TRAINING MANUAL FOR STATE & DISTRICT SURVEILLANCE...
22
INTEGRATED DISEASE SURVEILLANCE PROJECT TRAINING MANUAL FOR STATE & DISTRICT SURVEILLANCE OFFICERS INTRODUCTORY MODULE ON DISEASE SURVEILLANCE Module -1 1
Transcript of TRAINING MANUAL FOR STATE & DISTRICT SURVEILLANCE...
1
INTEGRATED DISEASE
SURVEILLANCE PROJECT
TRAINING MANUAL FOR
STATE & DISTRICT
SURVEILLANCE OFFICERS
INTRODUCTORY MODULE ON
DISEASE SURVEILLANCE
Module -1
1
2
CONTENTS
1. Introduction 3
2. Contents of Introduction to IDSP 4
3. Instruction for Trainees 5
4. Module Structure at a Glance 6
5. Introductory Module 6
6. Salient Points to Remember 6
7. Group Activities 8
8. Frequently Asked Questions 10
9. Handout on Introduction to Disease Surveillance 11
10. Evaluation Questions 18
3
1. INTRODUCTION
Integrated Disease Surveillance Project (IDSP) is a decentralized, state based
Surveillance System in the country. IDSP is intended to detect early warning
signals of impending outbreaks and help initiate an effective response in a timely
manner. It is also expected to provide essential data to monitor progress of on
going disease control Programmes and help in allocating health resources more
optimally.
Not all outbreaks can be predicted or prevented. However, precautionary
measures can be taken within the existing health infrastructure to reduce risks
of outbreaks and to minimize the scale of the outbreak if it occurs. The
effectiveness with which national Programmes are implemented and monitored,
the alertness for identification of early warning signals and the capacity for
initiating recommended specific interventions in a timely manner are important
objectives of IDSP.
The District Surveillance Officers and Medical officers play an important role in
the surveillance activity, which can be listed as follows:
� Supervision and quality control of Active Surveillance by Health Workers in
the field
� Conduct Passive Surveillance of important diseases identified under IDSP
(refer to page 17)
� Supervise compilation and transmission of reports to District Surveillance
Officer at weekly intervals from PHCs and CHCs
� Integrate Selected Sentinel Private Practitioners in the Programme from the
area of activity
� Initiate emergency response to surveillance reports received in the unit
� Facilitate epidemic investigations and outbreak response by the District
Surveillance Unit.
� The Medical officers in both private sector and public sector will participate
in IDSP. While both groups will report diseases under surveillance, the pubic
sector MOs will be the primary efferent arm of surveillance. The type of
surveillance undertaken by the MOs will be presumptive in nature or
syndromic in nature. The health workers will undertake only syndromic
surveillance. This will be complimented by confirmed case surveillance by
the participating laboratories.
� The content and plan for training suggested in this training manual will need
to be suitably modified and updated with live examples and exercises to
make it more relevant to IDSP regionally.
4
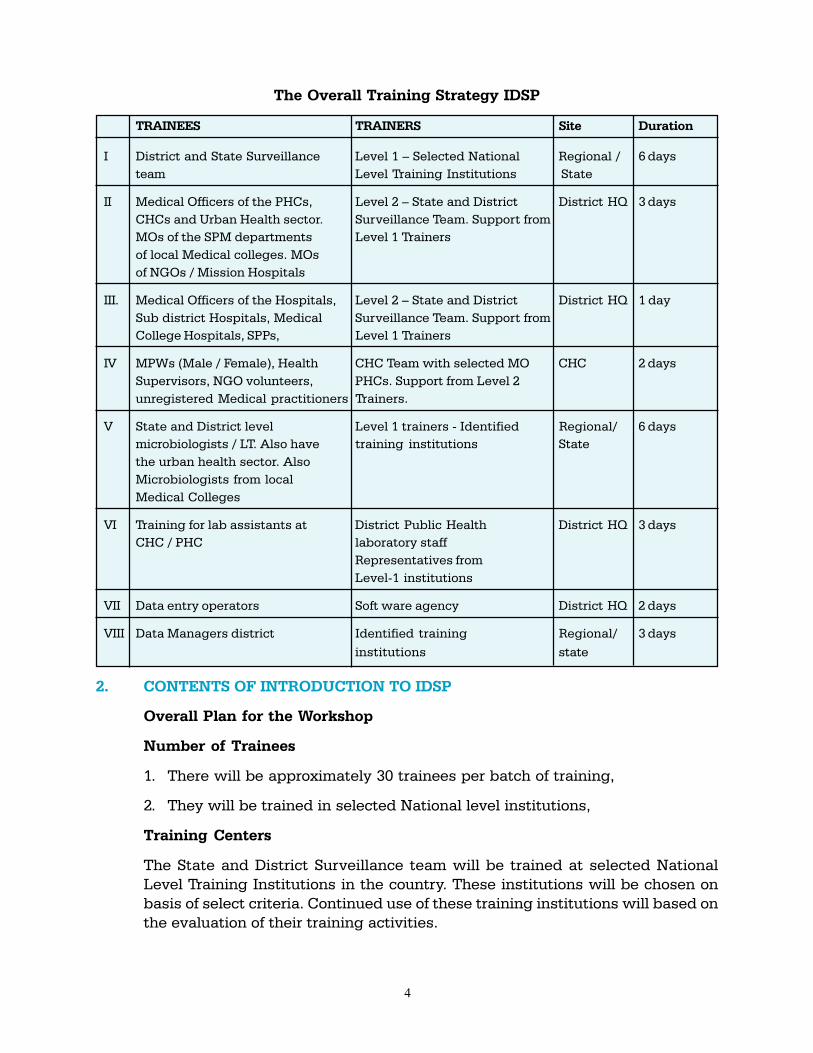
The Overall Training Strategy IDSP
TRAINEES TRAINERS Site Duration
I District and State Surveillance Level 1 – Selected National Regional / 6 days
team Level Training Institutions State
II Medical Officers of the PHCs, Level 2 – State and District District HQ 3 days
CHCs and Urban Health sector. Surveillance Team. Support from
MOs of the SPM departments Level 1 Trainers
of local Medical colleges. MOs
of NGOs / Mission Hospitals
III. Medical Officers of the Hospitals, Level 2 – State and District District HQ 1 day
Sub district Hospitals, Medical Surveillance Team. Support from
College Hospitals, SPPs, Level 1 Trainers
IV MPWs (Male / Female), Health CHC Team with selected MO CHC 2 days
Supervisors, NGO volunteers, PHCs. Support from Level 2
unregistered Medical practitioners Trainers.
