdash, S. (2013). Combination of ventilator care bundle and regular oral care with
chlorhexidine was associated with reduction in ventilator associated pneumonia. Egyptian
Journal of Anaesthesia, 29(3), 273-277.
El-Khatib, M. F., Zeineldine, S., Ayoub, C., Husari, A., & Bou-Khalil, P. K. (2010).
Critical care clinicians’ knowledge of evidence-based guidelines for preventing ventilator-
associated pneumonia. American Journal of Critical Care, 19(3), 272-276.
Fathy, A., Abdelhafeez, R., Abdel-Hady, E. G., & Elhafez, S. A. A. (2013). Analysis of
ventilator associated pneumonia (VAP) studies in Egyptian University Hospitals.
Egyptian Journal of Chest Diseases and Tuberculosis, 62(1), 17-25.
Frimpong, K., Stollings, J. L., Carlo, M. E., & Ely, E. W. (2014). ICU delirium viewed
through the lens of the PAD guidelines and the ABCDEF implementation bundle.
Garcia, R., Jendresky, L., Colbert, L., Bailey, A., Zaman, M., & Majumder, M. (2009).
Reducing ventilator-associated pneumonia through advanced oral-dental care: a 48-month
study. American Journal of Critical Care, 18(6), 523-532.
Ha, H. J., Park, J. H., & Kim, M. H. (2016). Knowledge and performance level of infection
control guidelines on indwelling urinary catheter, central venous catheter and ventilator

35
among intensive care nurses. Journal of the Korea Academia-Industrial cooperation
Society, 17(6), 113-120.
Hassan, Z. M., & Wahsheh, M. A. (2017). Knowledge level of nurses in Jordan on
ventilator‐associated pneumonia and preventive measures. Nursing in critical care, 22(3),
125-132.
He, S., Chen, B., Li, W., Yan, J., Chen, L., Wang, X., & Xiao, Y. (2014). Ventilator-
associated pneumonia after cardiac surgery: a meta-analysis and systematic review. The
Journal of thoracic and cardiovascular surgery, 148(6), 3148-3155.
Jahansefat, L., Vardanjani, M. M., Bigdelian, H., Massoumi, G., Khalili, A., & Mardani,
D. (2016). Exploration of knowledge of, adherence to, attitude and barriers toward
evidence-based guidelines (EBGs) for prevention of ventilator-associated pneumonia
(VAP) in healthcare workers of pediatric cardiac intensive care units (PCICUs): A Quali-
Quantitative survey. International Journal of Medical Research & Health Sciences, 5(9),
67-73.
Jansson, M., Ala-Kokko, T., Ylipalosaari, P., Syrjälä, H., & Kyngäs, H. (2013). Critical
care nurses’ knowledge of, adherence to and barriers towards evidence-based guidelines
for the prevention of ventilator-associated pneumonia–A survey study. Intensive and
Critical Care Nursing, 29(4), 216-227.
Jordan, A., Badovinac, A., Špalj, S., Par, M., Šlaj, M., & Plančak, D. (2014). Factors
influencing intensive care nurses' knowledge and attitudes regarding ventilator-associated
pneumonia and oral care practice in intubated patients in Croatia. American journal of
infection control, 42(10), 1115-1117.
Kandeel, N., & Tantawy, N. (2012). Current nursing practice for prevention of ventilator
associated pneumonia in ICUs. Life Science Journal, 9(3), 966-73.
Keeley, L. (2007). Reducing the risk of ventilator‐acquired pneumonia through head of
bed elevation. Nursing in critical care, 12(6), 287-294.
Khan, R. M., Aljuaid, M., Aqeel, H., Aboudeif, M. M., Elatwey, S., Shehab, R. &
Qushmaq, I. (2017). Introducing the comprehensive unit-based safety program for

