Transferencias Paralisis Radial
48
Tendon Transfers Doug Humphreys Division of Plastic Surgery Dalhousie University Halifax, Nova Scotia D A L H O U S I E D A L H O U S I E P L A S T I C S U R G E R Y P L A S T I C S U R G E R Y
-
Upload
tomasurizar -
Category
Documents
-
view
235 -
download
1
description
Transferencias Para Paralisis Radial
Transcript of Transferencias Paralisis Radial

Tendon Transfers
Doug Humphreys
Division of Plastic Surgery
Dalhousie University
Halifax, Nova Scotia
DA
LH
OU
SIE
D
AL
HO
US
IE
PL
AS
TIC
P
LA
ST
IC
SU
RG
ER
YS
UR
GE
RY

Tendon Transfers
• Definition– The Detachment Of A Functioning Muscle-
Tendon Unit From Its Insertion And Reattachment To Another Tendon Or Bone To Replace The Function Of A Paralyzed Muscle Or Injured Tendon

Tendon Transfers
• Indications 1) Restore Function To A Muscle Paralyzed As
A Result Of Injury Of The Peripheral Nerves, Brachial Plexus Or Spinal Cord
2) To Restore Function After Closed Tendon Ruptures Or Open Injuries To The Tendons Or Muscles
3) Restore Balance To A Hand Deformed From Neurological Conditions

Tendon Transfers
• General Principles1) Straight Line Of Pull
2) Expendable Donor
3) Adequate Strength
4) Correction Of Contracture
5) One Tendon – One Function
6) Amplitude Of Motion
7) Synergism
8) Tissue Equilibrium

Tendon Transfers
1) Correction Of Contracture– Keep All Joints Supple
• Soft Tissue Contracture Easier To Prevent Than Correct
Stiff Joints Will Not Move!!

Tendon Transfers
2) Adequate Strength– Donor Strength Must Be
Adequate To Perform New Function In Its Altered Position• Work Of Muscle Related
To Muscle Volume
– Transferred Muscles Lose One Grade Of Strength
Tendon Transfers
3) Amplitude Of Motion– Wrist Flexors And Extensors
• 33mm
– Finger Extensors And EPL• 50mm
– Finger Flexors• 70mm
Tendon Transfers
3) Amplitude Of Motion– Augmentation Of Effective Amplitude
a) Convert From Monarticular To Multiarticular – Utilize Tenodesis
b) Dissection Of Surrounding Fascial Attachments

Tendon Transfers
4) Straight Line Of Pull– Most Efficient Transfer
5) One Tendon – One Function– Single Tendon Cannot Perform Two Opposite
Functions Simultaneously– May Insert Into More Than One Tendon
• FCU EDC
Tendon Transfers
6) Synergism– Easier To Retrain
7) Expendable Donor– Use Of Muscle Must Not Result In Unacceptable
Functional Loss
8) Tissue Equilibrium– No Transfer Should Be Done Unless Tissues In
Optimal Condition• Scars Soft, No Induration

Tendon Transfers
• Surgical Principles– Carefully Planned Incisions
• Tendons Should Not Lie Beneath Scars
– Careful Mobilization Of Muscles• Prevent Neurovascular Pedicle Damage
– Subcutaneous Tunneling Of Transfers• No Small Fascial Windows
Radial Nerve Palsy

Tendon TransfersRadial Nerve Palsy
• Functional Deficits– Wrist Extension– Finger Extension– Extension And Radial Abduction Of The
Thumb