V State and District level Level 1 trainers - Identified Regional/ 6 days
microbiologists / LT. Also have training institutions State
the urban health sector. Also
Microbiologists from local
Medical Colleges
VI Training for lab assistants at District Public Health District HQ 3 days
CHC / PHC laboratory staff
Representatives from
Level-1 institutions
VII Data entry operators Soft ware agency District HQ 2 days
VIII Data Managers district Identified training Regional/ 3 days
institutions state
2. CONTENTS OF INTRODUCTION TO IDSP
Overall Plan for the Workshop
Number of Trainees
1. There will be approximately 30 trainees per batch of training,
2. They will be trained in selected National level institutions,
Training Centers
The State and District Surveillance team will be trained at selected National
Level Training Institutions in the country. These institutions will be chosen on
basis of select criteria. Continued use of these training institutions will based on
the evaluation of their training activities.

5
Monday through Saturday – 6 days
Content Time Day
1 Introductory Module on Disease Surveillance 2 Hrs 1
2 Management structure of IDSP 1 Hr 1
3 Module of Reporting Units, Participants and their Roles 2 Hrs 1
4 Private Sector Participation in Disease Surveillance 1 Hr 1
5 Diseases and Syndromes Under Surveillance: Case Definitions 4 Hrs 2
6 Laboratory Methods in IDSP for Confirmation of Diagnosis, 2 Hrs 2
Collection, Storage, Transportation of Specimen
7 Disease Surveillance: Basic epidemiology 3 Hrs 3
8 Analysis & Interpretation of Data 3 Hrs 3
9a Out Break Response Session-1 – Investigations 3 Hrs 4
9b Out Break Response Session-2 – Control and Feed back 3 Hrs 4
10 Surveillance of risk factors of Non-communicable disease 1 Hrs 5
11 Action, Response and Feedback
12 Monitoring, Supervision and Quality control 3 Hrs 5
13 Intra and Inter-sectoral Coordination & Social Mobilization 2 Hr 5
14 Human Resource Development in IDSP 1 Hr 6
15 Evaluation of Training sessions 1 Hr 6
Open Session and Feed back 1 Hrs 6
3 INSTRUCTIONS FOR TRAINEES
� These modules have been designed as a self-contained unit of learning. You
are expected to learn in small groups of 6-8 persons under the guidance of a
facilitator.
� You are expected to share your experiences with other trainees.
� The module has been divided into various units to cover various aspects of
the topic.
� The learning objectives of the unit will inform you what is expected from you
once you complete the unit
� Important teaching learning points have been provided separately so that
the participants can focus on these aspects thoroughly during the sessions.
It is important to understand these points well
� The Handout provided with the unit is more comprehensive and must be
read by the all the participants.
� Please go through each learning activity and complete the exercise(s) given
at the end of the unit.
