Treatment of Mastocytosis - MaRIH FILIERE SANTE · Treatment of Mastocytosis Olivier Hermine MD,...
42
Treatment of Mastocytosis Olivier Hermine MD, PhD Hematology Department, Necker Hospital Centre National de référence des mastocytoses, Necker Hospital INSERM U1163 CNRS ERL 8654 Institut Imagine, Necker Hospital Paris, France
Transcript of Treatment of Mastocytosis - MaRIH FILIERE SANTE · Treatment of Mastocytosis Olivier Hermine MD,...

Treatment of Mastocytosis
Olivier Hermine MD, PhD
Hematology Department, Necker Hospital
Centre National de référence des mastocytoses, Necker Hospital
INSERM U1163 CNRS ERL 8654
Institut Imagine, Necker Hospital
Paris, France

Disclosures
• AB science Co Founder, Consultant, Stock Holder, Research grants
• Novartis Research grants
• Celgene research grants

Definitions and Classifications

Definition - Mast cell accumulation in various organs (Skin, GI tract, Liver, Bone and Bone Marrow, etc) -Myeloproliferative disorder; Aggressive vs indolent disease
- Association with hematological disorders - Clinical heterogeneity (Infiltration vs Mediators release)
Photos Pr Bodemer et Dr Barete
Mastocytosis
Children
<2 years
Frequent regression
Reactive disease ?
Adult Young vs Ederly
Adult age onset
Chronic disease
No regression
Clonal disease
Mast cell Leukemia and Sarcoma :
Rare, Rapid Fatal outcome

Mastocytosis : Spectrum of the disease

Mastocytosis : Spectrum of the disease
MCAS

Updated WHO Classification of Mastocytosis 2016
Cutaneous mastocytosis (CM)
- Maculopapular CM (MPCM) = urticaria pigmentosa (UP)
- Diffuse CM (DCM)
- Mastocytoma of skin
Systemic mastocytosis (SM)
- Indolent SM (ISM)
- Smoldering SM (SSM)
- SM with associated hematologic neoplasm (AHN)*
- Aggressive SM (ASM)
- Mast cell leukemia (MCL)
Mast cell sarcoma
-------------------------------------------------------------------------------------
*The previous term SM-AHNMD (SM with clonal hematologic
non-mast cell-lineage disease) and the new term AHN can be
used synonymously.

Prognosis
Blood 2009

Prognosis
Blood 2009
Indolent Mastocytosis >80%
Agressive Mastocytosis <20%

Diagnosis

Mastocytosis Diagnosis
1. DARIER ’S SIGN FOR CUTANEOUS MASTOCYTOSIS
(Skin involvement is not required)
2. HISTOLOGY FOR CUTANEOUS AND/OR SYSTEMIC
MASTOCYTOSIS (required)
- TOLUIDINE BLUE
- ANTI -TRYPTASE STAINING
- CD117+, CD2+ and/or CD25+, CD15-
3. MAST CELL MEDIATORS
- Total tryptase >20ng/ml
- Soluble C-kit level

Clinical and Biological investigations
• Symptoms: handicap fonctionnel, asthenia, prurit, flush, depression, diarrhea, pollakiuria, vascular instabilities
• Clinical: Weight-nutrition, Skin, tumoral syndrome (Lymph nodes, splenomegaly, hepatomegay)
• Biology: CBC, Liver Enzymes, Albumin, tryptase, IgE, Vitamin D.
• Organ infiltration: skin biopsy, bone marrow, others (digestive tract, liver…). Bone marrow aspiration, Mast cell phenotype
• Screening of c-kit mutation (Skin, infiltrated organ, peripheral blood ?)
• Bone check up: X Ray in case of symptoms, Bone density+++.
• Associated Hematological Neoplasm

Diagnosis Criteria and Classification

Physiopathology

MC TC MC T
Stem Cell
CD34+
Bone Marrow
Circulation SCF
IL-10
IL-6
SCF
CD34+
c-kit high
FceRI neg
CD13+
MC C
IL-4 SCF
?
Simplified pathways of human MC
differentiation
Tissues
IL-4 Survival : SCF
NGF
IL-4
IFN-g
…...