Tendon TransfersRadial Nerve Palsy
• Timing Of Tendon Transfers– Controversial
• Early – Internal Splint At Time Of Nerve Repair
• Conventional– Performed After Reinnervation Of Paralyzed Muscles
Fails To Occur By 3 Months After Expected
• Late
Tendon TransfersRadial Nerve Palsy
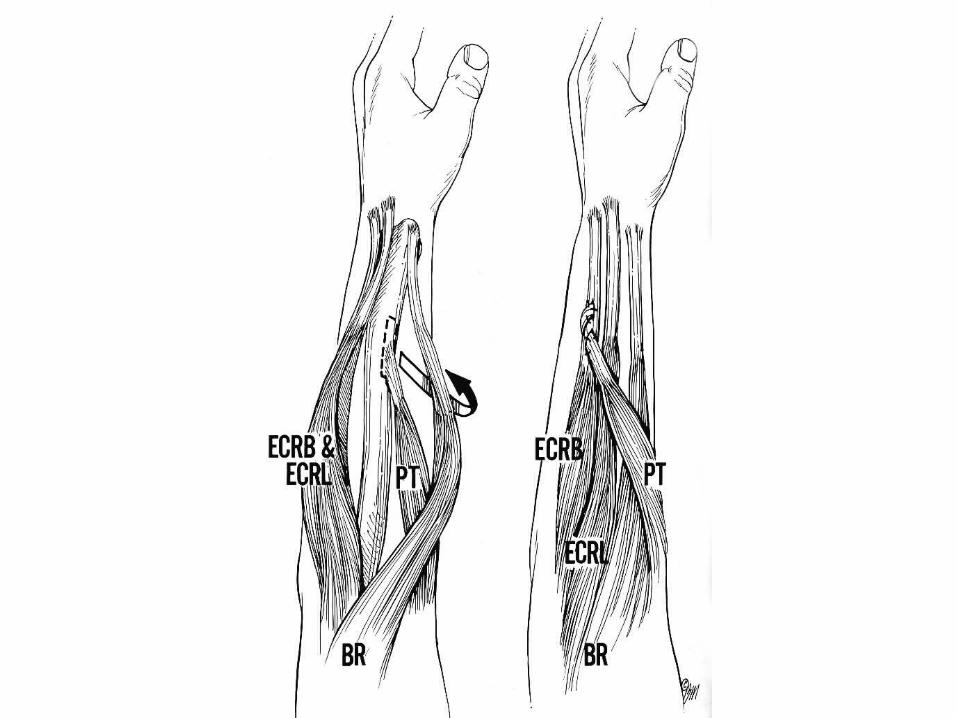
• Early Transfer– Pronator Teres to ECRB– Temporary Substitute Until Reinnervation– Suboptimal Reinnervation – Acts To Augment
Function
• Historical Perspective– Evolved During The Two World Wars– Classic Jones Transfer (1916)
• PT ECRL and ECRB
• FCU EDC III-V
• FCR EIP, EDC II, and EPL
Tendon TransfersRadial Nerve Palsy


Tendon TransfersRadial Nerve Palsy
FCU Transfer


• Incision 1:– FCU And PL Transected Proximally– FCU Freed Up Proximally
• Incision 2:– Deep Fascia Overlying FCU Incised And Muscle Freed
Proximally– Limit – Neurovascular Pedicle
• Incision 3:– Insertion Of PT Freed With Strip Of Periosteum– EPL Tendon Identified
Tendon TransfersRadial Nerve Palsy




Tendon TransfersRadial Nerve Palsy
• Setting The Proper Tension– Err On Suturing Extensor Tendons Tightly– PT ECRB
• Wrist 45° Extension
• Tendon Sutured With Maximal Tension
– FCU EDC • Wrist and MP Joints In Neutral
• Adjust EDC Tension Individually
• +/- EDM

Tendon TransfersRadial Nerve Palsy
• Setting The Proper Tension– PL EPL
• Wrist In Neutral• Maximal Tension On EPL And PL
• Test Passive ROM– Wrist In Extension
• Passively Flex Fingers Into Palm
– Wrist In Flexion• MP Joints In Full Extension• Should Not Hyperextend

Tendon TransfersRadial Nerve Palsy
• Postoperative Management– Splint For 4 Weeks
• Wrist 15-30° Pronation• Forearm 45° Extension• MP Joints Slight Flexion (10-15°)• Thumb – Maximal Extension And Abduction• PIP Joints – Left Free
– 4 To 6 Weeks• Removable Splint• Planned Exercise Program – With Therapist

Tendon TransfersRadial Nerve Palsy
• Potential Problems– Excessive Radial Deviation
– From Removing FCU– Further Aggravated If PT Inserted Into ECRL– Problem With PIN Palsy
• Solutions– FCU Transfer Contraindicated With PIN Palsy– Reinsert ECRL Into 4th Metacarpal
– Bowstringing Of EPL• Solution
– Hook EPL Around Insertion Of APL