6
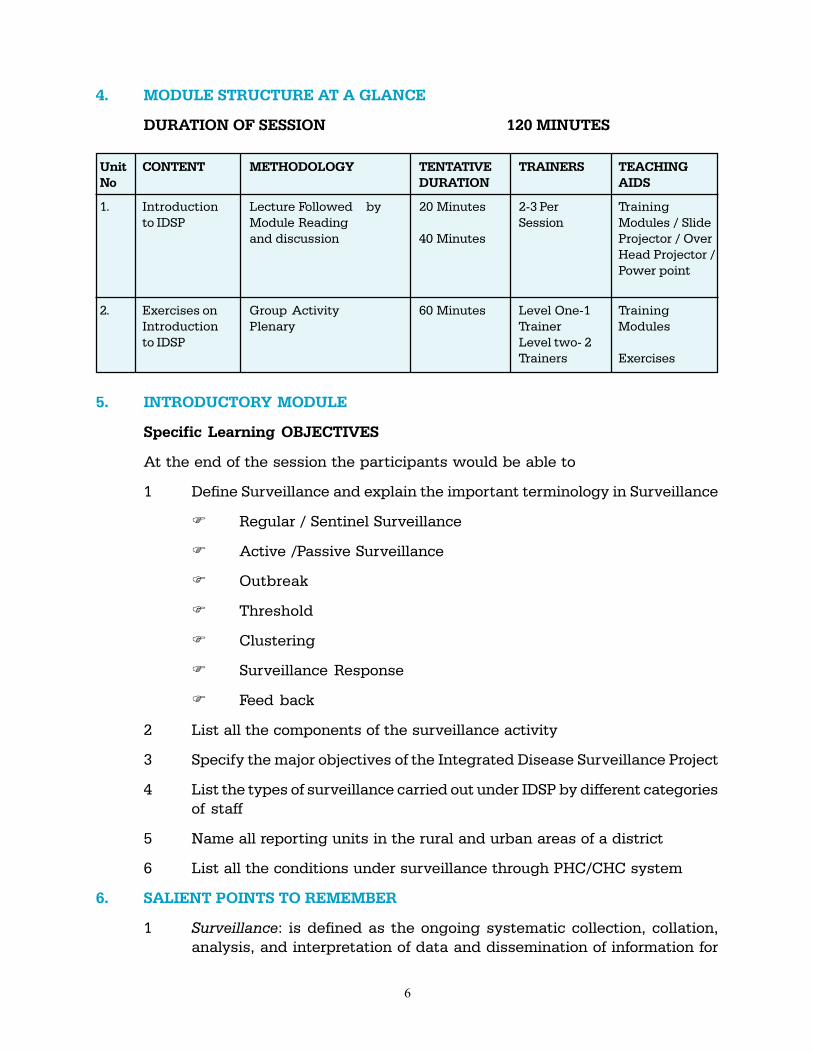
4. MODULE STRUCTURE AT A GLANCE
DURATION OF SESSION 120 MINUTES
Unit CONTENT METHODOLOGY TENTATIVE TRAINERS TEACHING
No DURATION AIDS
1. Introduction Lecture Followed by 20 Minutes 2-3 Per Training
to IDSP Module Reading Session Modules / Slide
and discussion 40 Minutes Projector / Over
Head Projector /
Power point
2. Exercises on Group Activity 60 Minutes Level One-1 Training
Introduction Plenary Trainer Modules
to IDSP Level two- 2
Trainers Exercises
5. INTRODUCTORY MODULE
Specific Learning OBJECTIVES
At the end of the session the participants would be able to
1 Define Surveillance and explain the important terminology in Surveillance
� Regular / Sentinel Surveillance
� Active /Passive Surveillance
� Outbreak
� Threshold
� Clustering
� Surveillance Response
� Feed back
2 List all the components of the surveillance activity
3 Specify the major objectives of the Integrated Disease Surveillance Project
4 List the types of surveillance carried out under IDSP by different categories
of staff
5 Name all reporting units in the rural and urban areas of a district
6 List all the conditions under surveillance through PHC/CHC system
6. SALIENT POINTS TO REMEMBER
1 Surveillance: is defined as the ongoing systematic collection, collation,
analysis, and interpretation of data and dissemination of information for
7
public health action. Without action data collection is not surveillance.
Refer to Section 9.01 in the Handout to the module on introduction
2 Activities related with surveillance involve Collection of data, Compilation
of data, Analysis and Interpretation, Follow up Action and Feed back at
different levels of activity.
Refer to Section 9.02 and 9.03 in Handout to module on introduction
3 Activities related to case management of affected patients even though
important for public health system is not surveillance activity.
4 The main weakness of disease surveillance which IDSP is trying to
overcome are: Lack of integration of private sector in surveillance activity,
Poor laboratory capacity, Lack surveillance infrastructure in the urban
regions, slow and inefficient sharing of surveillance information at the
district level, Limited capacity to undertake analysis and response at the
district level, Non inclusion of NCDs in surveillance Programme.
Refer to National Project Implementation Plan (PIP) on present system of
surveillance.
5 In IDSP three parallel system of surveillance will be undertaken. They
are:
1) Syndromic surveillance (Suspect case) performed by the Health
workers/ MOs;
2) Presumptive surveillance (Probable case) based on history and
physical examination by qualified medical officers only; and
3) Laboratory surveillance (Confirmed case) by laboratories
participating in the Programme.
They are independent systems reporting separately to the district surveillance
officer.
Refer to Section 9.10 in the Handout to introduction
6 Additional inputs to surveillance as part of IDSP is in: Improving laboratory
diagnostic capacity at all levels; Improving communication through
improved use of computers for surveillance; Developing human resources
of personnel by providing training; and Developing infrastructure to
facilitate sharing of surveillance information at the district and state levels.
Refer to section 9.05 of the section on Handout to introductory module
7 Health workers and Medical officers may undertake surveillance through
syndromic diagnosis without specifying disease conditions. The main
syndromes are 1) Fever less than 1 week with a) Rash, b) Convulsions, c)
Bleeding d) without any localizing signs. The other syndromes include 2)
8
Cough, 3) AFP 4) Jaundice 5) Unusual syndromes causing death or
hospitalization.
8 The MO may make presumptive diagnosis on the following conditions as
part of surveillance activity Malaria, Typhoid, Cholera, Tuberculosis,
Measles, Polio and Plague. Or other conditions like Meningo— encephalitis
and Acute Respiratory Distress Syndromes.
9 At the peripheral laboratory TB and Malaria will be confirmed by
laboratory. Rapid diagnostic test for Typhoid will be performed. By this, it
will remain as probable case of typhoid till the results are confirmed by
blood culture at the district laboratory.