MC TC MC T
Stem Cell
CD34+
Bone Marrow
Circulation SCF
IL-10
IL-6
SCF
CD34+
c-kit high FceRI neg
CD13+
MC C
IL-4 SCF
?
Simplified pathways of human MC
differentiation
Tissues
IL-4 Survival : SCF
NGF
IL-4
IFN-g
…...

Oncogenic Mutations of c-kit in Mastocytosis
1
2
Oncogenic Signal
Adult Mutations 85%
Clonal disease +++
No regression
Pediatric Mutations 75%
Clonal disease +++
Regression
Exons 8 to 11 Exon 17 WT

Oncogenic Mutations of c-kit in Mastocytosis
1
2
Oncogenic Signal
Adult Mutations 85%
Clonal disease +++
No regression
Pediatric Mutations 75%
Clonal disease +++
Regression
Sarcoma
Adult
Exons 8 to 11 Exon 17 WT

Oncogenic Mutations of c-kit in Mastocytosis
1
2
Oncogenic Signal
Adult Mutations 85%
Clonal disease +++
No regression
Pediatric Mutations 75%
Clonal disease +++
Regression
Sarcoma
Adult
Exons 8 to 11 Exon 17 WT
Indolent
Vs
Agressive ?
AHN
MCL

SRSF2-P95 Hotspot Mutation is Highly Associated with Aggressive Forms
of Mastocytosis and Mutations in Epigenetic Regulator Genes
•Katia Hanssens, Fabienne Brenet, Julie Agopian, Sophie Georgin-Lavialle, Gandhi Damaj, Laure Cabaret, Maria Olivia Chandesris, Paulo de Sepulveda, Olivier Hermine, Patrice Dubreuil *§ and Erinn Soucie* (Haematologica; in press)

Figure 1
Mutations Hierarchy in Mastocytosis
K Hanssens, haematologica in press S Schwaab, Blood 2013

Travis 1988
Horny 2004
Sotlar 2010
Pardanani 2009
Damaj et al 2013
AHNMD; n (%) 20 (33) 22 (33) 48 134 (40%) 62
Myeloid % 82 90 83 89 82
MDS % 32 9 8 3 28
CMML % 39 27 23 16
MPN % 9 21 45 16
AL % 10 21 3 5
Lymphoid % 11 18
Lymphoma% 6 5 8
MM% N=2 10 4 5 (MGUS)
CLL% 2
•*Damaj et al, CEREMAST, Unpublished data
Associated Hematological Malignancies

Sotlar J Pathol
2010
Horny JCP,
2004
Pardanani Blood 2009
Tefferi Leuk,emia
2009
Traina Plosone
2012
*Damaj 2013
N 48 20 134 23 8 62
D816; n(%) 45 (94) 16 (80) 50 (63) 44 (86)
JAK-2; n(%) na na 6 (8) 2 (7.5)
TET-2; n(%) na na na 8 (35) 5 (62) 12 (32)
ASXL1; n (%) na na na 2(25) 6 (17)
FGFR4; n(%) na na na 7 (18)
CBL; n(%) (12.5)
TET2, ASXL1 are positive, only in the myeloid AHNMD
*Damaj et al, CEREMAST, Unpublished data
Genes mtations in Associated Hematological
Malignancies

6%
30%
11%
4%
49%
CM, n=8
ISM, n=39
ASM, n=14
MCS/MCL, n=5
SM AHNMD,n=64
Ederly patients
130 patients (80 Men 50
Women)
Age 75 years [70-90]
AHN
Leucémie, n=7 11%
MDS, n=21 33% MPF, n=29
45%
MGUS/ myélome,
n=3 5%
Lymphome, n=2 3%
non précisé,
n=2 3%
0
2
4
6
8
10
12
14
mutationTET2
mutationJAK 2
mutationSRSF2
mutationASLX1
mutationIDH2
mutationCBL
mutationU2AF1
mutatioNRAS