Tendon TransfersRadial Nerve Palsy
• Potential Problems– Absence Of Palmaris Longus
• Solutions– Include Thumb Extrinsics In FCU EDC Transfer
» Violates One Tendon – One Function Principle
– Use Brachioradialis
» Possible Only With PIN Palsy
» Requires Extensive Freeing Up
» More Difficult To Reeducate
– Use FDS III Or IV

Tendon TransfersRadial Nerve Palsy
FCR Transfer(Starr, Brand, Tsuge)

Tendon TransfersRadial Nerve Palsy
• FCR EDC
• PT ECRB, When Required– Performed As Before
• PL EPL – Performed As Before– If Absent
• EPL Joined With EDC To FCR Transfer

Tendon TransfersRadial Nerve Palsy
• Incision – Between FCR And PL
• FCR Freed To Middle Of Forearm
• FCR Passed Around Radial Border– Subcutaneous Tunnel
• Two Best Tendons Sutured To FCR– Other Two Sutured To Neighbors
Sutured With Wrist & MP’s In Neutral

Tendon TransfersRadial Nerve Palsy
Superficialis Transfer(Boyes)

Tendon TransfersRadial Nerve Palsy
• PT ECRB
• FDS III EDC III,IV,V
• FDS IV EIP & EPL
• FRC APL & EPB
Tendon TransfersRadial Nerve Palsy
• PT Tendon Exposed– Volar – Radial Incision
• Sublimis Tendons Exposed– Transverse Incision Palm– Divided Proximal To Chiasm
Pass Tendons Through Interosseous Membrane Or Around Radial And Ulnar Borders
Tendon TransfersRadial Nerve Palsy
• Potential Problems– Protect Anterior And Posterior Interosseous
Arteries• One Opening On Either Side Of The Artery
– Avoid Kinking The Median Nerve• FDS III Routed To The Radial Side Of Profundus
– Between FDP And FPL
• FDS IV Routed To The Ulnar Side Of Profundus
Tendon TransfersRadial Nerve Palsy
• Transfer– FDS III
• EDC (Long, Ring and Little)
– FDS IV • EIP and EPL
Advantages– Independent Motion Of Thumb And Index
– Palmaris Absent


• Indian J Orthop. 2011 Nov-Dec; 45(6): 558–562.
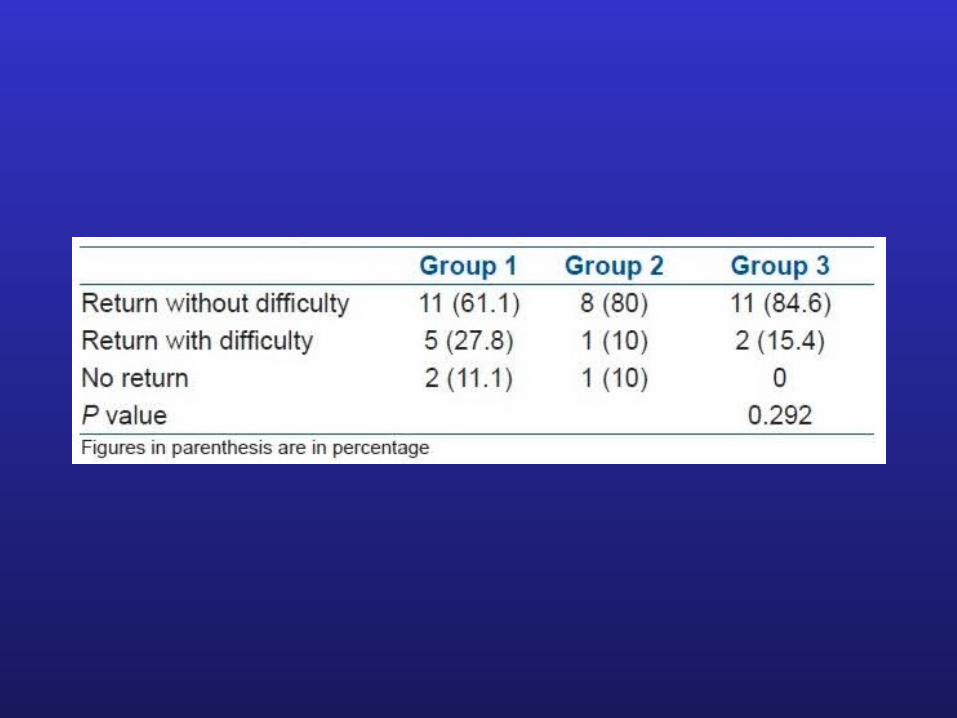
• Outcome of tendon transfer for radial nerve paralysis: Comparison of three methods
• Alia Ayatollahi Moussavi, Alireza Saied, and Ali Karbalaeikhani1