10 The reporting units participating in IDSP are the following: PHC / CHC
and sentinel private hospitals/ Nursing homes / Clinics in the rural regions,
District Hospitals, ESI, Railway hospitals and Private hospitals / Private
Nursing homes in the urban regions. In addition all medical colleges will
participate as reporting units in IDSP.
11 The main reason why private sector participation is crucial to the success
of disease surveillance in India is 1). More than 70% of the first contact
health facilities are in the private sector, 2). The urban infrastructure for
surveillance is very weak.
Refer to module on private sector participation in IDSP for more details
12 The types of integration expected in IDSP include 1). Sharing of surveillance
information of diseases across disease control Programme Managers and
district administration, 2). Effective partnership with private sector 3)
Bringing Medical colleges into surveillance activity, 4). Set up a system of
surveillance, which would cater to both communicable and non-
communicable diseases important for the region.
Refer to Section 9.06 on Handout to module on introduction for more details
7. GROUP ACTIVITIES AND EXERCISES
Points For Discussion
Three Groups of 7-8 Participants
The Group Activity
� Selection of Group Leader
� Selection of Reporters
� Each group will discuss the two points for Group Discussion given
below
� At least one of the resource persons will join the Group

9
Group Discussion Points
Discussion Point-1
Possible Reasons for inclusion as priority diseases in IDSP
Your state has identified the following diseases to be state specific
diseases:
—————————————————————————————————
Examine the same for priority disease based on the following criteria:
� Burden of Disease – Morbidity, Mortality, Disability etc
� Epidemic Potential
� Availability of public Health Action to prevent the diseases
� National and International commitment
Comment on the current list of diseases under surveillance in IDSP as
given in the manual
� Cholera
� Hepatitis
� Typhoid
� ARI
� Malaria
� Tuberculosis
� Measles
� Polio
� Unusual Syndromes causing death or hospitalization
� Plague
� Meningo- encephalitis, Acute Respiratory Distress Syndrome
� Hemorrhagic Fevers etc
Discussion Point-2
Discuss the rationale of 3 types of surveillance diagnosis in the Integrated Disease
Surveillance Project.
� Syndromic – diagnosis made on the basis of clinical pattern by
medical/paramedical personnel and Members of the community.
� Presumptive – diagnosis made on typical history and clinical
examination by Medical officers
� Confirmed – clinical diagnosis confirmed by an appropriate
laboratory test.
What are the implications of different surveillance diagnosis in interpretation of
data?
Syndromic Surveillance
The paramedical health staff will undertake disease surveillance based on broad
categories of presentation.
10
What Diseases of Interest under IDSP can present with the following
syndromes?
1. Fever
� Less than 7 days duration without any localizing signs
� With Rash
� With Altered Sensorium or Convulsions
� Bleeding from Skin or mucus membrane
� Fever more than 7 days with or without localizing sings
2. Cough more than 3 weeks duration
3. Acute Flaccid Paralysis
4. Diarrhoea
5. Jaundice
6. Unusual Events causing death or hospitalization
In your opinion, what do you think the District Surveillance Officer should do
to facilitate the surveillance activity?
In your opinion, what do you think the Medical Officers need to do to make
the IDSP function effectively?
8. FREQUENTLY ASKED QUESTIONS
1) Will IDSP increase the workload of the health workers in collecting
additional data and sending them to CHC or PHC?
There is practically no new activity planned at the periphery as part of
the IDSP. The current reporting of diseases by HWs will be further
facilitated by provided forms and formats specified for disease
surveillance. The total number of diseases under surveillance is also
reduced to improve quality of reporting. The net result is reducing the
workload on peripheral health worker for surveillance related work.
2) How much time commitment would be needed by the DSO for
surveillance related activity?
District Surveillance Officer plays a crucial role in IDSP and full time
commitment is necessary for the successful implementation of the
Programme.
3) Will the vertical disease control Programmes be compromised with
IDSP?
The Vertical Disease Control Programmes will continue to function and
has an important role in initiating effective implementation measures for
11
control of specific diseases. Only the surveillance component of the
Programmes will be integrated through IDSP. This will avoid duplication
of resources and improve efficiency of surveillance activities. All the
information generated will be shared with all Programme managers at
the district and state level.
9. HANDOUT ON INTRODUCTION TO DISEASE SURVEILLANCE
There is no value to surveillance system unless the information is used for action
that prevents or control disease.
9.1 What is public health surveillance?
Surveillance: is defined as the ‘ongoing systematic collection, collation, analysis,
and interpretation of data; and dissemination of information to those who need to
know in order that action be taken
A more complete definition of surveillance is: The ongoing systematic collection,
analysis and interpretation of health data essential to planning, implementation,
and evaluation of public health practice closely integrated with timely dissemination
of these date to those who need to know. The final link in the surveillance chain is
the application of these data to prevent and control diseases. A surveillance system
includes a functional capacity for data collection, analysis and dissemination linked
to public health programmes (CDC 1988)
Surveillance is the backbone of public health Programme and provides
information so that effective action can be taken to control and prevent disease
of public health importance.
In some cases action must be immediate – within hours – in order to prevent
large-scale epidemics and deaths, such as Cholera, Meningitis and Food Poisoning.
In others, control and prevention activities are long term response to information
about diseases as tuberculosis, HIV, and Non communicable disease risk factors,
for which action may be taken in weeks, months or even in years.
