Transcatheter Alcohol-Mediated Perivascular Renal...
10
PERIPHERAL Transcatheter Alcohol-Mediated Perivascular Renal Denervation With the Peregrine System First-in-Human Experience Tim A. Fischell, MD, a,b Adrian Ebner, MD, c Santiago Gallo, MD, c Fumiaki Ikeno, MD, d Laura Minarsch, RT, e Félix Vega, VMD, f Nicole Haratani, RN, BSN, b Vartan E. Ghazarossian, PHD b ABSTRACT OBJECTIVES This study evaluated the first clinical use of a new endovascular approach to renal denervation, using chemical neurolysis, via periadventitial infusion of dehydrated alcohol (ethanol) to perform “perivascular” renal artery sympathetic denervation. BACKGROUND Renal denervation remains a promising technology for the treatment of hypertension and other disorders. METHODS A novel 3-needle delivery device (Peregrine System Infusion Catheter, Ablative Solutions, Inc., Kalamazoo, Michigan) was introduced into the renal arteries of 18 subjects with refractory hypertension. Microdoses of alcohol were infused bilaterally via the 3 needles into to the adventitial space (0.30 ml/artery, 37 arteries). Renal artery angiography was performed at the time of the procedure and at 6 months (n ¼ 16). The primary safety endpoints were complications associated with the catheter insertion and delivery of the neurolytic agent or any major vascular access complications. The secondary performance endpoint was a reduction in office-based systolic blood pressure at 6 months compared with baseline. RESULTS Procedural success was achieved in 100% of subjects (N ¼ 18) and arteries (N ¼ 37). There were no study- related adverse clinical events at follow-up. One death of a subject was recorded but determined by the investigator and an independent medical monitor to be non–study related. There were no angiographic observations of renal artery stenosis, aneurysms, or other renal artery abnormalities at 6 months (32 renal arteries). Sixteen of the 18 subjects had a 6-month follow-up. The mean office systolic blood pressure decreased from 175 17 mm Hg to 151 26 mm Hg (24 mm Hg). There was an average reduction of antihypertensive medications from 3.4 (baseline) to 2.0 per subject at 6 months. CONCLUSIONS Chemical renal denervation using the infusion of very low doses of alcohol directly into the adventitial space appears to be feasible and safe. This approach may be a promising alternative approach to perform catheter-based renal denervation. These results need to be confirmed in larger scale clinical studies. (J Am Coll Cardiol Intv 2016; 9:589–98) © 2016 by the American College of Cardiology Foundation. From the a Borgess Heart Institute, Kalamazoo, Michigan; b Ablative Solutions, Inc., Kalamazoo, Michigan; c Sanatorio Italiano, Asunción, Paraguay; d Stanford University, Stanford, California; e MMC Medical, Laguna Beach, California; and f Preclinical Consultation, San Francisco, California. Ablative Solutions, Inc. provided funding for this study. Drs. Fischell and Ghazarossian are principals in and cofounders of Ablative Solutions and hold equity in the company. Dr. Vega and L. Minarsch are consultants to Ablative Solutions, Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received August 11, 2015; revised manuscript received November 22, 2015, accepted November 23, 2015. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 9, NO. 6, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jcin.2015.11.041
Transcript of Transcatheter Alcohol-Mediated Perivascular Renal...
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 5 . 1 1 . 0 4 1
PERIPHERAL
Transcatheter Alcohol-MediatedPerivascular Renal DenervationWith the Peregrine SystemFirst-in-Human Experience
Tim A. Fischell, MD,a,b Adrian Ebner, MD,c Santiago Gallo, MD,c Fumiaki Ikeno, MD,d Laura Minarsch, RT,e
Félix Vega, VMD,f Nicole Haratani, RN, BSN,b Vartan E. Ghazarossian, PHDb
ABSTRACT
Fro
As
Co
pri
Ab
dis
Ma
OBJECTIVES This study evaluated the first clinical use of a new endovascular approach to renal denervation, using
chemical neurolysis, via periadventitial infusion of dehydrated alcohol (ethanol) to perform “perivascular” renal artery
sympathetic denervation.
BACKGROUND Renal denervation remains a promising technology for the treatment of hypertension and other
disorders.
METHODS A novel 3-needle delivery device (Peregrine System Infusion Catheter, Ablative Solutions, Inc., Kalamazoo,
Michigan) was introduced into the renal arteries of 18 subjects with refractory hypertension. Microdoses of alcohol were
infused bilaterally via the 3 needles into to the adventitial space (0.30 ml/artery, 37 arteries). Renal artery angiography was
performed at the time of the procedure and at 6 months (n¼ 16). The primary safety endpoints were complications associated
with the catheter insertion and delivery of the neurolytic agent or any major vascular access complications. The secondary
performance endpoint was a reduction in office-based systolic blood pressure at 6 months compared with baseline.
RESULTS Procedural success was achieved in 100% of subjects (N ¼ 18) and arteries (N ¼ 37). There were no study-
related adverse clinical events at follow-up. One death of a subject was recorded but determined by the investigator and an
independent medical monitor to be non–study related. There were no angiographic observations of renal artery stenosis,
aneurysms, or other renal artery abnormalities at 6 months (32 renal arteries). Sixteen of the 18 subjects had a 6-month
follow-up. Themean office systolic blood pressure decreased from 175� 17mmHg to 151� 26mmHg (�24mmHg). There
was an average reduction of antihypertensive medications from 3.4 (baseline) to 2.0 per subject at 6 months.
CONCLUSIONS Chemical renal denervation using the infusion of very low doses of alcohol directly into the adventitial
space appears to be feasible and safe. This approach may be a promising alternative approach to perform catheter-based
renal denervation. These results need to be confirmed in larger scale clinical studies. (J Am Coll Cardiol Intv 2016;
9:589–98) © 2016 by the American College of Cardiology Foundation.
m the aBorgess Heart Institute, Kalamazoo, Michigan; bAblative Solutions, Inc., Kalamazoo, Michigan; cSanatorio Italiano,
unción, Paraguay; dStanford University, Stanford, California; eMMC Medical, Laguna Beach, California; and fPreclinical
nsultation, San Francisco, California. Ablative Solutions, Inc. provided funding for this study. Drs. Fischell and Ghazarossian are
ncipals in and cofounders of Ablative Solutions and hold equity in the company. Dr. Vega and L. Minarsch are consultants to
lative Solutions, Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to
close.
nuscript received August 11, 2015; revised manuscript received November 22, 2015, accepted November 23, 2015.

ABBR EV I A T I ON S
AND ACRONYMS
BP = blood pressure
eGFR = estimated glomerular
filtration rate
OBP = office-based blood
pressure
RF = radiofrequency
Fischell et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
Alcohol-Mediated Renal Denervation M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8
590
F rom the 1930s through the 1950s, sur-gical sympathectomy was used totreat severe hypertension (1–3).
Despite successful lowering of blood pres-sure (BP) observed with surgical denervation,this technique was abandoned due to rela-tively high morbidity and mortality and as aresult of the development of effective oralantihypertensive medications.