• 41 pacientes / 3 Grupos• FCU Extensión dedos
– PL EPL (Abducción y extensión D1)
• FCR Extensión dedos– PL EPL (Abducción y extensión D1)
• FDS 3º Extensión dedos– FDS 4º EPL
• En todos si se necesitaba restaurar extension muñeca: PT ECRB
• Si no tenian PL, eran excluidos

• Postop– Valva ABP con muñeca y dedos en extensión
por 4 semanas– Luego 3 meses nocturna– Fisioterapia desde el 1º mes
• Grupo 1– 18 Pacientes
• Grupo 2– 10 Pacientes
• Grupo 3– 13 Pacientes
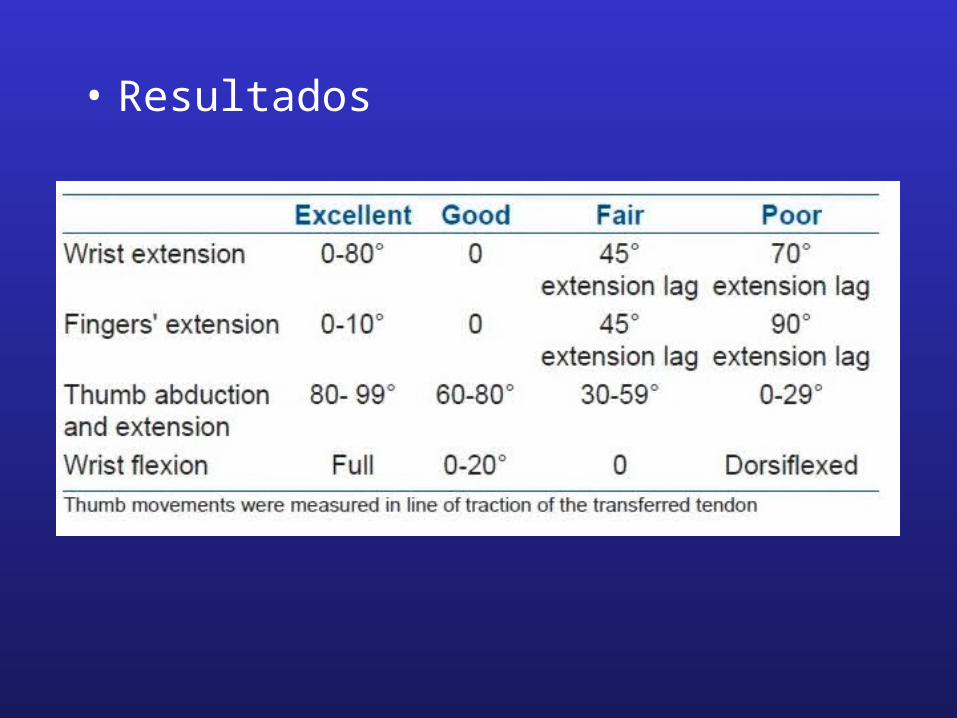
• Resultados

• Resultados
• Sin diferencias:– ROM muñeca, D1, dedos
– DASH: 35 / 38 / 30
• 95% Se volveria a operar• Extension simultanea de muñeca-dedos
– Solo 4 del grupo 3
• Contractura en flexion – 3 pacientes del grupo 3
• Pronosupinacion conservada en todos
• Varios presentaron disminución flexion muñeca– Ninguno lo reporto
• Todos lograron buen grip– No fue medido por falta de instrumentos
• Sin desviaciones radiales