9.2 What are the Key Elements of a Surveillance System?
All surveillance systems involve six key elements:
� Detection and notification of health event
� Investigation & confirmation (Epidemiological, clinical, laboratory)
� Collection of data
� Analysis and interpretation of data
� Feed back and dissemination of results
� Response – a link to public health Programme specially actions for
prevention and control
12
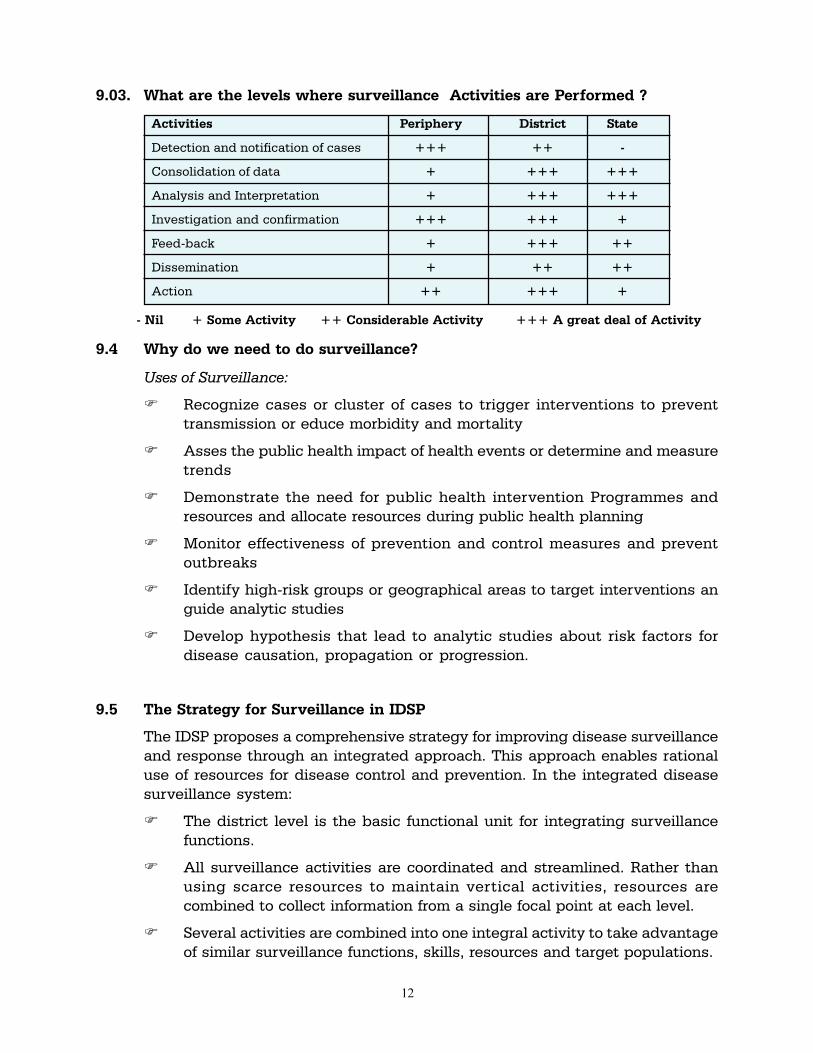
9.03. What are the levels where surveillance Activities are Performed ?
Activities Periphery District State
Detection and notification of cases +++ ++ -
Consolidation of data + +++ +++
Analysis and Interpretation + +++ +++
Investigation and confirmation +++ +++ +
Feed-back + +++ ++
Dissemination + ++ ++
Action ++ +++ +
- Nil + Some Activity ++ Considerable Activity +++ A great deal of Activity
9.4 Why do we need to do surveillance?
Uses of Surveillance:
� Recognize cases or cluster of cases to trigger interventions to prevent
transmission or educe morbidity and mortality
� Asses the public health impact of health events or determine and measure
trends
� Demonstrate the need for public health intervention Programmes and
resources and allocate resources during public health planning
� Monitor effectiveness of prevention and control measures and prevent
outbreaks
� Identify high-risk groups or geographical areas to target interventions an
guide analytic studies
� Develop hypothesis that lead to analytic studies about risk factors for
disease causation, propagation or progression.
9.5 The Strategy for Surveillance in IDSP
The IDSP proposes a comprehensive strategy for improving disease surveillance
and response through an integrated approach. This approach enables rational
use of resources for disease control and prevention. In the integrated disease
surveillance system:
� The district level is the basic functional unit for integrating surveillance
functions.
� All surveillance activities are coordinated and streamlined. Rather than
using scarce resources to maintain vertical activities, resources are
combined to collect information from a single focal point at each level.
� Several activities are combined into one integral activity to take advantage
of similar surveillance functions, skills, resources and target populations.
13
� The IDSP integrates both public and private sector by involving the private
practitioners, private hospitals, private labs, NGOs, etc and also emphasis
on community participation.
� Integrates communicable and non-communicable diseases.
� Integration of both rural and urban health systems as rapid urbanization
has resulted in the health services not keeping pace with the growing
needs of the urban populace. The gaps in receiving health information from
the urban areas needs urgently to be bridged.
� Integration with the medical colleges both private and public
� The main components of IDSP include Laboratory strengthening, improved
information management system, Human resource development and
developing supporting structure for integration.