More recently, catheter-based renal sympatheticdenervation has been performed using a point-by-pointradiofrequency (RF) ablation catheters and ultra-sound ablation fromwithin the renal artery (4–11). Thistechnique has been shown to disrupt renal sympatheticnerve activity (4–7), resulting in significant and sus-tained reduction in BP in patients with severe andmedically refractory hypertension (4–14).
TABLE 1 Patient Inclusion Criteria
Adult patient, 18–75 years of age, male or female.
Patient has a clinic systolic blood pressure $160 mm Hg (or $150mm Hg in patients with type 2 diabetes) based on an average of3 office/clinic measurements taken manually.
Patient is on a stable medication regimen of at least 3 antihypertensivemedications of different classes (for at least 4 weeks), 1 of whichmust be a diuretic.
Patient has an estimated glomerular filtration rate $45 ml/min, basedon the chronic kidney disease–epidemiology equation.
Patient has suitable renal artery anatomy (no clear abnormalities)based on investigator’s evaluation of the angiogram includingsingle renal artery of 5 to 7 mm in diameter (2 arteries areacceptable if diameter of second artery is #2 mm), no renal arteryaneurysm(s), no excessive renal artery tortuosity, no previousstenting or balloon angioplasty of the renal arteries.
Patient has provided written informed consent.
SEE PAGE 599
Despite encouraging early results, the randomized,sham-controlled, SYMPLICITY HTN-3 (Renal Dener-vation in Patients With Uncontrolled Hypertension)study failed to demonstrate significant BP loweringcompared with the sham (15,16). Although these re-sults might have been unexpected based on the earlyand reproducible success with this technique, manyhave now pointed to a lack of adequate sympatheticdenervation, a lack of operator experience, as well ascomplexities related to medication adjustments andcompliance in both the treatment and sham groups aspossible causes of the trial’s failure (17,18).
Recent studies have also suggested that it may bechallenging to create adequate renal sympatheticdenervation with RF due to inconsistent circumfer-ential denervation and a lack of adequate depth ofnerve injury (19), particularly because the sympatheticnerves may traverse a course at distances of 10 to12 mm deep to the intimal surface (20,21). There mayalso be potential safety concerns associated with theuse of transmural thermal injury traversing the intimaland medial layers of the renal artery, particularly if amore aggressive ablation strategy is used (22–26).
In an attempt to overcome some of the perceivedlimitations of “energy-based” approaches, we devel-oped and reported encouraging pre-clinical resultsusing very small volumes of alcohol, a known potentneurolytic agent, delivered precisely and locally tothe adventitial space of the renal artery as a means toperform perivascular chemical renal sympatheticdenervation (27,28).
The purpose of the current study was to evaluatethe safety and feasibility of performing chemicalneurolysis via adventitial infusion of microdoses ofdehydrated alcohol as a means to perform renal artery
sympathetic denervation, in a first-in-human experi-ence, in patients with refractory hypertension.
METHODS
This was a first-in-human, single-center, pros-pective feasibility study intended to test thesafety of a novel 3-needle-based delivery device(Peregrine System Infusion Catheter, AblativeSolutions, Inc., Kalamazoo, Michigan) to performchemical renal sympathetic denervation in patientswith refractory hypertension, with the use of micro-doses (0.3 ml per renal artery) of dehydrated alcoholas the neurolytic agent.
The protocol for this study was reviewed andapproved by the Bioethics Committee of the Office ofthe Superintendent of Health, Paraguay. Nineteensubjects were enrolled after signing the EthicsCommittee-approved informed consent form. Theinclusion and exclusion criteria are outlined inTables 1 and 2 and are similar to those used in mostRF-based renal artery sympathetic denervation clin-ical trials at the time of this study (3–6,12). All subjectshad to have “resistant hypertension,” defined as anoffice-based systolic BP reading of >160 mm Hg (>150mm Hg if the subject had type 2 diabetes) while takingat least 3 antihypertensive medications, including adiuretic agent. There were no inclusion/exclusioncriteria in the study related to renal artery length.
Clinical and laboratory assessments were obtainedin-hospital and at 1, 3, and 6 months after bilateralrenal denervation. The primary safety data includedprocedure- and device-related adverse events andany post-procedure adverse cardiovascular orvascular complications, deterioration in renal func-tion, or renal artery abnormality at angiographicfollow-up at 6 months.
Baseline office-based BP (OBP) was measured atthe time of enrollment, pre- and post-procedure, and

TABLE 2 Patient Exclusion Criteria
Patient has known or suspected secondary hypertension.
Patient has type 1 diabetes mellitus.
Patient requires long-term oxygen support.
Patient has primary or secondary pulmonary hypertension.
Patient has a known bleeding diathesis or is taking anticoagulantdrugs during the 7 days before treatment.
Patient has thrombocytopenia (platelet count <100,000platelets/ml).
Patient is pregnant or nursing.
Patient has significant imaging-assessed renovascular abnormalitiesincluding short length of main renal artery (<1.5 cm), renal arterystenosis >70% of the normal diameter segment, andfibromuscular dysplasia.
Patient has history of nephrectomy, kidney tumor, or hydronephrosis.
Patient is known to have a unilateral nonfunctioning kidney or unequalrenal size (>2 cm difference in renal length between kidneys).
Patient has a renal transplant.
Patient has a history of kidney stones.
Patient has a history of heterogeneities in the kidney such as cystsand tumors.
Patient has a history of pyelonephritis.
Patient has a history of myocardial infarction, unstable anginapectoris, or cerebrovascular accident within the past 6 months.
Patient has hemodynamically significant valvular heart disease.
Patient has heart failure (New York Heart Association functionalclass III or IV) or has an ejection fraction #30%.
Patient has a known allergy to contrast media.
Patient has a life expectancy of <12 months.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6 Fischell et al.M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8 Alcohol-Mediated Renal Denervation
591
then at follow-up visits. OBP at each time point wasreported as the mean of 3 consecutive BP readings,taken 5 min apart and performed by study partici-pating site nurse or subinvestigator. AmbulatoryBP monitoring (ABPM) measurement was not avail-able at the trial site and was not included in thisstudy protocol. Subjects were instructed to maintaintheir medications at their pre-intervention dosesthroughout the 6-month follow-up period.
There were challenges in validating medicationcompliance, particularly after the renal denervationprocedure. Medication compliance data were evalu-able in 12 of the 16 evaluable subjects at 6-monthfollow-up. Laboratory measurements, includingroutine chemistry, blood urea nitrogen, creatinine,estimated glomerular filtration rate (eGFR), liverfunction tests, complete blood count, partial throm-boplastin time, international normalized ratio, andurine analysis, were obtained at baseline and at eachfollow-up visit. A 12-lead electrocardiogram was ob-tained at baseline, discharge, and 1-month follow-up.A central university-based (Stanford University) in-dependent qualified angiography reviewer read theangiographic renal artery studies from the time oftreatment for all 18 subjects (37 renal arteries) as wellas at the 6-month endpoint. A flow diagram for thestudy is shown in Figure 1.