36
mechanically ventilated patients in Saudi Arabian intensive care units. Annals of thoracic
medicine, 12(1), 11.
Klompas, M., Branson, R., Eichenwald, E. C., Greene, L. R., Howell, M. D., Lee, G. ... &
Yokoe, D. S. (2014). Strategies to prevent ventilator-associated pneumonia in acute care
hospitals: 2014 update. Infection Control & Hospital Epidemiology, 35(S2), S133-S154.
Kollef, M. H., Chastre, J., Fagon, J. Y., François, B., Niederman, M. S., Rello, J. ... &
Rehm, C. (2014). Global prospective epidemiologic and surveillance study of ventilator-
associated pneumonia due to Pseudomonas aeruginosa. Critical care medicine, 42(10),
2178-2187.
Labeau, S., Vandijck, D. M., Claes, B., Van Aken, P., Blot, S. I., & Executive Board of
the Flemish Society for Critical Care Nurses. (2007). Critical care nurses’ knowledge of
evidence-based guidelines for preventing ventilator-associated pneumonia: an evaluation
questionnaire. American Journal of Critical Care, 16(4), 371-377.
Lerma, F. Á., García, M. S., Lorente, L., Gordo, F., Añón, J. M., Álvarez, J., ... & Jam, R.
(2014). Guidelines for the prevention of ventilator-associated pneumonia and their
implementation. The Spanish “Zero-VAP” bundle. Medicina Intensiva, 38(4), 226-236.
Lim, K. P., Kuo, S. W., Ko, W. J., Sheng, W. H., Chang, Y. Y., Hong, M. C., ... & Chang,
S. C. (2015). Efficacy of ventilator-associated pneumonia care bundle for prevention of
ventilator-associated pneumonia in the surgical intensive care units of a medical center.
Journal of Microbiology, Immunology and Infection, 48(3), 316-321.
Lin, Y. S., Chang, J. C., Chang, T. H., & Lou, M. F. (2011). Critical care nurses’
knowledge, attitudes and practices of oral care for patients with oral endotracheal
intubation: a questionnaire survey. Journal of clinical nursing, 20(21‐22), 3204-3214.
Llauradó, M., Labeau, S., Vandijck, D., Rello, J., Rosa, A., Riera, A. ... & Benítez, M. L.
(2011). Southern European intensive care nurses’ knowledge of evidence-based guidelines
for preventing ventilator-associated pneumonia. Medicina Intensiva (English Edition),
35(1), 6-12.
Llaurado-Serra, Ulldemolins M, M., Güell-Baró, R., Coloma-Gómez, B., Alabart-
Lorenzo, X., López-Gil, A. & CAPCRI Study Investigators. (2015). Evaluation of head-

37
of-bed elevation compliance in critically ill patients under mechanical ventilation in a
polyvalent intensive care unit. Medicina Intensiva, 39(6), 329-336.
Lord, R. K., Mayhew, C. R., Korupolu, R., Mantheiy, E. C., Friedman, M. A., Palmer, J.
B., & Needham, D. M. (2013). ICU early physical rehabilitation programs: financial
modeling of cost savings. Critical care medicine, 41(3), 717-724.
Lorente, L., Lecuona, M., Galván, R., Ramos, M. J., Mora, M. L., & Sierra, A. (2004).
Periodically changing ventilator circuits is not necessary to prevent ventilator-associated
pneumonia when a heat and moisture exchanger is used. Infection Control & Hospital
Epidemiology, 25(12), 1077-1082.
Mahmoodpoor, A., Peyrovi-far, A., Hamishehkar, H., Bakhtyiari, Z., Mirinezhad, M. M.,
Hamidi, M., & Golzari, S. E. J. (2013). Comparison of prophylactic effects of
polyurethane cylindrical or tapered cuff and polyvinyl chloride cuff endotracheal tubes on
ventilator-associated pneumonia. Acta Medica Iranica, 51(7), 461.
Mietto, C., Pinciroli, R., Patel, N., & Berra, L. (2013). Ventilator Associated Pneumonia:
Evolving Definitions and Preventive StrategiesDiscussion. Respiratory care, 58(6), 990-
1007.
Mogyoródi, B., Dunai, E., Gál, J., & Iványi, Z. (2016). Ventilator-associated pneumonia
and the importance of education of ICU nurses on prevention–Preliminary results.
Interventional Medicine and Applied Science, 8(4), 147-151.
Morris, A. C., Hay, A. W., Swann, D. G., Everingham, K., McCulloch, C., McNulty, J.,
... & Walsh, T. S. (2011). Reducing ventilator-associated pneumonia in intensive care:
impact of implementing a care bundle. Critical care medicine, 39(10), 2218-2224.
Munro, N., & Ruggiero, M. (2014). Ventilator-associated pneumonia bundle:
reconstruction for best care. AACN Advanced Critical Care, 25(2), 163-175.
Muscedere, J., Rewa, O., Mckechnie, K., Jiang, X., Laporta, D., & Heyland, D. K. (2011).
Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: a
systematic review and meta-analysis. Critical care medicine, 39(8), 1985-1991.