Figure 1
P = 0.003 ASXL1 negative. median OS: 92.33 (95% CI, not reached)
AXSL1 positive: median OS: 12.86 (95% CI, 5.56 – 20.17)
ASXL1 but not TET2 muations adversely impact overall survival
of patients suffering systemic mastocytosis with associated clonal
hematologic non mast cell diseaes Gandhi Damaj1,2,3, Magalie Joris1, Olivia Chandesris2,4, Katia Hanssens5, Erinn Soucie5, Danielle Canioni6, Brigitte Kolb7, Isabelle Durieu8, Emanuel Gyan9, Cristina Livideanu10, Stephane Chèze11, Momar Diouf12, Reda Garidi13, Sophie Georgin-Lavialle14, Vahid Asnafi15, Ludovic Lhermitte15, Christian Lavigne16, David Launay17, Michel Arock18,19, Olivier Lortholary20, Patrice Dubreuil5* and Olivier Hermine2,3,4*

Schwaab et al., Blood 2013; 122:2460–2466; Jawhar et al., Leukemia 2016; 30:136-143
Overall frequency and prognostic impact of mutated
genes in 70 advanced KIT D816V+ SM patients
0%
20%
40%
60%
80%
100%
60% of patients had ≥2 mutated genes in addition to KIT D816V
Overall survival in advanced SM depending on mutations in the SRSF2/ASXL1/RUNX1 (S/A/R) panel
S/A/Rneg
S/A/Rpos