PROCEDURE. The renal artery was engaged using a7-F guiding catheter, introduced via the femoralartery under fluoroscopic guidance. Intravenousunfractionated heparin was given to attain an acti-vated clotting time $250 s. Modest sedation per theinstitution’s standard practice was used in all caseswith relatively low doses of fentanyl and midazolam(50 mg and 5 mg, respectively, intravenously). Nogeneral anesthesia was used in any subject.
Angiography was performed of the renal arteriesbefore intervention. After the initial angiography, thePeregrine System Infusion Catheter was advancedthrough the guiding catheter and into the distal halfof the renal artery, typically at the midpoint.
The Peregrine System Infusion Catheter is usedunder fluoroscopic guidance by a single operator withstandard endovascular techniques and allows safe andreproducible fluid infusion into the adventitial andperiadventitial spaces of a target vessel (CentralIllustration, Figures 2 and 3). The three 0.008-inch(220-mm) needles of the Peregrine catheter are con-tained in a pre-deployment state within the guidetubes. Once deployed, the 3 guide tubes, spaced 120�
apart, are moved outward and serve to reproducibly“center” and stabilize the device within the renalartery (Central Illustration, Figures 2 and 3). Theseatraumatic tubes have radiopaque distal tip markers toclearly define the position of the tubes (Figure 3C). Thepredictable 360� spread of neurolytic agent (alcohol)has been confirmed in pre-clinical testing (27).
Once the infusion (distal) section of the device waspositioned within the target site, the 3 guide tubeswere simultaneously deployed against the intimalsurface using the advancement mechanism in thecontrol handle (Central Illustration, Figure 3C). Thespecialized handle was then used to simultaneouslyadvance the three 0.008-inch needles. These micro-needles are radiopaque so that they can be easily seenunder fluoroscopy (Figure 3D). The needles wereadvanced to their pre-set depth of 3.5 � 0.25 mm deepto the intima (i.e., beyond the tip of the guide tube)and into the adventitial space. This allows an infusiondepth that approximates the border between therenal artery adventitia and periadventitia and thatcorresponds to a depth of the middle of the renalsympathetic nerve field, as observed in pressure-fixed human histopathological studies (20,21). Usingthis technique, it is essentially impossible to infusethe alcohol into the renal artery lumen.
The neurolytic agent (0.3 ml of dehydrated alcoholinjection, USP (Akorn, Inc., Lake Forest, Illinois) wasthen delivered with a 60-s infusion using a 1-ml Luer-lock syringe, connected at infusion port located at theproximal end of the handle. Once the alcohol was
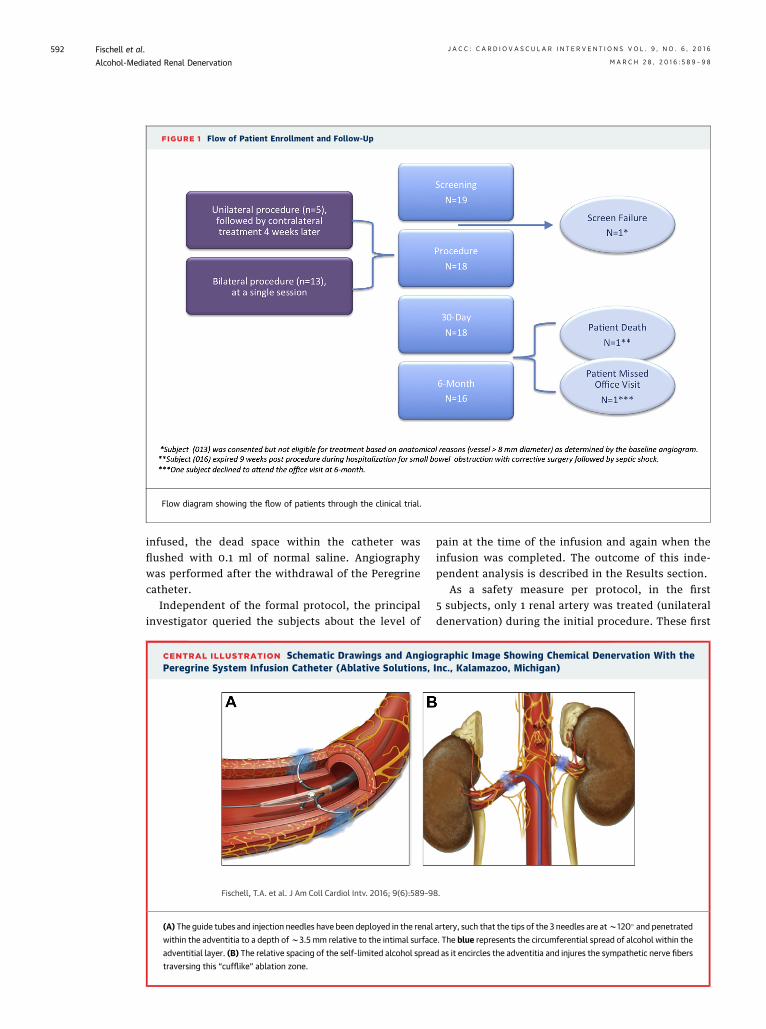
FIGURE 1 Flow of Patient Enrollment and Follow-Up
Flow diagram showing the flow of patients through the clinical trial.
Fischell et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
Alcohol-Mediated Renal Denervation M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8
592
infused, the dead space within the catheter wasflushed with 0.1 ml of normal saline. Angiographywas performed after the withdrawal of the Peregrinecatheter.
Independent of the formal protocol, the principalinvestigator queried the subjects about the level of
CENTRAL ILLUSTRATION Schematic Drawings and AngioPeregrine System Infusion Catheter (Ablative Solutions,
Fischell, T.A. et al. J Am Coll Cardiol Intv. 2016; 9(6):589–9
(A) The guide tubes and injection needles have been deployed in the renal
within the adventitia to a depth ofw3.5 mm relative to the intimal surfac
adventitial layer. (B) The relative spacing of the self-limited alcohol sprea
traversing this “cufflike” ablation zone.
pain at the time of the infusion and again when theinfusion was completed. The outcome of this inde-pendent analysis is described in the Results section.