9.6 Objectives of Integrated Disease Surveillance Project
The overall general objective of the IDSP is to provide a rational basis for decision-
making and implementing public health interventions that are efficacious in
responding to priority diseases. Keeping this in mind the main objectives of the
IDSP are:
1. To establish a decentralized district-based system of surveillance for
communicable and non-communicable diseases so that timely and effective
public health actions can be initiated in response to health challenges in
the urban and rural areas
2. To integrate existing surveillance activities (to the extent possible without
having a negative impact on their activities) so as to avoid duplication and
facilitate sharing of information across all disease control programmes and
other stakeholders so that valid data is available for health decision making
at district, state and national levels.
What is Integration?
In IDSP, different types of integration are proposed. These include:
1. Sharing of surveillance information of disease control programmes
2. Developing effective partnership with health and non-health sectors in
surveillance
3. Including Non-communicable and Communicable diseases in the
surveillance system
4. Effective partnership of private sector and NGOs in surveillance activities
5. Bringing Academic institution and Medical colleges into the primary public
health activity of disease surveillance.
14
9.7 Important Information in Disease Surveillance
To plan any disease control Programme and to identify and control outbreaks, it
is important to know the following:
� Who get the diseases?
� How many get them?
� Where they get them?
� When they get them?
� Why they get them?
� What needs to be done as public health response?
9.8 Components of the Surveillance Activity
There are five steps in the surveillance procedure, which must be carried out at
each level, starting from the primary Health Centre (PHC). Each level must have
the capacity for analyzing and using surveillance data for early detection,
prevention and control of outbreaks. These include:
� Collection of data
� Compilation of data
� Analysis and interpretation
� Follow up action
� Feedback
9.9 Prerequisites for effective surveillance
� Use of standard case definitions
� Ensure regularity of the reports
� Action on the reports
For developing an effective disease surveillance system, the district health officer/
PHC medical officer must also be clear about:
� What information to gather?
� How often to compile and analyze the data?
� How often and to whom to report?
� What proforma or formats to use?
� What action to take?
The data collected should be uniform, regular and timely. Standard case
definitions are important to ensure uniformity in reporting so that all reporting
15
units use the same criteria for reporting cases. It is also important to have a list
of all reporting units so that the regularity and timeliness of the reports is
checked. If no cases are seen, a nil report should be submitted. All levels in the
system must:
� Have the standard case definitions
� Have a list of all reporting units
� Monitor receipt of reports in time
� Monitor completeness of reports
The standard case definition of diseases is given in a separate manual.
Depending on the level of expertise and specificity disease surveillance in IDSP
will be of three categories.
9.10 Classification of Surveillance in IDSP:
� Syndromic–diagnosis made on the basis clinical pattern by paramedical
personnel and Members of the community.
� Presumptive–diagnosis made on typical history and clinical examination by
Medical officers
� Confirmed– clinical diagnosis by a medical officer and / or positive laboratory
identification.
Important Components of IDSP where additional Inputs will be provided:
1. Laboratory Diagnosis of diseases – Improving the quality of laboratory
services at the periphery and at the district levels
2. Improving communication through establishment of dial up network and
rapid flow of digital transfer of information from periphery to district and
from district to the state level.
3. Improving administrative structures so that better sharing of information
and responses will take place
4. Improving human resource to under take surveillance by providing training
at different levels of surveillance.
9.11 Reporting Units participating in regular passive surveillance under IDSP:
The Syndrome of fever will kept under regular passive surveillance at the
periphery by the reporting units in both public and private sector in rural and
urban areas of the district. Primarily Passive Surveillance will be undertaken at
all reporting units by the Medical Officer. Each reporting unit will be provided a
unique identifier so that computerization and identity and type can be recognized.
16
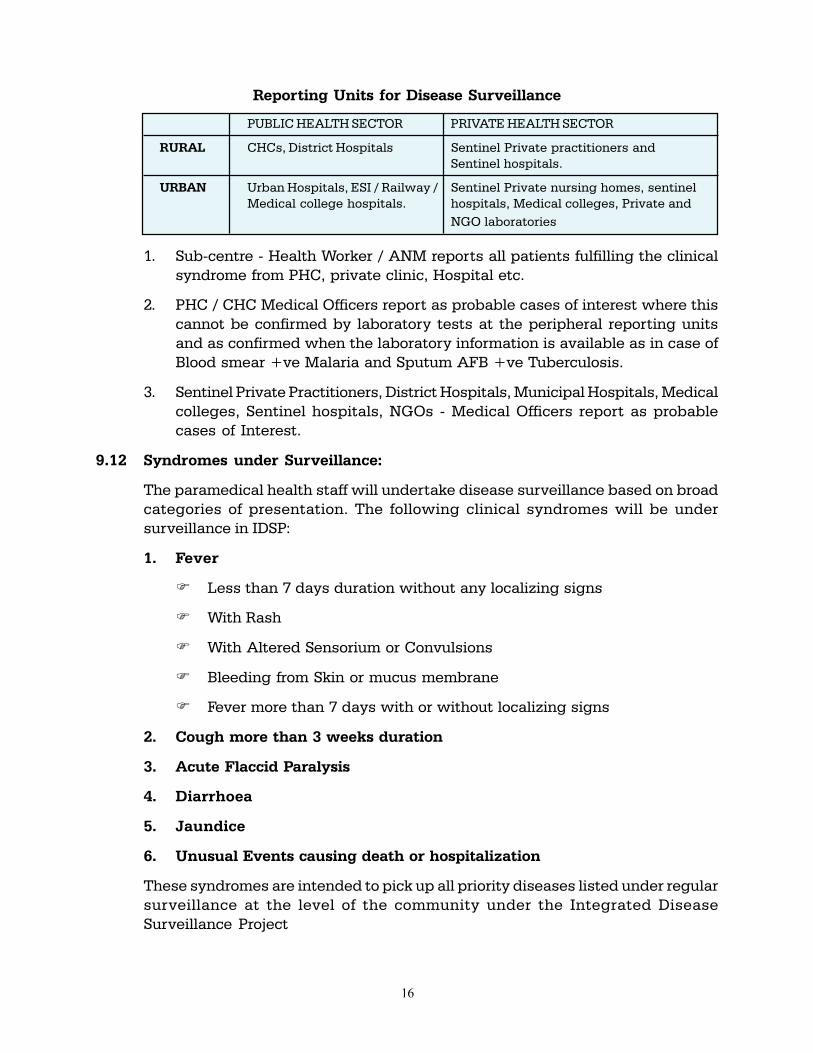
Reporting Units for Disease Surveillance
PUBLIC HEALTH SECTOR PRIVATE HEALTH SECTOR
RURAL CHCs, District Hospitals Sentinel Private practitioners and
Sentinel hospitals.
URBAN Urban Hospitals, ESI / Railway / Sentinel Private nursing homes, sentinel
Medical college hospitals. hospitals, Medical colleges, Private and
NGO laboratories
1. Sub-centre - Health Worker / ANM reports all patients fulfilling the clinical
syndrome from PHC, private clinic, Hospital etc.
2. PHC / CHC Medical Officers report as probable cases of interest where this
cannot be confirmed by laboratory tests at the peripheral reporting units
and as confirmed when the laboratory information is available as in case of
Blood smear +ve Malaria and Sputum AFB +ve Tuberculosis.
3. Sentinel Private Practitioners, District Hospitals, Municipal Hospitals, Medical
colleges, Sentinel hospitals, NGOs - Medical Officers report as probable
cases of Interest.
9.12 Syndromes under Surveillance:
The paramedical health staff will undertake disease surveillance based on broad
categories of presentation. The following clinical syndromes will be under
surveillance in IDSP:
1. Fever
� Less than 7 days duration without any localizing signs
� With Rash
� With Altered Sensorium or Convulsions
� Bleeding from Skin or mucus membrane
� Fever more than 7 days with or without localizing signs
2. Cough more than 3 weeks duration
3. Acute Flaccid Paralysis
4. Diarrhoea
5. Jaundice
6. Unusual Events causing death or hospitalization
These syndromes are intended to pick up all priority diseases listed under regular
surveillance at the level of the community under the Integrated Disease
Surveillance Project

17
Fever with & without localizing signs Malaria, Typhoid, JE, Dengue, Measles
Cough more than 3 weeks Tuberculosis
Acute Flaccid Paralysis Polio
Diarrhoea Cholera
Jaundice Hepatitis, Leptospirosis, Dengue, Malaria, Yellow fever
Unusual Syndromes Anthrax, Plague, Emerging epidemics
9.13 Core Conditions under surveillance in IDSP
(i) Regular Surveillance:
Vector Borne Disease : 1. Malaria
Water Borne Disease : 2. Acute Diarrhoeal Disease (Cholera)
: 3. Typhoid
Respiratory Diseases : 4. Tuberculosis
Vaccine Preventable Diseases : 5. Measles
Diseases under eradication : 6. Polio
Other Conditions : 7. Road Traffic Accidents
(Linkup with police computers)
Other International commitments: : 8. Plague
Unusual clinical syndromes : 9. Meningoencephalitis/Respiratory
(Causing death / hospitalization) Distress, Hemorragic fevers, other
undiagnosed conditions
(ii) Sentinel Surveillance
Sexually transmitted diseases/Blood borne : 10. HIV/HBV, HCV
Other Conditions : 11. Water Quality Monitoring
: 12. Outdoor Air Quality
(Large Urban centers)
(iii) Regular periodic surveys:
NCD Risk Factors : 13. Anthropometry, Physical activity, Blood
Pressure, Tobacco, Nutrition etc.
(iv) Additional State Priorities : Each state may identify up to five additional conditions for
surveillance.
Do surveillance for disease conditions important for public health action:
� The number of core diseases are limited to improve quality of surveillance
and to reduce workload on the peripheral health worker.
� Diseases and other conditions of regional importance will be under
surveillance in addition to the above core list in all states.
� The list will be reviewed and modified according the needs of surveillance
at least once in 2 years
� Viral Hepatitis and ARI are also under active consideration at various
levels and may be included subsequently.
18
10. EVALUATION QUESTIONS
Choose the Most optimum Answer for the following:
1. IDSP is ……………..Centered in its activity (Country, State, District, CHC)
2. One of the important reasons why a disease condition is included for surveillance
in the IDSP Programme is because …… (emerging disease, High case fatality,
treatment costs very high, Affects special groups, Availability of public health
response).
3. Integration of IDSP means ………………(Inclusion of private sector in its activities,
Inclusion of NCD in surveillance, Sharing of surveillance information with all stake
holders in the district, Inclusion of Non health sector in surveillance activity, All the
above, None of the above)
4. IDSP will help to monitor….of Disease (Incidence, Prevalence, Trends, Burden)
5. Integration of Medical Colleges will help ………………in IDSP (to recruit large
number of subjects with disease, to detect outbreaks early, in urban surveillance,
monitor quality of surveillance)
6. The medical officers will perform ………….. (Syndromic Surveillance, Probable
Disease based surveillance, confirmed case surveillance, All the above, None of
the above)
Choose True or False
1. Disease surveillance is undertaken to assess the burden of disease in the
community.
2. Disease Surveillance is collection, analysis and interpretation of data for public
health action.
3. Additional Inputs in surveillance through IDSP is Strengthening of laboratory,
Improving communication and providing essential training.
4. New Groups of people are recruited to do surveillance in IDSP separate from
existing system.
INTEGRATED DISEASE SURVEILLANCE PROJECT
(IDSP)
TRAINING MANUAL
FOR
STATE & DISTRICT SURVEILLANCE
OFFICERS
March 2005March 2005March 2005March 2005March 2005
Government of India
Directorate General of Health Services
Ministry of Health and Family Welfare
Nirman Bhawan, New Delhi
ABBREVIATIONS
ABER Annual Blood Examination Rate
AFB Acid Fast Bacilli
AFP Acute Flaccid Paralysis
AIDS Auto Immune Deficiency Syndrome
ANC Ante Natal Care
ANMs Auxiliary Nurse Midwife
API Annual Parasitic Incidence
ARI Acute Respiratory Infection
AWWs Angan Wadi Workers
BMI Body Mass Index
CDC Centers for Disease Control and Prevention
CFR Case Fatality Rate
CHC Community Health Center
CME Continued Medical Education
CMO Chief Medical Officer
CSF Cerebrospinal Fluid
CSU Central Surveillance Unit
CVD Cardio-Vascular Disease
DEIT District Epidemic Investigation Team
DF Dengue Fever
DGHS Directorate General fo Health Services
DH District Hospital
DHF Dengue Haemorrhagic Fever
DHO District Health Officer
DHS Director of Health Services
DIO District Immunization Officer
DME Director of Medical Education
DMO District Malaria Officer
DSO District Surveillance Officer
DSS Dengue Shock Syndrome
DSU District Surveillance Unit
DTO District Tuberculosis Officer
ELISA Enzyme-linked Immuno-sorbent Assay
EQAS External Quality Assurance System
ESI Employee’s State Insurance
ETB Extra-pulmonary Tuberculosis
FW Family Welfare
GIS Geographical Information System
HA Health Assistants
HAV Hepatitis A Virus
HBV Hepatitis B Virus
HCV Hepatitis C Virus
HDV Hepatitis D Virus
HEV Hepatitis E Virus
HRD Human Resource Development
HIV Human Immunodeficiency Virus
IAP Indian Association of Pediatrics
ICMR Indian Council of Medical Research
21
IDSP Integrated Disease Surveillance Project
IEC Information Education Communication
IgG Immunoglobulin G
IgM Immunoglobulin M
IMA Indian Medical Association
IT Information Technology
JE Japanese Encephalitis
LT Lab Technician
MHO Medical & Health Officer
MO Medical Officer
MoH & FW Ministry of Health & Family Welfare
MOU Memorandum of Understanding
MP Malarial Parasite
MPW Multi Purpose Workers
M&E Monitoring & Evaluation
NACO National AIDS Control Organization
NCD Non Communicable Diseases
NFHS National Family Health Survey
NGO Non Governmental Organization
NICD National Institute of Communicable Diseases
NIE National Institute of Epidemiology
NPSP National Polio Surveillance Project
OPD Out Patient Department
OPV Oral Polio Vaccine
ORS Oral Rehydration Solution
OT Ortho toludine
PCR Polymerase Chain Reaction
PH Public Health
PHC Primary Health Center
PF Plasmodium falciparum
POL Petrol Oil Lubricants
PTB Pulmonary Tuberculosis
QA Quality Assurance
QC Quality Control
RCH Reproductive & Child Health
RMP Registered Medical Participationer
RNTCP Revised National TB Control Programme
RRT Rapid Response Team
RT Radical Treatment
RTA Road Traffic Accidents
SHGs Self Help Group
SPPs Sentinel Private Practioners
SPR Slide Positivity Rate
SSU State Surveillance Unit
TB Tuberculosis
URTI Upper Respiratory Tract Infection
VPD Vaccine Preventable Disease
VTM Viral Transport Medium
WHO World Health Organisation
CONTENTS
Module Subject Page No.
1. Introductory Module 1
2. Management Structure 19
3. Reporting Units, Participants and their roles 31
4. Private Sector Participation 49
5. Case Definitions 65
6. Laboratory Methods 93
7. Basic Epidemiology 137
8. Outbreak Investigation 159
9. Analysis and Interpretation of Data 183
10. Feedback 209
11. Monitoring, Supervision and Quality Control 223
12. Intra and Intersectoral Coordination and Social Mobilization 233
13. Human Resources Development 243
14. Surveillance of Risk Factors of NCD 257
![Stage-1 Stage-2 [ ] Surveillance [ ] Re-Certificationmutucertification.com/wp-content/uploads/2016/02/RSPO-Assessment... · Stage-2 [ ] Surveillance [ ] Re-Certification ... District](https://static.fdocuments.in/doc/165x107/5cad9fc188c99333788b813a/stage-1-stage-2-surveillance-re-certificat-stage-2-surveillance.jpg)