Clinical and Molecular Based Risk Score
Jawhar et al., Leukemia 2016; 29

Mastocytosis and psychological stress
Alexythymia ++++
Cognitive functions impairement
Depression
Evidence for Cognitive Impairment in Mastocytosis:Prevalence, Features and Correlations to Depression
Daniela Silva Moura1,2*, Serge Sultan7,8, Sophie Georgin-Lavialle1,3,4, St ephane Barete1,3,5,
Olivier Lortholary1,6, Raphael Gaillard9,10, Olivier Hermine1,3,11,12*
1 Centre de reference des mastocytoses, Hopital Necker Enfants malades, Fondation Imagine Paris, Universite Paris Descartes, Sorbonne, Paris Cite, Paris, France,
2 Universite Paris Descartes, Sorbonne, Paris Cite, Laboratoire de Psychopathologie et Processus de Sante EA 4057, IUPDP Institut de Psychologie, Paris, France, 3 CNRS
UMR8147, Hopital Necker Enfants malades, Paris, France, 4 Service de Medecine Interne, Hopital Europeen Georges Pompidou, Universite Paris Descartes, Sorbonne, Paris
Cite, Paris, France, 5 Departement de dermatologie, Hopital Tenon, Universite Pierre et Marie Curie, Paris, France, 6 Universite Paris Descartes, Sorbonne, Paris Cite, Service
de maladies infectieuses et tropicales, Hopital Necker Enfants malades, Paris, France, 7 Universite de Montreal, Quebec, Canada, 8 Centre de Recherche du CHU Sainte-
Justine, Montreal, Quebec, Canada, 9 INSERM; Universite Paris Descartes, Sorbonne Paris Cite, Laboratoire de Physiopathologie des maladies Psychiatriques, Centre de
Psychiatrie et Neurosciences U894, Paris, France, 10 Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine Paris Descartes, Service Hospitalo Universitaire,
Centre Hospitalier Sainte-Anne, Paris, France, 11 Universite Paris Descartes, Sorbonne, Paris Cite, Service d’hematologie adulte, Hopital Necker-Enfants malades, Paris,
France, 12 Fondation Imagine, IHU Hopital Necker-Enfants malades, Paris, France
Abst ract
Mastocytosis is a heterogeneous disease characterized by mast cells accumulation in one or more organs. We have reportedthat depression is frequent in mastocytosis, but although it was already described, little is known about the prevalence andfeatures of cognitive impairment. Our objective was to describe the prevalence and features of cognitive impairment in alarge cohort of patients with this rare disease (n = 57; mean age= 45) and to explore the relations between memoryimpairment and depression. Objective memory impairment was evaluated using the 3rd edition of the Clinical Memory scaleof Wechsler. Depression symptoms were evaluated using the Hamilton Depression Rating Scale. Age and education levelswere controlled for all patients. Patients with mastocytosis presented high levels of cognitive impairment (memory and/orattention) (n = 22; 38.6%). Cognitive impairment was moderate in 59% of the cases, concerned immediate auditory (41%)and working memory (73%) and was not associated to depression (p$ 0.717). In conclusion, immediate auditory memoryand attention impairment in mastocytosis are frequent, even in young individuals, and are not consecutive to depression. Inmastocytosis, cognitive complaints call for complex neuropsychological assessment. Mild-moderate cognitive impairmentand depression constitute two specific but somewhat independent syndromes in mastocytosis. These results suggestdifferential effects of mast-cell activity in the brain, on systems involved in emotionality and in cognition.
Citat ion: Moura DS, Sultan S, Georgin-Lavial le S, Barete S, Lortholary O, et al. (2012) Evidence for Cognitive Impairment in Mastocytosis: Prevalence, Features andCorrelations to Depression. PLoS ONE 7(6): e39468. doi:10.1371/journal.pone.0039468
Editor: Kenji Hashimoto, Chiba University Center for Forensic Mental Health, Japan
Received February 17, 2012; Accepted May 21, 2012; Published June 20, 2012
Copyright : ß 2012 Moura et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: DSM is recipient from a grant from Canceropole Ile-de-France (Appel d’offre SHS2009). SSis a recipient of grants from the French Institut National duCancer (SHS 2010, 2011). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Compet ing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected] (DSM); [email protected] (OH)
Int roduct ion
Mastocytosis is a rare and heterogeneous disease characterised
by accumulation of mast cells in one or several organs [1–3].
Based on organ dysfunction, systemic mastocytosis is divided
into indolent (. 90% of cases) and aggressive forms [3,4].
Although in its indolent form mastocytosis is not a life
threatening disease, deregulated mast cells activation and
degranulation lead to the liberation of a panel of mediators
(such as serotonin, histamine, tryptase, heparin, substance P,
interleukins (IL8, IL4, IL10), TNF alpha…). Patients suffer from
various clinical symptoms related to mast-cell degranulation
and/ or infiltration. These symptoms can be chronic (pruritus,
urticaria pigmentosa, headache, articular and muscular pain,
memory loss, attention impairment, depression) or paroxysmal
(Flush, anaphylactic like episodes, syncope) [5]. Chronic
symptoms of mastocytosis can be especially disabling and can
significantly affect patients in their personal, social and
professional life domains [6]. In this study, we report an
assessment of chronic memory and attention impairment in
mastocytosis and we explore the interrelationships with depres-
sion, age, education level, treatment and forms of the disease.
Cognitive complaints (memory and attention disturbances) are
common in mastocytosis and in our recent work 38% of patients
reported to feel concerned by these symptoms [6]. To date, only
the study of Rogers and collaborators has evaluated cognitive
impairments in 10 patients diagnosed with systemic mastocytosis
by using a valid psychometric measure of memory function [7].
These authors brought for the first time evidence for memory and
attention impairment in 70% of their sample of patients with
systemic mastocytosis. They suggested that mast cellsderegulation
impact memory function through mediators released including
histamine. Other neuropsychiatric symptoms such as depression
are also present with high frequency in mastocytosis. The
prevalence of depression was estimated 40%, 70% and 64%
according to methods and cut offs used for investigation [6–8].
While prevalence and features of depression in mastocytosis has
PLoS ONE | www.plosone.org 1 June 2012 | Volume 7 | Issue 6 | e39468

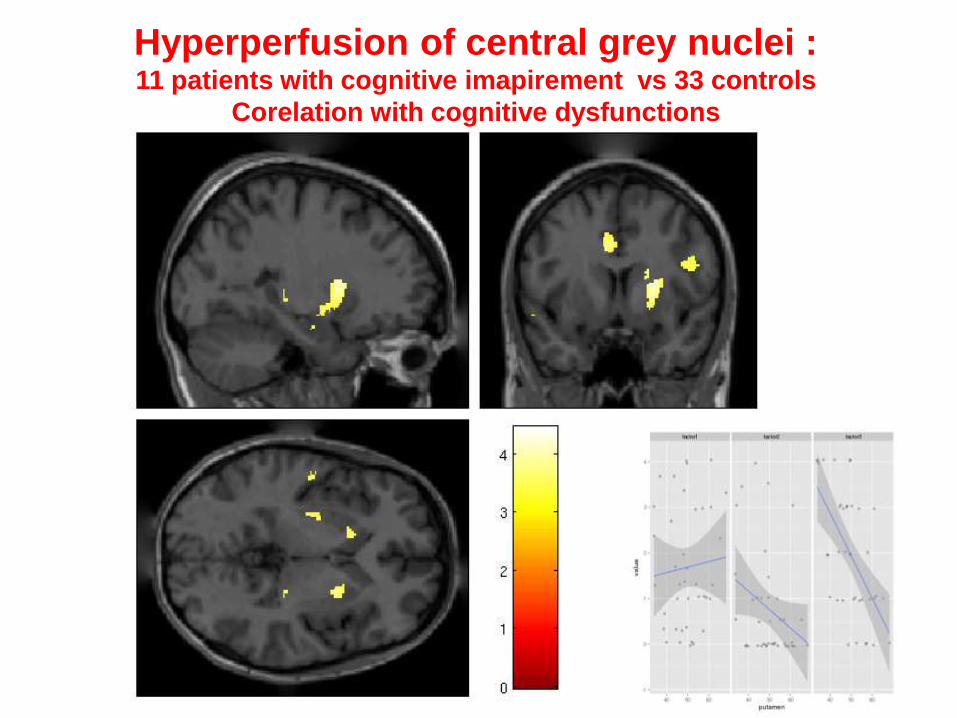
Hyperperfusion of central grey nuclei : 11 patients with cognitive imapirement vs 33 controls
Corelation with cognitive dysfunctions
p<0.001
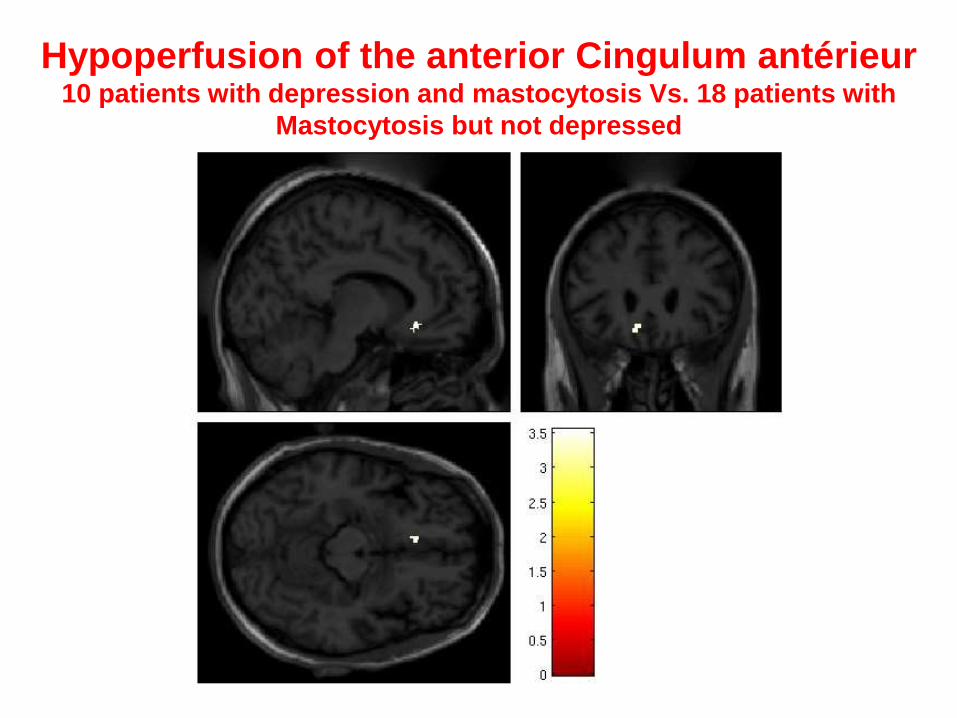
Hypoperfusion of the anterior Cingulum antérieur 10 patients with depression and mastocytosis Vs. 18 patients with
Mastocytosis but not depressed
p<0.001

IDO
Trypytophan metabolism and Mastocytosis Georgin Lavialle et al, Molecular Psychiatry, 2016
TNFa
Tryptophane
Kynurenine
Acid
xanthurenic
Acid
quinolenic
Neurotoxicity
Oxidative stress
apoptosis
-
+
Cognition (?)
serotonin
Low serotonin
Depression ?
Proteases
Histamine
Others
ASL
abnormalities

Treatment

Therapeutic Decision
• Agressive disease : Reduction of life
expectancy and organ failure
• Indolent disease : No life expectancy
reduction, no organ failure , Handicap
associated with symptoms (patient vs
physician)

Treatment of Indolent Diseases

Identification of all systemic manifestations in
patients suffering from mastocytosis
• From 2004, 363 mastocytosis patients and 90 controls in France were asked to rate their overall disability (OPA score) and the severity of 38 individual symptoms.
• A specific questionnaire (AFIRMM V1), encompassing these 38 symptoms, has been created and validated.
PLoS ONE. 2008 May 28;3(5):e2266

Identification of all systemic manifestations in
patients suffering from mastocytosis

Eviction of mast cells stimulants: depend on the patient history
Aim at inhibiting mediator release by mast cell or mediators effects.
- Anti-H1 : pruritus, flush and sometimes GI pains.
- Anti-H2 : essentially GI pains.
- Aspirin : for flushing, tachycardia, but may cause vascular collapse!!!
- Corticoids : for local treatment of cutaneous lesions, ascite, malabsorption, GI
cramps (budesonide: corticoïde à délitement entéral)
- Cromoglycate disodium : non specific mediator release symptoms
- Anti-leucotriènes (montelukast-singulair): for respiratory manifestations
- Epinephrin : Hypotension
- Biphosphonates : bone pain and bone loss
Symptomatic Therapies of Mastocytosis

ITK for indolent diseases
• New ITK
• Inhibiton of Mast cell activation (c-kit, Lyn, Fyn, etc)
• Cytoreductive on Mast cells (optional ++)
• Not cytoreductive on other cells
• Not toxic (short term and long term)
– Genotoxic, carcinogenic
– Cardiotoxic (Abl++, Src, VEGF, Herg chanel, etc)


Masitinib – Kinase inhibitory activity profile Masitinib is a tyrosine kinase inhibitor that target mast cells and macrophages.
[1] Dubreuil 2009, PLoSONE.4(9):e7258 ; AB Science. [2] Davis 2011, Nat Biotechnol;29(11):1046
Target IC50 [nM] Kd [µM]
KIT wild-type (WT) 200 0.008
FYN 240 0.14
LYN 225 0.061
D816V KIT (exon 11) 5,000
KIT mutation (exon 17) 0.3
MCSFR-1 90 0.0076
PDGFRb 300 0.0084
PDGFRα 50 0.0025
Kinase Inhibition Profile of Masitinib
Masitinib (AB1010) Midostaurin (PKC412)

DAY 0
Case Report in Dog Mast Cell Tumor
DAY 3 DAY 18