38
National Infection Control Guidelines. (2016). Draft for Consultation.
https://www.moh.gov.sg/content/moh_web/home/Publications/guidelines/infection_cont
rol_guidelines/national-infection-control-guidelines--2016-draft-for-consultati.html.
Needham, D. M., Korupolu, R., Zanni, J. M., Pradhan, P., Colantuoni, E., Palmer, J. B. &
Fan, E. (2010). Early physical medicine and rehabilitation for patients with acute
respiratory failure: a quality improvement project. Archives of physical medicine and
rehabilitation, 91(4), 536-542.
Nseir, S., Zerimech, F., Fournier, C., Lubret, R., Ramon, P., Durocher, A., & Balduyck,
M. (2011). Continuous control of tracheal cuff pressure and microaspiration of gastric
contents in critically ill patients. American journal of respiratory and critical care
medicine, 184(9), 1041-1047.
Obiero, C. W., Seale, A. C., & Berkley, J. A. (2015). Empiric treatment of neonatal sepsis
in developing countries. The Pediatric infectious disease journal, 34(6), 659-661.
Osman, M. A. A. R., & Aggour, R. L. (2014). Oral care practices in Egypt intensive care
units–a national survey. J Periodent Med Clin Pract, 1(2), 172-182.
Poelaert, J., Haentjens, P., & Blot, S. (2014). Association among duration of mechanical
ventilation, cuff material of endotracheal tube, and postoperative nosocomial pneumonia
in cardiac surgical patients: a prospective study. The Journal of thoracic and
cardiovascular surgery, 148(4), 1622-1627.
Porhomayon, J., & Pourafkari, L. (2017). Ventilator-associated pneumonia and the role of
tapered endotracheal tube with subglottic suctioning. Journal of critical care, 39, 291.
Resar, R., Griffin, F. A., Haraden, C., & Nolan, T. W. (2012). Using care bundles to
improve health care quality. IHI Innovation Series white paper. Cambridge,
Massachusetts: Institute for Healthcare Improvement.
Rodrigues, M. E., Lopes, S. P., Pereira, C. R., Azevedo, N. F., Lourenço, A., Henriques,
M., & Pereira, M. O. (2017). Polymicrobial ventilator-associated pneumonia: fighting in
vitro Candida albicans-Pseudomonas aeruginosa biofilms with antifungal-antibacterial
combination therapy. PloS one, 12(1), e0170433.