As a safety measure per protocol, in the first5 subjects, only 1 renal artery was treated (unilateraldenervation) during the initial procedure. These first
graphic Image Showing Chemical Denervation With theInc., Kalamazoo, Michigan)
8.
artery, such that the tips of the 3 needles are atw120� and penetrated
e. The blue represents the circumferential spread of alcohol within the
d as it encircles the adventitia and injures the sympathetic nerve fibers
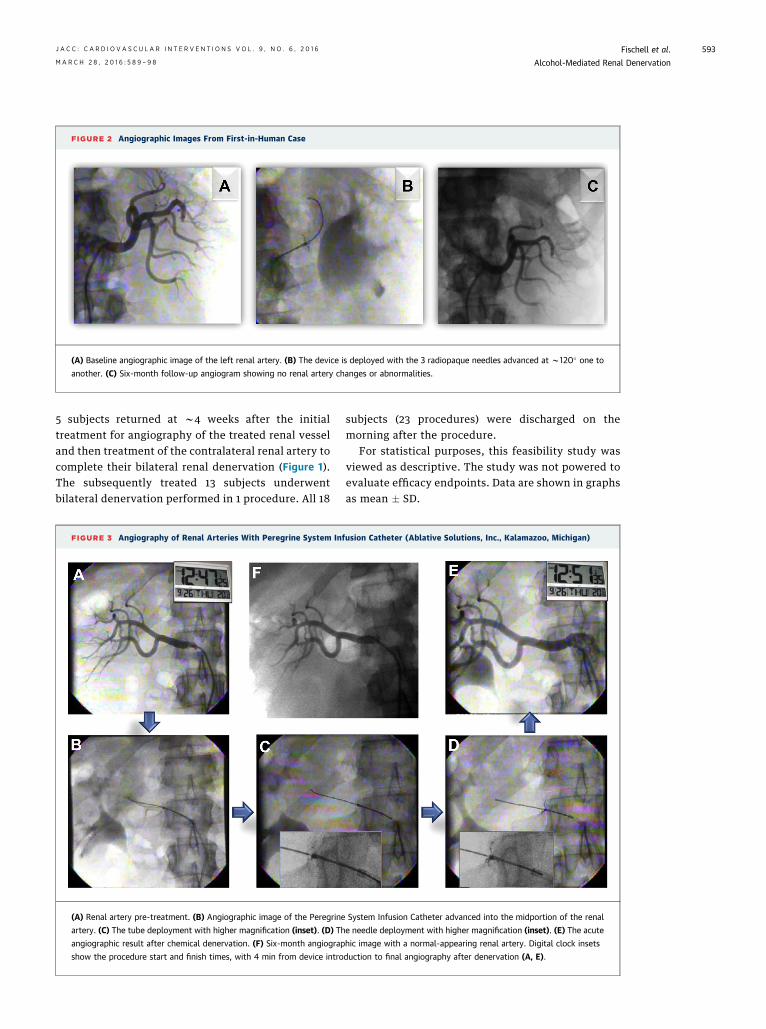
FIGURE 2 Angiographic Images From First-in-Human Case
(A) Baseline angiographic image of the left renal artery. (B) The device is deployed with the 3 radiopaque needles advanced at w120� one to
another. (C) Six-month follow-up angiogram showing no renal artery changes or abnormalities.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6 Fischell et al.M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8 Alcohol-Mediated Renal Denervation
593
5 subjects returned at w4 weeks after the initialtreatment for angiography of the treated renal vesseland then treatment of the contralateral renal artery tocomplete their bilateral renal denervation (Figure 1).The subsequently treated 13 subjects underwentbilateral denervation performed in 1 procedure. All 18
FIGURE 3 Angiography of Renal Arteries With Peregrine System In
(A) Renal artery pre-treatment. (B) Angiographic image of the Peregrine
artery. (C) The tube deployment with higher magnification (inset). (D) Th
angiographic result after chemical denervation. (F) Six-month angiograp
show the procedure start and finish times, with 4 min from device intro
subjects (23 procedures) were discharged on themorning after the procedure.
For statistical purposes, this feasibility study wasviewed as descriptive. The study was not powered toevaluate efficacy endpoints. Data are shown in graphsas mean � SD.
fusion Catheter (Ablative Solutions, Inc., Kalamazoo, Michigan)
System Infusion Catheter advanced into the midportion of the renal
e needle deployment with higher magnification (inset). (E) The acute
hic image with a normal-appearing renal artery. Digital clock insets
duction to final angiography after denervation (A, E).
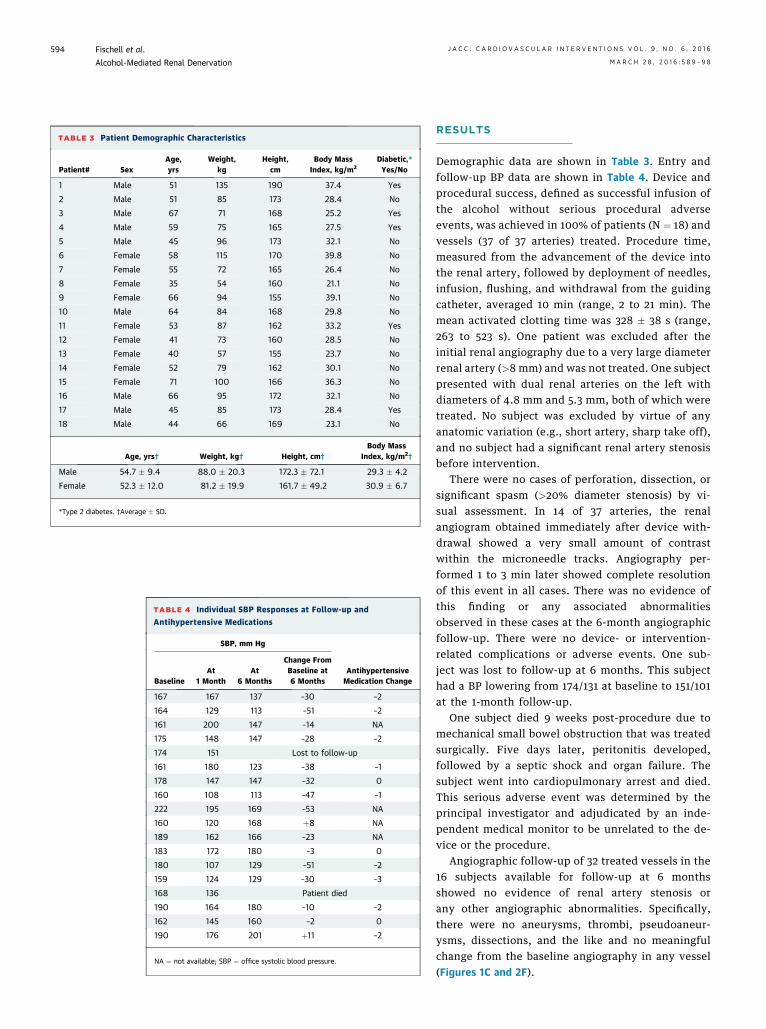
TABLE 3 Patient Demographic Characteristics
Patient# SexAge,yrs
Weight,kg
Height,cm
Body MassIndex, kg/m2
Diabetic,*Yes/No
1 Male 51 135 190 37.4 Yes
2 Male 51 85 173 28.4 No
3 Male 67 71 168 25.2 Yes
4 Male 59 75 165 27.5 Yes
5 Male 45 96 173 32.1 No
6 Female 58 115 170 39.8 No
7 Female 55 72 165 26.4 No
8 Female 35 54 160 21.1 No
9 Female 66 94 155 39.1 No
10 Male 64 84 168 29.8 No
11 Female 53 87 162 33.2 Yes
12 Female 41 73 160 28.5 No
13 Female 40 57 155 23.7 No
14 Female 52 79 162 30.1 No
15 Female 71 100 166 36.3 No
16 Male 66 95 172 32.1 No
17 Male 45 85 173 28.4 Yes
18 Male 44 66 169 23.1 No
Age, yrs† Weight, kg† Height, cm†
Body MassIndex, kg/m2
†
Male 54.7 � 9.4 88.0 � 20.3 172.3 � 72.1 29.3 � 4.2
Female 52.3 � 12.0 81.2 � 19.9 161.7 � 49.2 30.9 � 6.7
*Type 2 diabetes. †Average � SD.
