Treatment of Asthma using OMT 2005 Thomas L. Northup …€¦ · Treatment of Asthma using OMT …...
40
March 006 The AAO Journal/1 Treatment of Asthma using OMT … pages 24-26 and 28-31 2005 Thomas L. Northup Lecture: What if? Dennis J. Dowling, DO, FAAO …page 11 Thomas L. Northup, DO FORUM FOR OSTEOPATHIC THOUGHT TRADITION SHAPES THE FUTURE VOLUME 16 NUMBER 1 MARCH 2006
Transcript of Treatment of Asthma using OMT 2005 Thomas L. Northup …€¦ · Treatment of Asthma using OMT …...

March�006 The AAO Journal/1
Treatment of Asthma using OMT… pages 24-26 and 28-31
2005 Thomas L. NorthupLecture: What if?Dennis J. Dowling, DO, FAAO
…page 11
ThomasL.Northup,DO
Forum For osteopathIc thought
tradItIon shapes the Future Volume 16 number 1 march 2006

�/The AAO Journal March�006
Instructions to Authors
TheAmericanAcademy of Osteopathy®(AAO)Journalisapeer-reviewedpublicationfordisseminatinginformationonthescienceandartofosteopathicmanipulativemedicine.Itisdirectedtowardosteopathicphysicians,students,internsandresidentsandparticularlytowardthosephysicianswithaspecialinterestinosteopathicmanipulativetreatment.
The AAO Journal welcomescontributionsinthefollowingcategories:
Original Contributions Clinicalorappliedresearch,orbasicscienceresearchrelatedtoclinicalpractice.
Case Reports Unusualclinicalpresentations,newlyrecog-nizedsituationsorrarelyreportedfeatures.
Clinical Practice Articlesaboutpracticalapplicationsforgen-eralpractitionersorspecialists.
Special Communications Items related to theartofpractice, suchaspoems,essaysandstories.
Letters to the Editor CommentsonarticlespublishedinTheAAO Journal ornewinformationonclinicaltop-ics.Lettersmustbesignedbytheauthor(s).Noletterswillbepublishedanonymously,orunderpseudonymsorpennames.
Book Reviews Reviewsofpublicationsrelatedtoosteopathicmanipulativemedicineand tomanipulativemedicineingeneral.
NoteContributions are accepted from membersoftheAOA,facultymembersinosteopathicmedical colleges, osteopathic residents andinternsandstudentsofosteopathiccolleges.Contributionsbyothersareacceptedonanindividualbasis.
Submission SubmitallpaperstoAnthonyG.Chila,DO,FAAO, Editor-in-Chief, Ohio University,CollegeofOsteopathicMedicine(OUCOM),GrosvenorHall,Athens,OH45701.
Editorial ReviewPaperssubmittedtoThe AAO JournalmaybesubmittedforreviewbytheEditorialBoard.Notificationofacceptanceorrejectionusuallyisgivenwithinthreemonthsafterreceiptofthepaper;publicationfollowsassoonaspos-siblethereafter,dependinguponthebacklogof papers. Some papers may be rejectedbecauseofduplicationof subjectmatter ortheneedtoestablishprioritiesontheuseoflimitedspace.
Requirements for manuscript submission:
Manuscript 1. Type all text, references and tabularmaterialusingupperandlowercase,double-spacedwithone-inchmargins.Numberallpagesconsecutively.
�.Submitoriginalplusthreecopies.Retainonecopyforyourfiles.
3.Checkthatallreferences,tablesandfiguresarecitedinthetextandinnumericalorder.
4. Include a cover letter that gives theauthor’s full name and address, telephonenumber,institutionfromwhichworkinitiatedandacademictitleorposition.
5.Manuscriptsmustbepublishedwiththecorrectname(s)of theauthor(s).Nomanu-scripts will be published anonymously, orunderpseudonymsorpennames.
6.Forhumanoranimalexperimentalinvesti-gations,includeproofthattheprojectwasap-provedbyanappropriateinstitutionalreviewboard,orwhennosuchboardisinplace,thatthemanner inwhichinformedconsentwasobtainedfromhumansubjects.
7.Describethebasicstudydesign;defineallstatistical methods used; list measurementinstruments, methods, and tools used forindependentanddependentvariables.
8.Inthe“MaterialsandMethods”section,identifyallinterventionsthatareusedwhichdo not comply with approved or standardusage.
Computer DisksWeencourageandwelcomecomputerdiskscontainingthematerialsubmittedinhardcopyform.ThoughwepreferMacintosh3-1/�”disks,MS-DOSformatsusingeither3-1/�”or5-1/4”discsareequallyacceptable.
AbstractProvidea150-wordabstractthatsummarizesthemainpointsofthepaperandit’sconclu-sions.
Illustrations 1. Be sure that illustrations submitted areclearlylabeled.
�. Photos should be submitted as 5” x 7”glossyblackandwhiteprintswithhighcon-trast. On the back of each, clearly indicatethe top of the photo. Use a photocopy toindicate theplacementof arrowsandothermarkersonthephotos.Ifcolorisnecessary,submitclearlylabeled35mmslideswiththetopsmarkedontheframes.Allillustrationswillbereturnedtotheauthorsofpublishedmanuscripts.
3.Includeacaptionforeachfigure.
Permissions Obtainwrittenpermissionfromthepublisherand author to use previously published il-lustrationsandsubmittheseletterswiththemanuscript.You also must obtain writtenpermissionfrompatientstousetheirphotosifthereisapossibilitythattheymightbeidenti-fied.Inthecaseofchildren,permissionmustbeobtainedfromaparentorguardian.
References 1. References are required for allmaterialderivedfromtheworkofothers.Citeallrefer-encesinnumericalorderinthetext.Iftherearereferencesusedasgeneralsourcematerial,butfromwhichnospecificinformationwastaken,listtheminalphabeticalorderfollow-ingthenumberedjournals.
�. For journals, include the names of allauthors,completetitleofthearticle,nameofthejournal,volumenumber,dateandinclu-sive page numbers. For books, include thename(s)oftheeditor(s),nameandlocationofpublisherandyearofpublication.Givepagenumbersforexactquotations.
Editorial ProcessingAllacceptedarticlesaresubjecttocopyedit-ing.Authorsareresponsibleforallstatements,including changes made by the manuscripteditor.NomaterialmaybereprintedfromThe AAO Journalwithoutthewrittenpermissionoftheeditorandtheauthor(s).

March�006 The AAO Journal/3
Advertising Rates for The AAO JournalOfficial Publication
of The American Academy of Osteopathy®
TheAOAandAOAaffiliateorganizationsandmembersoftheAcademyareentitled
toa�0%discountonadvertisinginthisJournal.
Call:TheAmericanAcademyofOsteopathy®
(317)879-1881formoreinformation.
Subscriptions:$60.00peryear(USA) $78.00peryear(foreign)
Advertising Rates: Size of AD:Fullpage$600placed(1)time 71/�x91/� $575placed(�)times $550placed(4)times1/�page $400placed(1)time 71/�x43/4 $375placed(�)times $350placed(4)times1/3page $300placed(1)time �1/4x43/4 $�75placed(1)times $�50placed(4)times1/4page $�00placed(1)time 31/3x43/4 $180placed(�)times $150placed(4)timesProfessionalCard:$60 31/�x�Classified:$1.00perword
In thIs Issue:AAOCalendarofCourses...................................................................................4Contributors.........................................................................................................6ComponentSocieties’CMECalendar...............................................................��
edItorIal
ViewfromthePyramids:Anthony G. Chila, DO, FAAO ..............................5
regular Features DigOn............................................................................................................7 FromtheArchives..........................................................................................8 BookReviews......................................................................................... 37-38 ElsewhereinPrint.........................................................................................39
2005 thomas l. northup lecture Whatif?.........................................................................................................11
Dennis J. Dowling, DO, FAAO
clInIcal practIce Amyofascialtriggerpointontheskull:Treatmentimprovespeak flowvaluesinacuteasthmapatients.............................................................�3 Wm. Thomas Crow, DO, FAAO and David Kasper, MBA
scIentIFIc paper/thesIs (Faao) Intercostalribrelease....................................................................................�6 Claudia L. McCarty, DO, FAAO
the student physIcIan Multidisciplinaryapproachtotreatmentina38-yearoldfemale, restraineddriverfollowinginjuriessustainedinarear-endcollision...........33 James L. Rook, MPH, OMS-IV, Western University of Health Sciences and Ann Marie Auburn-Dean, DO
tradItIon shapes the Future • Volume 16 number 1 march 2006
a peer-reVIewed Journal
The Mission of the American Academy of Osteopathy® is to teach, advocate, and research the science, art and philosophy of osteopathic medicine, emphasizing the integration of osteopathic principles, practices and manipulative treatment in patient care.
3500DePauwBoulevardSuite1080Indianapolis,IN46�68(317)879-1881FAX(317)879-0563
amerIcan academy oF osteopathy®
KarenM.Steele,DO,FAAO................. PresidentKennethH.Johnson,DO..............President-ElectStephenJ.Noone,CAE..........ExecutiveDirector
edItorIal adVIsory boardRaymondJ.Hruby,DO,FAAODeniseK.Burns,DOStephenM.Davidson,DOEileenL.DiGiovanna,DO,FAAOEricJ.Dolgin,DOWilliamJ.Garrity,DOStefanL.J.Hagopian,DOHollisH.King,DO,PhD,FAAOJohnMcPartland,DOStevePaulus,DO,MSPaulR.Rennie,DOMarkE.Rosen,DO
the aao JournalAnthonyG.Chila,DO,FAAO..... Editor-in-ChiefStephenJ.Noone,CAE..........SupervisingEditorDianaL.Finley,CMP................ManagingEditor
TheAAO JournalistheofficialpublicationoftheAmericanAcademy of Osteopathy®. Issues arepublishedinMarch,June,September,andDecem-bereachyear.
Third-classpostagepaidatCarmel,IN.Postmaster:Sendaddress changes to:AmericanAcademyofOsteopathy®, 3500 DePauw Blvd., Suite 1080,Indianapolis, IN., 46�68. Phone: 317-879-1881;FAX: (317) 879-0563; e-mail [email protected];AAOWebsite:http.//www.acad-emyofosteopathy.org
TheAAO Journalisnotitselfresponsibleforstate-mentsmadebyanycontributor.Althoughallad-vertisingisexpectedtoconformtoethicalmedicalstandards,acceptancedoesnotimplyendorsementbythisjournal.
Opinionsexpressedin The AAO Journalarethoseof authors or speakers and do not necessarilyreflectviewpointsoftheeditorsorofficialpolicyof theAmericanAcademyofOsteopathy®or theinstitutionswithwhich theauthorsareaffiliated,unlessspecified.
Forum for Osteopathic Thought
Tradition Shapes the Future • Volume 16 Number 1 March 2006

4/The AAO Journal March�006
American Academy of Osteopathy®
Calendar of Events
2006
Mar 20-22 Visceral/Structural Integration inBirmingham,Alabama
Mar 22 AAOBoardsofGovernorsandTrustees inBirmingham
Mar 22-26 AAO ConvocationinBirmingham
May 5-7 Diagnosis and Treatment of Low Back Pain inDurham,NC
May 19-21 Prolotherapy: Above the Diaphragm atUNECOM
Jun 16-18 OMT for Common Organic and Clinical ProblemsatUMDNJ-SOM
Jul 1 AOBNMMapplicationdeadline
Jul 14-16 Visceral Manipulation: Urogenital inSanFrancisco
Aug 18-20 The Still Technique (Applications of a Redis-covered Technique of Andrew Taylor Still, MD) atSouthpointHospitalinCleveland,OH
Sep 15-17 Advanced Clinical Jones Strain-Counterstrain: Emphasis on Extremities atUniversity
ofIndianapolis
Oct 15 One-daycourse–Introduction to Osteopathic Medicine for the Non-physician
Licensed Health Care ProviderinLasVegas
Oct 16-20 AOA ConventioninLasVegas
Nov 3-5 Prolotherapy: Below the Diaphragm atUNECOM
Dec 1 AOBNMMapplicationdeadline
Dec 1-3 Visceral Manipulation: Membranes inSanFrancisco
Functional Methods 2nd Edition
byWilliamJohnston,DO,FAAOHarryFriedman,DO,FAAO
DavidEland,DO,FAAO
ORDER INfORMATION:
_____Functional Methods�ndEditionSoftbound @$50.00eaplusshipping&handling
_____Functional Methods�ndEditionHardbound @$65.00ea(plusshippingandhandling)
(Call or write for foreign shipping rates)
ShIPPINg INfORMATION:
Name________________________________________
Street_________________________________________
City____________________State____Zip_________
DaytimePhone:________________________________
E-mailAddress:________________________________
Payment Information:
❒ VISA❒ MC❒ CHECK
CardNo.______________________________________
ExpirationDate____________________
Foryourcopies,contact:American Academy of Osteopathy®
3500 DePauw Blvd., Suite 1080Indianapolis, IN 46268
phone: (317) 879-1881; fAX: (317) 879-0563order online:www.academyofosteopathy.org

March�006 The AAO Journal/5
View from the Pyramids
Anthony G. Chila
AndrewTaylorStill’scontributiontotheimprovementofthepracticeofmedicinehas,inrecentyears,shownapropen-sityforinternationalexpression.AlthoughstillrecognizedasbeingofAmericanorigin,thecommunityofpractitionersabroadhasshowndiverseexpressionformanyyears.
Thetrainingandscopeofpracticeintheosteopathic
worldhasdistinguishedthreetypesofpractitioners:US-trainedDOs(GraduatesofAmericanOsteopathicAssociation[AOA]-accreditedosteopathicmedicalschools);Nonphysi-cianosteopaths(Graduatesofschoolsofosteopathyinfor-eigncountries,trainedinosteopathicprinciplesandpractice,butnothavingunlimitedpracticerights);Foreignphysicianswithosteopathicspecialties(Graduatesofforeignmedicalschools,specializinginOsteopathicPrinciplesandPractice[OPP]).1
TheAmericanAcademyofOsteopathy(AAO)hostedits1stInternationalForumin1996.ThisforumprovidedanopportunityfordiscussionanddeliberationforNonphysi-cianosteopaths.SubsequentyearshaveseentheeffectsoftheInternationalForumsfacilitatetheemergenceoftwomajorforcesfortheexpressionofosteopathicpractice:anOsteopathicInternationalAlliance(OIA)establishedbytheAmericanOsteopathicAssociation(AOA);aWorldOsteo-pathicHealthOrganization(WOHO)establishedthroughtheeffortsofUStrainedDOsandinternationalosteopaths.AAOmembershavebeenactivelyinvolvedwithbothinmember-shipandgoverningboards.TheWorldHealthOrganization(WHO)hasbeeninstrumentalininitiatinganinternationalprojectaddressing“guidelinesonthesafetyandefficacyofosteopathy.”Again,theAAOhasbeenactivelyinvolved.
Thereisanearlierhistoryofactivitywhichcanbeviewedasinformalpreparationforthesepost-1996organizationalaccomplishments.Variousaspectsofactivityspoketoanappreciationofheritagewhileexpressingdifferentiationintraditions.Itisinthisearliererathatonecanseethesowingofseedswhich,slowlyatfirst,butwithgraduallyincreasingmomentum,preparedthescenewhichisbeingwitnessedtoday.ThepracticesofindividualUStrainedDOsincountriesabroadduringtheyearsfollowingWorldWarI,theinter-waryears,andthepost-WorldWarIIyearscanbecited.TheestablishmentoftheBritishSchoolofOsteopa-
thy(BSO)byJohnMartinLittlejohnwasthebeginningofaEuropeantraditionwhichfacedresistancetodevelopmentsimilartothatoftheUSexperience.Thisrepresentedacyclewhichbeganwhenthiseducator,apatientandstudentofStill,becameafacultymemberandDeanoftheAmericanSchoolofOsteopathy(ASO),laterfoundedtheAmericanCollegeofOsteopathicMedicineandSurgerywithhistwobrothers,thenreturnedtohisnativecountry.TheoppositionoftheGeneralMedicalCouncilofGreatBritaintotheeffortsofLittlejohnwascertainlycomparabletotheoppositionoftheAmericanMedicalAssociationtoosteopathicdevelopmentintheUnitedStatesduringthisperiodoftime.ThedecadefollowingWorldWarIIsawthebeginningofmorefrequentcommuni-cationandteachingbetweenUSandBritishDOsinLondon.FulllicensureofUSDOshadnotbeenachievedatthattime,andinterestwasbeingshowninosteopathicpracticebysomeEuropeanMDs.Duringthesecondpost-WWIIdecade(1964),aBasicCourseinOsteopathyintheCranialFieldwaspresentedinParis,conductedbyateachingteamoftheSutherlandCranialTeachingFoundation(SCTF).Invariousways,thenext30yearssawtheemergenceofnationalorga-nizationsandregistriesleadingtomoreformaldefinitionofeducationalrequirementsandpracticestatutes.Ahistoryofinternationalactivityfromtheearlyyearsofthe�0thCenturythrough,perhaps,1975wouldprovideawonderfulprologuefortheeventsofthepast10years.
OneyearaftertheAAO-sponsored1stInternationalForum,in1997,theAndrewTaylorStillMemorialAddresswasdeliveredbyW.DouglasWard,PhD.DoctorWardhadservedastheAOADirectorofEducation(1977-1993)andasAssociateExecutiveDirectorforEducationalAffairs(1993-1996).InhisaddresstotheAOAHouseofDelegatesAnnualMeetingatChicago,henotedthat:“OsteopathicmedicineisnowthoroughlyintegratedintotheorganizationalstructureoftheUnitedStates.Itisonlyamatteroftime—perhaps100years—forthisstructuretoextendthroughouttheworld.”�
Timehasmovedveryrapidly,andtheshadowofAndrewTaylorStillcontinuestolengthen.
1. The DO.April�005;10�. The DO.November�005;4�
The Wide World of Osteopathy

6/The AAO Journal March�006
Contributors Regular Features
Dennis J. Dowling. What If? The33rdThomasL.NorthupLecture (�005) addresses a periodically recurring question.Inthisinstance,theauthordiscussesabonesetternamedJobSweet. This apprenticed practitioner was a descendent of afamilywhoseoriginscanbetracedto1637.Sweetwasbornin17�4,acenturybeforeAndrewTaylorStill.HewasadecadeslongpractitionerintheRhodeIslandregion.Typicalofbone-setterfamilytraditions,skillsandmethodswerepasseddownthroughgenerations.What If? pondersthequestionofSweet’sabilitytomodifytheevolutionofAmericanmedicineviatheimplementationofanewschoolofthought,Osteopathy. Thequestioncontinuesexploration throughrecommendationsforcurricularteaching.(p. 11).
Wm. Thomas Crow and David Kasper. A Myofascial Trigger Point On The Skull: Treatment Improves Peak flow Values In Acute Asthma Patients. Nine(9)patientswhowereexperiencingacuteasthmaticexacerbationsandwererefractorytostandardtreatmentwereseenbytheauthorsapproximately1-3hoursfollowingtreatment.Theauthorsidentifiedamyofascialtriggerpointattheleftparietaleminenceontheskull.Directpressureofthetriggerpointfor45seconds,afterwhicharepeatPeakFlowmeasurementwasobtained.Retrospectivestudyofthesepatients(ages16-55years)showeddramaticimprovement.Furtherstudyisindicated.(p. 23).
Claudia L. McCarty. Intercostal Rib Release. ThisScientific Paper/Thesis was submitted in partial fulfillmentof requirements for Fellowship in theAmericanAcademyofOsteopathy.TheauthorreceivedstatusasFellowin�000.Thepaperisextensive,offeringconsiderationsofEpidemiol-ogy,Physiology,Pathophysiology,Management.AReviewofResearchisalsoprovided.Forpublication,thesectiondealingwithaprotocolformanagementofacuteasthmaticexacerbationutilizingintercostalribreleasehasbeenchosen.Theauthormaybecontactedregardingothersectionsofthispaper.(p. 26).
JL Rook and AM Auburn. Multidisciplinary approach to treatment in a 38-year old female, restrained driver follow-ing injuries sustained in a rear-end collision. Complicatedsequelaefrommotorvehiclecollisionsareperplexingtomanypracticingphysicians.CurrentlyknownasCervicalWhiplashSyndrome (CWS) orWhiplashAssociated Disorder (WAD),multifactorial considerations are necessary. The authors de-scribesuccessfulmanagementofapatientseen14monthsaftersuchoccurrence,utilizingOsteopathicManipulativeTreatment(OMT)andTriggerPointInjections(TPI).(p. 33).
DIg ON. AndrewTaylorStilldidnot,inhiswriting,uni-formlyprovidereferencesfor“standardmedicalauthorities.”His Autobiography (1897) offers an example (pp. 44�-443,withillustration).ThroughcourtesyoftheFunkandWagnallsCompany,theillustrationofthemuscularsystemofthebodyaffordsStilltheopportunitytodiscuss“TheArmyofMuscles.”(p. 7)
fROM ThE ARChIVES. The Practice of Osteopathy (CarlPhilipMcConnellandCharlesClaytonTeall,1906)of-fersveryusefulconsiderationsfortreatmentofasthma.Reliefduringexacerbationisareadilyattainablegoal.Remedyoftheprocess isemphasizedduringthe intervalbetweenexacerba-tions.(p. 8).
BOOK REVIEW. The Science and Practice of Manual Therapy: Physiology, Neurology and Psychology (E.Lederman,�ndEd.,ChurchillLivingstone�005).ProfessorEyalLedermanrevisitsthequestionof“Whatishappeningunderthehandsofthemanual therapist?” twelveyears afterbeginning towritethefirsteditionofFundamentals of Manual Therapy. Thekeyelementsofpatient cognition, active involvementofpatient,effectivefeedback,repetitionandsimilaritytonormalizedmove-mentsareaddressed. (p. 37). Cranial Osteopathy: Principles and Practice (T.Liem,�ndEd.,Elsevier�004).TorstenLiem,DO(GB)hasprovidedacomprehensiveandhighlystructuredtextaddressingthemorphology,clinicalassociations,diagnosisandtreatmentofstructuresofthehumancranium.Thiseffortis theoutcomeof revisionofhisprevious text andprovidessignificantincorporationofcontemporaryresearchinthisarea.(p. 38).
ELSEWhERE IN PRINT. UrinaryTractInfection(UTI)isthemostcommonlydiagnosedbacterialinfectioninwomen.Whilemajormorbidityormortalityarerare,economicandqual-ityoflifefactorsareconsiderable(Johns Hopkins University Advanced Studies in Medicine: Volume6,Number1-January�006 ; �4.)Linearmouthopeningisbeingreplacedbytemporo-mandibularopeningindex(TOI)asameasureofmandibularopening.Thelatterisindependentofage,gender,ramuslengthandgonialangle. It isalsomoreuseful indiagnosticgroupcategorization (CRANIO, The Journal of Craniomandibular Practice; Volume�4,Number1-January�006;�5).(p. 39).
CME CREDIT. Inresponsetoreaderrequests,AAOJ willofferCMECredittoreaderscompletingtheenclosedquiz.Atthistime,1HourII-BCreditwillbeoffered,withrequestforupgradeasAAOJ qualificationsarereviewedbytheAmerican Osteopathic Association. (p. 30).

March�006 The AAO Journal/7
Dig On
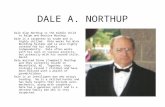
The Army of Muscles“Autobiography of A. T. Still”, pages 442-443Published by the authorKirksville, MO1897© by A.T. Still
Muscular System of Man.1. Frontal. 2. Orbicularis palpebrarum. 3. Zygomaticus minor. 4. Zy-gomaticus major. 5. Temporal. 6. Levator labii superioris. 7. Levator labii superioris alaeque nasi. 8. Compressor narium. 9. Orbicularis oris. 10. Depressor labii inferioris. 11. Buccinator. 12. Platysma. 13. Sternoclidomastoid. 14. Sternohyoid. 15. Trachea. 16. Scaleni. 17. Tra-pezius. 18. Occipitalis. 19. Masseter. 20. Splenius capitis. 21. Splenius colli. 22. Levator anguli scapulae. 23. Supraspinatus. 24. Infraspinatus. 25. Rhomboideus. 26. Teres minor. 27. Teres major. 28. Deltoid. 29. Subclavius. 30. Intercostal. 31. Pectoralis major. 32. Pectoralis minor. 33. Serratus magnus. 34. Latissimus dorsi. 35. Biceps of the arm. 35’. Long head of same. 35”. Short head of same. 36. Coracobrachialis. 37. Triceps. 38. Pronator radii teres. 39. Flexor carpi radialis. 40. Palmaris longus. 41. Supinator longus. 42. Extensor carpi radialis longior. 43. Extensor ossis metacarpi pollicis. 44. Extensor tendonof the little finger. 45. Annular ligament of wrist. 46. Abductor pollicis. 47. Flexor brevis pollices. 48. Palmaris brevis. 49. Extensor tendon of middle finger. 50. Rectus abdominis. 50’. Sheath of same. 51. Navel. 52. External oblique of abdomen. 53. Internal oblique of abdomen. 54. Poupart’s ligament. 55. Inguinal canal. 56. Serratus posticus in-ferior. 57. Crest of the ilium. 58. Tensor fasciae latae. 5a9. Iliopsoas. 60. Pectineus. 61. Adductor longus. 62. Gracilis. 63. Vastus externus. 64. Vastus internus. 65. Rectus femoris. 66. Quadriceps extensor femoris. 66’. Tendon of same. 67. Sartorius. 68. Gluteus maximus. 69. Gluteus medius. 70. Gluteus minimus. 71. Pyriformis. 72. Obturator internus. 73. Obturator externus. 74. Tuberosity of the ischium. 75. Sacrosciatic ligament. 76. Biceps of the thigh. 77. Semitendinosus. 78. Semimembranosus. 79. Patella. 80. Tibia. 81. Peroneus longus. 82. Tibialis anticus. 83. Extensor longus digitorum. 84. Extensor longus pollicis. 85. Gastrocnemius. 86. Flexor longus digitorium. 87. Tendo Achillis. 88. Soleus. 89. Tibialis posticus. 90. Flexor longus pollicis. 91. Annular ligament of the ankle. 92. Extensor brevis digitorum. 93. Extensor tendon of the toes.
Chapter XXXII.The Muscles-Brain Headquarters-The Army of Muscles-
The Secret of God-How to Live Long and Loud-Time Coming for Big Dinners-Command to Eat-Off to the Country-Oste-opathy Cures Seasickness-Country Friends-Quiet and Shady-Explaining the Cause of Lumbago-Tired Nature Seeks Repose.
THROUGHthekindnessofFunk&WagnallsCompanyofNewYork,wearepermittedthiselaboratecut,whichshowsaboutone-fourthofthemusclesofthehumanbody,eachofwhichisausefulservantinperformingthelaborsoflife.Igiveplacetothosebeautifulpicturesofsomeofthepartsofthatgreatestofallknownmachines,whobearsthenameofman.Willthoseofyouwhohavenothadthechancetostudyanatomyinschoolsorotherwise,pleaselookforafewmin-utesandseetheshapesofafewmuscles;seehownicelytheyareformedandproperlyplacedtodothegreatdutiestheyhavetoperforminlife?Youseetheyhavegreatstrength,andallequaltothedutiestheyhavetodischarge.Ifyoulookalloverthebeingfromheadtofoot,youfindbracesatallpartsofthebody,andtheyarepowerfulinqualityandsize,justtosuittheplace,andarefixedtoholdallbonesinposition,withmuchpower,leftafterdoingtheworkofbracing,toliftmuchadditionalweight.
Eachmuscleissodistinctfromallothermusclesinformandoffice,infactwemightcalleachmuscleanofficerwhoserankisadivisioncommander.Hemustanswertothegrandroll-callhimself,whichisfromthecommandinggeneral,whoseheadquartersandnamearethebrain.Eachmusclemustreporttothecommandinggeneralandsalutehimwithbecomingdignity,andthishighofficermustsaluteandrespectallsubordinates,orthegreatbattleoflifewillbelost.Hemustkeepiscourierstoeachdivisioncommanderinmotion,allthetimebearingdespatchesoftheconditionofallcampsthatarebeingreportedatheadquarters.Eachdivisioncommandershallreceiveandreallalldespatchesinthefieldofaction-thequartermast,commissary,company,squads,andsections,notofonecampordivision,butallofthewholearmy.

8/The AAO Journal March�006
From the Archives
Bronchial or spasmodic asthmaisachronicaffection,characterizedbyaparoxysmaldyspneaduetoaspasmodiccontractionofthemusclesofthebronchialtubesortoswell-ingoftheirmucousmembrane.
Osteopathic Etiology and Pathology.Themajorityoflesionscausingbronchialasthmaarefromthesecondtotheseventhdorsalregion,inclusive,eitherintheribsposteriorlyoranteriorly,orinthevertebrae.Theselesionsinvolvevasomotornervestothebronchioles,whichproducethenarrowingofthetubesandthuscausethedyspnea.Usuallythelesionisatthethird,fourthorfifthribontherightside,although,asstated,alesionmaybefoundaboveorbelowthispointattheanteriororposteriorendsoftheribsorinthevertebraecorrespondingtothesameregion.Probablylesionsarefoundmoreontherightside,becausemostpeoplearerighthanded;thesemusclesbeingbetterdevelopedwouldtend,whencontracted,todrawtheribsfromtheirarticulation.Thethird,fourthandfifthribsareusuallyfoundinvolvedbecauseitistheregionofgreatestvaso-motorinnervationtothebronchialtubes.
Inanumberofcasestherewillbefoundaposteriorcurvatureofthedorso-lumbarregion;andaccompanyingthisconditionwillbecatarrhanddilatationofthestomach,congestionoftheliver,and,perhaps,intestinalindigestionandconstipation.Carefulattentionshouldbegiventothedigestiveorgans.
Occasionallyalesionisfoundinvolvingthepneumogas-tricattheatlasandaxis.Suchalesionalsoirritatesfibresofthepneumogastrictothemusclesofthebronchiolesandthusproducesnarrowingofthetubesandconsequentlytheparox-ysms.Otherpointstonotearethecostalcartilagesandhyoidbone,andprobably,inafewinstances,lesionstothephrenic.
Attacksmaybeinducedreflexlybyvariousexcitants,asdust,diseasesoftheupperrespiratorytract,etc.,butthelesionstothevaso-motorandmotornervesarethepredispos-ingcauses.Laughlin1says:“Itisquestionablewhetherreflexcausesalonearesufficienttoproducegenuineasthmawithouttheexistenceofspecificlesionsaffectingthedirectnervecon-nectionsofthepartinvolved.”
Pathologically,trueasthmaisapureneurosis.Thereismoreorlesschronicinflammationofthebronchialtubes,shownbyinjectionandthickeningofthebronchialmucosainthemajorityofcases.Theremaybefoundthemorbidstatespeculiartochronicbronchitisandemphysema.Whetherthe
constrictionofthetubesisduetospasmsofthebronchialmusclesortoswellingofthemucosa,ortoboth,theprimary,predisposingandirritatinginfluencesarecommontoboth.Thesearevertebralandriblesionsaffectingthespinalnervesattheirexitandthesympatheticchainalongtheheadoftheribs;irritatinglesionstothevagi,constrictingpulmonaryvessels,andtothecervicalsympathetics,causingdisturbance
ofthesame,wouldbefactorsinthepathologicalchain.Reflexirritationsmaybefoundinvariousregions,buttheprincipalosseouslesions,accordingtoDr.Still,areontherightsidefromthesecondtothesixthdorsal.
Symptoms.Theattackmaycomeonatanytime,butusuallyitcomesoninthenightduringsleep.Theonsetmaybesuddenortheattackmaybeprecededbypremonitorysensations,suchastightnessinthechest,flatu-lence,sneezing,chillinessandacopi-
ousdischargeofpaleurine.Nervoussymptoms,headache,vertigo,neuralgia,andananxious,nervous,restlessfeelingmayprecedetheattack.Thereisasenseofoppressionandanxiety,followedbydyspnea.Soontherespiratoryeffortsbe-comeviolentandthepatientisobligedtosituporruntothewindowforair.Theshouldersareraised,thehandsareplaceduponsomethingfirmtokeeptheshouldersfixedsothattheaccessorymusclesofrespirationcanbe’broughtintoplay.Thecontractedtubesresisttheentranceofair.Expirationisprolongedandwheezy.
Inseverecasesthefacebecomespale,theskiniscoveredwithperspiration,theextremitiesarecold,thelips,finger-tipsandeyelidsarelivid,owingtodefectiveoxygenationoftheblood.Thepulseissmallandquickandthetemperatureisnor-malorsubnormal.Theattackmayterminatesuddenly,sometimeswithaspellofcoughing;thisisespeciallysoofseverecases,asthecoughisgenerallyabsentinbriefparoxysms.
Thecoughisatfirstverytightanddryandaccompaniedbyatough,scantyexpectorationwhichisexpelledwithgreatdifficulty.Thesputumcontainsroundedmassesofmatter,theso-called“perles”ofLaennec.Microscopically,theyarefoundtobeofaspiralstructure,containingcellsderivedfromthebronchialmucousmembraneandfattydegeneratedpuscells.Asecondformiscontainedintheinsideofthecoiledspiralofmucin,afilamentofgreatclearnessandtranslu-cency,thatismostprobablycomposedoftransformedmucin.Curschmann’sspiralsarefoundintheearlystagesoftheattackandforatimetheseweresupposed,bytheirirritation,
Bronchial asthmaThe Practice of Osteopathy.CarlPhilipMcConnellandCharlesClaytonTeall.Copyright1906.pgs.517-5�1

March�006 The AAO Journal/9
toexcitetheparoxysms.Theirspiralformisunexplained.Curschmannbelievesthatthesespiralsarefoundinthefinerbronchiolesandtobeaproductofbronchiolitis.
Physical Signs.Inspectionshowsenlargementofthechestwhichisfixedandbarrel-shaped.Thebreathingislaboredandthechestmovesbutslightly.Thediaphragmislowered.Per-cussionyieldshyper-resonance,especiallyincaseswhichhavehadrepeatedattacksorwhentheasthmaisassociatedwithemphysema.Auscultation.Withinspirationandexpirationareheardsonoroussibilantrales,whicharemoremarkedonexpi-ration.Asthesecretionincreases,whichislaterintheattack,theralebecomesmoist.Theattacklastsforavariableperiod,rarelylessthananhour.Insevereattackstheparoxysmsrecurforthreeorfournightsormorewithspontaneousremissionsduringtheday.Insomecasesthereliefseemstobeabsolute,butinthemajorityofcasesthereismoreorlessoppressionandcoughforadayortwo,sometimesformanydays.
Diagnosis.Thephysicalsigns,examinationofthesputumandthehistoryofthecasemakesthediagnosiseasy.
Prognosis.Itisnotafataldiseaseandonlydangerouswhencomplicationsarise.Underosteopathictreatmenttheprognosisisusuallyfavorable,unlessthereareseriouscom-plications,asthisisadiseasethatosteopathyhastreatedwithsignalsuccess.Inlongstandingcasesemphysemainvariablydevelops.
Treatment. Asthma,unlesscomplicatedwithbronchialandlungdiseases,isreadilyrelievedduringtheparoxysms..Casesofmanyyears’standinghavebeencuredinafewtreat-ments.Itshouldbeborneinmindthatasthmaisarespiratoryneurosis.
Torelieveanattacktheosteopathshouldlocatethele-sion,ifpossible,andcorrectit.Ifthemusclesaresoseverelycontractedthatitisimpossibletomakeoutthenatureofthelesion,thenstronginhibition,withanupward,outwardmovementovertheanglesoftheribsinvolved,willbequitesufficient.Theobjecttobegainedineverycaseistorelievepressureorirritationtothevaso-motorormotornerves,sothatthenarrowedtubesmayberelaxed.Stronginhibition,suchasplacingthekneeinthepatient’sback,atthesametimepullingontheshoulders,willhavetemporaryeffect,butitisalwaysbesttoreducethelesionifpossible.Inseverecasesdilatationoftherectummayrelievetheparoxysm,andinafewinstanc-esitwillbenecessarytotreattheuteruslocally.
Duringtheintervalbetweentheattacksisthetimetorem-edythedisease.Thenoneisabletolocateexactlythepositionofthedisturbedtissuesthatarecausingtheparoxysmsandapplytreatmentintheregionsgivenunderetiology.Many
casesofasthmaarecuredinfromonetothreemonths’treat-ment.Onetreatmentaweekissufficient,providedoneisableeachtimetoaccomplishsomethingtowardacorrectionofthelesinandthatthepatientdoesnotsufferduringthemeantime.Toofrequenttreatmentsmaysimplyactasanirritanttothenervouslesions.
Attentionshouldalwaysbegiventothedietandhygiene.Gastricdigestionshouldbecompletebeforeretiringoritmayinduceanattack.Complicationsaretreatedaccordingtothedisease..Examinetheupperrespiratorytract,thedigestivetract,andthepelvicorganswhenthereisreasontobelievetheparoxysmmaybeinducedreflexly.Laughlinsumsupthetreatmentasfollows:(1)Removalofspecificlesion;(�)removalofexcitingcauses;(3)removalofreflexcauses;and(4)treatmentofthepatienttoimprovetheconditionofthegeneralnervoussystem.
References1. Laughlin.Asthma.JAOA.Oct1904.

10/The AAO Journal March�006
s a medical professional, you understand what it takes to be the best atwhat you do. At Nordic Naturals, we do too. Nordic Naturals focuses
on one thing and one thing only: Fish Oils.
That’s why medical professionals like you consistently choose Nordic Naturalsfish oils for their practices. The fish oil you recommend to your patients canmake the difference in their compliance and results. Rely on Nordic Naturals.
For clinical support on the use of fish oils, contact us for a free copy of JosephMaroon, M.D.’s Spine Pain study.
For more information, a FREE sample, or third-party analysis, please call: 800.662.2544 x1 • email: [email protected] • or visit: nordicnaturals.com
Nordic Naturals fish oils surpass allinternational pharmaceutical standards forfreshness and purity, making Nordic Naturalsthe logical choice for you and your practice. Pure and Great Tasting Omega Oils
“My patients prefer NordicNaturals because it is easyto take every day and athigh-dose levels. The purity, potency, and lackof repeating are key to my patients’ compliance.”
Dr. Joseph MaroonProfessor of Neurosurgery –University of Pittsburgh Team Physician – Pittsburgh Steelers
NewSuper Concentrates!
58% EPA
45% EPA
A

March�006 The AAO Journal/11➝
Thomas L. Northup Lecture, 2005American Academy of Osteopathy®
What if?Dennis J. Dowling
Awarsuchasthecontinenthadneverpreviouslyseenhaddevastatedthecountry.Brotherhadbeenpitchedagainstbrotherandthetollhadcreatedalterationsinhowcommerce,politics,education,andmedicinehadbeenpracticed.
Itwasduringthistimethataloneitinerantdoctortraveledhundredsofmilesattherequestofafamilyinneedtodowhathe felt was his life’s work, healing the sick.The lone ridermade the trip to see to the needs of the young woman whowascrippledwithwhatwasdescribedasadislocatedhipbone.Hisreputationhadbeenwellestablishedwithinhisimmediateregionbecauseofallofthemiraculouscuresthatwereassoci-atedwithhishands.
Thepatient,thedaughterofaprominentsoldierandpoliti-cian,hadbeenunsuccessfullytreatedbyconventionalmedicalapproaches. In fact, the family physician and several otherlearneddoctorswantedtobepresentduringthetreatment.Afterhisarrival,atimeforthedemonstrationwassetfor10:00AMthenextmorning.Thespectatordoctorsleftfortheirhomesandthehostsoughttogethisguestsettled.Beingwearyandtired,butnotingthegreatpainthepatientwasexperiencing,thedoc-torexpressedhisdesiretosetabouttoworkimmediatelyandnotwaitforthenextday.The13-year-oldgirlwasalittletakenaback with the doctor’s disheveled and apparently eccentricappearance.However, thedoctorapproached thepatientandexplainedincomfortingtoneswhatitwasthathewasgoingtodototreather.Oncehehadsecuredhercooperation,heaskedforpermissionfromherfather,aswasproperforthetime,totouchherhipandleg.Likethedoctor,thepatient’sfatherwasnotsomuchinterestedindemonstrations,onlyinhisdaughter’scomfortandreadilyagreedforthetreatmenttobegin.Inafewminutes,manipulationoftheregionhadbeencompletedandthedoctorinstructedthepatienttowalkaroundtheroom.Muchtothesurpriseofthepatientandherfather,shewalkedaroundtheroomwithoutpain.Bythetimethephysiciansarrivedthenextmorning,thedoctorwasonhiswayhomeward.1Ifhehadbeenmoreofashowman,perhapshecouldhavechangedthewaymedicinewaspracticedontheAmericancontinentforever.
ForanyonewhohasreadstoriesaboutAndrewTaylorStill,thisscenariowouldnotsoundthatunusual.PerhapsitsoundslikesomethingfromHildreth’sThe Lengthening Shadow of Dr. Andrew Taylor Still.Intruth,itoccurredalittlelessthan80yearsbeforeA.T.Still“flunghighthebannerofosteopathy.”Thedoc-torofthestorywasnotAndrewTaylorStill,butwasabonesetternamedJobSweet,andtheyearwasmostlikely1795.
Duringtherevolutionarywar,Dr.Sweetwasoftencalled
toNewport,RhodeIslandtosetthebonesofFrenchsoldiers,somethingthattheirowndoctorscouldnotaccomplish.Hewasadoctorlikemanyoftheerawere:amanwhohealedthesick.LikeothersoftheSweetclan,whichcanbetracedasfarbackas1637whenJohnSweetcametothecolonies,Jobwassaidtohave“inherited”hisbonesettingtalent.
Hewasbornin17�4,practicedfordecadesintheRhodeIslandregion,andlikeothermembersofhisfamilyappearedtohaveanuncannyknowledgeofanatomydespitelackingaformaleducation.Once,whilebeingshownsomeexhibitsinasciencehallinBostonbyalearnedprofessorandphysician,heremarkedthatoneofthefootbonesofadisplayedskeletonwasinthewrongorientation.Thephysicianprotestedthatitwasexpertlyassembledbutuponlaterexamination,determinedthatJobSweetwascorrect.�
Itwasnotuntilthetwentiethcenturythatsomemembersofthefamilybecamemedicalschooltrainedphysicians.Dr.JobSweetmadethetripfromRhodeIslandtoNewYorktotreatTheodosiaBurr,thedaughterofColonelAaronBurr,thethirdvice-presidentof theUnitedStatesofAmerica. Itwasmanyyearsbeforetheunfortunateduel(July7th1804at7AM)3thathasbeenabigpartofBurr’slegendorhissubsequentattempttoestablishaseparateempireintheMidwestpartoftheconti-nent.JobSweetmayhavebeenthemostskilledbonesetterofa familyofpractitioners thathadfirstemigratedfromWalestotheAmericancontinentintheseventeenthcentury.Aswasthetraditionofthetimes,thesecretswerepassedfromgenera-tiontogenerationpriortoandafterDr.Sweet’streatmentofTheodosiaBurr.
Ashasbeenindicated,itoccurrednearly90yearspriortoDr.Still’sestablishmentofthefirstschoolofosteopathyaswellasnearly60yearspriortoWhartonHood’streatisesupportingbonesetting4.ItoccurredshortlyafterColonelBurrhadbecomea single parent. He was extremely devoted to his daughterTheodosiaandtohistwostep-sonsandinsisteduponathor-ougheducationforall.Theodosiacouldreadandwriteseveralmodern and classical languages and engage in conversationconcerningallmatteroftopics,includingpolitics.Shemeanttheworldtohimandheconsultedalltypesofphysiciansregardingherconditionwithoutmuchbenefit.Apparently,JobSweetac-complishedwhat“modernmedicine”couldnot.However,beingarelativelyshyman,hefinishedhistaskandretreatedtohishomewithoutfanfareorshowmanship.Whatifhehadwaiteduntil10:00AMthefollowingmorning?Couldthathavebeen

1�/The AAO Journal March�006
asimportantasthesametimeonJune��nd,1874?Whatifthedoctorshadbeenimpressedwithhisskillsanddesiredtolearnmore?Washereticenttobethecenterofattentionorwasitatacticalmovetoavoidexposureofthefamilysecretstocriticaleyes?WhatifbonesettinghadbeenincorporatedintocolonialAmericanmedicaltreatment?
ColonelBurrwasatonetimeaveryinfluentialmanandasapoliticianactuallycameveryclosetwicetobecomingpresi-dentoftheUnitedStates.Infact,hetiedThomasJeffersoninelectoralvotesandonlylosttobecomevice-presidentfollowing36ballotsbytheHouseof Representatives. Hewasalwaysinterestedinwielding power. Couldhe have exerted his in-fluence to incorporatebonesetting into theAmerican medical sys-tem?Intruth,therewasnoorganized systemofmedicine.Therewastheeducated physician orthe apprenticed physi-cian.Dr.Sweetqualifiedasthelatter.
The first medicalschoolattheCollegeofPhiladelphia was onlyestablished a few yearspriorin1765.Dr.Sweetwasalready41-years-oldbythistime.KingsCol-lege, which would be-come Columbia, wouldnot have a medicalschool until 1768. Har-vard,thethirdinstitutiontohostamedicalschool,would not establish itscollegeofmedicineuntilthe conclusion of theRevolutionary War in1781. Most medical-school-trainedphysiciansontheNorthAmericancontinentuptothatpointandevenforalongtimeafterwards,weretrainedattheUniversityofEdinburgh5.ThevictimsofbattleswagedduringtheRevolutionaryWarweretreatedbyphysicianshavingallsortsoftraining,butmostlikelybythecommonapprenticed-trainedvariety.Therewerealsobattlesbeingfought,politicallyandotherwisebythephysiciansofthelateeighteenthcentury.Shippen,Morgan,andRush,aswellasahostofothers,contestedto seewhowould control themedical professionof the era.CouldAaronBurrhaveintroducedDr.JobSweetandhissystemofcaretotheworldatlarge?CouldDr.Sweetteachwhathadonlybeenpasseddownfromparentstochildren?Woulditbe“osteopathy”asweknowit?Itwouldnothave,mostprobably,beentreatedasasystemofmedicinedifferentthanwhatwaspracticedandwouldmostlikelyhavebeenaddedtothethen
currentprocessesofphlebotomy,amputations,andpoisonousmedicinals.Itwouldhavebeenmerelyanadditionalmodality.Inaway,itwouldnotbeviewedanydifferentlythanhowsomeMDs see osteopathy today: manipulation as a possible formoftreatmenttobeaddedtotheothertoolsandnotasawholesystemofhealthcare.
ThebiggerquestiontoponderregardingthestoryofJobSweetis,“WhatifDr.SweethadhadthementalityofAndrewTaylorStill?”CouldhehaveinitiatedtheevolutionofAmeri-canmedicineawayfromitsallopathiccourse?Hewouldhave
needed to have had theintellectual curiosity ofAndrewTaylorStill,ac-companiedbytheeccen-tric ego that gave innerstrength and a sense ofrighteousness, as wellas the significanteventsthatwentintothefound-ing of osteopathy. Hewould have needed theconvictionthatheshouldteach the family secretstoothersforthegoodofmankind.Hewouldhaveneededtoplanttheseedsofthenewmedicineinaphilosophy that lookedatthepatientandnotthedisease;attheinteractionofthepartsofthewholeandnottheeffectofthesymptoms; at the inte-grative processes of theindividual in seeking orrestoringhisownhealthwiththeaidofthephysi-cianandnotthepassiverole when physicianstook extraordinary andoftentimes dangerousmeasures. The eventsof the founding of os-
teopathycameaboutatthemostpropitioustimeforitsbirth.Yet,Dr.Stillclaimedthatithadalwaysbeenpresent.Toquotetheolddoctor,“IdonotclaimtobetheauthorofthisscienceofOsteopathy.Nohumanhandhasframeditslaws;Iasknogreaterhonorthantohavediscoveredit.”6IthadbeenthereforDr.StilltofindanditwasthereforJobSweetorsomeotherhealertodiscover.Instead,itremainedhiddenasdosomanyofthe“secrets”thathavebeendescribedbygreatphysiciansformillennia.Glimpsesofgreatthingshavebeenobservedonlybrieflytothenbeburiedandforgotten.Whydidn’tJobSweetdiscoverosteopathy?Hewasnottherightperson.TherewouldandcouldhavebeennooneotherthanAndrewTaylorStilltoexposeosteopathytotheworld.
Thepracticeofwondering “What If?” is not somethingnew.Sciencefictionstorieshaveexploredtheconceptforhun-

March�006 The AAO Journal/13
➝
dredsofyearsandcomicbookshaveengagedintheprocessfordecades.Popularnovelsandmoviesarejustthejuxtapositionofimagination,creativity,andreality.Wealldoitinourmindswhetherwevoiceitornot.Wedoitprospectivelyandretro-
spectively.WhatifIdidn’tmake that turn? Maybe Iwouldn’thavegottenintothataccident.WhatifIhadpicked the right numbersin the lottery?What if Ihadn’tgonetoosteopathicmedical school? Wouldsomeonehavebeentheretohelpthepatientswhenthey needed it most?Weuse“whatifs”tolookbackat the roads not taken aswell as looking forwardduring decision-makingtimes to try to determinethealternatives.
Itisevenpracticedbyhistorians. The Military
HistoryQuarterlyhaspublishedtwopopularbookstitled“What If?”7,8,whicharecollectionsofarticlesthathaveappearedwithinitspages.Thetermthatisusedbytheeditorsis“counterfac-tualhistory”indicatingthatachangedkeyeventinhistoryisexploredforthepossibleconsequences.Ratherthanjustbeingfiction,thestoriesindicateagreatdealabouttheimpactoftheeventsastheyactuallydidoccur.WhatwouldhavehappenedhadAlexander the Great been killed when he attacked thePersiansnineyearspriortohiseventualdeath?Certainly,therewouldhavebeennocityofAlexandriainEgypt,nolibraryofgreatknowledge,noPtolemypharaohs,noCleopatra,andnoconquestoftheknownworld.Perhaps,therewouldhavebeenanearlierorlaterdevelopmentofaRomanEmpire9.
WouldtheAmericanRevolutionhavesucceededwithoutitsiconicleader,GeorgeWashington?BesideshismiraculousescapefromBrooklynwithallofhistroopsduringanalmostpreternaturalfog10,hecamewithinmomentsofbeingshotintheback.TheBritishmarksmanwhoinventedthebreechloadingmusketcouldhardlyhavemissed thestately6’3” redheadedcommanderwhomheeasilyrecognized.However,being themanthathewas,hecouldnotbringhimselftobehavedishon-orably by shooting the unsuspecting general11.We can alsowonderwhatwouldhavehappened ifhewasnot treatedbyphysiciansafteranupperrespiratoryinfection.ItwasnotavirusorbacteriumthatkilledPresidentWashingtonbuthisdoctorswhophlebotomizedhimuntil, inhisweakenedcondition,hesuccumbedtohisillness.
Scientists also engage in the same sort of “What If?”thinking.WhatifHeronofAlexandria,alsoknownasHeroor“Mchanikos,theMachineMan”,hadcombinedhisknowledgeofothermachineswithhisinventionofthesteamengine?Thiswasnearlyeighteenhundredyearspriortotheappearanceofthesteamboatandlocomotive.SomehistoriansthinkthatHerononlyconsideredhisinventionatoywhileothersthinkthattheeconomicsofthedayandavailabilityofslaveandcheaplabor
precludedtheuseofmechanicaldevices1�.SomanyofHeron’sinventions13 were lost: hydraulics that automatically openedtempledoorsandpoweredmachines,mechanicalbirdsthatsangandmoved,therepeatingcrossbowthatwasa“machinegun”thatcouldfireseveralpowerfulboltsperminute,clockswhosefunction remained a mystery for nearly two thousand years,andtheautomatedtheaterthatwasas“computerized”asanyDisneyanimatronicexhibition.HewasasprolificandingeniousasEdisonandwecandeviseallsortsofalternativefuturesex-tendingfromthispoint.Explorerswouldhavetraveledhoursordaysacrossseasandoceansthathadpreviouslythwartedtheirefforts.FlyingmachinessuchasenvisionedbyDaVinciwouldhavetraveledfromcitytocity.Empiressuchaswehaveneverpreviouslyimaginedwouldhaverisenandfallen.Theindustrialeracouldhaveoccurred17centuriesearlierthanitdid.
AndrewTaylorStillengagedinhisown“WhatIf?”mus-ings.OneoftheseconcernedhisCivilWarexperiences:
“Duringthehottestperiodofthefightamusket-ballpassedthroughthelapelsofmyvest,carryingawayapairofglovesIhadstuckinthebosomofit.Anotherminie-ballpassedthroughthebackofmycoatjustabovethebuttons,makinganentryandexitaboutsixinchesapart.HadtherebelsknownhowclosetheywereshootingatOsteopathy,perhapstheywouldnothavebeenquitesocareless.”14
Hemusthavealsowonderedwhatcouldhavebecomeofhimwhenheaccidentallycameuponagroupofpro-slaverspriortotheoutbreakofthewar.TheyweredrillinginafieldwhilehewasonhiswaytovisitMrs.Jones,whowasill.Hetookadefiantstance:
“Whatintheh--lareyoufellowsupto?”IwasansweredbytheCaptainincommand:“Whereintheh--lareyougoing?”Isawinamomentthat
myfirmnesshadproducedgoodeffect,andtherewasnofurtherdanger.Irodeupandstoppedinfrontofthecompany,shookhandswiththeCaptain,toldhimtogivethecommandtomeandIwoulddrillhismen,andshowhimhowJimLaneandJohnBrowndidit,concludingwith:
“Ifyoudon’thaveyourmenbettertrained,andJimLane

14/The AAO Journal March�006
evermeetsyou,hewillshakeyouup.”TheCaptainturnedhismenovertome,andIdrewthem
upinline,putthemthroughallthecavalrymovements,tangledthemup,straightenedthemout,andtoldtheCaptainhemustdrillbetter,sotheycouldgetoutoftightplaceswhentheymet
us.Then I turned the company over to the original CaptainOwens,whosaid:
“Attention,company;thisisDr.Still,thed--destabolitionistoutofh--l,whoisnotafraidofh--lorhighwater.Whenyouaresick,goforhim;hesavedmywife’slifeincholera,andIknowhimtobesuccessfulanyplaceyouareamindtoputhim.Inpoliticsheisourenemy,insicknesshehasproventobeourfriend.”Andclosedbysaying:“Doc,gohometodinnerwithme,andIwillgowithyoutoseeMrs.Jones.”IwentwiththeCaptaintodinner,andhemadehiswordgoodbygoingwithme.Fromthat,timeuntilthecloseofthepro-slaveryquestionin1857Imet,passed,and repassedhismenwithout fearormolestation.15
Therearesomanyotherosteopathic“WhatIfs?”:WhatifDr.Still’sfirstwifeandchildrenhadnotdiedofdisease?Whatif hehadnot treatedhisownheadacheswith a rope swing?Whatifhehadnotbeensointerestedandknowledgeableaboutanatomy?Whatifhehadbeenamoresuccessfulallopathicphy-sician?Whatifhehadbeenalesssuccessfulosteopath?WhatifDr.StillhadhadtheAmericanSchoolofOsteopathy(ASO)grantanMDdegreeinsteadofaDiplomateandlateraDoctorinOsteopathydegree?16WhatifAbramStillhadbeenalawyerinstead?Wouldhehavebecome“A.T.Still,Esq.–LightningLawyer”instead?Thelistcangoonandonyetthefactsremainthathisactionsleadtothefoundingoftheosteopathicprofessionandmorethan55,000osteopathicphysicianstoday.
Muchconjecturecanbedirectedatothereventsinthehis-toryoftheprofession.TheStillNationalMuseumpublishedanarticleinanewsletteryearsagorelatingthatsomeofDr.Still’sadmirersgavehimamementofromtheCivilWar,whichhekeptonhisporchforyears.Hemusthavestruckhispipeagainstitmanytimesandmayhaveeventappeditwiththewalkingstickthathealwayscarried.Afterhisdeath,itwaslaterdiscovered
thatthecannonshellheldliveammo.TherealcounterfactualstorywouldbetoconsiderwhatwouldhavehappenedtotheprofessionhadDr.StilldiedbeforeDecember1�th,1917.WouldtherehavebeenapowerstrugglethatwouldhavetorntheASOandtheprofessionapartatatimewhenitwaslesscapableof
weatheringthestress?Evenimmediatelyafterhisdeath,therewerestrugglesamongtheboardmemberswhenanon-DOnon-familymember,Mrs.MaeDeWittHamiltonthenexthigheststockholderafterDr.A.T.Stillinthecorporation,wasselectedpresident.CharlesStill,DOhadsoldoffmanyofhissharesinthecorporationthatownedtheASOandhadnoclout.17Theloyalties of the members of the board and the faculty werevery much tested at that time.The school had survived theearlyschismswithElmerBarberandMarcusWard,aswellasconflictswiththeLittlejohns,WilliamSmithandseveralothersbutthoseeventsoccurredpriortoDr.Still’sdeath.Some,eventhoughtheyweredisruptiveatthetime,definitelyreinforcedtheprofession.Ifitwerenotfortheseconflicts,therewouldbenoChicagoCollegeofOsteopathicMedicineandprobablynoosteopathyinEurope.ThestrengthtomaintaintheprofessionshouldDr.Stillhaddiedin1900mayhavecomefromBlancheStill.Alongwithherhusband,GeorgeLaughlin,sheco-foundedtheA.T.StillCollegeofOsteopathyandSurgery in19��. ItmergedtwoyearslaterwiththeoriginalschooltobecometheKirksvilleOsteopathicCollege.18
Theprofessionhashadmanyothercrossroadsorkeyeventsthatcouldhaveresultedinotheroutcomes.Oneofthesecon-cernedtheSpanishinfluenzapandemicof1917-1918.19,�0,�1,��,�3Itisnotsomuchthattheprofessionchanged,butletusimaginewhatwouldhavehappenedhadtherebeennoosteopathicphysi-cians.Morethan500,000Americansdiedrelatedtothedisease.Taskerdidasurveyandpublishedtheresultsfrom1,350DOsand43,500casesoffluwithjust160deaths.�4KendrickSmith,anM.D./D.O.,collecteddatafrom�,445osteopathicphysicianswhocollectively treated110,1��caseswith0.�5%mortalityor�75deaths�5.Theprojectednumberforthiscohortgiventhegeneralmortalityrateshouldhavebeenatleast11,01�dead.That indicates that 10,737 people survived who would have

March�006 The AAO Journal/15
otherwisedied.Ifweextrapolateevenfurtherandconsiderthatagenerationoccursevery�0yearswitheachpersonhavingtwochildren, thenwecanestimate thatover170,000Americansalivetodayaredescendantsofthosefortunatepatients.Ifwetake thehalfmillionwhodiedandapplya0.�5%mortality,1�,500wouldhavediedinstead.Thatisrelativelynearwhatthenormalstatisticsareformostrecentvirulentfluepidemics.Itwouldhavethenplacedbehindthe1957-1958and1968-1969epidemicswith70,000and33,000Americansinrelateddeathsrespectively�6.ThedifferencewiththeSpanishflupandemicisthatitdidnotjustkilltheveryold,theveryyoung,ortheverysick;itkilledindiscriminately.Theremayhavebeen15,000,000moreAmericanstodayhadtherebeenlymphatictreatmentforall.Withmorethan�0milliondeadfromthepandemicworld-wide,manytimesthecombatantcasualtiesfromWorldWarI,thenumberwhocouldhavesurvivedifthefocushadbeenonfacilitatingthenaturalimmunologicaldefenseswouldbeincred-ible.Theneedtohavealternativestothetreatmentofinfluenzamaybeevenmorepressingtodaysincewehaveseenthelackofdiscovery,preparednessandefficacyinmanyofthecurrentinterventions.However,wecannotrestonthesuccessesofthepast.Whenosteopathicphysicianssavedallthosethousandsofpeople,theywerestillmakinghousecallsandsometimestreat-ingpatientstwoandthreetimesperday.We,asaprofession,shouldprepareforthefutureneedsofpatientsshouldanothersuchvirulentpandemicoccur.
Twodecadeslater,WatsonandPercival�7didathreeyearstudyofchildrenhospitalizedforpneumoniaintwometropolitanhospitals.Atonehospital, thechildrenreceivedOMTandatthenon-osteopathichospital,standardcare.WheretheTaskerandSmitharticleswere theresultsofaretrospectivesurvey,WatsonandPercivalproducedaprospectivestudythatmetorfarexceededthesophisticationofmanyoftheotherepidemio-logicalstudiesoftheera.Thechildrenwithbronchopneumoniahadnearlyone-thirdthemortalityoftheuntreatedgroup.Themortality for children with lobar pneumonia in both groupswasessentiallythesame.Onehundredandfiftychildrenwithbronchopneumoniaweretreatedattheosteopathichospitaland90%livedversusthe70%ofthe331childrenwholivedattheother hospital.This indicates that 44 children survived whootherwisewouldhavebeenexpectedtosuccumbandtherearepossibly700descendantsalivetodaybecausetheirancestorswerefortunateenoughtobepatientsofosteopathicphysicians.AlthoughWatsonandPercivalhadonlypercentagestoreportthedifferences,theirreviewofthedatawasdetailedandwellrecorded.A Chi test on the data would be very statisticallysignificant.Isthereapossibilitythatsomeoneinthisaudienceisadescendentofthetreatedchildren?
Wecanwonderiftherewasnolymphatictreatmentandnoosteopathicmedicine.Wecanwonderiftheremayhavebeenmoreinterestinsuchalternativetreatmenthadtherebeennodevelopmentofrelativelyeffectivemedications.Priortothelate1930s,therewereanti-seraandinoculationsbutnotmuchelse.Thesulfaantibioticswereonlyafewyearsoldandnotveryavailable.ThemouldhadsettledontoFleming’scultureplatesbutitwasyearsbeforeithadanyconsequenceinthewaragainstinfection.Otherthanosteopathictreatment,therereallywasahodge-podgeofapproachesforinfectiousdiseases.Theheroic
ageofmedicinehadnotyetrunitscourse.Extraordinarymeth-ods,themainstayofthe“allopathic”orthodoxapproachwerestillrampant.Sweatingfevers,dangeroushomeandprescrip-tionremedieswerestillinuse,andthetypicalphysiciancouldjustwatchandwait.Osteopathicmedicine,withitshands-onapproachmadeadifference.Frommorerecentstudies,weun-derstandtoagreaterdetailthemechanismofactionandthetrueeffectivenessofosteopathicmanipulationintreatinginfectiousdiseases.�8�930Wecanwonderifosteopathicmedicinewouldhavebecomemorepopularhadtherebeennodevelopmentofantibiotics.Wecanalsoconsiderthattheremaybegreaterinter-estinthecurrentagesincetherearegrowingconcernsregardingpharmaceuticalsaswellasantibioticresistencesonthepartofmanypathogens.
Thegrowthoftheosteopathicprofessiondidnotjustcon-cernthenumberofphysicians.Themembersoftheprofessionalsoaddedtotheknowledgeanddevelopment.Wherewouldwebewithouttheircontributions?Wecanonlyhopethattherewouldhavebeensomeone todiscoverCranialOsteopathy iftherewasnoWilliamGarnerSutherlandorMuscleEnergyiftherewasnoFredMitchell,Sr..WouldtherehavebeenCoun-terstrainifLawrenceJoneshadn’tconsideredwhattodowitha patient who was severely bent forward?What ifThomasNorthuphadnotexisted?Firstofall,theremaynothavebeenanAmericanAcademyofOsteopathy.ItwasThomasNorthupwhotooktheinitiativetogetstudygroupsorganized31.
Inthefirstthreedecadesofthetwentiethcentury,thereweresectionalsocietiesthatwouldmeetattheAOAconventionsinroomsthattheywouldsecureatthehotels.Dr.PerrinWilsonranthesacroiliacsection,whichwassometimescalledthe“So-cietyofSacroiliacTechnicians.”Dr.Northuphadhissightssetlowerandwasinchargeofagroupthatfocusedonthefoot.In1937,Dr.Northupwroteto135colleaguesintheAOAinvitingthemtoabreakfastmeetingonJuly6th.Sixtythreecameandthegenesisofasocietytodevelopthescienceandartofosteo-pathic manipulative treatment, arrange programs to improveosteopathicphysicians’skills,encouragethedevelopmentanddistributionofteachingofnewmethods,andpublishoriginalarticleswasestablished.TheSocietyofSacroiliacTechniciansevolvedtobecomeTheOsteopathicManipulativeTherapeuticandClinicalResearchAssociationbythenextyear’sconvention,whenitwasrecognizedasacomponentsociety.ThisbecameTheAcademyofAppliedOsteopathyin1944anditunderwentanothernamechangein1970toitscurrentstatus,TheAmericanAcademyofOsteopathy.3�
We have to also assume that if there was no ThomasNorthup,therewouldbenoGeorgeNorthup.TheyoungerDr.NorthupwasalsotheeditoroftheJournal of the American Os-teopathic Associationfor�6years,editoroftheAAO Yearbook and Osteopathic Research: Growth and Development, author of Osteopathic Medicine: An American Revolution,andwasapresidentoftheAmericanOsteopathicAssociationin1958to1959.33Betweenthem,thecontributionsofThomasandGeorgeNorthuptotheprofessionhavebeeninvaluable.
Withinthehistoryoftheprofession,therearefewseminaleventsthathavehadanimpactonitsgrowthordangertoitsexistence like theCaliforniasituation thatexplodedin196�.

16/The AAO Journal March�006
Proposition�� eliminated the mechanism to license any ad-ditionalosteopathicphysicianswithinthestatewhilesimulta-neouslyallowingfortheexchangeofaDOforanMDdegree.TheprocesscouldnothavecomeaboutwithouttheconspiracyandcooperationofaselectgroupofleadersandmembersoftheCaliforniaOsteopathicAssociation.JohnCline,MD,195�presidentoftheAMA,surveyedosteopathiccollegesin1953-55andrecommendedthatMDscouldteachinosteopathiccollegesHealsoadvocatedthatthe“cult”labelberemovedfromDOsandthatstatemedicalsocietiescoulddeterminetheprofessionalrelationshipbetweenMDsandDOs.However,theAMAwouldmaintainthesamerequirementsthattheyhadforothernon-al-lopathicpractitionerswhomtheyotherwisefoundacceptableand assimilated; would remove philosophical and historicalreferences; and would adhere to only thoseAMA approvedscientific principles.The College of Osteopathic PhysiciansandSurgeonsaswellas theCaliforniaOsteopathicAssocia-tionacceptedtheseprovisionsandthelatteramalgamatedwiththeCaliforniaMedicalAssociationin1961.COPSbecametheCaliforniaCollegeofMedicine.Proposition��wassupposedtosealthedealbyeliminatingthefurtherlicensingofosteo-pathicphysicians.TwothousandbecameMDsintheconversionprocesseswhile400didnot.Ofthe400,manyactuallymain-tainedpracticesoutofstate.IftheactualnumberofDOswhomaintainedtheirlicensefellbelow40,thepropositionallowedforthetotaldissolutionoftheosteopathicboard.TheAOAlostnearlyone-seventhofitsmembersandthereappearedtobethepossibilityofacascade.Partoftheironyisthattheconvertedphysicians,the“littlem.d.s”stilldidnotattaintherecognitiontheysoughtfromthespecialtysocietiesacrossthecountry,bytheir“colleagues”withinCaliforniaandespeciallybyotherstatemedical licensingboards.Acoregroup inCaliforniabandedtogetherand1�yearslaterwontherightforfutureDOstobelicensed.Eventuallyanewschool,theCollegeofOsteopathicMedicineofthePacific,wasdeveloped.Ratherthanrolloveranddie,theprofessionarosetobestrongerandmoresecure.Thatisthehistory.34,35
Wecanentertainseveralcorridorsof“WhatIfs?”.WhatiftheCMAandtheAMAhadbidedtheirtimeandnegotiatedwithseveralstateosteopathicmedicalsocietiessimultaneously.IftherewereDOsinCaliforniawhowishedtobeMDs,thentherewerecertainlymanyotherswhohadthesamedesirefromotherpartsofthecountry.Eveninthepresenttherearemany‘wannabe MDs’.The conversion process could have causedsuchadominoeffectthatitmayhavemadeitimpossiblefortheosteopathicprofessiontoeverrecover.Perhaps,themilitaryinthemid1960swouldhaveonlyacceptedanosteopathicallyschooledphysician ifheor shehad receiveda license tobeanMD.Wecanalso lookat it from theperspective that theamalgamationattemptfailedandthat therewouldhavebeennoProposition��.Withouttheenticementtobecomeinstantlyrecognizable,the�,000whoconvertedwouldnothavebecomeMDs.Insteadofthegenerationofnewschoolsthatarosemorethanadecadelater,theprofessionmayhaveremainedwiththesamesixosteopathicschools.Perhaps,thateventhadmoretodowiththegrowthoftheosteopathicprofessionoverthelast30to40yearsthanwithasetback.
Whataboutthepresentandthefuture?Whatifosteopathic
educationwasosteopathic?Thatisnotanattemptatsarcasmorironybutanobservationoftheconditionofthingsastheyare.AstheliberaleconomistStuartChase(1888-1985),said,“De-mocracy,ashasbeensaidofChristianity,hasneverreallybeentried.”Thesamecanbesaidanygovernmentalphilosophicalapproachortheologyaswellasforosteopathicmedicine.Oste-opathyhasnottrulyhappened–notinourschools,residencies,andnotinourspecialtycolleges.Althoughwecouldanalyzeanyofthese,Iwouldliketospecificallyaddressoneofmygreatestinterests:osteopathicmedicalschooleducation.Itwouldbeasimpleextensiontoaddresstheotherinstitutions.TheschoolsofosteopathicmedicinehaverootsstretchingbacktotheoriginalinstitutioninKirksvilleandthedeansofalloftheschoolsmustbeosteopathicphysiciansandallmusthavedepartmentstoteachosteopathicmanipulativemedicine.Therehavebeenmany“ten-fingered”deansandfacultyattheseschoolsovertheyears.Ofcourse,therehavealsobeendeanswhohavehadconsiderablyfewerfingers,atleastfiguratively.ThetruthisthattheacademicprogramsareoftennotthatdifferentthanonewouldfindinanMDschoolwith the exceptionof the additionalOsteopathicManipulativeMedicine(OMM)course.If it is justseenasamanipulationcourse,justamodalitytopulloutatcertaintimeswhenconvenient,thenwehavefailed.
Project100 that isbeingpromotedby theUnitedStatesBoneandJointDecadeorganizationisseekingtointegratesomelevelsofmusculoskeletalmedicinein100%oftheMDschools.Eveniftheyincludetraininginmanipulation,itwillnotbethesame.Itwillbemissingthecorecomponenttodrivethesuccess-fulapplication:theosteopathicphilosophy.SincethedaysoftheFlexnerreport,therehasbeengreatattentiontowardsfulfillingtherequirementsthatanMDschoolmustfulfill.ItwasforthisreasonthattheCollegeofOsteopathicPhysiciansandSurgeonswasabletobesoeasilyconvertedtoanon-osteopathiccollegeofmedicinein196�.Withmorethan�0schools,thereareasmanydifferentwaystoorganizethecurriculum.Itisalmostliketheoldstatementthatifthereweretwoosteopathsinatown,therewouldneedtobethreehospitals.Thereisa“homerule”phenomenonthatresultsinalackofconsistency.Thereneedstobeaparadigmshift.Inordertobecomeosteopathic,theyneedtofollowosteopathicstructureandfunctionintheircurriculardesign. Many of the schools have instituted Problem-BasedLearning(PBL)orothercurricularvariations.Theseprogramsaretypically“diseaseoriented”andhavelittletodowiththeosteopathicapproach.Often,theosteopathiccomponentislim-itedtothequestion“WhatOMTwouldweuse”attheendofamedicaldiscussiononetiology,pathophysiology,andtreatment.Thatdoesnotmakeitosteopathic.Generally,wearelookingatanacademicframeworkatmostschoolsthathasmoretodowithseparatesystemsthanitdoeswithtrueintegration.Thereislittleorno“BodyUnity”.WehavePhDs,MDs,aswellasDOswhoteachinourschoolswhoneverbringtheconceptsofosteopathicprinciplesandpracticeintotheirteachinginthelabo-ratorycourses,didacticcoursesandtheclinicalrotations.Atleastthenon-osteopathicpersonnelhavesomelevelofexcuse;theDOsdonot.Theydonotactasosteopathicrolemodelsforourstudents.Ourosteopathicstudentsandphysiciansseelessandlessdistinctionbetweenthemselvesandtheirnon-osteopathiccolleagues.36,37,38,39,40,41TheobviouscauseisthattheDOshave

March�006 The AAO Journal/17
becomemoreassimilatedintothepracticeof“routine”medi-cine.Bythefailureofnotbeingreinforcedinthebasictenetsofosteopathy,theschools,residencies,andspecialtycollegeshaveallowedtheslippageofphysiciansawayfromthefold.Thelastpost-graduateopportunity,theosteopathicinternship,4�,43,44,45,46isitselffallingaway.Inordertocombatthis,wemustrestructureandstrengthenthefoundation.Thesolutionisnotintechnology,generalist-to-specialistratios,distancelearning,researchoranyothermechanismoftheday.47Allofthosehaveimportanceastoolsforthesupportofwhatshouldbedone.
Wehaveseentheemphasisonprimarycare.Osteopathicphysiciansaremorefrequentlyprimarycarephysicians,butthatisnottheirexclusivepurview.Osteopathicphysiciansapparentlycommunicatewiththeirpatientsdifferently48,butthisiseasilyremediatedforotherphysicianpractitioners.Wehaveheardthatweare“Doctorstreatingpatients,notsymptoms.”IfIwasanMD,Iwouldbeinsultedandwouldreplytothiswith“HeyItreatpatientsandnotsymptoms,too!”IhavebeenfortunatetohavebeentaughtbyandworkedwithseveralexcellentMDswhorep-resentedourphilosophybetterthanmanyofourDOcolleagues.Thefactthatsomeonehasthefourthandfifteenthlettersaftertheirnamedoesnotmakethemosteopathic.Thesolutionisinareturntoosteopathy.TheprofessionmustundergoaparadigmshifttoWWDSD-“WhatWouldDr.StillDo?”ThegreatestgiftsthatIhavebeengivenbymymentorsandotherteachershavenotbeenosteopathicmanipulativetechniques.Withoutadoubt,theyhavetaughtmeagreatdealaboutthose.Instead,ithasbeenthewayinwhichIcanthinkaboutapersoninhealthandevendisease.TherearemanythingsthatIcandoroutinelythatjustseemtowork.However,wheneverIgetconfused,disrupted,orstoppedbyaclinicalsituation,Ireconfiguremythinkingtoapplytheosteopathicprinciples.Itisthesethatweneedtoreinforcewiththosewhoseektojoinourprofession.Weneedtofollowthedirectionsfromourfounderwhenhesaid,“Myobjectistomaketheosteopathaphilosopher…Iwanttoestablishinhismind,thecompassandsearchlightbywhichtotravelfromtheeffecttothecauseoftheabnormalityofthebody.”49
FollowingDr.Still’sdirectionsthat“Basicprinciplesmustatalltimesprecedeeachphilosophicalconclusion.”50,Iwouldliketotaketheopportunityofthisprivilegetospeakbeforeyoutorecommendatemplatethatcouldbeappliedeasilytoanyofthecurriculaofthecollegesofosteopathicmedicineaswellastomanyothersituations:Allacademiceventsshouldbeorganizedaccordingtoosteopathicprinciplesandphilosophy.51,5�,53,54,55,56,57Isay“all”butfeelthatifwecanaimforthestarsandthenreachthemoon,wewillstillaccomplishagreatdeal.Wewouldbeginwiththebasicprinciplesthatarefamiliartoallhere:
1. StructureandFunctionareinterrelated A. Normal 1) StructuregovernsFunction �) FunctionmodifiesStructure B. Abnormal 1) AbnormalStructureresultsinAbnormalFunction �) AbnormalFunctionresultsinAbnormalStructure
�. ThePerson(Body)isaUnit A. Interactionofdifferentsystems 1) Neurological
�) Dermatological 3) Musculoskeletal 4) Hematological 5) Cardiovascular 6) Pulmonary 7) Gastrointestinal 8) Genitourinary 9) Endocrine 10) Immunological 11) Behavioral/Psychological B. Mind,Body,Spiritconnections 1) Psychosomatics3. Thebodyhasaninherentabilitytoperform: A. Regulation 1) Normal • Maintainsystems �) Abnormal • Alteredregulation B. Adaptation 1) Normal • Reacttosmallalterationsinenvironments • External • Internal �) Abnormal (a) Pooradaptation (b) Inappropriatereaction C. Compensation 1) Toinherentordevelopedinadequacies (a) Normal • Congenital malformations • Genetic • Functional inadequacies (b) Abnormal • Overcompensation • Under-compensation • Maintenanceofadaptationpastusefulness D. Repair 1) Normal • Tissuerepair �) Abnormal (a) Scarformations (b) Adhesions E. Defense 1) Normal (a) Internalderangements (b) Externalinvasions �) Abnormal (a) Inappropriatereactiontoirritants (b) Recognitionofhostelementsas“enemy”4. Dysfunctionofthebody A. Istheinteractionofthe: 1) Host(person) �) Activatingevent (a) Endogenous (b) Exogenous B. Diseaseoccurswhenthebodyis 1) Overwhelmed �) Under-prepared
5. Rationaltreatmentisbasedontheaboveprinciples A. Treatmentdecisionisbasedonproper: 1) History

18/The AAO Journal March�006
�) Examination 3) Experience 4) Knowledge 5) Understanding B. Thefunctionofthephysicianisto: 1) Facilitatethebody’sinherentcapacities �) Minimizeeffectsofdisease (a) Endogenousalterations (b) Exogenousthreats C. Methods 1) Lifestyle (a) Environment (b) Diet (c) Exercise (d) Social/Familial (e) Habits �) OsteopathicMedicalInterventions 3) OsteopathicSurgicalInterventions 4) OsteopathicManipulativeTreatment
Theoverallcurriculumshouldfollowthisandeachindividualcoursewoulddolikewisebyhavingthecoursesgroupedtheoreti-cally:
ThePersonasawhole–theemphasisofosteopathicmedicineisonthehost
• Behavioralmedicine • OMM 1. StructureandFunctionareinterrelated–understanding
howthecomponentsarebuiltandwhattheydo;howthetwointeractandmodifyeachother
a. Structure • GrossAnatomy • Embryology • Histology • Neuroscience • Neurology • Cardiovascular • Pulmonary • Renal • Gastrointestinal b. Function • Biochemistry • Physiology • Endocrinology • ClinicalNutrition �. Thebodyhasaninherentabilityto: a. Defend,Heal,Compensate,Repair • Dermatology • Immunology/Allergy • Hematology 3. Diseaseoccurswhenthebodyis: a. Overwhelmed • Microbiology • Infectiousdisease • ClinicalToxicology b Underprepared • Genetics • Pathology 4. Rationaltreatmentfacilitatesalloftheaboveprocesses • OsteopathicManipulativeTreatment • Medicine • Cardiology • Pulmonary
• Gastroenterology • Nephrology • Neurology • Endocrinology • Pharmacology • FamilyPractice • Psychiatry • Surgery • General • Otorhinolaryngology • Orthopedics • Urology • Ophthalmology • Obstetrics/Gynecology • Pediatrics • Radiology
Therecouldberepetitionwithoutredundancy.Ateachlevel– Curricular,Year, Subject,Topic, and Lecture – the courseobjectivesandcomponentsshouldbeorganizedaccordingtotheosteopathicprinciples.Inotherwords,thestudentswouldbeexposedtotheseprinciplesoverandoveragainandnotjustintheOMMcourse.WhethertheprofessorsareaDO,anMD,oraPhD,theycouldbeorientedtostructuretheapproachofthelectureorthecoursetofollowtheframeworkofosteopathicprinciples.Oneofthegreatquestionsineducationis“Howdoyougetsomeonetothink?”Amongthemanysuggestionsarerepetitionandprovocationtoapplykeyconcepts.Insteadofbe-ingonlylecturesintheOMMcourse,thestudentswouldlearnanapproachthattheycouldutilizeeverydayoftheircareers.Dr. Still wrote that “Osteopathic physicians must be able togiveareasonforthetreatmenttheygive,notsomuchtothepatient,buttothemselves.”58Ratherthanseeingnodifferencebetweenthemselvesandothers,theosteopathicwaycouldbedemonstratedagainandagain.ThefollowingisanexamplethatisinnowayexhaustiveforaPulmonarycourse:
Pulmonaryconsiderations:
b. Thebodyisaunit: • Respirationdeliversoxygentothewholebody
throughdiffusionbythepumpingoftheheart • Theheartaswellasbloodvesselsare responsibleforthedelivery • Thelungsaffectbloodpressure(angiotensin) • TheprocessofbreathingiscontrolledbytheCNS • Theairpassagesbeginintheheadandneckand
extendtothechest • Respirationisanactionofthewholebody • ThePrimaryRespiratoryImpulseoftheCranial
mechanismaffectspulmonaryrespiratory function • Chemotacticaswellasothercentersexistinthe
braintoregulatebreathing c. Structureandfunctionareinter-related: • Thenasalpassagesandoralpharynxmoisturize
theair • Theringsofthetracheaprovidesupportand
protectionforastructurethatshouldremain

March�006 The AAO Journal/19
uncompressedbypositionornormalapplied pressures
• Themultiplebronchiolesandaveoliprovidea greatersurfaceareafordiffusionthanifasingle surfacewasadapted
• Theproximityofthecapillariesprovidesfor turnoverofCO
�andO
�
• Thefunctionofhemoglobininthereleaseof CO
�andabsorptionofO
�
• Thediaphragmactslikeabellowscreating negativepressurewithinthethoraciccavitythus drawinginair
• Theribsprovideaframeworkfortheactionof themusclesallowingforachangeindiameterof allplanesandtherebyincreasethevolume
• Thesecondarymusclesofrespirationassist inchangingthepositionoftheribsandalter
thevolume • Thecostalcartilageisflexibleandtwistsduring
inhalationanduntwistswhenthediaphragm relaxesandtheycontributetoexhalation
d. Thebodyhasaninherentabilitytodefend,heal, repair,andadapt:
• Thehairsinthenaresfilterparticulatematter • Someinfectingagentsandparticulatematter
iscapturedinmucousmixedwithsalivaand swallowedfordestructionintheacidofthe stomach
• Theciliaactasan“escalator”anddeliversome foreigncomponentsbacktotheorophayrnx
• Therearelargelymphnodesadjacenttoall bronchiwithmanyterminalandconducting lymphaticstructuresadjacenttoalllungtissue
• Thestructureschangebasedonaltitudewith expansionofchestcavityandadaptationto loweroxygenenvironments
• Thereisaphysiologicalswitchtoair componentswhentherehasbeendamage. NormalpeopleareCO
�dependentfortheir
drivetobreathewhilepatientswithemphysema areO
�dependent
e. Diseaseoccurswhenthebodyisoverwhelmed orunderprepared: • Weareexposedtomillionsifnotbillionsof
pathogenseachdayyetdon’tbecomeillunless ourimmunesystemsareatareducedcapacity
orunlessthepathogenisabletooverwhelmthe defenses
• Smokingimmobilizestheciliathatlinethe respiratorytract
• Tobaccoproductsincreasethelikelihoodof aberrantcellstoreplicate
• Allergicreactionsoccurbecauseofanover whelmingandoftentimesinappropriateimmune response
• Asthmaisacombinationandcascadeof reactionsincludingprecipitatingelements, bronchospasticreaction,andinflammatory response
f. Rationaltreatmentisbasedontheaboveprinciples (i.e.Asthma):
• Decreasetheworkandeffortofbreathing (i) provideoxygen (ii) relaxspasticmuscles (iii)removeribmotionrestrictions • Increasetheefficiencyofstructures (i) Beta-agonistmedications-increaseefficacy ofthemechanism (ii) Corticosteroids-facilitatereductionof inflammation (iii)Increaseexcursionofthediaphragm (iv)Stimulatesympatheticresponse (v) TreatC3,C4,&C5inthecervicalspine toremoverestrictionstothescalenesand thephrenicnerves (vi)Ribraising (vii)Treatthepelvicdiaphragmtoallowthe changesinabdominalcavitypressure changes • Encouragethedefensiveandadaptiveinherent mechanisms (i) Lymphatic - Thoracicpump - Hepaticpump - Splenicpump - Dalrymplepedalpump - Effleurage - Galbreathtechnique (i) Chestpercussion (ii) Vaccination -Influenza -Pneumoccocus • Provideinterventions (i) Removepossibleenvironmentaland otherirritants (ii) Usemastcellstabilizingmedications (iii)Preventlatephaseinflammatoryresponse withlowdoseinhaledandothersteroids (iv)Lifestylechanges - Exercise - Diet (v) Patienteducation Therearemanyresourcesthatcanbeused59.TheEduca-
tionalCouncilforOsteopathicPrinciples(ECOP)hasdevelopedaCoreCurriculumthatcontainsthebasicframework.ItwastheoriginaldocumentthatleadtothecreationoftheFoundations for Osteopathic Medicine textbookandmanyof thebrilliantmembersofourprofessionworkedonitscreation.ECOPhasalsocreatedtheCOILS,Clinically Osteopathically Integrated Learning Scenarios60asateachinginstrumentforpost-gradu-atetraining.AlthoughIconsiderittobeaflawedinstrument,theOsteopathicSOAPNoteisastepintherightdirectionofpresenting a framework for organized osteopathic thinking.Therearemanyotherresourceslocatedinarticles61andtext-books.6�,63,64Wecanrelyuponthegoodsenseandguidanceofourfounder,Dr.AndrewTaylorStill.45,46Someofthescience

�0/The AAO Journal March�006
ofoveronehundredyearshasreaffirmedhislegacytous.Theman-powerresourcescanbedrawnfromthemembersofECOP,themembersofthedepartmentsofOsteopathicManipulativeMedicine,theFAAOs,themembersoftheAAO,andultimately,anyosteopathicphysicianwhoholdsthephilosophyandprin-ciplescloseinmind,handandheart.Ifwecanaccomplishsomeprogressinthisregardwithintheschools,thenwecanextendtheconceptbeyondinawaythattrulydemonstratestheunique-nessofosteopathicmedicine.Quitepossibly,wemaynotneedtotransformourpost-graduateprogramssincethosetrainedintheabovedescribedmannercouldnaturallybringitabout.
Thefutureoftheprofessionisdependentonanumberof“WhatIfs?”Isittoomuchofaconceittohopethatwecanre-establishthebasicprinciplesintoallpartsofourprofession?WecancontinuetheevolutionofmedicinethatDr.Stillplannedbyfacilitatinganinstructionofosteopathyasitshouldbelearnedandpracticed.Perhapsitcouldmeetitsdestinybybecomingthepredominantsystemofmedicalcareinfivecenturies.
(ThesceneisfromStarTrekVoyagerandCaptainKath-rynJanewayislyingproneonatreatmenttableinherprivatequarterswhiletheEmergencyHolographicPhysicianistreatingher with manipulation for her headaches and other physicalcomplaints.)
HolographicDoctor:“Yourtrapeziusishardasarock.Youhaven’tbeenfollowingtherelaxationregimenIprescribedforyou.”
CaptainJaneway: “I’vebeentoobusy.”HolographicDoctor: “Theusualstory.Haveyoubeenget-
tingenoughsleep?”CaptainJaneway: “Moreorless.Mostlyless.”HolographicDoctor: “Andhaveyourheadachesbeenget-
tinganyworse?”CaptainJaneway: “No.They’renotgettinganybetter
either.They’relikehotneedlesdriv-ingintomyskull.”
HolographicDoctor: “Thesesymptomsarehardlysurpris-ing,Captain.Youworkabsurdlylonghours,underconstantstress,eatingontherun,withoutsufficientexerciseorrest.Yourbodyiscryingoutformercy.”
CaptainJaneway: “Itcertainlyisrightnow!Theremustbesomeeasierwaytodothis,Doctor.Ahypospraymaybe?”
HolographicDoctor: “Alwayslookingforthesimplefix.Sometimesthere’snosubstituteforintensiveosteopathicpressuretherapy…”65
IwouldliketothanktheBoardofTrusteesandthemembersoftheAmericanAcademyofOsteopathyfortheirselectionofmetogivethislecture.TherearesomanyotherindividualswhomIwouldalsoliketothank:myfamilyforthehelpandunderstand-inginallofmyactivities;mymentors,StanleySchiowitz,DO,FAAOandEileenDiGiovanna,DO,FAAOfortheirguidance;and the many professors, clinicians and students who havetaughtmealloftheseyears.,Ialsowouldliketospecifically
thankMichaelSeffinger,DOwhokindlysharedhisknowledgeandmaterialconcerningtheCaliforniaamalgamationaswellasdiscussingwithmetheconceptsofthislecture.Finally,Ioweagreatdealofappreciationtoallofthoseosteopathicphysi-cians,especiallyAndrewTaylorStill,whobytheireffortsandknowledgehavemadeitpossibleforustodoourlife’swork,thecareofpatients.Thankyouforyourkindattention.
References:1. JoyRJT.Thenaturalbonesetterswithspecialreferencetothe
SweetfamilyofRhodeIsland.Bulletin of Medicine.VolXXX-VIII.No5.Sep-Oct1954.
�. McPartlandMR.ThebonesetterSweetsofSouthCounty,RhodeIsland.Yankee.Jan1968.http://www.genealogy.com/us-ers/h/o/l/Rose-Sweet-Holladay/FILE/000�text.txt
3. LomaskM.AaronBurr:The Years from Princeton to Vice-Pres-ident 1756-1805.Farrar-Strauss-Giroux.NY.1979.
4. IchtS.Massage, Manipulation and Traction.RobertE.KriegerPublishingCompany.Huntington,NewYork.1976.pp14�-144.
5. BordleyJandHarveyAM.Two Centuries of American Medi-cine.W.B.SaundersCo.Philadelphia.1976.p10-36.
6. StillAT.Autobiography of A. T. StillinTruhlarREDoctor A.T. Still in the Living.Privatelypublishedbytheauthor.Cleveland.1950.
7. CowleyR.(Editor)What if?BerkelyPublishingGroup.NewYork.1999.
8. CowleyR.(Editor)What if?�ed.BerkelyPublishingGroup.NewYork.�001.
9. OberJ.Conquestdenied:theprematuredeathofAlexandertheGreatinCowley,R.(Editor)What if?BerkelyPublishingGroup.NewYork.1999.pp37-56.
10. McCulloughD.Whatthefogwrought:therevolution’sDunkirk.August1939.1776inCowleyR.(Editor)What if?BerkelyPublishingGroup.NewYork.1999.pp189-�00
11. FlemingT.Unlikelyvictory:ThirteenwaystheAmericanscouldhavelosttherevolutioninCowley,R.(Editor)What if?BerkelyPublishingGroup.NewYork.1999.155-186.
1�. HistoryChannel.13. WoodcroftB.The Pneumatics of Hero of Alexandria from the
Original Greek. TaylorWaltonandMaberly,London. 1851.http://www.history.rochester.edu/steam/hero/index.html
14. StillAT.Autobiography of A. T. Still. p76.15. StillAT.Autobiography of A. T. Still.pp63-65.16. WalterG.W.The First School of Osteopathic Medicine.The
ThomasJeffersonUniversityPress.Kirksville,Missouri.199�.p7.
17. WalterGW.The First School of Osteopathic Medicine.TheThomasJeffersonUniversityPress.Kirksville,Missouri.199�.p99.
18. DiGiovannaEL.An Encyclopedia of Osteopathy.AmericanAcademyofOsteopathy,Indiannapolis,Indiannna,�001,p�6
19. Kolata,G.Flu: The Story of the Great Influenza Pandemic of 1918 and the Search for the Virus that Caused It.Farra,StraussandGiroux,NewYork,1999.
�0. KohnGC(Ed.)Encyclopedia of Plague and Pestilence.FactsonFile.1995.305.
�1. IezzoniL.Influenza 1918: The Worst Epidemic in American History,TVBooks,NewYork,1999
��. HoehlingAA.The Great Epidemic,Little,BrownandCom-pany.Boston.1961.
�3. D’AlonzoGE,Jr.InfluenzaEpidemicorPandemic?TimetoRollUpSleeves,VaccinatePatients,andHoneOsteopathicManipulativeSkills. JAOA.Sep�004.104:370–371.
�4. TaskerE.E.Spanishinfluenza-whatandwhy?JAOA. 1919:19.

March�006 The AAO Journal/�1
�5. SmithRK.Onehundredthousandcasesofinfluenzawithadeathrateofone-fortiethofthatofficiallyreportedundercon-ventionalmedicaltreatment.JAOA.19�0:�0:17�-175.Reprint-edinJAOA.�000.100:3�0-3�3.
�6. KohnGC(Ed.)Encyclopedia of Plague and Pestilence,FactsonFile.1995.34�-43.
�7. WatsonJOandPercivalEN.PneumoniaresearchinchildrenatLosAngelesCountyHospital. JAOA. 39(3):153-159.
�8. MeaselJW,Jr.Theeffectofthelymphaticpumpontheimmuneresponse:I.Preliminarystudiesontheantibodyresponsetopneumococcalpolysaccharideassayedbybacterialagglutina-tionandpassivehemagglutination. JAOA.Sep198�.8�:�8.
�9. Jackson,KMSteele,TFDugan,EP,KukulkaG,BlueWandRobertsA.EffectoflymphaticandsplenicpumptechniquesontheantibodyresponsetohepatitisBvaccine:apilotstudy JAOA.Mar1998.98:155.
30. SleszynskiSLandKelsoA.Comparisonofthoracicmanipu-lationwithincentivespirometryinpreventingpostoperativeatelectasis. JAOA.1993:93:834-845.
31. GoodridgeJP.AHistoryofTheAmericanAcademyofOste-opathy.Unpublished.�001.
3�. AmericanAcademyofOsteopathy.33. DiGiovannaEL.An Encyclopedia of Osteopathy,American
AcademyofOsteopathy,Indiannapolis,Indiana.�001.p69.34. GevitzN.The DOs: Osteopathic Medicine in America – 2nd
Edition.TheJohnsHopkinsUniversitypress.Baltimore.�004.115-134.
35. SeffingerMA.Personalcommunication.36. AguwaMIandLiechtyDK.Professionalidentificationand
affiliationofthe199�graduateclassofthecollegesofosteo-pathicmedicine.JAOA.Aug1999.99:408-4�0.
37. SpaethDGandPheleyAM.UseofosteopathicmanipulativetreatmentbyOhioosteopathicphysiciansinvariousspecialties. JAOA.Jan�003.103:16-�6.
38. FryLJ.Preliminaryfindingsontheuseofosteopathicmanipu-lativetreatmentbyosteopathicphysicians. JAOA.Jun1996.96:91-96.
39. DPRusso,STStoll,andJHShores.DevelopmentoftheAttitudesTowardOsteopathicPrinciplesandPracticeScale(ATOPPS):preliminaryresults. JAOA.Sep�003.103:4�9-434.
40. ShlapentokhV;O’DonnellN,andGreyMB.Osteopathicin-terns’attitudestowardtheireducationandtraining.JAOA.Aug1991.91:786.
41. JohnsonSMandBordinatD.Professionalidentity:keytothefutureoftheosteopathicmedicalprofessionintheUnitedStates [letter]. JAOA.Jun1998.98:3�5.
4�. RodosJJ.LoyaltytotheprofessionnottheAOA:evidencebasenecessaryformembersupportofassociationpolicies[letter].JAOA.September�005.105:(9):4�6.
43. O’ConnorJJ.Bridgingperspectives,butregrettingdemiseofinternship[letter].JAOA.�004.104:365-366.
44. SmithAB.Evaluatingtherationaleoftheosteopathicintern-ship.June�004.JAOA.104(6):�30-�31.
45. ClarkRC.Osteopathicmedicaltraining:developingtheseasonedosteopathicphysicianJAOA.November�004.104:(11):45�-455.
46. NooneSJ.Theerosionofosteopathicidentity,American Acad-emy of Osteopathy Newsletter.October�005.p�.
47. Ross-LeeB,KissLE,andWeisserMA.Anosteopathicpre-scriptionformedicaleducationreform:part�.Specialtymixandcommunityintegration.JAOA.Aug1997.97:463-468.
48. CareyTS,MotykaTM,GarrettJM,andKellerRB.Doosteo-pathicphysiciansdifferinpatientinteractionfromallopathicphysicians?Anempiricallyderivedapproach.JAOA. Jul�003.103:313–318.
49. TruhlarRE.Doctor A. T. Still in the Living.PrivatelyPublished.Cleveland,Ohio.1950.p117.
50. TruhlarRE.Doctor A. T. Still in the Living,PrivatelyPublished,Cleveland,Ohio.1950.p117.
51. StillAT.The Philosophy of Osteopathy.Kirksville,Missouri.1899.
5�. StillAT.The Philosophy and Mechanical Principles of Oste-opathy.Hudson-KimberlyPub.CO.KansasCity,Missouri.190�.
53. LittlejohnJM.Theprincipleofosteopathy.JAOA.7:(6):�37-�46reprintedinJAOA. Mar�000.100:191-�00.
54. PetersonB.AcompilationofthethoughtsofGeorgeW.Nor-thup,DO,onthephilosophyofosteopathicmedicine.JAOA.Jan1998.98:53-57
55. SeffingerMA,KingHH,WardRC,JonesJM,RogersFJ,andPattersonMM.OsteopathicphilosophyinWardRC(Ed.)Foundations for Osteopathic Medicine,(�ndEd),Lippincott,Williams&Wilkins.Philadelphia.�003,pp3-18.
56. HuletGD.A Text Book of the Principles of Osteopathy,5thEdi-tion.Pasadena,California.A.T.StillResearchInstitute.19��.
57. DowlingDJandMartinkeDJ.ThephilosophyofosteopathicmedicineinDiGiovannaE,SchiowitzS,andDowling,DJ.Eds.,An Osteopathic Approach to Diagnosis and Treatment, 3rdEdition.LippincottWilliams&Wilkins.Philadelphia.�004.10-15.
58. TruhlarRE.Doctor A. T. Still in the Living.PrivatelyPublished.Cleveland,Ohio.1950.p11�.
59. GloverJC.Wheredowegofromhere?The AAO JournalMarch�005.15(1):11-15
60. ECOP.Clinically Osteopathically Integrated Learning Sce-narios.TheAmericanAssociationofCollegesofOsteopathicMedicine.�001.
61. RogersFJ.Themusclehypothesis:amodelofchronicheartfailureappropriateforosteopathicmedicine.JAOA.Oct�001.101:576–583
6�. KucheraMLandKucheraWA.Osteopathic Considerations in Systemic Dysfunction–Revised�ndEdition.GreydenPress.Columbus,Ohio.1994.
63. WardRC.(Ed.)Foundations for Osteopathic Medicine (2nd Ed).Lippincott,Williams&Wilkins.Philadelphia.�003.
64. DiGiovannaE.SchiowitzS,andDowlingDJ,Eds.An Os-teopathic Approach to Diagnosis and Treatment,3rdEdition.Lippincott,Williams&Wilkins.Philadelphia.�004.
65. StarTrekVoyager.“ScientificMethod”.October�9th.1997.❒
Accepted for publication: October 2005
Address correspondence to:DennisJ.Dowling,DO,FAAOOMMAssociates,PC575UnderhillBlvd.,Suite1�6Syosset,NY11791E-Mail:[email protected]

��/The AAO Journal March�006
April 21-23, 2006NeuroFascial Release Course EastPhoenix,AZContact: SteveDavidson,DO 800/359-777�
May 4-7, 2006109th Annual ConventionIndianaOsteopathicAssociationCME:30+Category1A(anticipated)HyattRegencyIndianapolis,INContact: IOA 317/9�6-3009or 800/94�-0501
Component Societies’ CME Calendar and other Osteopathic Affiliated Organizations
May 4-7, 200651st Annual ConferenceFloridaAcademyofOsteopathyOrlando,FLCME:��Category1A(anticipated)Contact:KennethWebster,EdD phone:7�7/581-9069 fax:7�7/581-8537 E-mail:[email protected]
June 17-21, 2006Basic CourseTheCranialAcademyFoundersInnVirginiaBeach,VACME:40Category1A(anticipated)Contact: TheCranialAcademy 317/594-0411
OklahomaStateUniversityCenter forHealthSciences,CollegeofOsteopathicMedicineisseekingtofillafull-time,non-tenure(clinical)or tenure-trackfacultypositionin theDepartmentofOMM.ThispositionisactivelyinvolvedinpatientcareandteachingmedicalstudentsandresidentsatCollegeambulatoryclinics,aswellasthehospitalinpatientservice.AppropriateeffortandactivityinclinicalresearchandservicewillalsobenecessaryaswellasaclinicalrecordofsufficientdepthtoqualifyforfacultyappointmentattherankofAssistantorAssociateProfessor.RequiresaD.O.degree,eligibilityforlicensureinthestateofOklahoma,Boardeli-gibilityandadevotedinterestineducation.Preferresidencyand/orfellowshiptrainingandteachingexperience.Competi-tivesalarywithexcellentfringebenefits.Applicationswillbereviewedasreceived;openuntilfilled.Mustapplyonlineat:https://jobs.okstate.edu,searchHealthSciencescampus.OSUisanaffirmativeaction/equalopportunityemployer.
Assistant/Associate ProfessorDepartment of Osteopathic
Manipulative Medicine
June 22-24, 2006AACOM’s 2006 Annual MeetingChallenges and OpportunitiesRenaissanceHarborplaceHotelBaltimore,MDContact:AACOM 301/968-4143
June 22-25, 2006Annual Conference – “Bent Twigs: Pediatric Osteopathy and Beyond”TheCranialAcademyFoundersInnVirginiaBeach,VACME:40Category1A(anticipated)Contact: TheCranialAcademy 317/594-0411

March�006 The AAO Journal/�3
➝
AbstractBackground
4.4to6.�percentoftheadultpopula-tionhasaphysicianconfirmeddiagnosisof asthma. Physicians use pulmonaryfunctionalteststoaccuratelyassessandreproducethepulmonaryfunctionalstateofanasthmaticornon-asthmaticpatient.Myofascialtriggerpointsinvariouspartsof the body have been documented tohavephysiologicaleffectsontheorgansofthebody.
ObjectiveA myofascial trigger point on the
skullwas identifiedandtreatedinninepatientswithanacuteasthmaticexacer-bationandwhowereatthetimerefrac-torytostandardrescuetreatments.
MethodsA Peak Flow Meter was used to
determine peak flow. These measure-mentswereobtainedafter theuseof arescueinhalerornebulizerbutbeforetheexperimental treatment.A trigger-pointwasfoundattheleftparietaleminenceontheskullinpatients.Thetrigger-pointwastreatedusingdirectpressure,andthescalp was folded around the point.Anadditional measurement was obtainedapproximately three minutes after thetreatmentwasapplied.
ResultsThe percent change in peak flow
for patients classified as mild variedfrom8�%to89%.For themoderatelyinvolved, thepercent changewas5�%to87%.Onlyonepatientwasclassifiedassevereandtheincreasewasapproxi-mately53%.Asignificantchangeinpeakflowwasseenwith thepatients treatedwiththeosteopathicmanipulativetreat-menttechniquedescribed(p<0.0003).
A myofascial trigger point on the skull: Treatment improves peak flow values in acute asthma patientsWm. Thomas Crow and David Kasper
ConclusionWhile the retrospective study
showed interest ing and dramat-ic results, further study is needed.
KeywordsAsthmaMyofascialtriggerpointsOsteopathicManipulation
Abbreviations(FEV1) forcedexpiratoryvolumein
onesecond(PEFR) peakexpiratoryflowrates
IntroductionInEuropeandtheUnitedStates4.4
to 6.� percent of the adult populationhave a physician confirmed diagnosisof asthma.1, �Asthma cost nearly $500milliondollarsinemergencydepartmentvisits in 1994, according to the mostrecentdataavailable.3
Physiciansusepulmonaryfunctionalteststoassessthepulmonaryfunctionalstate of an asthmatic or non-asthmaticpatient. Data from these pulmonaryfunction tests can quantify the diseaseseverity,assessandmonitorthediseaseprogression, and lastly determine thepatient’s appropriate future course oftreatment.4
Peak flow meters are increasinglybeing used to objectively measure theseverityofairflowobstruction.Currently,the“goldstandard”parameterinscreen-
ing patients for airflow obstruction isforcedexpiratoryvolumeinonesecond(FEV1).However,physiciansareusingpeak expiratory flow rates (PEFR) viapeakflowmetersasanacceptablealter-nativescreeningtoolinidentifyingandmanagingtheirasthmaticpatients.5PEFRis an easily reproducible measurementwithpredictednormalvaluescalculatedbasedonheight,age,andsexwithnodif-ferencesamongracialgroups.5,6Byusingpeakflowmeterstomonitorthediseasecourseandassessingtheresponsetomed-ications, early intervention can reducetheriskofhospitalization.7-10Overall,theincreasinguseinthepeakflowmeterisdue to itsportability, simplicity inuse,economicvalueandoverallpracticalityintestinglungfunction.5,6
PEFRisnowacceptedastheleastinvasive measurement in measuringairway obstruction.Three attempts arerecordedtakingthebestofthethreere-cordings.6,11-13Measurementscanbecor-relatedtoseverityofexacerbation(Table1).Regardingblowingintothepeakflowmeter, someauthors concludewith themagnitudeandorderoftheblowstherewasnosystematicrelationshipnortrendbetweenthosetwovariablessincesomepatientsimproved,whileothersdeterio-ratedduringtheirthreeattempts.11
Amyofascialtriggerpointhasbeendefinedasalocalized,hyperirritablespotinapalpabletautbandofskeletalmusclefiber.14 The clinical characteristics of
PEFCOMPARISONS
PEF Condition
<50%predictedvalueorpersonalbest SevereExacerbation
50%-80%ofpredictedorpersonalbest ModerateExacerbation
>80%predictedorpersonalbest MildExacerbation
Table 18

�4/The AAO Journal March�006
a myofascial trigger point include: (a)localized tenderness in a taut band ofmuscle; (b) a local twitch response tocross-fiberstimulationofthetautband;(c)paintodeeppalpationthatisrecog-nizedaspain;(d)andautonomicdysfunc-tion.Travell and Simons proposed anintegratedworkinghypothesistoexplaintheunderlyingpathophysiologyassoci-atedwithmyofascialtriggerpoints.15Inshort, the theory states that injury canleadtomotorendplateirritability,whichmaycausefrequentlocaldepolarizationsofthemusclefibers,resultinginanener-gycrisiswitharelativelossofsufficientquantitiesofhigh-energyphosphatestoallow the calcium-dependent lengthen-ing of the myofibril unit.This in turncanleadtodecreasedcapillaryflowintothe muscle secondary to the increasedmuscletension,loweringofthelocalpH,andreleaseofsensitizingsubstancesintothemuscle thatcancauseactivationofmusclenociceptorsandpain.16
Referredpainfrommyofascialtrig-gerpointscanmimicvisceralpainsyn-dromesandvisceralpainsyndromescaninducemyofascialtriggerpointdevelop-mentandmyofascialpainanddysfunc-tion.14,15AnexampleofthismyofascialtriggerpointmimickingvisceralpainwasreportedbyTravellandSimons. In theanteriorchestwallintherightpectoralisminor,a triggerpointcancausesupra-ventriculartachycardiaaswellasothercardiac pain.Triggerpoints have beenknowntocauseormimicchronicpelvicpain, interstitial cystitis, prostatodynia,andirritativevoidingsymptomsaswellaschronicabdominalpain.14,15,17-�3
MethodsThis retrospective study involved
thecollectionorstudyofexistingdata,documents, and charts recorded by
the investigator in such a manner thatsubjects cannot be identified, directlyorthroughidentifierslinkedtothesub-jectsandisexemptfromIRBapprovalunderFederalRegulation.[15C.F.R.§�7.101(b)(4)]
SubjectsAllninepatients(age16to55years)
had a prior history and diagnosis ofasthma.Theyhadexperiencedanacuteasthmaticexacerbationandhadusedthestandardinhalerornebulizer.Theyself-referredtoanofficewhentheyfelttheyhadlessthanthedesiredresultsfromthestandardrescuetreatment.Patientswereseenfromonetothreehoursaftertheirstandard treatment.The patients wereclassifiedastoseverityoftheasthmaticepisodefollowingthestandardtreatmentofinhalersand/ornebulizerbyuseofthepublishedguidelinesforpeakexpiratoryflow.8
MeasurementsAmodelHS710PeakFlowMeter
(Respironics HealthScanAsthma &Allergy Products, Cedar Grove, NewJersey)wasusedtodeterminethepeakflow.Thiswasaccomplishedbyhavingthepatientexhaleintoamouthpieceat-tachedtotheFlowMeter.Theexhalationwasrepeatedthreetimeswiththehigh-est value accepted as the score.Thesemeasurements were obtained after theuseofarescueinhalerornebulizerbutbeforetheexperimentaltreatment.Oneadditional measurement was obtainedapproximately three minutes after theexperimentaltreatment.
TreatmentA trigger-point was found at the
leftparietaleminenceontheskullinthepatients.
The trigger-point was treated us-ing direct pressure and folding thescalparoundthepoint.Whilesimilartocounterstrain,thetriggerpointwasheldforapproximately45secondsnot90to1�0secondssuggestedforcounterstraintechniques.
ResultsThe number of patients classified
as mild, moderate or severe is showninTable �.Additionally,Table � pro-videstherawdataforboththepre-andpost-experimentaltreatmentPeakFlowvaluesforeachofthenineindividuals.Theweightandageofthepatientswereremoved from the table due to HIPPArequirements.
The percent change in peak flowfor patients classified as mild variedfrom 8�% to89%.For themoderatelyinvolved, thepercent changewas5�%to 87%. In this report, there was onlyasinglepatientclassifiedassevereandthe increase was approximately 53%.Thus,overall,mostpatientsdidshowanimprovement.
Thepre-experimentaltreatmentandpost-experimentaltreatmentvaluesofthePeakFlowMeterforeachsubjectwereanalyzedusingamatch-pair t-test.APvalue of 0.05 or less was accepted assignificant.Infact,asignificantimprove-mentinpeakflowwasdeterminedwhenthedatawereanalyzed(p<0.0003).
DiscussionWhiletheretrospectivestudyshowed
interestinganddramaticresults,furtherstudyisneeded.Theneurologicalbasisforthechangecannotbedirectlyinferredfrom any of the data. One etiology ofasthmaisbelievedtobeanoverstimu-lation of the parasympathetic nervoussystem.Itisinterestingtospeculatethat
IDENTIFIER PrePEF(L/min) PostPEF(L/min) %ChangeofPre/Post SEVERITY %PrePEFtoNormal %PostPEFtoNormal
1 450 550 81.8�% Mild 83.06% 101.51%
� 550 6�0 88.71% Mild 96.09% 108.3�%
4 550 670 8�.09% Mild 96.09% 117.05%
9 �60 500 5�.00% Moderate 50.98% 98.04%
8 �75 350 78.57% Moderate 53.9�% 68.63%
6 3�5 375 86.67% Moderate 57.0�% 65.79%
7 300 450 66.67% Moderate 58.8�% 88.�4%
3 350 550 63.64% Moderate 61.15% 96.09%
5 ��5 4�5 5�.94% Severe 37.96% 71.69%
Table 2: Patient Data

March�006 The AAO Journal/�5
this myofascial trigger point treatmentmayhaveimpactedtheparasympatheticnervoussystemandreducedtheactivitythus improving respiratory function asdemonstrated by the increase in peakflow.
ConclusionFurther study is needed in a pro-
spective, double-blinded study to seeif thesefindingsare supported in largescaletrial.
AcknowledgmentPeggyStewartforherhelpwiththe
statisticalanalysisandotherhelp.
References1. HahnDandBeasleyJ.Diagnosed
andpossibleundiagnosedasthma:aWisconsinResearchNetwork(WReN)study.Journal of Family Practice.1994:38:373-9.
�. HedmanJ,KaprioJ,PoussaT,andNieminenM.Prevalenceofasthma,aspirinintolerancenasalpolyposisandchronicobstructivepulmonarydiseaseinapopulationbasedstudy.International Journal of Epidemiology.1999:�8:717-55.
3. WeissK,SullivanS,andLyttleC.TrendsinthecostofillnessforasthmaintheUnitedStates1985-1994.Jour-nal of Allergy and Clinical Immunol-ogy. �000:106:493-9.
4. GoldW.Pulmonary Function Testing, 3rded.Philadelphia.WBSaunders.�000.
5. D’SouzaW,CraneJ,andBeasleyR.Self-management plans.�nded.Lon-don.WBSaunders.�001.
6. RamirezNandLockeyR.Manage-ment of acute asthma in the office set-ting.1sted.Philadelphia.ACP.�00�.
7. BannerA,ShahR,andAddingtonW.Rapidpredictionofneedforhospi-talizationinacuteasthma. JAMA.1976:�35:1337-38.
8. KimmelS.Useofthepeakflowmeterinofficepractice. Am Fam Physician. 1986:34:107-11.
9. PlymatKandBunnC.Monitoringasthmawithamini-Wrightpeakflow-meter.Nurse Pract.1985:10:�5-7,47.
10. WilliamsM.Expiratoryflowrates:theirroleinasthmatherapy.Hosp Pract.198�:17:95-110.
11. DahlqvistM,EisenE,WegmanD,andKriebelD.Reproducibilityofpeakexpiratoryflowmeasurements.Occup Med.1993:8:�95-30�.
1�. BrownLandSlyM.Comparison
ofmini-WrightandstandardWrightpeakflowmeters.Annals of Allergy.1980:45:7�-4.
13. OwnbyD,AbarzuaJ,andAndersonJ.Attemptingtopredicthospitaladmissioninacuteasthma.AJDC. 1984:138:106�-66.
14. TravellJandSimonsD. Myofascial Pain and Dysfunction: The Myofascial trigger point Manual.Baltimore.Wil-liamsandWilkins.1983:1.
15. TravellJGandSimonsDG.Myofascial Pain and Dysfunction: The Myofascial trigger point Manual.Baltimore.Wil-liamsandWilkins.199�:�.
16. AudetteJF,WangF,andSmithH.Bi-lateralactivationofmotorunitpoten-tialswithunilateralneedlestimulationofactivemyofascialmyofascialtriggerpoints.American Journal of Physical Medicine & Rehabilitation.83(5):368-74,389.�004.
17. SimonsDG.Cardiologyandmyofas-cialmyofascialtriggerpoints.JanetG.Travell’scontribution.Texas Heart Institute Journal.30(1):3-7.�003.
18. TravellJandRinzlerSH.Reliefofcardiacpainbylocalblockofsomatictriggerareas.Proc Soc Exp Biol Med. 1946:63:480-�.
19. FitzGeraldMPandKotarinosR.Rehabilitationoftheshortpelvicfloor.I:Backgroundandpatientevaluation.International Urogynecology Journal.14(4):�61-8.�003.
�0. CimenA,CelikM,andErdineS.Myo-fascialpainsyndromeinthedifferen-tialdiagnosisofchronicabdominalpain.Agri Dergisi.16(3):45-7.�004.
�1 Doggweiler-WiygulRandWiygulJP.Interstitialcystitis,pelvicpain,andtherelationshiptomyofascialpainanddysfunction:areportonfourpatients.World Journal of Urology.�0(5):310-4.�00�.
��. WeissJM.Pelvicfloormyofascialmyofascialtriggerpoints:manualtherapyforinterstitialcystitisandtheurgency-frequencysyndrome.Journal of Urology.166(6):���6-31.�001.
�3. Doggweiler-WiygulR.Urologicmyo-fascialpainsyndromes. Current Pain & Headache Reports.8(6):445-51.�004.❒
Accepted for Publication: Dec. 2005
Address correspondence to:EastOrlandoOsteopathicNMM/FPResidency7975LakeUnderhillRoad,Ste�10Orlando,FL3�8��E-Mail:[email protected]
AAO Bookstore Offers Second Edition
Coding ResourceActing on a recommendation from the
Publications Committee, the Board of Trust-ees has approved the addition of a new publication to the Academy’s inventory of resources on osteopathic medicine. The AAO is now the exclusive distributor of this publication within the osteopathic medical profession.
Douglas J. Jorgensen, DO, CPC and his brother, Raymond T. Jorgensen, MS, CPC are certified professional coders and the au-thors of A Physician’s Guide to Billing and Coding Second Edition. In the foreword, the authors state: “The book provides a direct approach to utilize the best evaluation and management (E&M) recommendations to date, on a conservative basis, while staying within the federal guidelines…Optimizing reimbursement means better capture of the money you deserve, which translates into an excellent return on time invested with more bonuses and/or gain at the year-end.”
“Recalling medical school days…Re-member the Kreb’s Cycle and the Loop of Henle, not to mention the array of nerves, arteries and vein’s? If you could learn those intricacies, then you can certainly learn a few simple coding rules and techniques…” You can place your order now with the Acad-emy. Order AAO Catalogue #PR3000. Price: $25.00 + $6.00 shipping/handling. This is one small purchase that should quickly com-pound your investment many times over.
Name______________________________
Street_____________________________(NOP.O.Box#s)
City_______________________________
State___________Zip________________
DaytimePhone______________________PaymentInformation:❒ VISA❒ MC❒ CHECK
____ @$31.00each(includesU.S.S/H-Forinternationalshippingrates,pleasecalltheAAOoffice)
____ Chargemycreditcard
____________Total$amountoforder
CardNo.___________________________
ExpirationDate______________________
Signature___________________________
Foryourcopies,contact:American Academy of Osteopathy®
3500DePauwBlvd.,Suite1080Indianapolis,IN46�68
phone:(317)879-1881•Fax:(317)879-0563ororderonline:www.academyofosteopathy.org

�6/The AAO Journal March�006
Asthma Protocol – Acute Exacerbation – Intercostal Rib Technique
A.Standardpharmacologictherapyshouldbeinprogress.
B.Explaintothepatientthatyouaregoingtouseatechniquethatmayhelptherespiratorymusclesrelaxsothattheycanworkbetterandbreatheeasier.
C.Thepatientshouldbeseatedeitheratthefootoforonthesideofatreatmenttable(gurney).
D. Thephysicianstandsperpendicularto,andfacingtowardtheleftsideofthepatient.
l. Thephysicianplacesthefingerpadsofthefourdigitsofonehandovertheintercostalmusclesbetweenthefirstfourribsandaboveribfiveanteri-orlynearthesternalborder.
�. Posteriorly,thephysicianplacesthefingerpadsofthefourdigitsofthephysician’sotherhandoverthecorrespondingintercostalspaces(levels1to4)betweenthetransverseprocessesoftheverte-braeandtheangleoftheribs.
3. Physician’supperarmsareclosetothephysician’sribs.
Note: the physician’s posterior handshouldbehigherthantheanteriorhandbasedontheanatomicalstructureoftherib,posteriorribsarehigherthananteriorribsatthesameintercostallevel.
4. Thephysiciannextexertsamild/moderate compressive pressure(deeppalpation)with thefingerpads, to the intercostalmuscles,directed in an anterior/posteriordirectiondowntothelevelofthefascia. (Theamountofpressurewilldependonthedegreeofspas-ticityintheintercostalmuscles).
5. Treatmentisdonewithoutregardtoinhalation/exhalation
Intercostal rib releaseClaudia L. McCarty
phase.6. Whilecontinuingtoholdthe
compressivepressureontheintercostalmuscles,thephy-sician’sfingerpadsaredrawnlaterallytowardthephysician,justuntiltaut.
7. Thisposition(inwardandlateral)ishelduntilarelease(changeintissuetextureand/ortension)isfeltundertheexaminer’sfingers.Thetissuechangemaystartwithsomeellipticalmovement/sensationsunderthephysician’sfingerpadsandfinishwithrelaxationoftheintercostalmusclesandachangeinchestexcursion.
8. Thisprocedureshouldtakeap-proximatelyone-and-a-halftotwominutesatthislevel.
9. Thephysicianthenchangeshandplacementbyslowlyreleasingtheanterior/posteriorpressureandallowingthetissuetomovemediallyawayfromtheoriginaltautposition.
10. Thephysician’sfingerpadsarethenrelocatedtoalowerposi-tionandplacedontheintercos-talmusclesbetweenribs4-5,5-6,6-7,7-8,againnearthecostalmarginsanteriorlyandbetweenthetransverseprocessesandribanglesposteriorly.
Ifnecessary,placementandcorrespond-ingpositionmaybeevaluatedbyplacingonefingeronaribposteriorlyandmovingtheribanterior/posteriorly,checkingformotionatthesamelevelontheanteriorsurface.
11. Physician’supperarmsareclosetothephysician’sribs.
1�. Thephysiciannowexertsamild/moderatecompressivepressure(deeppalpation)totheintercostalmuscles,directedinananterior/posteriordirectiontothelevelofthefascia.The
amountofpressuredependsonthedegreeofspasticityintheintercostalmuscles.
13. Treatmentisdonewithoutregardtoinhalation/exhalationphase.
14. Whilecontinuingtoholdthecompressive(inward)pressureontheintercostalmuscles,thefingerpadsarethendrawnlater-allytowardthephysician,untiljusttaut.
15. Thispositionishelduntilarelease(changeintissuetextureand/ortension)isfeltbeneaththeexaminer’sfingers.Thismaystartwithsomeellipticalmovement/sensationsunderthephysician’sfingerpadsandendinrelaxationoftheintercostalmuscles.
Again, this procedure should take ap-proximatelyone-halftotwominutesatthislevel.
16. Thephysicianthenreleasesthehandplacementbyslowlyreleasingtheanterior/posteriorcompressivepressureandallow-ingthetissuetoslowlymovemediallyawayfromtheoriginaltautposition.
17. Movingtotheoppositesideofthepatient,thephysicianrepeatstheprocedure.
During an acute episode, it may benecessary to repeat the treatment witheachnebulizertreatment,dependingonthe severityof theexacerbation.Treat-mentmaybestoppedormodifiedatanytime.
Note:Duringanacuteexacerbation,theC
�dysfunction,whichisareflectionof
vagalstimulationshouldNOTbetreated.TreatmentofC
�duringanacuteattack
mayoverstimulatethevagusnerveandworsenbronchospasm.

March�006 The AAO Journal/�7
Theintercostalribreleaseprocedureis performed in a similar manner forthe chronic asthmatic patient. In thechronicpatient,treatmentmaybedonein either the seated or supine position.Treatment position will be determinedbythepatient’sasthmastatusatthetimeoftreatment.Additionally,inthechronicpatient,thephysicianmustaddresstheC
�
dysfunction, any thoracic dysfunctionsT
1-6,releasethediaphragmT
11-L
�,and
addresstheextensiondysfunctionofthecranium.Lymphaticdrainageshouldalsobe encouraged.The chronic asthmaticpatientistreatedatweeklysessionsuntilmedicationuseandfrequencyofexacer-bationsarediminished.Itmaybeneces-sarytotreatthepatientmorefrequentlyduringenvironmentalasthmaperiods.
This technique incorporates proper-tiesoffascial-ligamentousrelease(FLR),balancedligamentoustension(BLT)andfacilitated positional release (FPR).Afulcrumisestablishedbetweenthephysi-cianandthepatientinthepositioningoftheforearmsandfingerpads,asin(FLR).A facilitating force or compression isapplied between the two hands (FPR).Drawingthe tissue laterally toward thephysician and awaiting the release in-corporatesBLT.Thetensionisbalancedwiththatofthedegreeofspasmwithinthetissuesbeingtreated.Deeppressurepalpationplaysarole in this techniqueaswell.
Chila remindsus that, “Inperform-ing manipulative procedures, the bodyresponds comprehensively to an exter-nally applied force. From the momentofcontactwiththeskin,avenuesfortheimplementationofvariationsofforceareprovidedbypalpatoryclues.Thebody’scovering,theskin,mayberegardedasamassadrenergicmediumthatisusefulinthefacilitationandamplificationofpro-prioceptiveinterchangebetweenuniquepersons, the patient and the physician.Thesustainedeffectiveresponsefollow-ingtreatmentiscontingentonselectiveandcontrolledvariationofforcefromanappropriatefulcrum.
Whentheseconditionsaremet,inher-entneuroregulatorymechanismsactingin accordance with the capacity of thepatient will facilitate the resolution ofthe dysfunction. Generally speaking,thebody’sconnectivetissuesareundersomedegreeofloadandextension.The
increase and subsequent reversal ofextension produces a degree of tissueresponselessthantherelativelyunloadedstate.Thisphenomenonisreferredtoashysteresis.1Hysteresisistheoccurrenceofsomeflowanddissipationofenergythroughouttheloadedtissue.Hysteresisoccurs less with successive cycles ofextension, indicating stabilization ofresponse.Connectivetissuesundersus-tainedloadwillextendinresponsetotheload.Thiscontinuedextensionisreferredtoas“creep.”Animposedconstantloadwillresultin“relaxation”astheextensionremainsconstant.”1
RationalePossibleexplanationsfortheefficacy
of this treatment includethefascialre-leaseofboththeinternalandexternalin-tercostalmuscles.Sincefasciaenvelopsandcovers themuscles,decreasing theoverlyingtensionwouldlikelyincreasechestexcursion.Themusclesthemselveswouldrespondtothefacilitatingpressureofinwardcompression,deeppalpationorinhibition.The internal intercostals aremusclesof exhalation,which arequietin normal breathing. During an acuteexacerbation of asthma, exhalation isrestricted secondary to bronchospasmandairwayinflammation.
Inasthma,airwayobstructionisdueto(1)profoundconstrictionofthesmallerairwaysbyallergy-inducedspasmofthesmoothmuscleinwallsoftheseairways;(�) plugging of the airways by excesssecretionsofaverythickmucusand(3)thickeningofthewallsoftheairwaysdueto inflammationandhistamine inducededema.�
Itispossiblethattheefficacyoftheproposedtreatmentmayoccurasaresultofdecreasingtheworkofbreathingbyimproving compliance and decreas-ing airway resistance.Compliance is ameasureofthemagnitudeofchangeinlung volume accomplished by a givenchangeinthetransmuralpressuregradi-ent.Changesinthoracicdimensionsarealways accompanied by correspondingchangesinlungdimension.
The primary determinant of airwayresistanceistheradiusoftheconductingairways.Airway resistance is affectedby sympathetic and parasympatheticstimulationofairwaycaliberinresponsetoventilationandperfusion.�
Chila1suggestedinFoundations,theinherent neuroregulatory mechanismsacting in accordance with the capacityof the patient facilitates the resolutionof the dysfunction. Kuchera mentionsthatincreasingtheexcursionofthechestby1cmwillincreasethevolumeofairexchangedby�00cc.3Airhungerandairtrappingcouldbesignificantlyreducedby intercostal muscle relaxation anddecreasedfascialtension.
As discussed earlier, the work ofbreathing during an exacerbation ofasthma, requires a significant increasein total body energy expenditure.� Re-ducing this workload should allow thepatient’s inherentability tore-establishhomeostasis.
Comparison of techniquesTheproposedtechniquesharessome
similaritieswithothertechniquesfoundinreviewingboththeosteopathiclitera-tureandosteopathictextbooks.
Hoag notes that manipulative tech-niquesdiffer for the acute and chronicattack, and that it might be necessaryto treatanacuteattackseatedorsemi-reclining. He proposed that manipula-tion should be directed to the thoracicspine.4
DiGiovanna5describeshowthework-loadofbreathingshouldbereducedandadditionallyrecommendstreatmentinthechronicpatientaswell.5
PaulandBuser6treatedtheacuteasth-matic in theEDusingaseatedposturefor rib raising and respiratory motionaugmentation.Treatment of the uppercervicalunitwasavoided.
Purse7 sometimes used a modifiedseatedtechniquewiththepatient’sbacktotheoperatorwithhandsspreadaroundthe thorax, pressure was then applieddownward&caudallywithexhalation.
Belcastro8etal,usedanintercostalre-lease,whichwasdescribedas“eachhandbeingplacedlaterallyonthemiddleandlowerthoraciccage.Arhythmiccaudadmotion contributes to the stretching ofintercostalmuscles.”
Wilsonin1946notedthat“I like toset my patient up at the end of thesemanipulationsandplacemyfingersoverthefirstribsandmythumbsbetweenthetransverseprocesses4thand5th thoracicvertebrae. In this position I use direct
➝

�8/The AAO Journal March�006
pressurethroughthethumbsandfingersforabouttwominutes.Thispressurealoneinanacuteepisodeisofteneffective.”9
Rowane and Rowane10 also use aseated posture, with the patient facingawayfromtheoperator.Treatmentwasdirected toT
l-T
6, especiallyon the left
fornormalizationofthesympatheticin-nervationofthelungs.
SimilaritiesarenotedwithSutherland,RowaneandRowane,10PaulandBuser6and Wilson techniques that have thepatientseated.BoththeBelcastroetal8and Rowane and Rowane10 techniquesmentiontheintercostals.Belcastroetal8
specificallyaddressesthefascialreleaseoftheintercostalsusingtheribs.
The review of the textbooks andliteraturehas shownnumerouswaysofaddressing the asthmatic patient withmanipulativetechnique.Mostosteopathicmanipulativetechniquespresentlybeingtaught in theosteopathic collegeshavethe patient in a supine position.Thosethat have the patient seated utilize athrusttechniquetotheribsortransverseprocesses.Thereismentionofrhythmiccaudadmotion.8Ribraisingistraditionallydonewiththepatientinthesupineposi-tion.Thephysician’sfingers areplacedonthetransverseprocessesandanterior(upward)pressure is exerted tobalancethe ligamentous tension and affect thesympatheticinnervation.Ribarticulationisdonebygraspingtheribsneartheheadandalongtheshaftanddistractingasthepatientrotatesawaytogapthejoint.11
Other techniquesIn functional release, palpation at
the dysfunctional segment (spinal orappendiculer) provides for continuousfeedbackinformationaboutthepatient’sphysiologicresponsetomotion.Relativedegrees of compliance or resistance ofcomponentpartsarecomparedbyopera-tor-inducedmotion.Itdoessoinoppos-ingdirections.Themotions introducedarethosethatleadtoanincreasedsenseof compliance (decreased resistance)ofcomponentparts.1�
In fascial-ligamentous release, thepatient during the correctiveprocedureprovides muscular or respiratory as-sistance.Afulcrumissoughtwithinthephysician’sbodytomatchorbalancethefulcrumwithin thepatient’sbody.Thisfulcrumfacilitatesacontinuumofreflex
release from within the patient’s body.Thepatient’sbodyrespondscomprehen-sivelytoanexternalforceappliedduringmanipulativeprocedures.1
The fascia-ligamentous release tech-niquefortheribcagefollows.Thepatientissupine.Thephysicianplacesonehandposteriorly, beneath the rib cage, withthe fingertips just beyond the spinousprocessesoftheassociatedthoracicverte-brae.Placetheotherhandontheanteriorheadsoftheribs.Anelbowonthekneeestablishes the fulcrum. Ifwe combinethis with the upper thorax fascial-liga-mentousrelease,thepatient’sheadrestsonapillow.Onehandandarmcontacttheupperthoracictransverseprocesses,withthephysician’sfingersspreadslightlytocontact the ribsoneach side.Place theoppositehandonthesternum.Theelbowonthetabletop,beneaththepatient’sheadestablishesthefulcrum.1
Belcastrodescribedintercostalfascialrelease, et al. The specific techniquewas described as follows: Each of thephysician’shands isplaced laterallyonthe middle and lower thoracic cage.Arhythmic caudadmotion is then added,which contributes to the stretching ofintercostalmuscles.8
Deep-touch palpation, the fingerscompress the skin surface, palpatingthrough skin and subcutaneous tissuesto the superficialmuscle layer.Furthercompressionleadstopalpationofdeepermuscles,fasciaandbone.Deeppalpationutilizesforcesofcompressionandshear.Compression is a forceappliedperpen-dicularly to the skin surface.Shear is aforceappliedparalleltotheskinsurface.In some instances,deeppalpationcom-binesbothcompressionandshearintheexplorationofdeeptissuetexture.14
Facilitatedpositionalreleaseinvolvesplacingthedysfunctionintofirstaneutralposition,addingacompressiveforceandthetakingthedysfunctionintoapositionofease.13
Polarityisanadditionalconsideration.Thistechniquedirectsspecificcombina-tionsofgender-specificpositioning.Itisanadditionalconsiderationintreatingtheasthmaticpatient.
Theproposedintercostalribtechniqueincorporatessomefeaturesofthesepre-viously published techniques but withenoughvariationtoofferadifference.
SummaryIn treating asthmatic patients both
acutelyandchronicallywithosteopathictechniques, mechanical considerationshaveadifferentpriority.Itisclearthatthepatient’stotalpictureinvolvesbetterex-changeofairnotonlyinagrosssensebutinacellularsenseaswell.Theproblemsthatpersistevenwiththebestmedicinaltreatmentaremechanical.
Theproblem,simplyput,isaninabilitytoexhale.Exhalationisprimarilyafunc-tionofcomplianceorchestwallelasticityand muscular function. One must alsoconsiderthepulmonarytissueelasticity.Intheasthmapatient,theparenchymaisnotaproblemsofarasstretchorresilienceisconcerned.Secretionsmayaffectsurfacetensionbutthisisasmallcomponent,rela-tivelyspeaking,intheoverallscheme.
Themainproblemisthatligamentousandmuscularcomponentshavebeen inashortenedandhypertonicconditionthemajorityofthetime.Thisisknownasaninhalationpositionoronx-ray,aflatteneddiaphragm.Thesignificanceofthissitua-tionisthatitnowrequiresworktoexhalewhichisnormallyapassiveprocess.
The cause of death in an asthmaticpatientwhodiesduringanadmissionforstatus asthmaticus is respiratory failureor rather respiratory muscular exhaus-tion.(Retractions,secondarymusclesofrespirationinexcessiveuse,paradoxicalrespirationsetc.)
Withosteopathic treatment, theme-chanical issues are addressed directly.The structural goals includedecreasingtheworkofbreathingby increasing thefunctionalrangeofmotionoftheribcageandthediaphragm.Asecondaryeffectofthisistopromotelymphaticdrainageofthepleural spacesand theparenchymaltissuesasaresultoftherestorationoflargeexpansileandcontractilemotionsinthetissues.Thisdrivesfluidsandsecretionsintotheterminallymphaticsatthebron-chioles, andat theparietal pleura.Thisosteopathically addresses the inflamma-torycomponentofasthma.
Ifthismanipulativeapproachiscom-binedwiththeadministrationofappropri-atemedication,thetotaldosageisoftenreducedsignificantlyandtheefficacyofthemedicineisextremelyenhanced.Thismayreducethenumberofhospitaladmis-sionsdramatically.Inthelongtermcareoftheasthmaticpatient,thesetechniques

March�006 The AAO Journal/�9
oftenreducethefrequency,duration,andseverity of attacks. It also reduces theutilizationofhighdosemedicationsoverextendedperiodsoftime.
Theintercostalribtechniqueoffersanadditionaloptioninthetreatmentofboththeacuteandchronicasthmaticpatient.Seated,thepatientislessthreatenedandmore cooperative.There is no interfer-ence with pharmacological or medicalmanagement.
Theworkofbreathing isdecreased.Physician touch and presence reassurethepatient.
References1. ChilaAG.Fascial-Ligamentous
ReleaseinWardRC,ExecutiveEditor.Foundations for Osteopathic Medicine. Baltimore,MD.Williams&Wilkins.1997.pp819-830.
�. SherwoodL.The Respiratory System in Human Physiology,3rdEdition.USA.WadsworthPublishingCom-pany.1997.pp418-465.
3. KucheraMLandKucheraWA.Osteo-pathicConsiderationsandActionsoftheThoraxinOsteopathic Principles in Practice,�ndPrinting,�ndEdition.Columbus,OHGreydenPress.1993.pp��4-��9.
4. HoagJM,ColeWV,andBradfordSG.OsteopathicManagementinDisor-dersInvolvingImmuneMechanismsinOsteopathic Medicine.NewYork.McGraw-HillBookCo,Inc.1969.pp693-397.
5. DiGiovannaEL.Thepulmonarypa-tient.InDiGiovannaEL,SchiowitzS.An Osteopathic Approach to Diagnosis and Treatment,�ndEdition.Philadel-phia,PA.Lippincott-RavenPublishers.1997.pp466-467.
6. PaulFAandBuser,BR.Osteopathicmanipulativetreatmentapplicationsfortheemergencydepartmentpatient.JAOA.1996.96:403-409.
7. PurseFM.Manipulativetherapyofup-perrespiratoryinfectionsinchildren.JAOA.1966.65:971-985.
8. BelcastroMR,BachesCR,andChilaAG.Bronchiolitis:apilotstudyofOMT,bronchodilatorsandothertherapy.JAOA.1984.83:9:67�-676.
9. WilsonPT.Theosteopathictreatmentofasthma.JAOA.1959.45:491-49�.
10. RowaneWAandRowane,MP.Anos-teopatahicapproachtoasthma.JAOA.1999.99:5:�59-�64.
11. LippoincottHA.TheosteopathictechniqueofWm.G.Sutherland,DO.1949.AAO Yearbook.pp6-9.
1�. JohnsonWLandFriedmanHD.IntroductioninFunctional Methods.Indianapolis,IN.AmericanAcademyofOsteopathy.1994.
13. SchiowitzS.FacilitatedPositionalRe-leaseinDiGeiovannaEL,SchiowitzS.An Osteopathic Approach to Diagnosis and Treatment,�ndEdition.Philadel-phia,PA.Lippincott-RavenPublishers.1997.p91.
14. BealMC.OsteopathicBasicsinThe Principles of Palpatory Diagnosis and Manipulative Treatment.Newark,OH.AmericanAcademyofOsteopathy.pp10�-103.❒
Accepted for publication: Dec. 2002
Address correspondence to:ClaudiaL.McCarty,DO,FAAOOMMAssociates,PC575UnderhillBlvd.,Suite1�6Syosset,NY11791E-mail:[email protected]
CME QUIZThepurposeofthequizfoundonthe
nextpageistoprovideaconvenientmeansofself-assessmentforyourreadingofthescientificcontentinthe“AMyofascialtrig-gerpointon theskull treatment improvespeakflowvaluesinacuteasthmapatients”byWm.ThomasCrowandDavidKasperANDinanFAAOthesispaper,“IntercostalRibRelease”byClaudiaL.McCarty.Foreachofthequestions,placeacheckmarkinthespaceprovidednexttoyouranswersothatyoucaneasilyverifyyouranswersagainstthecorrectanswersthatwillbepub-lishedintheJune�006issueoftheAAOJ.
ToapplyforCategory�-BCMEcredit,transfer your answers to theAAOJ CMEQuizApplication Form answer sheet onthenextpage.TheAAOwillrecordthefactthatyousubmitted the formforCategory�-BCMEcreditandwillforwardyourtestresults to theAOA Division of CME fordocumentation.
fACULTY POSITIONS
Kirksville College of Osteopathic Medicine, the founding college of os-teopathic medicine, seeks physicians to fill clinical faculty vacancies for the department of Osteopathic Manipulative Medicine. faculty respon-sibilities include course development, instruction, research, and stu-dent advisement. Qualified candidates will be board certified or board eligible, with teaching experience preferred. On the cutting edge of os-teopathic medical education, there is a wealth of opportunity for faculty to grow professionally while using the latest instructional technology. In addition, faculty members participate in a wide variety of clini-cal activities which may include hospital consultation and treatment, specialty, outpatient care, nursing home and senior care, and mentoring of residents and osteopathic medical students. This person will have a faculty appointment in the department of OMM for A.T. Still University of health Sciences at its Kirksville College of Osteopathic Medicine.
Academic rank and salary will be commensurate with credentials and experience. Application review continues until positions are filled. Please send letter of interest, curriculum vitae, and 3 references to:
ATSUhuman Resources800 West Jefferson
Kirksville, MO [email protected]
Equal Employment Opportunity Employer

30/The AAO Journal March�006
AMERICAN OSTEOPAThIC ASSOCIATION CONTINUINg MEDICAL EDUCATION
ThisCMECertificationofHomeStudyFormisintendedtodocumentindividualreviewofarticlesintheJournal of the American Academy of OsteopathyunderthecriteriadescribedforCategory�-BCMEcredit.
CME QUIZ
CME CERTfICATION Of hOME STUDY fORMThisistocertifythatI,___________________________,pleaseprintfullname
READthefollowingarticlesforAOACMEcredits.Questions 1-3: Name of Article: A Myofascial Trigger Point on the Skull Treatment Improves Peak Flow Values in Acute Asthma PatientsAuthor: Wm. Thomas Crow, DO, FAAO and David Kasper, MBAPublication: Journal of the American Academy of Osteopathy,Volume16,No.1,March�006,pp17-�1
Questions 4-6: Name of Article: Intercostal Rib Release: Asthma ProtocolAuthor: Claudia L. McCarty, DO, FAAOPublication: Journal of the American Academy of Osteopathy,Volume16,No.1,March�006,pp�9-3�
Category 2-B credit may be granted for these article.
00___________ _______________________AOANo. College,YearofGraduation
Signature_____________________________________________
StreetAddress_________________________________________
City,State,Zip_________________________________________
fOR OffICE USE ONLY
Category:�-B Credits___________________
Date:________________________________________________
AOANo.00__________________________________________
Physician’sName______________________________________
Complete the quiz to the right and mail to the AAO. The AAO will forward your completed test results to the AOA. You must have a 70% accuracy in order to receive CME credits.
Answer sheet to June 2006
AAOJ CME quiz will appear in the March 2006 issue.
Mail this page with your quiz answers to:American Academy of Osteopathy®
3500 DePauw Blvd, Suite 1080Indianapolis, IN 46268
December 2005 AAOJ CME
quiz answers:1. D 2. D3. A4. A5. B
Dr. Crow’s Article:1. Atriggerpointwasfoundfortreatmentofasthmaat A. Theleftparietaleminence B. Therightparietaleminence C. ThelevelofT4left D. TheleftofT5right E. TheedgeoftheleftSCM
�. Peakflowmeters A. Arethegoldstandardforinpatientmeasurementsofasthma B. Assesstidalvolumeofthelungs C. Haveracebaseddifferentvalues D. Useheight,ageandsex E. Useonlyoneattempt
3. Thetreatmentofascalptriggerpointshowedimprovementinpeakflowvaluesinacuteasthma.
TrueorFalse
Dr. McCarty’s article:4. Inwhichofthefollowingpositionsisthepatientusuallytreated
withIntercostalRibReleaseTechniqueduringanacuteasth-maticattack?
A. LateralRecumbent B. Prone C. Seated D. Standing E. Supine
5. Theanterior/posteriorpressureusedduringtheIntercostalRibReleaseTechniqueisapplieddowntowhichtissuelevel?
A. Bone B. Fascia C. Muscle D. Skin E. Tendon
6. KucheraandKucherahavereportedthatforeach1cmofincreaseinchestexcursion,thevolumeofairexchangewillincreasebyhowmuch?
A. �5cc B. 75cc C. 100cc D. �00cc E. 600cc
Forum for Osteopathic Thought
Tradition Shapes the Future • Volume 16 Number 1 March 2006

March�006 The AAO Journal/31
regIstratIon rates
on or beFore 4/5/06 aFter 4/5/06AAO Member $550 $650Intern/Resident/Student $450 $550AAONon-Member $765 $865
AAOacceptsVisaorMastercard
CreditCard#______________________________________
Cardholder’sName__________________________________
DateofExpiration___________________________________
Signature__________________________________________
RegIstratIon Form
Diagnosis and Treatment of Low Back Pain
May 5-7, 2006FullName_______________________________________
NicknameforBadge_______________________________
StreetAddress____________________________________
________________________________________________
City___________________State_______Zip__________
Officephone#____________________________________
Fax#:__________________________________________
E-mail:_________________________________________By releasing your fax number/E-mail address, you have given the AAO permission to send marketing information regarding courses
via the fax/E-mail.
AOA#_________College/YrGraduated______________
Diagnosis and Treatmentof Low Back Pain
May 5-7, 2006Hilton Hotel, Durham, NC
Course Description: Level IILow back pain continues to be one of the most common
presentationstothephysicians’office.Thiscoursewillpresentparticipants with practical approaches to the evaluation andtreatmentoflowbackpain. Emphasiswillbeontheoveralltreatmentapproachutilizingvarious typesofOMTbasedonthe clinical scenario. Specific techniques will include highvelocitylowamplitude(HVLA),muscleenergy,counterstrainandmyofascialrelease.Additionaltreatmentapproacheswhichcanbeintegratedintotheoverallcareoflowbackpainwillbereviewed,however,demonstrationsandpracticewillbelimitedtoosteopathicmanipulativetechniques.
Learning Objectives:Participantsshouldbeableto:1)Understandthefunctional
anatomyofthelowbackregion;�)Correlatesomaticdysfunc-tion to the pathophysiology of low back pain; 3) Efficientlydiagnosesomaticdysfunctioninthelumbar,pelvisandsacralregionsandcorrelatewithclinicalpresentationsof lowbackpain;4)Selectandperformappropriate typesofOMTbasedondiagnosticfindings;5)Understandhow to integrateothertreatmentapproaches,suchasexerciseprescriptionandinjectiontechniques,intothecareofthepatientwithlowbackpain;and6)Documentfindingsandselectcodesforreimbursement.
Prerequisites:Theparticipantshouldhaveabasicunderstandingoffunc-
tionalanatomyand(1)LevelIcourse
CME:The program anticipates being approved for �0 hours of
AOACategory1-ACMEcreditpendingapprovalbytheAOACCME.
Program Time Table:Friday,May5..............................................8:00 am -5:30pmSaturday,May6..........................................8:00 am -5:30pmSunday,May7..........................................8:00 am -1�:30pm
(Friday&Saturdayinclude(�)15minutebreaksanda(1)hourlunch;Sundayincludesa30minutebreak)
Course Location & Hotel Accommodations:HiltonDurhamnearDukeUniversity
3800HillsboroughRoad,Durham,NC�7705www.hiltonhotel.com;Phone:919/564-�91�
AAORoomRate:$99.00RoomRateDeadline:4/6/06
IneedAAFPcredit❒ Irequireavegetarianmeal❒(AAO makes every attempt to provide snacks/meals that will meet participant’s needs. But, we cannot guarantee to satisfy all requests.)
GuyA.DeFeo,DOProgramChair

3�/The AAO Journal March�006
Additional faculty: ThomasRavin,MD GeorgePasquarello,DO,FAAO Courses Description: Level III
Thisisacoursedesignedtoinstructparticipantsinthephysiologyofwoundrepairusingcadaversandprosections.Participantswillreviewtheanatomicalrelationshipsoftendon5/15andligamentstructuresandgaininsightintothereferredpainpatternsoftendonsandligaments.Also,participantswilllearndiagnosticandinjectiontechniquesfortendonandligamentinstability.Thecoursewillalsoincludealectureoncodingandbilling.
Learning Objectives:Attheendofeachsession,participantsshould: •Readilyevaluateforjointinstability •Readilydiagnosetendoninstability •Knowhowtoinjectunstabletendonsandjoints
CME:Theprogramanticipatesbeingapprovedfor�0hoursofAOACat-egory1-ACMEcreditpendingapprovalbytheAOACCME.
Prolotherapy: Above the Diaphragm
(Special emphasis on cervical and thoracic spines, ribcage, shoulder, elbow, wrist and hand.)
May 19-21, 2006UNECOM, Biddeford, ME
MarkS.Cantieri,DO,FAAOProgramChair
Program Time Table:Friday,May19...........................................8:00am–5:30pmSaturday,May�0.......................................8:00am–5:30pmSunday,May�1.......................................8:00am–1�:30pm
(Friday&Saturdayinclude(�)15minutebreaksanda(1)hourlunch;Sundayincludesa30minutebreak.)
Course Location:UNECOM
11HillsBeachRoad,Biddeford,ME04005www.une.edu
Hotel Accommodations:Forhotelpossibilities,visit:
www.expedia.com;www.travelocity.com;www.priceline.com;orwww.BizRate.com
SearchforSouthPortland,BiddefordorKennebunkport.Arentalcar is recommendedsince thecampus is locatedabout15-�0minutesfrommosthotelsandrestaurants.
regIstratIon rates
on or beFore to 4/19/06 aFter 4/19/06AAO Member $1,�00 $1,500AAONon-Member $1,415 $1,715
(Non-members – see membership application on page 23)Sorry, no discounts
AAOacceptsVisaorMastercard
CreditCard#______________________________________
Cardholder’sName_________________________________
DateofExpiration__________________________________
Signature_________________________________________
RegIstratIon Form
Prolotherapy: Above the Diaphragm
May 19-21, 2006FullName_______________________________________
NicknameforBadge_______________________________
StreetAddress____________________________________
________________________________________________
City___________________State_______Zip__________
Officephone#____________________________________
Fax#:__________________________________________
E-mail:_________________________________________By releasing your fax number/E-mail address, you have given the AAO permission to send marketing information regarding courses
via the fax/E-mail.
AOA#_________College/YrGraduated______________
Irequireavegetarianmeal❒(AAOmakeseveryattempttoprovidesnacks/mealsthatwillmeetparticipant’s needs. However, we cannot guarantee to satisfy allrequests.)

March�006 The AAO Journal/33
➝
BackgroundIn19�8,orthopedicsurgeonCrowe
was thefirst individual touse the termwhiplashtodescribeneckinjuryrelatedtomotorvehicleaccident.1Withgreaterrelianceonmotorized transportation inthe �1st century, the rate of whiplashrelatedinjuriesinWesterncountrieshasincreasedsignificantly.Newterminologyhasarisentodescribethecomplexityofinjuryrelatedtoboththeacuteandchronicphaseofwhiplash.Nowtermedcervicalwhiplashsyndrome(CWS)�orwhiplashassociateddisorder(WAD)3,itembodiesanarrayofmuscular,skeletal,neurologi-calandpsychosocialimpairments.
Treatmentoptionsandoutcomesforindividuals suffering fromWAD/CWShavebeenextensiveandvaryinsuccess.Modalitiesincludepharmacologicalman-agementofpain,acupuncture,physicaltherapy,chiropractic,hypnosis,surgery,osteopathic manipulative techniques(OMT)andtriggerpointinjections(TPI).Thetreatmentplanmustbeindividual-izedforeachpatientandshouldincludeamultidisciplinaryrehabilitativeapproachinordertoprovidepainmanagementandrestorationoffunction.
Wepresentthisreportaswefeelthatthispatientrepresentsamorecomplicat-edcaseofWAD/CWSsufferingchroniceffects from her injury. Furthermore,hercasedemonstratestreatmentfailurein theearlyprocessofmanagementbyother clinicians. Moreover, we believethat the combined modalities of OMTandTMIutilizedatourclinichavebeeninstrumentalinthehealingprocessofthispatient.
Multidisciplinary approach to treatment in a 38-year-old female, restrained driver following injuries sustained in a rear-end collisionJ.L Rook and A.M. Auburn
Patient ReportThisreportdescribesa38-year-old
Caucasianfemalewhowastherestraineddriverofavehicle,whichwhilemakingarightturn,wasstruckfrombehind.Thepatientdescribestheimpactassendingherforward,backwardandtotheright.Immediately following the accident,thepatientwasabletoexitthevehicle,ambulate without difficulty and onlyreported stiffness. She did not experi-ence any loss of consciousness (LOC)anddidnotrequireemergencymedicalservices. However, two days follow-ing the accident, the patient began toexperiencevertigo, neck and lowbackpain, headache in the occipital region,nauseawithdryheavesandsubsequentdifficultywithforwardbending.Atthistime,shesoughtmedicalattentionatalo-calemergencydepartment.Evaluationbytheemergencyroomphysicianrevealednoevidenceoffractureorlifethreaten-inginjuryandthepatientwasdischargedwith an anticholinergic and a non-ste-roidalanti-inflammatory(NSAID).Shesubsequentlysoughtinterventionintheform of physical therapy, chiropracticandcranial-sacralwithminimalimprove-mentinfunctionandnegligibledeclineofsymptomatology.
Approximately14monthsfollowingheraccident,thepatientpresentedtoourclinic forevaluation.Shecomplainsofoccipital-neckpain(6outof10qualityinstaticpositioning,increasingto8-9of10withmovement),mid-uppershoulderpain(4of10quality,increasingvariablyto9of10),right-sidedlumbrosacralpain(3of10quality, increasingvariably to5-6of10),vertigoassociatedwithfor-
ward and rotational head movements,intermittent diplopia, decreased abil-itytoperformactivitiesofdailyliving,increasing fatigue, and increasing dif-ficulties coping with her impairments.Past medical and surgical history areremarkablefortwopreviousstrabismuscorrections,twodilatationandcurettage(D&C)procedures,andacesareansec-tion.Familyhistoryisnon-contributoryand the patient reports no medical orfoodallergies.Atthetimeofevaluation,thepatient’smedicationusageincludesMotrin,Wellbutrin,Zyprexa,Tramadolandamultivitamin.
Onphysicalexam,thepatientisanobese femalewithaBMIof37.1 (71”and�66lbs),whoisinobviousdiscom-fort and mild distress. She is afebrile,normotensive and non-tachycardic.Gaitanalysiswaswith-innormallimits(WNL), Romberg was negative, deeptendonreflexes(DTR)were�+/4bilater-allyinbothupperandlowerextremitiesandthepatientdemonstrated4/5musclestrengthbilaterallyinbothherupperandlowerextremities.
Osteopathic examination revealedthe following findings: C1 R(R), C�FRS(L), C5 FRS(R), C6 FRS(L), in-creasedCRIapproximately15/minwithrestricted movement and increased tis-sue texture abnormalities (TTA) in theposteriorandlateralcranium;Roccipitalcompression,Ltorsion,Llateralstrain,SR(R)strainwithrestrictedmovementoftheLoccipital-mastoidandLsphenoidal-squamous pivot sutures;TTA at the Roccipital-cervical junctionextending totheRlevator,rhomboids,scalenes,ster-

34/The AAO Journal March�006
nocleidomastoid (SCM) and trapezius,collectively; stacked ERS(L) ofT5-T8with concomitant L posterior rib dys-function;increasedtextureabnormalityoftheLerectorspinae;+RstandingandRseatedflexiontestswithtendernesstopalpation (TTP) at the R lumbrosacral(LS) junction,L1-L3NRrSl,L4FRSr,L5FRSrandaR/Lsacraltorsion.Fur-thermore,orthopedictestingdoneprevi-ouslyyieldedthefollowingresults:(-)RSpalding, (+)L Spalding, (-) bilateralseatedstraightlegraise(SLR),(-)Soto-Hall,(-)Ely’s,(+)RYeoman’s,and(+)RPatrickFABERE.
Othersignificantphysicalexamfind-ingsincludedneuromuscularimbalancesecondarytobilateralhipflexortestingwith notedTTA and decreased length(R>L),TTP (R>L) in the ileo-lumbarandsacro-iliacligamentsindicatingliga-mentus laxityandfinally thefollowingmyofascialtriggerpoints:Roccipital,Ruppertrapezius,Rlevator,Rscalene,RSCM,Rrhomboidandalongthecervicalandlumbarerectorspinae.
Basedonourphysicalexamfindingscoupled with the patient’s history, weconclude that the patient has multiplesomatic dysfunctions (SD) as noted inphysicalexam,myalgia/myositis,occipi-talandLSligamentuslaxity,cephalgiaand chronic pain syndrome secondarytoaboveandahistoryofvertigoassoci-atedwithnausea.ThedecisiontobeginaregimenofOMTprecededbyTPIwithafrequencyevery1-3weeksastoleratedwas initiated immediately. In addition,the patient was referred for physicaltherapy using neuromuscular balancetraining(�-3timesperweek).
As of the date of this report, thepatient has undergone six treatmentsutilizing a combination of OMT withandwithoutprecedingTPI:1)TPI/OMT;�)OMT;
3)TPI/OMT;4)TPI/OMT;5)TPI/OMT; and, 6) OMT. TPI is preparedinourclinicusingthefollowing: 4ccmarcaine,�ccprocaine,0.5ccwydase(hyaluronidase), 1 cc serapin and � cctraumeel. For treatment 5, an additionof Kenalog (0.5 cc) was added to thestandardmixture.
In response to each treatment ses-sion, the patient reported immediateimprovementsthatwerefurtherverifiedwith re-evaluation demonstrating im-
proved range of motion, restoration ofmusculoskeletal formandfunctionanddecreasedTTP.
AtthecompletionofsixtreatmentsusingtheacombinationofTPIandOMTthe patient admitted to decreased epi-sodesofvertigoandnausea,animprovedlevelofenergyandgreaterabilitytoac-complishADL’s.
DiscussionInthispaper,wedescribeafemale
patientwithwhiplashassociateddisordermanifestingasaprogressivechronicpainsyndrome(CPS).Patientswhohavede-velopedCWS/WADsymptomsthatarestill present beyond three months usu-allydonotfullyrecover.4Infact,somepatients,likeours,progresstowardspsy-chologicalsymptomatologythatimpairoverall physical and cognitive ability5
furthercomplicatingthehealingprocess.Thispatientrespondedwelltoamulti-disciplinarytreatmentstrategyutilizingcombinedTPI/OMT complemented byphysicaltherapythatincorporatedneu-romuscularre-education.
Simons et al have best describedtrigger points as hyperirritable spots,bothfocalanddiscrete thatare locatedwithin a taut band of skeletal muscle.6Trigger points may be either active,7causingpainatrestorlatent,8leadingtomovementrestrictionsandmuscleweak-ness.Inaddition,theycaninducereferredpain,tenderness,motordysfunctionandautonomicphenomena.6
The decision to use manual tech-niquesorTPIforthetreatmentoftriggerpointassociatedsymptomsismultifac-toral.9TPI is an effective technique toproviderapidrelieffromthesymptomsassociatedwithtriggerpoints,10especial-lythosethathaveamorelatentnature.9
Unfortunately,fewcontrolledstudiesex-istthatexaminetheeffectivenessofTPIforthereliefofchronicpain.Moreover,we areunawareof any studies or casereports that have reviewed the use ofTPIfollowedbyOMT.However,ithasbeendemonstratedthatstretchingofthemusclegroupfollowingTPIincreasesitsefficacy11andthisisfurtheraccomplishedbyengaging themusclesbetweenboththeirfullyshortenedandfullylengthenedpositions.9The premise of OMT is torelievesomaticdysfunctionbyengagingtheanatomicand/physiologicbarrierin
amusculoskeletalunittorestorebalanceoffunctionandform.1�,13
Buildingupontheconceptofmusclestretching and activity to increase theeffectiveness ofTPI is the use of neu-romuscular re-education inourpatient.Aspreviouslymentioned,latenttriggerpoints are associated with restrictionsin motion and muscle weakness.Thisensuing neuro-muscular imbalance iscomplicated by a complex series ofpathophysiologicmechanisms.14,15There-fore,havingthepatientperformaseriesof repetitive contractions that train theneuromuscular system to memorize aseriesofmotorpatterns,anengram,isthebasis of neuromuscular re-education.16
The result is restoration of the normalarthrokineticsofagonistandantagonistmusclegroupswithequivalentbalanceintheinputandoutputchannelsofunderly-ingneurologicalunits.
Thereisasignificantabsenceinthemedical literature that discusses viabletreatmentoptionsforindividualssuffer-ing from CPS.As the leading form ofdisabilityinadults17andwithcurrentfig-uressuggestingthatapproximately10%oftheU.Spopulationislivingwiththedisablingaffectsofoneormorechronicmusculoskeletal disorders,18 physiciansmustbeabletoprovidetherapeuticop-tionswhichallowtheirpatientstomain-tainqualityoflife.Westronglybelievethatthiscasereportillustratesthesuccessthatcanbeachievedinpatientoutcomebyprescribingamultidisciplinarytreat-mentapproachthatencompassesrestora-tionoffunction,eliminationofpainandre-educationofform.
References1. CompanaBA.Softtissuespineinjuries
andbackpain.InP.Rosen&R.Barken(Eds.),Emergency medicine concepts and clinical practice,4thed.St.Louis:Mosby.1998:878-905.
�. ChildsSG.Cervicalwhiplashsyndrome:hyperextension-hyperflexioninjury.Orthopedic Nursing.�004:�3:106-110.
3. SpitzerWO,SkovronML,SalmiLR,CassidyJD,ZeissE.Scientificmono-graphoftheQuebectaskforceonwhip-lash-associateddisorders:redefining“Whiplash”anditsmanagement.Spine.1995:�0:S1-S73.
4. BarnsleyL,LordS,BogdukN.Whip-lashinjury.Pain.1994:58:�83-307.
5. KessellsRPC,AlemanA,VerhagonWM,VanLuijtelaarELJM.Cognitive

March�006 The AAO Journal/35
functioningafterwhiplashinjury:ameta-analysis.J Int Neuropsych Soc. �000:6:�71-�78.
6. SimonsDG,TravellJG,SimonsLS.Travell and Simons myofascial pain and dysfunction: the trigger point manual,�nded.Baltimore.Williams&Wilkins.1999:5.
7. HanSC,HarrisonP.Myofascialpainsyndromeandtriggerpointmanage-ment.Reg Anesth.1997:��:89-101.
8. LingFW,SlocumbJC.Useoftrig-gerpointinjectionsinchronicpelvicpain.Obstet Gynecol Clin North Am.1993:�0:809-815.
9. SimonsDG,TravellJG,SimonsLS.Travell and Simons myofascial pain and dysfunction: the trigger point manual,�nded.Baltimore.Williams&Wilkins.1999:94-173.
10.AlvarezDJ,RockwellPG.Triggerpoints:diagnosisandmanagement.Am Fam Phys.�00�:653-660.
11.ZohnDA,MennellJM.Musculoskeletal pain: diagnosis and physical treatment.Boston.Brown.1976:1�6-1�9,190-193.
1�.FryetteHH.Principles of osteopathic technique.Carmel,CA.AmericanAcad-emyofOsteopathy.1954.
13.MitchellFL,MoranPS,PruzzoNA.An evaluation and treatment manual of osteopathic muscle energy procedures. ValleyPark.MitchellMoran&PruzzoAssociates.1979.
14.GreenmanPE. Principles of Manual Medicine,�nded.Baltimore.Williams&Wilkins.1996:449-5�4.
15.JandaV.Evaluationofmuscleimbal-ance.In:LiebensonC,etal.,(Eds.)
Rehabilitation of the spine.Baltimore.Williams&Wilkins.1996.
16.KergerS.Exerciseprinciples.In:KarageanesSJ(Ed.)Principles of manual sports medicine.Baltimore.Wil-liams&Wilkins.�005:65-76.
17.ColeTM,EdgertonVR.Musculoskel-etaldisorders.In:ColeTM,EdgertonVR,eds.Report of the Task Force on Medical Rehabilitation Research.June�8-�9,1990.HuntValleyInn,HuntVal-ley,MD.Bethesda.NationalInstitutesofHealth.1990:61-70.
18.ImamuraST,FischerAA,Imamura,TeixeiraMJ,TchiaYengLin,KaziyamaHS,etal.Painmanagementusingmyo-fascialapproachwhenothertreatmentfailed.Phys Med Rehab ClinNorth Am.1997:8:179-196.❒
Accepted for publication: Nov. 2005
Address correspondence to:
JamesL.Rook,OMS-IVWesternUniversityofHealthSciencesCollegeofOsteopathicMedicineofthe
Pacific309E.�ndSt.Pomona,CA91766E-Mail:[email protected]
and
AnnMarieAuburn-Dean,DO37005�ndSt.SEGrandRapids,MI4951�Fax:616/656-3701
Kaplan clInIc
arlIngton, VaseeKs omm physIcIan
Kaplan Clinic, an indepen-dent integrative-medicine prac-ticeinArlington,VAwithateach-ing affiliationwithGeorgetownUniversity School ofMedicine,isseekingaphysicianwithstrongosteopathic manipulation skillsto fill a permanent, full-timeposition. Candidates should beboardeligible/certifiedinfamilyorinternalmedicine.
Founded �0 years ago, theClinic is the oldest integrative-medicine practice in theWash-ington, DC area. The Clinicspecializes in treating patientswith chronic pain and illness.Our �1-person team of physi-cians,psychotherapists,physicaltherapists, nurses and supportstaffworktogethertoprovideawiderangeofconventionalandalternative treatments, includ-ing acupuncture, homeopathicandherbalremedies,nutritionalcounseling, psychotherapy, andmind-bodyclasses.
The Clinic is a 10-minutedrive from the nation’s capital;the metropolitan area is rich incultural, recreational, educa-tional, and social opportunities.Ifyouareinterestedinbuildingafamily-medicineandpain-man-agementpracticewhileenjoyingaguaranteedincome,productiv-ity bonus, and excellent benefitpackage (including liability in-surance, license fees and CMEallowance).
Please,emailyourCVto:JulieThompson,RN,
[email protected]:703/�37-3105
phone:703/53�-489�
Classified AdsmIchIgan
Medicalofficebuildingforsale.BetweenLakeErieandI-75.�0minutesfromhospitalsinMonroe,MIandToledo,OH.Floorareaspace1,�74sq.ft.3examrooms,office,�restrooms,library/kitchen,largewaitingroomandlargestorageroom.Pavedcarportandamplefrontparking.Naturalgas,citywaterandcitysewer.ContactIsabelleChapelloafter�:00pm.Phone734/848-5565.Buildinglocation:10643ValleywoodDrive,LunaPier,MI.
IndIanapolIs
WestviewHospitaliscurrentlyacceptingapplicationsforits�-yearNMM/OMMresidencyprograminIndianapolis,Indiana.Interestedcandidatesshouldcall317-9�0-7338forfurtherinformation.

36/The AAO Journal March�006

March�006 The AAO Journal/37
The Science and Practice of Manual Therapy: Physiology, Neurology and Psychology E. Lederman, second ed.. Churchill Livingstone, 2005. Paperback, 336 pp., 186 illus, ISBN 0 443 07432 1. Price: $67.95
Oneofthemanychallengesfacingosteopathyandmanualtherapyingeneralisunderstand-ingtheprocessesandmechanismsthatoccurinourpatientsinresponsetotherapeuticmanualtechniques.Thisunderstandingincludesthebiophysical,cognitive,affective,spiritualandsocialdomains.Anappreciationofhowthesedomainsfunctionandinteractisessentialtoenabletheosteopathtodynamicallyassessapatientandidentifythemosteffective‘entrypoint’fortheirtreat-ment. TwelveyearsafterbeginningtowritethefirsteditionofFundamentals of Manual Therapy.ProfessorEvalLedermanagainrevisitsthequestionof“Whatishappeningunderthehandsofthemanualtherapist?”Inthisversion,Ledermanhaswrittenatextaimedatallmanualtherapists,andhasreworkedhisideasandtheoriesinlightofresearchthathasemergedintheinterim.Thisprovidesavitalbridgebetweentreatmenttechniqueandscience-increasinglynecessaryinthecur-rentclimate.Asbefore,thetextisorganisedintothreemainsectionswhichexploretheresponsestomanualinterventioninthetissue,neurologicalandalsopsychophysiologicaldimensions. Atatissuelevel,manualtechniquesareexaminedinthecontextofrepair,adaptationandfluidmovement.Theselectionofsuitablemanualtechniquesdependinguponthephaseofinjuryare
discussedtogetherwithcontra-indicationsandhowthetherapistmayeffectivelyfacilitatetheoptimumenvironmentfortissuerepairandadaptation.Thisextendsintoactivelyengagingthepatientintheirhealingbyencouragingthemtoapplytheseprinciplesintheirdailyactivities.Acentralconceptinthetissuedimensionisunderstandingthemeansbywhichcellsignalling(especiallycellsinvolvedinrepair)mayhemodulatedbymanualintervention.Theconceptofmechanotransductioniswellcontextualisedandexploredwithinamanualtherapycontext,andposesmanyinterestingfollowonquestionsforthereader. Ledermanproposesthatitisintheneurologicaldimensionthattheosteopathandpatientinterfacewithmanualtechniquesastheir‘sharedlanguage’.Healingand‘re-abilitation’aremodulatedcentrallyinthepatienttotheperiphery,andthisprocessmaybefacilitatedbythepractitioner.Fivekeyelementsareidentifiedasbeingtherapeuticallyimportant:patientcognition,activeinvolvementofpatient,effectivefeedback,repetitionandsimilaritytonormalisedmovements.Vitaltothisistheunderstandingthatthetreatmentprocessistherapeuticrelationshipguidedbythepractitionerandfullyengagingthepatientatalllevels(tissues,peripheralandcentralnervoussystem,emotions,thoughts,etc.)tohealthemselves.Ledermanemphasisesthattreatmentisnotsimplysomethingthatisdonetothepatient’stissuesfromtheirperiphery. Thefinalsectionexaminestheinvolvementofpsychologicalandpsychophysiologicalfactorsinmanualtherapy.TheeffectsofmanualinterventiongobeyondthelocaltissuesbeingtouchedandLedermanreviewswhole-personeffectsandprocessesencounteredduringinjury,therapeuticinterventionandrecovery.Alterationsinbodyimageandself-esteemareimportanthereandoftenhealinginthebiophysicaldomainsisimpededbythefailuretoaddresstheramificationsofinjuryinthecognitiveandaffectivedomains.Thewellknownlinkbetweenemotionandpostureisexaminedanddiscussedintermsofaninteractingsomatopsychic-psychosomaticse-quenceandhowtheseresponsesaredeveloped.Thepsychophysiologyunderlyingmanualtherapyisexploredandhowtheseprocessesaredeeplyenmeshedwiththelimbic,neuroendocrineandautonomicnervoussystemsarereviewedtherapeutictouchandtechniquesarediscussedinthecontextofre-orderingandre-integratingthebody-self. ThisisasuperbrevisionandexpansionuponFundamentals of Manual Therapy.Itiswellwrittenandorganisedwithnumerouscleardiagramsthatillustratethetext.IhaveusedFundamentals of Manual Therapyasacoretextbookintheteachingofundergraduatelevelosteopathystudents,andthisupdatededitionismostwelcomeasitfurtherdevelopsandupdatesthesameconceptsinafreshandaccessibleway. AlthoughLedermanhastakengreatefforttowriteatextthatallmanualtherapyprofessionswillfindrelevant,Iwouldsuggestthattheechoofunderlyingosteopathicprinciplesisevidentthroughoutthetext,andassuchthebookwillproveparticularlypopularamongstbothpracticingosteopathsandstudents.
---------------------------------------ReprintedwithpermissionfromElsevierpublishing;theInternationalJournalofOsteopathicMedicine,Volume8,NO.3.Sept�005.
Book ReviewReviewer: David J. H. Baskeyfeld

38/The AAO Journal March�006
Liem, Torsten: Cranial Osteopathy, Principles and Practice. Second Edition, Published in English. ©2004, Elsevier Limited; Paperback, 728 pp. including glossary and Index, 514 illus. Price: $105.00.
TorstenLiem,DO is a registrant of theGeneralOsteopathicCouncil (GB). He serves asPrincipalofOsteopathie Schule Deutschland (Germany)aswellasanMScprograminPediatricOsteopathy.HeisamemberoftheResearchCommitteeoftheAkademie der Osteopathie (AFO).HispublicationsincludePraktisches Lehrbuch der Kraniosakralen Osteopathie, Praxis der Kra-niosakralen OsteopathieandOsteopathie-Die sanfte Lösung von Blockaden. HehasservedasCo-EditoroftheLietfaden Osteopathie andCo-FounderandformerChiefEditorofthejournalOsteopathische Medezin.
ThepresenttextisasubstantialreworkingofPraxis der Kraniosakralen Osteopathie. Havingmovedwellbeyondtheoriginalintentionofbriefrevision,theresultisamajorcontributiontotheconceptsandpracticeofOsteopathy in the Cranial Field. WithparticularattentiontotheoriginalthoughtofSutherland,whoseconceptwasinfluencedbyStill,thecontributionofMagounandmanyofthestudentsofSutherlandareappropriatelyrecognized.Forewordstothetextarepro-videdbyJean-PierreBarral,FredL.Mitchell,Jr.andRichardA.Feely.Eachoneacknowledgesthecomprehensivenessofthiseffort.
Thetextconsistsof�0chapters.AsindicatedbytheauthorinhisPreface to the second edition (�005):
“Theresultsofnewresearchandunderstandingoftheanatomicalstructuresandtheirphysiologicalsignificanceaswellasadditionaldiag-nosticandtherapeuticproceduresarepresented.Osteopathicapproachestothetemporomandibularjointareincreasinglybeingusedinplaceoforthopedictreatmentsofthejaw.Inthelightofthisitbecomesessentialfortheosteopathtopossessasoundbodyofknowledge.Allotherchaptershavealsobeenupdatedtoreflectthepresentstateofknowledge.”
TheIntroduction (pp.1-�8),isanexcellentpresentationoftopicssuchaspalpation,frequencyofprimaryrespiration,methodsofmanualdiagnosis,principlesandmethodsoftreatment,stagesoftreatmentandthefulcrum,treatmentofelectrodynamicfields,andassessmentofthecourseoftreatment.Theinformationpresentedissupportedby87referencesindicativeofthebroad,inter-nationalandmultidisciplinaryactivitycontributingtothestudyofthisformofpractice.
Inanygivenchapterthroughoutthetext,excellenceofillustrationandphotographycontributessignificantlytoeaseofunder-standingforusebythepractitioner.Morphology,clinicalassociations,diagnosticandtreatmentapproachesprovidetheframe-workforeachchapter.Itisthisclarityandconsistencyoforganizationwhichwillprovevaluablefortheteacherandthestudent.Substantialnumbersofreferencesareprovidedforeachchapter.
Chapter11,The mandible and temporomandibular joint canberegardedasthetour de force ofthetext.145pagesinlength,thischapterisamasterfulexpositionoftheosteopathicprofession’straditionalviewofthisjointanditsinvolvementinwholebodyresponsestoitsdysfunction.Asanexample,thesectionaddressingThe temporomandibular joint and body posture (pp.3�8-343)providesaframeworkforassessmentwhichcanbeutilizedinanyformofclinicalpractice.
TheGlossary representsanefforttocontributetoclarificationoftermshavingahistoryofcommunicationdifficulty.ThefocusisderivedfromthepublicationsofWGSutherland,REBeckerandthe1951editionofHIMagoun’sOsteopathy in the Cranial Field. Descriptiveterminologyisgivenpreferenceoverepistemologicalconsiderations.
Thistextprovidesacomprehensive,consistentlystructuredanddetailedcoverage(referenced)ofthematerialpresented. Thelinedrawingsandphotographsemployedabundantlythroughoutenhanceandmakemoreapproachabletheintricaciesofpalpation,diagnosisandtreatmentparticulartotheunderstandingandutilizationofOsteopathy in the Cranial Field.
Book ReviewReviewer: Anthony G. Chila

March�006 The AAO Journal/39
Urinary Tract Infection in Women LindaFrench,MD
ABSTRACTPURPOSE:Toreviewtheepidemiology,diagnosis,andtreatmentofurinarytractinfection(UTI)inwomen.EPIDEMIOLOGY:UTIisthemostcommonlydiagnosedbacterialinfectioninwomen.Uncomplicatedcystitisrarelyleads
tomajormorbidityormortality,buteconomiccostsandimpactonqualityoflifeareconsiderable.Populationsatincreasedriskofcomplicationsincludeolderwomen,pregnantwomen,andwomenwhohavediabetes,areimmunocompromised,orhaveanatomicorfunctionaldisordersoftheurinarytract.
REVIEWSUMMARY:ApresumptivediagnosisofuncomplicatedUTIcanbemadebasedonhistoryalone,orwithlimiteddiagnostictestingsuchasdipstickurinalysis.Cultureshouldbeobtainedifthepatienthasriskfactorsforcomplicateddisease,presumedtreatmentfailure,orfrequentrecurrences.A3-daycourseoftrimethoprim-sulfamethoxazolehasbeenrecommendedasthepreferredinitialtreatmentforuncomplicatedUTIaslongasresistancetothedrugremainssufficientlylow.Otheroptionsforfirstlinetreatmentincludeofloxacin,nitrofurantoinmacrocrystals,andcephalexin.Womenwithfrequentrecurrencesmayusecontinuousprophylaxis,postcoitalprophylaxis,orself-treatmentofrecurrentepisodes.Cranberryjuiceorpillsreducerecur-rences.Inpostmenopausalwomenintravaginalestrogencanreducerecurrences.
TYPEOFAVAILABLEEVIDENCE:Meta-analyses,controlledtrials,cohortstudies,case-controlstudies,andnationallyrecognizedandforeigntreatmentguidelines.
GRADEOFAVAILABLEEVIDENCE:Fairtogood.CONCLUSION:DiagnosisofUTIbasedonsuggestivehistoryaloneissafebutleadstoovertreatment.Inregardtotreat-
ment,thereisconcernaboutemergingantibioticresistance.Futureresearchshouldincludehead-to-headtrialsofinexpensivegenericantibioticsforthetreatmentofUTIs.
Reprintedwithpermissionfrom: Adv Stud Med.�006:6(l):�4-�9.
Differences in Initial Symptom Scores Between Myogenous TMD Patients with high and Low Temporomandibular Opening IndexVictorJ.Miller,BSc,BChD;VesnaV.Karic,DDS,MSc;SandraL.Myers,DDS
ABSTRACTThetemporomandibularopeningindex(TOI)isamoreusefulmeasureofmandibularmovementthanlinearmouthopening,
sinceitisindependentofage,gender,ramuslength,andgonialangle.Itisalsousefulwhencategorizingtemporomandibulardisorder(TMD)patientsintodiagnosticgroups.Twosubgroupsofmyogenouspatientshavebeenidentified,onewithahighandonewithalowtemporomandibularopeningindex.Thisstudyexaminedinitialsymptomseverityinthesetwosubgroups.Thirty-three(33)patientswithamyogenoustemporomandibulardisorderwererecruited.Twenty-six(�6)werefemaleandsevenmale.Elevenwerefoundtobeinthehightemporomandibularopeningindexgroupandtheremaining��inthelowgroup.Symp-tomseverityscoresweredeterminedpriortothestartoftreatment.Pain,jointsounds,headache,andneckpainwereallratedbypatientsonafour-pointverbalresponsescale.ThesesymptomscoreswerecomparedbetweenthetwosubgroupsusingtheWilcoxontwosampletest.Thereappearedtobeasignificantdifferencebetweenthetwogroups(p=0.00�5).TMDpatientswithhightemporomandibularopeningindexappearedtohavemoreseveresignsandsymptomsofTMDthanpatientswithalowindex.
Reprintedwithpermissionfrom:CRANIO: The Journal of Craniomandibular Practice.�006:�4(1):�5.
Elsewhere in Print

40/The AAO Journal March 2006
3500 DePauw Boulevard, Suite 1080Indianapolis, IN 46268
ADDRESS SERVICE REQUESTED
NON-PROFIT ORG.U.S. POSTAGE
PAIDPERMIT #14
CARMEL, INDIANA
New addition to AAO Bookstore
Special Pre-Publication Sale!Contributions to Osteopathic Literature –
Myron C. Beal, DO, FAAO
$20.00 through March 31, 2006
Excerpts from the book’s ForewordFor those of us who have observed the development of the osteopathic medi-cal profession from the perspective of teachers, practitioners, and researchers of traditional osteopathic principles and practice, the name Myron C. Beal, DO, FAAO is well known and evokes feelings of respect and admiration. His osteopathic career has spanned the second half of the 20th Century and his contributions have served to propel the profession to the brink of 21st Century healthcare leadership. Ever the propo-nent of solid research design, Dr. Beal appreciated the fullness of osteopathic philosophy in action by emphasiz-ing palpatory skill in the osteopathic examination as an interaction between the patient and examiner. He appreci-ated the difference between sensing and perception, recognizing the mind body integration ever present in osteopathic philosophy and actualized in osteopathic education.
Hollis H. King, DO, PhD, FAAO, Editor
Order Information:❒ Contributions to Osteopathic Literature – Myron C. Beal, DO, FAAO @ $20.00 + $6 S/H in U.S. (NOTE: Please add $1.00 for each additional book ordered.)
Total $ amount of order: __________
Shipping Information:Name __________________________________________________________________
Street Address ___________________________________________________________(NO P.O. Box #s)
City _____________________________ State ____________ Zip _________________
Daytime Phone _________________ Email Address: ____________________________
Payment Information:❒ VISA ❒ MC ❒ CHECK
Card No. ________________________________________________________________
Expiration Date __________________________________________________________
Signature: _______________________________________________________________
For your copies, contact: American Academy of Osteopathy®,
3500 DePauw Blvd., Suite 1080, Indianapolis, IN 46268-1136; phone: (317) 879-1881; FAX: (317) 879-0563
Order on-line at: www.academyofosteopathy.org