39
S. Krishna Prakash. (2014). Nosocomial infection-an overview [Online] Available
from:http://www.researchgate.net/publication/18951524_Nosocomial_infections_an_ov
erview.
Samra, S. R., Sherif, D. M., & Elokda, S. A. (2017). Impact of VAP bundle adherence
among ventilated critically ill patients and its effectiveness in adult ICU. Egyptian Journal
of Chest Diseases and Tuberculosis, 66(1), 81-86 .
Samrah, S., Bashtawi, Y., Hayajneh, W., Almomani, B., Momany, S., & Khader, Y.
(2016). Impact of colistin-initiation delay on mortality of ventilator-associated pneumonia
caused by A. baumannii. The Journal of Infection in Developing Countries, 10(10), 1129-
1134.
Schallom, M., Dykeman, B., Metheny, N., Kirby, J., & Pierce, J. (2015). Head-of-bed
elevation and early outcomes of gastric reflux, aspiration and pressure ulcers: a feasibility
study. American Journal of Critical Care, 24(1), 57-66.
Sedwick, M. B., Lance-Smith, M., Reeder, S. J., & Nardi, J. (2012). Using evidence-based
practice to prevent ventilator-associated pneumonia. Critical Care Nurse, 32(4), 41-51.
Shitrit, P., Meirson, M., Mendelson, G., & Chowers, M. (2015). Intervention to Reduce
Ventilator‐Associated Pneumonia in Individuals on Long‐Term Ventilation by
Introducing a Customized Bundle. Journal of the American Geriatrics Society, 63(10),
2089-2093.
Siempos, I. I., Ntaidou, T. K., & Falagas, M. E. (2010). Impact of the administration of
probiotics on the incidence of ventilator-associated pneumonia: a meta-analysis of
randomized controlled trials. Critical care medicine, 38(3), 954-962.
Sole, M. L., Su, X., Talbert, S., Penoyer, D. A., Kalita, S., Jimenez, E., ... & Bennett, M.
(2011). Evaluation of an intervention to maintain endotracheal tube cuff pressure within
therapeutic range. American Journal of Critical Care, 20(2), 109-118.
Spalding, M. C., Cripps, M. W., & Minshall, C. T. (2017). Ventilator-Associated
Pneumonia. Critical Care Clinics, 33(2), 277-292.

41
Valencia, M., Ferrer, M., Farre, R., Navajas, D., Badia, J. R., Nicolas, J. M., & Torres, A.
(2007). Automatic control of tracheal tube cuff pressure in ventilated patients in
semirecumbent position: a randomized trial. Critical care medicine, 35(6), 1543-1549.
Van Oort, P. M., Nijsen, T., Weda, H., Knobel, H., Dark, P., Felton, T. ... & Sterk, P. J.
(2017). BreathDx–molecular analysis of exhaled breath as a diagnostic test for ventilator–
associated pneumonia: protocol for a European multicentre observational study. BMC
pulmonary medicine, 17(1), 1.
W Williams, D., AO Lewis, M., J Marino, P., & P Wise, M. (2012). The oral cavity,
biofilms and ventilator-associated pneumonia. Current Respiratory Medicine Reviews,
8(3), 163-169.
Yang, L., Ye, L., Zheng, Z., & Zhang, M. (2014). Evaluation of the effectiveness and
safety of the awakening and breathing coordination, delirium monitoring/management,
and early exercise/mobility bundle: several confounders to be considered. Critical care
medicine, 42(10), e680-e681.
Yao, L. Y., Chang, C. K., Maa, S. H., Wang, C., & Chen, C. C. H. (2011). Brushing teeth
with purified water to reduce ventilator-associated pneumonia. Journal of Nursing
Research, 19(4), 289-297.
Yaseen, R. W., & Salameh, T. N. (2015). Saudi Critical Care Nurses' Knowledge Of and
Barriers toward Adherence to Prevention of Ventilator Associated Pneumonia Guidelines.
Journal of Nursing and Health Science, 4(2), 65-9.
Yeganeh, M., Yekta, H., Farmanbar, R., & Khalili, M. (2016). Knowledge of evidence‐
based guidelines in Ventilator‐Associated Pneumonia prevention. Journal of evidence-
based medicine.
Zolfaghari, P. S., & Wyncoll, D. L. (2011). The tracheal tube: gateway to ventilator-
associated pneumonia. Critical Care, 15(5), 310.

41
APPENDIX 1 Critical Care Nurses’ Knowledge on Prevention of Ventilator
Associated Pneumonia (VAP) and Barriers of Adherence to Preventive
Measures.
1. Characteristics of Nurse Participants
Subject Number:
1.Age
2.Gender □ Male □ Female
3.Education □ High school
□ Master degree
□ Bachelor’s
□ PhD
4.Working experience
in the ICU (As
years)
5.Number of beds in
ICU
6.Previous VAP
education
□ Yes □ No
7. (If you answered
the item 6 as “yes”)
Educational
resource
□ School
□ Courses
□ Web resources
□ In-service education
□ Congress/conferences
□ Other
8. (If you answered
the item 6 as “yes”)
Perceived quality
of the VAP
education
□ Excellent □ Very good
□ Good □ Fair
□ Poor
9.Need for education
on VAP
□ Yes □ No
10.Is there any
protocol in
hospital for
prevention of
VAP
□ Yes □ No