TABLE 4 Individual SBP Responses at Follow-up and
Antihypertensive Medications
SBP, mm Hg
AntihypertensiveMedication ChangeBaseline
At1 Month
At6 Months
Change FromBaseline at6 Months
167 167 137 –30 –2
164 129 113 –51 –2
161 200 147 –14 NA
175 148 147 –28 –2
174 151 Lost to follow-up
161 180 123 –38 –1
178 147 147 –32 0
160 108 113 –47 –1
222 195 169 –53 NA
160 120 168 þ8 NA
189 162 166 –23 NA
183 172 180 –3 0
180 107 129 –51 –2
159 124 129 –30 –3
168 136 Patient died
190 164 180 –10 –2
162 145 160 –2 0
190 176 201 þ11 –2
NA ¼ not available; SBP ¼ office systolic blood pressure.
Fischell et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
Alcohol-Mediated Renal Denervation M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8
594
RESULTS
Demographic data are shown in Table 3. Entry andfollow-up BP data are shown in Table 4. Device andprocedural success, defined as successful infusion ofthe alcohol without serious procedural adverseevents, was achieved in 100% of patients (N ¼ 18) andvessels (37 of 37 arteries) treated. Procedure time,measured from the advancement of the device intothe renal artery, followed by deployment of needles,infusion, flushing, and withdrawal from the guidingcatheter, averaged 10 min (range, 2 to 21 min). Themean activated clotting time was 328 � 38 s (range,263 to 523 s). One patient was excluded after theinitial renal angiography due to a very large diameterrenal artery (>8 mm) and was not treated. One subjectpresented with dual renal arteries on the left withdiameters of 4.8 mm and 5.3 mm, both of which weretreated. No subject was excluded by virtue of anyanatomic variation (e.g., short artery, sharp take off),and no subject had a significant renal artery stenosisbefore intervention.
There were no cases of perforation, dissection, orsignificant spasm (>20% diameter stenosis) by vi-sual assessment. In 14 of 37 arteries, the renalangiogram obtained immediately after device with-drawal showed a very small amount of contrastwithin the microneedle tracks. Angiography per-formed 1 to 3 min later showed complete resolutionof this event in all cases. There was no evidence ofthis finding or any associated abnormalitiesobserved in these cases at the 6-month angiographicfollow-up. There were no device- or intervention-related complications or adverse events. One sub-ject was lost to follow-up at 6 months. This subjecthad a BP lowering from 174/131 at baseline to 151/101at the 1-month follow-up.
One subject died 9 weeks post-procedure due tomechanical small bowel obstruction that was treatedsurgically. Five days later, peritonitis developed,followed by a septic shock and organ failure. Thesubject went into cardiopulmonary arrest and died.This serious adverse event was determined by theprincipal investigator and adjudicated by an inde-pendent medical monitor to be unrelated to the de-vice or the procedure.
Angiographic follow-up of 32 treated vessels in the16 subjects available for follow-up at 6 monthsshowed no evidence of renal artery stenosis orany other angiographic abnormalities. Specifically,there were no aneurysms, thrombi, pseudoaneur-ysms, dissections, and the like and no meaningfulchange from the baseline angiography in any vessel(Figures 1C and 2F).
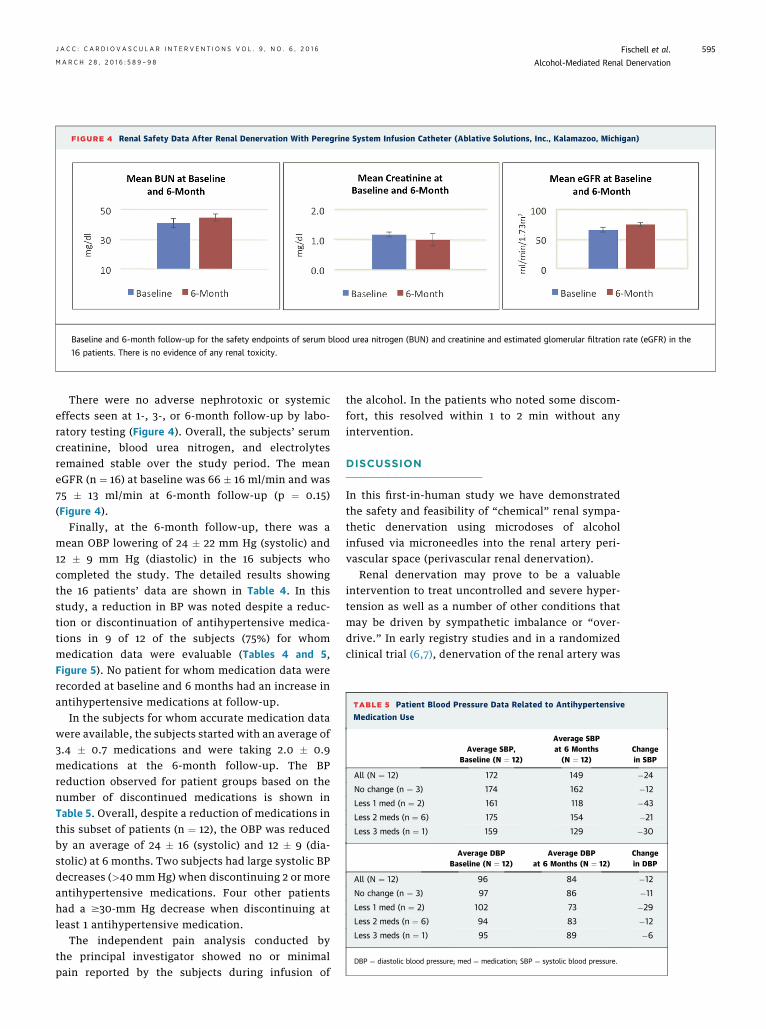
FIGURE 4 Renal Safety Data After Renal Denervation With Peregrine System Infusion Catheter (Ablative Solutions, Inc., Kalamazoo, Michigan)
Baseline and 6-month follow-up for the safety endpoints of serum blood urea nitrogen (BUN) and creatinine and estimated glomerular filtration rate (eGFR) in the
16 patients. There is no evidence of any renal toxicity.
TABLE 5 Patient Blood Pressure Data Related to Antihypertensive
Medication Use
Average SBP,Baseline (N ¼ 12)
Average SBPat 6 Months(N ¼ 12)
Changein SBP
All (N ¼ 12) 172 149 �24
No change (n ¼ 3) 174 162 �12
Less 1 med (n ¼ 2) 161 118 �43
Less 2 meds (n ¼ 6) 175 154 �21
Less 3 meds (n ¼ 1) 159 129 �30
Average DBPBaseline (N ¼ 12)
Average DBPat 6 Months (N ¼ 12)
Changein DBP
All (N ¼ 12) 96 84 �12
No change (n ¼ 3) 97 86 �11
Less 1 med (n ¼ 2) 102 73 �29
Less 2 meds (n ¼ 6) 94 83 �12
Less 3 meds (n ¼ 1) 95 89 �6
DBP ¼ diastolic blood pressure; med ¼ medication; SBP ¼ systolic blood pressure.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6 Fischell et al.M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8 Alcohol-Mediated Renal Denervation
595
There were no adverse nephrotoxic or systemiceffects seen at 1-, 3-, or 6-month follow-up by labo-ratory testing (Figure 4). Overall, the subjects’ serumcreatinine, blood urea nitrogen, and electrolytesremained stable over the study period. The meaneGFR (n ¼ 16) at baseline was 66 � 16 ml/min and was75 � 13 ml/min at 6-month follow-up (p ¼ 0.15)(Figure 4).
Finally, at the 6-month follow-up, there was amean OBP lowering of 24 � 22 mm Hg (systolic) and12 � 9 mm Hg (diastolic) in the 16 subjects whocompleted the study. The detailed results showingthe 16 patients’ data are shown in Table 4. In thisstudy, a reduction in BP was noted despite a reduc-tion or discontinuation of antihypertensive medica-tions in 9 of 12 of the subjects (75%) for whommedication data were evaluable (Tables 4 and 5,Figure 5). No patient for whom medication data wererecorded at baseline and 6 months had an increase inantihypertensive medications at follow-up.
In the subjects for whom accurate medication datawere available, the subjects started with an average of3.4 � 0.7 medications and were taking 2.0 � 0.9medications at the 6-month follow-up. The BPreduction observed for patient groups based on thenumber of discontinued medications is shown inTable 5. Overall, despite a reduction of medications inthis subset of patients (n ¼ 12), the OBP was reducedby an average of 24 � 16 (systolic) and 12 � 9 (dia-stolic) at 6 months. Two subjects had large systolic BPdecreases (>40 mm Hg) when discontinuing 2 or moreantihypertensive medications. Four other patientshad a $30-mm Hg decrease when discontinuing atleast 1 antihypertensive medication.
The independent pain analysis conducted bythe principal investigator showed no or minimalpain reported by the subjects during infusion of
the alcohol. In the patients who noted some discom-fort, this resolved within 1 to 2 min without anyintervention.
DISCUSSION
In this first-in-human study we have demonstratedthe safety and feasibility of “chemical” renal sympa-thetic denervation using microdoses of alcoholinfused via microneedles into the renal artery peri-vascular space (perivascular renal denervation).
Renal denervation may prove to be a valuableintervention to treat uncontrolled and severe hyper-tension as well as a number of other conditions thatmay be driven by sympathetic imbalance or “over-drive.” In early registry studies and in a randomizedclinical trial (6,7), denervation of the renal artery was
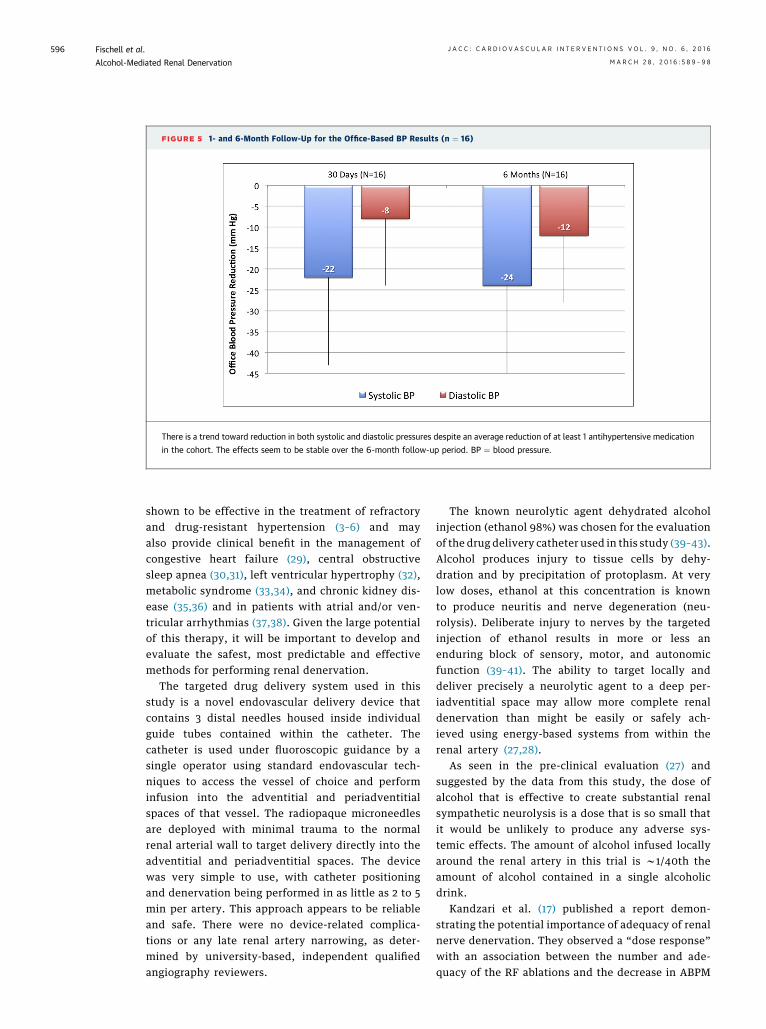
FIGURE 5 1- and 6-Month Follow-Up for the Office-Based BP Results (n ¼ 16)
There is a trend toward reduction in both systolic and diastolic pressures despite an average reduction of at least 1 antihypertensive medication
in the cohort. The effects seem to be stable over the 6-month follow-up period. BP ¼ blood pressure.
Fischell et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
Alcohol-Mediated Renal Denervation M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8
596
shown to be effective in the treatment of refractoryand drug-resistant hypertension (3–6) and mayalso provide clinical benefit in the management ofcongestive heart failure (29), central obstructivesleep apnea (30,31), left ventricular hypertrophy (32),metabolic syndrome (33,34), and chronic kidney dis-ease (35,36) and in patients with atrial and/or ven-tricular arrhythmias (37,38). Given the large potentialof this therapy, it will be important to develop andevaluate the safest, most predictable and effectivemethods for performing renal denervation.
The targeted drug delivery system used in thisstudy is a novel endovascular delivery device thatcontains 3 distal needles housed inside individualguide tubes contained within the catheter. Thecatheter is used under fluoroscopic guidance by asingle operator using standard endovascular tech-niques to access the vessel of choice and performinfusion into the adventitial and periadventitialspaces of that vessel. The radiopaque microneedlesare deployed with minimal trauma to the normalrenal arterial wall to target delivery directly into theadventitial and periadventitial spaces. The devicewas very simple to use, with catheter positioningand denervation being performed in as little as 2 to 5min per artery. This approach appears to be reliableand safe. There were no device-related complica-tions or any late renal artery narrowing, as deter-mined by university-based, independent qualifiedangiography reviewers.
The known neurolytic agent dehydrated alcoholinjection (ethanol 98%) was chosen for the evaluationof the drug delivery catheter used in this study (39–43).Alcohol produces injury to tissue cells by dehy-dration and by precipitation of protoplasm. At verylow doses, ethanol at this concentration is knownto produce neuritis and nerve degeneration (neu-rolysis). Deliberate injury to nerves by the targetedinjection of ethanol results in more or less anenduring block of sensory, motor, and autonomicfunction (39–41). The ability to target locally anddeliver precisely a neurolytic agent to a deep per-iadventitial space may allow more complete renaldenervation than might be easily or safely ach-ieved using energy-based systems from within therenal artery (27,28).
As seen in the pre-clinical evaluation (27) andsuggested by the data from this study, the dose ofalcohol that is effective to create substantial renalsympathetic neurolysis is a dose that is so small thatit would be unlikely to produce any adverse sys-temic effects. The amount of alcohol infused locallyaround the renal artery in this trial is w1/40th theamount of alcohol contained in a single alcoholicdrink.
Kandzari et al. (17) published a report demon-strating the potential importance of adequacy of renalnerve denervation. They observed a “dose response”with an association between the number and ade-quacy of the RF ablations and the decrease in ABPM

PERSPECTIVES
WHAT IS KNOWN? Renal denervation remains a promising
technology for the treatment of hypertension and other disor-
ders. Recent results from radiofrequency-based renal denerva-
tion have cast questions regarding the efficacy of renal
denervation.
WHAT IS NEW? We evaluated the first clinical use of a new
endovascular approach to renal denervation, using chemical
neurolysis, via peri-adventitial infusion of dehydrated alcohol
(ethanol) to perform “perivascular” renal artery sympathetic
denervation. Chemical renal denervation may provide a safe
alternative to radiofrequency (thermal) renal denervation and
may allow more consistent renal denervation.
WHAT IS NEXT? Additional clinical evaluation of renal dener-
vation, in general, and chemical renal denervation, will be
required using ABPM and randomized and sham controlled trials
to further evaluate the safety and efficacy of renal denervation.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6 Fischell et al.M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8 Alcohol-Mediated Renal Denervation
597
in a post-hoc analysis of the SYMPLICITY HTN-3 re-sults. Thus, it is likely that a lack of adequate depth ofnerve injury and a lack of predictable circumferentialnerve ablation may lead to inadequate denervation insome patients when using RF systems (17,18,20,21).
The histopathology from the preclinical evaluationof alcohol infusion demonstrated predictable andcircumferential renal sympathetic nerve injury, withnearly complete sparing of injury to the intimaand media of the renal artery, using doses of 0.15 to0.6 ml of alcohol per artery (27). The ability to pre-dictably damage the renal sympathetic nerves in adose-dependent fashion using very low volumes ofalcohol delivered in the adventitial space and withminimal or no injury to the normal renal arterial wallstructures is appealing. However, these pre-clinicaldata also suggest that while the dose used in this first-in-humans study (0.3 ml/artery) represents a safedose with a signal of efficacy, a dose of 0.6 ml/arteryhas shown similar safety and superior efficacy (27).Further clinical testing using this higher dose will beof interest.
Although there are limitations using thermal abla-tion for renal denervation, it remains to be determinedhow effectively chemical denervationwith alcoholwillovercome these drawbacks. However, the pre-clinicaldata and these early clinical data from the currentstudy are encouraging and suggest that chemicaldenervation with microdoses of alcohol is safe andessentially painless and may effectively reduce BP inpatients with resistant hypertension, even in the faceof a reduction of antihypertensive medications.
STUDY LIMITATIONS. This was intended as a safetyand feasibility study. As a result, there are limitationsin assessing efficacy and OBP lowering due to thesmall sample size of this study. There were also noABPM measurements and no separate control group.The dose chosen for the study (0.3 ml/artery),although showing good safety and a signal forefficacy, may be improved on by using a higherdose. Finally, compliance with antihypertensivemedication treatment was inconsistent and mayhave created a negative bias due to the self-discontinuation of medications by many of the pa-tients after their procedure(s).
CONCLUSIONS
We report the first clinical use of adventitial, targetedlocal delivery of very low doses of a neurolytic agent,dehydrated alcohol, to perform renal sympatheticdenervation. These data suggest that chemical “peri-vascular” renal denervation with alcohol is a feasibleand safe alternative to energy-based renal denerva-tion. Additional blinded, randomized clinical trials,with the addition of control patients and ABPM mea-surements, will be necessary to further evaluate thisrenal denervation therapy.
ACKNOWLEDGMENTS The authors acknowledgeYoshiaki Mitsutake, MD, PHD, Stanford University;Wook Bum Pyun, MD, PHD, Ewha Womans University,Seoul, South Korea; Agility Medical; and the experttechnical contributions of Darren Kent, Jeff A. Burke,and Phil C. Burke, REV-1 Engineering.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Tim A. Fischell, Michigan State University, Borgess HeartInstitute, 1521 Gull Road, Kalamazoo, Michigan 49048.E-mail: [email protected].
RE F E RENCE S
1. Harris SH. Renal sympathectomy: its scopeand limitations. Proc R Soc Med 1935;28:1497–510.
2. Smithwick RH, Thompson JE. Splanchnicectomyfor essential hypertension; results in 1,266 cases.JAMA 1953;152:1501–4.
3. Schlaich MP, Sobotka PA, Krum H, et al. Renaldenervation as a therapeutic approach for hyper-tension: novel implications for an old concept.Hypertension 2009;54:1195–201.
4. Krum H, Schlaich M, Whitbourn R, et al.Catheter-based renal sympathetic denervation for
resistant hypertension: a multicentre safety andproof-of-principle cohort study. Lancet 2009;373:1275–81.
5. SYMPLICITY HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistanthypertension: durability of blood pressure
Fischell et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 6 , 2 0 1 6
Alcohol-Mediated Renal Denervation M A R C H 2 8 , 2 0 1 6 : 5 8 9 – 9 8
598
reduction out to 24 Months. Hypertension 2011;57:911–7.
6. SYMPLICITY HTN-2 Investigators, Esler MD,Krum H, Sobotka PA, Schlaich MP, Schmieder RE,Böhm M. Renal sympathetic denervation in pa-tients with treatment-resistant hypertension (TheSymplicity HTN-2 Trial): a randomised controlledtrial. Lancet 2010;376:1903–9.
7. Sakakura K, Roth A, Ladich E, et al. Controlledcircumferential renal sympathetic denervationwith preservation for the renal arterial wall usingintraluminal ultrasound: a next generationapproach for treating sympathetic overactivity.EuroIntervention 2015;10:1230–8.
8. Kandzari DE, Bhatt DL, Sobotka PA, et al.Catheter-based renal denervation for resistant hy-pertension: rationale and design of the SYMPLICITYHTN-3 trial. Clin Cardiol 2012;35:528–35.
9. Mahfoud F, Cremers B, Janker J, Link B,Vonend O, Ukena C. Renal hemodynamics andrenal function after catheter-based renal sympa-thetic denervation in patients with resistant hy-pertension. Hypertension 2012;60:419–24.
10. Krum H, Schlaich M, Sobotka P, et al. Device-based antihypertensive therapy: therapeuticmodulation of the autonomic nervous system.Circulation 2011;123:209–15.
11. Lambert GW, Hering D, Esler MD, et al. Health-related quality of life after renal denervation inpatients with treatment-resistant hypertension.Hypertension 2012;60:1479–84.
12. Ormiston JA, Watson T, van Pelt N, et al. First-in-human use of the OneShot� renal denervationsystem from Covidien. EuroIntervention 2013;8:1090–4.
13. Schlaich MP, Hering D, Sobotka PA, et al. Renaldenervation in human hypertension: mechanisms,current findings, and future prospects. CurrHypertens Rep 2012;14:247–53.
14. Schlaich MP, Krum H, Sobotka PA, Esler MD.Renal denervation and hypertension. Am JHypertens 2011;24:635–42.
15. Bhatt DL, Kandzari DE, O’Neill WW, et al.A controlled trial of renal denervation for resistanthypertension. N Engl J Med 2014;370:1393–401.
16. Bakris G, Townsend R, Liu M, et al.,SYMPLICITY HTN-3 Investigators. Impact of renaldenervation on 24-hour ambulatory blood pres-sure: results from SYMPLICITY HTN-3. J Am CollCardiol 2014;64:1071–8.
17. Kandzari DE, Bhatt DL, Brar S, et al. Predictorsof blood pressure response in the SYMPLICITYHTN-3 trial. Eur Heart J 2015;36:219–27.
18. Papademetriou V. Renal denervation for drug-resistant hypertension: there is still hope. Car-diovasc Revasc Med 2015;16:202–3.
19. Vink EE, Goldschmeding R, Vink A,Weggemans C, Belijs RL, Blankestijn PJ. Limiteddestruction of renal nerves after catheter-basedrenal denervation: results of a human case study.Nephrol Dial Transplant 2014;29:1608–10.
20. Tzafriri A, Mahfoud F, Keating JH, et al.Innervation patterns may limit response to endo-vascular renal denervation. J Am Coll Cardiol2014;64:1079–87.
21. Sakakura K, Ladich E, Cheng Q, et al. Anatomicassessment of sympathetic peri-arterial renalnerves in man. J Am Coll Cardiol 2014;64:635–43.
22. Karanasos A, Van Mieghem NV, Bergmann MW,et al. Multimodality intra-arterial imaging as-sessment of the vascular trauma induced byballoon-based and nonballoon based renal dener-vation systems. Circ Cardiovasc Interv 2015;8:e002474.
23. Kaltenbach B, Id D, Franke JC, et al. Renalartery stenosis after renal sympathetic denerva-tion. J Am Coll Cardiol 2012;60:2694–5.
24. Persu A, Sapoval M, Azizi M, et al. Renal arterystenosis following renal denervation: a matter ofconcern. J Hypertens 2014;32:2101–5.
25. Vonend O, Antoch G, Rump LC, et al. Sec-ondary rise in blood pressure after renal dener-vation. Lancet 2012;380:778.
26. Versaci F, Trivisonno A, Olivieri C, et al. Laterenal artery stenosis after renal denervation: is itthe tip of the iceberg? Int J Cardiol 2014;174:406–7.
27. Fischell TA, Vega F, Raju N, et al. Ethanol-mediated perivascular renal sympathetic dener-vation preclinical validation of safety and efficacyin a porcine model. EuroIntervention 2013;9:140–7.
28. Fischell TA, Fischell DR, Ghazarossian VE,et al. Next generation renal denervation: chemical“perivascular” renal denervation with alcohol us-ing a novel drug infusion catheter. CardiovascRevasc Med 2015;16:221–7.
29. Sobotka PA, Krum H, Bohm M, et al. The roleof renal denervation in the treatment of heartfailure. Curr Cardiol Rep 2012;14:285–92.
30. Linz D, Mahfoud F, Schotten U, et al. Renalsympathetic denervation suppresses postapneicblood pressure rises and atrial fibrillation in amodel for sleep apnea. Hypertension 2012;60:172–8.
31. Witkowski A, Prejbisz A, Florczak E, et al.Effects of renal sympathetic denervation onblood pressure, sleep apnea course, and glyce-mic control in patients with resistant hyperten-sion and sleep apnea. Hypertension 2011;58:559–65.
32. Brandt MC, Mahfoud F, Reda S, et al. Renalsympathetic denervation reduces left ventricular
hypertrophy and improves cardiac function in pa-tients with resistant hypertension. J Am Coll Car-diol 2012;59:901–9.
33. Schlaich MP, Hering D, Sobotka P, et al.Effects of renal denervation on sympathetic acti-vation, blood pressure, and glucose metabolism inpatients with resistant hypertension. Front Physiol2012;3:10.
34. Mahfoud F, Schlaich M, Kindermann I, et al.Effect of renal sympathetic denervation onglucose metabolism in patients with resistant hy-pertension: a pilot study. Circulation 2011;123:1940–6.
35. Schlaich MP, Bart B, Hering D, et al. Feasibilityof catheter-based renal nerve ablation and effectson sympathetic nerve activity and blood pressurein patients with end-stage renal disease. Int JCardiol 2013;168:2214–20.
36. Hering D, Mahfoud F, Walton AS, et al. Renaldenervation in moderate to severe CKD. J Am SocNephrol 2012;23:1250–7.
37. Linz D, Mahfoud F, Schotten U, et al. Renalsympathetic denervation provides ventricular ratecontrol but does not prevent atrial electricalremodeling during atrial fibrillation. Hypertension2013;61:225–31.
38. Ukena C, Bauer A, Mahfoud F, et al. Renalsympathetic denervation for treatment of elec-trical storm: first-in-man experience. Clin ResCardiol 2012;101:63–7.
39. Moller JE, Helweg-Larsen J, Jacobsen E. His-topathological lesions in the sciatic nerve of therat following perineural application of phenol andalcohol solutions. Danish Med Bull 1969;16:116–9.
40. Streitparth F, Walter A, Stolzenburg N, et al.MR-guided periarterial ethanol injection for renalsympathetic denervation: a feasibility study inpigs. Cardiovasc Intervent Radiol 2013;36:791–6.
41. Wali FA, Suer AH, Hayter A, Tugwell AC. Theeffect of ethanol on spontaneous contractions andon the contraction produced by periarterial nervestimulation and by acetylcholine in the rat isolatedileum. Gen Pharmacol 1987;18:631–5.
42. Kocabas H, Salli A, Demir AH, Ozerbil OM.Comparison of phenol and alcohol neurolysis oftibial nerve motor branches to the gastrocnemiusmuscle for treatment of spastic foot after stroke: arandomized controlled pilot study. Eur J PhysRehabil Med 2010;46:5–10.
43. Wilkes D, Ganceres N, Doulatram G, Solanki D.Alcohol neurolysis of the sciatic and femoralnerves to improve pressure ulcer healing. PainPract 2009;9:145–9.
KEY WORDS adventitial, alcohol, chemical,ethanol, first-in-human, neurolysis, renaldenervation, sympathetic nerves