42
3. Nurses 'Barriers to Adherence to VAP Prevention Guidelines
Statements about barriers Always Sometimes Never
1.Lack of VAP prevention knowledge
2.Lack of educational programs on VAP
such as in-service education or courses
3. Shortage of staff in the ICU
4. Lack of equipment such as gloves and
face masks
5.Lack of written VAP protocol in the
hospital
6. Forgetting to practice the sterile
technique
7. Lack of time to deliver proper infection
control
8. Hospital system insufficiencies

43
2. Nurses’ Knowledge on VAP Prevention
I Don't know False True Statements about VAP prevention No
The Ventilator Associated Pneumonia (VAP) is
pneumonia that occurs > or equal 48 hours after
endotracheal intubation(T)
1
VAP is cause of highest mortality rate among nosocomial
infections (T)
2
VAP is the most prevalent infection in intensive care
units (T)
3
If possible, intubation should be avoided to prevent VAP
(T)
4
Whenever feasible, noninvasive positive pressure
ventilation should be used to prevent VAP (T)
5
It is necessary to manage patients without sedation
whenever possible to prevent VAP(T)
6
Benzodiazepines should always be preferred to manage
agitation (F)
7
Sedation should be interrupted daily to prevent VAP(T)
8
It is necessary to assess readiness to extubate of the
patient daily to prevent VAP (T)
9
Pairing spontaneous breathing trials with spontaneous
awakening trials is not necessary (F)
10
Minimizing pooling of secretions above the endotracheal
tube cuff is necessary to prevent VAP(T)
11
Changing the ventilator circuit regularly is necessary to
prevent VAP (F)
12
Elevating the head of the bed to 30–45 is important in
prevention of VAP(T)
13
Early exercise and mobilization may increase the
possibility of VAP(F)
14
Regular oral care with chlorhexidine is necessary to
prevent VAP(T)
15
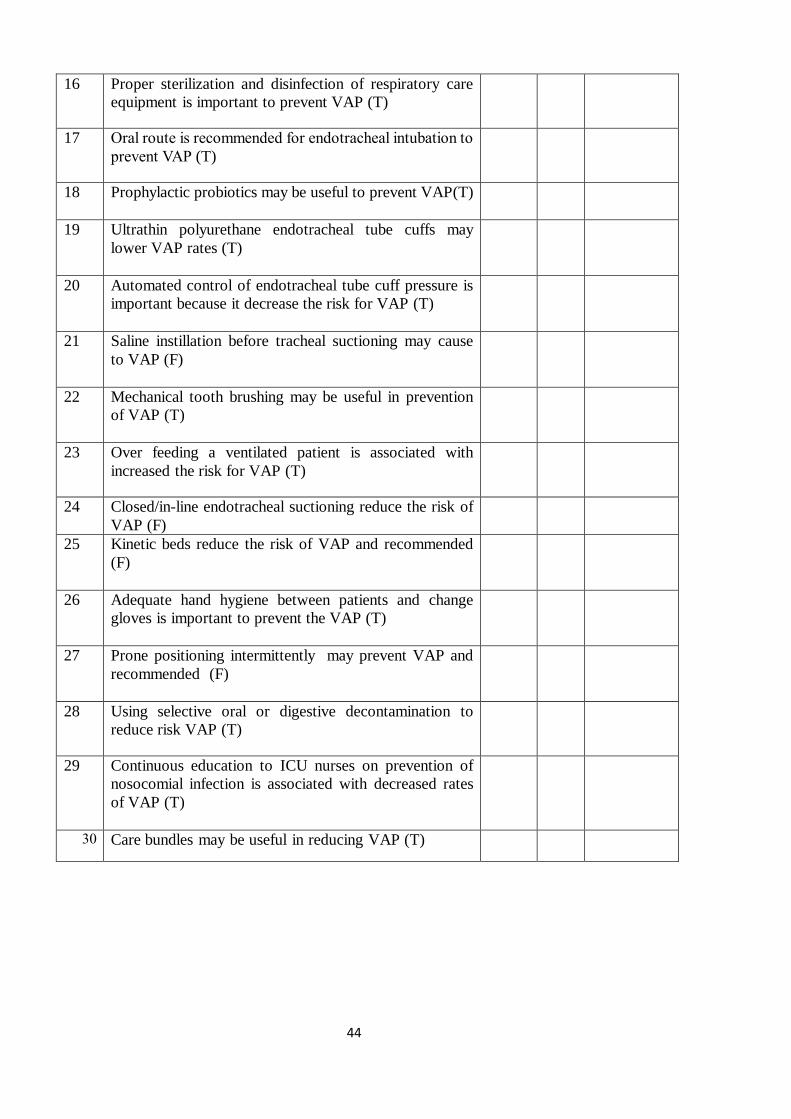
44
Proper sterilization and disinfection of respiratory care
equipment is important to prevent VAP (T)
16
Oral route is recommended for endotracheal intubation to
prevent VAP (T)
17
Prophylactic probiotics may be useful to prevent VAP(T)
18
Ultrathin polyurethane endotracheal tube cuffs may
lower VAP rates (T)
19
Automated control of endotracheal tube cuff pressure is
important because it decrease the risk for VAP (T)
20
Saline instillation before tracheal suctioning may cause
to VAP (F)
21
Mechanical tooth brushing may be useful in prevention
of VAP (T)
22
Over feeding a ventilated patient is associated with
increased the risk for VAP (T)
23
Closed/in-line endotracheal suctioning reduce the risk of
VAP (F)
24
Kinetic beds reduce the risk of VAP and recommended
(F)
25
Adequate hand hygiene between patients and change
gloves is important to prevent the VAP (T)
26
Prone positioning intermittently may prevent VAP and
recommended (F)
27
Using selective oral or digestive decontamination to
reduce risk VAP (T)
28
Continuous education to ICU nurses on prevention of
nosocomial infection is associated with decreased rates
of VAP (T)
29
Care bundles may be useful in reducing VAP (T) 03

45
APPENDIX 2 King Abdullah University Hospital Ethical Approval form

46
APPENDIX 3 Islamic Hospital Ethical Approval Form

47
APPENDIX 4 Ethical Approval Near East institutional Reviews Board

48
APPENDIX 5 INFORMED CONSENT FORM FOR ADULTS
You are invited to participate in a research study conducted by Prof. Dr. Nurhan Bayraktar
and Moath Alkhazali, from the Near East University Faculty of Health Sciences, Nursing
Department. This study was planned to determinate the knowledge and prevention and barriers
prophylaxis among nurses. You were selected as a possible participant in this study, because
findings of the study may be useful in improving nurses’ awareness and preventing this important
public health problem. If you decide to participate, a questionnaire will be used as data collection
tool in this study. The questionnaire contains questions regarding for demographics, knowledge and
barriers of nurses on VAP prevention with 3 choices (true,false,i dont know). However, I cannot
guarantee that you personally will receive any benefits from this research. Any information that is
obtained in connection with this study and that can be identified with you will remain confidential
and will be disclosed only with your permission or as required by law. Subject identities will be
kept confidential by don’t using the name, and using participant coding. Your participation is
voluntary. Your decision whether or not to participate will not affect your relationship with Near
East Hospital. If you decide to participate, you are free to withdraw your consent and discontinue
participation at any time without penalty. If you have any questions about the study, please feel free
to contact [[email protected]].[05338398451 [email protected]].
If you have questions regarding your rights as a research subject, please contact the Near East
Institutional Review Board. You will be offered a copy of this form to keep. Your signature
indicates that you have read and understand the information provided above, that you willingly
agree to participate, that you may withdraw your consent at any time and discontinue participation
without penalty, that you will receive a copy of this form, and that you are not waiving any legal
claims.
Participant Name, Surname:
Address:
Phone:
Signature:
Witness
Name, Surname: Address:
Phone:
Signature:
Interviewer:
Name, Surname:
Address: