Towards Personalized Medicine in Treatment and Care of Patients with Peritoneal Metastases of
246
Towards Personalized Medicine in Treatment and Care of Patients with Peritoneal Metastases of Colorectal Cancer Erienne Marie-Luise Véronique de Cuba
Transcript of Towards Personalized Medicine in Treatment and Care of Patients with Peritoneal Metastases of

Towards Personalized Medicine in Treatment and Care of Patients
with Peritoneal Metastases of Colorectal Cancer
Erienne Marie-Luise Véronique de Cuba
Towards Personalized M
edicine in Treatment and C
are of Patients with Peritoneal M
etastases of Colorectal C
ancer Erienne de C
uba
INVITATION
voor het bijwonen vande openbare verdediging
van het proefschrift
Towards Personalized Medicine in Treatment
and Care of Patients with Peritoneal Metastases of Colorectal Cancer
door
Erienne Marie-Luise Véronique de Cuba
Donderdag, 9 juni 2016Om 13.45
In de aula van deVrije Universiteit
De Boelelaan 1105te Amsterdam
met aansluitend receptie
ParanimfenPien Delis-van Diemen
[email protected] Kwakman
Erienne de CubaHoutmankade 43 HS
1013 MR, [email protected]
Erienne Marie-Luise Véronique de Cuba was born on the 25th of October 1983 on the sunny island of Aruba as the eldest child in a family of four. After completing high school (VWO) in 2002 on the one happy island at the Colegio Arubano, she proceeded to study medicine in Groningen at the Rijksuniversiteit Groningen.
In December 2009 she completed her medical studies, during which she concluded several internships focussed on gastro-intestinal malignancies and a research project at the department of Gastroenterology and Hepatology of
the Academic Medical Center Amsterdam on the treatment of pancreatic pseudocysts after pancreatitis under the leadership of Prof.dr. P. Fockens.
She started her PhD in February 2010 on clinical and molecular profiling of patients presenting with peritoneal metastases of colorectal cancer under the guidance of dr. E.A. te Velde, prof.dr. H.J. Bonjer and prof.dr. G.A. Meijer. at the VU University Medical Center.
In the fall of 2013 she started her residency in surgical pathology at the VU Medical Center in Amsterdam under the supervision of prof.dr. E. Bloemena and prof.dr. P. van der Valk. The author currently resides with her husband in Amsterdam.
13653_DeCuba_OM_v1.indd 1 19-04-16 12:33

13653_DeCuba_OM_v1.indd 2 19-04-16 12:33

Towards personalized medicine in treatment and care of patients with peritoneal
metastases of colorectal cancer
Erienne Marie-Luise Véronique de Cuba

The work described in this thesis was performed at the Tumor Profiling Unit of the Department of Pathology and the division of Surgical Oncology of the Department of Surgery of the VU University Medical Center in Amsterdam, the Netherlands.
Printing of this thesis was financially supported by
ISBN: 978-94-6299-346-4
Cover and illustrations: Erienne de Cuba Lay-out: Nikki Vermeulen - www.ridderprint.nlPrinting: Ridderprint BV - www.ridderprint.nl
Copyright © 2016, Erienne de CubaAll rights reserved. No parts of this publication may be reproduced, stored in a retrieval system or transmitted in any form or means without the prior permission in writing from the author.

VRIJE UNIVERSITEIT
Towards personalized medicine in treatment and care of patients with peritoneal
metastases of colorectal cancer
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aande Vrije Universiteit Amsterdam,op gezag van de rector magnificus
prof.dr. V. Subramaniam,in het openbaar te verdedigen
ten overstaan van de promotiecommissievan de Faculteit der Geneeskunde
op donderdag 9 juni 2016 om 13.45 uurin de aula van de universiteit,
De Boelelaan 1105
door
Erienne Marie-Luise Véronique de Cubageboren te Oranjestad, Aruba

promotoren: prof.dr. G.A. Meijer prof.dr. H.J. Bonjer
copromotor: dr. E.A. te Velde

“Impossible is a word to be found only in the dictionary of fools”
- Napoleon Bonaparte
Voor mijn moeder

Table of contents
Chapter 1 General introduction and outline of the thesis
Part I Clinical Decision Making / Treatment Allocation
Chapter 2 Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases - Systematic review of all literature and meta-analysis of observational studies - Cancer Treat Rev. 2013 Jun;39(4):321-7
Chapter 3 Morbidity associated with colostomy reversal after cytoreductive surgery and HIPEC Ann Surg Oncol. 2014 Mar;21(3):883-90
Part II Molecular Approach – Possible Aids in Future Clinical Decision Making –
Chapter 4 Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer; - Future possibilities for personalised treatment by use of biomarkers - Virchows Arch. 2012 Sep;461(3):231-43
Chapter 5 Adhesion molecules in peritoneal metastases of colorectal cancer: - Function, prognostic relevance and therapeutic options - Accepted Clin Exp Metastasis April 2016
Chapter 6 Versican and vascular endothelial growth factor expression levels in peritoneal metastases from colorectal cancer are associated with survival after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy Clin Exp Metastasis. 2016 Apr;33(4):297-307
Chapter 7 Angiogenesis related markers and prognosis after Cytoreductive Surgery and Hyperthermic Intra-peritoneal Chemotherapy for Metastatic Colorectal Cancer Ann Surg Oncol. 2016 May;23(5):1601-8

Chapter 8 Glucose transporter 1 (SLC2A1) and vascular endothelial growth factor A (VEGFA) predict survival after resection of colorectal cancer liver metastasis Ann Surg. 2016 Jan;263(1):138-45
Chapter 9 Tailoring heated intraperitoneal Mitomycin C for peritoneal metastases originating from colorectal carcinoma - A translational approach to improve survival - Br J Cancer. 2015 Mar 3;112(5):851-6
Chapter 10 Prognostic value of BRAF and KRAS mutation status in stage II and III microsatellite instable colon cancers Int J Cancer. 2016 Mar 1;138(5):1139-45


Chapter 1General Introduction and
Outline of the Thesis


General Introduction and Outline of the Thesis | Chapter 1
11
1Colorectal Cancer – GeneralColorectal cancer (CRC) is one of the most prevalent epithelial cancers, with an annual worldwide incidence of over 1 million cases. 1,2 In the Netherlands, 15.000 new patients are diagnosed each year. Annually a total of 5.000 patients ultimately succumb to the disease. 3 This is largely due to spread of the disease to distant sites such as liver or lung. 1,2,4 In addition to the haematogenous spread of CRC to the aforementioned sites, it is also known to spread locally to the peritoneal surface. 3,5
Table 1. Colorectal cancer divided into stages with survival per stage
TNM UICC/AJCC Stage
Stage atfirst diagnosis
Five year Survival
Tis N0 M0 0
T1-2 N0 M0 I 39% 90%
T3-4 N0 M0 II
T1-4 N1-2 M0 III 37% 69%
T1-4 N0-2 M1* IV 20% 12%
Adapted from www.oncoline.nl & Siegel et al. 1-3Tis= carcinoma in situ; T1=tumour invades submucosa; T2=tumour invades muscularis propria; T3=tumour invades through mucularis propria into subserosa or into non-peritonealised pericolic or perirectal tissues; T4=tumour penetrates visceral peritoneum or directly invades other organs and/or structures; N0=no metastases in regional lymph nodes; N1-2= regional lymph node metastases present; M0= no distant metastases; M1=distant metastases present* The M1 category includes patients with peritoneal metastases.
Colorectal Cancer – Peritoneal Metastases
Epidemiology
Metastatic disease (Stage IV) is present in approximately 20% of patients at time of diagnosis (Table 1). Additionally, metastases develop in up to half of all CRC patients during the course of the disease. 4,5 Roughly 10-25% of CRC patients develop peritoneal metastases (PM), of which 25% present with the peritoneum as the sole sight of distant metastases. 1,3,6-8 The peritoneum is a composed of a single layer of mesothelial cells on top of a basal membrane underneath of which there is loose connective tissue, which cover the abdominal wall and internal organs. 4,6,7,9 Peritoneal metastases (PM) are believed to be the result of tumour cell shedding into the peritoneal cavity, either spontaneously or as e result of spill during surgical procedures (Fig.1). These tumour cells are believed to subsequently spread through the abdominal cavity by means of the physiological flow of peritoneal fluid and gravitational forces. The process of attachment of tumour cells to the mesothelial cells of the peritoneum is believed to involve several steps and multiple molecules, ultimately

Chapter 1 | General Introduction and Outline of the Thesis
12
resulting in the development of solid tumour deposits on the peritoneal surface thus known as peritoneal metastases (PM) or peritoneal carcinomatosis. 10,11
Figure 1. Schematic overview of peritoneal dissemination of colorectal cancer, showing in a sagittal section, the proposed mechanism of transcoelomic spread of tumour cells which can ultimately lead to the formation of peritoneal metastases.
Clinical Course of the patient presenting with Peritoneal Metastases
Clinical features
The deposition and growth of the tumour cells on the surface of the peritoneum can lead to tumour deposits which can ultimately involve any intra-abdominal organ or structure which is covered by the peritoneum. Preferential sites for intra-abdominal tumour implantation on the peritoneal surface include: the omentum, the mesentery, the surface of the bowel, Douglas’ pouch, the right paracolic gutter and the diaphragm. 12-14 Patients initially present either with no or aspecific symptoms, which are often indistinguishable from the symptoms seen in malignant disease in general. Ultimately, the invasion of malignant cells and growth of peritoneal implants on the bowel surface can lead to bowel obstruction and ascites. 15 However, it should be noted that a considerable proportion of patients do not report any symptoms at the time of diagnosis. This is especially the case when the peritoneal implants are of limited size and little to no ascites is present. 16

General Introduction and Outline of the Thesis | Chapter 1
13
1Diagnosis
The adequate assessment of intra-abdominal tumour burden is essential for the initial diagnosis of PM. The diagnosis is made by visualization of the PM, either by imaging or by laparotomy or laparoscopy. Firstly, it is crucial to assess the extent of disease spread in order to assess whether further treatment is prudent. In addition it is also crucial for the evaluation of treatment response and follow-up. 16 Notwithstanding, the currently available diagnostic tools are lacking for proper assessment in this sub-group of CRC patients. 16,17
Tumour marker testing, such as serum CEA levels, have been shown to be able to diagnose recurrent CRC, including PM. 16 However, these raised levels only indicate recurrence of disease, not the volume or location of intra-abdominal tumour deposits. Both volume and location are critical factors in the selection of patients for aggressive surgical treatment 16
Computed Tomography (CT)- and/or Positron Emission Tomography (PET) scanning also lack the sensitivity and specificity needed for the timely detection of, especially, smaller peritoneal tumour nodules (<1cm). 16,18-20 17The value of pre-operative imaging in PM has not only been described to be dependent on lesion size, but also dependent on the evaluating radiologist. 18 It has been proposed that one difficulty in the interpretation is that the peritoneum follows the natural contours of the intra-abdominal organs, making it difficult to assess whether it is affected by disease spread by these modalities, especially in the case of limited peritoneal involvement and/or small (<1cm) nodules. Furthermore, one study also shows that the greatest inaccuracy of pre-operative CT imaging for PM is seen in the pelvis, one of the preferential sites for peritoneal implantation of tumour cells. 20 Consequently, the extent of the peritoneal carcinomatosis is often underestimated. The extent of intra-abdominal spread can only truly correctly be assessed and documented during either laparoscopy or laparotomy. 21 Laparoscopy continues to be one of the most effective methods of PM detection, which also gives the treating physician the opportunity to collect tissue for definite pathological diagnosis. 22 Yet, this remains an invasive procedure, which is accompanied by the risks associated with any operative procedure. Furthermore, adhesions from prior surgeries can potentially hinder adequate and complete inspection of the peritoneal surface. 23 However, pre-operative imaging by means of CT- and/or PET-scanning still remains essential. Firstly, for the detection of extra-peritoneal disease, such as liver- and/or lung metastases, in order to properly screen and select potential candidates for treatment, as CRS and HIPEC is largely reserved for patients with isolated PM. Secondly, in the case a patient presents with symptoms, logistically it is faster to perform imaging studies to assess disease burden than to immediately operate if the symptoms are not directly life-threatening.

Chapter 1 | General Introduction and Outline of the Thesis
14
Possible treatment strategies for peritoneal metastases of colorectal cancer
Treatment – Systemic TherapiesIn the past, peritoneal metastases have been solely regarded as a condition only amenable to treatment with a palliative intent, due to the belief that the condition inevitably leads to a rapid demise of the patient. 24-26 There is a considerable paucity of data concerning the outcome of systemic therapies in specifically patients with PM of CRC. One hurdle in the interpretation of the efficacy of treatment in this subgroup of metastatic colorectal cancer patients is the difficulty in assessing treatment response with imaging using standard RECIST criteria, as is customary with systemic metastases such as liver- and lung metastases. 27 Due to this difficulty in objectifying treatment response this subgroup of metastatic CRC patients is underrepresented in randomized controlled trials assessing chemotherapeutic regiments in metastatic colorectal cancer. 24,26-30 The few studies assessing the response to treatment in patients presenting with PM focus on regiments including 5-FU and only some on the addition of oxaliplatin and irinotecan in retrospective cohorts. 24,26 On average, the survival of these patients ranges from six to 12 months. The general tendency observed in these studies is that patients with PM fare considerably less well than patients with metastases confined to either the liver or the lung. However, it should be mentioned that a substantial proportion of the patients analyzed in these studies do not present with isolated PM, but in combination with either liver or lung metastases. 26,27,31 This makes it difficult, if not impossible, to assess the effect of systemic treatment in patients with isolated PM of CRC. The advent of newer treatment strategies, including those with monoclonal antibodies against the Epidermal Growth-Factor Receptor (EGFR) and Vascular Endothelial Growth-Factor (VEGF), have shown promising results in patients with metastasized colorectal cancer in general. 27-30 Yet, the effect of treatment with these targeted therapies in isolated PM of CRC is still largely unknown. Only one study in which patients were treated with an anti-VEGF agent (Bevacizumab) show that a subgroup of patients with PM, both isolated or in combination with haematogenous metastases, show an overall survival of about 15 months. 24,32 Another cohort of patients with PM, isolated or in combination with other metastatic sites, were treated with Bevacizumab, Cetuximab or Panitumumab in palliative setting showed overall survival of about 18 months versus 10 months in those who were only treated with standard cytotoxic therapy. 8,33,34 This suggests that there is possibly an effect of biological agents in PM of CRC. However this effect is still markedly less than the effect observed in patients with haematogenous metastases. 28,30 This could mean that the biologic basis of PM is distinct, which in turn could translate into a relative resistance to treatment with systemic chemotherapy. Yet, the fact remains that very little is known about the effects of (modern) systemic chemotherapy treatment on isolated PM, in contrast to hepatic or pulmonary metastases of CRC.

General Introduction and Outline of the Thesis | Chapter 1
15
1Treatment - The advent and implementation of Cytoreductive Surgery and Hyperthermic IntraPEritoneal ChemotherapySurgical treatment of both hepatic and pulmonary metastases is the mainstay of current treatment for metastasized CRC, under the condition that these metastases are amenable to resection. Often the surgical resection is followed by treatment with systemic chemotherapy. 32 Adjuvant systemic chemotherapy after radical resection of liver metastases, with or without the addition of so-called biologicals has been shown to give a disease free survival rate of about 50%. 35,36 However, for a considerable time this approach was not considered feasible or desirable for patients presenting with PM due to the observation that most of these patients succumb to the disease well within a year after diagnosis if either left untreated or if they are treated exclusively with (standard) palliative chemotherapy. It was however noted that there is a subgroup of patients that only present with PM, with no hepatic or pulmonary metastases. This led to the theory that PM are a form of localized spread, and thus should be amenable to a form of localized treatment, i.e. surgery. 8,34 Risk factors described for tumour seeding on the peritoneal surface include advanced T-stage of the primary tumour (pT4) and bowel perforation. 37 Subsequently, a novel treatment was developed in the late eighties-early nineties consisting of an aggressive surgical approach, CytoReductive Surgery (CRS), combined with Hyperthermic IntraPEritoneal Chemotherapy (HIPEC). 8,34,38 The aim of this procedure is to surgically remove all macroscopically visible intra-abdominal tumour deposits. 39 This treatment is administered only when the patient presents with isolated PM. Patients with other metastatic sites, such as liver and lung, are largely excluded. 39 During the initial laparotomy (performed from xyphoid to os pubis) the abdomen is systematically explored by dividing it into 13 different regions for inspection (fig.1). In this manner both the volume and location of the peritoneal implants are assessed. To record this in a standardized fashion, the Peritoneal Cancer Index (PCI) system is used. This tool aids in quantifying the distribution and implant size in both the abdomen and pelvis. The abdomen and pelvis are divided into nine regions and the remaining regions are composed of the jejunum and ileum (two regions each for upper and lower part). Subsequently the lesion size (LS) in each region is recorded. The size-score ranges from zero to three. LS-0 means there are no visible lesions in the inspected region. LS-1 is utilized for lesion up to 0.5cm in size. LS-2 is used to describe lesions that vary between 0.5 to five cm. And finally, lesions larger than 5cm are classified as LS-3. It should be noted that the scoring takes place after a complete adhesiolysis and complete inspection of the entire peritoneal surface. After completion of the scoring the score is presented as a numerical score that ranges from 1 up to 39. 40 In the Netherlands, a simplified PCI (sPCI) is routinely used. This sPCI does not divide the abdomen into 13 regions, but into seven. These include: pelvis & sigmoid; right lower-abdomen; small bowel & mesentery; omentum & transverse colon;

Chapter 1 | General Introduction and Outline of the Thesis
16
subhepatic space & stomach; right subphrenic space and left subphrenic space. The extent of peritoneal involvement is quantified by counting the number of affected regions (ranges from zero to seven). 41 Generally patients with a PCI score of less than 20 or, if the sPCI is used, five or less regions affected, are considered most suitable for CRS and HIPEC. 39 The extent of peritoneal involvement, measured as PCI or sPCI, is a well-documented prognostic indicator for patients undergoing CRS & HIPEC. 34,39 It is believed that this is due to the fact that if the disease is “limited” there is a greater chance of successfully resecting all of the tumourous implants. 39 Patients who are excluded from treatment based on the extent and resectability of their disease are commonly referred to the oncologist for palliative treatment. 40 The objective of the CRS is to remove all macroscopic disease from the abdomen or to leave only limited residual tumour (<2.5mm) if complete resection is not feasible. 39,40 During the surgical procedure, often multiple resections are carried out to remove all intra-abdominal tumour, amongst which are resections of the intestines, parts of the stomach, the gall-bladder and even the spleen. In addition, peritonectomy procedures are frequently performed. 8 The extent of resection is recorded using the Completeness of Cytoreduction Score (CC or CCS), of which there are several variants. Jacquet and Sugarbaker proposed a scoring system in which; a CC-0 indicates no peritoneal seeding was observed after complete exploration; a CC-1 score indicates the remaining tumour nodules to be smaller than <2.5mm; CC-2 is utilized to indicate residual disease that ranges between 2.5 and 25 mm in diameter and lastly, a CC-3 score indicates nodules greater than 25 mm in diameter are left in-situ or irresectable tumour deposits at any site within the abdominal cavity or pelvis. 40 The French group scores complete cytoreduction as R0-R1 and incomplete as R2. The reason for grouping the R0 and R1 categories lies in the difficulty of confirming an R0 in peritoneal carcinomatosis while in addition the outcome for both groups has been described as being quite similar. 38,39,42-46 The Dutch HIPEC group utilizes a similar scoring system, however the different categories are scored as R1 (no macroscopic residual tumour), R2a (largest residual nodule <2.5mm) and R2b (largest remaining nodule >2.5mm). Several studies have shown a direct relation between the completeness of CRS and the survival after treatment, making the completeness of the CRS one of the most important prognostic factors in this population. 34,39,45,47 After a macroscopically complete CRS has been performed, intraperitoneal chemotherapy is administered to eradicate the microscopic residual disease. Administration techniques differ slightly per region. Firstly, the intraperitoneal chemotherapy can be administered per-operatively , usually with hyperthermia (HIPEC) or it can be administered post-operatively, starting on the first day after the CRS through day five. The last technique is known as early post-operative intraperitoneal chemotherapy, EPIC for short. Additionally, the per-operative variant can be performed either in an open (coliseum technique) or closed

General Introduction and Outline of the Thesis | Chapter 1
17
1fashion. Furthermore, the chemotherapeutic compounds and doses also can vary. Until now, in the Netherlands Mitomycin C (MMC) has mainly been the chemotherapeutic agent of choice for this procedure. The inflow temperature of the intra-abdominal perfusate lies between 41-42 degrees Celsius. At this point, the MMC is added at 35 mg/m2 body surface in three fractions at 30 minute intervals. 41 However, in recent years the use of Oxaliplatin for HIPEC has also gained popularity in the Netherlands, and was mostly used for repeat procedures. 41
Reconstruction of the gastrointestinal continuity is classically performed after the intraperitoneal lavage in order to prevent entrapment of tumour cells in the suture lines that in theory could cause recurrence.
Treatment Outcome – Morbidity, Mortality & SurvivalSince the introduction of the CRS & HIPEC technique several institutions have reported very promising results in the treatment of peritoneal carcinomatosis, showing 5-year survival rates of up to 35-45%. 38,39,42,44-46 As with other major surgical procedures, the CRS & HIPEC procedure is accompanied by a relatively high major morbidity (grade III/IV) rate ranging from 12% to 52%. 48,49 Common complications observed after CRS and HIPEC include: hematological complications, bleeding, intra-abdominal collections, infections, embolism and the formation of fistula. 45,50 The mortality rate reported for this approach ranges from one up to 10%. 46,51,52 The complication rate accompanying CRS and HIPEC is considered acceptable, especially when compared to other major gastrointestinal surgical procedures carried out with curative intent. 45 However, it must be noted that there is a learning-curve described for this procedure and that subsequently the morbidity and mortality figures for the more experienced centers are at the lower spectrum of the earlier stated range. 53,54 High volume CRS and HIPEC centres show treatment associated morbidity rates ranging from 12-34% and mortality rates ranging from one to six percent. 45 In addition, the type of resection performed during the CRS has been reported to have an impact on the perioperative outcome of CRS & HIPEC patients. 45 Both left upper-quadrant peritonectomy and small bowel resection were described as having a negative effect on the perioperative outcome after CRS & HIPEC. 45
On average, CRC patients with stage IV disease show a five-year survival rate of approximately 12%. 2 The only RCT conducted in 2003, comparing best systemic chemotherapy with CRS & HIPEC showed a gain in median survival from 12.6 to 22.4 months in patients with isolated PM. In this cohort, a subgroup of patients - in whom there was no residual macroscopic tumour – even showed a five-year survival equal to that of patients undergoing resection for CRLM’s (35-45%). 39,55-57 Moreover, the median

Chapter 1 | General Introduction and Outline of the Thesis
18
overall survival reported in several studies on PM of CRC treated with CRS and HIPEC ranges from 19 to 62 months, showing the best outcome in patients in which a complete cytoreduction was achieved. 34,58-61 The resection of hepatic metastases is the surgical procedure that is currently still the golden standard approach for the treatment a hepatic metastases. 57 Seeing as both procedures carry comparable risks and clinical benefits, we propose that CRS and HIPEC has the potential of becoming the golden standard for the treatment of PM of CRC.
Systemic Chemotherapy versus CRS & HIPECCurrently, there is no data available to compare patients that present with PM of CRC, treated with either curative resection with or without Heated IntraPEritoneal Chemotherapy (HIPEC) or best systemic chemotherapy. However, as stated previously, there is some indication that systemic chemotherapy is less beneficial in PM when compared to its effect in hepatic and lung metastases. 25,26
In general terms, the advent and further development of CRS and HIPEC has radically changed the clinical outcome of patients with isolated PM over the past two decades. Overall, the data presented support the belief that this treatment provides a very promising therapeutic option for this subgroup of patients with metastatic CRC.
There are still several clinical needs that remain to be addressed in order to achieve maximum benefit of this aggressive combined surgical approach in this particular population of metastatic CRC patients.
1. Diagnosis 2. TreatmentAllocation
3. Treatment 4. Aftercare 5. Prognosis
Figure 2. Schematic overview of the clinical course of the colorectal cancer patient presenting with peritoneal metastases

General Introduction and Outline of the Thesis | Chapter 1
19
1Clinical Needs
Currently, the treatment and prognosis of CRC patients is largely based on the tumour, node, metastasis staging classification. 62 Patients with resectable metastatic colorectal cancer, either to the liver or the peritoneum, have benefitted from the aggressive surgical management. At present, the selection of patients with PM for CRS and HIPEC is made roughly on clinical parameters and intraoperative findings, such as the exclusion of hepatic and pulmonary metastases and the PCI score with the aim of successfully resecting all intra-abdominal tumour deposits. 34 However, to date no strong pre-operative predictors of irresectability have been identified. 63 Thus, several clinical needs, or challenges if you will, still exist in this particular population of metastasized colorectal cancer patients. 64
Notwithstanding the extensive work-up, sometimes even including laparoscopic PCI assessment, there are reports that approximately 25% of the patients deemed suitable for CRS and HIPEC are ultimately deemed irresectable and undergo a so-called open-close procedure. 63 This is largely due to either a PCI score of more than 20 or extensive small-bowel involvement, which could not be identified pre-operatively. 63 Extensive involvement of the small-bowel would mean that a significant portion of the small-bowel would need to be resected to achieve a macroscopically complete resection, which leads to short-bowel syndrome.39 Sadly, this constitutes a sizeable proportion (about 20%) of patients in specialized CRS and HIPEC centres. Secondly, it has been observed that patients with a “favourable profile”, based on both PCI and resection outcome after CRS and HIPEC still show a very different treatment outcome than was previously expected based on the aforementioned clinical parameters. Thus, additional stratification tools are essential for the optimization of the entire procedure. In addition, the chemotherapy that is used in HIPEC is still based on the “one size fits all” principle, without any biological stratification. Lastly, when the patient has successfully undergone treatment and has been disease-free for an extended period of time also the prediction of prognosis and aftercare of these patients is of major clinical importance. For example; improving follow-up strategies, stoma-care and possible reversal procedures. With the advent of newer surgical and medical treatments available, we believe the choice for certain strategies in patients with PM requires further personalization, i.e. the implementation of personalized medicine. Further insight into the baseline characteristics, natural course of this metastatic entity, pathobiology and treatment mechanisms is necessary in order to better understand and interpret treatment outcome after CRS and HIPEC. We

Chapter 1 | General Introduction and Outline of the Thesis
20
strongly believe an evident need exists for both clinical and molecular profiling to aid in addressing the aforementioned clinical needs.
Aim & Outline of this thesis
With the identification of several clinical needs, we aim to gain more insight into these clinical challenges that are encountered during the entire course of treatment of CRS and HIPEC patients. This thesis is divided into two main parts. Part one focuses on clinical decision making in order to address some of the challenges faced in this particular population of CRC patients. The second part focuses on how biology could aid clinical decision making in the future.
Clinical Decision Making / Treatment Allocation
Firstly, adequate patient selection for CRS and HIPEC is paramount in effectively treating the individual patient for his or her disease and/or effective aftercare. For this purpose, the first part of this thesis focuses on clinical profiling for treatment allocation and aftercare. Chapter 2 focuses on whether or not patients with both hepatic and peritoneal metastases should be treated with a combination of CRS of the liver and peritoneal surfaces and HIPEC. In Chapter 3 we analyzed the outcome of colostomy reversal procedures in CRS and HIPEC patents in order to enable us to improve prediction of success or failure based on several clinical parameters. This knowledge will ultimately facilitate the counseling of these patients during aftercare. Molecular Approach – Possible Aids in Future Clinical Decision Making
Based on the hypothesis that the phenotype, and thus clinical behaviour, of PM in CRC is driven by underlying biological mechanisms, read outs of disease biology, i.e. biomarkers, will be of help for more refined identification of suitable patients.
Chapter 4 and 5 provide two reviews on biomarkers in PM of CRC with the aim to provide an overview of promising molecular changes reported to be involved in peritoneal dissemination of CRC and to evaluate the potential for clinical application of these biomarkers.
Adhesion to the peritoneal surface is considered one of the key steps in peritoneal dissemination of malignant disease. 10,65 In addition to attachment, angiogenesis, i.e. the formation of new blood vessels, is crucial for the progression of micrometastases to clinically relevant macrometastases. 66 This process depends on interactions between several cell types and extracellular matrix components. Even though this process is not

General Introduction and Outline of the Thesis | Chapter 1
21
1fully understood, there are indications of involvement of the adhesion molecule Versican (VCAN), by possible interaction with Vascular Endothelial Growth Factor (VEGF), a well-known and potent angiogenic factor. In Chapter 6 we subsequently assess the possible role of VCAN, an adhesion molecule, in combination with VEGF as a prognostic biomarkers in CRC patients with PM after treatment with CRS and HIPEC.
Multiple studies have shown the relevance of angiogenesis, measured by the formation of microvessels in colorectal cancer. 67 These studies were predominantly carried out in the setting of either the primary tumour or haematogenuous metastases. To date the expression of the angiogenesis related markers HIF1a, SDF1, CXCR4 and VEGF in peritoneally disseminated CRC is largely unknown and remains to be elucidated. In addition, it is not known if these markers are of prognostic relevance. In Chapter 7 we describe the expression of the aforementioned angiogenesis related markers and microvessel density and whether or not these have prognostic implications in patients with PM of CRC undergoing CRS and HIPEC. Additionally, in Chapter 8 we retrospectively investigated the individual and combined prognostic value of HIF1a, GLUT1 and VEGF expression in patients with colorectal liver metastases and assessed the added value of these molecular biomarkers to established clinicopathological prognostic factors.
Patients with PM originating from CRC are curatively treated by CRS and HIPEC with MMC. In order to better stratify patients and ultimately improve upon the treatment itself, in Chapter 9 we tackle the patient selection and personalization of treatment for CRS and HIPEC patients by attempting to predict MMC sensitivity in-vitro and assess its possible clinical relevance in patient derived tissue from a cohort of CRS and HIPEC patients.
Lastly, it has been described that tumours with the microsatellite instability (MSI) genotype tend to metastasize less to the liver. 68 In contrast, tumours that have the tendency to metastasize to the peritoneum often show mucinous histology and MSI genotype. 69 Hypothetically this could imply that these tumours preferentially metastasize to either the peritoneum or lymph nodes. In Chapter 10 we sought to further characterize the clinical features and oncologic outcomes of BRAF and KRAS mutant early-stage MSI CRCs. However, we only focus on the effect of these changes on cancer specific and overall survival, not directly on pattern of metastatic spread. Because in general PM has a worse outcome 26, we believe this to be a first step in the future development of molecular profiling of early stage tumours in order to be able to predict which of these tumours will develop PM in the future.

Chapter 1 | General Introduction and Outline of the Thesis
22
References
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108.
2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29. doi:10.3322/caac.20138.
3. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. doi:10.3322/caac.21166.
4. Nederlandse Kankerregistratie. wwwcijfersoverkankernl. Available at: http://www.cijfersoverkanker.nl/. Accessed November 20, 2013.
5. Kindler HL, Shulman KL. Metastatic colorectal cancer. Curr Treat Options in Oncol. 2001;2(6):459–471.
6. Koppe MJ, Boerman OC, Oyen WJG, Bleichrodt RP. Peritoneal Carcinomatosis of Colorectal Origin. Annals of Surgery. 2006;243(2):212–222. doi:10.1097/01.sla.0000197702.46394.16.
7. Jayne. Jayne 2002 Br J Surg Peritoneal carcinomatosis. Br J Surg. 2002:1–6.
8. Sugarbaker PH. Peritonectomy procedures. Annals of Surgery. 1995;221(1):29–42.
9. van der Wal JBC, Jeekel J. Biology of the peritoneum in normal homeostasis and after surgical trauma. Colorectal Dis. 2007;9 Suppl 2:9–13. doi:10.1111/j.1463-1318.2007.01345.x.
10. Ceelen WP, Bracke ME. Peritoneal minimal residual disease in colorectal cancer: mechanisms, prevention, and treatment. Lancet Oncology. 2009;10(1):72–79. doi:10.1016/S1470-2045(08)70335-8.
11. van der Bij GJ, Oosterling SJ, Beelen RHJ, Meijer S, Coffey JC, van Egmond M. The Perioperative Period is an Underutilized Window of Therapeutic Opportunity in Patients With Colorectal Cancer. Annals of Surgery. 2009;249(5):727–734. doi:10.1097/SLA.0b013e3181a3ddbd.
12. Gerber SA, Rybalko VY, Bigelow CE, et al. Preferential Attachment of Peritoneal Tumor Metastases to Omental Immune Aggregates and Possible Role of a Unique Vascular Microenvironment in Metastatic Survival and Growth. The American Journal of Pathology. 2006;169(5):1739–1752. doi:10.2353/ajpath.2006.051222.
13. Meyers MA. Distribution of intra-abdominal malignant seeding: dependency on dynamics of flow of ascitic fluid. Am J Roentgenol Radium Ther Nucl Med. 1973;119(1):198–206.
14. Meyers MA. Metastatic seeding along the small bowel mesentery. Roentgen features. Am J Roentgenol Radium Ther Nucl Med. 1975;123(1):67–73.
15. Ketcham AS, Hoye RC, Pilch YH, Morton DL. Delayed intestinal obstruction following treatment for cancer. Cancer. 1970;25(2):406–410.
16. Verwaal VJ, Zoetmulder FAN. Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. European Journal of Surgical Oncology (EJSO). 2004;30(3):280–285. doi:10.1016/j.ejso.2003.12.003.
17. Esquivel J, Chua TC, Stojadinovic A, et al. Accuracy and clinical relevance of computed tomography scan interpretation of peritoneal cancer index in colorectal cancer peritoneal carcinomatosis: a multi-institutional study. J Surg Oncol. 2010;102(6):565–570. doi:10.1002/jso.21601.
18. de Bree E, Koops W, Kröger R, van Ruth S, Verwaal VJ, Zoetmulder FAN. Preoperative computed tomography and selection of patients with colorectal peritoneal carcinomatosis for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. European Journal of Surgical Oncology (EJSO). 2006;32(1):65–71. doi:10.1016/j.ejso.2005.09.016.
19. Koh J-L, Yan TD, Glenn D, Morris DL. Evaluation of preoperative computed tomography in estimating peritoneal cancer index in colorectal peritoneal carcinomatosis. Ann Surg Oncol. 2009;16(2):327–333. doi:10.1245/s10434-008-0234-2.
20. Jacquet P, Jelinek JS, Steves MA, Sugarbaker PH. Evaluation of computed tomography in patients with peritoneal carcinomatosis. Cancer. 1993;72(5):1631–1636.
21. Elias D, Honoré C, Dumont F, et al. Results of systematic second-look surgery plus HIPEC in asymptomatic patients presenting a high risk of developing colorectal peritoneal carcinomatosis. Annals of Surgery. 2011;254(2):289–293. doi:10.1097/SLA.0b013e31822638f6.
22. Elias D, Goeré D, Di Pietrantonio D, et al. Results of systematic second-look surgery in patients at high risk of developing colorectal peritoneal carcinomatosis. Annals of Surgery. 2008;247(3):445–450. doi:10.1097/SLA.0b013e31815f0113.
23. Rau B, Hünerbein M. Diagnostic laparoscopy: indications and benefits. Langenbecks Arch Surg. 2005;390(3):187–196. doi:10.1007/s00423-004-0483-x.

General Introduction and Outline of the Thesis | Chapter 1
23
124. Klaver YLB, Simkens LHJ, Lemmens VEPP,
et al. Outcomes of colorectal cancer patients with peritoneal carcinomatosis treated with chemotherapy with and without targeted therapy. Eur J Surg Oncol. 2012. doi:10.1016/j.ejso.2012.03.008.
25. Klaver YLB, Lemmens VEPP, Creemers GJ, Rutten HJT, Nienhuijs SW, de Hingh IHJT. Population-based survival of patients with peritoneal carcinomatosis from colorectal origin in the era of increasing use of palliative chemotherapy. Annals of Oncology. 2011;22(10):2250–2256. doi:10.1093/annonc/mdq762.
26. Franko J, Shi Q, Goldman CD, et al. Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: a pooled analysis of north central cancer treatment group phase III trials N9741 and N9841. Journal of Clinical Oncology. 2012;30(3):263–267. doi:10.1200/JCO.2011.37.1039.
27. Tol J, Koopman M, Cats A, et al. Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl J Med. 2009;360(6):563–572. doi:10.1056/NEJMoa0808268.
28. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. doi:10.1056/NEJMoa032691.
29. Van Cutsem E, Köhne C-H, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408–1417. doi:10.1056/NEJMoa0805019.
30. Golfinopoulos V, Salanti G, Pavlidis N, Ioannidis JPA. Survival and disease-progression benefits with treatment regimens for advanced colorectal cancer: a meta-analysis. Lancet Oncology. 2007;8(10):898–911. doi:10.1016/S1470-2045(07)70281-4.
31. Koopman M, Antonini NF, Douma J, et al. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced colorectal cancer (CAIRO): a phase III randomised controlled trial. Lancet. 2007;370(9582):135–142. doi:10.1016/S0140-6736(07)61086-1.
32. Tan GHC, Teo MCC, Chen W, et al. Surgical management of colorectal peritoneal metastases: treatment and outcomes compared with hepatic metastases. J Gastrointest Cancer. 2013;44(2):170–176. doi:10.1007/s12029-012-9452-8.
33. Klaver YLB, Leenders BJM, Creemers G-J, et al. Addition of Biological Therapies to Palliative Chemotherapy Prolongs Survival in Patients With Peritoneal Carcinomatosis of Colorectal Origin. Am J Clin Oncol. 2012. doi:10.1097/COC.0b013e3182438c55.
34. Elias D, Lefevre JH, Chevalier J, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of Clinical Oncology. 2009;27(5):681–685. doi:10.1200/JCO.2008.19.7160.
35. Stein A, Schmoll H-J. Systemic treatment of liver metastases from colorectal cancer. Ther Adv Med Oncol. 2013;5(3):193–203. doi:10.1177/1758834012473347.
36. Voest EE, Snoeren N, Schouten SB, et al. A randomized two-arm phase III study to investigate bevacizumab in combination with capecitabine plus oxaliplatin (CAPOX) versus CAPOX alone in post radical resection of patients with liver metastases of colorectal cancer. ASCO Meeting Abstracts. 2011;29(15_suppl):3565.
37. Klaver CEL, Musters GD, Bemelman WA, et al. Adjuvant hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with colon cancer at high risk of peritoneal carcinomatosis; the COLOPEC randomized multicentre trial. BMC Cancer. 2015;15:428. doi:10.1186/s12885-015-1430-7.
38. Zoetmulder FA, van der Vange N, Witkamp AJ, Kaag MM, Boot H, Beijnen JH. [Hyperthermic intra-peritoneal chemotherapy (HIPEC) in patients with peritoneal pseudomyxoma or peritoneal metastases of colorectal carcinoma; good preliminary results from the Netherlands Cancer Institute]. Ned Tijdschr Geneeskd. 1999;143(37):1863–1868.
39. Verwaal VJ. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. Journal of Clinical Oncology. 2003;21(20):3737–3743. doi:10.1200/JCO.2003.04.187.
40. Sugarbaker PH. Peritoneal Carcinomatosis: Principles of Management. Springer; 1996.
41. Kuijpers AMJ, Mirck B, Aalbers AGJ, et al. Cytoreduction and HIPEC in The Netherlands: Nationwide Long-term Outcome Following the Dutch Protocol. Ann Surg Oncol. 2013. doi:10.1245/s10434-013-3145-9.

Chapter 1 | General Introduction and Outline of the Thesis
24
42. Sugarbaker PH. Intraperitoneal chemotherapy and cytoreductive surgery for the prevention and treatment of peritoneal carcinomatosis and sarcomatosis. Semin Surg Oncol. 1998;14(3):254–261.
43. Rampone B. 9. Peritoneal carcinomatosis of colorectal cancer.
44. Elias D, Blot F, Otmany El A, et al. Curative treatment of peritoneal carcinomatosis arising from colorectal cancer by complete resection and intraperitoneal chemotherapy. Cancer. 2001;92(1):71–76.
45. Chua TC, Saxena A, Schellekens JF, et al. Morbidity and mortality outcomes of cytoreductive surgery and perioperative intraperitoneal chemotherapy at a single tertiary institution: towards a new perspective of this treatment. Annals of Surgery. 2010;251(1):101–106. doi:10.1097/SLA.0b013e3181b5ae43.
46. Shen P, Hawksworth J, Lovato J, et al. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy with mitomycin C for peritoneal carcinomatosis from nonappendiceal colorectal carcinoma. Ann Surg Oncol. 2004;11(2):178–186.
47. Chua TC, Esquivel J, Pelz JOW, Morris DL. Summary of current therapeutic options for peritoneal metastases from colorectal cancer. J Surg Oncol. 2012. doi:10.1002/jso.23189.
48. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Annals of Surgery. 2004;240(2):205–213.
49. Chua TC, Yan TD, Saxena A, Morris DL. Should the treatment of peritoneal carcinomatosis by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy still be regarded as a highly morbid procedure?: a systematic review of morbidity and mortality. Annals of Surgery. 2009;249(6):900–907. doi:10.1097/SLA.0b013e3181a45d86.
50. Burgers P, van der Hoeven J, Velde te EA, Boot H. Kliniek en behandeling van postoperatieve enterocutane fistels na cytoreductieve chirurgie gecombineerd met HIPEC. Ned Tijdschr Oncol. 2009.
51. Chua TC, Yan TD, Zhao J, Morris DL. Peritoneal carcinomatosis and liver metastases from colorectal cancer treated with cytoreductive surgery perioperative intraperitoneal chemotherapy and liver resection. European Journal of Surgical Oncology. 2009;35(12):1299–1305. doi:10.1016/j.ejso.2009.07.005.
52. Avital IZ, Brücher BLDM, Nissan A, Stojadinovic A. Randomized clinical trials for colorectal cancer peritoneal surface malignancy. Surgical Oncology Clinics of North America. 2012;21(4):665–688. doi:10.1016/j.soc.2012.07.004.
53. Smeenk RM, Verwaal VJ, Zoetmulder FAN. Learning curve of combined modality treatment in peritoneal surface disease. Br J Surg. 2007;94(11):1408–1414. doi:10.1002/bjs.5863.
54. Yan TD, Links M, Fransi S, et al. Learning curve for cytoreductive surgery and perioperative intraperitoneal chemotherapy for peritoneal surface malignancy--a journey to becoming a Nationally Funded Peritonectomy Center. Ann Surg Oncol. 2007;14(8):2270–2280. doi:10.1245/s10434-007-9406-8.
55. Verwaal VJ, Kusamura S, Baratti D, Deraco M. The eligibility for local-regional treatment of peritoneal surface malignancy. J Surg Oncol. 2008;98(4):220–223. doi:10.1002/jso.21060.
56. Verwaal VJ, Bruin S, Boot H, van Slooten G, van Tinteren H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol. 2008;15(9):2426–2432. doi:10.1245/s10434-008-9966-2.
57. Abdalla EK, Vauthey J-N, Ellis LM, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Annals of Surgery. 2004;239(6):818–25; discussion 825–7.
58. Glehen O. Cytoreductive Surgery Combined With Perioperative Intraperitoneal Chemotherapy for the Management of Peritoneal Carcinomatosis From Colorectal Cancer: A Multi-Institutional Study. Journal of Clinical Oncology. 2004;22(16):3284–3292. doi:10.1200/JCO.2004.10.012.
59. Glehen O, Cotte E, Schreiber V, Sayag-Beaujard AC, Vignal J, Gilly FN. Intraperitoneal chemohyperthermia and attempted cytoreductive surgery in patients with peritoneal carcinomatosis of colorectal origin. Br J Surg. 2004;91(6):747–754. doi:10.1002/bjs.4473.
60. Franko J, Ibrahim Z, Gusani NJ, Holtzman MP, Bartlett DL, Zeh HJ III. Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis. Cancer. 2010;116(16):3756–3762. doi:10.1002/cncr.25116.

General Introduction and Outline of the Thesis | Chapter 1
25
161. Mahteme H, Hansson J, Berglund A, et al.
Improved survival in patients with peritoneal metastases from colorectal cancer: a preliminary study. British Journal of Cancer. 2004;90(2):403–407. doi:10.1038/sj.bjc.6601586.
62. Sobin LH, Compton CC. TNM seventh edition: what“s new, what”s changed: communication from the International Union Against Cancer and the American Joint Committee on Cancer. Cancer. 2010;116(22):5336–5339. doi:10.1002/cncr.25537.
63. van Oudheusden TR, Braam HJ, Luyer MDP, et al. Peritoneal Cancer Patients Not Suitable for Cytoreductive Surgery and HIPEC During Explorative Surgery: Risk Factors, Treatment Options, and Prognosis. Ann Surg Oncol. 2015;22(4):1236–1242. doi:10.1245/s10434-014-4148-x.
64. Verwaal VJ, van Tinteren H, van Ruth S, Zoetmulder FAN. Predicting the survival of patients with peritoneal carcinomatosis of colorectal origin treated by aggressive cytoreduction and hyperthermic intraperitoneal chemotherapy. Br J Surg. 2004;91(6):739–746. doi:10.1002/bjs.4516.
65. Paschos KA, Canovas D, Bird NC. The role of cell adhesion molecules in the progression of colorectal cancer and the development of liver metastasis. Cellular Signalling. 2009;21(5):665–674. doi:10.1016/j.cellsig.2009.01.006.
66. Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013.
67. Wu Y, Jin M, Xu H, et al. Clinicopathologic significance of HIF-1α, CXCR4, and VEGF expression in colon cancer. Clin Dev Immunol. 2010;2010. doi:10.1155/2010/537531.
68. Tran B, Kopetz S, Tie J, et al. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer. 2011;117(20):4623–4632. doi:10.1002/cncr.26086.
69. Catalano V, Loupakis F, Graziano F, et al. Mucinous histology predicts for poor response rate and overall survival of patients with colorectal cancer and treated with first-line oxaliplatin- and/or irinotecan-based chemotherapy. British Journal of Cancer. 2009;100(6):881–887. doi:10.1038/sj.bjc.6604955.


Chapter 2Cytoreductive surgery and HIPEC for
peritoneal metastases combined with curative treatment of colorectal liver metastases
Systematic review of all literature and meta-analysis of observational studies
E.M.V. de Cuba
R. Kwakman
D.L. Knol
H.J. Bonjer
G.A. Meijer
E.A. te Velde
Cancer Treat Rev. 2013 Jun;39(4):321-7

Chapter 2 | CRS & HIPEC for combination PM and CRLM
28
Abstract
Objective: Assess the overall outcome in colorectal cancer (CRC) patients that present with a combination of peritoneal metastases (PM) and liver metastases (CRLM) after curative resection and hyperthermic intraperitoneal chemotherapy (HIPEC) in the current literature.
Methods: A systematic literature search according to the PRISMA guidelines was conducted using the PubMeddatabase of the U.S. National library of Medicine using the keywords: colorectal cancer, liver metastasis, extra-hepatic, peritoneal metastases, peritoneal carcinomatosis, cytoreductive surgery (CRS), HIPEC and combinations hereof. Papers focusing on CRS and HIPEC for PM combined with curative treatment of CRLM were included, provided sufficient information on survival outcomes could be extracted. Duplicate publications were excluded. Meta-analysis was performed using the method described by Tierney et al.
Results: After screening and full-text assessment of 39 papers, six articles were included containing data on combined PM and CRLM in patients treated with curative resection of both sites and HIPEC or early postoperative intraperitoneal chemotherapy (EPIC). Three articles provided enough statistical information for meta-analysis. Pooled hazard ratio (HR) was extracted from survival curves and was 1.24 (CI 0.96–1.60). A comparison was made with patients presenting with isolated PM undergoing CRS and HIPEC and with patients with disseminated disease undergoing (modern) systemic chemotherapy.
Conclusions: In the absence of randomized controlled studies, we found in this systematic review and meta-analysis of patients with a combination of colorectal metastases in the liver as well as in the peritoneum show a trend towards a lower overall survival after curative resection and HIPEC, when compared to patients with isolated peritoneal metastases after CRS and HIPEC (pooled HR1.24, CI 0.96–1.60). However, patients with metastatic CRC show a tendency towards increased median overall survival after CRS and HIPEC combined with resection of liver metastases when compared to treatment with modern systemic chemotherapy.

CRS & HIPEC for combination PM and CRLM | Chapter 2
29
2
Introduction
Colorectal carcinoma (CRC) is the third most common cancer worldwide. 1 Approximately half of CRC patients develop distant metastasis, mainly through haematogenous dissemination to the liver via the portal circulation 2,3 These colorectal liver metastases (CRLM) are preferably treated by surgical resection, 3-5 achieving a 5-year survival rate of 35-45%. 4,6,7
Distant metastases from CRC to the peritoneum, i.e. peritoneal metastases (PM) develop in 10-25 % of the CRC patients and in up to 25% the peritoneum is the sole site of metastasis. 3,8 It is not known whether this is a different aetiology of metastasizing, and if so, if it is influenced by the (biology of) the primary tumour, the host, the metastasis or a combination of the aforementioned 9. Based on the observed metastasis pattern, PM is generally considered a local form of CRC dissemination 10. Local aggressive treatment is therefore warranted in a select group of patients presenting with PM 6,11
Traditionally, untreated PM is associated with poor survival of about 6-12 months. Even modern systemic chemotherapy does not seem to yield any clinically significant gain in survival for patients presenting with PM. 12-14 In the early 1990’s a treatment with a curative intent for patients with PM of CRC, without evidence of distant metastasis was introduced, which consists of surgery (cytoreductive surgery, CRS) combined with heated intraperitoneal chemotherapy (HIPEC). 15,16 In a prospective randomised controlled trial (RCT) a subgroup of patients - in whom there was no residual macroscopic tumour - showed a five-year survival equal to that of patients undergoing resection for CRLM’s (35-45%). 7,17 Data obtained from several non-randomized comparative studies support this finding, reporting 5-year overall survival rates of up to 51%. 12,18
It is not known what percentage of CRC patients present with PM in combination with liver metastases. In combination with other distant metastases it is estimated to be approximately 75% 3,8,19 The presence of liver metastasis is considered a contra-indication for CRS & HIPEC. 6,8,20 Moreover, the presence of PM is also considered a contraindication for curative resection of CRLMs. 19,21,22
Since both separate sites of metastasis have been curatively treated by surgery, cases have been reported of patients with PM of CRC that have been treated with a combination of resection, including that of liver metastases and HIPEC. This has proven to be feasible 6,10,23,24. We conducted a systematic review, according to the PRISMA guidelines, focussing on papers reporting the clinical outcomes of patients with a combination of PM and CRLM, treated with CRS and HIPEC combined with curative treatment for the concomitant CRLM. In addition, a meta-analysis of published data was performed.

Chapter 2 | CRS & HIPEC for combination PM and CRLM
30
Materials and Methods
Literature search
A systematic literature search was conducted using the PubMed database of the U.S. National library of Medicine using the following keywords: colorectal cancer, liver metastasis, extra-hepatic, peritoneal metastases, peritoneal carcinomatosis, cytoreductive surgery, HIPEC and combinations hereof (Table 1) Papers focussing on cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of CRLM, but providing enough information on survival outcome after treatment with curative intent were included.These search terms were employed in order to include as many publications as possible on the subject. Additional papers were incorporated by manually cross-referencing from publications retrieved in the initial search. Only full-text papers in English were included that have been published between 1990 and April 2012. Considerable effort was made to detect possible duplication of published data by reviewing the institutions, authors and period of follow-up reported.
Table 1: Search strategy
Colorectal cancer
AND
extrahepatic
peritoneal metastasis
peritoneal carcinomatosis
cytoreductive surgery
HIPEC
liver metastasis AND
HIPEC
cytoreductive surgery
extrahepatic
peritoneal metastasis AND
cytoreductive surgery AND
HIPEC HIPEC
peritoneal carcinomatosis AND
cytoreductive surgery AND
HIPEC HIPEC

CRS & HIPEC for combination PM and CRLM | Chapter 2
31
2
Inclusion- & Exclusion criteria
Initially, all available observational cohort studies were considered. Studies on CRC patients with peritoneal- in combination with liver metastases, treated with a combination of CRS & HIPEC and curative treatment of the liver metastases were included for individual review. Additional review was conducted when deemed necessary. Studies in which data on the PM in combination with CRLM curatively treated with CRS & HIPEC and hepatic resection or an ablative technique could not be extracted from the published article were excluded from the final analysis. When studies overlapped or duplicated, those articles with more complete data on the subgroup of interest were retained.
Quality assessment & Data extraction
To assess study quality we used the North-England evidence-based guidelines. 25-27
Categories of evidence:Ia: Evidence obtained from meta-analysis or randomized controlled trialsIb: Evidence obtained from at least one RCTIIa: Evidence obtained from at least one well-designed controlled study without
randomizationIIb: Evidence Obtained from at least one other type of well-designed controlled study
without randomizationIII: Evidence obtained from well-designed non-experimental descriptive studies such as
comparative studies, correlation studies and case studiesIV: Evidence obtained from expert committee reports or opinions, or clinical experiences
of respected authorities
We extracted relevant data from all full-text articles. These included the following parameters: First author, year of publication, study design, level of evidence, study population characteristics, number of patients in the PM in combination with CRLM group as a percentage of the entire study population, time of follow-up, and all available survival data. To ensure accuracy and minimize bias, all noticed discrepancies were discussed and settled through consensus discussion.
Statistical analysis
Survival outcomes reported in the included series was the main area of interest. The median overall survival was the outcome used to report the initial comparison between the different cohorts.

Chapter 2 | CRS & HIPEC for combination PM and CRLM
32
In the absence of randomized controlled trials on this subject, we further assess the survival outcomes of patients curatively treated for the combination of PM and CRLM versus PM alone by subsequently analysing included series with comparative cohorts. They were included in the meta-analysis on the condition that the published article provides enough statistical information to do so. All included studies were weighed using the inverse variance, the precision, to assess the effects of the cohorts included. Hazard ratio (HR) was used as measure for comparison in the meta-analysis, which was extracted from each published cohort included from the Kaplan-Meier by using the method previously described by Tierney et al. 28. The subsequent pooled HR and its corresponding 95% confidence interval (CI) were subsequently calculated using a fixed model as described by DerSimonian et al. 29 For the generation of the corresponding figures, we utilized a web-based meta-analysis tool 30 . Further statistical analysis of the data was performed using the statistical package for the social sciences (SPSS Inc, Chicago IL) version 18 for OSx.
Results
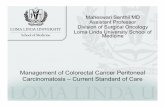
We identified a grand total of 939 publications for screening and selection. Fig. 1 shows the flowchart depicting the literature search and selection process.
Observational studies and meta-analysis
After meticulous screening and selection, six articles of interest remained. Reasons for excluding 33 full-text articles are summarized in figure 1, one of which is exclusion of 4 duplicate or overlapping publications (based on same patient cohort in time). To correct for this, we included the most recently published article with complete data on the subgroup of interest in our analysis. The remaining six articles provided minimally the median overall survival of the group with a combination of PM and CRLM curatively treated with CRS and HIPEC in combination with hepatectomy, radio-frequency ablation (RFA) or cryosurgery. All eligible studies were published in between 2004 and 2010. Representing data on a total of 139 patients, with the biggest cohort being included in the most recent study, comprising of 70 patients. 21 The follow-up per study ranged from 1 month up to five years. 20,21,31-34 All studies reported overall survival for this particular subpopulation. It was only possible to extract individual patient data from 1 study 32. The median overall survival reported ranged from 6 months and 36 months (fig.2). Figure two depicts reported range of overall survival reported in these six studies in contrast to the range in overall survival reported in literature on 1) several (sub)groups of patients presenting with isolated PM treated with CRS and HIPEC 6,7,12,18,35-38 and 2) patients extracted from several series with PM of CRC treated with (modern) systemic chemotherapy, including biologicals. 13,14,39-41

CRS & HIPEC for combination PM and CRLM | Chapter 2
33
2
1
930 records identified through database searching
9 additional records identified through other sources
765 after removal of duplicates
765 records screened 728 records excluded
39 full-text articles assessed for eligibility
6 studies included in qualitative synthesis
33 full-text articles excluded
3 studies included in quantitative synthesis
(meta-analysis)
Identification
Screening
Eligibility
Included
1 describing only PM patients
3 describing only CRLM patients
5 failures to retrieve PM in combination with CRLM data
4 double publication
3 describing multiple primary malignancies
8 reviews
5 only debulking
1 only debulking in combination with systemic chemotherapy
1 comparison PM versus CRLM,
not combination
1 HIPEC after failure prior treatment
1 Quality of life study
Figure 1: Flowchart of inclusion of the studies.
All patients in the six analysed studies underwent CRS and HIPEC or EPIC for the treatment of the PM of CRC. The treatment of CRLM varied per study. All main characteristics of these studies are summarized in table 2. By considering the known prognostic factors affecting treatment outcome after CRS and HIPEC for patients with PM of CRC as described previously 7,44, some aspects stand out that differ between the studies; We noticed that there is considerable difference between the baseline characteristics of the population undergoing CRS plus HIPEC (PCI, presence of malignant ascites, occlusive syndrome). The methods of reporting the total intra-abdominal disease burden, excluding the CRLM, differ per study. In some the Gilly method is applied and in others the peritoneal cancer index is utilized. Overall, the PCI range can be broken down into PCI ≥ 11-20 and PCI ≤ 11. Two studies also included patients with PCI ≥ 11-20 20,34, while the remaining four studies included predominantly patients with PCI ≤ 11 21,31-
33. Overall in all six studies the cohort reported is comprised predominantly of patients in whom an R0 resection was achieved. Elias et al only included patients (100%) in which an R0 was achieved 21.

Chapter 2 | CRS & HIPEC for combination PM and CRLM
34
Tabl
e 2:
Mai
n ch
arac
teris
tics o
f six
arti
cles
incl
uded
in th
e qu
alita
tive
anal
ysis
1st a
utho
rYe
ar o
f Pu
blic
atio
nPM
+ C
RL
M
Num
ber
of
patie
nts
(as %
of t
otal
st
udy
popu
latio
n)
Med
ian
OS
(mnt
hs)
PM
Trea
tmen
t m
etho
d
HIP
EC
/ E
PIC
co
mpo
und
HIP
EC
m
etho
d
Per-
oper
ativ
e sy
stem
ic
chem
othe
rapy
us
ed
CR
LM
tr
eatm
ent
met
hod
LE
Car
mig
nani
2004
subp
opul
atio
n16
(59.
3%)
15.2
CR
S +
HIP
EC/E
PIC
MM
C /
5-FU
Col
iseu
m
tech
niqu
eU
nkno
wn
Res
ectio
n or
le
ft in
-situ
III
Kia
nman
esh
2007
subp
opul
atio
n16
(37%
)36
.0C
RS
+ H
IPEC
MM
C -
Cis
plat
inU
nkno
wn
Unk
now
nR
esec
tion
III
Chu
a20
09su
bpop
ulat
ion
16 (2
9.1%
)
*C
RS
+ H
IPEC
/EPI
CM
MC
/ 5-
FUU
nkno
wn
Unk
now
nR
esec
tion
+ C
ryo-
surg
ery
III
Varb
an20
09su
bpop
ulat
ion
14 (9
.9%
)23
.0C
RS
+ H
IPEC
MM
CC
lose
d te
chni
que
Unk
now
nR
esec
tion,
C
ryo-
surg
ery
+ R
FA
III
Cav
alie
re20
10su
bpop
ulat
ion
7 (6
.2%
)6.
0C
RS
+ H
IPEC
MM
C -
Cis
plat
in
Oxa
lipla
tin
Col
iseu
m
tech
niqu
e +
clos
ed
5-FU
+
Leuc
ovor
inU
nkno
wn
III
Elia
s20
10su
bpop
ulat
ion
70 (1
5.9%
)24
.7C
RS
+ H
IPEC
/EPI
CM
MC
/ 5-
FUM
ultip
le5-
FU +
Le
ucov
orin
Unk
now
nII
I
* M
MC
= M
itom
ycin
C, R
FA=
Rad
io-F
requ
ency
Abl
atio
n, L
E= L
evel
of E
vide
nce
*The
med
ian
over
all s
urvi
val c
ould
not
be
extra
cted
, how
ever
it w
as p
ossi
ble
to c
alcu
late
the
corr
espo
ndin
g H
R u
sing
the
Tier
ney
et a
l met
hod

CRS & HIPEC for combination PM and CRLM | Chapter 2
35
2
One study also included patients with malignant ascites and occlusive syndrome, both factors that have been reported to negatively impact survival after treatment. 20,44
Data on lymph node status and response to adjuvant chemotherapy were not available for further analysis.Furthermore, two out of six studies provided detailed description of the associated CRLM. The number reported ranged from 1-7, with a median of 1. 32,33 The article by Varban et al also reported a median diameter of 3 cm, ranging from 0.4-12 cm. 33 The remaining publications did not provide data on the number, site and diameter of the associated CRLM.In light of the overall either retrospective or not-controlled nature of the studies, we performed a meta-analysis of available observational studies. For the meta-analysis, three out of six studies assessed in detail provided sufficient statistical information for adequate analysis. 28 A combined total of 100 patients were included in these studies with a combination of PM and CRLM of CRC. When compared to CRC patients whom present with isolated PM, the calculated HR was 1.24 (CI 0.96-1.60).
0 10 20 30 40 50 60 70 801
2
3
4
5
6
Median Overall Survival Reported in Months
Modern SC
5-FU based SC
CRS & HIPEC - Only R0
Combined treatment of PM & CRLM with CRS &
HIPEC
CRS & HIPEC
RCT: 22.4
Subgroup
10.4 - 23.9
5.2 - 12.6
6.0 - 36.0
19.0 - 62.7
28.0 - 62.7
Figure 2: Reported median overall survival in several subgroups of patients presenting with PM of CRC. Modern SC = Cohort of PM patients treated with modern systemic chemotherapy (irinotecan, oxaliplatin, biological) 14,18,39,39-41. 5-FU based SC= chemotherapy regiment based on 5-FU. 7,8,18,42,43 Combined treatment of PM & CRLM with CRS & HIPEC = Patients presenting with combination of PM and liver metastasis treated with CRS and HIPEC. 20,21,31-34 CRS & HIPEC = Good quality non-randomized comparative trials on patients with isolated PM treated with cytoreduction and HIPEC. 6,18,35,36 Only CCRO= Patients presenting with isolated PM in which complete cytoreduction was achieved, followed by HIPEC. 18,37
Arrow: Reported Median Overall Survival extracted from only Randomized Controlled Trial conducted by Verwaal and colleagues. 7

Chapter 2 | CRS & HIPEC for combination PM and CRLM
36
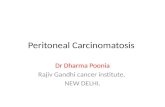
0.0 0.4 0.8 1.2 1.6 2.0 0.0 Forest Plot
0.0 0.4 0.8 1.2 1.6 2.0 0.0 Forest Plot
STUDY HR
Chua 2009 (16)
Elias 2010 (70)
Varban 2009 (14)
0.92 (0.32 - 2.32)
1.17 (0.71 - 1.94)
1.31 (0.96 - 1.77)
Pooled HR 1.24 (0.96 - 1.60)
Figure 3: Forest plot of the three selected studies that provided sufficient statistical information
Discussion
Currently the presence of liver metastasis is a contraindication for treatment of diagnosed peritoneal metastases (PM) with cytoreductive surgery (CRS) and hyperthermic intra-peritoneal chemotherapy (HIPEC). 6,8,20 Conversely, the presence of PM is considered a contraindication for curative resection of CRLMs. 19,21,22 Despite the fact that presence of CRLM is officially a contraindication for CRS and HIPEC, there is a selected group of patients presenting with a combination of CRLM and PM of CRC that are curatively treated by an aggressive surgical approach. 20,21,31-34,45 In 2008 consensus was reached which stated that concomitant liver metastases are only to be resected when confined to three or less well-resectable lesions. 17,24,46-48 In addition eligible patients should have a good performance status and low co-morbidity. 46,47,49 Literature also reports that disease which responds adequately to neo-adjuvant systemic chemotherapy, i.e. reduction of overall tumour burden or no progressive disease during treatment, as having a less aggressive tumour biology. This is cited as a favourable factor in selecting patients for this aggressive approach. 33,46
After analysis of the available data, we found that there are no prospective randomized controlled trails for this particular subgroup of PM of CRC patients. The selected group of patients undergoing this aggressive approach mostly consists of those with three or less, well resectable CRLM and relatively low PCI. During our systematic review of published literature we also identified a total of eight reviews, however three were centred on CRLM and extrahepatic disease in general without the addition of CRS and HIPEC 50-52, three reviewed only CRS and HIPEC in patients with isolated PM 53-55 and the remaining two included data on patients with PM in combination with CRLM 56,57. One article centred

CRS & HIPEC for combination PM and CRLM | Chapter 2
37
2
largely on CRLM and extrahepatic disease and discussed one study by Elias et al in their manuscript 56. The review article published more recently, in 2009, discussed a number of studies included in our review as well. However, they did not apply the PRISMA guidelines in their literature search and due to the timeframe in which their analysis was performed they did not include two publications on the subject published in 2009. 32,33,57 Both these studies are of importance, because they were published after the 2008 consensus was reached and thus have included a carefully selected group of patients with mostly less than three CRLMs. In addition, the size of the published original series in literature is relatively small and of an observational nature. Therefore, we performed a meticulous (meta-) analysis of the available data, in the absence of randomized trials. This first meta-analysis of the published data will facilitate clinical decision-making and aid in identifying the boundaries of our treatment in this group of metastatic CRC patients. As depicted in table 2 the included studies varied in different treatments administered. Not only for PM of CRC, but also for the associated CRLM. For PM, comparison is a challenge, because the studies vary in respects to the intra-peritoneal regimen used (EPIC vs HIPEC), i.e. the procedure is not standardized. With variations in exposure techniques, administered drugs, doses, duration, optimal temperature and flow rates, makes the comparison between the different cohorts of patients a difficult task. 52 Also different systemic chemotherapy was administered, even though it has been reported that modern chemotherapeutic regimens do not seem to alter the outcome in this subgroup of metastatic colorectal cancer patients 49,58 One tendency observed in reporting was that studies prior to the consensus meeting of 2008 do include patients with concomitant CRLM, but reported no detailed data on the number, site, resectability and diameter of the lesions. Thus no conclusion can be drawn on the baseline variables concerning the present CRLMs in our analysis. However, two out of four studies published after 2008 have reported the presence of CRLM in more detail. These included patients with median 1 CRLM, ranging from 1-7, with limited PCI (mostly ≤11). Both studies show promising treatment results, with median overall survival rates ranging from 23-36 months. In addition, they report no statistically significant difference in overall survival between patients with isolated PM and those with concomitant CRLM. 32,33 However, in one study they also point out that the peritoneal cancer index of the patients with a combination of PM and CRLM is significantly lower at baseline when compared to those with isolated PM.32
We extracted data from three studies for a meta-analysis according to the Tierney method 28. We found a pooled HR of 1.24 (CI0.96-1.60). This indicates that patients with a combination of PM and CRLM at first glance seem to fare less well when compared to patients with isolated PM treated with CRS and HIPEC. (Fig 2 & 3) However, this finding is not statistically significant. To date, patients that are excluded from CRS & HIPEC are usually referred to the oncologist for best systemic therapy in a palliative setting. Currently, there

Chapter 2 | CRS & HIPEC for combination PM and CRLM
38
is no data available to compare patients that present with a combination of PM and CRLM of CRC, treated with either curative resection and HIPEC or best systemic chemotherapy. In recent years there has been considerable progress in overall survival with modern chemotherapy regiments in metastatic colorectal cancer. 59,60 However, results from data extracted from the CAIRO series and an article by Franko and colleagues show that median overall survival in patients with isolated PM, treated with several systemic chemotherapy regiments ranges from 5.2 to 23.9. (Fig.2) 13,35,39-41 14 One obstacle in interpreting this data is however the fact that CRS and HIPEC patients are a highly selected group of patients in contrast to the rather heterogeneous population of metastatic colorectal cancer treated with systemic chemotherapy. 14,18The study conducted by Franko et al does however contain a large number of patients presenting with PM in combination with CRLM (62.7%). 14 The reported median overall survival for the entire cohort was 12.7 months. The data extracted from the studies used are of moderate quality, due to the fact that some cohorts were rather small in size. As a result the ultimate result of the meta-analysis could be considerably influenced by the effect of one rather large study containing seventy patients. 21 The confidence interval ranging from 0.96 to 1.60 does imply a statistical uncertainty of this calculated HR. However, in light of the paucity of data concerning this particular subgroup of patients we still feel that our approach is scientifically valid and useful for facilitating clinical decision-making and identifying the boundaries of our treatment in this group of metastatic CRC patients.Based on current literature and our most recent findings, patients presenting with a combination of PM and CRLM of seem to fare less well when compared to patients presenting with isolated PM. However, this could be explained as due to the additional tumour burden if one considers the abdomen as a whole. Nonetheless, based on our analysis there is currently no evidence to support exclusion of patients with additional metastases to the liver from aggressive, potentially curative, treatment. Figure 2 also shows a tendency towards better overall survival in carefully selected patients with a combination of PM and CRLM who are treated with curative resection of both sites plus HIPEC. Taking into consideration the abovementioned, careful assessment of the current literature and the available data for meta-analysis suggest that a combination of CRS and HIPEC with curative treatment for CRLM will in all likelihood result in improved survival, compared to treatment with modern systemic chemotherapy alone. However, further research comparing the different treatment modalities in a well-defined and matched subgroup of CRS and HIPEC patients is necessary.Prediction of the patients in whom the disease will be restricted to local growth in both sites versus those in which it will disseminate further and shift via the haematogenous and/or the lymphatic route will prevent futile surgical intervention. But until we reach the era in which molecular markers can lead the way in treatment decisions in this population we

CRS & HIPEC for combination PM and CRLM | Chapter 2
39
2
will have to rely on clinical and pathological parameters, such as the aggressiveness of the tumour (chemotherapy response), resectability and overall intra-abdominal tumour burden.In conclusion, overall the international reported experience with cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases is limited, as highlighted by the small amount of literature retrieved on the subject. In the absence of randomized controlled studies, we found in this systematic review and meta-analysis of a selected group of patients with a combination of colorectal metastases in the liver as well as in the peritoneum seem to have a lower median overall survival after curative resection and HIPEC, when compared to patients with peritoneal metastases only after CRS and HIPEC. However, when patients were treated with CRS and HIPEC and curative treatment of liver metastases, we found indications for improved (median) overall survival as compared to patients treated with modern systemic chemotherapy. 13,14,21 In addition, a recent study on the specific complications associated with hepatobilliary procedures in CRS and HIPEC patients reports a low rate of said complications. 61 Hence, there is currently no solid evidence on which to validate exclusion of carefully selected patients from potentially curative resection and HIPEC. Twenty-five percent of patients that are eligible for curative resection of liver metastases will not undergo treatment due to presence of extrahepatic disease, mostly peritoneal metastases. 62 In addition, a currently unknown proportion of potential CRS and HIPEC candidates are also excluded due to haematogenous spread to the liver. Keeping in mind these statistics, we consider further studies on cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases to be warranted.

Chapter 2 | CRS & HIPEC for combination PM and CRLM
40
References1. Parkin DM, Bray F, Ferlay J, Pisani P. Global
cancer statistics, 2002. CA Cancer J Clin 2005;55(2):74–108.
2. Bird NC, Mangnall D, Majeed AW. Biology of colorectal liver metastases: A review. J Surg Oncol 2006;94(1):68–80.
3. Koppe MJ, Boerman OC, Oyen WJG, Bleichrodt RP. Peritoneal Carcinomatosis of Colorectal Origin. Annals of Surgery 2006;243(2):212–22.
4. Abdalla EK, Vauthey J-N, Ellis LM, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Annals of Surgery 2004;239(6):818–25; discussion825–7.
5. Scheele J, Altendorf-Hofmann A. Resection of colorectal liver metastases. Langenbecks Arch Surg 1999;384(4):313–27.
6. Glehen O. Cytoreductive Surgery Combined With Perioperative Intraperitoneal Chemotherapy for the Management of Peritoneal Carcinomatosis From Colorectal Cancer: A Multi-Institutional Study. Journal of Clinical Oncology 2004;22(16):3284–92.
7. Verwaal VJ. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. Journal of Clinical Oncology 2003;21(20):3737–43.
8. Jayne. Jayne 2002 Br J Surg Peritoneal carcinomatosis. Br J Surg 2002;:1–6.
9. de Cuba EMV, Kwakman R, van Egmond M, et al. Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : Future possibilities for personalised treatment by use of biomarkers. Virchows Arch 2012;:1–31.
10. Elias D, Sideris L, Pocard M, et al. Results of R0 Resection for Colorectal Liver Metastases Associated With Extrahepatic Disease. Ann Surg Oncol 2004;11(3):274–80.
11. Verwaal VJ, Bruin S, Boot H, van Slooten G, van Tinteren H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol 2008;15(9):2426–32.
12. Cao Y, Tan A, Gao F, Liu L, Liao C, Mo Z. A meta-analysis of randomized controlled trials comparing chemotherapy plus bevacizumab with chemotherapy alone in metastatic colorectal cancer. Int J Colorectal Dis 2009;24(6):677–85.
13. Klaver YLB, Simkens LHJ, Lemmens VEPP, et al. Outcomes of colorectal cancer patients with peritoneal carcinomatosis treated with chemotherapy with and without targeted therapy. Eur J Surg Oncol 2012;
14. Franko J, Shi Q, Goldman CD, et al. Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: a pooled analysis of north central cancer treatment group phase III trials N9741 and N9841. Journal of Clinical Oncology 2012;30(3):263–7.
15. Sugarbaker PH. Patient selection and treatment of peritoneal carcinomatosis from colorectal and appendiceal cancer. World J Surg 1995;19(2):235–40.
16. Sugarbaker PH. Peritonectomy procedures. Annals of Surgery 1995;221(1):29–42.
17. Verwaal VJ, Kusamura S, Baratti D, Deraco M. The eligibility for local-regional treatment of peritoneal surface malignancy. J Surg Oncol 2008;98(4):220–3.
18. Elias D, Lefevre JH, Chevalier J, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of Clinical Oncology 2009;27(5):681–5.
19. Maggiori L, Elias D. Curative treatment of colorectal peritoneal carcinomatosis: current status and future trends. Eur J Surg Oncol 2010;36(7):599–603.
20. Kianmanesh R, Scaringi S, Sabate J-M, et al. Iterative Cytoreductive Surgery Associated With Hyperthermic Intraperitoneal Chemotherapy for Treatment of Peritoneal Carcinomatosis of Colorectal Origin With or Without Liver Metastases. Annals of Surgery 2007;245(4):597–603.
21. Elias D, Glehen O, Pocard M, et al. A Comparative Study of Complete Cytoreductive Surgery Plus Intraperitoneal Chemotherapy to Treat Peritoneal Dissemination From Colon, Rectum, Small Bowel, and Nonpseudomyxoma Appendix. Annals of Surgery 2010;251(5):896–901.
22. Aoki T, Umekita N, Tanaka S, Noda K, Warabi M, Kitamura M. Prognostic value of concomitant resection of extrahepatic disease in patients with liver metastases of colorectal origin. Surgery 2008;143(6):706–14.
23. Elias D, Ouellet JF, Bellon N, Pignon JP, Pocard M, Lasser P. Extrahepatic disease does not contraindicate hepatectomy for colorectal liver metastases. Br J Surg 2003;90(5):567–74.

CRS & HIPEC for combination PM and CRLM | Chapter 2
41
2
24. Elias DM. Peritoneal carcinomatosis or liver metastases from colorectal cancer: similar standards for a curative surgery? Ann Surg Oncol 2004;11(2):122–3.
25. Eccles M, Clapp Z, Grimshaw J, et al. North of England evidence based guidelines development project: methods of guideline development. BMJ 1996;312(7033):760–2.
26. Eccles M, Clapp Z, Grimshaw J, et al. Developing valid guidelines: methodological and procedural issues from the North of England Evidence Based Guideline Development Project. Qual Health Care 1996;5(1):44–50.
27. Eccles M, Rousseau N, Freemantle N. Updating evidence-based clinical guidelines. J Health Serv Res Policy 2002;7(2):98–103.
28. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007;8:16.
29. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7(3):177–88.
30. Chang A, editor. StatTools [Internet]. [cited 2012 Jun. 6]. Available from: http://www.stattools.net/ForestPlot_Pgm.php
31. Carmignani CP, Ortega-Perez G, Sugarbaker PH. The management of synchronous peritoneal carcinomatosis and hematogenous metastasis from colorectal cancer. European Journal of Surgical Oncology (EJSO) 2004;30(4):391–8.
32. Chua TC, Yan TD, Zhao J, Morris DL. Peritoneal carcinomatosis and liver metastases from colorectal cancer treated with cytoreductive surgery perioperative intraperitoneal chemotherapy and liver resection. European Journal of Surgical Oncology 2009;35(12):1299–305.
33. Varban O, Levine EA, Stewart JH, McCoy TP, Shen P. Outcomes associated with cytoreductive surgery and intraperitoneal hyperthermic chemotherapy in colorectal cancer patients with peritoneal surface disease and hepatic metastases. Cancer 2009;115(15):3427–36.
34. Cavaliere F, De Simone M, Virzì S, et al. Prognostic factors and oncologic outcome in 146 patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: Italian multicenter study S.I.T.I.L.O. European Journal of Surgical Oncology 2011;37(2):148–54.
35. Franko J, Ibrahim Z, Gusani NJ, Holtzman MP, Bartlett DL, Zeh HJ III. Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis. Cancer 2010;116(16):3756–62.
36. Mahteme H, Hansson J, Berglund A, et al. Improved survival in patients with peritoneal metastases from colorectal cancer: a preliminary study. British Journal of Cancer 2004;90(2):403–7.
37. Avital IZ, Brücher BLDM, Nissan A, Stojadinovic A. Randomized clinical trials for colorectal cancer peritoneal surface malignancy. Surgical Oncology Clinics of North America 2012;21(4):665–88.
38. Yan TD. Systematic Review on the Efficacy of Cytoreductive Surgery Combined With Perioperative Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis From Colorectal Carcinoma. Journal of Clinical Oncology 2006;24(24):4011–9.
39. Klaver YLB, Leenders BJM, Creemers G-J, et al. Addition of Biological Therapies to Palliative Chemotherapy Prolongs Survival in Patients With Peritoneal Carcinomatosis of Colorectal Origin. Am J Clin Oncol 2012;
40. Tol J, Koopman M, Cats A, et al. Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl J Med 2009;360(6):563–72.
41. Koopman M, Antonini NF, Douma J, et al. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced colorectal cancer (CAIRO): a phase III randomised controlled trial. Lancet 2007;370(9582):135–42.
42. Sadeghi B, Arvieux C, Glehen O, et al. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer 2000;88(2):358–63.
43. Chu DZ, Lang NP, Thompson C, Osteen PK, Westbrook KC. Peritoneal carcinomatosis in nongynecologic malignancy. A prospective study of prognostic factors. Cancer 1989;63(2):364–7.
44. Shen P, Hawksworth J, Lovato J, et al. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy with mitomycin C for peritoneal carcinomatosis from nonappendiceal colorectal carcinoma. Ann Surg Oncol 2004;11(2):178–86.
45. Elias D, Benizri E, Pocard M, Ducreux M, Boige V, Lasser P. Treatment of synchronous peritoneal carcinomatosis and liver metastases from colorectal cancer. European Journal of Surgical Oncology (EJSO) 2006;32(6):632–6.
46. Elias D, Liberale G, Vernerey D, et al. Hepatic and Extrahepatic Colorectal Metastases: When Resectable, Their Localization Does Not Matter, But Their Total Number Has a Prognostic Effect. Ann Surg Oncol 2005;12(11):900–9.

Chapter 2 | CRS & HIPEC for combination PM and CRLM
42
47. Esquivel J, Elias D, Baratti D, Kusamura S, Deraco M. Consensus statement on the loco regional treatment of colorectal cancer with peritoneal dissemination. J Surg Oncol 2008;98(4):263–7.
48. Baratti D, Kusamura S, Deraco M. The Fifth International Workshop on Peritoneal Surface Malignancy (Milan, Italy, December 4-6, 2006): methodology of disease-specific consensus. 2008. p. 258–62.
49. Carpizo DR, D’Angelica M. Liver resection for metastatic colorectal cancer in the presence of extrahepatic disease. Lancet Oncology 2009;10(8):801–9.
50. Yang X-J, Li Y, al-shammaa Hassan AH, et al. Cytoreductive Surgery Plus Hyperthermic Intraperitoneal Chemotherapy Improves Survival in Selected Patients with Peritoneal Carcinomatosis from Abdominal and Pelvic Malignancies: Results of 21 Cases. Ann Surg Oncol 2008;16(2):345–51.
51. Pawlik TM, Schulick RD, Choti MA. Expanding Criteria for Resectability of Colorectal Liver Metastases. The Oncologist 2008;13(1):51–64.
52. Carpizo DR, Are C, Jarnagin W, et al. Liver Resection for Metastatic Colorectal Cancer in Patients with Concurrent Extrahepatic Disease: Results in 127 Patients Treated at a Single Center. Ann Surg Oncol 2009;16(8):2138–46.
53. Rampone B. Current role of hyperthermic intraperitoneal chemotherapy in the treatment of peritoneal carcinomatosis from colorectal cancer. WJG 2010;16(11):1299.
54. Confuorto G, Giuliano ME, Grimaldi A, Viviano C. Peritoneal carcinomatosis from colorectal cancer: HIPEC? Surgical Oncology 2007;16:149–52.
55. Roviello F, Caruso S, Marrelli D, et al. Treatment of peritoneal carcinomatosis with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: State of the art and future developments. Surgical Oncology 2011;20(1):e38–e54.
56. de Haas RJ, Wicherts DA, Adam RE. Resection of Colorectal Liver Metastases with Extrahepatic Disease. Dig Surg 2008;25(6):461–6.
57. Izzo F, Piccirillo M, Palaia R, Albino V, Di Giacomo R, Mastro AA. Management of colorectal liver metastases in patients with peritoneal carcinomatosis. J Surg Oncol 2009;100(4):345–7.
58. Klaver YLB, Lemmens VEPP, Creemers GJ, Rutten HJT, Nienhuijs SW, de Hingh IHJT. Population-based survival of patients with peritoneal carcinomatosis from colorectal origin in the era of increasing use of palliative chemotherapy. Annals of Oncology 2011;22(10):2250–6.
59. Kopetz S, Chang GJ, Overman MJ, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. Journal of Clinical Oncology 2009;27(22):3677–83.
60. Hong YS, Kim TW. [Chemotherapy for colorectal cancer]. Korean J Gastroenterol 2009;54(6):355–63.
61. Glockzin G, Renner P, Popp FC, et al. Hepatobiliary procedures in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol 2011;18(4):1052–9.
62. Thaler K, Kanneganti S, Khajanchee Y, Wilson C, Swanstrom L, Hansen PD. The evolving role of staging laparoscopy in the treatment of colorectal hepatic metastasis. Arch Surg 2005;140(8):727–34.

Chapter 3Morbidity associated with colostomy reversal
after cytoreductive surgery and HIPEC
E.M.V. de Cuba
V.J. Verwaal
I.H.J.T. de Hingh
L.J.J. van Mens
S.W. Nienhuijs
A.G.J. Aalbers
H.J. Bonjer
E.A. te Velde
Ann Surg Oncol. 2014 Mar;21(3):883-90

Chapter 3 | Colostomy reversal after CRS & HIPEC
44
Abstract
Background: CytoReductive Surgery (CRS) and Hyperthermic IntraPEritoneal Chemotherapy (HIPEC) has improved the survival in selected colorectal cancer patients with Peritoneal Metastases (PM). In these patients, the risk of a low-anastomosis is sometimes diminished through the creation of a colostomy. Currently, the morbidity and mortality associated with the reversal of the colostomy in this population is unknown.
Methods: Our study involved two prospectively collected databases including all patients who underwent CRS and HIPEC. We identified all consecutive patients who had a colostomy and requested a reversal. The associations between four clinical and ten treatment-related factors with the outcome of the reversal procedure were determined by univariate analysis.
Results: Twenty-one patients out of 336 patients (6.3%) with a stoma with a mean age of 50.8 years (SD 10.2) underwent a reversal procedure. One patient was classified as ASA grade III, six as ASA grade II and the remaining as ASA grade I. Median time elapsed between HIPEC and reversal was 394 days (range 133-1194). No life-threatening complications or mortality were observed after reversal. The reversal related morbidity was 67%. Infectious complications were observed in seven patients (33%). Infectious complications after HIPEC were negatively correlated with the ultimate restoration of bowel continuity (P=0.05). The bowel-continuity was successfully restored in 71% of the patients.
Conclusions: Although the restoration of bowel continuity after CRS and HIPEC was successful in most patients, a relatively high complication rate was observed. Particularly patients with infectious complications after HIPEC have a diminished chance of successful restoration of bowel continuity.

Colostomy reversal after CRS & HIPEC | Chapter 3
45
3
Introduction
Colorectal carcinoma (CRC) is the third most common cancer worldwide, accounting for approximately one million newly diagnosed patients per year and over 600.000 deaths due to this disease. 1 Roughly 10-25% of CRC patients develop peritoneal metastases (PM), of which 25% present with the peritoneum as the sole sight of distant metastases. 2-4 The peritoneum is a thin membrane, which covers the abdominal wall and internal organs. 5 Peritoneal metastases are believed to be the result of tumor cell shedding into the peritoneal cavity, either spontaneously or as e result of spill during surgical procedures, ultimately resulting in the development of tumor deposits on the peritoneal surface. 6,7 In the past, peritoneal metastases have been solely regarded as a condition only amenable to treatment with a palliative intent, due to the belief that the condition inevitably leads to a rapid demise of the patient. However, isolated peritoneal metastases are regarded as a form of localized disease spread and thus amenable to local control, i.e. surgery known as CytoReductive Surgery (CRS), combined with Hyperthermic IntraPEritoneal Chemotherapy (HIPEC). 8-11
During the CRS, often multiple resections are carried out to remove all intra-abdominal tumor, amongst which are resections of the intestines. CRS and HIPEC is known as a procedure with a relatively high major morbidity (grade III/IV) rate ranging from 12% to 52%. 12 A large portion of tumor bulk is situated in Douglas’ pouch, following the natural intra-peritoneal flow. 13 Consequently the rectum is transected below this point, resulting in a low or ultra-low anastomosis if the surgeon would opt for immediate reconstruction of the bowel continuity.These ultra-low anastomoses are known to carry a high risk of complications such as leakage. 14,15 To avoid ultra-low anastomoses, and thus lower the risk of additional complications in an already highly morbid procedure, colostomies are created. 15,16
Several studies have reported a reduced quality of life (QoL) in patients living with a colostomy. 17,18 This results in a proportion of patients requesting a reversal procedure to restore the bowel continuity as soon as medically prudent. 17 Nevertheless, several studies have reported that colostomy reversal is accompanied by significant morbidity and mortality, describing rates of anastomotic leakage of up to 25% and mortality of up to 14%.17,19
The morbidity and mortality accompanying such a reversal procedure in a population that has previously undergone extensive surgery in the form of CRS and HIPEC is currently unknown. Our aim is to investigate all consecutive colostomy reversal procedures in a prospective cohort of CRS and HIPEC patients.

Chapter 3 | Colostomy reversal after CRS & HIPEC
46
Patients and Methods
Patient selection and data collection
We studied two prospectively collected databases evaluating all patients who underwent CRS and HIPEC in two Dutch Institutes (National Cancer Institute - Antoni van Leeuwenhoek Hospital and the Catharina Hospital in Eindhoven) between January 2000 and December 2009. We subsequently identified all patients who received a stoma as part of the CRS and HIPEC procedure with an active wish to reverse the procedure. All consecutive patients that received a colostomy with a follow-up of more than 6 months after the reversal procedure were included for further analysis. We excluded patients with an ileostomy and reversal of the colostomy due to dysfunction of the colostomy.Patients were followed up according to the standard of care at both institutions, which is in accordance with the Dutch HIPEC protocol. 15,20 Patient characteristics gathered included: age, gender, medical history, co-morbidity, ASA-grade and tumor-type. Treatment related factors assessed included: HIPEC procedure details, hospital stay, time between HIPEC procedure and colostomy reversal, reversal procedure details, mortality, hospital stay after reversal procedure, number of invasive procedures for the reversal procedure and whether or not the reversal procedure was ultimately successful. The post-operative complications were graded in grades, ranging from Grade I to Grade V. 21 (Supplementary Data)
Surgical procedure
The CRS and HIPEC procedure was carried out in a uniform fashion by the surgical teams of both institutes according to a previously published protocol. 15 The objective of CRS is to remove all macroscopically visible tumor in the abdominal cavity with only limited disease remaining (<2.5mm). The parietal peritoneum is routinely stripped and the omentum surgically removed according the technique pioneered by Sugarbaker et al. 10 All affected viscera are surgically removed. Bowel continuity is restored after the intra-abdominal lavage with the cytostatic compound, to prevent the post-operative entrapment of tumor cells that may cause local recurrence in the future. In most patients in whom Douglas pouch was affected and rectal resections were therefore unavoidable, a colostomy was created in order to avoid ultra-low anastomosis (Hartmann’s Procedure). 15
The HIPEC procedure was performed according to the coliseum technique (open) in all cases in both institutes. The duration of the HIPEC procedure was 90 minutes at a temperature constantly between 39 to 41 degrees Celsius. Mitomycin C (MMC) was the cytostatic drug of choice in all cases.

Colostomy reversal after CRS & HIPEC | Chapter 3
47
3
Data analysis
Data analysis was performed utilizing the statistical package for the socials sciences (SPSS Inc., Chicago IL) version 20 for OsX. Descriptive statistics were used to describe clinical and treatment related factors in the cohort.Clinical and treatment related factors were analyzed for an association with: (1) the occurrence of complications after the reversal procedure, (2) whether or not the bowel continuity was successfully restored. Differences were computed using the unpaired t-test for numerical data that is normally distributed, the Mann-Whitney U test for numerical data that is not normally distributed or the Chi-square test for unpaired ordinal and categorical data. A p-value ≤0.05 was considered statistically significant.
Results
From January 2000 to December 2009, 747 consecutive patients underwent treatment with CRS and HIPEC. Of these patients we identified 32 patients (9.5%) who underwent a reversal procedure after the recovery period. We excluded six patients based on the presence of an ileostomy after CRS and HIPEC, three patients were excluded because the reversal was unavoidable due to dysfunction or leakage of the colostomy and two patients were excluded from the analysis due to a clinical follow-up after the reversal procedure of less than six months.
Patient Characteristics
All patient characteristics are listed in Table 1. This cohort consisted of 21 patients, seven males (33%) and 14 females (66%). The mean age was 50.8 years with a standard deviation of 10.2 years. Prior to the CRS and HIPEC a median of two abdominal procedures were performed per patient (range 1-4). On average four resections were performed during the CRS and HIPEC procedure. Resections included: peritonectomies, surgical removal of organs and viscera affected by disease spread (ovariae, uterus, sections of small and large intestine, spleen and stomach) and in six out of 21 (28.6%) the synchronous removal of the primary tumor. In 17 out of 21 eligible patients (81%) a macroscopically complete cytoreduction was achieved. In the remaining four cases a complete cytoreduction was not technically feasible and a minimum of residual disease was left in situ (<2.5mm = R2a). All these patients presented with PMP (Table 2).

Chapter 3 | Colostomy reversal after CRS & HIPEC
48
Outcome Reversal
The median time elapsed between colostomy reversal and the initial CRS and HIPEC procedure was 394 days (range 133-1194 days). In seven patients the reversal procedure was carried out within one year of follow-up after CRS and HIPEC. The rate of documented co-morbidities remained unchanged (Table 1). The median hospital stay after reversal was eight days (range 4-36).Complications post-reversal procedure occurred in 14 out of 21 patients (67%). Grade II complications were observed in four patients and Grade III complications in 10 patients. No Grade IV complications or mortality was observed after the reversal procedure. The median number of invasive procedures necessary to alleviate the colostomy reversal associated complications was one (range 1-5). Median follow up after the reversal procedure was 34 months (range 8-119).Three out of 21 patients ended up with an ileostomy (14%). This was due to complications sustained after reversal, as shown in table 1. In one patient multiple laparotomies were performed to resolve fistulas, which resulted in an ileostomy. Another patient had an anastomotic stenosis post-reversal and the last patient presented with an acute ileus due to intra-abdominal adhesions. In an additional three patients the colostomy was not reversed due to tumor recurrence determined during the reversal procedure. Of these patients, two had a macroscopic incomplete resection during CRS and HIPEC for PMP (R2a). Ultimately, the bowel continuity was successfully restored in 71% of the patients that underwent the procedure. Additionally, one patient who received an ileostomy after the reversal subsequently underwent a successful reversal procedure of the ileostomy. Ultimately the bowel continuity was successfully restored in 76% of all patients.
Univariate Analysis of Risk Factors
No significant correlation was observed between four clinical factors and 10 treatment related factors and (1) the occurrence of complications after the reversal procedure, (2) the placement of an ileostomy after the reversal and finally (3) whether or not the bowel continuity was successfully restored (P>0.05), as listed in Table 3. Assessment of the four clinical and 10 treatment-related factors in relation to (1) the occurrence of complications after the reversal procedure, (2) the placement of an ileostomy after the reversal and finally (3) whether or not the bowel continuity was successfully restored showed that an infectious complication (including abscess formation) post CRS andHIPEC and the presence of a fistula led to more ileostomy placements in completely resected patients (R1) (P=0.05) and was also negatively correlated with the ultimate restoration of bowel continuity (P=0.05). High complication grade, the presence of an infectious complication and the need for invasive procedures following the reversal

Colostomy reversal after CRS & HIPEC | Chapter 3
49
3
procedure were all negatively correlated with the successful restoration of bowel continuity in completely resected patients (P=0.05, P=0.003 and P=0.05 respectively).
200-2009In total 747 patients CRS &
HIPEC
336 (45%) colostomy
411 (55%) no colostomy
32 reversal (9.5%) 304 no reversal (90.5%)
21 patients (6.3%) eligible for in-
depth analysis of clinical parameters
Exclusion:- 6 ileostomy
- 3 dysfunction of colostomy
- 2 <6 months clinical follow-up
3 patients receive ileostomy
3 patients not restored recurrence
15 patients successful
restoration bowel continuity
2 patients keep ileostomy
1 patient succesful restoration of
bowel continuity
Figure 1: Flow-chart depicting patient flow after CRS and HIPEC

Chapter 3 | Colostomy reversal after CRS & HIPEC
50
Tabl
e 1:
Det
aile
d cl
inic
al o
verv
iew
of 2
1 pa
tient
s req
uest
ing
and
unde
rgoi
ng c
olos
tom
y re
vers
al
Pt #
Gen
der
Age
Com
orbi
dity
ASA
Cla
ssifi
catio
nTu
mor
Typ
eA
dj.
Che
mo
Proc
. pr
ior
to
HIP
EC
Mnt
hs
betw
een
HIP
EC
an
d R
ev.
Com
plic
atio
n H
IPE
C (g
rade
)
Num
ber
of In
vasi
ve
Inte
rven
tions
to
Tre
at
Com
plic
atio
n H
IPE
C
Com
plic
atio
n R
ever
sal
Proc
edur
e (g
rade
)
Num
ber
of In
vasi
ve
Inte
rven
tions
to
Tre
at
Com
plic
atio
n R
ever
sal
Res
ult
Rev
ersa
l
1**
F58
-I
PMP
-2
9A
nem
ia (I
I)+
2M
58-
IPM
P-
231
Pneu
mot
hora
x (I
II)
Fist
ula
(III
)1
+
3F
54-
IPM
P-
313
Inva
sion
in U
rete
r à
rese
ctio
n &
pla
cem
ent
JJ st
ent (
III)
Iatro
geni
c (I
II)
1+
4F
48D
MII
, Hep
A+B
, H
yper
chol
este
rola
emia
III
PMP
-2
19A
nast
omot
ic le
akag
e (I
II)
3In
fect
ious
&
Inci
sion
al
Her
niat
ion
(III
)
1+
5**
F39
-I
PMP
-2
7Fi
stul
a &
Iatro
geni
c (I
II)
2Fi
stul
a (I
II)
5Ile
osto
my
6M
46-
IA
deno
carc
inom
a-
115
+
7M
37-
IA
deno
carc
inom
a+
114
Iatro
geni
c &
Fi
stul
a (I
II)
2+
8F
62H
yper
tens
ion
IIA
deno
carc
inom
a-
312
Infe
ctio
us (I
I)A
cute
ileu
s du
e to
ad
hesi
ons (
III)
1Ile
osto
my
9F
44M
S, A
nem
ia, D
ES
Dau
ghte
rII
PMP
+3
12A
bsce
ss fo
rmat
ion
(III
)1
Ileus
(II)
+
10M
31-
IPM
P-
213
Pulm
onar
y Em
bolis
m
(II)
No
reve
rsal
du
e to
re
curr
ence
11F
50C
U, H
yper
tens
ion
IIA
deno
carc
inom
a+
112
Ane
mia
(II)
+
12M
55-
IPM
P-
238
Acu
te il
eus c
ause
d by
ad
hesi
ons (
III)
2A
nast
omot
ic
sten
osis
à
Shor
t Bow
el
(III
)
+
13**
F43
-I
Ade
noca
rcin
oma
+1
9+

Colostomy reversal after CRS & HIPEC | Chapter 3
51
3
Tabl
e 1:
Det
aile
d cl
inic
al o
verv
iew
of 2
1 pa
tient
s req
uest
ing
and
unde
rgoi
ng c
olos
tom
y re
vers
al (C
ontin
ued)
Pt #
Gen
der
Age
Com
orbi
dity
ASA
Cla
ssifi
catio
nTu
mor
Typ
eA
dj.
Che
mo
Proc
. pr
ior
to
HIP
EC
Mnt
hs
betw
een
HIP
EC
an
d R
ev.
Com
plic
atio
n H
IPE
C (g
rade
)
Num
ber
of In
vasi
ve
Inte
rven
tions
to
Tre
at
Com
plic
atio
n H
IPE
C
Com
plic
atio
n R
ever
sal
Proc
edur
e (g
rade
)
Num
ber
of In
vasi
ve
Inte
rven
tions
to
Tre
at
Com
plic
atio
n R
ever
sal
Res
ult
Rev
ersa
l
14F
40H
ypot
hyro
idis
mI
PMP
-1
15A
nem
ia (I
I)In
fect
ious
(II)
+
15F
62-
IPM
P-
216
Infe
ctio
us (I
II)
1N
o re
vers
al
due
to
recu
rren
ce16
**F
38-
IA
deno
carc
inom
a+
34
+
17F
60M
I, Ep
ileps
yII
Ade
noca
rcin
oma
-1
15+
18F
54-
IA
deno
carc
inom
a-
113
Ana
stom
otic
St
enos
is (I
II)
1Ile
osto
my
19**
M66
Dep
ress
ion,
H
yper
tens
ion,
H
yper
chol
este
rola
emia
, H
ypot
hyro
idis
m
IIPM
P-
16
Abs
cess
(III
)1
No
reve
rsal
du
e to
re
curr
ence
20**
M65
Ost
eopo
rosi
sII
Ade
noca
rcin
oma
-4
4A
cute
ileu
s due
to
adhe
sion
s (II
I)
1In
cisi
onal
H
erni
atio
n (I
II)
1+
21**
F57
-I
Ade
noca
rcin
oma
-U
nkno
wn
8A
bsce
ss
& A
cute
ile
us d
ue to
ad
hesi
ons (
III)
1+

Chapter 3 | Colostomy reversal after CRS & HIPEC
52
Supplementary Table 1: Classification of surgical complications according to Dindo et al.
Complication Grade Definition
Grade I Any deviation from the normal postoperative course without the need for pharmacological treatment or invasive procedures, such as surgical, endoscopic or radiological interventions. Drugs as anti-emetics, antipyretics, analgesics, diuretics and administration of electrolytes are allowed. Also physiotherapy and wound infections opened at the bedside also are included in this grade
Grade II Requiring pharmacological treatment with drugs other than those allowed for grade I complications. This includes blood transfusions and total parenteral nutrition
Grade III Requiring surgical, endoscopic or radiological interventionGrade IVGrade V
Life-threatening complication requiring Intensive Care management. This includes central nervous system complications. Death of the patient
No Complications (33%)
Grade II Complications (14%)
Grade III Complications (53%)N=11
N=7
N=3
Figure 2: Distribution of complications and complication grade after reversal
Table 2: Detailed overview of clinical course in four patients after R2a resection
Pt. #Resection Outcome HIPEC
Gender Age Tumor TypeMnths between HIPEC and Rev.
Results Reversal Reason
3 R2a F 54 PMP 13 +
4 R2a F 48 PMP 19 +
10 R2a M 31 PMP 13 - Recurrence
15 R2a F 62 PMP 16 - Recurrence
F= female, M=male, PMP=Pseudomyxoma Peritoneii, +=successful restoration, -=failure of restoration

Colostomy reversal after CRS & HIPEC | Chapter 3
53
3
Table 3: Univariate analysis of risk factors in optimally resected patients (n=17)
Variable Comp.Rev-
Comp. Rev+ P-Value Ileostomy- Ileostomy+ P-Value Cont.
Rest.-Cont.Rest.+ P-Value
Clinical Age (mean) 49 yrs 52 yrs NS 51 yrs 52 yrs NS 53 yrs 51 yrs NSGender Male (N=) Female (N=)
14
57 NS
68
03 NS
13
58 NS
ASA Classification I (N=) II (N=)
41
75 NS
95
21 NS
22
94 NS
Tumor Type PMP (N=) Adenocarcinoma (N=)
14
66 NS
68
12 NS
22
58 NS
Treatment RelatedAdjuvant Chemotherapy No (N=) Yes (N=)
32
93 NS
95
30 NS
40
85 NS
Complicated HIPEC No (N=) Yes (N=)
32
57 NS
77
12 NS
22
67 NS
Inf. Comp. HIPEC No (N=) Yes (N=)
50
84 NS
122
12 P=0.05
12
122 P=0.05
Complication Grade (HIPEC) Not applicable (N=) II (N=) III (N=)
310
525 NS
724
111 NS
211
624 NS
Time Elapsed between CRS & HIPEC and reversal < 1 year (N=) ≥ 1 year (N=)
32
48 NS
68
12 NS
22
85 NS
Complicated Reversal No (N=) Yes (N=) NA NA -
59
03 NS
05
48 NS
Inf. Comp. Reversal No (N=) Yes (N=) NA NA -
113
12 NS
03
122 P=0.003
Complication Grade (reversal) Not applicable (N=) II (N=) III (N=) NA NA -
536
003 NS
003
536 NS
Invasive procedures needed to resolve complications reversal Not applicable (N=) No (N=) Yes (N=) NA NA -
536
003 NS
003
53
6 NS
Comp.Rev-= Patients with no complications after reversal procedure, Comp. Rev+= Patients with complications after reversal procedure, Ileostomy-=Patients who did not need an ileostomy after reversal procedure, Ileostomy+= Patients who needed an ileostomy after reversal procedure, Cont.Rest.-= Patients in who the reversal procedure was unsuccessful, Cont.Rest.+= Patients in who the reversal procedure was successfulNA= Not applicable NS=Not significant, P>0.05

Chapter 3 | Colostomy reversal after CRS & HIPEC
54
Discussion
An increase in median overall survival has been reported since the introduction of CRS and HIPEC, reporting a median overall survival in some series of up to 62 months. 6,22 This might cause an increase in requests for stoma reversal procedures with the goal to improve the QoL experienced by the longer surviving HIPEC patient. 17,18 Patients with a colostomy have been reported to encounter difficulties both of a physical and psychological nature. 18
Currently, very little is known about the incidence of colostomy reversal requests in CRS and HIPEC patients and the possible associated complications. Available data on stoma reversal procedures are based on studies in heterogeneous patient populations with several underlying pathologies (oncologic and benign), making implementation into clinical practice in CRS and HIPEC patients challenging. 17
For this procedure in particular, the major aspect is the patient`s wish concerning his or her QoL. 17 As a result we included the patients that actively requested the procedure because they deemed their QoL to be lower due to the colostomy. The majority of the patients will not undergo a reversal procedure after initial CRS and HIPEC treatment, because it is believed that the expected gain in QoL does not outweigh the associated risks. CRS and HIPEC is associated with high post-operative morbidity, resulting in technically challenging surgeries due to the large amount of adhesions. Patients are not encouraged to undergo a reversal procedure, because that would entail one or more subsequent, highly morbid procedures in a relatively short amount of time. Secondly, even though treatment is with curative intent, inevitably the disease will recur in some. This renders these cases not amenable for reversal. 23 Lastly, a proportion of patients will not request a reversal due to the fact that they do not experience diminished QoL with the colostomy or they are still recovering the QoL deficit caused by treatment. 18,24
However, if actively requested 71% of the patients will undergo successful restoration of bowel continuity. Infectious complications, including the formation of fistula, were detrimental for the outcome of the reversal. These patients received significantly more ileostomies and had ultimately less successful bowel continuity restorations (P=0.05).We observed that in three patients adequate staging was not possible prior to undertaking the reversal procedure, translating into failure of the planned reversal procedure due to the intra-operative discovery of recurrent disease. This is a known clinical difficulty in the CRS and HIPEC population. This finding underlines the importance of improvement of clinical tools used for the follow-up of CRS and HIPEC, which is currently done with sub-optimal imaging and biomarkers. 25 The translational study conducted by van Dam and colleagues illustrates the potential added value of novel techniques such as fluorescent tumor-specific antibodies in intra-operative (laparoscopic) imaging in CRS and HIPEC patients. 26 Despite

Colostomy reversal after CRS & HIPEC | Chapter 3
55
3
the considerable effort necessary for further development, we believe that these tools will certainly aid in further advancing overall care in the CRS and HIPEC population. 25
All patients were treated and followed up in accordance with the Dutch HIPEC protocol. 15,20 In this cohort, patients who underwent a macroscopically incomplete (R2a) resection had a significantly higher chance of not undergoing a reversal procedure due to recurrence of disease. It is known from literature that the resection outcome after CRS and HIPEC is one of the most important treatment related prognostic factors. 8,15
We found a relatively high incidence of complications (67%) in comparison to literature. 27 Our cohort consisted of patients that have an extensive oncologic and surgical history, which could partially explain the complication rate seen. 14,27,28 The number of previous procedures was high (median two, range 1-4). This HIPEC cohort appeared to have more favorable clinical characteristics, such as lower ASA classification and a younger age in comparison to previously published cohorts in which colostomy reversal outcomes were reported in both malignant and benign disease. 14,27 In one of the previously published cohorts 37% of the patients were classified as ASAIII/IV, as opposed to our cohort, which only included 1 patient (5%) who was classified as ASAIII. In the oncologic cohort 67% of the patients was above 60 years of age in contrast to 25% in our cohort. 14 The median age in the benign disease cohort was 63 years, as opposed to 54 in our post CRS and HIPEC cohort. 17
The nature of complications observed here is comparable to that seen in a previously published cohort. 27 Likewise, they often require additional invasive procedures, thus lengthening the duration of hospitalization. As was also observed in our cohort, infectious complications have been previously described as a possible limiting factor for stoma reversal. 14
The peritoneum is known to play an essential role in the containment of intra-abdominal infectious complications and wound healing. 5 It is currently unknown how the entire CRS and HIPEC treatment affects the integrity of the tissue, which is used for the continuity restoration. Moreover, to the best of our knowledge, there are currently no publications that investigated this particular clinical question in the HIPEC populations treated with other techniques (open vs. closed) or different HIPEC compounds, such as Oxaliplatin. The effect of stripping of the affected peritoneum on the containment of intra-abdominal infectious complications and wound healing in this cohort of patients has not been studied to date. Theoretically, the natural intra-abdominal defense could be compromised due to the removal of potentially large parts of peritoneum during CRS, the physiologic effect of the additional intra-abdominal trauma and subsequent release of inflammatory cytokines. 5

Chapter 3 | Colostomy reversal after CRS & HIPEC
56
Furthermore, the effect of the intra-abdominal lavage with a chemotherapeutic agent such as MMC on wound healing after treatment is still largely unknown.
In conclusion, we found a relatively high complication rate following the Hartmann’s reversal procedure. Ultimately, the bowel restoration success rate is 71%, considering that patients with infectious complications after HIPEC have a diminished chance of successful restoration of bowel continuity.
The results of our study are informative for surgeons facing the requests of the highly selected and successfully treated CRS and HIPEC patients to reverse the colostomy. The decision to have the procedure reversed is first and foremost based on the wish of the patient, provided that the patient is in an acceptable condition and tumor-free prior to undergoing surgery.

Colostomy reversal after CRS & HIPEC | Chapter 3
57
3
References1. Parkin DM, Bray F, Ferlay J, Pisani P. Global
cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108.
2. Koppe MJ, Boerman OC, Oyen WJG, Bleichrodt RP. Peritoneal Carcinomatosis of Colorectal Origin. Annals of Surgery. 2006;243(2):212–222. doi:10.1097/01.sla.0000197702.46394.16.
3. Jayne. Jayne 2002 Br J Surg Peritoneal carcinomatosis. Br J Surg. 2002:1–6.
4. Sugarbaker PH. Patient selection and treatment of peritoneal carcinomatosis from colorectal and appendiceal cancer. World J Surg. 1995;19(2):235–240.
5. van der Wal JBC, Jeekel J. Biology of the peritoneum in normal homeostasis and after surgical trauma. Colorectal Dis. 2007;9 Suppl 2:9–13. doi:10.1111/j.1463-1318.2007.01345.x.
6. de Cuba EMV, Kwakman R, Knol DL, Bonjer HJ, Meijer GA, Velde te EA. Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases: Systematic review of all literature and meta-analysis of observational studies. Cancer Treatment Reviews. 2012:1–7. doi:10.1016/j.ctrv.2012.11.003.
7. Ceelen WP, Bracke ME. Peritoneal minimal residual disease in colorectal cancer: mechanisms, prevention, and treatment. Lancet Oncology. 2009;10(1):72–79. doi:10.1016/S1470-2045(08)70335-8.
8. Elias D, Lefevre JH, Chevalier J, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of Clinical Oncology. 2009;27(5):681–685. doi:10.1200/JCO.2008.19.7160.
9. Carpizo DR, D’Angelica M. Liver resection for metastatic colorectal cancer in the presence of extrahepatic disease. Lancet Oncology. 2009;10(8):801–809. doi:10.1016/S1470-2045(09)70081-6.
10. Sugarbaker PH. Peritonectomy procedures. Annals of Surgery. 1995;221(1):29–42.
11. Sugarbaker PH. Management of peritoneal-surface malignancy: the surgeon’s role. Langenbecks Arch Surg. 1999;384(6):576–587.
12. Chua TC, Yan TD, Saxena A, Morris DL. Should the treatment of peritoneal carcinomatosis by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy still be regarded as a highly morbid procedure?: a systematic review of morbidity and mortality. Annals of Surgery. 2009;249(6):900–907. doi:10.1097/SLA.0b013e3181a45d86.
13. van den Tol PM, van Rossen EE, van Eijck CH, Bonthuis F, Marquet RL, Jeekel H. Reduction of peritoneal trauma by using nonsurgical gauze leads to less implantation metastasis of spilled tumor cells. Annals of Surgery. 1998;227(2):242–248.
14. Dulk den M, Smit M, Peeters KCMJ, et al. A multivariate analysis of limiting factors for stoma reversal in patients with rectal cancer entered into the total mesorectal excision (TME) trial: a retrospective study. Lancet Oncology. 2007;8(4):297–303. doi:10.1016/S1470-2045(07)70047-5.
15. Verwaal VJ. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. Journal of Clinical Oncology. 2003;21(20):3737–3743. doi:10.1200/JCO.2003.04.187.
16. Matthiessen P, Hallböök O, Rutegård J, Simert G, Sjödahl R. Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial. Annals of Surgery. 2007;246(2):207–214. doi:10.1097/SLA.0b013e3180603024.
17. Vermeulen J, Gosselink MP, Busschbach JJV, Lange JF. Avoiding or reversing Hartmann’s procedure provides improved quality of life after perforated diverticulitis. J Gastrointest Surg. 2010;14(4):651–657. doi:10.1007/s11605-010-1155-5.
18. Nugent KP, Daniels P, Stewart B, Patankar R, Johnson CD. Quality of life in stoma patients. Diseases of the Colon and Rectum. 1999;42(12):1569–1574.
19. Banerjee A, Shorthouse A. Towards even fewer colostomies.... Lancet. 1995;346(8979):859.
20. Kuijpers AMJ, Mirck B, Aalbers AGJ, et al. Cytoreduction and HIPEC in The Netherlands: Nationwide Long-term Outcome Following the Dutch Protocol. Ann Surg Oncol. 2013. doi:10.1245/s10434-013-3145-9.
21. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Annals of Surgery. 2004;240(2):205–213.
22. Chua TC, Morris DL, Esquivel J. Impact of the peritoneal surface disease severity score on survival in patients with colorectal cancer peritoneal carcinomatosis undergoing complete cytoreduction and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2010;17(5):1330–1336. doi:10.1245/s10434-009-0866-x.

Chapter 3 | Colostomy reversal after CRS & HIPEC
58
23. Verwaal VJ, Zoetmulder FAN. Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. European Journal of Surgical Oncology (EJSO). 2004;30(3):280–285. doi:10.1016/j.ejso.2003.12.003.
24. Duckworth KE, McQuellon RP, Russell GB, et al. Patient rated outcomes and survivorship following cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy (CS + HIPEC). J Surg Oncol. 2012;106(4):376–380. doi:10.1002/jso.23089.
25. de Cuba EMV, Kwakman R, van Egmond M, et al. Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : Future possibilities for personalised treatment by use of biomarkers. Virchows Archiv. 2012:1–31. doi:10.1007/s00428-012-1287-y.
26. van Dam GM, Themelis G, Crane LMA, et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-α targeting: first in-human results. Nature Medicine. 2011:1–6. doi:10.1038/nm.2472.
27. Vermeulen J, Coene PPLO, Van Hout NM, et al. Restoration of bowel continuity after surgery for acute perforated diverticulitis: should Hartmann’s procedure be considered a one-stage procedure? Colorectal Dis. 2009;11(6):619–624. doi:10.1111/j.1463-1318.2008.01667.x.
28. Gooszen AW, Gooszen HG, Veerman W, et al. Operative treatment of acute complications of diverticular disease: primary or secondary anastomosis after sigmoid resection. Eur J Surg. 2001;167(1):35–39. doi:10.1080/110241501750069792.

Chapter 4Understanding molecular mechanisms in
peritoneal dissemination of colorectal cancer;Future possibilities for personalised
treatment by use of biomarkers
E.M.V. de Cuba
R. Kwakman
M. van Egmond
L.J.W. Bosch
H.J. Bonjer
G.A. Meijer
E.A. te Velde
Virchows Arch. 2012 Sep;461(3):231-43

Chapter 4 | Molecular mechanisms in PM of CRC
60
Abstract
Objective: When colorectal cancer (CRC) metastasizes, this is mostly to the liver via the portal circulation. In addition, 10-25% of CRC patients eventually show metastases in the peritoneum. A selection of these patients is treated with Cytoreductive Surgery (CRS) and Hyperthermic Intra-Peritoneal Chemotherapy (HIPEC). However, several clinical needs still exist in which biomarkers could play an important role. Relatively little is known about the biology of peritoneal spread of CRC. The development of peritoneal metastases (PM) involves several steps, including: detachment of malignant cells; anoikis evasion; attachment to and invasion of the peritoneal surface ultimately ending in a colonization phase in which the malignant cells thrive in the newly formed niche. In this paper we provide an overview of molecules associated with peritoneal dissemination and explore the clinical possibilities of these candidate biomarkers.
Methods: A literature search was conducted using the PubMed database of the U.S. National Library of Medicine and Medline to identify studies on the biological behaviour of peritoneal metastases (PM) of CRC.
Results: In a series of over 100 studies on PM published between 1990 and 2010, IGF-1, HIF1α, VEGF, EGFR and ITGB1 emerge as most interesting candidates for possible clinical application.
Conclusions: Even though these promising candidate biomarkers have been identified, all of these require extensive further validation prior to clinical application. Yet, the pace of the omics revolution makes that the question is not if, but when biomarkers will be introduced to improve diagnosis and ultimately outcome of patients with PM due to CRC.

Molecular mechanisms in PM of CRC | Chapter 4
61
4
Introduction
Colorectal carcinoma (CRC) is a major health problem, being the third most common cancer worldwide. Each year more than one million people develop CRC and over 600.000 patients die of this cancer, despite improvements in diagnostic and treatment modalities. 1 Approximately half of CRC patients develop metastases, mainly to the liver via the portal vein system. 2,3 Another category of distant metastases from CRC are those to the peritoneum, i.e. peritoneal metastases (PM). In up to 25% of patients with metastatic CRC, the peritoneum is the sole site of metastasis. 3,4 Untreated PM is associated with poor survival of about 6-12 months, while systemic chemotherapy alone does not appear to yield any clinically significant survival benefit. 5,6
In the early 1990’s, a treatment with a curative intent for patients with PM of CRC, without evidence of distant metastasis to other sites, was introduced. This consists of debulking surgery (cytoreductive surgery, CRS) combined with heated intraperitoneal chemotherapy (HIPEC). 7,8 This approach is based on the hypothesis that peritoneal dissemination is a form of local rather than systemic spread, which in theory makes PM amenable to a form of local disease control, i.e. surgery. 9 This theory is further supported by the observation that a subgroup of patients, in whom no residual macroscopic tumour is left post-resection, shows a five-year survival of 35-45%. 10 This is equal to the survival of patients undergoing resection for liver metastasis, which to date is part of the standard of care for liver metastases of colorectal origin (CRLM). 3,10,11
Thus, patients with resectable metastatic colorectal cancer, either to the liver or the peritoneum, have benefitted from the aggressive surgical management. However, because treatment with CRS and HIPEC has a morbidity and mortality rate of 15-18% and 5%, respectively, it is of utmost importance to be able to carefully select those patients who will benefit most from this treatment. 4,5,10,12 In addition, major challenges in diagnosing and treating PM remain. For example, most early peritoneal lesions are smaller than 1 cm, and as such not visible on pre-operative CT- or PET-scans, which hampers both timely diagnosis and adequate monitoring of patients with PM. 12 Furthermore, the chemotherapy that is used in HIPEC is still based on the ‘one size fits all’ principle, without any biological stratification.Presently, the selection of patients is made roughly on clinical parameters and intra-operative findings. Based on the hypothesis that the phenotype, and thus clinical behaviour, of PM in CRC is driven by underlying biological mechanisms, read outs of disease biology, i.e. biomarkers, will be of help for more refined identification of suitable patients. Additionally, adequate targets may be of great value in prognosis assessment, imaging and guidance of therapy.

Chapter 4 | Molecular mechanisms in PM of CRC
62
The aim of the present paper is therefore to provide an overview of promising molecular changes reported to be involved in peritoneal dissemination of CRC and to evaluate the potential for clinical application of these biomarkers.
Materials and methods
A literature search was conducted using the PubMed database of the U.S. National Library of Medicine and Medline using the following keywords: peritoneal metastasis, CRC, biological behaviour, detachment, motility, anoikis, attachment, invasion, angiogenesis, proliferation, epithelial to mesenchymal transition, immunohistochemistry (IHC), proteins, HIPEC and combinations of these keywords. These search terms were used in order to include as many articles as possible on the subject. Additional papers were included by cross-referencing from papers retrieved in the first search. Articles from 1990 up to 2010 on biomarkers in PM of CRC were included for individual review, and only so when fitting the scope of this paper. A second reader conducted additional review when necessary. Studies on ovarian-, gastric-, and carcinoma of the pancreas spread to the peritoneum were included for review as well. Reports on in-vivo, in-vitro as well as ex-vivo experiments were included.
Results
The process of metastasis in general comprises different phases: First, tumour cells detach from the primary tumour, second, they migrate to the distant site and third they adapt to the new microenvironment, i.e. niche, and grow out. 13,14
The niche in question, the peritoneum, is the surface of the abdominal wall. It is made up of a single layer of mesothelial cells on a basement membrane supported by a connective tissue or stroma compartment, also referred to as the submesothelium, which forms the niche for PM. This submesothelium consists of stromal cells and extracellular matrix (ECM), which is composed of laminin, collagen, fibronectin, proteoglycan and elastin. 15
Cellular Mechanisms involved in peritoneal spread
Below, candidate biomarkers are discussed in the order of the sequential steps of the metastatic process. However, as considerable interactions exist between these processes, this classification is by no means absolute.

Molecular mechanisms in PM of CRC | Chapter 4
63
4
1. Detachment and increased motility
Upon detachment from the primary CRC, in addition to anoikis evasion, tumour cells have to enable motility in order to reach the target organ. 16 This is acquired by downregulation of cell-cell adhesion molecules (CAM’s) and changes in the cytoskeleton, such as the extension of lammellipodia and filopodia. 17
Cell-cell adhesion molecules include the integrin family of proteins, cadherins, selectins and members of the immunoglobulin superfamily (e.g. ICAM and VCAM), which are discussed below in section 3. Also, other adhesion molecules, like CDH2, and cell surface molecules with signal transduction function, like EGFR and c-MET play a role here. 18 These phenotypic alterations that take place during invasion, with tumour cells exhibiting reduced adhesion and increased motility, are also referred to as epithelial-mesenchymal transition (EMT). 17,19 In the context of PM, the molecule TWIST is reported to be involved in this process.
Twist homolog 1 (TWIST)
TWIST is a transcription factor that is most abundantly expressed in tissues of mesodermal origin. TWIST is known as an EMT trigger. 13,14 Studies aiming to block the function of TWIST by siRNA in ovarian adenocarcinoma cells have shown suppression of adhesion molecules and matrix metalloproteinases (MMPs). Levels of migration, invasion and adhesion to peritoneal mesothelium were significantly lower in siTWIST cells, supporting that downregulation of TWIST could, in theory, ultimately inhibit peritoneal dissemination. 20
Met proto-oncogene (c-MET)
c-MET is a proto-oncogene that encodes for the hepatocyte growth factor receptor (HGFR). It has tyrosine kinase activity and is essential in embryonic development and wound healing. 21 Activation of MET by hepatocyte growth factor (HGF) initiates an invasive growth program 22, which physiologically occurs during embryonic development and organ regeneration, but that is hijacked by cancer cells to promote invasion. 23 Abnormal MET expression in cancer has been linked to poor survival in several malignancies, including CRC. 24 c-MET was found to play an important role in peritoneal dissemination of ovarian carcinoma (OvCa) cells in culture, most probably through an α5β1 integrin-dependent mechanism. 25 Using tissue microarrays (TMAs), cell lines and animal models, the role of c-MET in PM of OvCa was investigated. The disease specific survival of patients with high c-MET protein expression was significantly lower than those with low expression (N=138). In experiments using ECM components, primary mesothelial cells, full-thickness human peritoneum and in-vivo mouse peritoneum, marked inhibition of dissemination was noted by siRNA targeting c-MET. 25,26 Furthermore, a reduction in α5β1 protein and

Chapter 4 | Molecular mechanisms in PM of CRC
64
mRNA, accompanied by a reduction in MMP2 and MMP9 activity, was noted. 25 As such, theoretically c-MET represents a very attractive candidate biomarker of PM formation risk as well as a possible therapeutic target in prevention of peritoneal dissemination.
Epidermal growth factor receptor (EGFR)
EGFR is a cell surface protein and when its ligand binds, a signalling cascade starts that leads to cell proliferation. 3,10,11,26 Activation of EGFR is thought to promote the downregulation of E-cadherin, causing disruption of adherens junctions, through induction of MMP9. This interaction has been investigated in OvCa by blocking with an siRNA directed against MMP9. 27 This study involved two cell lines and tissue samples from 146 primary OvCas, including 17 paired samples of primary tumour and PM. Treatment with recombinant MMP9 or transient expression of MMP9 was sufficient to regain function and reduce E-cadherin levels in the cell lines, which subsequently caused a migratory and invasive response. These findings were validated by IHC on TMAs containing patient material, which exhibited co-localization of activated EGFR and MMP9 accompanied by E-cadherin loss. 27 Clinically elevated levels of both EGFR and MMP9 have been associated with worse survival. 28-30
Other markers associated with detachment and increased motility in in-vitro and in-vivo studies in the context of PM are HGF, RHOA and CDH2. 24,27,31-34 However, the clinical significance of up or down regulation of these specific genes in PM of CRC remains to be verified.
2. Anoikis evasion
Anoikis is a form of programmed cell death that takes place when cells detach from the surrounding extracellular matrix (ECM), thereby loosing integrin-ligand interactions, as occurs during tumour cell invasion. 13,35 In normal tissue anoikis is critical in maintaining tissue homeostasis by preventing tissue proliferation in unwanted sites. Evading anoikis is a condition for cancer cells to survive and is believed to be an essential step in metastasis. 36,37 This also is the case during the process of PM formation where detached cells exhibit anchorage independent growth, meaning that they are able to survive without intact cell-cell signalling, a requisite for cell survival in normal cells. 38 In PM, this is most likely achieved by forming tumour cell clusters and retaining the ability to proliferate in cell clusters, as opposed to the adherence to platelets as described in haematogenous spread. 35,39
In peritoneal spread, two molecules are reported to play a role in anoikis evasion.

Molecular mechanisms in PM of CRC | Chapter 4
65
4
Kallikrein-related peptidases
The process of evading anoikis in PM involves the activation of the kallikrein-related peptidases (KLKs), a group of serine proteases. There are 15 proteins belonging to the kallikrein family. 40 Known functions of the KLKs include degradation of ECM molecules, contributing to activation of growth factors and proteases. One of the most well known KLKs, utilized in diagnosis and follow-up of prostate cancer, is KLK3 or prostate specific antigen (PSA). 41 Interestingly, there is a link between cell clustering and KLK expression. Cell clustering is a frequent event in OvCa ascites, which may contribute to anoikis evasion. 40 The aggregation of these malignant cells was associated with a higher protein expression of KLK7. 40 Hence, it is assumed that treatment response is, at least partly, governed by anoikis resistance under the influence of KLK7. Further investigation revealed that α5β1 integrins and KLK7 co-express in OvCa. Based on these findings an association between KLK7 levels and PM via cell aggregates and α5β1 integrin mediated cell-adhesion was assumed. Several integrin inhibitors, such as Volociximab 42,43 are currently under development and are of interest as targeted therapy in PM, based not only on the abovementioned results but also on a proof of principle study with blocking of β1 integrin (ITGB1 ) in a murine and ex-vivo peritoneal model, described under “Adhesion to peritoneal surface”. 44
KLKs have also been investigated as prognostic markers in CRC in primary tumours. A higher KLK 7 protein expression was found to be associated with a shorter overall and disease free survival in a study containing 105 patients. 45,46 In addition, analysis of a panel of KLKs shows overexpression of KLK5, KLK7 and KLK 14 to be prognostically relevant in patients with primary CRC in a multivariate analysis. 46
V-Src sarcoma viral oncogene homolog (Src)
Src is a tyrosine kinase that is described as a key player in cell-matrix contact-mediating focal adhesions, in cell-cell contact-mediating adherens junctions and in cell-anchorage dependent signalling. 39,47 A Src-dependent mechanism has been reported that provides transient protection of colonic epithelial cells from anoikis. 48 Using a Src-specific inhibitor, loss of protection from anoikis was shown in various experiments. 48,49 CRC cell line experiments have shown that enforced Src expression increases resistance to anoikis. 50 As well as having a role in anoikis evasion, upregulation of c-SRC causes adherent cells to scatter and to extend their lamellipodia, thus making tumour cells highly motile. 50 In a murine model, blocking of Src showed reduced peritoneal dissemination compared to control transfectants. These results support the hypothesis that c-SRC may play a role in detachment and motility of CRC cells.

Chapter 4 | Molecular mechanisms in PM of CRC
66
3. Adherence to peritoneal surface
After evasion of anoikis, detached malignant cells will have to adhere to the peritoneal surface to be able to ultimately invade and colonize the peritoneum. Adherence to the peritoneal surface depends largely on the interaction between malignant cells and ECM components through integrins, cadherins, and cell-adhesion molecules.
Integrins
Integrins are a family of receptors that play a major role in cell-ECM attachment and signalling. Integrins may also play a role in attachment of malignant cells to the peritoneum. The integrin family consists of 24 members, and function in different combinations of α and β subunits. 2,18 Integrins are expressed on epithelial as well as endothelial cells, leukocytes and platelets. Altered expression patterns of integrins are frequently associated with a malignant phenotype, supporting invasive and metastatic behaviour. 51,52
One of the integrins involved is the ITGB1. In a surgical trauma animal model, blocking ITGB1 caused less tumour cells to adhere to the peritoneum, followed by impaired outgrowth of tumours. These results were confirmed in an ex-vivo peritoneal and in-vivo mesothelial model. This suggests a role for integrins in the adherence and growth of tumour cells on (surgically traumatized) peritoneum. 44 Another integrin, α5β3, has been identified in PM of pancreatic cancer. It is the primary receptor for Cyr61, one of the molecules described under “Inducing Angiogenesis”. The experiments involving this receptor-ligand couple were carried out on a murine pancreatic cancer model, using microarray analysis, RT-PCR and IHC to confirm the results. 33 With IHC, co-localization of Cyr61 and α5 was observed, suggesting that the interaction between Cyr61 and α5β3 promotes the formation of PM. 33
Cadherin 1 (CDH1 or E-cadherin)
This protein is part of the cadherin family of cell adhesion molecules, consisting of glycoproteins that mediate cell-cell adhesion in epithelial cells. Reduced cell surface expression of this protein has been observed in many cancers, including oesophageal, colon, breast and OvCa. 53 As a consequence these cells show easy disaggregation, facilitating invasion and metastasis. 39,54
In PM of CRC one in-vivo study has been described with a LoVo clone showing E-cadherin downregulation to be associated with metastasis. 55 These cells formed a primary colon carcinoma in the host model, which was then resected. Seven out of ten mice showed isolated mesenteric lymph node metastases, not peritoneal carcinomatosis, post-resection, compared to 10 disease free mice in the control group.

Molecular mechanisms in PM of CRC | Chapter 4
67
4
In an OvCa model however, downregulation of E-cadherin by siRNA was followed by upregulation of α5β1integrin. 34 In this study, intra-peritoneal administration of an α5β1integrin antibody significantly reduced ascites and the number of metastases compared to the control group. 34 In a cohort of 107 OvCa patients the overexpression of α5-integrin correlated with worse survival. 34 Altogether, these findings imply an effect of downregulation of E-cadherin through an integrin-mediated pathway.
InterCellular Adhesion Molecule 1 (ICAM-1)
The ICAMs are a subfamily of the immunoglobulin superfamily of cell adhesion molecules. ICAM 1 is one of five ICAMs. 18 The role of ICAM 1 has been investigated in a pneumoperitoneum-simulated environment using a CRC cell line and a mesothelial cell monolayer. 56 In this study increased adhesion of CRC cells to the stimulated mesothelium was observed. 56 In an attachment assay to detect MMP’s activity in naive (unstimulated) mesothelium, it was confirmed that increased expression of ICAM-1 led to increased adhesion of malignant cells. 57 Moreover, the link between ICAM1-CD43 interaction and MMP production was analysed on invasion of attached cells. An increase in adhesion and invasion was noted, which was manifested by an increase in MMP expression. 57
Epithelial cell adhesion Molecule (Ep-CAM)
Ep-CAM is a type 1 transmembrane glycoprotein and not structurally related to the four major families of cell adhesion molecules. 58 Ep-CAM is frequently highly expressed in malignancies of epithelial origin, including CRC. 58,59
In peritoneal dissemination of OvCa the expression of Ep-CAM in primary, metastatic and recurrent epithelial OvCa was studied. 60 Using real-time polymerase chain reaction (qRT-PCR) and IHC in patient material and cell lines, high expression of Ep-CAM was detected in all three disease stages, with a significant difference in Ep-CAM expression levels between metastatic, recurrent and chemotherapy-resistant OvCa compared to normal ovarian epithelium. 60
CD 44 molecule (CD44)
The protein encoded by the CD44 gene is a cell surface glycoprotein that plays a role in cell-adhesion, cell-cell interaction and migration. It is a receptor for hyaluronic acid and can interact with MMPs and collagens as well. It participates in several cellular functions, one of which is metastasis. 61
Alternative splicing of CD44 pre-mRNA results in different isoforms of the protein. In CRC CD44 exon v6 splice variants are present in advanced stages of disease. 62,63

Chapter 4 | Molecular mechanisms in PM of CRC
68
In PM, in-vitro adhesion assays have been performed with the use of mesothelial cell cultures and OvCa cells. A CD44 monoclonal antibody partially inhibited adhesion of tumour cells to the mesothelium. In nude mice, treatment with CD44 monoclonal antibody led to significantly less tumour implants on the peritoneal surface. 61 Although some adhesion of OvCa cells to the mesothelial layer still occurred, albeit to a lesser extent, it ultimately lead to less PM. 61,64
Interactions have also been reported between chemokine receptors present on malignant cells and targets in the mesothelium in OvCa. Examples of this mechanism are the binding of CXCR4 to CXCL12 and the binding of MUC16 to Mesothelin. 65,66
Altogether these data suggest that the blocking of these attachment-mediating molecules could be of clinical importance. For example, in the peri-operative window, blocking of these candidates could lead to less implantation and subsequently less tumour outgrowth. 44,56,57,61
4. Invasion of the peritoneum
Proteolytic enzymes to degradate the ECM are necessary for tumour cells to be able to invade beyond the basement membrane. These enzymes are secreted by tumour cells themselves or by the stromal cells surrounding them. 67 ECM degrading metallopeptidases (MMPs) have been extensively linked to this step in peritoneal dissemination. 13
The matrix metallopeptidases (MMPs)
Proteins of the MMP family break down the ECM in normal physiological processes as well as in disease, including cancer. 68 MMPs facilitate invasion of the tumour cells into the nearby stroma by degrading multiple types of ECM proteins. They play a role in metastasis of CRC, including in liver- and lung metastases. 68,69
In gastric carcinoma overexpression of MMP7 in primary tumours, as seen by IHC and RT-PCR, was an independent risk factor for formation of PM. 16 In OvCa overexpression of MMP9 was reported to promote a migratory and invasive phenotype in functional experiments performed in two OvCa cell lines. 27 Altogether, the invasion of the peritoneal surface by cancer cells has been linked to altered MMP2, MMP7 & MMP9 expression in several gastro-intestinal tract malignancies. 16,27,69-71 For this reason, attempts have been made to treat PM with MMP inhibitors. Indeed, inhibition of MMPs with the drug Batimastat in rats inhibited development of CRC metastasis. 72 However, intra-peritoneal administration of this drug resulted in marked peritoneal inflammation and ascites, reason why no clinical studies with Batimastat in humans have been initiated to date.In addition, the Wilms Tumour gene protein 1 (WT1) and TIMP2 are also reported to promote invasion. Contact between malignant cells and the submesothelial collagen results in WT1 overexpression and subsequent invasion in OvCa. 73 Furthermore, decreased

Molecular mechanisms in PM of CRC | Chapter 4
69
4
invasive capacity is observed after blocking WT1 by siRNA. 73 TIMP-2 is a tissue inhibitor of metalloproteinases, for which a twofold upregulation of TIMP-2 mRNA was observed in the PM of CRC patients, next to upregulation of HIF-1α and IGF-1 that are described below. 74 TIMP-2 is part of the TIMP gene family and proteins encoded by this gene are inhibitors of the matrix metallopeptidases (MMPs). 75 In contrast to other TIMP family members, TIMP-2 also has the ability to directly suppress the proliferation of endothelial cells. 76
Several other genes have also been implicated in invasion of the peritoneum. These include: c-MET23,32, ITGB1 38,44,77,78 and CDH1 61, which have been discussed previously under “Adhesion to the peritoneal surface”.
5. The colonization phase - Survival in the new niche
Sustaining proliferative signalling, enabling replicative immortality and evading growth suppressors
One of the most fundamental characteristics of malignant cells is their ability to sustain proliferation. Cancer cells can achieve this by various methods, such as producing growth factors and receptors for autocrine stimulation and by stimulating the tumour-associated stroma to deliver various growth factors. 79 Additionally, changing receptor and downstream signalling facilitates ligand-independent signalling, also leading to proliferation induction. 13 In this category, IGF-1, VEGF and HIF1α have been reported in PM.
Insulin like growth factor 1
Insulin like growth factor 1 (IGF-1) is part of a family of peptides that play important roles in growth and development in mammals. 80 In a microarray study on PM and liver metastasis from CRC patients, IGF-1 mRNA was exclusively and fairly consistently overexpressed in PM when compared to liver metastasis. 74 Conversely, circulating levels of insulin-like growth factor binding protein 3 (IGFBP3), an endogenous antagonist of IGF-1, correlates with slower progression in patients with metastatic CRC. 81,82 Both these findings imply a role for IGF-1 in the formation of PM and underline that gene expression profiles differ per site of metastasis. 74,81
Inducing angiogenesis
As all cells, cancer cells are in need of nutrients for survival and 150-180µm is the maximum distance at which these nutrients can diffuse from blood vessels. Beyond this distance the tumour cannot proliferate without active angiogenesis, since the resulting hypoxia induces apoptosis. 13,83,84 One of the mechanisms used by cancer cells to overcome this limitation is the induction of angiogenesis, a process in which genes like Hypoxia Inducible Factor 1 (HIF1) and Vascular Endothelial Growth Factor (VEGF) play a role. 13,83,85

Chapter 4 | Molecular mechanisms in PM of CRC
70
Hypoxia inducible factor (HIF) 1
Hypoxia within the tumour microenvironment can induce angiogenesis by release of HIF1, which regulates production of VEGF. 83,85
In the same study discussed above, 20 colorectal adenocarcinomas and eight high-grade appendiceal adenocarcinomas were analysed for genome wide mRNA expression using oligonucleotide microarrays. Site-specific gene expression profiles were observed. A twofold upregulation of HIF1α specific for PM was noted in this cohort, next to TIMP-2 and IGF1, which were discussed above. 74 HIF1α has also been described as being upregulated in primary CRC when compared to normal mucosa. 83
Vascular endothelial growth factor (VEGF) and Vascular endothelial growth factor receptor (VEGFR)
VEGF has been extensively described as one of the most important angiogenic factors in solid tumours. 13 An IHC study of PM tissue samples from patients with adenocarcinoma of the appendix or colon demonstrated that higher VEGF expression was associated with a worse clinical prognosis. However, no significant correlation was noted between micro-vessel density and survival. 86 Mutations in VEGF, as well as the tumour suppressor gene p53 have been shown to play a role in metastasis of CRC. 2 About 50% of patients with metastatic disease are known to be positive for both mutations in p53 and VEGF. 2,87 VEGF targeted therapies are clinically widely used in combination with chemotherapeutic agents in patients with histologically confirmed CRC metastasis and measurable disease in the absence of absolute contraindications. 87 In a PM of CRC murine model, blocking of VEGFR with DC101, a VEGFR-2 specific antibody, has been shown to have a negative effect not only on angiogenesis but also on the proliferation of both tumour cells and endothelial cells, effectively showing significantly reduced intra-abdominal tumour burden and ascites formation. 88-90
Immune aggregates & VEGF
As an alternative mechanism for the pathogenesis of PM, one paper described the preferential attachment of malignant cells to immune aggregates in the omentum. In a murine model using several cell lines, including one OvCa cell line, these immune aggregates in the omentum were noted to have a complex network of capillaries with a high vascular density. 91 The mesothelial cells overlying these immune aggregates were observed to be hypoxic and VEGF-A production co-localized with these hypoxic regions. This mechanism was hypothesised to contribute to the survival of these tumour cells on the peritoneum, due to apparent constitutive readiness of the vasculature in the immune aggregates to expand. 91,92 Interestingly, these immune aggregates have also been observed

Molecular mechanisms in PM of CRC | Chapter 4
71
4
in humans. 93-97 Theoretically, their presence and reported make-up could form a plausible explanation for the attachment of free cancer cells to these sites in the peritoneal surface.
Cysteine-rich protein 61 (Cyr61)
Cyr61, already referred to above, is a secreted matricellular protein that binds to integrins. 98 The Connective tissue growth factor, Cysteine-rich protein, and Nephroblastoma overexpressed gene (CCN) family consists of six members that play a role in processes such as fibrosis, angiogenesis and wound healing. 98 Overexpression of Cyr61 in tumour cells has been linked to PM in pancreatic cancer. 33 Cyr61 is the ligand for the α5β3 integrin, described under “Attachment to peritoneum”. Therefore, Cyr61 is known to activate both angiogenesis and cell-cell attachment related signalling pathways in PM. 33
Molecules such as CD44 and α5β3 have also been linked to angiogenesis in disseminated disease in several experiments. 33,61,64 These results are mostly based on comparative genomic hybridization and IHC (validation) studies in pancreatic, colorectal and OvCa. Taken together, these findings support an important role of angiogenesis in the process of peritoneal dissemination. For this reason, interfering with angiogenesis has been investigated as a method for treating PM. In nude mice, inhibition of growth of PM of CRC was demonstrated when intra-peritoneally injected tumour cells were treated with the angiogenesis inhibitor TNP-470. 99 TNP-470 inhibits methionine aminopeptidase type II, which causes proliferation of endothelial cells. 99-101 The TNP-470 treated mice in this study had significantly less tumour foci intra-peritoneally, smaller tumours and a longer survival compared to the control group. 99 These effects are similar to those that have been reported in the aforementioned VEGFR-blocking experiments, suggesting that anti-angiogenic therapy holds promise in the treatment of PM. A summary of the process of peritoneal dissemination and the proposed effects of the identified molecules in PM of CRC is depicted in figure1. Of all the described molecules, albeit highly experimental, several show not only biological relevance, but have been shown to have either a prognostic effect in PM or hold promise as a therapeutic target in the future. (Table1)

Chapter 4 | Molecular mechanisms in PM of CRC
72
Primary tumour Free floating Cancer Cells
Cancer Cell
Peritoneum
Attached Cancer cells
Invading Cancer Cells
Small Peritoneal Metastasis
Detachment and motility
Invasion; MMP’s
Adhesion to peritoneal surface;
ITGB1
CDH1
ICAM-1
Anoikis Evasion;
KLK 7
Src
Other;
IGF-1
HIF1α
TIMP2
VEGF
Figure 1: The roles of the identified molecules in PM of CRC per dissemination step
Table 1: Summary of targets with possibility for clinical implementation in PM in the future
Promising Target in PM
Biological relevance in PM
Difference with CRLM
Prognostic relevance Possible therapeutic implications
IGF-1 Growth factor Yes, >2-fold change in mRNA 74
Not clear Monoclonal antibody Figitumumab 102,103
KLK7 Anoikis Evasion Not clear Yes, worse overall survival in CRC 45,46
Inhibition of KLK7 would lead to less evasion of anoikis. 40 However, interaction with α5β1 integrin, thus integrin inhibitors such as Volociximab may also be of interest. 42,43
HIF1 Angiogenesis Yes, >2 fold change in mRNA 74
Not clear, trend was observed
HIF1 inhibitors could potentially be of interest in PM. HIF1 upregulation seems also to be specific for PM 74,104
VEGF Angiogenesis No Yes, high VEGF expression correlated to worse survival 86
Currently anti-VEGF antibody therapies already in use in clinical setting, very promising for clinical application. 87

Molecular mechanisms in PM of CRC | Chapter 4
73
4
Table 1: Summary of targets with possibility for clinical implementation in PM in the future
Promising Target in PM
Biological relevance in PM
Difference with CRLM
Prognostic relevance Possible therapeutic implications
Cyr61 Angiogenesis No Not clear Is the ligand for α5β3. If possibility for blocking this interaction blocking of attachment to peritoneal surface ensues and subsequent angiogenesis is inhibited. 33
TWIST Detachment and motility
No Not clear In experimental model blocking of TWIST showed less migration, invasion and adhesion to peritoneal surface. In theory powerful inhibition of PM formation. 20
c-MET Detachment and motility
No Yes, higher expression of c-MET correlated to worse survival 24
In multiple experimental models blocking of c-MET showed marked inhibition of dissemination. Theoretically attractive therapeutic target. 25
EGFR Detachment and motility
No Not clear Cetuximab is a clinical grade antibody already widely in use for metastasized CRC. No clinical data on specific EGFR inhibition in PM is available.
Integrins Adhesion molecule
Not clear Not clear In multiple experimental models blocking of integrins showed marked inhibition of dissemination. Theoretically attractive therapeutic target. 44,77,78 Several integrin inhibitors currently under development. 42,43
ICAM-1 Adhesion molecule
Not clear Not clear Highly experimental, dubious if therapeutically significant. Theoretically blocking of ICAM-1 leads to less PM due to less attachment to peritoneum. 56
Ep-CAM Adhesion molecule
Not clear Yes, higher expression of Ep-CAM correlated to worse survival 60
Dubious if therapeutically significant. Theoretically blocking of Ep-CAM leads to less PM due to less attachment to peritoneum.
CD44 Adhesion molecule
Not clear Yes, exon v6 variant in advanced disease 62,63
Highly experimental, dubious if therapeutically significant. Blocking of CD44 does not completely block attachment to peritoneum in experimental model. 61
MMPs Proteolytic enzyme
No Yes, higher expression of MMP7 in primary tumour independent risk factor for PM. 16
In experimental model, treatment with Batimastat showed inhibition of PM. However serious adverse events reported, thus no clinical studies to date. 72

Chapter 4 | Molecular mechanisms in PM of CRC
74
Table 2: Targets extracted from PM of CRC studies and possible clinical implications
Target expressed in HIPEC patient material from PM of CRC
Possible clinicalimplementation
Correlation with outcome of HIPEC patients after treatment with CRS and HIPEC
IGF-1 74,102,103 Therapeutic Unknown
TIMP2 16,74 Possible stratification tool Unknown
HIF1 74,84 Possible stratification toolTherapeutic
Unknown
VEGF 86,87 Possible stratification toolTherapeutic
Yes 86
Discussion
PM of CRC, but also other malignancies, form a serious threat for the patient’s survival. While systemic drug therapy has only limited effect on the patient’s outcome, the best option for changing the clinical course is aggressive surgery in combination with HIPEC. At least a subset of patients has been demonstrated to benefit from this approach. Yet despite the reported survival benefit reported after CRS & HIPEC in patients with PM of CRC, several unmet clinical needs still exist, mainly in the field of diagnostics. Basically, these fall apart into three topics; A first major issue is the challenge to be able to diagnose the presence of PM earlier, at a stage when the disease is less wide spread. Secondly, there is a need for diagnostic tools to discriminate between patients who are likely to benefit from this intensive treatment, and those that will not, and thus would be exposed to the risk of morbidity and mortality of this treatment in vain. A third, but perhaps more remote goal, is to arrive, even in this disease state, to a more personalised approach. In an ideal situation the cytoreductive drugs used during HIPEC would be more in tune with the biological characteristics of the individual tumour, rather than the current ‘one size fits all’ approach.A common denominator in trying to achieve these goals is making use of relevant information on the biology of the disease process, because these biological mechanisms ultimately dictate the clinical phenotype. This biological information can be read out from patient samples at the DNA, RNA or protein level, but in principle also by molecular imaging modalities. These reporter molecules are then referred to as biomarkers. As the present review shows, the field of biomarkers for these three indications is still rather in its infancy. Most observations concern initial proof of concept studies, there is hardly any validation in independent series, and no prospective stratification studies yet. Most work has been done on retrospectively collected tissue samples, and limited efforts have been conducted to develop assays that would work in clinical diagnostic settings. Also, the field of molecular imaging of PM is still in its early days.More specifically, with respect to biomarkers for early detection of PMs, several clinical studies have shown that a lower peritoneal cancer index (PCI), i.e. the amount of PM

Molecular mechanisms in PM of CRC | Chapter 4
75
4
present at the start of treatment, as well as the extent to which the surgeon has succeeded in removing all PM, are both strongly associated with disease outcome after CRS and HIPEC for PM of CRC. 4,10,105 Yet, detection of small lesions remains a challenge, making pre- and intra-operative assessment of the extent of PM difficult. 12 Recently, targeted imaging strategies have been applied in PM of OvCa by means of intra-operative tumour specific fluorescent imaging using a Folate Receptor-α-targeted fluorescent agent. 106 This allows for more precise resection of small lesions otherwise overlooked. 106 Theoretically, similar approaches could work in PM of CRC, e.g. targeting molecules like EGFR and VEGFR. As for pre-operative imaging, alternative PET-tracers to 18-FDG could provide the additional accuracy needed for timely diagnosis of PM. However, challenges here also exist in the fact that the currently available pre-operative imaging modalities such as CT, PET and MRI come with technical limitations, such as a maximum resolution of the obtained image.After meticulous analysis of the available literature we have to conclude that currently the only targets that have the potential to be assessed in a clinical setting in the near future are IGF1, TIMP2, HIF1 and VEGF. These are the only known targets to have been solely extracted by analysis of PM of CRC in two separate studies. 74,86 It is also known that HIF1 regulates production of VEGF 83,85, making VEGF, an even more interesting target. As to biomarkers for the prediction of response to CRS & HIPEC for PM of CRC, i.e. discriminating between patients that may and patients that probably will not benefit from the treatment, only VEGF has been reported to be associated with outcome after CRS and HIPEC. 86 Yet all four markers currently lack enough promise for translation on short notice into a diagnostic test of use in a clinico-pathological setting in the assessment of material acquired from PM of CRC. (Table 2)
With respect to personalised therapy approaches, currently little data exist on candidate biomarkers for prediction of response to Mitomycin C (MMC) despite the fact that this drug has been around for quite some time. Interestingly, MMC based functional assays are used for the diagnosis of Fanconi anaemia, a rare hereditary disorder in which the function of one of several genes in the Fanconi pathway is disrupted. So far, however, no clear role for the Fanconi pathway has been established in CRC. Also other biomarkers that may be associated with response to cross linking agents have not yet been evaluated in CRC PM. 107 To date, established targeted therapies in CRC include drugs against EGFR, like Cetuximab, or anti-angiogenic drugs like Bevacuzimab. For the former drug, a number of biomarkers exist, of which KRAS mutation status is most established, while for the latter so far no good biomarkers have been established. 108,109 Remarkably, most of the molecules involved have not yet been reported as having an effect on survival in PM of CRC, except for VEGF.

Chapter 4 | Molecular mechanisms in PM of CRC
76
Areas for further investigation
The present review of literature suggests that there is opportunity for both discovery studies and further validation of the identified candidates for implementation in treatment stratification in patients with PM of CRC. Mainly the lack of genome-wide studies on well-defined patient cohorts poses an interesting avenue of research to identify other molecules possibly omitted by the thus far implemented candidate based approach.Several other aspects of metastasis also require further elucidation. One of which is acquiring insight into the differences or similarities between the biology of primary colorectal tumours versus their corresponding metastases. Secondly, a better understanding of metastasis promoting features of the peritoneal environment itself, including tumour-stroma interaction.
Conclusions
Currently, several promising candidates have been identified that may have potential for use as a biomarker in PM of CRC, but all of these require extensive further validation. Therefore, rapid changes in clinical decision-making and therapy design based on current data would be premature. Yet, the pace of the omics revolution makes that the question is not if, but when biomarkers will be introduced to improve diagnosis and ultimately outcome of patients with PM due to CRC. This will certainly have the potential for a significant reduction in treatment related morbidity and mortality in this population by bringing the right treatment to the right patient.

Molecular mechanisms in PM of CRC | Chapter 4
77
4
References1. Parkin DM, Bray F, Ferlay J, Pisani P. Global
cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108.
2. Bird NC, Mangnall D, Majeed AW. Biology of colorectal liver metastases: A review. J Surg Oncol. 2006;94(1):68–80. doi:10.1002/jso.20558.
3. Koppe MJ, Boerman OC, Oyen WJG, Bleichrodt RP. Peritoneal Carcinomatosis of Colorectal Origin. Annals of Surgery. 2006;243(2):212–222. doi:10.1097/01.sla.0000197702.46394.16.
4. Maggiori L, Elias D. Curative treatment of colorectal peritoneal carcinomatosis: current status and future trends. Eur J Surg Oncol. 2010;36(7):599–603. doi:10.1016/j.ejso.2010.05.007.
5. Cao C, Yan TD, Black D, Morris DL. A Systematic Review and Meta-Analysis of Cytoreductive Surgery with Perioperative Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis of Colorectal Origin. Ann Surg Oncol. 2009;16(8):2152–2165. doi:10.1245/s10434-009-0487-4.
6. Klaver YLB, Lemmens VEPP, Creemers GJ, Rutten HJT, Nienhuijs SW, de Hingh IHJT. Population-based survival of patients with peritoneal carcinomatosis from colorectal origin in the era of increasing use of palliative chemotherapy. Annals of Oncology. 2011;22(10):2250–2256. doi:10.1093/annonc/mdq762.
7. Sugarbaker PH. Patient selection and treatment of peritoneal carcinomatosis from colorectal and appendiceal cancer. World J Surg. 1995;19(2):235–240.
8. Sugarbaker PH, Jablonski KA. Prognostic features of 51 colorectal and 130 appendiceal cancer patients with peritoneal carcinomatosis treated by cytoreductive surgery and intraperitoneal chemotherapy. Annals of Surgery. 1995;221(2):124–132.
9. Cavaliere F, De Simone M, Virzì S, et al. Prognostic factors and oncologic outcome in 146 patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: Italian multicenter study S.I.T.I.L.O. European Journal of Surgical Oncology. 2011;37(2):148–154. doi:10.1016/j.ejso.2010.10.014.
10. Verwaal VJ. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. Journal of Clinical Oncology. 2003;21(20):3737–3743. doi:10.1200/JCO.2003.04.187.
11. Abdalla EK, Vauthey J-N, Ellis LM, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Annals of Surgery. 2004;239(6):818–25; discussion 825–7.
12. Verwaal VJ, Zoetmulder FAN. Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. European Journal of Surgical Oncology (EJSO). 2004;30(3):280–285. doi:10.1016/j.ejso.2003.12.003.
13. Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013.
14. Nguyen DX, Bos PD, Massagué J. Metastasis: from dissemination to organ-specific colonization. Nat Rev Cancer. 2009;9(4):274–284. doi:10.1038/nrc2622.
15. van der Wal JBC, Jeekel J. Biology of the peritoneum in normal homeostasis and after surgical trauma. Colorectal Dis. 2007;9 Suppl 2:9–13. doi:10.1111/j.1463-1318.2007.01345.x.
16. Yonemura Y, Endou Y, Fujita H, et al. Role of MMP-7 in the formation of peritoneal dissemination in gastric cancer. Gastric Cancer. 2000;3(2):63–70.
17. Yilmaz M, Christofori G. EMT, the cytoskeleton, and cancer cell invasion. Cancer Metastasis Rev. 2009;28(1-2):15–33. doi:10.1007/s10555-008-9169-0.
18. Paschos KA, Canovas D, Bird NC. The role of cell adhesion molecules in the progression of colorectal cancer and the development of liver metastasis. Cellular Signalling. 2009;21(5):665–674. doi:10.1016/j.cellsig.2009.01.006.
19. Guarino M, Rubino B, Ballabio G. The role of epithelial-mesenchymal transition in cancer pathology. Pathology. 2007;39(3):305–318. doi:10.1080/00313020701329914.
20. Terauchi M, Kajiyama H, Yamashita M, et al. Possible involvement of TWIST in enhanced peritoneal metastasis of epithelial ovarian carcinoma. Clin Exp Metastasis. 2007;24(5):329–339. doi:10.1007/s10585-007-9070-1.
21. Ma PC, Maulik G, Christensen J, Salgia R. c-Met: structure, functions and potential for therapeutic inhibition. Cancer Metastasis Rev. 2003;22(4):309–325.
22. Gentile A, D’Alessandro L, Lazzari L, et al. Met-driven invasive growth involves transcriptional regulation of Arhgap12. Oncogene. 2008;27(42):5590–5598. doi:10.1038/onc.2008.173.

Chapter 4 | Molecular mechanisms in PM of CRC
78
23. Boccaccio C, Comoglio PM. Invasive growth: a MET-driven genetic programme for cancer and stem cells. Nat Rev Cancer. 2006;6(8):637–645. doi:10.1038/nrc1912.
24. Osada S, Matsui S, Komori S, et al. Effect of hepatocyte growth factor on progression of liver metastasis in colorectal cancer. Hepatogastroenterology. 2010;57(97):76–80.
25. Sawada K, Radjabi AR, Shinomiya N, et al. c-Met overexpression is a prognostic factor in ovarian cancer and an effective target for inhibition of peritoneal dissemination and invasion. Cancer Research. 2007;67(4):1670–1679. doi:10.1158/0008-5472.CAN-06-1147.
26. Davies RL, Grosse VA, Kucherlapati R, Bothwell M. Genetic analysis of epidermal growth factor action: assignment of human epidermal growth factor receptor gene to chromosome 7. Proc Natl Acad Sci USA. 1980;77(7):4188–4192.
27. Cowden Dahl KD, Symowicz J, Ning Y, et al. Matrix Metalloproteinase 9 Is a Mediator of Epidermal Growth Factor-Dependent E-Cadherin Loss in Ovarian Carcinoma Cells. Cancer Research. 2008;68(12):4606–4613. doi:10.1158/0008-5472.CAN-07-5046.
28. Nicosia SV, Bai W, Cheng JQ, Coppola D, Kruk PA. Oncogenic pathways implicated in ovarian epithelial cancer. Hematol Oncol Clin North Am. 2003;17(4):927–943.
29. Davidson B, Goldberg I, Gotlieb WH, et al. High levels of MMP-2, MMP-9, MT1-MMP and TIMP-2 mRNA correlate with poor survival in ovarian carcinoma. Clin Exp Metastasis. 1999;17(10):799–808.
30. Kamat AA, Fletcher M, Gruman LM, et al. The clinical relevance of stromal matrix metalloproteinase expression in ovarian cancer. Clin Cancer Res. 2006;12(6):1707–1714. doi:10.1158/1078-0432.CCR-05-2338.
31. Gentile A, Trusolino L, Comoglio PM. The Met tyrosine kinase receptor in development and cancer. Cancer Metastasis Rev. 2008;27(1):85–94. doi:10.1007/s10555-007-9107-6.
32. Benvenuti S, Comoglio PM. The MET receptor tyrosine kinase in invasion and metastasis. J Cell Physiol. 2007;213(2):316–325. doi:10.1002/jcp.21183.
33. Holloway SE, Beck AW, Girard L, et al. Increased expression of Cyr61 (CCN1) identified in peritoneal metastases from human pancreatic cancer. Journal of the American College of Surgeons. 2005;200(3):371–377. doi:10.1016/j.jamcollsurg.2004.10.005.
34. Sawada K, Mitra AK, Radjabi AR, et al. Loss of E-Cadherin Promotes Ovarian Cancer Metastasis via 5-Integrin, which Is a Therapeutic Target. Cancer Research. 2008;68(7):2329–2339. doi:10.1158/0008-5472.CAN-07-5167.
35. Douma S, Van Laar T, Zevenhoven J, Meuwissen R, Van Garderen E, Peeper DS. Suppression of anoikis and induction of metastasis by the neurotrophic receptor TrkB. Nature. 2004;430(7003):1034–1039. doi:10.1038/nature02765.
36. CHIARUGI P, GIANNONI E. Anoikis: A necessary death program for anchorage-dependent cells. Biochemical Pharmacology. 2008;76(11):1352–1364. doi:10.1016/j.bcp.2008.07.023.
37. Horbinski C, Mojesky C, Kyprianou N. Live Free or Die. The American Journal of Pathology. 2010;177(3):1044–1052. doi:10.2353/ajpath.2010.091270.
38. Gimond C, van Der Flier A, van Delft S, et al. Induction of cell scattering by expression of beta1 integrins in beta1-deficient epithelial cells requires activation of members of the rho family of GTPases and downregulation of cadherin and catenin function. J Cell Biol. 1999;147(6):1325–1340.
39. Weinberg RA. The Biology of Cancer. 1st ed. Garland Science; 2006.
40. Dong Y, Tan OL, Loessner D, et al. Kallikrein-Related Peptidase 7 Promotes Multicellular Aggregation via the 5 1 Integrin Pathway and Paclitaxel Chemoresistance in Serous Epithelial Ovarian Carcinoma. Cancer Research. 2010;70(7):2624–2633. doi:10.1158/0008-5472.CAN-09-3415.
41. Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Redwine E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. New England Journal of Medicine. 1987;317(15):909–916. doi:10.1056/NEJM198710083171501.
42. Bhaskar V, Zhang D, Fox M, et al. A function blocking anti-mouse integrin alpha5beta1 antibody inhibits angiogenesis and impedes tumor growth in vivo. J Transl Med. 2007;5:61. doi:10.1186/1479-5876-5-61.
43. Ramakrishnan V, Bhaskar V, Law DA, et al. Preclinical evaluation of an anti-alpha5beta1 integrin antibody as a novel anti-angiogenic agent. J Exp Ther Oncol. 2006;5(4):273–286.
44. Oosterling SJ, van der Bij GJ, Bögels M, et al. Anti-β1 Integrin Antibody Reduces Surgery-Induced Adhesion of Colon Carcinoma Cells to Traumatized Peritoneal Surfaces. Annals of Surgery. 2008;247(1):85–94. doi:10.1097/SLA.0b013e3181588583.

Molecular mechanisms in PM of CRC | Chapter 4
79
4
45. Talieri M, Mathioudaki K, Prezas P, et al. Clinical significance of kallikrein-related peptidase 7 (KLK7) in colorectal cancer. Thromb Haemost. 2009. doi:10.1160/TH08-07-0471.
46. Talieri M, Li L, Zheng Y, et al. The use of kallikrein-related peptidases as adjuvant prognostic markers in colorectal cancer. 2009;100(10):1659–1665. doi:10.1038/sj.bjc.6605033.
47. Kim LC, Song L, Haura EB. Src kinases as therapeutic targets for cancer. Nat Rev Clin Oncol. 2009;6(10):587–595. doi:10.1038/nrclinonc.2009.129.
48. Hofmann C, Lippert E, Falk W, Schölmerich J, Rogler G, Obermeier F. Primary human colonic epithelial cells are transiently protected from anoikis by a Src-dependent mechanism. Biochemical and Biophysical Research Communications. 2009;390(3):908–914. doi:10.1016/j.bbrc.2009.10.075.
49. Windham TC, Parikh NU, Siwak DR, et al. Src activation regulates anoikis in human colon tumor cell lines. Oncogene. 2002;21(51):7797–7807. doi:10.1038/sj.onc.1205989.
50. Sakamoto M, Takamura M, Ino Y, Miura A, Genda T, Hirohashi S. Involvement of c-Src in carcinoma cell motility and metastasis. Jpn J Cancer Res. 2001;92(9):941–946.
51. Felding-Habermann B. Integrin adhesion receptors in tumor metastasis. Clin Exp Metastasis. 2003;20(3):203–213.
52. Varner JA, Cheresh DA. Integrins and cancer. Curr Opin Cell Biol. 1996;8(5):724–730.
53. Guilford P, Hopkins J, Harraway J, et al. E-cadherin germline mutations in familial gastric cancer. Nature. 1998;392(6674):402–405. doi:10.1038/32918.
54. Birchmeier W, Weidner KM, Hülsken J, Behrens J. Molecular mechanisms leading to cell junction (cadherin) deficiency in invasive carcinomas. Semin Cancer Biol. 1993;4(4):231–239.
55. Pocard M, Debruyne P, Bras-Gonçalves R, Mareel M, Dutrillaux B, Poupon MF. Single alteration of p53 or E-cadherin genes can alter the surgical resection benefit in an experimental model of colon cancer. Diseases of the Colon & Rectum. 2001;44(8):1106–1112.
56. Ziprin P, Ridgway PF, Peck DH, Darzi AW. Laparoscopic enhancement of tumour cell binding to the peritoneum is inhibited by anti?intercellular adhesion molecule-1 monoclonal antibody. Surg Endosc. 2003;17(11):1812–1817. doi:10.1007/s00464-002-8766-1.
57. Alkhamesi NA, Roberts G, Ziprin P, Peck DH. Induction of Proteases in Peritoneal Carcinomatosis, the Role of ICAM-1/CD43 Interaction. Biomark Insights. 2007;2:377–384.
58. Balzar M, Winter MJ, de Boer CJ, Not Available SVL. The biology of the 17-1A antigen (Ep-CAM). Journal of Molecular Medicine. 1999;77(10):699–712. doi:10.1007/s001099900038.
59. Xie X, Wang C-Y, Cao Y-X, et al. Expression pattern of epithelial cell adhesion molecule on normal and malignant colon tissues. WJG. 2005;11(3):344–347.
60. Bellone S, Siegel ER, Cocco E, et al. Overexpression of Epithelial Cell Adhesion Molecule in Primary, Metastatic, and Recurrent/Chemotherapy-Resistant Epithelial Ovarian Cancer. International Journal of Gynecological Cancer. 2009;19(5):860–866. doi:10.1111/IGC.0b013e3181a8331f.
61. Lessan K, Aguiar DJ, Oegema T, Siebenson L, Skubitz AP. CD44 and beta1 integrin mediate ovarian carcinoma cell adhesion to peritoneal mesothelial cells. The American Journal of Pathology. 1999;154(5):1525–1537.
62. Herrlich P, Pals S, Ponta H. CD44 in colon cancer. European Journal of Cancer. 1995;31A(7-8):1110–1112.
63. Mulder JW, Wielenga VJ, Polak MM, et al. Expression of mutant p53 protein and CD44 variant proteins in colorectal tumorigenesis. Gut. 1995;36(1):76–80.
64. Cannistra SA, Kansas GS, Niloff J, DeFranzo B, Kim Y, Ottensmeier C. Binding of ovarian cancer cells to peritoneal mesothelium in vitro is partly mediated by CD44H. Cancer Research. 1993;53(16):3830–3838.
65. Kajiyama H, Shibata K, Terauchi M, Ino K, Nawa A, Kikkawa F. Involvement of SDF-1alpha/CXCR4 axis in the enhanced peritoneal metastasis of epithelial ovarian carcinoma. Int J Cancer. 2008;122(1):91–99. doi:10.1002/ijc.23083.
66. Gubbels JAA, Belisle J, Onda M, et al. Mesothelin-MUC16 binding is a high affinity, N-glycan dependent interaction that facilitates peritoneal metastasis of ovarian tumors. Mol Cancer. 2006;5(1):50. doi:10.1186/1476-4598-5-50.
67. Kataoka H, Tanaka H, Nagaike K, Uchiyama S, Itoh H. Role of cancer cell-stroma interaction in invasive growth of cancer cells. Hum Cell. 2003;16(1):1–14.
68. Vihinen P, Kähäri V-M. Matrix metalloproteinases in cancer: prognostic markers and therapeutic targets. Int J Cancer. 2002;99(2):157–166. doi:10.1002/ijc.10329.
69. Yamada T, Oshima T, Yoshihara K, et al. Overexpression of MMP-13 gene in colorectal cancer with liver metastasis. Anticancer Res. 2010;30(7):2693–2699.

Chapter 4 | Molecular mechanisms in PM of CRC
80
70. Sc EJCB, D GRP, Sc RGB, Sc TRB, Sc MMB, Sc PZB. Investigation of Tumor-Peritoneal Interactions in the Pathogenesis of Peritoneal Metastases using a Novel Ex Vivo Peritoneal Model1. Journal of Surgical Research. 2010;164(2):e265–e272. doi:10.1016/j.jss.2010.09.041.
71. Peng L, Xing X, Li W, et al. PRL-3 promotes the motility, invasion, and metastasis of LoVo colon cancer cells through PRL-3-integrin β1-ERK1/2 and-MMP2 signaling. Mol Cancer. 2009;8(1):110. doi:10.1186/1476-4598-8-110.
72. Aparicio T, Kermorgant S, Dessirier V, Lewin MJ, Lehy T. Matrix metalloproteinase inhibition prevents colon cancer peritoneal carcinomatosis development and prolongs survival in rats. Carcinogenesis. 1999;20(8):1445–1451.
73. Barbolina MV, Adley BP, Shea LD, Stack MS. Wilms tumor gene protein 1 is associated with ovarian cancer metastasis and modulates cell invasion. Cancer. 2008;112(7):1632–1641. doi:10.1002/cncr.23341.
74. Varghese S, Burness M, Xu H, Beresnev T, Pingpank J, Alexander HR. Site-Specific Gene Expression Profiles and Novel Molecular Prognostic Factors in Patients with Lower Gastrointestinal Adenocarcinoma Diffusely Metastatic to Liver or Peritoneum. Ann Surg Oncol. 2007;14(12):3460–3471. doi:10.1245/s10434-007-9557-7.
75. Hojilla CV, Mohammed FF, Khokha R. Matrix metalloproteinases and their tissue inhibitors direct cell fate during cancer development. British Journal of Cancer. 2003;89(10):1817–1821. doi:10.1038/sj.bjc.6601327.
76. NCBI, ed. TIMP2 TIMP metallopeptidase inhibitor 2 [Homo sapiens] - Gene - NCBI.
77. Raa ST, Oosterling SJ, van der Kaaij NP, et al. Surgery promotes implantation of disseminated tumor cells, but does not increase growth of tumor cell clusters. J Surg Oncol. 2005;92(2):124–129. doi:10.1002/jso.20273.
78. van der Bij GJ, Oosterling SJ, Beelen RHJ, Meijer S, Coffey JC, van Egmond M. The Perioperative Period is an Underutilized Window of Therapeutic Opportunity in Patients With Colorectal Cancer. Annals of Surgery. 2009;249(5):727–734. doi:10.1097/SLA.0b013e3181a3ddbd.
79. Bhowmick NA, Neilson EG, Moses HL. Stromal fibroblasts in cancer initiation and progression. Nature. 2004;432(7015):332–337. doi:10.1038/nature03096.
80. Kjeldsen T, Andersen AS, Wiberg FC, et al. The ligand specificities of the insulin receptor and the insulin-like growth factor I receptor reside in different regions of a common binding site. Proc Natl Acad Sci USA. 1991;88(10):4404–4408.
81. Fuchs CS, Goldberg RM, Sargent DJ, et al. Plasma Insulin-like Growth Factors, Insulin-like Binding Protein-3, and Outcome in Metastatic Colorectal Cancer: Results from Intergroup Trial N9741. Clinical Cancer Research. 2008;14(24):8263–8269. doi:10.1158/1078-0432.CCR-08-0480.
82. Goldberg RM. A Randomized Controlled Trial of Fluorouracil Plus Leucovorin, Irinotecan, and Oxaliplatin Combinations in Patients With Previously Untreated Metastatic Colorectal Cancer. Journal of Clinical Oncology. 2003;22(1):23–30. doi:10.1200/JCO.2004.09.046.
83. Greijer AE, Delis-van Diemen PM, Fijneman RJA, et al. Presence of HIF-1 and related genes in normal mucosa, adenomas and carcinomas of the colorectum. Virchows Archiv. 2008;452(5):535–544. doi:10.1007/s00428-008-0578-9.
84. Nijkamp MW, Hoogwater FJH, Steller EJA, et al. CD95 is a key mediator of invasion and accelerated outgrowth of mouse colorectal liver metastases following radiofrequency ablation. Journal of Hepatology. 2010;53(6):1069–1077. doi:10.1016/j.jhep.2010.04.040.
85. Wu Y, Jin M, Xu H, et al. Clinicopathologic significance of HIF-1α, CXCR4, and VEGF expression in colon cancer. Clin Dev Immunol. 2010;2010. doi:10.1155/2010/537531.
86. Logan-Collins JM, Lowy AM, Robinson-Smith TM, et al. VEGF Expression Predicts Survival in Patients with Peritoneal Surface Metastases from Mucinous Adenocarcinoma of the Appendix and Colon. Ann Surg Oncol. 2007;15(3):738–744. doi:10.1245/s10434-007-9699-7.
87. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. doi:10.1056/NEJMoa032691.
88. Shaheen RM, Ahmad SA, Liu W, et al. Inhibited growth of colon cancer carcinomatosis by antibodies to vascular endothelial and epidermal growth factor receptors. British Journal of Cancer. 2001;85(4):584–589. doi:10.1054/bjoc.2001.1936.
89. Bruns CJ, Shrader M, Harbison MT, et al. Effect of the vascular endothelial growth factor receptor-2 antibody DC101 plus gemcitabine on growth, metastasis and angiogenesis of human pancreatic cancer growing orthotopically in nude mice. Int J Cancer. 2002;102(2):101–108. doi:10.1002/ijc.10681.
90. Bruns CJ, Liu W, Davis DW, et al. Vascular endothelial growth factor is an in vivo survival factor for tumor endothelium in a murine model of colorectal carcinoma liver metastases. Cancer. 2000;89(3):488–499.

Molecular mechanisms in PM of CRC | Chapter 4
81
4
91. Sorensen EW, Gerber SA, Sedlacek AL, Rybalko VY, Chan WM, Lord EM. Omental immune aggregates and tumor metastasis within the peritoneal cavity. Immunol Res. 2009. doi:10.1007/s12026-009-8100-2.
92. Gerber SA, Rybalko VY, Bigelow CE, et al. Preferential Attachment of Peritoneal Tumor Metastases to Omental Immune Aggregates and Possible Role of a Unique Vascular Microenvironment in Metastatic Survival and Growth. The American Journal of Pathology. 2006;169(5):1739–1752. doi:10.2353/ajpath.2006.051222.
93. Beelen RHJ, Oosterling SJ, van Egmond M, van den Born J, Zareie M. Omental milky spots in peritoneal pathophysiology (spots before your eyes). Perit Dial Int. 2005;25(1):30–32.
94. Beelen RH. Role of omental milky spots in the local immune response. Lancet. 1992;339(8794):689.
95. Krist LF, Koenen H, Calame W, et al. Ontogeny of milky spots in the human greater omentum: an immunochemical study. Anat Rec. 1997;249(3):399–404.
96. Yildirim A, Aktaş A, Nergiz Y, Akkuş M. Analysis of human omentum-associated lymphoid tissue components with S-100: an immunohistochemical study. Rom J Morphol Embryol. 2010;51(4):759–764.
97. Yildirim A, Akkus M, Nergiz Y, Yuruker S. Immunohistochemical analysis of CD31, CD36, and CD44 antigens in human omentum. Saudi Med J. 2004;25(3):308–312.
98. Babic AM, Kireeva ML, Kolesnikova TV, Lau LF. CYR61, a product of a growth factor-inducible immediate early gene, promotes angiogenesis and tumor growth. Proc Natl Acad Sci USA. 1998;95(11):6355–6360.
99. Fan Y-F, Huang Z-H. Angiogenesis inhibitor TNP-470 suppresses growth of peritoneal disseminating foci of human colon cancer line Lovo. WJG. 2002;8(5):853–856.
100. Griffith EC, Su Z, Niwayama S, Ramsay CA, Chang YH, Liu JO. Molecular recognition of angiogenesis inhibitors fumagillin and ovalicin by methionine aminopeptidase 2. Proc Natl Acad Sci USA. 1998;95(26):15183–15188.
101. Hines J, Ju R, Dutschman GE, Cheng Y-C, Crews CM. Reversal of TNP-470-induced endothelial cell growth arrest by guanine and guanine nucleosides. J Pharmacol Exp Ther. 2010;334(3):729–738. doi:10.1124/jpet.110.169110.
102. Olmos D, Postel-Vinay S, Molife LR, et al. Safety, pharmacokinetics, and preliminary activity of the anti-IGF-1R antibody figitumumab (CP-751,871) in patients with sarcoma and Ewing’s sarcoma: a phase 1 expansion cohort study. Lancet Oncol. 2010;11(2):129–135. doi:10.1016/S1470-2045(09)70354-7.
103. Haluska P, Worden F, Olmos D, et al. Safety, tolerability, and pharmacokinetics of the anti-IGF-1R monoclonal antibody figitumumab in patients with refractory adrenocortical carcinoma. Cancer Chemother Pharmacol. 2010;65(4):765–773. doi:10.1007/s00280-009-1083-9.
104. Nijkamp MW, van der Bilt JDW, de Bruijn MT, et al. Accelerated Perinecrotic Outgrowth of Colorectal Liver Metastases Following Radiofrequency Ablation is a Hypoxia-Driven Phenomenon. Annals of Surgery. 2009;249(5):814–823. doi:10.1097/SLA.0b013e3181a38ef5.
105. Yan TD. Systematic Review on the Efficacy of Cytoreductive Surgery Combined With Perioperative Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis From Colorectal Carcinoma. Journal of Clinical Oncology. 2006;24(24):4011–4019. doi:10.1200/JCO.2006.07.1142.
106. van Dam GM, Themelis G, Crane LMA, et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-α targeting: first in-human results. Nature Medicine. 2011:1–6. doi:10.1038/nm.2472.
107. Van der Speeten K, Stuart OA, Chang D, Mahteme H, Sugarbaker PH. Changes induced by surgical and clinical factors in the pharmacology of intraperitoneal mitomycin C in 145 patients with peritoneal carcinomatosis. Cancer Chemother Pharmacol. 2011;68(1):147–156. doi:10.1007/s00280-010-1460-4.
108. De Roock MD W, De Vriendt MSc V, MD NN, MD PFC, MD PST. KRAS, BRAF, PIK3CA, and PTEN mutations: implications for targeted therapies in metastatic colorectal cancer. Lancet Oncology. 2011;12(6):594–603. doi:10.1016/S1470-2045(10)70209-6.
109. Prahallad A, Sun C, Huang S, et al. Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feedback activation of EGFR. Nature. 2012;483(7387):100–103. doi:10.1038/nature10868.


Chapter 5Adhesion molecules in peritoneal
metastases of colorectal cancer:Function, prognostic relevance
and therapeutic options
N.R. Sluiter
E.M.V. de Cuba
R. Kwakman
G. Kazemier
G.A. Meijer
E.A. te Velde
Accepted Clin Exp Metastasis April 2016

Chapter 5 | Adhesion molecules in PM of CRC
84
Abstract
Background: Peritoneal dissemination is diagnosed in 10-25% of colorectal cancer (CRC) patients. Selected patients are treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC). For these patients, earlier diagnosis, optimised selection criteria and a personalised approach are warranted. Biomarkers could play a crucial role here. However, little is known about possible candidates. Considering tumour cell adhesion as a key step in peritoneal dissemination, we aim to provide an overview of the functional importance of adhesion molecules in peritoneal dissemination and discuss the prognostic, diagnostic and therapeutic options of these candidate biomarkers.
Methods: A systematic literature search was conducted according to the PRISMA guidelines.
Results: In 132 in vitro, ex vivo and in vivo studies published between 1995 and 2013, we identified twelve possibly relevant adhesion molecules in various cancers that disseminate peritoneally. The most studied molecules in tumour cell adhesion are integrin α2β1, CD44s and MUC16. Furthermore, L1CAM, EpCAM, MUC1, sLex and Lex, chemokine receptors, Betaig-H3 and uPAR might be of clinical importance. ICAM1 was found to be less relevant in tumour cell adhesion in the context of peritoneal metastases.
Conclusions: Based on currently available data, sLea and MUC16 are the most promising prognostic biomarkers for colorectal peritoneal metastases that may help improve patient selection. Comparing these results to literature on adhesion molecules in haematogenous spread, we propose that haematogenous and transcoelomic spread differ in respect to several adhesion molecules. However, our extensive assessment of available literature reveals that knowledge on metastasis-specific genes and their possible candidates is far from complete.
Abbreviations: CRC (colorectal carcinoma), PM (peritoneal metastases), PMP (Pseudomyxoma peritonei), ECM (extracellular matrix), VCAM1 (vascular Cell Adhesion Molecule), ICAM1 (Intercellular Adhesion Molecule), L1CAM (L1 Cell Adhesion Molecule), sLea (sialyl Lewis a), Lex (Lewis x), sLex (sialyl Lewis x), MUC16 (mucin 16), MUC1 (mucin 1), CXCR4 (chemokine (C-X-C) motif receptor 4), CX3CL1 (chemokine (C-X3-C motif) ligand 1), EpCAM (Epithelial Cell Adhesion Molecule), beta ig-h3 (transforming growth factor beta induced gene-h3), uPAR (urokinase receptor)

Adhesion molecules in PM of CRC | Chapter 5
85
5
Introduction
Colorectal carcinoma (CRC) is the third most common cancer worldwide [1]. Approximately half of CRC patients develop distant metastasis, mainly through haematogenous dissemination to the liver [2,3]. Ten to 25% of CRC patients eventually develop peritoneal metastases (PM) [3,4] and in up to 25% of these patients the peritoneum is the only site of metastasis [4,5]. Typically, untreated PM are associated with poor survival rates, even when treated with modern systemic chemotherapy [6-8].
Macroscopic complete cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) is the preferred therapeutic strategy for patients with isolated PM [9,10], resulting in a five-year survival rate equal to that of patients undergoing resection for colorectal liver metastases (35–45%) [11,12] and a median survival of 33 months [6,13,14].
Despite the success of CRS and HIPEC, this treatment has morbidity and mortality rates of 15-34% and 5% respectively [5,6,11,15]. Therefore, selection of those patients that will benefit most from this treatment is of utmost importance. Other challenges in this field are earlier diagnosis and a more personalised approach, indicating that the choice of treatment should depend on a cancer’s specific biology instead of a ‘one size fits all’ approach [16]. Based on the hypothesis that the clinical behaviour of PM in CRC is dictated by biological mechanisms, read-outs of biological information (i.e., biomarkers) are very promising aids in addressing these clinical needs.
More specifically, understanding molecular mechanisms entails knowledge on molecules contributing to peritoneal dissemination. Peritoneal dissemination is considered to be a multi-step process in which tumour cells must detach from their primary tumour, gain motility and evade anoikis. Once a viable, free cancer cell is present in the peritoneal cavity, adherence to the peritoneal surface is required in order to ultimately invade the peritoneum, proliferate and form PM [16].
Accordingly, the presence of free-floating cancer cells in the peritoneal cavity is known to increase the risk of peritoneal dissemination [9, 7-20]. Hence, exfoliation of cancer cells into the peritoneal cavity might lead to PM formation in patients presenting with CRC growing through the serosa (T4 stage) [9,21,22]. Also patients undergoing abdominal surgery have an increased risk of PM formation, possibly through the combination of surgery-induced tumour spill and upregulation of adhesion molecules due to post-operative inflammation [9,20,23]. Thus, in several groups of patients, tumour cell adhesion to the

Chapter 5 | Adhesion molecules in PM of CRC
86
peritoneum appears to be pivotal in peritoneal dissemination. Molecules responsible for adhesion might therefore be promising biomarkers that can be used in diagnosis, prognosis and therapy of PM. Considering tumour cell adhesion as a key step in the formation of PM [16,24], we aimed to provide an overview of the functional importance of several attachment markers and to subsequently evaluate their roles in diagnosis, prognosis and therapy.
Methods
Literature search
A systematic literature search was conducted using the PubMed database of the U.S. National library of Medicine (Medline and pre-Medline). Table 1 shows the breakdown of search terms and Boolean combinations.
Table 1: Search strategy
Cancer types Peritoneal metastases Adhesion molecules
Cancer AND AND
Carcinoma AND Peritoneal Attachment
Colorectal Peritoneum Adherence
Colon Mesothelium AND Adhesion AND
Rectal Metastas* Molecule*
Gastric Peritoneal carcinomatosis Cell adhesion molecules*
Pancreas Pseudomyxoma Peritonei* Cell adhesion*
Pancreatic Peritoneal neoplasms/secondary*
Pseudomyxoma peritonei
ORColorectal neoplasms* Stomach neoplasms*Pancreatic neoplasms*Ovarian neoplasms*

Adhesion molecules in PM of CRC | Chapter 5
87
5
Inclusion- and exclusion criteria
All full-text papers, in English, published between January 1995 and January 2013 were considered in order to identify as many important adhesion molecules as possible. For this purpose, in vitro, ex vivo and in vivo studies on PM from colorectal, ovarian, gastric and pancreatic cancer as well as pseudomyxoma peritonei (PMP) were assessed. No reviews and case-reports were included. Other papers were incorporated by manually cross-referencing from publications retrieved in the initial search.
An additional review was conducted when deemed necessary. When studies overlapped or were duplicated, the articles with the most complete data on tumour cell adhesion to the peritoneum were retained. Figure 1 depicts the literature search and the selection process.
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
For more information, visit www.prisma-‐statement.org.
PRISMA 2009 Flow Diagram
Records identified through database searching
(n = 2783)
Scre
enin
g In
clude
d El
igib
ility
Id
entif
icatio
n Additional records identified through other sources
(n = 43)
Records after duplicates removed (n = 2825)
Records screened (n = 2825)
Records excluded (n = 2599)
• Articles deal neither with PM nor with adhesion
Full-‐text articles assessed
for eligibility (n = 226)
Full-‐text articles excluded (n = 94)
• No PM (44) • No adhesion (27) • No separate
analyses in patients with PM (13)
• Population with PM too small (3)
• Other types of cancer (1)
• Molecule does not contribute to PM formation (1)
• Double publication (4)
• No full-‐text article available (1)
Studies included in qualitative synthesis
(n = 132)
Figure 1: PRISMA flow chart for inclusion of the studies

Chapter 5 | Adhesion molecules in PM of CRC
88
Results
The key mechanism in PM formation is adherence of malignant cells to the peritoneal surface. Figure 2 illustrates the main interactions responsible for this process. Below, the functional and clinical importance of the adhesion molecules will be discussed.
Integrins a
Integrins a
Sialophorin c
L1CAM d
MUC16 e
CX3CR1 f
uPAR g
Le x hCD44 b
Laminin, fibronectin
, vitro
nectin, co
llagen I and IV
Hyaluronate
ICAM1 and VCAM1
ICAM1Neuropilin
-1
Mesothelin
CX3CL1
Vitronectin
E-selectin
Mesothelialcell
Adhering cancer cell
Figure 2: Adhesive interactions mediating tumour cell adhesion to the peritoneum. a: especially a2b1 expressed on colorectal [49], ovarian [34-42;144], gastric [28;29;31;46;145] and pancreatic [30;50;146] cancer cells; b: especially CD44 and CD44s expressed on colorectal [64] , ovarian [27;35;66-68;76;77;91], gastric [29;78] and pancreatic [30] cancer cells; c: expressed on colorectal, ovarian and pancreatic cancer cells [96]; d: expressed on ovarian cancer cells [99-101]; e: expressed on ovarian [94;123;124] and pancreatic [123] cancer cells; f: expressed on ovarian cancer cells [140]; g: expressed on ovarian cancer cells [58]; h: expressed on ovarian cancer cells [94;106].

Adhesion molecules in PM of CRC | Chapter 5
89
5
Integrins and integrin ligands
IntegrinsIntegrins belong to the superfamily of cell adhesion receptors. This family consists of 24 members, each of which is a heterodimer composed of α and β subunits [25]. In particular, integrin β1 [26-30] and integrin α2 [26-29, 31, 32] were shown to be upregulated in cancer cells with high peritoneal seeding potential. Multiple in vitro and ex vivo blocking experiments with ovarian [33-42], gastric [28, 31, 43-45], colon [46] and pancreatic [29, 47] cancer cells further endorse the roles of integrin α2β1 in cancer cell attachment to the peritoneum. Besides mediating adhesion of free-floating tumour cells, α2β1 might also be important in the adhesion of ovarian cancer cell aggregates (i.e. spheroids) to the peritoneum, in this way promoting PM formation [40, 41].
The above-mentioned studies not only support the role of integrin α2β1 in tumour cell attachment to the peritoneum, but also suggest that integrin blocking might be a useful strategy for prevention and treatment of PM. In vivo studies suggested a role for anti-integrin β1 antibodies in prevention of colorectal [46], gastric [27, 45] and pancreatic [47] tumour cell adhesion to (traumatised) peritoneum. Furthermore, the NF-kb inhibitor dehydroxymethylepoxyquinomicin (DHMEQ) reduced integrin β1 and α2 expression and was effective, both in vitro and in vivo, in preventing PM formation from gastric cancer [48]. For this purpose, other compounds that diminish integrin β1 expression, such as phospholipids [49], endostatin and simvastatin [42, 50] might be effective as well and interesting to pursue further.
Although some studies describe a less prominent role for integrin β1 [39, 52, 53] in PM formation, the majority of published literature showed the opposite. Literature on several other subunits only concerns their roles in vitro [34, 39-41, 47, 53, 54]. Their roles in vivo, therefore, remain unclear.
Integrin ligandsMultiple in vitro studies have indicated that the main mesothelial ligands participating in the interaction with integrins are the ECM components vitronectin [39, 47, 53, 55, 56], fibronectin [27, 30, 34, 40, 41, 45], laminin [27, 30, 34, 40, 41, 44, 45, 57, 58] and collagen I and IV [27, 30, 34, 40, 41, 45]. These ECM components might serve as treatment targets as well, since blocking them with antibodies and peptide sequences can reduce tumour cell adhesion. For example, the fibronectin amino acid sequence RGDS and the laminin sequence YIGSR inhibited in vitro and in vivo peritoneal dissemination from gastric and ovarian cancer [25, 58, 59]. Another possible therapeutic option in gastric cancer is coupling of Adriamycin to the laminin-5 peptide sequence SWKLPPS, as it increased its in vitro anticancer activity [58].

Chapter 5 | Adhesion molecules in PM of CRC
90
Proteoglycans
CD44The CD44 molecule is a cell-surface proteoglycan participating in cell-cell interaction, cell adhesion and cell migration [60]. In particular, CD44 isoforms originating from alternative splicing are thought to be important in tumour metastasis. The molecule is expressed on mesothelial cells and several types of cancer cells (Fig. 1). Its overexpression in gastric [28], ovarian [26] and in pancreatic [61, 62] cancer with high peritoneal seeding potential indicates a putative role for CD44 in PM formation. In vitro and ex vivo blocking experiments in several types of cancer illustrated the role of CD44 as adhesion molecule in PM formation [46, 61-67] and particularly indicated a role for the CD44s splice variant [28, 30, 68]. Accordingly, CD44 and CD44s mediated adhesion might partially be responsible for augmented cancer cell adhesion during post-operative inflammatory conditions. During this response, reactive oxygen species (ROS) [69, 70] and cytokines, for example TGF-β1, IL-1b and TNF-a [69, 71], are generated that upregulate CD44 expression and may also be responsible for the expression of other adhesion molecules [67].
Due to its suggested function in PM, CD44s is a theoretically attractive therapeutic target. In vivo blocking of this molecule prevented PM in ovarian, gastric and pancreatic cancer [28, 30, 59, 66]. Other molecules contributing to CD44 mediated cell adhesion might also serve as therapeutic targets, e.g. urokinase plasminogen activator (uPA), multidrug resistance 1 polypeptide (MDR1) and multidrug resistance protein 2 (MRP2) [72]. A third option is inhibiting CD44 glycolysation, since this process is possibly involved in CD44 mediated adhesion [64]. The CD44s splice variant has, despite its role in PM, an uncertain prognostic and diagnostic value [73-77].
HyaluronanConcluding from in vitro, ex vivo and in vivo studies, the main CD44 ligand of interest is the ECM proteoglycan hyaluronan [28, 61, 63, 73, 78]. Since both tumour promoting and tumour repressing effects were reported after intraperitoneal hyaluronan application [79-81], its therapeutic value is controversial. Intraperitoneal application of the hyaluronan-degrading enzyme hyaluronidase, however, does yield promising in vitro results [28, 34, 61, 63]. Hyaluronidase possibly acts by degradation of mesothelial-associated hyaluronan, thereby preventing hyaluronan from interacting with CD44 on tumour cells. Another strategy is improving chemotherapeutic agent delivery to malignant cells by coupling them to hyaluronan. In vivo, promising results were seen for intraperitoneal use of hyaluronan bound cisplatin [82] and hyaluronate (ONCOFID-P) [83] bound to paclitaxel in ovarian cancer and for hyaluronan (ONCOFID-S) bound to campthotecin (SN38) in CRC [84]. Lastly, in vitro and in vivo experiments indicated a possible role for adhesion barriers, such as Seprafilm and Hyalurobarrier, in inhibiting peritoneal dissemination [80, 85-87].

Adhesion molecules in PM of CRC | Chapter 5
91
5
Other proteoglycansSeveral other proteoglycans have been described in tumour cell adhesion to the peritoneum. The proteoglycans syndecan-1, syndecan-2, syndecan-4, glypican-1 and glypican-3 were upregulated in gastric cancer with high in vitro and in vivo peritoneal seeding potential [88], suggesting a role for these molecules in peritoneal dissemination. Considering that several compounds blocking heparan sulfate and chondroitin sulfate proteoglycans, such as heparin, heparin sulfate, dermatan sulfate, chondroitin glycosaminoglycans, heparitinase, chondroitinase ABC, or methylumbelliferyl xyloside, inhibit ovarian [27, 28, 53, 88] and colorectal [89] cancer cell adhesion to ECM components, blocking these proteoglycans could be a promising therapeutic option.
Immunoglobulin superfamily
The immunoglobulin superfamily is a large group of cell adhesion proteins, which include vascular cell adhesion molecule 1 (VCAM 1), intercellular adhesion molecule 1 (ICAM 1) and L1 cell adhesion molecule (L1CAM) [2, 90].
ICAM1ICAM1 is a cell surface molecule typically expressed on endothelial cells, cells of the immune system, cancer cells [42, 67, 69, 71, 91, 92] and mesothelial cells [67, 69-71, 91, 92]. Ziprin et al. (2004) [93] demonstrated in vitro tumour cell adhesion to the peritoneum to be mediated by the interaction between mesothelial ICAM1 and CD43 (sialophorin) on colorectal, ovarian and pancreatic cancer cells. This interaction might be important under postoperative inflammatory conditions, as the inflammatory mediators TNFα [67, 69, 71, 92], IL-1α [69], IL-1β [69], IL-6 [67] and reactive oxygen species (ROS) [71] enhanced ICAM1 expression and stimulated PM formation. Thus, theoretically, anti-ICAM1 antibodies [42, 67] or ICAM1 downregulation with heparin [92] and Simvastatin treatment [42] may be used in prevention of PM under inflammatory conditions. However, several in vitro studies on the role of ICAM1 as an adhesion molecule in PM did not show reproducible findings [42, 67, 71, 92]. Surprisingly, an in vivo study in gastric cancer even indicated that ICAM1 possibly inhibits PM formation due to ICAM1/LFA1 mediated mononuclear cell recruitment [94]. These contradictory findings make ICAM1 a dubious therapeutic target.
VCAM1The membrane protein VCAM1 mediates leukocyte-endothelial cell adhesion and signal transduction [95]. The mesothelial VCAM1 is possibly responsible for tumour cell adhesion by interacting with integrin α1β1 and α4β7 on tumour cells [91]. Enhanced VCAM1 expression induced by TNF-α, ILβ [69, 71] and ROS [71] might contribute to the

Chapter 5 | Adhesion molecules in PM of CRC
92
increased risk of PM formation after surgery. Accordingly, downregulating this molecule with anti-VCAM1 antibodies [33, 42, 70] or simvastatin [41] might prevent peritoneal dissemination.
L1CAML1CAM is described in various processes contributing to tumour progression, such as differentiation, proliferation, migration, invasion and tumour cell adhesion [96]. Its upregulation on ovarian cancer cells with high peritoneal seeding potential indicates a role for L1CAM in PM formation. In this process, as suggested by in vitro and in vivo ovarian cancer experiments, it probably mediates adhesion to the peritoneum by interacting with mesothelial neuropilin 1 (NRP1) [97]. Although L1CAM has not yet been proven to be valuable in the prognostic and diagnostic field [98], several therapeutic strategies targeting this molecule might be promising. One option might be antibody treatment, which reduced in vivo PM formation from ovarian cancer without producing side effects [96]. Another in vivo ovarian cancer study indicated possible therapeutic relevance for radioimmunotherapy combining anti-L1CAM antibodies (chCE7 and L1-11A) with 67CU-radiotherapy [99].
Blood group antigen proteins
Several blood group antigens and related structures are expressed on tumour cells [28, 30, 100-102], including sialyl Lewis a (sLea, a blood group antigen), Lewis x and sialyl Lewis x (Lex and sLex, two blood group antigen related structures). However, only Lex [91, 103] and sLex [28, 30, 33, 104] appear to mediate tumour cell adhesion by interacting with mesothelial E-selectin [104]. Although in vitro and in vivo antibody experiments made the contribution of sLea unlikely [28, 30, 33; 100], in vivo PM formation from pancreatic cancer was inhibited after decreasing sLex and sLea biosynthesis by blocking fucosyltransferase 3 (FUT3) [105].
Despite its debatable role in tumour cell adhesion to the peritoneum, sLea detection using immunohistochemistry [102], immunocytology [101] or immunoassays in serum [106] correlated to the presence of PM, peritoneal recurrence [107, 108] and poor prognosis [101, 106-110]. In the diagnostic and prognostic field, especially serum and peritoneal lavage levels of CA19-9, a monoclonal antibody against sLea, were shown to be predictive. However, due to its low sensitivity and contradictory results in patients with gastric cancer, CRC and PMP [77, 101, 103, 110-115], CA19-9 is not yet qualified for clinical use as a single marker. Nevertheless, CA19-9 levels are possibly valuable in combination with other markers, for example CEA [116-118].

Adhesion molecules in PM of CRC | Chapter 5
93
5
Mucins
Members of the mucin family are either present as secreted or as transmembrane proteins. Both forms are believed to be involved in inflammation and cancer [119]. When it comes to peritoneal spread, Mucin 16 (MUC16) is considered the most important member of this family. In vitro and in vivo studies suggested that cancer cell adhesion to the peritoneum partly relies on the interaction between MUC16 on ovarian cancer cells and mesothelin on mesothelial cells [120-124]. This interaction is probably mediated by the N-linked oligosaccharides of MUC16. Theoretically, blocking these oligosaccharides with lectins is an attractive therapeutic option [121]. In diagnosing PM, preoperative MUC16 serum levels in gastric cancer patients showed sensitivities ranging from 38,6% to 55% and specificities between 93,9% and 100% [110-113, 125, 126]. However, the prognostic value of MUC16 remains inconclusive [78, 125-127].
MUC1 is another mucin described in PM and is expressed on cancer cells [128-131]. It is questionable as to whether this mucin has a role in the attachment phase, since it does not bind mesothelin [120]. Accordingly, the role of MUC1 in clinical settings is so far not convincing [131, 132].
Epithelial cell adhesion molecule (EPCAM)
EpCAM is a homotypic calcium independent cell adhesion molecule not belonging to one of the previously mentioned groups of molecules [133]. Its expression on cancer cells [98] and its upregulation in PM from gastric cancer [134] suggest a function for this molecule in PM. Its role as adhesion molecule in PM, however, was not confirmed by in vivo antibody experiments in ovarian cancer [98].
In contrast, studies on the therapeutic value of EpCAM were promising, indicating that this molecule might promote peritoneal dissemination through other functions. This is illustrated by treatment with the trifunctional antibody catumaxomab (anti-EpCAM x anti-CD3) that eradicated PM from ovarian cancer in mice by reactivating tumour-resident T-cells [135]. Catumaxomab was also investigated as monotherapy in a phase I/II study, in which this compound was shown to be relatively safe and possibly effective in gastric, colorectal and pancreatic cancer [136]. Concerning its possible diagnostic and prognostic value, data on EpCAM is inconsistent [101, 137].
Other molecules of interest
Several less frequently studied molecules possibly contribute to tumour cell adhesion as well. These are chemokine receptors, transforming growth factor beta induced gene-h3

Chapter 5 | Adhesion molecules in PM of CRC
94
(beta ig-h3) and urokinase receptor (uPAR). Although literature on the molecules described in this section suggest that they contribute to cancer cell adhesion to the peritoneum, further research should confirm this assumption.
The chemokine (C-X3-C motif) receptor 1 (CX3CR1) is expressed by ovarian cancer cells and was shown to mediate in vitro tumour cell adhesion to mesothelial cells by interacting with mesothelial chemokine (C-X3-C motif) ligand 1 (CX3CL1) [138]. Expression of another chemokine, chemokine (C-X-C) motif receptor 4 (CXCR4), is expressed on both mesothelial and cancer cells and correlates to worse survival rates in ovarian cancer patients. In vitro and in vivo blocking of CXCR4 with its antagonist ADM3100 was thereby shown to inhibit PM formation [137].
Peritoneal cavityFree floating cancer cell
Integrin α2β1
EpCAMCD44
CD44
Peritoneal metastasis
Peritoneal surface
1
2
3
4 5
Figure 3: Most promising therapeutic options in prevention (left) and treatment (right) of PM: (1) anti-integrin α2β1 antibodies; (2) peptide sequences; (3) anti-CD44 antibodies; (4) hyaluronan bound to cytostatic agents; (5) catumaxomab, a trifunctional antibody with binding sites for EpCAM, T-cells and accessory cells.
uPAR might also be relevant in PM formation and is detected at the interaction sites of ovarian carcinoma cells and mesothelial cells. In vitro experiments indicated that uPAR mediates tumour cell adhesion by interacting with mesothelial vitronectin [55].

Adhesion molecules in PM of CRC | Chapter 5
95
5
Table 2: Summary of targets with possible clinical implication in PM
Target in PM Prognostic relevance Diagnostic relevance Possible therapeutic implications
Integrins Yes:·Higher expression of
αvβ3 correlated to worse prognosis [30].
Not clear Promising:·Antibodies against integrin α2
and β1 and ECM components [26; 28; 30; 31; 33; 43; 46; 47; 49; 50; 58];
·Peptide sequences of ECM components [60; 62];
·NF-κb inhibitor (DHMEQ) [51]; ·Phospholipids [52]; ·Adriamycin bound to SWKLPPS,
intraperitoneal [61].CD44 Debatable [76; 78; 79] Yes:
·Higher CD44s expression correlated to worse survival [77; 78]
Promising:·Antibodies against CD44 and
CD44s [28; 30; 47; 62; 64; 66; 67; 69-71; 76];
·Hyaluronidase, intraperitoneal [28; 35; 66];
·Adhesion barriers [70; 80]; ·Cisplatin [85],
paclitaxel [86] or campthotecin [87] bound to hyaluronan.
VCAM1 Not clear Not clear Dubious, blocking VCAM1 leads theoretically to less PM [43; 73].
ICAM1 Not clear Not clear Dubious, blocking ICAM1 leads theoretically to less PM [33; 43; 70; 73; 95].
L1CAM No [99] Dubious [99] Highly experimental:·Antibodies [101]; · 67CU-radiotherapy combined with
antibodies, intraperitoneal [102].Blood group
antigensYes:·CA19-9 levels in serum
and peritoneal fluid [104; 105; 109; 110; 114; 115; 118-121]
Yes:·CA19-9 levels in serum
and peritoneal fluid [80; 104; 109; 110; 112; 113; 117]
Highly experimental:·Antibodies against Lex [106]; ·Blocking FUT3 [108].
MUC16 Yes:·MUC16 levels in serum
and peritoneal lavage [113; 114; 128; 129];
·MUC1 PT-PCR [133].
Dubious [80; 128-130] Highly experimental:·Antibodies [125]; ·Blocking mesothelin
[123; 124; 126]; ·Anti-MUC1 antibody (C595)
combined with docetaxel [131].EpCAM No [104] Dubious [104; 141] Promising:
·Bispecific antibodies EpCAM/CD3 [138]
·Catuxomab monotherapy, intraperitoneal [139]
Chemokine receptors
Not clear Not clear Highly experimental: ·Antibodies against CX3CR1 and
CX3CL1 (162); ·ADM3100 [142].
uPAR Not clear Not clear Highly experimental:·Antibodies [58].

Chapter 5 | Adhesion molecules in PM of CRC
96
Lastly, beta ig-h3 is an adhesion molecule expressed on mesothelial cells. Upregulation is associated with increased in vitro gastric cancer cell adhesion and the presence of PM [139], suggesting a role for this molecule in PM.
Discussion
The present study was designed to identify molecules from literature that mediate tumour cell adhesion to the peritoneum and to evaluate their roles in diagnosis, prognosis and therapy of PM. Targeting adhesion molecules may not only prevent tumour cell adhesion and eventually tumour outgrowth in patients at high risk for peritoneal dissemination but the expression of adhesion molecules on tumour cells also allows us to use therapies targeting adhesion molecules in existing peritoneal carcinomatosis (Table 2, figure 3) . Hence, advancing studies on the therapeutic and diagnostic value of adhesion molecules seems a very promising and rational way for optimising and personalising treatment of patients presenting with peritoneally metastasised CRC.
In PM formation, the roles of CD44s, integrin α2β1 and MUC16 appeared to be well investigated. Due to their in vitro and ex vivo adhesive functions, L1CAM, proteoglycans, Betaig-H3 and uPAR might contribute to peritoneal dissemination as well. However, their exact functions and clinical possibilities have to be elucidated. Accordingly, in vitro, ex vivo and in vivo antibody experiments should be developed to assess their adhesive potential. Furthermore, while two systematic reviews support our findings on most adhesion molecules [16, 144], most literature regarding the involvement of adhesion molecules in PM yields contradictory findings. This may be related to heterogeneity of published methods and varying sample sizes. In diagnosis and prognosis of PM, detection of MUC16 and blood group antigens might be useful. Prior to clinical implementation, however, extensive validation of these molecules is necessary. Validation in well-defined patient cohorts is also required for EpCAM, integrin α2β1 and CD44, molecules that have emerged as possibly useful therapeutic targets (table 2, figure 3). Remarkably, while EpCAM showed therapeutic significance in ex vivo and in vivo experiments, its role in in vitro adhesion to the peritoneum was not confirmed. This discrepancy might be attributable to the finding that EpCAM carries out multiple functions, including cell adhesion, cellular signaling, migration, proliferation and differentiation [133, 145-147]. As such, the combination of these mechanisms, as opposed to only a single function (i.e. adhesion), might be of greater importance in promoting PM. The role of adhesion in haematogenous metastases has been described in several literature studies. Bird et al. (2006) [2] focused on the development of liver metastases from CRC. In both haematogenous spread and spread across the peritoneal cavity –i.e. transcoelomic

Adhesion molecules in PM of CRC | Chapter 5
97
5
spread, cancer cells first must detach from the primary tumour to enter the circulation or the peritoneal cavity respectively. Cancer cells, carried by the blood stream or floating in the peritoneal cavity must evade immune defences in order to reach their host organ. At the site of the host organ, adhesive interactions between the organ and cancer cells are required for the development of a metastasis [2, 16, 144]. Adhesion molecules responsible for these interactions in liver dissemination were found to be CD44, blood group antigens, mucins, E-selectin and carcinoembryonic antigen (CEA) [2]. This review, however, did not identify blood group antigens, E-selectin and CEA to be important in peritoneal dissemination. Additionally, L1CAM, proteoglycans, Betaig-H3 and uPAR might contribute to PM formation, although these molecules were not described in the formation of liver metastases. Thus, we propose that haematogenous and transcoelomic spread differ in respect to several adhesion molecules.
Several studies stress the importance of new molecular targets to improve therapy and selection of patients with PM of CRC [8, 13, 14]. The adhesion molecules EpCAM, α2β1 and CD44s were seen to mediate tumour cell adhesion to the peritoneum and might be particularly useful in the prevention of minimal residual disease in high-risk patients, such as patients with T4 colon tumours [21, 22]. In addition, blocking tumour cell adhesion in the perioperative period may be effective in preventing peritoneal dissemination [23]. A preventive HIPEC procedure might possibly be of additional value in high stage CRC [13]. With respect to a more personalised approach, blocking specific interactions between the mesothelial lining and tumour cell could be of even greater benefit in patients at high risk of peritoneal tumour spread.
This extensive assessment of available literature reveals that knowledge on metastasis-specific genes and their possible clinical implications is far from complete. An ‘–omics’ approach, synchronously assessing multiple biomarkers, might help to identify more biomarker candidates. The recently identified biomarkers may possibly be relevant in the therapeutic field (α2β1, CD44s and EpCAM) and in the diagnostic and prognostic field (MUC16 and blood group antigens). However, these biomarkers require independent validation in order to increase the reproducibility of studies –a common problem in the area of genomics and proteomics [148]. Accordingly, their therapeutic, diagnostic and prognostic value should be assessed in well-defined patient cohorts prior to clinical implementation. Ultimately, increasing reproducibility of genome-wide studies and extensive validation of possible biomarkers could lead to major advances in our understanding of metastasis-specific genes and their clinical possibilities. For CRC patients with PM, the gained knowledge on the diagnostic and therapeutic options of biomarkers will potentially lead to earlier diagnosis and a more personalised, or even preventive, approach and ultimately to better outcomes.

Chapter 5 | Adhesion molecules in PM of CRC
98
References1 Parkin DM, Bray F, Ferlay J, Pisani P (2005).
Global cancer statistics, 2002. CA Cancer J Clin 55(2):74-108.
2 Bird NC, Mangnall D, Majeed AW (2006). Biology of colorectal liver metastases: A review. J Surg Oncol 94(1):68-80.
3 Koppe MJ, Boerman OC, Oyen WJ, Bleichrodt RP (2006). Peritoneal carcinomatosis of colorectal origin: incidence and current treatment strategies. Ann Surg 243(2):212-22.
4 Jayne DG, Fook S, Loi C, Seow-Choen F (2002). Peritoneal carcinomatosis from colorectal cancer. Br J Surg 89(12):1545-50.
5 Maggiori L, Bretagnol F, Ferron M, Chevalier Y, Panis Y (2011). Laparoscopic colorectal anastomosis using the novel Chex((R)) circular stapler: a case-control study. Colorectal Dis 13(6):711-5.
6 Cao Y, Tan A, Gao F, Liu L, Liao C, Mo Z (2009). A meta-analysis of randomized controlled trials comparing chemotherapy plus bevacizumab with chemotherapy alone in metastatic colorectal cancer. Int J Colorectal Dis 24(6):677-85.
7 Klaver YL, Simkens LH, Lemmens VE, Koopman M, Teerenstra S, Bleichrodt RP, de Hingh IH, Punt CJ (2012). Outcomes of colorectal cancer patients with peritoneal carcinomatosis treated with chemotherapy with and without targeted therapy. Eur J Surg Oncol 38(7):617-23.
8 Franko J, Shi Q, Goldman CD, Pockaj BA, Nelson GD, Goldberg RM, Pitot HC, Grothey A, Alberts SR, Sargent DJ (2012). Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: a pooled analysis of north central cancer treatment group phase III trials N9741 and N9841. J Clin Oncol 30(3):263-7.
9 Sugarbaker PH (1995). Patient selection and treatment of peritoneal carcinomatosis from colorectal and appendiceal cancer. World J Surg 19(2):235-40.
10 Sugarbaker PH, Jablonski KA (1995). Prognostic features of 51 colorectal and 130 appendiceal cancer patients with peritoneal carcinomatosis treated by cytoreductive surgery and intraperitoneal chemotherapy. Ann Surg 221(2):124-32.
11 Verwaal VJ, van RS, de BE, van Sloothen GW, van TH, Boot H, Zoetmulder FA (2003). Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol 21(20):3737-43.
12 Verwaal VJ, Kusamura S, Baratti D, Deraco M (2008). The eligibility for local-regional treatment of peritoneal surface malignancy. J Surg Oncol 98(4):220-3.
13 Elias D, Gilly F, Boutitie F, Quenet F, Bereder JM, Mansvelt B, Lorimier G, Dube P, Glehen O (2010). Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol 28(1):63-8.
14 Kuijpers AM, Mirck B, Aalbers AG, Nienhuijs SW, de Hingh IH, Wiezer MJ, van RB, van Ginkel RJ, Havenga K, Bremers AJ, de Wilt JH, Te Velde EA, et al (2013). Cytoreduction and HIPEC in the Netherlands: nationwide long-term outcome following the Dutch protocol. Ann Surg Oncol 20(13):4224-30.
15 Verwaal VJ, Zoetmulder FA (2004). Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. Eur J Surg Oncol 30(3):280-5.
16 de Cuba EM, Kwakman R, van EM, Bosch LJ, Bonjer HJ, Meijer GA, Te Velde EA (2012). Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : future possibilities for personalised treatment by use of biomarkers. Virchows Arch 461(3):231-43.
17 Nakanishi H, Kodera Y, Yamamura Y, Ito S, Kato T, Ezaki T, Tatematsu M (2000). Rapid quantitative detection of carcinoembryonic antigen-expressing free tumor cells in the peritoneal cavity of gastric-cancer patients with real-time RT-PCR on the lightcycler. Int J Cancer 89(5):411-7.
18 Kanellos I, Demetriades H, Zintzaras E, Mandrali A, Mantzoros I, Betsis D (2003). Incidence and prognostic value of positive peritoneal cytology in colorectal cancer. Dis Colon Rectum 46(4):535-9.
19 Yamamoto S, Akasu T, Fujita S, Moriya Y (2003). Long-term prognostic value of conventional peritoneal cytology after curative resection for colorectal carcinoma. Jpn J Clin Oncol 33(1):33-7.
20 Takebayashi K, Murata S, Yamamoto H, Ishida M, Yamaguchi T, Kojima M, Shimizu T, Shiomi H, Sonoda H, Naka S, Mekata E, Okabe H, et al (2014). Surgery-induced peritoneal cancer cells in patients who have undergone curative gastrectomy for gastric cancer. Ann Surg Oncol 21(6):1991-7.

Adhesion molecules in PM of CRC | Chapter 5
99
5
21 Shepherd NA, Baxter KJ, Love SB (1997). The prognostic importance of peritoneal involvement in colonic cancer: a prospective evaluation. Gastroenterology 112(4):1096-102.
22 Hompes D, Tiek J, Wolthuis A, Fieuws S, Penninckx F, Van CE, D’Hoore A (2012). HIPEC in T4a colon cancer: a defendable treatment to improve oncologic outcome? Ann Oncol 23(12):3123-9.
23 van der Bij GJ, Oosterling SJ, Beelen RH, Meijer S, Coffey JC, van Egmond M (2009). The perioperative period is an underutilized window of therapeutic opportunity in patients with colorectal cancer. Ann Surg 249(5):727-34.
24 Hanahan D, Weinberg RA (2011). Hallmarks of cancer: the next generation. Cell 144(5):646-74.
25 Takada Y, Ye X, Simon S (2007). The integrins. Genome Biol 8(5):215.
26 Strobel T, Cannistra SA (1999). Beta1-integrins partly mediate binding of ovarian cancer cells to peritoneal mesothelium in vitro. Gynecol Oncol 73(3):362-7.
27 Casey RC, Oegema TRJ, Skubitz KM, Pambuccian SE, Grindle SM, Skubitz APN (2003). Cell membrane glycosylation mediates the adhesion, migration, and invasion of ovarian carcinoma cells. Clin Exp Metastasis 20(2):143-52.
28 Nakashio T, Narita T, Akiyama S, Kasai Y, Kondo K, Ito K, Takagi H, Kannagi R (1997). Adhesion molecules and TGF-beta1 are involved in the peritoneal dissemination of NUGC-4 human gastric cancer cells. Int J Cancer 70(5):612-8.
29 Nishii T, Yashiro M, Shinto O, Sawada T, Ohira M, Hirakawa K (2009). Cancer stem cell-like SP cells have a high adhesion ability to the peritoneum in gastric carcinoma. Cancer Sci 100(8):1397-402.
30 Hosono J, Narita T, Kimura N, Sato M, Nakashio T, Kasai Y, Nonami T, Nakao A, Takagi H, Kannagi R (1998). Involvement of adhesion molecules in metastasis of SW1990, human pancreatic cancer cells. J Surg Oncol 67(2):77-84.
31 Kawamura T, Endo Y, Yonemura Y, Nojima N, Fujita H, Fujimura T, Obata T, Yamaguchi T, Sasaki T (2001). Significance of integrin alpha2/beta1 in peritoneal dissemination of a human gastric cancer xenograft model. Int J Oncol 18(4):809-15.
32 Sakakura C, Hagiwara A, Nakanishi M, Shimomura K, Takagi T, Yasuoka R, Fujita Y, Abe T, Ichikawa Y, Takahashi S, Ishikawa T, Nishizuka I, et al. (2002). Differential gene expression profiles of gastric cancer cells established from primary tumour and malignant ascites. Br J Cancer 87(10):1153-61.
33 Kishikawa T, Sakamoto M, Ino Y, Kubushiro K, Nozawa S, Hirohashi S (1995). Two distinct patterns of peritoneal involvement shown by in vitro and in vivo ovarian cancer dissemination models. Invasion Metastasis 15(1-2):11-21.
34 Lessan K, Aguiar DJ, Oegema T, Siebenson L, Skubitz AP (1999). CD44 and beta1 integrin mediate ovarian carcinoma cell adhesion to peritoneal mesothelial cells. Am J Pathol 154(5):1525-37.
35 Moser TL, Pizzo SV, Bafetti LM, Fishman DA, Stack MS (1996). Evidence for preferential adhesion of ovarian epithelial carcinoma cells to type I collagen mediated by the alpha2beta1 integrin. Int J Cancer 67(5):695-701.
36 Matsuoka T, Yashiro M, Nishimura S, Inoue T, Fujihara T, Sawada T, Kato Y, Seki S, Hirakawa-YS Chung K (2000). Increased expression of alpha2beta1-integrin in the peritoneal dissemination of human gastric carcinoma. Int J Mol Med 5(1):21-5.
37 Fishman DA, Kearns A, Chilukuri K, Bafetti LM, O’Toole EA, Georgacopoulos J, Ravosa MJ, Stack MS (1998). Metastatic dissemination of human ovarian epithelial carcinoma is promoted by alpha2beta1-integrin-mediated interaction with type I collagen. Invasion Metastasis 18(1):15-26.
38 Buczek-Thomas JA, Chen N, Hasan T (1998). Integrin-mediated adhesion and signalling in ovarian cancer cells. Cell Signal 10(1):55-63.
39 Ahmed N, Riley C, Rice G, Quinn M (2005). Role of integrin receptors for fibronectin, collagen and laminin in the regulation of ovarian carcinoma functions in response to a matrix microenvironment. Clin Exp Metastasis 22(5):391-402.
40 Burleson KM, Casey RC, Skubitz KM, Pambuccian SE, Oegema TRJ, Skubitz APN (2004). Ovarian carcinoma ascites spheroids adhere to extracellular matrix components and mesothelial cell monolayers. Gynecol Oncol 93(1):170-81.
41 Casey RC, Burleson KM, Skubitz KM, Pambuccian SE, Oegema TRJ, Ruff LE, Skubitz AP (2001). Beta 1-integrins regulate the formation and adhesion of ovarian carcinoma multicellular spheroids. Am J Pathol 159(6):2071-80.

Chapter 5 | Adhesion molecules in PM of CRC
100
42 Wagner BJ, Lob S, Lindau D, Horzer H, Guckel B, Klein G, Glatzle J, Rammensee HG, Brucher BL, Konigsrainer A (2011). Simvastatin reduces tumor cell adhesion to human peritoneal mesothelial cells by decreased expression of VCAM-1 and beta1 integrin. Int J Oncol 39(6):1593-600.
43 Lin MT, Chang CC, Lin BR, Yang HY, Chu CY, Wu MH, Kuo ML (2007). Elevated expression of Cyr61 enhances peritoneal dissemination of gastric cancer cells through integrin alpha2beta1. J Biol Chem 282(47):34594-604.
44 Takatsuki H, Komatsu S, Sano R, Takada Y, Tsuji T (2004). Adhesion of gastric carcinoma cells to peritoneum mediated by alpha3beta1 integrin (VLA-3). Cancer Res 64(17):6065-70.
45 Nishimura S, Chung YS, Yashiro M, Inoue T, Sowa M (1996). Role of alpha 2 beta 1- and alpha 3 beta 1-integrin in the peritoneal implantation of scirrhous gastric carcinoma. Br J Cancer 74(9):1406-12.
46 Oosterling SJ, van der Bij GJ, Bogels M, ten Raa S, Post JA, Meijer GA, Beelen RHJ, van Egmond M (2008). Anti-beta1 integrin antibody reduces surgery-induced adhesion of colon carcinoma cells to traumatized peritoneal surfaces. Ann Surg 247(1):85-94.
47 Sawai H, Okada Y, Funahashi H, Matsuo Y, Takahashi H, Takeyama H, Manabe T (2006). Interleukin-1alpha enhances the aggressive behavior of pancreatic cancer cells by regulating the alpha6beta1-integrin and urokinase plasminogen activator receptor expression. BMC Cell Biol 7:8.
48 Mino K, Ozaki M, Nakanishi K, Haga S, Sato M, Kina M, Takahashi M, Takahashi N, Kataoka A, Yanagihara K, Ochiya T, Kamiyama T, et al. (2011). Inhibition of nuclear factor-kappaB suppresses peritoneal dissemination of gastric cancer by blocking cancer cell adhesion. Cancer Sci 102(5):1052-8.
49 Jansen M, Jansen PL, Otto J, Kirtil T, Neuss S, Treutner KH, Schumpelick V (2006). The inhibition of tumor cell adhesion on human mesothelial cells (HOMC) by phospholipids in vitro. Langenbecks Arch Surg 391(2):96-101
50 Yokoyama Y, Ramakrishnan S (2007). Binding of endostatin to human ovarian cancer cells inhibits cell attachment. Int J Cancer 121(11):2402-9.
51 Cannistra SA, Ottensmeier C, Niloff J, Orta B, DiCarlo J (1995). Expression and function of beta 1 and alpha v beta 3 integrins in ovarian cancer. Gynecol Oncol 58(2):216-25.
52 Maubant S, Cruet-Hennequart S, Dutoit S, Denoux Y, Crouet H, Henry-Amar M, Gauduchon P (2005). Expression of alpha V-associated integrin beta subunits in epithelial ovarian cancer and its relation to prognosis in patients treated with platinum-based regimens. J Mol Histol 36(1-2):119-29.
53 Kokenyesi R, Murray KP, Benshushan A, Huntley ED, Kao MS (2003). Invasion of interstitial matrix by a novel cell line from primary peritoneal carcinosarcoma, and by established ovarian carcinoma cell lines: role of cell-matrix adhesion molecules, proteinases, and E-cadherin expression. Gynecol Oncol 89(1):60-72.
54 Fukuda K, Saikawa Y, Yagi H, Wada N, Takahashi T, Kitagawa Y (2012). Role of integrin alpha1 subunits in gastric cancer patients with peritoneal dissemination. Mol Med Report 5(2):336-40.
55 Heyman L, Kellouche S, Fernandes J, Dutoit S, Poulain L, Carreiras F (2008). Vitronectin and its receptors partly mediate adhesion of ovarian cancer cells to peritoneal mesothelium in vitro. Tumour Biol 29(4):231-44.
56 Carreiras F, Lehmann M, Sichel F, Marvaldi J, Gauduchon P, Le Talaer JY (1995). Implication of the alpha v beta 3 integrin in the adhesion of the ovarian-adenocarcinoma cell line IGROV1. Int J Cancer 63(4):530-6.
57 Matsuoka T, Hirakawa K, Chung YS, Yashiro M, Nishimura S, Sawada T, Saiki I, Sowa M (1998). Adhesion polypeptides are useful for the prevention of peritoneal dissemination of gastric cancer. Clin Exp Metastasis 16(4):381-8.
58 Akita N, Maruta F, Seymour LW, Kerr DJ, Parker AL, Asai T, Oku N, Nakayama J, Miyagawa S (2006). Identification of oligopeptides binding to peritoneal tumors of gastric cancer. Cancer Sci 97(10):1075-81.
59 Hirabayashi Y, Yamaguchi K, Shiraishi N, Adachi Y, Saiki I, Kitano S (2004). Port-site metastasis after CO2 pneumoperitoneum: role of adhesion molecules and prevention with antiadhesion molecules. Surg Endosc 18(7):1113-7.
60 Aruffo A, Stamenkovic I, Melnick M, Underhill CB, Seed B (1990). CD44 is the principal cell surface receptor for hyaluronate. Cell 61(7):1303-13.
61 Harada N, Mizoi T, Kinouchi M, Hoshi K, Ishii S, Shiiba K, Sasaki I, Matsuno S (2001). Introduction of antisense CD44S CDNA down-regulates expression of overall CD44 isoforms and inhibits tumor growth and metastasis in highly metastatic colon carcinoma cells. Int J Cancer 91(1):67-75.

Adhesion molecules in PM of CRC | Chapter 5
101
5
62 Yeo TK, Nagy JA, Yeo KT, Dvorak HF, Toole BP (1996). Increased hyaluronan at sites of attachment to mesentery by CD44-positive mouse ovarian and breast tumor cells. Am J Pathol 148(6):1733-40.
63 Gardner MJ, Catterall JB, Jones LM, Turner GA (1996). Human ovarian tumour cells can bind hyaluronic acid via membrane CD44: a possible step in peritoneal metastasis. Clin Exp Metastasis 14(4):325-34.
64 Catterall JB, Jones LM, Turner GA (1999). Membrane protein glycosylation and CD44 content in the adhesion of human ovarian cancer cells to hyaluronan. Clin Exp Metastasis 17(7):583-91.
65 Li CZ, Liu B, Wen ZQ, Li HY (2008). Inhibition of CD44 expression by small interfering RNA to suppress the growth and metastasis of ovarian cancer cells in vitro and in vivo. Folia Biol (Praha) 54(6):180-6.
66 Strobel T, Swanson L, Cannistra SA (1997). In vivo inhibition of CD44 limits intra-abdominal spread of a human ovarian cancer xenograft in nude mice: a novel role for CD44 in the process of peritoneal implantation. Cancer Res 57(7):1228-32.
67 Ziprin P, Ridgway PF, Pfistermuller KLM, Peck DH, Darzi AW (2003). ICAM-1 mediated tumor-mesothelial cell adhesion is modulated by IL-6 and TNF-alpha: a potential mechanism by which surgical trauma increases peritoneal metastases. Cell Commun Adhes 10(3):141-54.
68 Cannistra SA, DeFranzo B, Niloff J, Ottensmeir C (1995). Functional heterogeneity of CD44 molecules in ovarian cancer cell lines. Clin Cancer Res 1(3):333-42.
69 van Grevenstein WMU, Hofland LJ, Jeekel J, van Eijck CHJ (2006). The expression of adhesion molecules and the influence of inflammatory cytokines on the adhesion of human pancreatic carcinoma cells to mesothelial monolayers. Pancreas 32(4):396-402.
70 ten Raa S, van Grevenstein HMU, ten Kate M, Mangundap KM, Hofland LJ, Jeekel H, Sluiter W, van Eijck CHJ (2007). The influence of reactive oxygen species on the adhesion of pancreatic carcinoma cells to the peritoneum. Cell Adh Migr 1(2):77-83.
71 Yu G, Tang B, Yu PW, Peng ZH, Qian F, Sun G (2010). Systemic and peritoneal inflammatory response after laparoscopic-assisted gastrectomy and the effect of inflammatory cytokines on adhesion of gastric cancer cells to peritoneal mesothelial cells. Surg Endosc 24(11):2860-70.
72 Chen H, Hao J, Wang L, Li Y (2009). Coexpression of invasive markers (uPA, CD44) and multiple drug-resistance proteins (MDR1, MRP2) is correlated with epithelial ovarian cancer progression. Br J Cancer 101(3):432-40.
73 Berner HS, Davidson B, Berner A, Risberg B, Kristensen GB, Trope CG, Van de Putte G, Nesland JM (2000). Expression of CD44 in effusions of patients diagnosed with serous ovarian carcinoma--diagnostic and prognostic implications. Clin Exp Metastasis 18(2):197-202.
74 Kayastha S, Freedman AN, Piver MS, Mukkamalla J, Romero-Guittierez M, Werness BA (1999). Expression of the hyaluronan receptor, CD44S, in epithelial ovarian cancer is an independent predictor of survival. Clin Cancer Res 5(5):1073-6.
75 Yamamichi K, Uehara Y, Kitamura N, Nakane Y, Hioki K (1998). Increased expression of CD44v6 mRNA significantly correlates with distant metastasis and poor prognosis in gastric cancer. Int J Cancer 79(3):256-62.
76 Sillanpaa S, Anttila MA, Voutilainen K, Tammi RH, Tammi MI, Saarikoski SV, Kosma VM (2003). CD44 expression indicates favorable prognosis in epithelial ovarian cancer. Clin Cancer Res 9(14):5318-24.
77 Baratti D, Kusamura S, Nonaka D, Langer M, Andreola S, Favaro M, Gavazzi C, Laterza B, Deraco M (2008). Pseudomyxoma peritonei: clinical pathological and biological prognostic factors in patients treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC). Ann Surg Oncol 15(2):526-34.
78 Catterall JB, Gardner MJ, Jones LM, Turner GA (1997). Binding of ovarian cancer cells to immobilized hyaluronic acid. Glycoconj J 14(7):867-9.
79 Yamaguchi K, Hirabayashi Y, Shiromizu A, Shiraishi N, Adachi Y, Kitano S (2001). Enhancement of port site metastasis by hyaluronic acid under CO2 pneumoperitoneum in a murine model. Surg Endosc 15(5):504-7.
80 Tan B, Wang JH, Wu QD, Kirwan WO, Redmond HP (2001). Sodium hyaluronate enhances colorectal tumour cell metastatic potential in vitro and in vivo. Br J Surg 88(2):246-50.
81 Jones LM, Gardner MJ, Catterall JB, Turner GA (1995). Hyaluronic acid secreted by mesothelial cells: a natural barrier to ovarian cancer cell adhesion. Clin Exp Metastasis 13(5):373-80.
82 Li SD, Howell SB. CD44-targeted microparticles for delivery of cisplatin to peritoneal metastases (2010). Mol Pharm 7(1):280-90.

Chapter 5 | Adhesion molecules in PM of CRC
102
83 Banzato A, Bobisse S, Rondina M, Renier D, Bettella F, Esposito G, Quintieri L, Melendez-Alafort L, Mazzi U, Zanovello P, Rosato A (2008). A paclitaxel-hyaluronan bioconjugate targeting ovarian cancer affords a potent in vivo therapeutic activity. Clin Cancer Res 14(11):3598-606.
84 Serafino A, Zonfrillo M, Andreola F, Psaila R, Mercuri L, Moroni N, Renier D, Campisi M, Secchieri C, Pierimarchi P (2011). CD44-targeting for antitumor drug delivery: a new SN-38-hyaluronan bioconjugate for locoregional treatment of peritoneal carcinomatosis. Curr Cancer Drug Targets 11(5):572-85.
85 Hubbard SC, Burns JW (2002). Effects of a hyaluronan-based membrane (Seprafilm) on intraperitoneally disseminated human colon cancer cell growth in a nude mouse model. Dis Colon Rectum 45(3):334-41.
86 Pucciarelli S, Codello L, Rosato A, Del Bianco P, Vecchiato G, Lise M (2003). Effect of antiadhesive agents on peritoneal carcinomatosis in an experimental model. Br J Surg 90(1):66-71.
87 Haverlag R, van Rossen ME, van den Tol MP, Bonthuis F, Marquet RL, Jeekel J (1999). Hyaluronate-based coating solution for prevention of surgical adhesions has no major effect on adhesion and growth of intraperitoneal tumour cells. Eur J Surg 165(8):791-5.
88 Kokenyesi R (2001). Ovarian carcinoma cells synthesize both chondroitin sulfate and heparan sulfate cell surface proteoglycans that mediate cell adhesion to interstitial matrix. J Cell Biochem 83(2):259-70.
89 Jacobi CA, Ordemann J, Bohm B, Zieren HU, Sabat R, Muller JM (1997). Inhibition of peritoneal tumor cell growth and implantation in laparoscopic surgery in a rat model. Am J Surg 174(3):359-63.
90 Paschos KA, Canovas D, Bird NC (2009). The role of cell adhesion molecules in the progression of colorectal cancer and the development of liver metastasis. Cell Signal 21(5):665-74.
91 Gardner MJ, Jones LM, Catterall JB, Turner GA (1995). Expression of cell adhesion molecules on ovarian tumour cell lines and mesothelial cells, in relation to ovarian cancer metastasis. Cancer Lett 91(2):229-34.
92 Alkhamesi NA, Ziprin P, Pfistermuller K, Peck DH, Darzi AW (2005). ICAM-1 mediated peritoneal carcinomatosis, a target for therapeutic intervention. Clin Exp Metastasis 22(6):449-59.
93 Ziprin P, Alkhamesi NA, Ridgway PF, Peck DH, Darzi AW (2004). Tumour-expressed CD43 (sialophorin) mediates tumourmesothelial cell adhesion. Biol Chem 385(8):755-61.
94 Tanaka H, Yashiro M, Sunami T, Ohira M, Hirakawa Y (2002). Lipid-mediated gene transfection of intercellular adhesion molecule-1 suppresses the peritoneal metastasis of gastric carcinoma. Int J Mol Med 10(5):613-7.
95 Jones EY, Harlos K, Bottomley MJ, Robinson RC, Driscoll PC, Edwards RM, Clements JM, Dudgeon TJ, Stuart DI (1995). Crystal structure of an integrin-binding fragment of vascular cell adhesion molecule-1 at 1.8 A resolution. Nature 373(6514):539-44.
96 Arlt MJE, Novak-Hofer I, Gast D, Gschwend V, Moldenhauer G, Grunberg J, Honer M, Schubiger PA, Altevogt P, Kruger A (2006). Efficient inhibition of intra-peritoneal tumor growth and dissemination of human ovarian carcinoma cells in nude mice by anti-L1-cell adhesion molecule monoclonal antibody treatment. Cancer Res 66(2):936-43.
97 Stoeck A, Schlich S, Issa Y, Gschwend V, Wenger T, Herr I, Marme A, Bourbie S, Altevogt P, Gutwein P (2006). L1 on ovarian carcinoma cells is a binding partner for Neuropilin-1 on mesothelial cells. Cancer Lett 239(2):212-26.
98 Kodera Y, Nakanishi H, Ito S, Misawa K, Ito Y, Nakayama G, Koike M, Fujiwara M, Yamamura Y, Nakao A (2009). Expression of L1 cell adhesion molecule is a significant prognostic factor in pT3-stage gastric cancer. Anticancer Res 29(10):4033-9.
99 Knogler K, Grunberg J, Zimmermann K, Cohrs S, Honer M, Ametamey S, Altevogt P, Fogel M, Schubiger PA, Novak-Hofer I (2007). Copper-67 radioimmunotherapy and growth inhibition by anti-L1-cell adhesion molecule monoclonal antibodies in a therapy model of ovarian cancer metastasis. Clin Cancer Res 13(2 Pt 1):603-11.
100 Asao T, Nagamachi Y, Morinaga N, Shitara Y, Takenoshita S, Yazawa S (1995). Fucosyltransferase of the peritoneum contributed to the adhesion of cancer cells to the mesothelium. Cancer 75(6 Suppl):1539-44.
101 Schott A, Vogel I, Krueger U, Kalthoff H, Schreiber HW, Schmiegel W, Henne-Bruns D, Kremer B, Juhl H (1998). Isolated tumor cells are frequently detectable in the peritoneal cavity of gastric and colorectal cancer patients and serve as a new prognostic marker. Ann Surg 227(3):372-9.
102 Ikeda Y, Mori M, Kamakura T, Saku M, Sugimachi K (1995). Immunohistochemical expression of sialyl Tn and sialyl Lewis(a) antigens in stromal tissue correlates with peritoneal dissemination in stage IV human gastric cancer. Eur J Surg Oncol 21(2):168-75.

Adhesion molecules in PM of CRC | Chapter 5
103
5
103 Kiguchi K, Iwamori M, Mochizuki Y, Kishikawa T, Tsukazaki K, Saga M, Amemiya A, Nozawa S (1998). Selection of human ovarian carcinoma cells with high dissemination potential by repeated passage of the cells in vivo into nude mice, and involvement of Le(x)-determinant in the dissemination potential. Jpn J Cancer Res 89(9):923-32.
104 Gebauer F, Wicklein D, Stubke K, Nehmann N, Schmidt A, Salamon J, Peldschus K, Nentwich MF, Adam G, Tolstonog G, Bockhorn M, Izbicki JR, et al. (2013). Selectin binding is essential for peritoneal carcinomatosis in a xenograft model of human pancreatic adenocarcinoma in pfp--/rag2-- mice. Gut 62(5):741-50.
105 Aubert M, Panicot-Dubois L, Crotte C, Sbarra V, Lombardo D, Sadoulet MO, Mas E (2000). Peritoneal colonization by human pancreatic cancer cells is inhibited by antisense FUT3 sequence. Int J Cancer 88(4):558-65.
106 Gaspar MJ, Arribas I, Coca MC, ez-Alonso M (2001). Prognostic value of carcinoembryonic antigen, CA 19-9 and CA 72-4 in gastric carcinoma. Tumour Biol 22(5):318-22.
107 Kochi M, Fujii M, Kanamori N, Kaiga T, Kawakami T, Aizaki K, Kasahara M, Mochizuki F, Kasakura Y, Yamagata M (2000). Evaluation of serum CEA and CA19-9 levels as prognostic factors in patients with gastric cancer. Gastric Cancer 3(4):177-86.
108 Nakamori S, Furukawa H, Hiratsuka M, Iwanaga T, Imaoka S, Ishikawa O, Kabuto T, Sasaki Y, Kameyama M, Ishiguro S, Irimura T (1997). Expression of carbohydrate antigen sialyl Le(a): a new functional prognostic factor in gastric cancer. J Clin Oncol 15(2):816-25.
109 Nakagoe T, Sawai T, Tsuji T, Jibiki MA, Nanashima A, Yamaguchi H, Yasutake T, Ayabe H, Arisawa K, Ishikawa H (2002). Difference in prognostic value between sialyl Lewis(a) and sialyl Lewis(x) antigen levels in the preoperative serum of gastric cancer patients. J Clin Gastroenterol 34(4):408-15.
110 Ikeda Y, Oomori H, Koyanagi N, Mori M, Kamakura T, Minagawa S, Tateishi H, Sugimachi K (1995). Prognostic value of combination assays for CEA and CA 19-9 in gastric cancer. Oncology 52(6):483-6.
111 Nakata B, Hirakawa-YS Chung K, Kato Y, Yamashita Y, Maeda K, Onoda N, Sawada T, Sowa M (1998). Serum CA 125 level as a predictor of peritoneal dissemination in patients with gastric carcinoma. Cancer 83(12):2488-92.
112 Hwang GI, Yoo CH, Sohn BH, Shin JH, Park YL, Kim HD, Kim YS, Han WK, Pae WK (2004). Predictive value of preoperative serum CEA, CA19-9 and CA125 levels for peritoneal metastasis in patients with gastric carcinoma. Cancer Res Treat 36(3):178-81.
113 Yamamoto M, Baba H, Kakeji Y, Endo K, Ikeda Y, Toh Y, Kohnoe S, Okamura T, Maehara Y (2004). Prognostic significance of tumor markers in peritoneal lavage in advanced gastric cancer. Oncology 67(1):19-26.
114 Yang SH, Lin JK, Lai CR, Chen CC, Li AF-Y, Liang WY, Jiang JK (2004). Risk factors for peritoneal dissemination of colorectal cancer. J Surg Oncol 87(4):167-73.
115 Park IJ, Choi GS, Jun SH (2009). Prognostic value of serum tumor antigen CA19-9 after curative resection of colorectal cancer. Anticancer Res 29(10):4303-8.
116 Li Y, Yang Y, Lu M, Shen L (2011). Predictive value of serum CEA, CA19-9 and CA72.4 in early diagnosis of recurrence after radical resection of gastric cancer. Hepatogastroenterology 58(112):2166-70.
117 Takahashi Y, Takeuchi T, Sakamoto J, Touge T, Mai M, Ohkura H, Kodaira S, Okajima K, Nakazato H (2003). The usefulness of CEA and/or CA19-9 in monitoring for recurrence in gastric cancer patients: a prospective clinical study. Gastric Cancer 6(3):142-5.
118 Marrelli D, Pinto E, De SA, Farnetani M, Garosi L, Roviello F (2001). Clinical utility of CEA, CA 19-9, and CA 72-4 in the follow-up of patients with resectable gastric cancer. Am J Surg 181(1):16-9.
119 Kufe DW (2009). Mucins in cancer: function, prognosis and therapy. Nat Rev Cancer 9(12):874-85.
120 Rump A, Morikawa Y, Tanaka M, Minami S, Umesaki N, Takeuchi M, Miyajima A (2004). Binding of ovarian cancer antigen CA125/MUC16 to mesothelin mediates cell adhesion. J Biol Chem 279(10):9190-8.
121 Gubbels JAA, Belisle J, Onda M, Rancourt C, Migneault M, Ho M, Bera TK, Connor J, Sathyanarayana BK, Lee B, Pastan I, Patankar MS (2006). Mesothelin-MUC16 binding is a high affinity, N-glycan dependent interaction that facilitates peritoneal metastasis of ovarian tumors. Mol Cancer 5(1):50.
122 Scholler N, Garvik B, Hayden-Ledbetter M, Kline T, Urban N (2007). Development of a CA125-mesothelin cell adhesion assay as a screening tool for biologics discovery. Cancer Lett 247(1):130-6.

Chapter 5 | Adhesion molecules in PM of CRC
104
123 Bergan L, Gross JA, Nevin B, Urban N, Scholler N (2007). Development and in vitro validation of anti-mesothelin biobodies that prevent CA125/Mesothelin-dependent cell attachment. Cancer Lett 255(2):263-74.
124 Theriault C, Pinard M, Comamala M, Migneault M, Beaudin J, Matte I, Boivin M, Piche A, Rancourt C (2011). MUC16 (CA125) regulates epithelial ovarian cancer cell growth, tumorigenesis and metastasis. Gynecol Oncol 121(3):434-43.
125 Emoto S, Ishigami H, Yamashita H, Yamaguchi H, Kaisaki S, Kitayama J (2012). Clinical significance of CA125 and CA72-4 in gastric cancer with peritoneal dissemination. Gastric Cancer 15(2):154-61.
126 Fujimura T, Kinami S, Ninomiya I, Kitagawa H, Fushida S, Nishimura G, Kayahara M, Shimizu K, Ohta T, Miwa K (2002). Diagnostic laparoscopy, serum CA125, and peritoneal metastasis in gastric cancer. Endoscopy 34(7):569-74.
127 Yamamoto M, Baba H, Toh Y, Okamura T, Maehara Y (2007). Peritoneal lavage CEA/CA125 is a prognostic factor for gastric cancer patients. J Cancer Res Clin Oncol 133(7):471-6.
128 Wang L, Ma J, Liu F, Yu Q, Chu G, Perkins AC, Li Y (2007). Expression of MUC1 in primary and metastatic human epithelial ovarian cancer and its therapeutic significance. Gynecol Oncol 105(3):695-702.
129 Van Elssen CH, Frings PW, Bot FJ, Van de Vijver KK, Huls MB, Meek B, Hupperets P, Germeraad WT, Bos GM (2010). Expression of aberrantly glycosylated Mucin-1 in ovarian cancer. Histopathology 57(4):597-606.
130 Nakanishi H, Kodera Y, Yamamura Y, Kuzuya K, Nakanishi T, Ezaki T, Tatematsu M (1999). Molecular diagnostic detection of free cancer cells in the peritoneal cavity of patients with gastrointestinal and gynecologic malignancies. Cancer Chemother Pharmacol 43 Suppl:S32-S36.
131 Wang L, Chen H, Pourgholami MH, Beretov J, Hao J, Chao H, Perkins AC, Kearsley JH, Li Y (2011). Anti-MUC1 monoclonal antibody (C595) and docetaxel markedly reduce tumor burden and ascites, and prolong survival in an in vivo ovarian cancer model. PLoS One 6(9):e24405.
132 Oei ALM, Moreno M, Verheijen RHM, Sweep FCGJ, Thomas CMG, Massuger LFAG, von Mensdorff-Pouilly S (2008). Induction of IgG antibodies to MUC1 and survival in patients with epithelial ovarian cancer. Int J Cancer 123(8):1848-53.
133 Patriarca C, Macchi RM, Marschner AK, Mellstedt H (2012). Epithelial cell adhesion molecule expression (CD326) in cancer: a short review. Cancer Treat Rev 38(1):68-75.
134 Imano M, Itoh T, Satou T, Yasuda A, Nishiki K, Kato H, Shiraishi O, Peng Y, Shinkai M, Tsubaki M, Yasuda T, Imamoto H, et al. (2012). High expression of epithelial cellular adhesion molecule in peritoneal metastasis of gastric cancer. Target Oncol 8(4):231-5
135 Schlereth B, Fichtner I, Lorenczewski G, Kleindienst P, Brischwein K, da Silva A, Kufer P, Lutterbuese R, Junghahn I, Kasimir-Bauer S, Wimberger P, Kimmig R, et al. (2005). Eradication of tumors from a human colon cancer cell line and from ovarian cancer metastases in immunodeficient mice by a single-chain Ep-CAM-/CD3-bispecific antibody construct. Cancer Res 65(7):2882-9.
136 Strohlein MA, Lordick F, Ruttinger D, Grutzner KU, Schemanski OC, Jager M, Lindhofer H, Hennig M, Jauch KW, Peschel C, Heiss MM (2011). Immunotherapy of peritoneal carcinomatosis with the antibody catumaxomab in colon, gastric, or pancreatic cancer: an open-label, multicenter, phase I/II trial. Onkologie 34(3):101-8.
137 Rossi Del Monte S, Ranieri D, Mazzetta F, Kazemi Nava A, Raffa S, Torrisi MR, Ziparo V (2012). Free peritoneal tumor cells detection in gastric and colorectal cancer patients. J Surg Oncol 106(1):17-23.
138 Kim M, Rooper L, Xie J, Kajdacsy-Balla AA, Barbolina MV (2012). Fractalkine receptor CX(3)CR1 is expressed in epithelial ovarian carcinoma cells and required for motility and adhesion to peritoneal mesothelial cells. Mol Cancer Res 10(1):11-24.
139 Li Z, Miao Z, Jin G, Li X, Li H, Lv Z, Xu HM (2012). betaig-h3 supports gastric cancer cell adhesion, migration and proliferation in peritoneal carcinomatosis. Mol Med Report 6(3):558-64.
140 Kajiyama H, Shibata K, Terauchi M, Ino K, Nawa A, Kikkawa F (2008). Involvement of SDF-1alpha/CXCR4 axis in the enhanced peritoneal metastasis of epithelial ovarian carcinoma. Int J Cancer 122(1):91-9.
141 Davidson B, Goldberg I, Reich R, Tell L, Dong HP, Trope CG, Risberg B, Kopolovic J (2003). AlphaV- and beta1-integrin subunits are commonly expressed in malignant effusions from ovarian carcinoma patients. Gynecol Oncol 90(2):248-57.

Adhesion molecules in PM of CRC | Chapter 5
105
5
142 Nishimura S, Chung YS, Yashiro M, Inoue T, Sowa M (1996). CD44H plays an important role in peritoneal dissemination of scirrhous gastric cancer cells. Jpn J Cancer Res 87(12):1235-44.
143 Grzesiak JJ, Tran Cao HS, Burton DW, Kaushal S, Vargas F, Clopton P, Snyder CS, Deftos LJ, Hoffman RM, Bouvet M (2011). Knockdown of the beta(1) integrin subunit reduces primary tumor growth and inhibits pancreatic cancer metastasis. Int J Cancer 129(12):2905-15.
144 Ceelen WP, Bracke ME (2009). Peritoneal minimal residual disease in colorectal cancer: mechanisms, prevention, and treatment. Lancet Oncol 10(1):72-9.
145 Trzpis M, McLaughlin PM, de Leij LM, Harmsen MC (2007). Epithelial cell adhesion molecule: more than a carcinoma marker and adhesion molecule. Am J Pathol 171(2):386-95.
146 Maetzel D, Denzel S, Mack B, Canis M, Went P, Benk M, Kieu C, Papior P, Baeuerle PA, Munz M, Gires O (2009). Nuclear signalling by tumour-associated antigen EpCAM. Nat Cell Biol 11(2):162-71.
147 Gosens MJ, van Kempen LC, van de Velde CJ, van Krieken JH, Nagtegaal ID (2007). Loss of membranous Ep-CAM in budding colorectal carcinoma cells. Mod Pathol 20(2):221-32.
148 Ransohoff DF (2004). Rules of evidence for cancer molecular-marker discovery and validation. Nat Rev Cancer 4(4):309-14.


Chapter 6Versican and vascular endothelial growth factor expression levels in peritoneal metastases from
colorectal cancer are associated with survival after cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy
N.R. Sluiter E.M.V. de Cuba R. Kwakman W.J.H.J. Meijerink P.M. Delis-van Diemen V.H.M. Coupé J.A.M. Beliën G.A. MeijerI.H.J.T. de Hingh E.A. te Velde
Clin Exp Metastasis. 2016 Apr;33(4):297-307

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
108
Abstract
Background: Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) can increase survival of colorectal cancer (CRC) patients with peritoneal metastases (PM). This treatment is associated with high morbidity and mortality rates. Therefore, improvement of patient selection is necessary. Assuming that the clinical phenotype is dictated by biological mechanisms, biomarkers could play a crucial role in this process. Since it is unknown whether and to what extent angiogenesis influences the course of disease in patients with PM, we investigated the expression of two angiogenesis-related markers and their relation to overall survival (OS) in CRC patients after CRS and HIPEC.
Patients & Methods: Clinicopathological data and tissue samples were collected from 65 CRC patients with isolated metastases to the peritoneum that underwent CRS and HIPEC. Whole tissue specimens from PM were evaluated for versican (VCAN) expression, VEGF expression and microvessel density (MVD) by immunohistochemistry. The relation between these markers and OS was assessed using univariate and multivariate analysis. Associations between VEGF expression, VCAN expression, MVD and clinicopathological data were tested.
Results: High stromal VCAN expression was associated with high MVD (p=0.001), better resection outcome (p=0.003) and high T-stage (p=0.027). High epithelial VCAN expression was associated with MVD (p=0.007) and a more complete resection (p<0.001). In multivariate analysis, simplified peritoneal cancer index (p=0.001), VEGF expression levels (p=0.012), age (p=0.030), epithelial VCAN expression levels (p=0.042) and lymph node status (p=0.053) were associated with OS.
Conclusions: Concluding, VCAN and VEGF were associated with survival in CRC patients with PM after CRS and HIPEC. Independent validation in a well-defined patient cohort is required to confirm the putative prognostic role of these candidate biomarkers.

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
109
6
Introduction
Cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) is the preferred therapeutic strategy for patients with isolated peritoneal metastases (PM) originating from colorectal cancer (CRC) [1, 2]. This approach results in a median survival ranging from 33 to 45 months [3-7]. A recent meta-analysis even suggests that the combination of CRS and HIPEC compared to treatment with modern systemic chemotherapy potentially improves outcome in a carefully selected group of patients with both PM and liver metastases [8].
Treatment with CRS and HIPEC has considerable morbidity and mortality rates of 15-34% and 5% respectively [3, 6, 9, 10], with anastomotic leakage being the most common cause of mortality. Consequently, a relatively long median hospital stay of 16 days is observed [5]. The high morbidity and mortality rates significantly impact the quality of life [7] and thus selection of patients that will benefit most from this treatment is key. Prediction of patient response to the surgical procedure and chemotherapeutic compounds will help bring the proper treatment to the right patient, providing a much needed step forward towards personalised medicine [11]. Assuming that the clinical phenotype of this disease is ultimately dictated by biological mechanisms, read-outs of these mechanisms (i.e., biomarkers) might aid in predicting treatment outcomes [12].
More specifically, identifying biomarkers requires knowledge of molecules that contribute to peritoneal dissemination. Peritoneal dissemination is viewed as a multistep process, in which the establishment of a metastatic lesion ultimately depends on colonisation of cancer cells and the creation of a metastatic niche [11]. At this step, the formation of a tumour-specific microenvironment is pivotal. Interactions between cancer cells and their surrounding stroma provide growth and survival signals necessary to evade apoptosis, to enable invasion and migration, and to provide oxygen and nutrients through angiogenesis [13-16]. Angiogenesis is crucial for tumour growth beyond 150-200 micrometres from the nearest blood vessel and for progression of micrometastases to macrometastases [14, 17, 18]. Consequently, angiogenesis influences tumour progression and is associated with higher morbidity and mortality rates in HIPEC patients, as is suggested by several authors [19, 20]. Angiogenesis depends on complex interactions between several cell types and extracellular matrix (ECM) components [17]. The exact interactions required for this process are not fully understood. In an other study we did not find correlations between the angiogenesis related markers hypoxia-inducible factor 1a (HIF1a), stromal derived factor 1 (SDF1), CXC chemokine receptor 4 (CXCR4) and vascular endothelial growth factor (VEGF) [19]. Several other studies, however, suggest a role for versican (VCAN)

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
110
[21-24]. VCAN is a sulphate proteoglycan overexpressed in a variety of human malignant tumours, including CRC [21, 25-31]. VCAN-mediated angiogenesis possibly depends upon interaction with VEGF. VEGF-A induced microvessel formation was accompanied by VCAN degradation and subsequent resynthesis [32]. In human astrocytoma cells VCAN was shown to form a complex with fibronectin and VEGF. This complex enhanced endothelial cell adhesion, proliferation and migration, possibly providing the molecular basis by which VCAN promotes angiogenesis [33]. It is not known, however, whether and to what extent VCAN influences the course of disease in PM patients. Additionally, the relation between VCAN expression, VEGF expression and angiogenesis has not yet been investigated in PM. The aim of the present study is to assess the possible role of VCAN as a prognostic biomarker in CRC patients with PM who underwent treatment with CRS and HIPEC. Secondly, correlations between VCAN and VEGF expression levels, microvessel density (MVD) and clinicopathological parameters were evaluated.
Methods
Treatment - CRS and HIPEC
In two tertiary referral centres, the Catharina Hospital Eindhoven from 2007 to 2010 and the VU University Medical Centre Amsterdam from 2010 to June 2013, 78 patients with PM of CRC were treated with CRS and HIPEC with curative intent. Both institutions performed the CRS and HIPEC procedure by following the same standardised protocol [5]. Complete debulking, stripping of the affected parietal peritoneum, and removal of the omentum and adnexa was performed as described by Sugarbaker et al. (1996) [1]. When deemed necessary, multi-organ resections were carried out. Subsequently, intra-abdominal lavage with Mitomycin C (MMC), 35 mg/m2 body surface, was performed with a target intraperitoneal temperature of 39-41 degrees Celsius for 90 minutes.
Patient selection and data collection
Patients with PM of non-colorectal origin (n=2) were excluded. Specimens of 11 patients were not eligible for analysis due to loss of tissue or technical difficulties, leaving 65 patients eligible for further analysis.
Clinicopathological characteristics and follow-up data were collected from patient records of both institutions (table 1). Resection outcome was determined according to the maximal size of residual tumour tissue. An R1 resection was recorded when no macroscopically visible tumour was left behind, an R2a resection when the residual macroscopic tumour was smaller than 2.5 millimetre and an R2b resection when macroscopically tumour deposits larger than 2.5 millimetre remained [34].

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
111
6
Tumour specimens were collected during CRS and preserved as formalin-fixed paraffin-embedded (FFPE) tissue. Collection, storage and use of clinicopathological data and tissue specimens were performed in compliance with the ‘Code for Proper Secondary Use of Human Tissue’ in The Netherlands.
Assays and immunohistochemistry protocols
Sections of histologically confirmed PM from CRC (4 μm) were mounted on glass slides and immunohistochemically stained for VCAN, VEGF and CD31. After deparaffinisation and rehydration, endogenous peroxidases were blocked with 0.3% hydrogen peroxide in methanol. Tissue sections were treated with 10mM citrate buffer (pH 6.0) in a microwave for 30 minutes at 90 Watts for the VCAN staining and for 5 minutes at maximum power followed by 10 minutes at 360 Watts for the VEGF and CD31 staining. Sections were subsequently incubated overnight at 4 degrees Celsius with primary mouse anti-VCAN antibody (clone 2-B-1, Seikagaku, Tokyo, Japan; dilution 1:300) and anti-VEGF antibody labelling the VEGF-121, VEGF-165 and the VEGF-189 isoforms (clone v91, Dako, Carpinteria, USA, dilution 1:50) and incubated for 1 hour at room temperature with anti-CD31 antibody (clone JC70A, Dako, Carpinteria, USA, dilution 1:50). Signals were visualised with a horseradish peroxidase-coupled anti-mouse polymer (Envision, Dako, Heverlee, Belgium) for VCAN and a poly-HRP-GAM/R/R IgG (PowerVision) for VEGF and CD31. This procedure was followed by diaminobenzidine (Dako) and Mayer’s haematoxylin counterstain.
Evaluation of protein expression
Initially, tissue samples were scored for VCAN and VEGF intensity in four categories (negative, weak, moderate and strong, figure 1) but dichotomised into two categories: negative and weak as low expression versus moderate and strong as high expression for VCAN and weak and moderate as low expression versus strong as high expression for VEGF. Cut-offs were determined that discriminated best between the low and high expressing groups using the Kaplan-Meier method. Scoring was done using a 20x magnification (20x/0.45, diameter 0.98 mm), depending on lesion size. Staining pattern and the location of protein expression were assessed. VCAN staining was expressed in the cytoplasm of tumour cells and in the stroma surrounding the tumour cells. Hence, both stromal and epithelial VCAN were analysed. Since VEGF was predominantly seen in the cytoplasm of tumour cells, its intensity was scored in the cytoplasmic compartment. All tissue sections were scored and examined blinded to clinicopathological data. Fifteen per cent of sections were analysed independently in a blinded fashion by a second investigator (NRS and EMVdC) with high inter-observer agreement for all stainings (Cohen’s weighted kappa value, VEGF Kw=0.82, epithelial Kw=0.65, stromal VCAN Kw=0.74).

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
112
Table 1: Clinicopathological characteristics of 65 CRC patients with PM.
Characteristic n/mean/median %/s.d./range
General characteristics
All 65
Mean OS (months), range 34.4 29.4-39.2
Gender
Male (%) 25 38.5
Female (%) 40 61.5
Age at CRS and HIPEC
Mean (s.d.) 59.6 11.6
Median (range) 62 31-78
Follow-up after CRS and HIPEC (months)
Mean (s.d.) 21.0 10.8
Median (range) 21.0 2-50
Primary tumour characteristics
Location primary tumour
Colon (%) 49 75.4
Rectum (%) 5 7.7
Rectosigmoid (%) 11 16.9
Tumour differentiation
Poor (%) 11 17.0
Moderate (%) 22 33.8
Well (%) 3 4.6
Unknown (%) 29 44.6
Tumour histology
Adenocarcinoma (%) 39 60.0
Mucinous (%) 22 33.8
Signet cell (%) 4 6.2
Lymph node involvement
Yes (%) 46 70.8
No (%) 17 26.2
Unknown (%) 2 3.1
T-stage primary tumour
T1 (%) 1 1.5
T2 (%) 2 3.1
T3 (%) 27 41.5
T4 (%) 34 52.3
Unknown (%) 1 1.5

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
113
6
Table 1: Continued
Characteristic n/mean/median %/s.d./range
Stage primary tumour
Stage 1 (%) 1 1.5
Stage 2 (%) 10 15.4
Stage 3 (%) 18 27.7
Stage 4 (%) 35 53.8
Unknown (%) 1 1.5
PM characteristics
Synchronous PM
Yes (%) 35 53.8
No (%) 30 46.2
Simplified PCI
<2 (%) 1 1.5
2-4 (%) 42 64.6
5 (%) 14 21.5
>5 (%) 8 12.3
Resection outcome
R1 (%) 37 56.9
R2a (%) 22 33.8
R2b (%) 6 9.2
Adjuvant chemotherapy
Yes (%) 41 63.1
No (%) 24 36.9
Pre-operative chemotherapy 6 months before HIPEC
Yes (%) 17 26.2
No (%) 48 73.8
OS (overall survival), CRS (cytoreductive surgery), HIPEC (hyperthermic intraperitoneal chemotherapy), PM (peritoneal metastases), simplified PCI (peritoneal cancer index).
MVD was determined by automated image analysis of CD31 staining patterns. In short, complete slides were scanned with a digital Mirax slide Scanner system (3DHISTECH, Budapest, Hungary). The scan resolution of all pictures at 20x was 0.23μm. Next, areas with tumour tissue were manually selected using the Panoramic Viewer software (3DHISTECH) and exported in the TIFF image-format. A computerised morphometric analysis of the CD31 stained slides was executed using ImageJ. The CD31 staining was used to quantify the amount of microvessels per area as the percentage of the field of view that was CD31 positive [35]. Morphometric measurements were performed without knowledge of sample identity. For survival analysis, MVD was dichotomised as ‘low’ and

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
114
‘high’ if respectively less than 31.0% -the mean MVD percentage- and more than 31.0% of the analysed area was stained positive for CD31.
Statistical Analysis
Associations between the staining intensities of the markers and clinicopathological variables were studied by means of the Spearman’s correlation coefficient (two continuous variables), the Fisher’s Exact Test (two categorical/dichotomous variables) or the Kruskal-Wallis test (a continuous non-normally distributed variable with a categorical/dichotomous variable) [36]. Associations were considered statistically significant for p-values smaller than or equal to 0.05 (two sided test).
Overall survival (OS) was defined as time in months from date of surgery to death from any cause. Patients were censored at date last known to be alive. Univariate associations between OS and potential prognostic variables were studied by means of Kaplan-Meier analysis and tested using the log-rank test (table 3). Variables with a p-value ≤ 0.1 and possible relevant markers were included in a multivariate Cox regression analysis. Variable selection in the Cox model was done using backward selection with a threshold p-value of 0.1 for exclusion from the model.
All data were reported according to the REMARK guidelines. Statistical analyses were performed using the package for the social sciences version 20 for OsX (IBM, Armonk, NY, USA).
Results
Associations between VCAN, VEGF, MVD and clinicopathological characteristics
Significant associations between markers and clinicopathological variables are listed in table 2. A complete overview of all associations is shown in supplementary tables 1a-d. VCAN was expressed in both the epithelial and the stromal compartment. Stromal VCAN was negative in 1.5%, weak in 28.4%, moderate in 32.8% and strong in 37.3% of patients (Figure 1a-c). The group patients with high stromal VCAN expression had an MVD of 34.4% (s.d. 12.6) and the group with low stromal VCAN expression an MVD of 22.4% (s.d. 7.7) (p=0.001). Furthermore, we found high VCAN expression in the stromal compartment to be associated with better resection outcome (p=0.003, odds ratio [OR] 0.17, 95% CI 0.053-0.53, table 2) and higher T-stage of the primary tumour (p=0.027, OR 3.59, 95% CI 2.40-5.37, table 2).

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
115
6
Epithelial VCAN was negative in 13.4%, weak in 14.9%, moderate in 26.9% and strong in 44.8% (Figure 1a-c). In the VCAN positive cells a cytoplasmic staining was seen, sometimes with a highly intense granular pattern, probably depicting the Golgi system [37]. In the patients with high epithelial VCAN expression an MVD of 33.9% (s.d. 12.4) was seen and in the patients with low epithelial VCAN expression an MVD of 22.9% (s.d. 9.6) (p=0.007). Both epithelial VCAN (p<0.001, OR 0.11, 95% CI 0.029-0.38, table 2) and a granular epithelial VCAN expression pattern (p=0.001, table 2) correlated with a more favourable resection outcome. In male patients, epithelial VCAN expression was mostly granular (p=0.028, table 2), which may be related to an androgen-mediated regulation of the VCAN gene [38].
Table 2: Significant associations between VCAN, VEGF, MVD and clinicopathological variables.
Low^ (%)
High^ (%) p-value Odds ratio
(95% CI)Stromal VCAN expression
Resection outcome R1 6 (28.6) 31 (70.5) 0.003* 0.168 (0.053-0.528)
R2a/R2b 15 (71.4) 13 (29.5)
T-stage T1/T2 3 (15.0) 0 (0) 0.027* 3.588 (2.396-5.373)
T3/T4 17 (85.0) 44 (100)
MVD, % (s.d.) 22.4 (7.7) 34.4 (12.6) 0.001**
Epithelial VCAN expression
Resection outcome R1 4 (21.1) 33 (71.7) <0.001* 0.105 (0.029-0.376)
R2a/R2b 15 (78.9) 13 (46.6)
MVD, % (s.d.) 22.9 (9.6) 33.9 (12.4) 0.007**Negative (%)
Not granular(%)
Granular (%) p-value Odds ratio
(95% CI)VCAN staining pattern
Resection outcome R1 3 (30.0) 7 (35.0) 27 (77.1) 0.001* -
R2a/R2b 7 (70.0) 13 (65.0) 8 (22.9)
Gender Male 4 (40.0) 3 (15.0) 18 (51.4) 0.028* -
Female 6 (60.0) 17 (85.0) 17 (48.6)
*Fisher’s exact test; **Kruskal-Wallis test; ^Low: negative and weak expression, high: moderate and weak expression.
VEGF expression in the cytoplasmic compartment of the tumour cells was detected in 100% of the patients. In 11.9% of these patients, weak VEGF expression, in 43.3% moderate VEGF expression and in 44.8% strong VEGF expression (Figure 1d-e) was observed. No association was observed between epithelial VEGF expression and MVD (p=0.596), epithelial VCAN expression (p=0.791) or stromal VCAN expression (p=0.595).

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
116
The mean and median MVD were 31.0 % (s.d. 12.4%) and 28.9 % (range 7.5-61.0%) respectively. MVD correlated to stromal and epithelial VCAN, but did not show associations with other markers or clinicopathological characteristics.
VEGF and epithelial VCAN are associated with OS in CRC patients with PM
Mean OS in the patient cohort was 34.4 months (95% CI 29.4-39.2, table 1). Mean survival in the group patients with low VEGF expression was 38.3 months and in the group patients with high VEGF expression 29.2 months (p=0.035). Mean survival in patients with high epithelial VCAN expression was 36.8 months and in patients with low epithelial VCAN expression 20.1 months (p=0.109). Furthermore, in patients with low and high stromal VCAN expression a mean survival of 34.9 months and 33.8 months was observed respectively (p=0.996, figure 2d). Mean survival in patients with low MVD was 36.5 months and in patients with high MVD mean survival was 29.0 months (p=0.747, figure 2b).Possibly important characteristics included in the multivariate analysis after being individually tested for correlation with OS were age (p=0.056), lymph node status (p=0.042), simplified Peritoneal Cancer Index (PCI) [39] (p=0.052), resection outcome (p=0.021), preoperative chemotherapy 6 months before HIPEC (p=0.007), VEGF (p=0.035) and epithelial VCAN (p=0.109) (Table 3).Variables that emerged as independent prognostic factors in the final model are listed in table 3. In this model, high VEGF expression was significantly associated with worsened OS (p=0.012, table 3, figure 2a). In contrast, high epithelial VCAN expression was significantly associated with longer OS (0=0.042, table 3, figure 2c). The observation of epithelial VCAN expression being significant in multivariate, but not in univariate analysis, is most probably attributable to the effect of confounding in the univariate analysis. This confounding effect is corrected for in multivariate analysis by including all possibly significant variables.
Table 3: Final model resulting from multivariate survival analysis.
Simplified PCI 0.235 0.097-0.570 0.001
VEGF expression 0.315 0.128-0.773 0.012
Age 1.048 1.004-1.094 0.030
VCAN expression 2.584 1.034-6.452 0.042
Lymph node status 0.296 0.086-1.014 0.053
*Variables tested for individual associations with OS (log rank): gender (p=0.292), age (p=0.056), histology class (p=0.123), differentiation grade (p=0.888), T-stage (p=0.581), lymph node status (p=0.042), stage (p=0.270), location primary tumour (p=0.807), synchronous metastases versus metachronous metastases (p=0.132), PCI index (p=0.052), resection outcome (p=0.021), chemotherapy in the 6 month before CRS and HIPEC (p=0.007), adjuvant chemotherapy (p=0.724), MVD (p=0.747), VEGF expression (p=0.035), stromal VCAN expression (p=0.996), epithelial VCAN expression (p=0.109), a granular VCAN staining pattern (p=0.779), simultaneous high VEGF and epithelial VCAN expression (p=0.129) and simultaneous high VEGF and stromal VCAN expression (p=0.158).

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
117
6
b
de f
ca
VC
AN
exp
ress
ion
VE
GF
expr
essi
on
epith
elia
l: ne
gativ
e (1
3.4%
)st
rom
al: w
eak
(28.
4%)
epith
elia
l: m
oder
ate
(26.
9%)
stro
mal
: stro
ng (3
7.3%
)
epith
elia
l: st
rong
(44.
8%),
gran
ular
pat
tern
stro
mal
: mod
erat
e (3
2.8%
)
epith
elia
l: w
eak
(11.
9%)
epith
elia
l: m
oder
ate
(43.
4%)
epith
elia
l: st
rong
(44.
8%)
5x 5x 5x
5x 5x 5x
20x
20x
20x
20x
20x
20x
MV
D
16.6
%
10x
23.0
%
10x
10x
35.4
%
Figu
re 1
: Rep
rese
ntat
ive
exam
ples
of v
ersi
can
(VC
AN
) (a,
b, c
) and
vas
cula
r end
othe
lial g
row
th fa
ctor
(VEG
F) (d
, e, f
) exp
ress
ion
patte
rns
and
mic
rove
ssel
den
sity
(MV
D) (
g, h
, i) i
n pe
riton
eal l
esio
ns. T
he m
agni
ficat
ion
is s
how
n on
the
mic
rogr
aphs
. Int
ensi
ties
wer
e cl
assi
fied
as n
egat
ive,
w
eak,
mod
erat
e or
stro
ng. S
corin
g pe
rcen
tage
s of a
ll m
arke
rs a
re li
sted
nex
t. St
rom
al V
CA
N e
xpre
ssio
n: n
egat
ive
(1.5
%),
wea
k (2
8.4%
), m
oder
ate
(32.
8%) a
nd st
rong
(37.
3%).
Epith
elia
l VC
AN
expr
essi
on: n
egat
ive (
13.4
%),
wea
k (1
4.9%
), m
oder
ate (
26.9
%) a
nd st
rong
(44.
8%).
VEG
F ex
pres
sion
: w
eak
(11.
9%),
mod
erat
e (4
3.3%
) and
stro
ng (4
4.8%
).

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
118
cSurvival
aSurvival
Time to death (months) Time to death (months)
Time to death (months)Time to death (months)
P=0.109 P=0.996
P=0.747P=0.035
Epithelial VCAN low (n=19)Epithelial VCAN high (n=46)
VEGF low (n=36)VEGF high (n=29)
bSurvival MVD low (n=34)
MVD high (n=23)
Stromal VCAN low (n=21)Stromal VCAN high (n=44)
dSurvival
Figure 2: Kaplan-Meier curves of all patients. The graphs depict the curves according to the dichotomised vascular endothelial growth factor (VEGF) (a), microvessel density (MVD) (b), epithelial versican (VCAN) (c) and stromal VCAN (d) categories.
Discussion
Although CRS and HIPEC increase survival rates of CRC patients with isolated PM [5-8], this treatment has considerable morbidity and mortality rates [3, 6, 9, 10]. Selection of patients that will benefit most from this treatment is key. Biomarkers could help in patient selection, preventing unnecessary morbidity in patients that will not benefit. Because it is not known whether and to what extent angiogenesis influences the course of disease in PM patients, the present study evaluated the expression of potential markers of angiogenesis –VCAN, VEGF and MVD- in these patients. In the multivariate analysis, VEGF and epithelial VCAN expression levels were found to be significantly associated with OS in CRC patients with PM after CRS and HIPEC (p=0.012 and p=0.042 respectively, table 3,

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
119
6
figure 2a and 2c). Furthermore, both high stromal and epithelial VCAN were related to increased microvessel density (MVD) (p=0.001 and p=0.007 respectively).
The currently observed association between VEGF and OS in CRC patients with PM is in accordance with several other clinical and preclinical studies demonstrating VEGF to have a role in PM formation and prognosis [20, 40-50]. The possible role of VEGF as a predictor of worse outcome corroborates the rationale for (neo-) adjuvant anti-VEGF based therapy in selected patients [20, 51, 52]. Neo-adjuvant administration of this drug was shown to improve outcome in patients after CRS and HIPEC [53]. Although a recent study described a twofold increase in morbidity in these patients after administration of bevacizumab [54], a meta-analysis including more than 3000 patients with metastasised CRC reported the amount and severity of treatment with bevacizumab to be acceptable [3].
The sulphate proteoglycan VCAN is thought to promote tumour development [21, 55] by mediating several processes such as proliferation [56-58], drug resistance [27, 56-62], cell adhesion [57-60], invasion [57, 58, 63] and angiogenesis [23, 24, 32, 33, 64, 65]. Angiogenesis in astrocytoma [33] and breast cancer [64] was suggested to result from interaction between VCAN and VEGF. In the present study, VEGF was not correlated to MVD, a finding supported by others [20]. Interestingly, stromal and epithelial VCAN levels did correlate with MVD. MVD is a measure of the number of vessels per high power field. Considering this number of vessels is not only determined by angiogenic factors, such as VEGF, but also by non-angiogenic factors such as oxygen and nutrient consumption rates, one might state that MVD does not necessarily adequately reflect the rate of angiogenesis [66]. Hence, it is possible that MVD is a marker of a more or less established vessel network, whilst VEGF is produced in the presence of hypoxic stimuli to stimulate angiogenesis [67]. Once vessels are established and an oxygen-rich environment is created, VEGF is no longer necessary for the formation of new vessels. In the presence of an established vessel network, other molecules, including VCAN, might be required for maintenance -and not creation- of a favourable microenvironment [14, 21]. To confirm this hypothesis, further experiments should focus on the exact mechanisms by which VEGF and VCAN possibly promote tumour growth in PM of CRC.
The present study revealed that epithelial VCAN is indicative for good survival in CRC patients with PM in multivariate analysis (p=0.042, table 3). This finding is supported by studies in primary CRC [37] and serous ovarian cancer [68]. The mechanism by which epithelial VCAN positively influences patient outcome might be related to tumour cell responses to chemotherapy [68]. Another study found cells transfected with V1 VCAN to be selectively sensitised to several apoptotic stimuli, for example to the chemotherapeutics

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
120
etoposide and cisplatin [61]. The influence of molecules such as VCAN in tumour response to chemotherapy stresses the importance of systematically analysing interactions between cancer cells and their environment in order to identify mechanisms contributing to drug sensitivity. In peritoneal cancer patients, sensitivity of tumour cells to heated MMC might -at least in part- account for good outcome in patients with high epithelial VCAN expression. A recent paper found low Bloom syndrome protein (BLM) expression to be associated with high MMC sensitivity in CRC cell lines. Low BLM expression was thereby related to improved survival in CRC patients with PM [69]. Since identification of sensitivity and resistance mechanisms could lead to mechanism-based therapies and further stratification of HIPEC patients, i.e. personalised medicine, further research is warranted in this particular field. Another interesting finding is that both epithelial and stromal VCAN expression and a granular expression pattern are associated with a better resection outcome. An explanation for this, albeit speculative, might be related to the role of VCAN in creation of a microenvironment for tumour cells [21, 23, 24, 55-60, 64, 65]. In this way, VCAN plays a role in determining the consistency and appearance of tumour spots on the peritoneal surface, thereby possibly contributing to the extent to which these spots can be detected and subsequently resected.
In the current study, several possible markers were investigated in a study cohort consisting of HIPEC patients, representing a well-defined group of cancer patients with metastases confined to the peritoneum. In these patients, we found in the multivariate analysis high epithelial VCAN and VEGF expression to be associated with improved and worsened outcome respectively. To our knowledge, this is the first study examining stromal and epithelial VCAN expression in PM. We presume that higher VCAN expression is associated with improved sensitivity to chemotherapy, but this hypothesis should be further studied in-vitro and in-vivo and in well-defined patient cohorts. Further studies focusing of VCAN and other potential biomarkers could help improve selection of patients with PM, in this way minimising unnecessary exposure to the high morbidity and mortality rates associated with HIPEC treatment. A more comprehensive understanding of VCAN based mechanisms contributing to peritoneal dissemination and patient responses to therapy will potentially result in a more personalised approach in CRC patients with PM, ultimately leading to better treatment outcomes.

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
121
6
References1 Sugarbaker PH. Patient selection and treatment
of peritoneal carcinomatosis from colorectal and appendiceal cancer. World J Surg 1995;19:235-240. doi: 10.1007/BF00308632
2 Sugarbaker PH, Jablonski KA. Prognostic features of 51 colorectal and 130 appendiceal cancer patients with peritoneal carcinomatosis treated by cytoreductive surgery and intraperitoneal chemotherapy. Ann Surg 1995;221:124-132. doi: 10.1097/00000658-199502000-00003
3 Cao Y, Tan A, Gao F, Liu L, Liao C, Mo Z. A meta-analysis of randomized controlled trials comparing chemotherapy plus bevacizumab with chemotherapy alone in metastatic colorectal cancer. Int J Colorectal Dis 2009;24:677-685. doi:10.1007/s00384-009-0655-9
4 Elias D, Gilly F, Boutitie F, Quenet F, Bereder JM, Mansvelt B, Lorimier G, Dubè P, Glehen O. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol 2010;28:63-68. doi: 10.1200/JCO.2009.23.9285
5 Kuijpers AM, Mirck B, Aalbers AG, Nienhuijs SW, de Hingh IH, Wiezer MJ, van Ramshorst B, van Ginkel RJ, Havenga K, Bremers AJ, de Wilt JH, Te Velde EA, Verwaal VJ. Kuijpers AM, Mirck B, Aalbers AG et al. Cytoreduction and HIPEC in the Netherlands: nationwide long-term outcome following the Dutch protocol. Ann Surg Oncol 2013;20:4224-4230. doi:10.1245/s10434-013-3145-9
6 Verwaal VJ1, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, Boot H, Zoetmulder FA. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol 2003;21:3737-3743. doi:10.1200/JCO.2003.04.187
7 Verwaal VJ, Kusamura S, Baratti D, Deraco M. The eligibility for local-regional treatment of peritoneal surface malignancy. J Surg Oncol 2008;98:220-223. doi:10.1002/jso.21060
8 de Cuba EM, Kwakman R, Knol DL, Bonjer HJ, Meijer GA, Te Velde EA. Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases: Systematic review of all literature and meta-analysis of observational studies. Cancer Treat Rev 2013;39:321-327. doi: 10.1016/j.ctrv.2012.11.003
9 Maggiori L, Bretagnol F, Ferron M, Chevalier Y, Panis Y. Laparoscopic colorectal anastomosis using the novel Chex((R)) circular stapler: a case-control study. Colorectal Dis 2011;13:711-715. doi: 10.1111/j.1463-1318.2010.02246.x
10 Verwaal VJ, Zoetmulder FA. Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. Eur J Surg Oncol 2004;30:280-285. doi:10.1016/j.ejso.2003.12.003
11 de Cuba EM1, Kwakman R, van Egmond M, Bosch LJ, Bonjer HJ, Meijer GA, te Velde EA. Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : future possibilities for personalised treatment by use of biomarkers. Virchows Arch 2012;461:231-243. doi:10.1007/s00428-012-1287-y
12 Taflampas P, Dayal S, Chandrakumaran K, Mohamed F, Cecil TD, Moran BJ. Pre-operative tumour marker status predicts recurrence and survival after complete cytoreduction and hyperthermic intraperitoneal chemotherapy for appendiceal Pseudomyxoma Peritonei: Analysis of 519 patients. Eur J Surg Oncol 2014;40:515-520. doi:S0748-7983(14)00005-5 [pii];10.1016/j.ejso.2013.12.021 [doi].
13 Pietras K, Ostman A. Hallmarks of cancer: interactions with the tumor stroma. Exp Cell Res 2010;316:1324-1331. doi: 10.1016/j.ejso.2013.12.021
14 Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011;144:646-674. doi: 10.1016/j.cell.2011.02.013
15 Gupta GP, Massague J. Cancer metastasis: building a framework. Cell 2006;127:679-695. doi: 10.1016/j.cell.2006.11.001
16 Fidler IJ. The pathogenesis of cancer metastasis: the ‘seed and soil’ hypothesis revisited. Nat Rev Cancer 2003;3:453-458. doi:10.1038/nrc1098
17 Folkman J, Shing Y. Angiogenesis. J Biol Chem 1992;267:10931-10934.
18 Gao D, Nolan DJ, Mellick AS, Bambino K, McDonnell K, Mittal V. Endothelial progenitor cells control the angiogenic switch in mouse lung metastasis. Science 2008;319:195-198. doi; 10.1126/science.1150224
19 de Cuba EMV, de Hingh IHJT, Sluiter NR, Kwakman R, Coupé VMH, Beliën JAM, Verwaal VJ, Meijerink WJHJ, Delis-van Diemen PM, Bonjer HJ, Meijer GA, te Velde EA. Angiogenesis-related markers and prognosis after Cytoreductive surgery and Hyperthermic Intraperitoneal Chemotherapy for metastatic colorectal cancer. Ann Surg Oncol, 2016. Doi: 10.1245/s10434-015-5023-0

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
122
20 Logan-Collins JM, Lowy AM, Robinson-Smith TM, Kumar S, Sussman JJ, James LE, Ahmad SA. VEGF expression predicts survival in patients with peritoneal surface metastases from mucinous adenocarcinoma of the appendix and colon. Ann Surg Oncol 2008;15:738-744. doi: 10.1245/s10434-007-9699-721 Du WW, Yang W, Yee AJ. Roles of versican in cancer biology--tumorigenesis, progression and metastasis. Histol Histopathol 2013;28:701-713. doi: HH-11-300
22 Ang LC, Zhang Y, Cao L, Yang BL, Young B, Kiani C, Lee V, Allan K, Yang BB. Versican enhances locomotion of astrocytoma cells and reduces cell adhesion through its G1 domain. J Neuropathol Exp Neurol 1999;58:597-605. doi: 10.1079/00005072-199906000-0004
23 Labropoulou VT, Theocharis AD, Ravazoula P, Perimenis P, Hjerpe A, Karamanos NK, Kalofonos HP. Versican but not decorin accumulation is related to metastatic potential and neovascularization in testicular germ cell tumours. Histopathology 2006;49:582-593. doi: 10.1111/j.1365-2559.2006.02558.x
24 Ghosh S, Albitar L, LeBaron R, Welch WR, Samimi G, Birrer MJ, Berkowitz RS, Mok SC. Up-regulation of stromal versican expression in advanced stage serous ovarian cancer. Gynecol Oncol 2010;119:114-120. doi: 10.1016/j.ygyno.2010.05.029
25 Ricciardelli C, Brooks JH, Suwiwat S, Sakko AJ, Mayne K, Raymond WA, Seshadri R, LeBaron RG, Horsfall DJ. Regulation of stromal versican expression by breast cancer cells and importance to relapse-free survival in patients with node-negative primary breast cancer. Clin Cancer Res 2002;8:1054-1060.
26 Suwiwat S, Ricciardelli C, Tammi R, Tammi M, Auvinen P, Kosma VM, LeBaron RG, Raymond WA, Tilley WD, Horsfall DJ. Expression of extracellular matrix components versican, chondroitin sulfate, tenascin, and hyaluronan, and their association with disease outcome in node-negative breast cancer. Clin Cancer Res 2004;10:2491-2498. doi: 10.1158/1078-0432.CCR-03-0146
27 Du WW, Yang BB, Shatseva TA, Yang BL, Deng Z, Shan SW, Lee DY, Seth A, Yee AJ. PLoS One 2010;5:e13828. doi: 10.1371/journal.pone.0013828
28 Ricciardelli C, Russell DL, Ween MP, Mayne K, Suwiwat S, Byers S, Marshall VR, Tilley WD, Horsfall DJ. Formation of hyaluronan- and versican-rich pericellular matrix by prostate cancer cells promotes cell motility. J Biol Chem 2007;282:10814-10825. doi: 10.1074/jbc.M606991200
29 Kusumoto T, Kodama J, Seki N, Nakamura K, Hongo A, Hiramatsu Y. Clinical significance of syndecan-1 and versican expression in human epithelial ovarian cancer. Oncol Rep 2010;23:917-925. Doi: 10.3892/or_00000715
30 Casey RC, Oegema TRJ, Skubitz KM, Pambuccian SE, Grindle SM, Skubitz APN. Cell membrane glycosylation mediates the adhesion, migration, and invasion of ovarian carcinoma cells. Clin Exp Metastasis 2003;20:143-152. doi: 10.1023/A:1022670501667
31 Lancaster JM, Dressman HK, Clarke JP, Sayer RA, Martino MA, Cragun JM, Henriott AH, Gray J, Sutphen R, Elahi A, Whitaker RS, West M, Marks JR, Nevins JR, Berchuck A. Identification of genes associated with ovarian cancer metastasis using microarray expression analysis. Int J Gynecol Cancer 2006;16:1733-1745. doi: 10.1111/j.1525-1438.2006.00660.x
32 Fu Y, Nagy JA, Brown LF, Shih SC, Johnson PY, Chan CK, Dvorak HF, Wight TN. Proteolytic cleavage of versican and involvement of ADAMTS-1 in VEGF-A/VPF-induced pathological angiogenesis. J Histochem Cytochem 2011;59:463-473. doi: 10.1369/0022155411401748
33 Zheng PS, Wen J, Ang LC, Sheng W, Viloria-Petit A, Wang Y, Wu Y, Kerbel RS, Yang BB. Versican/PG-M G3 domain promotes tumor growth and angiogenesis. FASEB J 2004;18:754-756. doi: 10.1096/fj.03-0545fje
34 Verwaal VJ, van RS, Witkamp A, Boot H, van SG, Zoetmulder FA. Long-term survival of peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol 2005;12:65-71. doi: 10.1007/s10434-004-1167-z
35 Kerkhof MH, Ruiz-Zapata AM, Bril H, Bleeker MC, Belien JA, Stoop R, Helder MN. Changes in tissue composition of the vaginal wall of prementopausal women with prolapse. Am J Obstet Gynecol 2014;210:168.e1-9. doi: 10.1016/j.ajog.2013.10.881
36 Breslow N. A generalized Kruskal-Wallis test for comparing K samples subject to unequal patterns of censorship. Biometrika 1970;57:579-594. doi: 10.1093/biomet/57.3.579
37 de Wit M, Belt EJ, Delis-van Diemen PM, Carvalho B, Coupé VM, Stockmann HB, Bril H, Beliën JA, Fijneman RJ, Meijer GA. Ann Surg Oncol 2013;20 Suppl 3:S348-S359. doi: 10.1245/s10434-012-2441-0
38 Read JT, Rahmani M, Boroomand S, Allahverdian S, McManus BM, Rennie PS. Androgen receptor regulation of the versican gene through an androgen response element in the proximal promoter. J Biol Chem 2007;282:31954-31963. doi: 10.1074/jbc.M702099200

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
123
6
39 Portilla AG, Shigeki K, Dario B, Marcello D. The intraoperative staging systems in the management of peritoneal surface malignancy. J Surg Oncol. 2008;98(4):228–31. doi: 10.1002/jso.21068
40 Williams E, Martin S, Moss R, Durrant L, Deen S. Co-expression of VEGF and CA9 in ovarian high-grade serous carcinoma and relationship to survival. Virchows Archiv. 2012;461(1):33–9.
41 Shaheen RM, Ahmad SA, Liu W, Reinmuth N, Jung YD, Tseng WW, et al. Inhibited growth of colon cancer carcinomatosis by antibodies to vascular endothelial and epidermal growth factor receptors. British Journal of Cancer. 2001;85(4):584–9. doi: 10.1054/bjoc.2001.1936
42 Imaizumi T, Aoyagi K, Miyagi M, Shirouzu K. Suppressive effect of bevacizumab on peritoneal dissemination from gastric cancer in a peritoneal metastasis model. Surg Today. 2010;40(9):851–7.
43 Bai Y, Deng H, Yang Y, Zhao X, Wei Y, Xie G, et al. VEGF-targeted short hairpin RNA inhibits intraperitoneal ovarian cancer growth in nude mice. Oncology. 2009;77(6):385–94. doi: 10.1159/000279385
44 Diniz Bizzo SM, Meira DD, Lima JM, Mororó JDS, Casali-da-Rocha JC, Ornellas MHF. Peritoneal VEGF burden as a predictor of cytoreductive surgery outcome in women with epithelial ovarian cancer. Int J Gynaecol Obstet. 2010;109(2):113–7. doi: 10.1016/j.ijgo.2009.11.021
45 Varghese S, Burness M, Xu H, Beresnev T, Pingpank J, Alexander HR. Site-Specific Gene Expression Profiles and Novel Molecular Prognostic Factors in Patients with Lower Gastrointestinal Adenocarcinoma Diffusely Metastatic to Liver or Peritoneum. Ann Surg Oncol. 2007;14(12):3460–71. 10.1245/s10434-007-9557-7
46 Zebrowski BK, Liu W, Ramirez K, Akagi Y, Mills GB, Ellis LM. Markedly elevated levels of vascular endothelial growth factor in malignant ascites. Ann Surg Oncol. 1999;6(4):373–8. doi: 10.1007/s10434-999-0373-047 Yoshikawa T, Tsuburaya A, Miyagi Y, Sekiguchi H, Kimura M, Cho H, Kobayashi O. Up-regulation of hypoxia-inducible factor-1 alpha and VEGF mRNAs in peritoneal dissemination of patients with gastric cancer. Anticancer Res. 2006;26(5B):3849–53.
48 Gerber SA, Rybalko VY, Bigelow CE, Lugade AA, Foster TH, Frelinger JG, Lord EM. Preferential Attachment of Peritoneal Tumor Metastases to Omental Immune Aggregates and Possible Role of a Unique Vascular Microenvironment in Metastatic Survival and Growth. The American Journal of Pathology. 2006;169(5):1739–52. doi: 10.2353/ajpath.2006.051222
49 Kobold S, Hegewisch-Becker S, Oechsle K, Jordan K, Bokemeyer C, Atanackovic D. Intraperitoneal VEGF inhibition using bevacizumab: a potential approach for the symptomatic treatment of malignant ascites? The Oncologist. 2009;14(12):1242–51. doi: 10.1634/theoncologist.2009-0109
50 Ninomiya S, Inomata M, Tajima M, Ali AT, Ueda Y, Shiraishi N, Kitano S. Effect of bevacizumab, a humanized monoclonal antibody to vascular endothelial growth factor, on peritoneal metastasis of MNK-45P human gastric cancer in mice. J Surg Res. 2009;154(2):196–202. doi: 10.1016/j.jss.2008.08.017
51 Shaheen RM, Tseng WW, Vellagas R, Liu W, Ahmad SA, Jung YD, Reinmuth N, Drazan KE, Bucana CD, Hicklin DJ, Ellis LM. Effects of an antibody to vascular endothelial growth factor receptor-2 on survival, tumor vascularity, and apoptosis in a murine model of colon carcinomatosis. Int J Oncol 2001;18:221-226.
52 Klaver YLB, Leenders BJM, Creemers G-J, Rutten HJT, Verwaal VJ, Lemmens VEPP, et al. Addition of Biological Therapies to Palliative Chemotherapy Prolongs Survival in Patients With Peritoneal Carcinomatosis of Colorectal Origin. Am J Clin Oncol. 2013;36(2):157-161. doi: 10.3892/ijo.18.2.221
53 Ceelen W, Van NY, Putte DV, Pattyn P. Neoadjuvant Chemotherapy with Bevacizumab May Improve Outcome after Cytoreduction and Hyperthermic Intraperitoneal Chemoperfusion (HIPEC) for Colorectal Carcinomatosis. Ann Surg Oncol 2014;21:3023-3028. doi: 10.1245/s10434-014-3713-7
54 Eveno C, Passot G, Goéré D, Soyer P, Gayat E, Glehen O, Elias D, Pocard M. Bevacizumab doubles the early postoperative complication rate after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol 2014;21:1792-1800. doi:10.1245/s10434-013-3442-3
55 Theocharis AD, Skandalis SS, Tzanakakis GN, Karamanos NK. Proteoglycans in health and disease: novel roles for proteoglycans in malignancy and their pharmacological targeting. FEBS J 2010;277:3904-3923. doi: 10.1111/j.1742-4658.2010.07800.x
56 Sheng W, Dong H, Lee DY, Lu WY, Yang BB. Versican modulates gap junction intercellular communication. J Cell Physiol 2007;211:213-219. doi: 10.1002/jcp.20921

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
124
57 Cattaruzza S, Schiappacassi M, Kimata K, Colombatti A, Perris R. The globular domains of PG-M/versican modulate the proliferation-apoptosis equilibrium and invasive capabilities of tumor cells. FASEB J 2004;18:779-781. doi:10.1096/fj.03-0660fje
58 Du WW, Fang L, Yang W, Sheng W, Zhang Y, Seth A, Yang BB, Yee AJ.. The role of versican G3 domain in regulating breast cancer cell motility including effects on osteoblast cell growth and differentiation in vitro - evaluation towards understanding breast cancer cell bone metastasis. BMC Cancer 2012;12:341. doi: 10.1186/1471-2407-12-341
59 Wu Y, Wu J, Lee DY, Yee A, Cao L, Zhang Y, Kiani C, Yang BB. Versican protects cells from oxidative stress-induced apoptosis. Matrix Biol 2005;24:3-13. doi: 10.1016/j.matbio.2004.11.007
60 Wu Y, Chen L, Zheng PS, Yang BB. beta 1-Integrin-mediated glioma cell adhesion and free radical-induced apoptosis are regulated by binding to a C-terminal domain of PG-M/versican. J Biol Chem 2002;277:12294-12301. doi:10.1074/jbc.M11074820061 LaPierre DP, Lee DY, Li SZ, Xie YZ, Zhong L, Sheng W, Deng Z, Yang BB. The ability of versican to simultaneously cause apoptotic resistance and sensitivity. Cancer Res 2007;67:4742-4750. doi: 10.1158/0008-5472.CAN-06-3610
62 Straussman R, Morikawa T, Shee K, Barzily-Rokni M, Qian ZR, Du J, Davis A, Mongare MM, Gould J, Frederick DT, Cooper ZA, Chapman PB, Solit DB, Ribas A, Lo RS, Flaherty KT, Ogino S, Wargo JA, Golub TR. Tumour micro-environment elicits innate resistance to RAF inhibitors through HGF secretion. Nature 2012;487:500-504. doi: 10.1038/nature11183
63 Ween MP, Hummitzsch K, Rodgers RJ, Oehler MK, Ricciardelli C. Versican induces a pro-metastatic ovarian cancer cell behavior which can be inhibited by small hyaluronan oligosaccharides. Clin Exp Metastasis 2011;28:113-125. doi: 10.1007/s10585-010-9363-7
64 Yee AJ, Akens M, Yang BL, Finkelstein J, Zheng PS, Deng Z, Yang B. The effect of versican G3 domain on local breast cancer invasiveness and bony metastasis. Breast Cancer Res 2007;9:R47. doi: 10.1186/bcr1751
65 Brown LF, Guidi AJ, Schnitt SJ, Van De Water L, Iruela-Arispe ML, Yeo TK, Tognazzi K, Dvorak HF. Vascular stroma formation in carcinoma in situ, invasive carcinoma, and metastatic carcinoma of the breast. Clin Cancer Res 1999;5:1041-1056.
66 Hlatky L, Hahnfeldt P, Folkman J. Clinical Application of Antiangiogenic Therapy: Microvessel Density, what It Does and Doesn’t Tell Us. JNCI Natl Cancer Inst. 2002;94(12):883-893. doi: 10.1093/jnci/94.12.88367 Chen L, Endler A, Shibasaki F. Hypoxia and angiogenesis: regulation of hypoxia-inducible factors via novel binding factors. Exp Mol Med. 2009;41(12):849–57. doi: 10.3858/emm.2009.41.12.103
68 Voutilainen K, Anttila M, Sillanpää S, Tammi R, Tammi M, Saarikoski S, Kosma VM. Versican in epithelial ovarian cancer: relation to hyaluronan, clinicopathologic factors and prognosis. Int J Cancer 2003;107:359-364. doi:10.1002/ijc.11423
69 Kwakman R, de Cuba EM, de Winter JP, de Hingh IH, Delis-van Diemen PM, Tijssen M, Rooimans MA, Krijgsman O, Carvalho B, Peters GJ, Bonjer HJ, Meijer GA, Te Velde EA. Tailoring heated intraperitoneal mitomycin C for peritoneal metastases originating from colorectal carcinoma: a translational approach to improve survival. Br J Cancer. 2015:1-6. doi: 10.1038/bjc.2015.18

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
125
6
Supplementary DataSupplementary table 1a: Associations between stromal versican (VCAN) expression, clinicopathological variables and other markers. PCI (peritoneal cancer index).
Stromal VCAN expression Low (%)^^ High (%)^^ p-value
Gender Male 10 (47.6) 15 (34.1)0.414*
Female 11 (52.4) 29 (65.9)Age at CRS and HIPEC (s.d.) 60.4 (13.4) 59.3 (10.9) 0.348^Tumour histology Adenocarcinoma 11 (52.4) 28 (63.6)
0.626*Mucinous 9 (42.9) 13 (29.5)
Signet cell 1 (4.8) 3 (6.8)Tumour differentiation Well 2 (16.7) 1 (5.3)
0.181*Moderate 6 (50.0) 15 (78.9)
Poor 4 (33.3) 3 (15.8)T-stage primary tumour T1/T2 3 (15.0) 0 (0)
0.027*T3/T4 17 (85.0) 44 (100)
Stage primary tumour Stage 1/2/3 6 (30.0) 22 (50.0)0.178*
Stage 4 14 (70.0) 22 (50.0)Lymph node involvement Negative 2 (10.0) 15 (34.9)
0.065*Positive 18 (90.0) 28 (65.1)
Location primary tumour Colon 18 (85.7) 31 (70.5)
0.525*Rectum 1 (4.8) 4 (9.1)
Rectosigmoid 2 (9.5) 9 (20.5)Synchronous PM Yes 15 (71.4) 20 (45.5)
0.065*No 6 (28.6) 24 (54.5)
Simplified PCI 1-4 15 (71.4) 28 (63.6)0.587*
5-7 6 (28.6) 16 (36.4)Resection outcome R1 6 (28.6) 31 (70.5)
0.003*R2 15 (71.4) 13 (29.5)
Associations with other markersEpithelial VCAN Low 11 (52.4) 8 (18.2)
0.008*High 10 (47.6) 36 (81.8)
VCAN staining pattern Negative 5 (23.8) 5 (11.4)
0.471*Not granular 6 (28.6) 14 (31.8)
Granular 10 (47.6) 25 (56.8)VEGF Low 13 (61.9) 23 (52.3)
0.595*High 8 (38.1) 21 (47.7)
MVD, % (s.d.) 22.4 (7.7) 34.4 (12.6) 0.001^
*Fisher’s exact test, ^Kruskal-Wallis test, ^^ Low: negative and weak expression, high: moderate and strong expression.

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
126
Supplementary table 1b: Associations between epithelial versican (VCAN), clinicopathological variables and other markers. PCI (peritoneal cancer index).
Epithelial VCAN expression Low (%)^^ High (%)^^ p-value
Gender Male 6 (31.6) 19 (41.3)0.579*
Female 13 (68.4) 27 (58.7)
Age at CRS and HIPEC (s.d.) 60.0 (12.5) 59.5 (11.4) 0.868^Tumour histology Adenocarcinoma 9 (47.4) 30 (65.2)
0.296*Mucinous 8 (42.1) 14 (30.4)
Signet cell 2 (10.5) 2 (4.3)Tumour differentiation Well 2 (25.0) 1 (4.3)
0.221*Moderate 4 (50.0) 17 (73.9)
Poor 2 (25.0) 5 (21.7)T-stage primary tumour T1/T2 2 (11.1) 1 (2.2)
0.189*T3/T4 16 (88.9) 45 (97.8)
Stage primary tumour Stage 1/2/3 7 (38.9) 21 (45.7)0.781*
Stage 4 11 (61.1) 25 (54.3)Lymph node involvement Negative 2 (11.8) 15 (32.6)
0.121*Positive 15 (88.2) 31 (67.4)
Location primary tumour Colon 15 (78.9) 34 (73.9)
0.639*Rectum 2 (10.5) 3 (6.5)
Rectosigmoid 2 (10.5) 9 (19.6)Synchronous PM Yes 11 (57.9) 24 (52.2)
0.787*No 8 (42.1) 22 (47.8)
Simplified PCI 1-4 12 (63.2) 31 (67.4)0.779*
5-7 7 (36.8) 15 (32.6)Resection outcome R1 4 (21.2) 33 (71.7)
<0.001*R2 15 (78.9) 13 (28.3)
Associations with other markersStromal VCAN Low 11 (57.9) 10 (21.7)
0.006*High 8 (42.1) 36 (78.3)
VCAN staining pattern Negative 9 (47.4) 1 (2.2)
<0.001*Not granular 10 (52.6) 10 (21.7)
Granular 0 35 (76.1)VEGF Low 10 (52.6) 26 (56.5)
0.791*High 9 (47.4) 20 (43.5)
MVD, % (s.d.) 22.9 (9.6) 33.9 (12.4) 0.007^
*Fisher’s exact test, ^Kruskal-Wallis test, ^^ Low: negative and weak expression, high: moderate and strong expression.

Versican and VEGF and prognosis after CRS & HIPEC | Chapter 6
127
6
Supplementary table 1c: Associations between vascular endothelial growth factor (VEGF), clinicopathological variables and other markers. PCI (peritoneal cancer index).
VEGF expression Low (%)^^ High (%)^^ p-value
Gender Male 10 (27.8) 15 (51.7) 0.073*
Female 26 (72.2) 14 (48.3)
Age at CRS and HIPEC (s.d) 58.6 (11.8) 60.8 (11.5) 0.795^Tumour histology Adenocarcinoma 23 (63.9) 16 (55.2) 0.783*
Mucinous 11 (30.6) 11 (37.9)
Signet cell 2 (5.6) 2 (6.9)Tumour differentiation Well 1 (6.7) 2 (12.5) 0.085*
Moderate 13 (86.7) 8 (50.0)
Poor 1 (6.7) 6 (37.5)T-stage primary tumour T1/T2 1 (2.8) 2 (7.1) 0.577*
T3/T4 35 (97.2) 26 (92.9)Stage primary tumour Stage 1/2/3 7 (38.9) 21 (45.7) 0.781*
Stage 4 11 (61.1) 25 (54.3)Lymph node involvement Negative 10 (27.8) 7 (25.9) 1.000*
Positive 26 (72.2) 20 (74.1)Location primary tumour Colon 26 (72.2) 23 (79.3) 0.908*
Rectum 3 (8.3) 2 (6.9)
Rectosigmoid 7 (19.4) 4 (13.8)Synchronous PM Yes 16 (44.4) 19 (65.5) 0.133*
No 20 (55.6) 10 (34.5)Simplified PCI 1-4 23 (63.9) 20 (69.0) 0.794*
5-7 13 (36.1) 9 (31.0)Resection outcome R1 24 (66.7) 13 (44.8) 0.086*
R2 12 (33.3) 16 (55.2)
Associations with other markersStromal VCAN Low 13 (36.1) 8 (27.6) 0.595*
High 23 (63.9) 21 (72.4)Epithelial VCAN Low 10 (27.8) 9 (31.0) 0.791*
High 26 (72.2) 20 (69.0)VCAN staining pattern Negative 5 (13.9) 5 (17.2) 0.888*
Not granular 12 (33.3) 8 (27.6)
Granular 19 (52.8) 16 (55.2)MVD, % (s.d.) 32.0 (12.5) 29.7 (12.8) 0.596^
*Fisher’s exact test, ^Kruskal-Wallis test, ^^ Low: weak and moderate expression, high: strong expression.

Chapter 6 | Versican and VEGF and prognosis after CRS & HIPEC
128
Supplementary table 1d: Associations between microvessel density (MVD), clinicopathological variables and other markers. PCI (peritoneal cancer index).
MVD Mean (s.d.) p-value
Gender Male 32.3 (11.5) 0.517*
Female 30.4 (13.3)
Age at CRS and HIPEC 0.449^ (r=-0.102)
Tumour histology Adenocarcinoma 32.8 (13.6) 0.358*
Mucinous 27.9 (10.7)
Signet cell 30.4 (11.7)
Tumour differentiation Well 24.5 (8.5) 0.711*
Moderate 29.1 (12.8)
Poor 26.2 (12.6)
T-stage primary tumour T1/T2 62.0 (15.0) 0.122*
T3/T4 59.3 (11.5)
Stage primary tumour Stage 1/2/3 58.0 (11.7) 0.207*
Stage 4 60.5 (11.6)
Lymph node involvement Negative 59.3 (12.1) 0.827*
Positive 59.3 (11.6)
Location primary tumour Colon 31.4 (13.4) 0.358*
Rectum 36.0 (11.0)
Rectosigmoid 27.2 (8.2)
Synchronous PM Yes 30.9 (10.9) 0.749*
No 31.2 (14.5)
PCI 1-4 59.8 (11.9) 0.757*
5-7 59.3 (11.4)
Resection outcome R1 33.2 (11.6) 0.105*
R2 27.6 (13.6)
Associations with other markers
Stromal VCAN Low 60.4 (7.7) 0.001*
High 59.3 (10.9)
Epithelial VCAN Low 22.9 (9,6) 0.007*
High 33.9 (12.4)
VCAN staining pattern Negative 24.3 (9.0) 0.271*
Not granular 33.6 (16.3)
Granular 31.2 (10.6)
VEGF Low 32.0 (12.5) 0.440*
High 29.7 (12.8)
*Kruskal-Wallis test, ^Spearman’s correlation coefficient

Chapter 7Angiogenesis related markers and prognosis after
Cytoreductive Surgery and Hyperthermic Intra-peritoneal Chemotherapy for
Metastatic Colorectal Cancer
E.M.V. de CubaI.H.J.T. de HinghN.R. SluiterR. Kwakman V. M. H. CoupéJ.A.M. BeliënV.J. VerwaalW.J.H.J. MeijerinkP.M. Delis-van DiemenH.J. BonjerG.A. MeijerE.A. te Velde
Ann Surg Oncol. 2016 May;23(5):1601-8

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
130
Abstract
Background: Patients presenting with peritoneal metastases (PM) of colorectal cancer (CRC) can be curatively treated with cytoreductive surgery (CRS) and Hyperthermic Intra-Peritoneal Chemotherapy (HIPEC). Angiogenesis is under control of multiple molecules of which HIF1a, SDF1, CXCR4, and VEGF are key players. We investigated these angiogenesis-related markers and their prognostic value in patients with PM arising from CRC treated with CRS & HIPEC.
Patients & Methods: Clinicopathological data and tissue specimens were collected in two tertiary referral centres from 52 patients that underwent treatment due to isolated PM of CRC. Whole tissue specimens were subsequently analysed for protein expression of HIF1a, SDF1, CXCR4 and VEGF by immunohistochemistry. Microvessel density (MVD) was analysed by CD31 immunohistochemistry. The relationship between overall survival (OS) and protein expression as well as other clinicopathological characteristics was analysed.
Results: Univariate analysis showed that high peritoneal cancer index (PCI), resection with residual disease and high expression of VEGF were negatively correlated with OS after treatment with CRS and HIPEC. (P<0.01, P<0.01 and P=0.02, respectively) However, no association was found between the other markers and OS. (P>0.05) Multivariate analysis showed an independent association between OS and PCI, resection outcome and VEGF expression. (Multivariate HR: 6.1, 7.8 and 3.8 respectively, P≤0.05) Conclusions: An independent association was found between high VEGF expression levels and worse OS after CRS and HIPEC. The addition of VEGF expression to the routine clinicopathological work-up, could help to identify patients at risk for early treatment failure. Furthermore, VEGF may be a potential target for adjuvant treatment in these patients.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
131
7
Introduction
Colorectal cancer (CRC) is a major health concern in the Western world. It is the third most common cancer worldwide for both males and females, accounting for over one million new cases and approximately 600.000 deaths annually. (1,3) In the course of their disease, roughly 25% of these patients will develop peritoneal metastases (PM), alone or in combination with other metastases. 1-3 In CRC, isolated peritoneal metastases are regarded as a form of localized disease spread and are thus considered amenable to local control, i.e. surgery. 4,5 PM are increasingly treated with curative intent, using cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC), as opposed to systemic chemotherapy. 6,7 Because treatment with CRS and HIPEC has morbidity and mortality rates of 15–18 % and 5 % respectively, it is of utmost importance to carefully select those patients who will benefit most from this treatment. 7-10 At present, patients are selected solely based on clinical parameters and intraoperative findings. Based on the hypothesis that phenotype of PM in CRC, and thus also clinical behavior, is driven by underlying biological mechanisms, readouts of disease biology (i.e., biomarkers) will aid in establishing a more refined identification of suitable patients. Additionally, molecular targets may be of great value in prognosis assessment, imaging and guidance of therapy.Metastasis formation depends on the combined processes of dissemination of tumor cells and development of a receptive microenvironment. One important condition for successful outgrowth of these tumor cells is the presence of sufficient oxygen, aided by the formation of new blood vessels referred to as angiogenesis. 11 Angiogenesis is under control of multiple molecules of which HIF1a, SDF1, CXCR4, and VEGF are key players. Vascular endothelial growth factor (VEGF) is the most important and best characterized angiogenic factor and also the target of the anti-cancer drug bevacuzimab. 12 The interaction of CXCR4 and SDF1 could advance tumor progression and metastases through the induction of VEGF-mediated angiogenesis 13. Furthermore, HIF1 is known to regulate the activation of VEGF directly 14,15. (Supp. figure 1)
Expression of HIF1, CXCR4, SDF1 and VEGF have each been reported to have clinical implications in several malignancies, including primary CRC. 16 Furthermore, multiple studies have shown the relevance of angiogenesis, measured by the formation of microvessels (i.e. microvessel density (MVD)) in CRC. 17 Therefore we hypothesized that these molecules may serve as prognostic markers in this population of metastasized CRC patients.

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
132
Materials and methods
Patients were included from two prospective registries. All consecutive patients treated with curative intent with CRS and HIPEC at the Catharina Hospital in Eindhoven from 2007 to 2010 and from the VU University Medical Center Amsterdam from 2010 and 2011, both tertiary referral centers for patients with peritoneal surface malignancy, were reviewed for inclusion. Only patients presenting with isolated PM were included for this retrospective study. Clinicopathological data were extracted from the patient records at both institutions. All tumors were staged according to the fifth version of the American Joint Committee on Cancer (AJCC) pathologic -node-metastasis (TNM) classification. Formalin and paraffin embedded (FFPE) tissue specimens obtained during CRS were collected from the archives and H&E slides were reviewed to verify the presence of tumor cells. Collection, storage and use of clinicopathological data and tissue specimens were performed in compliance with the “Code for Proper Secondary Use of Human Tissue in The Netherlands”. Treatment - Cytoreductive Surgery and HIPEC
The pre-operative work-up and the CRS and HIPEC procedure was carried out in a uniform fashion by both surgical teams according to the Dutch protocol using the open coliseum technique with Mitomycin C. 7,18
Tissue specimens and Immunohistochemistry Protocols
Four μm sections were mounted on glass slides, deparaffinized and rehydrated. Endogenous peroxidase was blocked using 0.3% hydrogen peroxide in methanol. All consecutive slides were subsequently immunohistochemically stained for all markers according to the optimized protocols summarized in supplementary table 1. All sections were counterstained with Mayer’s heamatoxylin. Scoring was performed utilizing a 10x objective or a 20x objective, depending on whether the staining was cytoplasmic (10x / 0,25. Diameter 2,01mm) or nuclear (20x / 0,45. Diameter 0,98 mm). The intensity observed in the neoplastic cells was subsequently scored as negative, weak, moderate and strong. For HIF1a, protein expression in the nuclei of tumor cells was scored, whereas for SDF1, CXCR4 and VEGF intensities were scored in the cytoplasm. (Figure 1) All tissue samples were analyzed blinded to corresponding clinicopathological information. Ten percent of samples were re-evaluated by a second investigator (GAM) in a blinded fashion and scored by consensus between first and second investigator as a quality control step. Intensity of the staining was subsequently dichotomized, i.e. “low expression” or “high expression” at different cut-offs for four

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
133
7
markers as shown in table 2. All analyses were performed using the dichotomized staining intensity score. As for CD31, all specimens were stained using an anti-CD31 antibody according to an optimized protocol summarized in supp. table 1. Finally, the average MVD was quantified in the peritoneal lesions using a computerized morphometric and image analysis approach, as previously described. 19 In short, complete slides where scanned using a digital Mirax slide Scanner system (3DHISTECH, Budapest, Hungary) with a 20x objective with a numerical aperture of 0.75 and a Sony DFW-X710 Fire Wire 1/3” type progressive SCAN IT CCD (pixel size 4.65 x 4.65 μm). The scan resolution of all images at 20x was 0.23μm. After scanning representative areas of the tumor deposits were annotated manually using the Panoramic Viewer software (3D Histech) and subsequently exported in the TIFF image-format. A computerized morphometric analysis of the CD31 stained slides was executed, using ImageJ. Subsequently the MVD was dichotomized as “high” and “low” MVD by setting the threshold at 27% of the analysed area stained for MVD, as based on the median.
Statistical Analysis
Data analysis was performed with the statistical package for the socials sciences (SPSS Inc., Chicago IL) version 20 for OsX. Descriptive statistics were used to describe clinical and treatment related factors in the cohort.The primary endpoint was overall survival (OS), which was defined as time (months) from date of CRS and HIPEC to death from any cause. Survivors were censored on the date they were last known to be alive. For analytical purposes, patients surviving less than 12.6 months post-treatment were additionally categorized as short survivors, and patients surviving more than 12.6 months as long survivors, based on results from the first and only randomized controlled trial comparing CRS and HIPEC and conventional chemotherapy. 7
Associations between several clinicopathological variables were tested for significance using the unpaired t-test or the Mann-Whitney U test (association between dichotomous and continuous variable, either distributed normally or not normally), and the Chi-square test for unpaired ordinal and categorical data. Associations between marker expression and clinicopathological variables were analyzed by means of the Chi-Square, Kruskall-Wallis or Mann-Whitney U test, depending on the type of variables analyzed. Survival was analyzed using the Kaplan-Meier method. Additionally, established clinicopathological variables were included in a multivariate Cox regression analysis to determine the independent effect of each variable. Input variables were all first tested in a univariate fashion for association with OS, and only significant terms were included in the multivariate model (multivariate Cox regression analysis). The variable selection in the multivariate Cox model was carried out using backward selection with a threshold p-value for exclusion that was set at 0.1.

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
134
A p-value ≤0.05 was considered statistically significant. All data reported was REMARK compliant. 20
Results
The initial study cohort consisted of 53 patients. One patient was lost to follow-up. The patient characteristics are summarized in table 1.The median survival for the entire cohort (n=52) was 26 months (supp. fig.2). A total of 25 events were recorded at the end of follow-up. Univariate analysis showed that tumor burden (simplified Peritoneal Cancer index, sPCI21) and resection outcome were negatively correlated with survival after treatment. (supp. table 2)Nine patients were excluded for technical reasons (loss of tissue stained for CXCR4, SDF1, VEGF and CD31 respectively), while for HIF1a ten patients were lost for the same reason. Thus, for final marker analysis, 43 and 42 patients remained for analysis of HIF1a, SDF1 and VEGF respectively. For MVD analysis (CD31) data was available from 36 cases. (table 2)
An association was noted between a high HIF1a expression and favorable resection outcome (p=0.03) and male gender and higher CXCR4 expression (P=0.01) No association was seen between expression levels of HIF1a, CXCR4, SDF1,VEGF and MVD with the (other) clinicopathological characteristics listed in table 1 (P>0.05, data not shown). In addition, there was no association between the expression of the four markers and the MVD. (P>0.05, data not shown)
A total of 21 events occurred during follow-up in the group of patients successfully analyzed for protein expression. Only for VEGF a significant difference in overall survival between groups with high versus low expression was observed (mean OS 23,8 months versus 36,1 months, respectively, P=0.02). (fig. 2) For HIF1a, CXCR4, SDF1, and MVD, there was no significant association between protein expression and OS (P>0.05). (fig. 2)In addition, expression for VEGF was associated with short and long survival after treatment with CRS & HIPEC. (P=0.02) This was not the case for the other four markers HIF1a, SDF1, CXCR4 and MVD (P>0.05).
In the multiple regression analysis, it was found that sPCI, resection outcome and VEGF expression (high versus low expression) were significant independent predictors of survival (P=0.02, P=0.05, P=0.008, respectively). High VEGF expression had a Hazard Ratio of 3.8, (95%CI 1.41 - 10.06), indicating an autonomous association between VEGF expression and OS (table 3).

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
135
7
Table 1: Patient and tumor characteristics
Total Number of Patients: 53 N= %
Gender Male Female
2330
43.4%56.6%
Age (Mean + SD) 58 years SD 12,0
Follow-up (Median, Range) 22.5 months 0-59
Location Primary TumorColon, incl. appendixRectosigmoidRectumDouble Tumor
39851
73.6%15.1%9.4%1.9%
Tumor TypeAdenocarcinomaMuc. AdenocarcinomaSignet-cell carcinoma
33164
62.3%30.2%7.5%
T-Classification Primary TumorT1T2T3T4
112328
1.9%1.9%43.4%52.8%
Lymph Node Status Primary TumorNegativePositiveUnknown
13391
24.5%73.6%1.9%
Timing Peritoneal MetastasesSynchronousMetachronous
3023
56.6%43.4%
Simplified Peritoneal Cancer Index<22-45>5Unknown
1321154
1.9%60.4%20.8%9.4%7.5%
Resection OutcomeR0/R1R2
476
88.7%11.3%
Chemotherapy after CRS & HIPECYesNoUnknown
36134
67.9%24.5%7.5%

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
136
a1b1 c1 d1
b2 c2 d2
b3 c3 d3
a2
a3
VEGFHIF1α SDF1 CXCR4
Figure 1: Expression pattern of b)HIF1a, c)SDF1, d)CXCR4 and a)VEGF staining in peritoneal metastases of colorectal cancer epithelium. Immunohistochemical staining patterns ranged from weak to strong epithelial (nucleus and cytoplasm) staining for all four markers. Representative examples of all stainings, ranging from weak (1) to strong (3) in peritoneal metastases epithelium are shown.
A B
ED
C
Figure 2: KM curves showing the correlation between high and low expression of repectively, (a) HIF1a, (b) SDF1, (c) CXCR4 (d) VEGF and (e) MVD and overall survival in patients undergoing curative CRS and HIPEC for the treatment of PM of CRC.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
137
7
Table 2: Low versus high expression of HIF1a, SDF1, CXCR4, VEGF, and MVD
Antigen “Low expression” “High expression”
HIF1a Negative, N=0Weak, N=13 (31.0%)
Moderate, N=15 (35.7%)Strong, N=14 (33.3%)
SDF1 Negative, N=0Weak, N=3 (7.0%)Moderate, N=12 (27.9%)
Strong, N=28 (65.1%)
CXCR4 Negative, N=0Weak, N=2 (4.7%)Moderate, N=16 (37.2%)
Strong, N=25 (58.1%)
VEGF Negative, N=0Weak, N=3 (7.0%)Moderate, N=19 (44.2%)
Strong, N=21 (48.8%)
MVD Low, N=19 (52.8%) High, N=17 (47.2%)
Table 3: Multivariate analysis of overall survival for the complete CRS and HIPEC cohort (N=52).
Variable Hazard-ratio 95% CI P-value
Simplified Peritoneal Cancer Index
- 2 to 4 abdominal regions affected
- 5 abdominal regions affected
- 5-7 abdominal regions affected
1.00 (ref)
3.01
6.06
-
1.04 – 8.72
1.28 – 28.70
0.02
Resection Outcome
- No residual tumour
- Residual tumour <2.5 mm
- Residual tumour >2.5 mm
1.00 (ref)
2.51
7.69
-
0.77 – 8.20
1.50 – 28.70
0.05
VEGF Expression 3.76 1.41 - 10.06 <0.01
Discussion
Isolated peritoneal metastases are increasingly being treated with curative intent by CRS and HIPEC, and with good clinical results. 22,23 However, known clinical factors alone appear to be insufficiently discriminatory for patient selection, as patients are often observed presenting with rapid recurrence after treatment despite having seemingly favorable prognostic clinical profile. The present study revealed an independent association between high VEGF expression levels and worse survival after CRS and HIPEC. The possible addition of VEGF expression to the routine pathological work-up could therefore potentially aid in identifying those patients at risk for early treatment failure despite their seemingly favorable clinical profile. In addition a correlation was noted between high expression of CXCR4 and male gender. Data in published literature on correlation between gender and CXCR4 expression are

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
138
scarce and conflicting and thus remain inconclusive. 24,25 Interestingly, we also found an association between high HIF1a expression and a more favorable resection outcome. One explanation, albeit speculative, could be that HIF1a competent tumor cells, i.e. with a relatively high HIF1a expression, behave less aggressively under hypoxic conditions than HIF1 negative tumor cells, because they are still dependent on the blood supply from blood vessels and have not yet (fully) developed the capacity to survive under such circumstances. 26-29 This could also explain the tendency observed towards better OS for patients with high expression of HIF1a (fig. 2). Besides the biological connection between these molecules, expression of HIF1a, CXCR4, SDF1 and VEGF have each been reported to have clinical implications in several malignancies. Both lack of HIF1a expression under hypoxic circumstances and overexpression have been previously linked to tumor progression, aggressive biological behavior and patient prognosis in several types of carcinomas. 26-31 CXCR4 is the most common chemokine expressed in tumors such as ovarian, breast and colorectal cancer. Its ligand, SDF1, has been described as highly expressed in metastatic sites, such as the lung, lymph nodes and liver and has been correlated with grade and prognosis in renal cell and breast carcinoma. 32,33 The prognostic value of high levels of VEGF has been demonstrated in multiple solid tumors and is associated with metastasis in CRC. 34 In addition, VEGF levels have been reported to predict survival in patients with carcinomatosis arising from several malignancies. 35-37 While in the present study VEGF expression levels appeared to have prognostic relevance, such an association was not observed for HIF1a, SDF1 and CXCR4 in the present cohort. On one hand, this may look counter intuitive, as VEGF is regulated by HIF1a, just like SDF1 and CXCR4, but on the other hand these regulatory networks in vivo are subject to many interactions and apparently in PM, other regulation mechanisms, including oncogenes, of VEGF expression prevail over HIF1a. In fact, the lack of prognostic significance of both SDF1 and CXCR4 in the present study may be consistent with this observation. 16,38
The current finding is also consistent with several other, both pre-clinical and clinical studies on PM arising from several epithelial malignancies like ovarian carcinoma in which VEGF has been shown to play a role in PM and prognosis. 35,39-47 Several studies have assessed the effect of blocking VEGF both on ascites formation and PM formation and progression. 39,41,43,44,46-49 All these studies show that blocking VEGF diminishes both ascites and PM and thus improves survival after surgical treatment. Most of these studies are pre-clinical and there are currently no clinical trials specifically addressing the effect of systemic treatment in peritoneal cancer patients. However, a subgroup analysis of clinical trials proving the efficacy of bevacizumab added to standard chemotherapy in the palliative treatment of metastatic CRC suggested that bevacizumab may also be beneficial for peritoneal cancer patients.50,51. Similar results were retrieved in a population based study 51.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
139
7
These findings have been supported by a recent study, in which 16% of patients received neoadjuvant treatment including bevacizumab. In this study the addition of bevacizumab was an independent, favorable prognostic factor for OS after CRS and HIPEC. 52 These findings, as well as evaluation of possible side-effects, await further validation. In a recent study, carried out specifically in the CRS and HIPEC population one group described the early post-operative major morbidity rate to be significantly higher after the administration of bevacizumab prior to CRS and HIPEC in a cohort consisting of 182 patients, of which 80 received bevacizumab. 53 However, in a meta-analysis including more than 3.000 patients treated with bevacizumab in metastatic CRC the authors concluded the therapy to be effective and the amount and severity of reported adverse-effects to be acceptable. 9 In addition to utilizing VEGF as a treatment target, it can also be utilized in the improvement of current pre- and intra-operative imaging. Encouraging results have been reported on the use of specific VEGF tracers (e.g. 89Zr-Bevacizumab), which can be used for the visualization of VEGF expression in-vivo. These interesting and ground-breaking developments could signal a new era in which the expression of certain molecules, e.g. VEGF, could aid not only in the treatment of our patients, but also in giving the treating CRS and HIPEC surgeon the much needed edge in the operating room by better visualization of even the smallest of tumor deposits. 54-56 Despite limitations of our study like a limited sample size, we believe the results shown are an important step towards furthering our knowledge of the molecular landscape of PM of CRC. The evidence gathered from (pre-)clinical studies indicate that VEGF expression possibly plays an important role in the pathogenesis of PM. In addition VEGF can be targeted with specific antibodies and these can also be labeled to improve visualization, both pre- and intra-operatively. This increasing evidence supports the notion that this oncogenic pathway deserves further study in this subgroup of metastatic CRC patients. In conclusion, high expression of VEGF was frequently observed in PM of CRC and in the present cohort higher VEGF expression levels correlated with worse overall survival after curative CRS and HIPEC. This may indicate that VEGF expression may not only serve as a prognostic marker, but also that adding anti-VEGF antibody based therapies, i.e. bevacizumab, could have additional therapeutic value in this subgroup of metastatic colorectal cancer patients.

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
140
References1. Parkin DM, Bray F, Ferlay J, Pisani P. Global
cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108.
2. Koppe MJ, Boerman OC, Oyen WJG, Bleichrodt RP. Peritoneal Carcinomatosis of Colorectal Origin. Annals of Surgery. 2006;243(2):212–222. doi:10.1097/01.sla.0000197702.46394.16.
3. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. doi:10.3322/caac.21166.
4. Elias D, Lefevre JH, Chevalier J, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of Clinical Oncology. 2009;27(5):681–685. doi:10.1200/JCO.2008.19.7160.
5. Carpizo DR, Are C, Jarnagin W, et al. Liver Resection for Metastatic Colorectal Cancer in Patients with Concurrent Extrahepatic Disease: Results in 127 Patients Treated at a Single Center. Ann Surg Oncol. 2009;16(8):2138–2146. doi:10.1245/s10434-009-0521-6.
6. Sugarbaker PH. Peritonectomy procedures. Annals of Surgery. 1995;221(1):29–42.
7. Verwaal VJ. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. Journal of Clinical Oncology. 2003;21(20):3737–3743. doi:10.1200/JCO.2003.04.187.
8. Maggiori L, Elias D. Curative treatment of colorectal peritoneal carcinomatosis: current status and future trends. Eur J Surg Oncol. 2010;36(7):599–603. doi:10.1016/j.ejso.2010.05.007.
9. Cao Y, Tan A, Gao F, Liu L, Liao C, Mo Z. A meta-analysis of randomized controlled trials comparing chemotherapy plus bevacizumab with chemotherapy alone in metastatic colorectal cancer. Int J Colorectal Dis. 2009;24(6):677–685. doi:10.1007/s00384-009-0655-9.
10. Verwaal VJ, Zoetmulder FAN. Follow-up of patients treated by cytoreduction and chemotherapy for peritoneal carcinomatosis of colorectal origin. European Journal of Surgical Oncology (EJSO). 2004;30(3):280–285. doi:10.1016/j.ejso.2003.12.003.
11. Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013.
12. Nieves BJ, D’Amore PA, Bryan BA. The function of vascular endothelial growth factor. Biofactors. 2009;35(4):332–337. doi:10.1002/biof.46.
13. Hong X, Jiang F, Kalkanis SN, et al. SDF-1 and CXCR4 are up-regulated by VEGF and contribute to glioma cell invasion. Cancer Letters. 2006;236(1):39–45. doi:10.1016/j.canlet.2005.05.011.
14. Chen L, Endler A, Shibasaki F. Hypoxia and angiogenesis: regulation of hypoxia-inducible factors via novel binding factors. Exp Mol Med. 2009;41(12):849–857. doi:10.3858/emm.2009.41.12.103.
15. Dvorak HF. Vascular permeability factor/vascular endothelial growth factor: a critical cytokine in tumor angiogenesis and a potential target for diagnosis and therapy. J Clin Oncol. 2002;20(21):4368–4380.
16. Wu Y, Jin M, Xu H, et al. Clinicopathologic significance of HIF-1α, CXCR4, and VEGF expression in colon cancer. Clin Dev Immunol. 2010;2010. doi:10.1155/2010/537531.
17. Barresi V, Di Gregorio C, Regiani-Bonetti L, Ponz-De Leon M, Barresi G, Vitarelli E. Stage I colorectal carcinoma: VEGF immunohistochemical expression, microvessel density, and their correlation with clinical outcome. Virchows Archiv. 2010;457(1):11–19. doi:10.1007/s00428-010-0933-5.
18. Kuijpers AMJ, Mirck B, Aalbers AGJ, et al. Cytoreduction and HIPEC in The Netherlands: Nationwide Long-term Outcome Following the Dutch Protocol. Ann Surg Oncol. July 2013. doi:10.1245/s10434-013-3145-9.
19. Kerkhof MH, Ruiz-Zapata AM, Bril H, et al. Changes in tissue composition of the vaginal wall of premenopausal women with prolapse. Am J Obstet Gynecol. 2014;210(2):168.e1–.e9. doi:10.1016/j.ajog.2013.10.881.
20. McShane LM, Altman DG, Sauerbrei W, et al. REporting recommendations for tumour MARKer prognostic studies (REMARK). British Journal of Cancer. 2005;93(4):387–391. doi:10.1038/sj.bjc.6602678.
21. Portilla AG, Shigeki K, Dario B, Marcello D. The intraoperative staging systems in the management of peritoneal surface malignancy. J Surg Oncol. 2008;98(4):228–231. doi:10.1002/jso.21068.
22. Avital IZ, Brücher BLDM, Nissan A, Stojadinovic A. Randomized clinical trials for colorectal cancer peritoneal surface malignancy. Surgical Oncology Clinics of North America. 2012;21(4):665–688. doi:10.1016/j.soc.2012.07.004.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
141
7
23. de Cuba EMV, Kwakman R, Knol DL, Bonjer HJ, Meijer GA, Velde te EA. Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases: Systematic review of all literature and meta-analysis of observational studies. Cancer Treatment Reviews. December 2012:1–7. doi:10.1016/j.ctrv.2012.11.003.
24. Du C, Yao Y, Xue W, Zhu W, Peng Y, Gu J. The expression of chemokine receptors CXCR3 and CXCR4 in predicting postoperative tumour progressionin stages I-II colon cancer:a retrospective study. BMJ Open. 2014;(4):1–6. doi:10.1136/bmjopen-2014-005012.
25. Chandler B, Detsika M, Khoo SH, Williams J, Back DJ, Owen A. Factors impacting the expression of membrane-bound proteins in lymphocytes from HIV-positive subjects. Journal of Antimicrobial Chemotherapy. 2007;60(3):685–689. doi:10.1093/jac/dkm230.
26. Furlan D, Sahnane N, Carnevali I, et al. Up-regulation and stabilization of HIF-1alpha in colorectal carcinomas. Surgical Oncology. 2007;16 Suppl 1:S25–S27. doi:10.1016/j.suronc.2007.10.014.
27. Blancher C, Moore JW, Talks KL, Houlbrook S, Harris AL. Relationship of hypoxia-inducible factor (HIF)-1alpha and HIF-2alpha expression to vascular endothelial growth factor induction and hypoxia survival in human breast cancer cell lines. Cancer Research. 2000;60(24):7106–7113.
28. Beasley NJP, Leek R, Alam M, et al. Hypoxia-inducible factors HIF-1alpha and HIF-2alpha in head and neck cancer: relationship to tumor biology and treatment outcome in surgically resected patients. Cancer Research. 2002;62(9):2493–2497.
29. Rohwer N, Dame C, Haugstetter A, et al. Hypoxia-inducible factor 1alpha determines gastric cancer chemosensitivity via modulation of p53 and NF-kappaB. PLoS ONE. 2010;5(8):e12038. doi:10.1371/journal.pone.0012038.
30. Koh MY, Spivak-Kroizman TR, Powis G. HIF-1alpha and cancer therapy. Recent Results Cancer Res. 2010;180:15–34. doi:10.1007/978-3-540-78281-0_3.
31. Goos JACM, de Cuba EMV, Coupé VMH, et al. Glucose Transporter 1 (SLC2A1) and Vascular Endothelial Growth Factor A (VEGFA) Predict Survival After Resection of Colorectal Cancer Liver Metastasis. Annals of Surgery. January 2015:1. doi:10.1097/SLA.0000000000001109.
32. Wehler TC, Graf C, Altherr K, et al. SDF1β expression in renal cell carcinoma correlates with grading and infiltration by CD8+ T-cells. Anticancer Res. 2011;31(9):2797–2803.
33. Mirisola V, Zuccarino A, Bachmeier BE, et al. CXCL12/SDF1 expression by breast cancers is an independent prognostic marker of disease-free and overall survival. Eur J Cancer. 2009;45(14):2579–2587. doi:10.1016/j.ejca.2009.06.026.
34. Bird NC, Mangnall D, Majeed AW. Biology of colorectal liver metastases: A review. J Surg Oncol. 2006;94(1):68–80. doi:10.1002/jso.20558.
35. Diniz Bizzo SM, Meira DD, Lima JM, Mororó JDS, Casali-da-Rocha JC, Ornellas MHF. Peritoneal VEGF burden as a predictor of cytoreductive surgery outcome in women with epithelial ovarian cancer. Int J Gynaecol Obstet. 2010;109(2):113–117. doi:10.1016/j.ijgo.2009.11.021.
36. Logan-Collins JM, Lowy AM, Robinson-Smith TM, et al. VEGF Expression Predicts Survival in Patients with Peritoneal Surface Metastases from Mucinous Adenocarcinoma of the Appendix and Colon. Ann Surg Oncol. 2007;15(3):738–744. doi:10.1245/s10434-007-9699-7.
37. Varghese S, Burness M, Xu H, Beresnev T, Pingpank J, Alexander HR. Site-Specific Gene Expression Profiles and Novel Molecular Prognostic Factors in Patients with Lower Gastrointestinal Adenocarcinoma Diffusely Metastatic to Liver or Peritoneum. Ann Surg Oncol. 2007;14(12):3460–3471. doi:10.1245/s10434-007-9557-7.
38. Harris AL. Hypoxia - a key regulatory factor in tumour growth. Nat Rev Cancer. 2002;2(1):38–47. doi:10.1038/nrc704.
39. Shaheen RM, Ahmad SA, Liu W, et al. Inhibited growth of colon cancer carcinomatosis by antibodies to vascular endothelial and epidermal growth factor receptors. British Journal of Cancer. 2001;85(4):584–589. doi:10.1054/bjoc.2001.1936.
40. Zebrowski BK, Liu W, Ramirez K, Akagi Y, Mills GB, Ellis LM. Markedly elevated levels of vascular endothelial growth factor in malignant ascites. Ann Surg Oncol. 1999;6(4):373–378.
41. Yoshikawa T, Tsuburaya A, Miyagi Y, et al. Up-regulation of hypoxia-inducible factor-1 alpha and VEGF mRNAs in peritoneal dissemination of patients with gastric cancer. Anticancer Res. 2006;26(5B):3849–3853.
42. Gerber SA, Rybalko VY, Bigelow CE, et al. Preferential Attachment of Peritoneal Tumor Metastases to Omental Immune Aggregates and Possible Role of a Unique Vascular Microenvironment in Metastatic Survival and Growth. The American Journal of Pathology. 2006;169(5):1739–1752. doi:10.2353/ajpath.2006.051222.

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
142
43. Imaizumi T, Aoyagi K, Miyagi M, Shirouzu K. Suppressive effect of bevacizumab on peritoneal dissemination from gastric cancer in a peritoneal metastasis model. Surg Today. 2010;40(9):851–857. doi:10.1007/s00595-009-4154-y.
44. Bai Y, Deng H, Yang Y, et al. VEGF-targeted short hairpin RNA inhibits intraperitoneal ovarian cancer growth in nude mice. Oncology. 2009;77(6):385–394. doi:10.1159/000279385.
45. Williams E, Martin S, Moss R, Durrant L, Deen S. Co-expression of VEGF and CA9 in ovarian high-grade serous carcinoma and relationship to survival. Virchows Archiv. 2012;461(1):33–39. doi:10.1007/s00428-012-1252-9.
46. Kobold S, Hegewisch-Becker S, Oechsle K, Jordan K, Bokemeyer C, Atanackovic D. Intraperitoneal VEGF inhibition using bevacizumab: a potential approach for the symptomatic treatment of malignant ascites? The Oncologist. 2009;14(12):1242–1251. doi:10.1634/theoncologist.2009-0109.
47. Ninomiya S, Inomata M, Tajima M, et al. Effect of bevacizumab, a humanized monoclonal antibody to vascular endothelial growth factor, on peritoneal metastasis of MNK-45P human gastric cancer in mice. J Surg Res. 2009;154(2):196–202. doi:10.1016/j.jss.2008.08.017.
48. Shah DK, Shin BS, Veith J, Tóth K, Bernacki RJ, Balthasar JP. Use of an anti-vascular endothelial growth factor antibody in a pharmacokinetic strategy to increase the efficacy of intraperitoneal chemotherapy. J Pharmacol Exp Ther. 2009;329(2):580–591. doi:10.1124/jpet.108.149443.
49. Passot G, Dupré A, Rivoire M, Mohamed F, Bakrin N, Glehen O. Intraperitoneal bevacizumab combined with cytoreductive surgery: a pre-clinical study of tolerance and pharmacokinetics in an animal model. Clin Transl Oncol. July 2012. doi:10.1007/s12094-012-0888-x.
50. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. doi:10.1056/NEJMoa032691.
51. Klaver YLB, Leenders BJM, Creemers G-J, et al. Addition of Biological Therapies to Palliative Chemotherapy Prolongs Survival in Patients With Peritoneal Carcinomatosis of Colorectal Origin. Am J Clin Oncol. February 2012. doi:10.1097/COC.0b013e3182438c55.
52. Ceelen W, Van Nieuwenhove Y, Putte DV, Pattyn P. Neoadjuvant Chemotherapy with Bevacizumab May Improve Outcome after Cytoreduction and Hyperthermic Intraperitoneal Chemoperfusion (HIPEC) for Colorectal Carcinomatosis. Ann Surg Oncol. 2014;21(9):3023–3028. doi:10.1245/s10434-014-3713-7.
53. Eveno C, Passot G, Goeré D, et al. Bevacizumab doubles the early postoperative complication rate after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol. 2014;21(6):1792–1800. doi:10.1245/s10434-013-3442-3.
54. van Dam GM, Themelis G, Crane LMA, et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-α targeting: first in-human results. Nature Medicine. September 2011:1–6. doi:10.1038/nm.2472.
55. Terwisscha van Scheltinga AGT, van Dam GM, Nagengast WB, et al. Intraoperative near-infrared fluorescence tumor imaging with vascular endothelial growth factor and human epidermal growth factor receptor 2 targeting antibodies. J Nucl Med. 2011;52(11):1778–1785. doi:10.2967/jnumed.111.092833.
56. Gaykema SBM, Brouwers AH, Lub-de Hooge MN, et al. 89Zr-bevacizumab PET imaging in primary breast cancer. J Nucl Med. 2013;54(7):1014–1018. doi:10.2967/jnumed.112.117218.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
143
7
Supplementary Data
HIF1
CXCR4 SDF1
VEGF
Angiogenesis
Progression
Proposed Interaction in PM Progression
Supplementary figure 1: Schematic representation of the interaction of the analyzed proteins; HIF1, CXCR4, SDF1 and VEGF
Supplementary figure 2: Kaplan-Meier curve total study cohort with follow-up (N=52)

Chapter 7 | Angiogenesis related markers and prognosis after CRS & HIPEC
144
TUMOR
STROMA
ADIPOSE TISSUE
Supplementary figure 3: Section of peritoneal metastases of colorectal cancer analyzed for micro-vessel density with CD31 expression
Supplementary table 1: Antibodies and Conditions used for the immunohistochemical stainings
Antibody Species Company Dilution Incubation Antigen retrieval Detection
HIF1a Mouse BD Pharmingen 1:500 30’ RT WB TRS 97 °C 45’ CSA
CXCR4 Rabbit SDIX 1:1000 o/n 4°C MW Citr 15’ Envision
SDF1 Mouse R&D Systems 1:400 o/n 4°C MW Citr 15’ Envision
VEGF Mouse DAKO 1:50 o/n 4°C MW Citr 15’ Powervision
CD31 Mouse DAKO 1:50 60’ RT MP Tris/EDTA 15’ Powervision
RT= Room temperature, o/n= overnight, WB= waterbath, MW=microwave Citr, TRS, Tris/ED=Citrate, TRIS and TRIS/ED buffer solution respectively.

Angiogenesis related markers and prognosis after CRS & HIPEC | Chapter 7
145
7
Supplementary Table 2: Univariate analysis of clinicopathological factors possibly influencing survival after CRS & HIPEC
Variable P-value
Gender
Age
Location Prim. Tumor
Tumor Type
T-classification Prim. Tumor
LN status
Timing PM
Simplified Peritoneal Cancer Index
Resection Outcome
Chemotherapy after CRS & HIPEC
NS
NS
NS
NS
NS
NS
NS
0.005
0.002
NS
NS = not significant, P>0.05


Chapter 8Glucose transporter 1 (SLC2A1) and
vascular endothelial growth factor A (VEGFA) predict survival after resection of colorectal
cancer liver metastasis
J.A.C.M. GoosE.M.V. de CubaV.M.H. CoupéB. DiosdadoP.M. Delis-Van DiemenC. KargaJ.A.M. BeliënW. Menke - Van der Houven van OordtA.A. GeldofG.A. MeijerO.S. HoekstraR.J.A. Fijneman
Ann Surg. 2016 Jan;263(1):138-45.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
148
Abstract
Background: In the majority of CRCLM patients, resection appears not to be curative, despite its curative intent. Overexpression of hypoxia-inducible factor 1α (HIF1α), glucose transporter 1 (SLC2A1; also known as GLUT1) and vascular endothelial growth factor A (VEGFA) have been associated with tumor progression and poor prognosis of CRC patients. The aim is to investigate the individual and combined prognostic value of HIF1α, SLC2A1 and VEGFA in a multi-institutional cohort of patients with resected colorectal cancer liver metastasis (CRCLM).
Methods: Tissue microarrays were generated using CRCLM and patient-matched primary CRC from patients who underwent CRCLM resection between 1990 and 2010. Prognostic value of HIF1α, SLC2A1 and VEGFA was determined by immunohistochemistry. A 500-fold cross-validated hazard rate ratio (HRRav) for overall survival was calculated.
Results: HIF1α, SLC2A1 and VEGFA expression could be evaluated in 328, 350 and 335 patients, respectively. High SLC2A1 expression was associated with good prognosis (HRRav0.67; P(HRR>1)<.01) and high VEGFA expression to poor prognosis (HRRav1.84; P(HRR<1)=.02), also after multivariate analysis including established clinicopathological prognostic variables (HRRav0.67; P(HRR>1)<.01 and HRRav1.50; P(HRR<1)=.02, respectively). SLC2A1 showed prognostic value particularly in patients treated with systemic therapy (P<.01), while the prognostic value of VEGFA expression was mainly observed in patients not treated with systemic therapy (P<.01). Prognosis was especially poor in patients with both low SLC2A1 and high VEGFA expression (P<.01). HIF1α expression was not associated with survival.
Conclusions: SLC2A1 and VEGFA expression are prognostic molecular biomarkers for CRCLM patients with added value to established clinicopathological variables.

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
149
8
Introduction
Approximately one out of two colorectal cancer (CRC) patients develop metastases during the course of disease, with dissemination to the liver in approximately 50-70% of cases.1 Historical five year survival rates of CRC patients with liver metastasis (CRCLM) did not exceed 10%.2 However, survival of CRCLM patients eligible for curative resection of the affected liver tissue, occasionally combined with radiofrequency ablation (RFA), has significantly improved.3 Selection of patients for CRCLM resection is based on clinicopathological prognostic parameters and staging including 18F-labeled fluorodeoxyglucose (18FDG) PET.4-6 Despite the significant improvements in CRC staging and therapy, only 36-58% of these patients will survive for more than five years after liver resection with curative intent, indicating that better prognostic biomarkers are needed.2,4 Hypoxia and hypoxia-inducible factors (HIF) are considered master regulators of metastasis. Activation of HIF1 has significant effects on several biological processes, in particular the metabolic shift in tumor cells from oxidative phosphorylation to glycolysis (i.e. Warburg effect), induction of angiogenesis, and increased metastasis.7-9 While HIF1α mRNA and protein expression levels are higher in primary CRC compared to normal colon tissue or adenomas, no clear relation between its expression and survival of CRC patients has been found. Moreover, its putative role as a prognostic biomarker seems to be inconsistent for different cancer types.10-12
The metabolic shift from aerobic oxidation to anaerobic glycolysis results in an increased cellular demand for glucose, which is achieved by increased expression of membranous glucose transporters. Overexpression of the solute carrier family 2 (facilitated glucose transporter), member 1 protein SLC2A1, also known as glucose transporter type 1 or GLUT1, is partly regulated by HIF1α and has been associated with tumor progression, metastasis and poor prognosis.10,13-17 18F-FDG PET imaging capitalizes on (deoxy)glucose uptake via SLC2A1, and increased tracer uptake in CRCLM has been associated with unfavorable outcome after resection.18
HIF1 activation also stimulates the release of the potent angiogenesis-stimulating factor vascular endothelial growth factor VEGF.19,20 VEGF expression is frequently elevated in tumor tissues and has been related to tumor progression, invasion and metastasis.21 Moreover, VEGF overexpression is an indicator of poor prognosis in various types of cancer.22,23 Therapeutic agents such as the monoclonal antibody bevacizumab specifically target VEGF, and addition of bevacizumab to conventional first-line therapy has significantly improved outcome of patients with advanced CRC.24 In addition, preoperative systemic therapy in combination with bevacizumab has improved radical resection rates and survival in patients with resectable CRCLM.25
This study retrospectively investigated the individual and combined prognostic value of HIF1α, SLC2A1 and VEGFA expression in various subgroups of patients with CRCLM and

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
150
assessed the added value of these molecular biomarkers to established clinicopathological prognostic parameters. Results were validated by a 500-fold cross-validation procedure.
Materials and methods
Patient study population
Formalin-fixed paraffin-embedded (FFPE) tissue samples were collected of patients who underwent CRCLM resection in seven Dutch hospitals affiliated with the DeCoDe PET group between 1990 and 2010. A detailed assembling procedure of the study population has been described previously.26,27 Summarized, tissue samples were collected from one histologically confirmed CRCLM specimen and an adjacent control liver tissue specimen. When available, also the corresponding primary tumor and adjacent control colon tissue were collected. Patients with multiple primary tumors were excluded. Collection, storage and use of clinicopathological data and tissue specimens were performed in compliance with the “Code for Proper Secondary Use of Human Tissue in The Netherlands”, and approved according to local and national regulations.28
Tissue microarrays
Tissue microarrays (TMAs) were generated according to protocols described previously.26,27,29 In brief, from morphologically representative areas of each FFPE donor block three core biopsies were taken (diameter 0.6 mm) and transferred into TMA recipient paraffin blocks using the 3DHISTECH TMA Master (v1.14, 3DHISTECH Ltd., Budapest, Hungary).
Immunohistochemistry
TMA sections of 4 μm were deparaffinized by xylene and rehydrated with a decreasing alcohol series. TMAs were immunohistochemically stained for HIF1α (1:500, mouse monoclonal antibody, BD Transduction Laboratories, Breda, The Netherlands) using catalyzed signal amplification (CSA) system (K1500, Dako, Heverlee, Belgium) as described previously.30 For the SLC2A1 staining, antigens were retrieved in citric acid (10mM, pH 6) by water bath (97°C) heating. Endogenous peroxidase quenching was performed in 0.3% hydrogen peroxidase in methanol for 25 minutes. Primary rabbit polyclonal antibody directed against human SLC2A1 (1:600, Abcam, Cambridge, United Kingdom) was incubated for 1 hour at room temperature and detected with secondary anti-rabbit antibodies (Envision Plus, Dako, Heverlee, Belgium). For VEGFA staining, antigen retrieval was performed in citric acid (10mM, pH 6) by microwave heating. Endogenous peroxidase quenching was performed as described above. Primary mouse monoclonal antibody directed against human VEGFA isoforms 121, 165 and 189 (1:50, DakoCytomation, Glostrup, Denmark)

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
151
8
was incubated overnight at 4°C. HRP-coupled polymers were used for primary antibody detection (Powervision, Dako, Heverlee, Belgium). Visualization was based upon liquid diaminobenzidine substrate chromogen system. Slides were counterstained with Mayer’s haematoxylin. FFPE renal cell carcinoma was stained as positive control for HIF1α expression and FFPE Caco-2 cells as positive controls for SLC2A1 and VEGFA expression. FFPE renal cell carcinoma and Caco-2 cells incubated without primary antibody served as negative controls.
Evaluation of protein expression
For digital capture of the immunohistochemical stainings, the Mirax slide scanner system was used, equipped with a 20x objective with a numerical aperture of 0.75 (Carl Zeiss B.V., Sliedrecht, The Netherlands) and a Sony DFW-X710 Fire Wire 1/3” type progressive SCAN IT CCD (pixel size 4.65 x 4.65µm), as described previously.26,27 Neoplastic epithelial cells in individual core biopsies were semiquantitatively scored for frequency (categories 0-25%, 26-50%, 51-75%, 76-100%) and intensity (categories negative, weak, moderate, strong) of nuclear HIF1α, membranous SLC2A1, and cytoplasmic VEGFA expression using dedicated TMA scoring software (v1.14.25.1, 3DHISTECH Ltd.,Budapest, Hungary). All core biopsies were independently evaluated by a second investigator, unaware of clinicopathological information at time of assessment (weighted kappa value Kw,HIF1α=0.85, Kw,SLC2A1=0.83 and Kw,VEGFA=0.78).
Statistical analysis
The prognostic value of protein expression was evaluated by 500-fold cross-validation.26,27 Per cross-validation cycle, the study population was randomly subdivided into a training and validation set of equal size. The optimal cut-off for dichotomizing scores in the training set into ‘low’ and ‘high’ expression was calculated using receiver operating characteristic (ROC) curve analysis for survival data with 3-year overall survival (OS) as the outcome of interest, resulting in a cut-off with best trade-off between sensitivity and specificity.31,32 This cut-off was then used to dichotomize scores of the corresponding validation set and the crude hazard rate ratio (HRR) was calculated in a Cox regression analysis with OS as outcome. Furthermore, per cycle a HRR was calculated upon addition of the following established clinicopathological prognostic variables in a multivariate Cox regression analysis: primary tumor-to-CRCLM interval < 12 months, lymph node positivity at time of diagnosis of the primary tumor, maximal CRCLM diameter > 5.0 cm, number of CRCLM > 1 and serum CEA level > 200 ng/ml.33 The average cross-validated hazard rate ratio (HRRav) was calculated from the 500-fold cross-validation procedure. In addition, the probability of having an actual HRR with opposite effect of the cross-validated HRRav was also calculated (i.e. P(HRR>1) for HIF1α and SLC2A1; P(HRR<1) for VEGFA). OS was

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
152
defined as the time in months after surgery until death in a follow-up period of 10 years. The relation between protein expression and OS in the total patient population and several patient subgroups was visualized by Kaplan Meier curves and a P-value was calculated by logrank testing, using the most frequently selected cut-off in the cross-validation procedure as the optimal cut-off for dichotomization. Correlations between proteins were calculated using Pearson’s chi-square test and combined prognostic value of the three markers was assessed by stepwise backward regression analysis, also including the clinicopathological variables, with P>.1 as exclusion criterion. Excluded from analyses were patients who died within 2 months after liver resection, when no data was available on survival status or time of survival, or when tissue cores were non-evaluable due to technical reasons (Fig. 1). All statistical tests were two-sided with P values considered significant when <.05. All data reported was REMARK compliant.34 Statistical analyses were performed using IBM SPSS Statistics 20.0 software (SPSS Inc., Illinois, USA) and R Statistics 3.0.1 software (RStudio Inc., Boston, USA).
CRC patients having had liver resection between 1990 and 2010 (n=507)
Excluded due to technical
reasons (n=71)
Excluded due to technical
reasons (n=49)
Excluded due to technical
reasons (n=64)
Available for HIF1αevaluation (n=328)
Available for SLC2A1evaluation (n=350)
Available for VEGFA evaluation (n=335)
CRCLM patients available for analysis (n=399)
Excluded from analysis (n=108)• Survival less than 2 months (n=61)• Unknown outcome or time of survival (n=47)
Figure 1: Flow diagram of the study cohort. A total of 507 patients with resectable CRCLM were available to the current study population. After exclusion of patients with OS shorter than 2 months, unknown outcome or OS or due to technical reasons, 328 patients remained available for evaluation of HIF1α expression, 350 patients for evaluation of SLC2A1 expression and 335 patients for evaluation of VEGFA expression

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
153
8
Results
Prognostic value of HIF1α, SLC2A1 and VEGFA
A total of 507 patients with resectable CRCLM were available to the current study population. CRCLM tissue was obtained from all patients and from 234 patients matched primary tumor tissue was also available. Cumulative five-year OS of the study population was 41.2% (Supplemental Digital Content 1). Characteristics of the study population have been extensively described previously; a summary of patient characteristics is given in Supplemental Digital Content 2.26,27
Expression of HIF1α, SLC2A1 and VEGFA in CRCLM was visualized by immunohistochemistry (Fig. 2). Intensity and frequency of stained CRCLM epithelial cells were evaluated for nuclear HIF1α expression in 328 patients (Fig. 1 and Supplemental Digital Content 3). The cross-validation procedure indicated a trend between high frequency of nuclear HIF1α expression and increased OS (HRRav 0.80; P(HRR>1)=.06; Supplemental Digital Content 4A), also upon inclusion of the established clinicopathological variables in a multivariate analysis (HRRav 0.77; P(HRR>1)=.06; Supplemental Digital Content 4B). Upon dichotomization of the whole study cohort using the most frequently selected cut-off for HIF1α expression in the 500 training sets (Supplemental Digital Content 5A), the cumulative median OS of patients with low HIF1α expression was 45 months and of patients with high HIF1α expression 52 months (P=.18, Fig. 3A). Intensity scores of nuclear HIF1α expression were not associated with OS (data not shown).For 350 patients, immunohistochemical staining of CRCLM epithelial cells was scored for intensity and frequency of membranous SCL2A1 expression (Fig. 1 and Supplemental Digital Content 3). OS of patients with high intensity scores for SLC2A1 expression was better than of patients with low SLC2A1 expression (HRRav 0.67; P(HRR>1)<.01; Supplemental Digital Content 4C). Prognostic value of SLC2A1 expression was hardly confounded by the standard clinical and pathological prognostic variables (HRRav 0.65; P(HRR>1)<.01; Supplemental Digital Content 4D). After dichotomization for SLC2A1 expression (Supplemental Digital Content 5B), cumulative median OS of patients with low and high SLC2A1 expression was 44 months and 55 months, respectively (P=.01; Fig. 3B). Frequency scores of SLC2A1 expression on membranes of CRCLM cells were not associated with OS (data not shown). VEGFA immunohistochemical staining was scored based on its cytoplasmic expression in neoplastic CRCLM epithelium in 335 patients (Fig. 1 and Supplemental Digital Content 3). High intensity scores of VEGFA expression were associated with decreased OS (HRRav 1.48; P(HRR<1)=.02; Supplemental Digital Content 4E). Inclusion of VEGFA expression in a multivariate analysis together with the established clinicopathological variables also demonstrated its independent association with poor prognosis (HRRav 1.50;

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
154
P(HRR<1)=.02; Supplemental Digital Content 4F). After dichotomization for VEGFA expression (Supplemental Digital Content 5C), cumulative median OS of patients with low cytoplasmic VEGFA levels was 61 months and of patients with high cytoplasmic VEGFA levels 35 months (P<.01; Fig. 3C). Frequency scores of cytoplasmic VEGFA expression were not associated with OS (data not shown).
Figure 2: Staining examples of (A) low HIF1α expression, (B) high HIF1α expression , (C) low SLC2A1 expression, (D) high SLC2A1 expression, (E) low VEGFA expression and (F) high VEGFA expression in epithelium of CRCLM
Prognostic value of HIF1α, SLC2A1 and VEGFA expression in patient subgroups
The prognostic value of the dichotomized scores for HIF1α, SLC2A1 and VEGFA expression in CRCLM was evaluated separately for patients with colon and rectal cancer. No association was found between HIF1α expression and OS, neither in colon cancer patients (P=.54; Supplemental Digital Content 6A) nor in rectal cancer patients (P=.12; Supplemental Digital Content 6D). A statistically non-significant trend was observed for the association between high SLC2A1 expression and OS in both colon and rectal cancer patients (P=.08; Supplemental Digital Content 6B and P=.09; Supplemental Digital Content

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
155
8
6E, respectively). High VEGFA expression in CRCLM was significantly associated with decreased OS in colon cancer patients (P<.01; Supplemental Digital Content 6C), but not in rectal cancer patients (P=.21; Supplemental Digital Content 6F).Next, prognostic value was evaluated separately in patients either or not treated with systemic therapy perioperative to CRCLM resection (Supplemental Digital Content 7). In neither subgroup HIF1α expression was related to OS (P=.12; Fig. 3D and P=.46; Fig. 3G, respectively). High levels of SLC2A1 expression were not associated with OS in patients not treated with systemic therapy (P=.20; Fig. 3E), but were associated with increased OS in patients treated with systemic therapy (P<.01; Fig. 3H). High VEGFA expression in CRCLM was associated with poor OS in patients who were not treated with systemic therapy (P<.01; Fig. 3F), but not in patients who were treated with systemic therapy (P=.16; Fig. 3I).
Combined prognostic value of HIF1α, SLC2A1 and VEGFA expression
Considering the biological relation between expression of HIF1, SLC2A1, and VEGFA, we investigated the potential added value of combining individual markers. HIF1α expression was significantly associated with SLC2A1 expression (P=.02; Supplemental Digital Content 8). VEGFA expression was not associated with either HIF1α (P=.12) or SLC2A1 expression (P=.85). In the multivariate Cox regression analysis, with OS as dependent variable and HIF1α, SLC2A1 and VEGFA expression as well as the established prognostic clinicopathological variables as independent variables, only SLC2A1 expression (HRR 0.66, 95%CI 0.43-1.00, P=.05) and VEGFA expression (HRR 1.53, 95%CI 1.01-2.32, P=.04) were retained in the final model (Supplemental Digital Content 9). Prognosis of patients having CRCLM with low SLC2A1 and high VEGFA expression levels was significantly worse compared to patients having CRCLM with high SLC2A1 and low VEGFA levels (P<.01; Fig. 4A). Moreover, combining SLC2A1 and VEGFA expression increased the OS difference between these subgroups both in patients who were not treated with systemic therapy (P<.01; Fig. 4B) and in patients who were treated with systemic therapy (P=.01; Fig. 4C).
HIF1α, SLC2A1 and VEGFA expression in patient-matched primary CRC and CRCLM
HIF1α, SLC2A1 and VEGFA expression could be compared for 155, 160 and 135 pairs of matched primary CRC and CRCLM tissue specimens, respectively (Supplemental Digital Content 10 and Supplemental Digital Content 11). HIF1α scores were concordant for 55.5% of primary CRC-CRCLM pairs (P=.54). SLC2A1 scores were concordant in 56.8% (P=.09) and VEGFA scores in 54.1% (P=.44) of CRC-CRCLM pairs. When pairs of primary CRC and matched synchronous or metachronous CRCLM were evaluated

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
156
separately, scores were similarly concordant (data not shown). Preoperative systemic therapy might affect tissue characteristics at time of surgery, however, when only patients were considered not treated with systemic therapy within six months prior to either primary CRC or CRCLM resection, scores were similarly concordant (Supplementary Table S7).
Figure 3: Kaplan-Meier graphs depicting OS in months for (A,B,C) the total study population, (D,E,F) patients in which CRCLM were not treated with systemic therapy and (G,H,I) patients in which CRCLM were treated with systemic therapy. OS was stratified by (A,D,G) HIF1α expression, (B,E,H) SLC2A1 expression and (C,F,I) VEGFA expression. Information of systemic therapy was unavailable for n=13, n=12 and n=10 patients of whom tissue samples were evaluated for HIF1α, SLC2A1 and VEGFA expression, respectively. P-values were calculated using the logrank test

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
157
8
Figure 4: Kaplan-Meier graph depicting OS in months stratified by combinations of SLC2A1 and VEGFA expression in CRCLM for (A) the total study population, (B) patients who were not treated with systemic therapy and (C) patients who were treated with systemic therapy. HRR compares patients with high SLC2A1 and low VEGFA expression with patients with low SLC2A1 and high VEGFA expression. P-values were calculated using the logrank test.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
158
Discussion
We investigated the prognostic value of HIF1α, SLC2A1 and VEGFA protein expression in a large series of patients with resectable CRCLM. With 500-fold cross-validation, we demonstrated that high expression of SLC2A1 in CRCLM epithelial cells was an indicator of good prognosis. High levels of VEGFA in CRCLM epithelium, on the other hand, were associated with decreased OS. In patients in whom SCL2A1 expression was low and VEGFA expression was high, prognosis was even worse. Expression of HIF1α was not significantly related to OS. The difference in cumulative median OS between patients with low and high expression was 11 months for SLC2A1 and 26 months for VEGFA. Multivariate analysis including HIF1α, SLC2A1 or VEGFA expression with established clinicopathological prognostic variables, such as lymph node positivity, presence of more than a single CRCLM, maximal CRCLM diameter larger than 5.0cm, serum CEA level higher than 200ng/ml, presentation of CRCLM within 12 months after diagnosis of the primary tumor, did not substantially affect the associations between protein expression and OS.It has been proposed that hypoxia plays a less prominent role in the development of CRCLM than of primary CRC, particularly for the outer cells of a metastatic lesion, since the liver has great vascular density.35 HIF-negative tumor cells behave more aggressively in hypoxic environments than HIF1-competent cells, as they become independent of angiogenic blood supply and therefore increase their anti-apoptotic and cell survival capabilities.36-39 This may explain the trend between low HIF1α expression and decreased OS and the association between low SLC2A1 expression, which positively correlated to HIF1α expression, and decreased OS. Although overexpression of HIF1α has been associated with increased survival in a variety of cancer types, amongst which prostate, head and neck, lung, ovarian and oral squamous cell carcinomas, no such conclusion could be drawn in the study population under investigation.11,37,40,41 Possibly, the actual prognostic value of HIF1α – and potentially also of SLC2A1 – in our study population has been somewhat underestimated. These proteins generally show focal, perinecrotic expression patterns and such immunohistochemical staining patterns are less easy to interpret when using TMAs compared to when using full tissue sections.10 Alternatively, although cells with a glycolytic phenotype have a selective advantage in metastasis, it has been demonstrated that the transition from aerobic to anaerobic metabolism is most relevant during early stages of tumor development.9,13 Therefore, the prognostic effects of HIF1α expression may be more prominent in early stage disease than in advanced disease, because its effects in metastatic lesions may become obscured by additional somatic alterations. In primary CRC patients, VEGFA overexpression has been linked to decreased survival in numerous studies and we now show that expression of VEGFA is also related to decreased survival in resectable CRCLM.22 The lack of correlation between VEGFA expression

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
159
8
and either HIF1α or SLC2A1 expression indicates that the prognostic value of VEGFA expression in CRCLM could largely be attributed to HIF1alpha-independent activation of VEGFA through other (oncogenic) pathways, such as via KRAS, PDGF or TGFβ signaling. Disruption of KRAS in human colon carcinoma cells has been associated with decreased VEGF activity, however, the clinical relevance of this relation has not yet been determined as efficacy of treatment with bevacizumab could not be predicted based on KRAS status.42,43 Correspondingly, although it has been demonstrated that VEGF RNA expression levels increased upon the introduction of PDGF and TGFβ to vascular cells, neither PDGF nor TGFβ protein expression has been associated with prediction of bevacizumab therapy response.44,45 Alternatively, increased expression of SLC2A1 or VEGFA might partly be a result of activation of the upstream effector HIF2α, rather than of HIF1α. Although HIF2α expression in CRC has conflictingly been associated with tumor progression, it might explain the contrasting prognostic effect of SLC2A1 and VEGFA expression observed in the current study. 46,47 Further investigation is required to confirm the correlations that might exist between these markers and the proteins under investigation. We also evaluated the potential to predict biomarker expression in CRCLM based on its expression level in matched primary CRC samples, since alterations occurring during carcinogenesis of the primary tumor are often maintained in corresponding CRCLM.48,49 For none of the proteins, however, expression was correlated between the primary tumor and matched CRCLM. Similar to hypoxia, it has been suggested that angiogenesis is less pronounced in CRCLM compared to primary CRC.35,50-52 This may explain the lack of correlation between expression of the biomarkers investigated in this study in primary CRC and corresponding CRCLM and could imply that determination of their expression in CRCLM, but not in the primary tumor, may be clinically useful. Molecular imaging can provide such information, which emphasizes its potential as added tool for preoperative assessment of patient eligibility for CRCLM resection.SLC2A1 expression showed similar prognostic value in both CRCLM originating from colon and rectal cancer. For VEGFA expression, the prognostic value appeared to be limited to colon cancer patients. It has been shown that VEGFA expression levels commonly are different for tumors in the proximal and distal parts of the colorectum.53 Additionally, VEGFA expression levels are generally lower in colon tumors with high level microsatellite instability (MSI), which are more common in the right colon.54,55 This might speculate that VEGFA expression plays a different role in the carcinogenesis of tumors in different parts of the large intestine and could explain why VEGFA expression only has prognostic value in colon cancer patients, but not in rectal cancer patients. Unfortunately, the MSI status was not known for the patients evaluated in our study, so we could not further investigate its potential confounding effect on the prognostic value of VEGFA. However, only 3% of CRCLM is estimated to be MSI and, as such, MSI is suggested only to play a minor role in CRCLM compared to primary CRC.56

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
160
Considering treatment with systemic therapy, SLC2A1 expression appeared to be associated with OS mainly in patients treated with systemic therapy. Tumor cells responding to therapeutic agents are usually cells with a higher metabolic rate than cells which are in a quiescent-like state.57-59 Highly active tumor cells have enhanced glycolytic capacity, which results in an upregulation of membranous SLC2A1 to meet the increasing demand for glucose.60,61 Overexpression of SLC2A1 in CRCLM may thus indicate a higher susceptibility of tumor cells to treatment with systemic therapy and therefore be a predictor of good prognosis specifically in this patient subgroup. VEGFA expression appeared to be a prognostic biomarker only in patients who were not treated with systemic therapy. This may indicate that conventional systemic therapies affect VEGFA-related biological processes, improving survival of patients with a poor prognosis. Addition of bevacizumab to standard systemic therapy regimens has greatly improved outcome.24,25 Although response to bevacizumab treatment could not be predicted based on VEGFA expression,62 VEGFA levels appeared to be reduced significantly following treatment with the antibody.63 In the present study population, 29 patients had been treated with bevacizumab (Supplemental Digital Content 7), of whom VEGFA expression could be evaluated in 20 patients (Supplemental Digital Content 12). Excluding these patients from survival analysis effectively improved the prognostic value of VEGFA expression (P<.01), suggesting that treatment with bevacizumab improves survival especially of patients with high VEGFA expression. In addition to the assessment of VEGFA expression in CRCLM tissue, it may also be of interest to assess VEGFA levels in the circulation. Unfortunately, such data was not available for the patients in the current study. Our results show that the combination of low SLC2A1 and high VEGFA expression in CRCLM was associated with poor prognosis, independent of treatment with systemic therapy. Therefore, assessment of SLC2A1 levels on top of VEGFA expression in CRCLM may improve outcome by selecting patients eligible for CRCLM resection and, furthermore, selecting patients highly expressing both VEGFA and SLC2A1 as best candidates for additional systemic treatment. Assessment of biomarker expression in vivo is commonly performed by molecular imaging modalities, such as PET. Tracers generally associated with SLC2A1 expression are already used in clinical PET (i.e. 18FDG) and addition of specific VEGFA tracers (e.g. 89Zr-bevacizumab) are used to visualize VEGFA expression. Currently, patients are often selected for CRCLM resection using 18FDG PET imaging, which may cause a selection bias in the study population under investigation. That is, increased SLC2A1 expression in CRCLM may result in increased uptake of 18FDG. In such cases, occult CRCLM are more likely to be discovered and subsequently resected, which may result in a favorable prognosis of these patients. Nevertheless, high uptake of 18FDG in CRCLM has previously also been related to worse outcome.18 However, it is not clear to which extent increased

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
161
8
tracer uptake is caused by epithelial cells or stromal cells, like macrophages; the latter generally also have a high glucose consumption, and high macrophage infiltration has been related to tumor cell survival in late stage disease.64,65 As many other factors next to SLC2A1 expression affect uptake of 18FDG, it remains questionable if SLC2A1 expression could be proportionally associated with 18FDG uptake.66 In conclusion, expression of SLC2A1 and VEGFA are biomarkers for outcome after CRCLM resection. Combined, expression of these proteins can be used to predict survival irrespective of systemic treatment. Further research is needed to externally validate our results and to explore possibilities to stratify patients based on SLC2A1, but also on VEGFA expression levels, for example via ex vivo evaluation of tumor tissue.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
162
References1. Welch JP, Donaldson GA. The clinical correlation
of an autopsy study of recurrent colorectal cancer. Ann Surg 1979; 189:496-502.
2. Leporrier J, Maurel J, Chiche L et al. A population-based study of the incidence, management and prognosis of hepatic metastases from colorectal cancer. Br J Surg 2006; 93:465-474.
3. Cunningham D, Atkin W, Lenz HJ et al. Colorectal cancer. Lancet 2010; 375:1030-1047.
4. Spolverato G, Ejaz A, Azad N et al. Surgery for colorectal liver metastases: The evolution of determining prognosis. World J Gastrointest Oncol 2013; 5:207-221.
5. Spelt L, Andersson B, Nilsson J et al. Prognostic models for outcome following liver resection for colorectal cancer metastases: A systematic review. Eur J Surg Oncol 2012; 38:16-24.
6. Ruers TJM, Wiering B, van der Sijp JRM et al. Improved selection of patients for hepatic surgery of colorectal liver metastases with (18)F-FDG PET: a randomized study. J Nucl Med 2009; 50:1036-1041.
7. Lu X, Kang Y. Hypoxia and hypoxia-inducible factors: master regulators of metastasis. Clin Cancer Res 2010; 16:5928-5935.
8. Dewhirst MW, Cao Y, Moeller B. Cycling hypoxia and free radicals regulate angiogenesis and radiotherapy response. Nat Rev Cancer 2008; 8:425-437.
9. Gatenby RA, Gillies RJ. Why do cancers have high aerobic glycolysis? Nat Rev Cancer 2004; 4:891-899.
10. Greijer AE, Delis-van Diemen PM, Fijneman RJA et al. Presence of HIF-1 and related genes in normal mucosa, adenomas and carcinomas of the colorectum. Virchows Arch 2008; 452:535-544.
11. Semenza GL. Targeting HIF-1 for cancer therapy. Nat Rev Cancer 2003; 3:721-732.
12. Mabjeesh NJ, Amir S. Hypoxia-inducible factor (HIF) in human tumorigenesis. Histol Histopathol 2007; 22:559-572.
13. de Wit M, Jimenez CR, Carvalho B et al. Cell surface proteomics identifies glucose transporter type 1 and prion protein as candidate biomarkers for colorectal adenoma-to-carcinoma progression. Gut 2012; 61:855-864.
14. Younes M, Lechago LV, Lechago J. Overexpression of the human erythrocyte glucose transporter occurs as a late event in human colorectal carcinogenesis and is associated with an increased incidence of lymph node metastases. Clin Cancer Res 1996; 2:1151-1154.
15. Haber RS, Rathan A, Weiser KR et al. GLUT1 glucose transporter expression in colorectal carcinoma: a marker for poor prognosis. Cancer 1998; 83:34-40.
16. Shen Y, Arbman G, Olsson B et al. Overexpression of GLUT1 in colorectal cancer is independently associated with poor prognosis. Int J Biol Markers 2011; 26:166-172.
17. Wood SM, Wiesener MS, Yeates KM et al. Selection and analysis of a mutant cell line defective in the hypoxia-inducible factor-1 alpha-subunit (HIF-1alpha). Characterization of hif-1alpha-dependent and -independent hypoxia-inducible gene expression. J Biol Chem 1998; 273:8360-8368.
18. Riedl CC, Akhurst T, Larson S et al. 18F-FDG PET scanning correlates with tissue markers of poor prognosis and predicts mortality for patients after liver resection for colorectal metastases. J Nucl Med 2007; 48:771-775.
19. Pugh CW, Ratcliffe PJ. Regulation of angiogenesis by hypoxia: role of the HIF system. Nat Med 2003; 9:677-684.
20. Giles RH, Lolkema MP, Snijckers CM et al. Interplay between VHL/HIF1alpha and Wnt/beta-catenin pathways during colorectal tumorigenesis. Oncogene 2006; 25:3065-3070.
21. Pavlidis ET, Pavlidis TE. Role of bevacizumab in colorectal cancer growth and its adverse effects: a review. World J Gastroenterol 2013; 19:5051-5060.
22. Des Guetz G, Uzzan B, Nicolas P et al. Microvessel density and VEGF expression are prognostic factors in colorectal cancer. Meta-analysis of the literature. Br J Cancer 2006; 94:1823-1832.
23. Asghar U, Hawkes E, Cunningham D. Predictive and prognostic biomarkers for targeted therapy in metastatic colorectal cancer. Clin Colorectal Cancer 2010; 9:274-281.
24. Hurwitz HI, Tebbutt NC, Kabbinavar F et al. Efficacy and safety of bevacizumab in metastatic colorectal cancer: pooled analysis from seven randomized controlled trials. Oncologist 2013; 18:1004-1012.
25. Gruenberger T, Arnold D, Rubbia-Brandt L. Pathologic response to bevacizumab-containing chemotherapy in patients with colorectal liver metastases and its correlation with survival. Surg Oncol 2012; 21:309-315.
26. Goos JACM, Coupe VMH, Diosdado B et al. Aurora kinase A (AURKA) expression in colorectal cancer liver metastasis is associated with poor prognosis. Br J Cancer 2013; 109:2445-2452.

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
163
8
27. Goos JACM, Hiemstra AC, Coupe VMH et al. Epidermal growth factor receptor (EGFR) and prostaglandin-endoperoxide synthase 2 (PTGS2) are prognostic biomarkers for patients with resected colorectal cancer liver metastases. Br J Cancer 2014; 111:749-755.
28. Stichting FMWV. Code Goed Gebruik van lichaamsmateriaal 2011. 2011. Ref Type: Internet Communication
29. Simon R, Mirlacher M, Sauter G. Tissue microarrays. Biotechniques 2004; 36:98-105.
30. Bos R, Zhong H, Hanrahan CF et al. Levels of hypoxia-inducible factor-1 alpha during breast carcinogenesis. J Natl Cancer Inst 2001; 93:309-314.
31. Zlobec I, Steele R, Terracciano L et al. Selecting immunohistochemical cut-off scores for novel biomarkers of progression and survival in colorectal cancer. J Clin Pathol 2007; 60:1112-1116.
32. Heagerty PJ, Zheng Y. Survival model predictive accuracy and ROC curves. Biometrics 2005; 61:92-105.
33. Fong Y, Fortner J, Sun RL et al. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg 1999; 230:309-318.
34. McShane LM, Altman DG, Sauerbrei W et al. Reporting recommendations for tumor marker prognostic studies. J Clin Oncol 2005; 23:9067-9072.
35. Richard DE, Berra E, Pouyssegur J. Angiogenesis: how a tumor adapts to hypoxia. Biochem Biophys Res Commun 1999; 266:718-722.
36. Furlan D, Sahnane N, Carnevali I et al. Up-regulation and stabilization of HIF-1alpha in colorectal carcinomas. Surg Oncol 2007; 16 Suppl 1:S25-S27.
37. Beasley NJP, Leek R, Alam M et al. Hypoxia-inducible factors HIF-1alpha and HIF-2alpha in head and neck cancer: relationship to tumor biology and treatment outcome in surgically resected patients. Cancer Res 2002; 62:2493-2497.
38. Rohwer N, Dame C, Haugstetter A et al. Hypoxia-inducible factor 1alpha determines gastric cancer chemosensitivity via modulation of p53 and NF-kappaB. PLoS One 2010; 5:e12038.
39. Blancher C, Moore JW, Talks KL et al. Relationship of hypoxia-inducible factor (HIF)-1alpha and HIF-2alpha expression to vascular endothelial growth factor induction and hypoxia survival in human breast cancer cell lines. Cancer Res 2000; 60:7106-7113.
40. Weber DC, Tille JC, Combescure C et al. The prognostic value of expression of HIF1alpha, EGFR and VEGF-A, in localized prostate cancer for intermediate- and high-risk patients treated with radiation therapy with or without androgen deprivation therapy. Radiat Oncol 2012; 7:66.
41. Fillies T, Werkmeister R, van Diest PJ et al. HIF1-alpha overexpression indicates a good prognosis in early stage squamous cell carcinomas of the oral floor. BMC Cancer 2005; 5:84.
42. Rak J, Mitsuhashi Y, Bayko L et al. Mutant ras oncogenes upregulate VEGF/VPF expression: implications for induction and inhibition of tumor angiogenesis. Cancer Res 1995; 55:4575-4580.
43. Garcia-Alfonso P, Grande E, Polo E et al. The role of antiangiogenic agents in the treatment of patients with advanced colorectal cancer according to K-RAS status. Angiogenesis 2014.
44. Brogi E, Wu T, Namiki A et al. Indirect angiogenic cytokines upregulate VEGF and bFGF gene expression in vascular smooth muscle cells, whereas hypoxia upregulates VEGF expression only. Circulation 1994; 90:649-652.
45. Bruhn MA, Townsend AR, Khoon Lee C et al. Proangiogenic tumor proteins as potential predictive or prognostic biomarkers for bevacizumab therapy in metastatic colorectal cancer. Int J Cancer 2014; 135:731-741.
46. Xue X, Taylor M, Anderson E et al. Hypoxia-inducible factor-2alpha activation promotes colorectal cancer progression by dysregulating iron homeostasis. Cancer Res 2012; 72:2285-2293.
47. Imamura T, Kikuchi H, Herraiz MT et al. HIF-1alpha and HIF-2alpha have divergent roles in colon cancer. Int J Cancer 2009; 124:763-771.
48. Knijn N, Mekenkamp LJM, Klomp M et al. KRAS mutation analysis: a comparison between primary tumours and matched liver metastases in 305 colorectal cancer patients. Br J Cancer 2011; 104:1020-1026.
49. Stange DE, Engel F, Longerich T et al. Expression of an ASCL2 related stem cell signature and IGF2 in colorectal cancer liver metastases with 11p15.5 gain. Gut 2010; 59:1236-1244.
50. Garcea G, Lloyd TD, Gescher A et al. Angiogenesis of gastrointestinal tumours and their metastases--a target for intervention? Eur J Cancer 2004; 40:1302-1313.
51. Wali RK, Roy HK, Kim YL et al. Increased microvascular blood content is an early event in colon carcinogenesis. Gut 2005; 54:654-660.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
164
52. Mooteri S, Rubin D, Leurgans S et al. Tumor angiogenesis in primary and metastatic colorectal cancers. Dis Colon Rectum 1996; 39:1073-1080.
53. Bendardaf R, Buhmeida A, Hilska M et al. VEGF-1 expression in colorectal cancer is associated with disease localization, stage, and long-term disease-specific survival. Anticancer Res 2008; 28:3865-3870.
54. Hollingsworth SJ, Drye ER, Tou SIH et al. Expression of angiogenic VEGF-A (soluble isoforms 121, 165) and lymphangiogenic VEGF-C in colorectal cancers with micro-satellite instability. J Surg Oncol 2005; 92:317-325.
55. Lynch HT, de la Chapelle A. Genetic susceptibility to non-polyposis colorectal cancer. J Med Genet 1999; 36:801-818.
56. Haddad R, Ogilvie RT, Croitoru M et al. Microsatellite instability as a prognostic factor in resected colorectal cancer liver metastases. Ann Surg Oncol 2004; 11:977-982.
57. Blagosklonny MV. Target for cancer therapy: proliferating cells or stem cells. Leukemia 2006; 20:385-391.
58. Singh A, Settleman J. EMT, cancer stem cells and drug resistance: an emerging axis of evil in the war on cancer. Oncogene 2010; 29:4741-4751.
59. Creighton CJ, Li X, Landis M et al. Residual breast cancers after conventional therapy display mesenchymal as well as tumor-initiating features. Proc Natl Acad Sci U S A 2009; 106:13820-13825.
60. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011; 144:646-674.
61. Lindeman GJ, Visvader JE. Insights into the cell of origin in breast cancer and breast cancer stem cells. Asia Pac J Clin Oncol 2010; 6:89-97.
62. Jubb AM, Hurwitz HI, Bai W et al. Impact of vascular endothelial growth factor-A expression, thrombospondin-2 expression, and microvessel density on the treatment effect of bevacizumab in metastatic colorectal cancer. J Clin Oncol 2006; 24:217-227.
63. Pohl M, Werner N, Munding J et al. Biomarkers of anti-angiogenic therapy in metastatic colorectal cancer (mCRC): original data and review of the literature. Z Gastroenterol 2011; 49:1398-1406.
64. Kubota R, Kubota K, Yamada S et al. Microautoradiographic study for the differentiation of intratumoral macrophages, granulation tissues and cancer cells by the dynamics of fluorine-18-fluorodeoxyglucose uptake. J Nucl Med 1994; 35:104-112.
65. Gil-Bernabe AM, Ferjancic S, Tlalka M et al. Recruitment of monocytes/macrophages by tissue factor-mediated coagulation is essential for metastatic cell survival and premetastatic niche establishment in mice. Blood 2012; 119:3164-3175.
66. Bos R, van Der Hoeven JJM, van Der Wall E et al. Biologic correlates of (18)fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J Clin Oncol 2002; 20:379-387.

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
165
8
Supplementary table S1: Patient Characteristics
Total Population Total Population
Clinicopathological variablen
/ mean/ median
%/ st.dev./ range
Clinicopathological variablen
/ mean/ median
%/ st.dev./ range
General characteristics Liver metastasis characteristics
All 507 Age at liver resection
Gender mean (st.dev.) 63.3 0.5
male (%) 320 63.1 median (range) 64.3 27.6-83.9
female (%) 187 36.9 Synchronous liver metastasis Δ
OS after liver resection in months yes (%) Δ 221 43.6
mean (st.dev.) 37.2 1.7 no (%) Δ 261 51.5
median (range) 27 3.0-212.0 unknown (%) Δ 25 4.9
Distribution liver metastases
left half 90 17.8
Primary CRC characteristics segment 1 (%) 18 3.6
Age at primary CRC resection segment 2 (%) 116 22.9
mean (st.dev.) 61.9 0.5 segment 3 (%) 135 26.6
median (range) 62.8 24.4-83.3 segment 4 (%) 134 26.4
Primary tumor location right half 259 51.0
left colon (%) 245 48.3 segment 5 (%) 171 33.7
right colon (%) 95 18.7 segment 6 (%) 212 41.8
rectum (%) 151 29.8 segment 7 (%) 211 41.6
unknown (%) 16 3.2 segment 8 (%) 182 35.9
Histological grade both left and right half 146 28.8
poorly differentiated (%) 38 7.5 unknown 12 2.4
moderately differentiated (%) 288 56.8 Maximal CRCLM diameter in cm Δ
well-differentiated (%) 14 2.8 mean (st.dev.) 4.1 0.1
unknown (%) 167 32.9 median (range) 3.5 0.2-22.0
Maximal CRC diameter in cm maximal diameter ≤ 5.0 cm (%) Δ 372 73.4
mean (st.dev.) 4.4 0.1 maximal diameter > 5.0 cm (%) Δ 126 24.8
median (range) 4 0.2-12.0 maximal diameter unknown (%) Δ 9 1.8
Positive lymph nodes detected Δ Number of CRCLM Δ
yes (%) Δ 190 37.5 mean (st.dev.) 2 0.1
no (%) Δ 154 30.4 median (range) 2 1-12
unknown (%) Δ 163 32.1 nr of CRCLM = 1 (%) Δ 248 48.9

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
166
Supplementary Table S1: Continued
Total Population Total Population
Clinicopathological variablen
/ mean/ median
%/ st.dev./ range
Clinicopathological variablen
/ mean/ median
%/ st.dev./ range
Systemic treatment of primary CRC nr of CRCLM > 1 (%) Δ 253 49.9
colon cancer nr of CRCLM unknown (%) Δ 6 1.2
preoperative (%) 9 2.6 Serum CEA level Δ
perioperative (%) 0 0 mean (st.dev.) 101.6 38.5
postoperative (%) 91 26.8 median (range) 15 0.5-6625.0
none (%) 226 66.5 serum CEA level ≤ 200 ng/ml (%) Δ 166 32.7
unknown (%) 14 4.1 serum CEA level > 200 ng/ml (%) Δ 13 2.6
rectal cancer serum CEA level unknown (%) Δ 328 64.7
preoperative (%) 25 16.5 Extrahepatic metastases
perioperative (%) 1 0.7 yes (%) 36 7.1
postoperative (%) 24 15.9 no (%) 423 83.4
none (%) 98 64.9 unknown (%) 48 9.5
unknown (%) 3 2 Resection in combination with RFA
primary tumor location unknown yes (%) 109 21.5
preoperative (%) 1 6.3 no (%) 357 70.4
perioperative (%) 0 0.0 unknown (%) 41 8.1
postoperative (%) 1 6.3 Systemic treatment of liver metastases
none (%) 12 75.0 preoperative (%) 60 11.8
unknown (%) 2 12.5 perioperative (%) 12 2.4
Radiotherapeutic treatment of primary CRC postoperative (%) 97 19.1
yes (%) 113 22.3 none (%) 321 63.3
no (%) 392 77.3 unknown (%) 17 3.4
unknown (%) 2 0.4OS: overall survival; CEA: carcino-embryonic antigen; RFA: radiofrequency ablation; Δ Clinical risk score variable [2]

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
167
8
Supplementary Table S2: Distribution of scores
Total Population
Frequency score n %
HIF1α
0-25% 226 68.9
26-50% 56 17.1
51-75% 20 6.1
76-100% 26 7.9
SLC2A1
0-25% 278 79.4
26-50% 42 12.0
51-75% 16 4.6
76-100% 14 4.0
VEGFA
0-25% 139 41.5
26-50% 59 17.6
51-75% 22 6.6
76-100% 115 34.3
Intensity score n %
HIF1α
negative 50 15.2
weak 124 37.8
moderate 63 19.2
strong 91 27.8
SLC2A1
negative 93 26.6
weak 35 10.0
moderate 43 12.3
strong 179 51.1
VEGFA
negative 14 4.2
weak 79 23.6
moderate 141 42.1
strong 101 30.1

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
168
Supplementary Table S3: Systemic therapy and decade of liver resection [26]
1990-2010 1990-1999 2000-20101990-1999
vs. 2000-2010
Clinicopathological variable n* % n % n % P
All 507 106 398
CRCLM treated with systemic therapy 169 33.3 22 20.8 146 36.7 .001
5FU only 6 3.6 3 13.6 3 2.1 .08
5FU + Leucovorin 39 23.1 16 72.7 22 15.1 .001
5FU + Leucovorin + Oxaliplatin 15 8.9 0 0.0 15 10.3 .04
5FU + Leucovorin + Irinotecan 2 1.2 0 0.0 2 1.4 .47
5FU + Leucovorin + other 1 0.6 0 0.0 1 0.7 .61
5FU + other 1 0.6 1 4.5 0 0.0 .05
Capecitabine only 7 4.1 0 0.0 7 4.8 .17
Capecitabine + Oxaliplatin 40 23.7 0 0.0 40 27.4 .001
Capecitabine + Oxaliplatin + Bevacizumab 27 16.0 0 0.0 27 18.5 .006
Capecitabine + Oxaliplatin + Bevacizumab + Cetuximab 2 1.2 0 0.0 2 1.4 .47
Capecitabine + Oxaliplatin + other 3 1.8 0 0.0 3 2.1 .37
Capecitabine + other 6 3.6 2 9.1 4 2.7 .46
Chemotherapeutic agent unknown 20 11.8 0 0.0 20 13.7 .02* Decade of liver resection unknown for n=3 patients, of which n=1 patient received systemic therapy.

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
169
8
Supplementary Table S4: Level of concordance between biomarker expression. Correlation of expression was calculated using chi-square testing.
low SLC2A1
high SLC2A1
Total
P=.02
low HIF1α
n = 14135.6%
n = 13032.8%
n = 27168.4%
high HIF1α
n = 4912.4%
n = 7619.2%
n = 12552.0%
Total n = 19048.0%
n = 20652.0%
n = 396
low VEGFA
high VEGFA
Total
P=.12
low HIF1α
n = 18447.4%
n = 7820.1%
n = 26267.5%
high HIF1α
n = 9825.3%
n = 287.2%
n = 12632.5%
Total n = 28272.7%
n = 10627.3%
n = 388
low SLC2A1
high SLC2A1
Total
P=.85
low VEGFA
n = 14635.4%
n = 15337.1%
n = 29972.6%
high VEGFA
n = 5413.1%
n = 5914.3%
n = 11327.4%
Total n = 20048.5%
n = 21251.5%
n = 412
Supplementary Table S5: Multivariate Cox regression analysis.
Covariate HRR 95%CI P
primary tumor-to-CRCLM interval < 12 months 1.12 0.74-1.70 .60
lymph node positivity at time of diagnosis of the primary tumor 1.45 0.95-2.21 .09
maximal CRCLM diameter > 5.0 cm 1.22 0.77-1.94 .40
number of CRCLM > 1 1.28 0.85-1.94 .25
serum CEA level > 200 ng/ml 0.80 0.55-1.17 .26
HIF1α expression 0.84 0.54-1.31 .44
SLC2A1 expression 0.66 0.43-1.00 .05
VEGFA expression 1.53 1.01-2.32 .04
HRR: hazard rate ratio; 95%CI: 95% confidence interval

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
170
Supplementary Table S6: Level of concordance between biomarker expression in primary CRC and corresponding CRCLM. Correlation of expression was calculated using chi-square testing.
expression in primary CRC Chi square
expr
essi
on in
CR
C li
ver
met
asta
ses
HIF1α low high Total
P=.54
low n = 6642.6%
n = 4629.7%
n = 11272.3%
high n = 2314.8%
n = 2012.9%
n = 4327.7%
Total n = 8957.4%
n = 6642.6%
n = 155
SLC2A1 low high Total
P=.09
low n = 5735.6%
n = 2515.6%
n = 8251.2%
high n = 4427.5%
n = 3421.2%
n = 7848.8%
Total n = 10163.1%
n = 5936.9%
n = 160
VEGFA low high Total
P=.44
low n = 5238.5%
n = 4331.9%
n = 9570.4%
high n = 1914.1%
n = 2115.6%
n = 4029.6%
Total n = 7152.6%
n = 6447.4%
n = 135

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
171
8
Supplementary Table S7: Level of concordance between biomarker expression in primary CRC and corresponding CRCLM of patients that were not treated with systemic therapy within six months preoperative to primary tumor resection and/or liver resection. Correlation of expression was calculated using chi-square testing.
expression in primary CRC Chi square
expr
essi
on in
CR
C li
ver
met
asta
ses
HIF1α low high Total P=.31
low n = 5141.5%
n = 3226.0%
n = 8367.5%
high n = 2217.9%
n = 1814.6%
n = 4032.5%
Total n = 7359.3%
n = 5040.7%
n = 123
SLC2A1 low high Total P=.19
low n = 4937.7%
n = 2317.7%
n = 7255.4%
high n = 3325.4%
n = 2519.2%
n = 5844.6%
Total n = 8263.1%
n = 4836.9%
n = 130
VEGFA low high Total P=.13
low n = 4339.1%
n = 3935.5%
n = 8274.5%
high n = 109.1%
n = 1816.4%
n = 2825.5%
Total n = 5348.2%
n = 5751.8%
n = 110

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
172
Supplementary Figure S1. Kaplan-Meier graph depicting OS in months of the total study
population. Patients with OS less than 2 months and unknown outcome or time of OS were
removed from analysis [26].
Supplementary Figure S1: Kaplan-Meier graph depicting OS in months of the total study population. Patients with OS less than 2 months and unknown outcome or time of OS were removed from analysis [26].

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
173
8
Supplementary Figure S2. Distribution of the cross-validated HRRs after (A) univariate analysis of HIF1α expression, (B) multivariate analysis of HIF1α expression, (C) univariate analysis of SLC2A1 expression, (D) multivariate analysis of SLC2A1 expression, (E) univariate analysis of VEGFA expression and (F) multivariate analysis of VEGFA expression with OS as outcome.
Supplementary Figure S2: Distribution of the cross-validated HRRs after (A) univariate analysis of HIF1α expression, (B) multivariate analysis of HIF1α expression, (C) univariate analysis of SLC2A1 expression, (D) multivariate analysis of SLC2A1 expression, (E) univariate analysis of VEGFA expression and (F) multivariate analysis of VEGFA expression with OS as outcome.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
174
Supplementary Figure S3. Distribution of the selected cut-off points for frequency and
intensity scores in the training sets of (A) HIF1α expression, (B) SLC2A1 expression and (C)
VEGFA expression. Cut-off points for (A) frequency scores are (1) 1-25% vs. 26-100%, (2)
1-50% vs. 51-100%, (3) 1-75% vs. 76-100% and for (B,C) intensity scores (1) negative vs.
Supplementary Figure S3: Distribution of the selected cut-off points for frequency and intensity scores in the training sets of (A) HIF1α expression, (B) SLC2A1 expression and (C) VEGFA expression. Cut-off points for (A) frequency scores are (1) 1-25% vs. 26-100%, (2) 1-50% vs. 51-100%, (3) 1-75% vs. 76-100% and for (B,C) intensity scores (1) negative vs. weak, moderate, strong, (2) negative, weak vs. moderate, strong, (3) negative, weak, moderate vs. strong. Stainings were dichotomized using the most frequently selected cut-off in the training sets.

GLUT1 and VEGFA predict survival after resection of CRLM | Chapter 8
175
8
Supplementary Figure S4. Kaplan-Meier graphs depicting OS in months for (A,B,C,)
patients with CRCLM originating from colon cancer and (D,E,F) patients with CRCLM
originating from rectal cancer. OS was stratified by (A,D) HIF1α expression, (B,E) SLC2A1
expression and (C,F) VEGFA expression. Origin of primary tumor (colon or rectum) was
unkown for n=8, n=5 and n=7 patients of whom tissue samples were evaluated for HIF1α,
Supplementary Figure S4: Kaplan-Meier graphs depicting OS in months for (A,B,C,) patients with CRCLM originating from colon cancer and (D,E,F) patients with CRCLM originating from rectal cancer. OS was stratified by (A,D) HIF1α expression, (B,E) SLC2A1 expression and (C,F) VEGFA expression. Origin of primary tumor (colon or rectum) was unknown for n=8, n=5 and n=7 patients of whom tissue samples were evaluated for HIF1α, SLC2A1 and VEGFA expression, respectively. P-values were calculated using the logrank test.

Chapter 8 | GLUT1 and VEGFA predict survival after resection of CRLM
176
CRC patients having had liver resection between 1990 and 2010 (n=507)
Excluded due to technical
reasons (n=79)
Excluded due to technical
reasons (n=74)
Excluded due to technical
reasons (n=99)
Available for HIF1αcorrelation analysis
(n=155)
Available for SLC2A1 Available for VEGFA
Primary CRC specimens unavailable (n=273)
correlation analysis (n=160)
correlation analysis (n=135)
Supplementary Figure S5. Flow diagram of patients of whom primary tumor specimens were available.
Supplementary Figure S6. Kaplan-Meier graphs depicting OS in months, stratified by
VEGFA expression for (A) patients in which CRCLM were not treated with Bevacizumab
and (B) patients in which CRCLM were treated with Bevacizumab. Information of treatment
with Bevacizumab was unavailable for n=10 patients of whom tissue samples were evaluated
for VEGFA expression.
Supplementary Figure S6: Kaplan-Meier graphs depicting OS in months, stratified by VEGFA expression for (A) patients in which CRCLM were not treated with Bevacizumab and (B) patients in which CRCLM were treated with Bevacizumab. Information of treatment with Bevacizumab was unavailable for n=10 patients of whom tissue samples were evaluated for VEGFA expression.
References1. Goos JACM, Coupe VMH, Diosdado B, Delis-
Van Diemen PM, Karga C, Belien JAM, et al. Aurora kinase A (AURKA) expression in colorectal cancer liver metastasis is associated with poor prognosis. Br J Cancer 2013;109:2445-2452.
2. Fong Y, Fortner J, Sun RL et al. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg 1999; 230:309-318.

Chapter 9Tailoring heated intraperitoneal Mitomycin C
for peritoneal metastases originating from colorectal carcinoma
A translational approach to improve survival
R. Kwakman*E.M.V. de Cuba*J.P. de Winter†I.H.J.T. de HinghP.M. Delis-van DiemenM. TijssenM.A. RooimansO. KrijgsmanB. CarvalhoG.J. PetersH.J. BonjerG.A. MeijerE.A. te Velde *Both authors contributed equally to this manuscript † Deceased
Br J Cancer. 2015 Mar 3;112(5):851-6

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
178
Abstract
Background: Patients with peritoneal metastases (PM) originating from colorectal carcinoma (CRC) are curatively treated by cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) with Mitomycin C (MMC). We aim to improve patient selection for HIPEC by predicting MMC sensitivity.
Methods: MMC sensitivity was determined for twelve CRC cell lines and correlated to mRNA expression of thirty-seven genes related to the Fanconi Anaemia(FA)-BRCA pathway, ATM-ATR pathway and enzymatic activation of MMC. Functionality of the FA-BRCA pathway in cell lines was assessed using a chromosomal breakage assay and Western Blot for key protein FANCD2. Bloom syndrome protein (BLM) was further analysed by staining for the corresponding protein with immunohistochemistry (IHC) on both CRC cell lines (n=12) and patient material (n=20).
Results: High sensitivity correlated with a low BLM (p=0.01) and BRCA2 (p=0.02) at mRNA expression level. However, FA-BRCA pathway functionality demonstrated no correlation to MMC sensitivity. In cell lines, weak intensity staining of BLM by IHC correlated to high sensitivity (p=0.04) to MMC. Low BLM protein expression was significantly associated to an improved survival in patients after CRS and HIPEC (p=0.04).
Conclusion: Low BLM levels are associated with high MMC sensitivity and an improved survival after HIPEC.

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
179
9
Introduction
Mitomycin C (MMC) is used for hyperthermic intraperitoneal chemotherapy (HIPEC), which combined with cytoreductive surgery (CRS), comprises the treatment of patients with peritoneal metastases (PM) originating from colorectal carcinoma (CRC) (Chua et al, 2012a). Due to the characteristics of PM, CRS will leave microscopic disease in situ, hence requiring HIPEC with MMC (Elias et al, 2012, Chua et al, 2012b). MMC is the drug of choice because of the direct cytotoxicity and the penetrance of only 1 to 2 mm(Cerretani et al, 2005, Van der Speeten et al, 2009) This is thought to cause minimal systemic side effects, while still eliminating minimal residual disease after CRS(van Ruth et al, 2003). A randomized clinical trial (RCT) in 2003 showed an median overall survival of 22.4 months in patients treated with HIPEC with MMC versus 12.6 months in patients treated with systemic chemotherapy alone (Verwaal et al, 2008). Several other clinical trials followed, revealing a comparable survival gain, with one trial even showing a median overall survival of 62 months (Cao et al, 2009, Glehen et al, 2004, de Cuba et al, 2013). Even when patients are stratified according to the extent of metastasis and residual disease after resection, a subset of patients have decreased survival, giving rise to our hypothesis that these patients might respond differently to MMC (Verwaal et al, 2008, Glehen et al, 2004). If identified, these patients could benefit from an altered approach with optimised tailored treatment with alternative drugs that are readily available and clinically applicable in the HIPEC setting, such as oxaliplatin, irinotecan and doxorubicin (Van der Speeten et al, 2009, Kusamura et al, 2008, Chua et al, 2012a).
MMC functions by intercalating or cross-linking DNA and creating DNA damage, disrupting DNA replication, heralding mitosis and ultimately leading to apoptosis (Szybalski and Iyer, 1964). The cancer cell has several ways of evading and/or repairing MMC-induced damage. One possible way is to inhibit MMC activation as MMC requires enzymatic reduction to become active (Cummings et al, 1998). Several reductases have this capacity, with DT-diaphorase being the most potent and widely researched (Szybalski and Iyer, 1964, Plumb and Workman, 1994, Fitzsimmons et al, 1996, Misra et al, 2002). Absence of this enzyme has been known to lead to increased resistance to MMC in cancer cells (Fitzsimmons et al, 1996). Another way for cancer cells to overcome MMC-induced damage is to repair this damage. This can be facilitated by either the Fanconi Anaemia-BRCA (FA-BRCA) pathway or the ATM-ATR pathway, which in turn both regulate the RAD51C Nuclear foci to mediate repair by homologous recombination or nucleotide excision repair (Figure 1) (D’Andrea and Grompe, 2003, Takemura et al, 2006). Theoretically, if either of these pathways remain intact or even hyperactivated, MMC-related DNA damage could be partially repaired and some degree of resistance can be expected, whereas a non-functional pathway may lead to MMC sensitivity as seen in lymphoblasts derived from FA patients

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
180
(Auerbach, 2009, Oostra et al, 2012). A similar principle has been exposed before in non-small cell lung carcinoma, where the knock-out of the FA-BRCA pathway led to a 3 to 5 fold increase in sensitivity to cisplatin, which bears some resemblance to MMC (Ferrer et al, 2004).
Double-strandbreak
RecruitmentofFAcorecomplex
proteins
Phosphorylati onofFANCD2
ActivationofBRCA2-RAD51C
Homologousrepair
ActivationofATM-ATR
CellcyclearrestthroughCHK1/2
andP53
ActivationofMRNcomplex
RAD50-RAD51activationNuceotide
excisionrepair
FA-BRCApathway
ATM-ATRpathway
ActiveMMC
MMC
DT-diaphoraseXanthinehydrogenase
P450cytochromeoxidorectaseNADH-cytochromeb5reductase
MMC activationenzymes
Figure 1: Activation of MMC and repair mechanisms of double-strand breaks. Both the FA-BRCA pathway and the ATM-ATR pathway are illustrated in summary. FA-BRCA and ATM-ATR pathways have common proteins and intersect on several levels (Kim and D’Andrea, 2012, Chen and Poon, 2008, Cummings et al, 1998, Kitagawa and Kastan, 2005)
With a mortality ranging from 3-5% and a morbidity ranging from 15% to 50%, it is necessary to select patients who will benefit maximally from CRS with HIPEC and exclude patients whose survival gain does not outweigh the treatment associated morbidity and mortality (Cao et al, 2009, Bretcha-Boix et al, 2010, Mizumoto et al, 2012, Rouers et al, 2006). However, no predictive biomarkers have been found to date that complement the clinical characteristics known to predict outcome (de Cuba et al, 2012). The aim of this study is to characterize biomarkers that predict treatment response to MMC in patients

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
181
9
receiving HIPEC for PM of CRC in order to tailor treatment and subsequently improve survival post-CRS and HIPEC.
Materials and methods
Cell lines and drug sensitivity
Twelve CRC cell lines: HCT116, HCT15, Colo205, Colo320, SW480, SW48, SW1398, CaCo-2, HT-29, LS174T, RKO and LIM1863, were kindly provided by the Tumor Profiling Unit of the Dept. of Pathology of VU University Medical Center. All cell lines, except LIM1863, were obtained from American Type Culture Collection (LGC Standards GmbH, Wesel, Germany). LIM1863 was kindly provided by Dr. R.H. Whitehead from the Ludwig Institute for Cancer Ltd (Melbourne branch) (Whitehead et al, 1987). The cell lines were routinely authenticated on the basis of aCGH copy number profile, viability, growth rate and morphology by microscopic examination. Drug sensitivity of cell lines was determined by the SRB assay (Bijnsdorp et al, 2010). The IC50 values were extracted from the produced graphs. Experiments were conducted in triplicate and the mean of the three experiments is shown. In order to assess FA-BRCA pathway functionality, negative and positive controls VU1131-T2-8 and VU1131-T2-8 +FANCC cell lines were taken along in the analysis. We categorised cell lines as sensitive, intermediate and resistant in comparison to control cell lines.
Expression Array
RNA was isolated of all 12 CRC cell lines(Ambion Inc, Austin, Texas, USA). Synthesis and cDNA labelling were performed according to the manufacturer’s recommendations including QC (Agilent Technologies, Palo Alto, CA, USA). Hybridization was performed on single 44K formatted expression arrays containing 41 675 60-mer oligonucleotides representing over 27 000 well-characterized full-length or partial human genes and expressed sequence tag clusters (G4112A, Agilent Technologies). Scanning was performed using a microarray scanner G2505B (Agilent Technologies) and Feature Extraction v9.5 using the manufacturers protocols (Agilent Technologies). LIMMA-package was used for of background correction, loss within array normalization and quantile between-array normalization (Smyth et al, 2005). Thirty-seven genes and their mRNA products related to the FA-BRCA pathway, ATM-ATR pathway and/or enzymatic MMC activation were selected based on literature and pathway analysis (Kim and D’Andrea, 2012, Chen and Poon, 2008, D’Andrea and Grompe, 2003, Takemura et al, 2006, Fitzsimmons et al, 1996, Cummings et al, 1998) and subsequently correlated to MMC sensitivity.

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
182
FA-BRCA pathway status – Chromosomal Breakage Assay and Western Blot
FA-BRCA pathway functionality was tested with a chromosomal breakage assay (Oostra et al, 2012). Instead of venous blood described in the abovementioned protocol, trypsinized cell cultures were used. Four slides were prepared per cell line, with MMC addition and without MMC. Metaphases were analysed using MetaphaseFinder and scored by an experienced technician. Fanconi anemia complementation group D2 protein (FANCD2) was analysed by Western blotting in MMC-sensitive cell lines (Ferrer et al, 2004). Western blot was performed using an FANCD2 mouse antibody (F17, Santa Cruz biotechnology Inc., Heidelberg, Germany) diluted at 1:500 in 2% dry milk in TBST and a peroxidase-conjugated anti-mouse immunoglobulin diluted at 1:5000 in 2% dry milk in TBST. Cells were treated with hydroxyurea to determine FA pathway activation by monoubiquitination of FANCD2 in response to DNA damage.
Immunohistochemistry
Immunohistochemistry was performed on 4 μm slides from FFPE blocks containing embedded CRC cell lines. Slides were stained using the HIER pH6 protocol, as described by the manufacturer. Rabbit anti-BLM antibody (Sigma-Aldrich co. LLC), obtained via the Human Protein Atlas (HPA), was utilized in dilution of 1:200 and subsequently incubated for 1 hour at room temperature. This antibody has been validated in previous research.(Lao et al, 2013) Secondary antibody PowerVision Poly-HRP anti-Rabbit/Mouse/Rat antibody (Leica Biosystems BV) was used. Scoring was performed with simple light microscopy and scored by two independent microscopists. As described by HPA, normal liver tissue was used as negative control and placental tissue as positive control. Patient material
All consecutive patients from a prospectively collected cohort in 2007-2010 undergoing CRS and HIPEC in an expert HIPEC centre (Catharina Hospital Eindhoven) with standardized treatment were investigated for BLM expression (n=33). Only patients with histologically confirmed diagnosis PM of CRC were included. Tumour samples with less than 70% tumour tissue were excluded after staining. Immunohistochemistry was performed with the same protocol as described above. Patient data were subsequently stratified by resection outcome and only R1 outcome, microscopic minimal residual disease (Verwaal et al, 2008), was included in survival analysis (n=20). Median follow-up was 35.3 months with a minimum of 24 months and a maximum of 64 months. Collection, storage and use of tissue and patient data were performed in accordance with the Code for Proper Secondary Use of Human Tissue in the Netherlands.

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
183
9
Statistical analysis
SPSS (version 17; IBM Corporation) was used to analyse results. We used linear regression to find a correlation between expression data and clustered sensitivity data. Correlation between clustered sensitivity and immunohistochemistry was assessed using a Chi-square test. Patient survival was analysed according to the Kaplan-Meier method. For all mentioned tests, a p value of less than 0.05 was considered significant.
Results
MMC sensitivity
The IC50 for each cell line was clustered into sensitive (0-50 nM; n=1), intermediate (50-200 nM; n=7) and resistant (>200 nM; n=4). Doubling time and MSS/MSI status did not correlate to sensitivity.
mRNA Expression
mRNA expression of thirty-seven genes related to the FA-BRCA, ATM-ATR and MMC activation pathway were analysed for a correlation with clustered sensitivity (Supplementary Table 1). BLM demonstrated a significant correlation with sensitivity at mRNA level (p = 0.01) as well as BRCA2 (p=0.02). Both BLM and BRCA2 were observed to be upregulated in the resistant cell lines (Figure 2). FANCD2 expression, as key protein in the FA-BRCA pathway, displayed no significant correlation with clustered sensitivity. None of the genes of the ATM-ATR pathway or any of the activation enzymes exhibited any correlation to clustered MMC sensitivity (See supplementary data). Combined expression levels of BLM and BRCA2 demonstrated no better correlation (p=0.01) than BLM alone. Multivariate analysis was not possible due to limited sample size.
FA-BRCA functionality
Representative cell lines of each sensitivity cluster (sensitive: SW48; intermediate: SW1398, LS174T; resistant: HCT15) were selected for chromosomal breakage assay. Over 90% of positive control cells (VU1131-T2-8) displayed more than 10 breaks per cell, consistent with a non-functional FA-BRCA pathway. Over 80% of negative control cells (VU1131-T2-8 + FANCC) showed less than three breaks per cells. SW48, HCT15 and LS174T were comparable with the negative control (over 80% of cells with less than three breaks) (Supplementary figure 1A). SW1398 exhibited slightly more breaks, yet demonstrated in over 80% of the cells less than five breaks and was considered negative for chromosomal breakage.

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
184
Figure 2: BLM and BRCA2 expression correlated to sensitivity to MMC. Resistant cell lines show higher levels of BLM expression (p=0.01) and higher levels of BRCA2 expression (p=0.02)
Sensitive cell line SW48 expressed a FANCD2 band on Western blot, indicating the presence of the FANCD2 protein, as well as a darker second band with slower mobility after 24h hydroxyurea treatment, illustrating that FANCD2 could be mono-ubiquitinated and thus be activated (Supplementary figure 1B).
Immunohistochemistry on Bloom Syndrome Protein (BLM)
Immunohistochemical staining revealed nuclear and less intense cytoplasmatic staining with significant intratumour heterogeneity, in concordance with previous studies(Suzuki et al, 2001). Considering the nuclear propensity of active BLM and the most active part of the tumour dictating the ultimate response, the strongest nuclear component of staining was scored and used for analysis. Intensity was scored as negative, weak, moderate or strong (Figure 3). Interobserver variability was less than 5%. We observed no correlation between mRNA and staining intensity. Correlation between clustered sensitivity and separate staining intensity was not significant (p=0.17). However, negative and weak intensity versus moderate and strong intensity was significantly associated with high versus low sensitivity (p = 0.04). In patient material, twenty out of 33 patient samples were selected by R1 resection outcome. Six patient samples were scored with low intensity (negative plus weak) and 14 patient samples with high intensity (moderate plus strong) for BLM protein (Figure 4). Median survival for R1 patients was 23 months (95% CI: 11.5 – 34.5). A significant longer survival was found in favour of low BLM expression (high: 15 mths[11.3 – 18.7] vs. low: NR; p=0.04) (Figure 5).

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
185
9
a. b.
c. d.
e. f.
Figure 3: Immunohistochemistry on BLM. a, b and c, blanco, negative (liver) and positive (placenta) controls respectively at 10x objective magnification. d, SW48 with weak staining (25x objective magnification). e, HT29 with moderate staining (25x objective magnification). f, Strong staining on Colo205 (25x objective magnification)
Negative Weak Moderate Strong
Low High
BLM staining
Figure 4: Immunohistochemistry on patient material for BLM. From left to right: negative, weak, moderate and strong intensity staining (25x objective magnification). Negative and weak were clustered for analysis into ‘low’ as well as moderate and strong into ‘high’. Low vs. high was significantly correlated to survival (p=0.04)

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
186
Figure 5: Kaplan-Meier curve of patients with a R1 outcome resection. Patients with a low BLM protein expression demonstrate significant better survival than patients with a high BLM protein expression (p=0.04)
Discussion
In this study, we demonstrate an association of low BLM with a high sensitivity to MMC and an improved survival. Considering BLM is linked to the FA-BRCA pathway, which is known to play a role in MMC sensitivity, this association seems not unexpected.
In order to select a potential biomarker, we investigated expression levels of 37 different genes involved in the FA-BRCA, ATM-ATR and MMC activation pathways, together responsible for both the activation of MMC and repairing MMC-induced damage, in association to the MMC sensitivity in 12 CRC cell lines. A significantly higher mRNA expression of both BRCA2 and BLM were found in cell lines resistant to MMC. We found that sensitivity to MMC not only associates to BLM on mRNA level, but also to BLM on protein level. Immunohistochemical analysis of BLM protein correlated to MMC sensitivity in our 12 CRC cell lines. Furthermore, in a prospectively collected cohort of patients with minimal residual disease after CRS, treated with HIPEC using MMC, BLM protein expression was associated with a decreased overall survival.
We linked MMC sensitivity to BLM and BRCA2, which strongly suggests a role for the FA-BRCA pathway in the development of chemoresistance in CRC, yet the chromosomal breakage assay demonstrated no dysfunction of the FA-BRCA pathway in CRC cell lines

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
187
9
of any MMC sensitivity level. Concordantly, we observed no association to FANCD2 mRNA or protein expression. This leads to the conclusion that although BLM correlates with MMC sensitivity, this seems to have no implications for the function of DNA repair of the FA-BRCA pathway. It appears that the FA-BRCA pathway can function with either decreased expression levels or is of only limited importance in the development of resistance to MMC in CRC. Hypothetically, the FA-BRCA pathway itself may not be involved in the mechanism dictating response to MMC, but the molecules involved could rather represent surrogate markers for another, still unidentified, pathway that interacts with both BRCA2 and BLM. Perhaps the increased genomic instability as mediated by low levels of BRCA2 and BLM leads to increased sensitivity to DNA cross-linking agents such as MMC. Discrepancies between mRNA and IHC we found in two cell lines, could be due to post-translational modifications. This complex process, consisting of several interacting proteins, is known to mediate protein expression and often relays mRNA expression in different levels of protein expression(Gomes et al, 2014).
Sensitivity to MMC is known to be correlated to DT-diaphorase, encoded by the NQO1 gene (Sharp et al, 2000, Fitzsimmons et al, 1996, Misra et al, 2002), yet the DT-diaphorase overexpressing cell line HT-29 is only intermediately sensitive in our cohort and none of the mRNA products of the MMC activation pathway were significantly correlated to MMC sensitivity. Activation of MMC by DT-diaphorase might be of inferior importance in sensitivity in CRC cell lines, perhaps due to the abundance of other MMC-activating enzymes in human cells, which readily transform MMC to its active metabolite (Cummings et al, 1998, Phillips et al, 2000).
BLM itself is a RecQ helicase that is primarily responsible for unwinding DNA and is known to participate in the BASC complex with BRCA1, the MRN complex (containing RAD50, MRE11 and NBS1) and interact directly with FANCD2 (Karow et al, 1997, Wang et al, 2000, Nimonkar et al, 2011, Ellis et al, 1995). On a cellular level, BLM is involved in stalled replication fork repair, homologous repair, non-homologous end joining and nucleotide excision repair (Pichierri et al, 2004, Davalos et al, 2004, Bischof et al, 2001, Sengupta et al, 2003). In contrast to several other DNA repair genes i.e. BRCA2, the clinical implications of altered BLM expression have not been as well-established in cancer (Colavito et al, 2010, Sitzmann and Wiebke, 2013, Liu et al, 2012, Zhang et al, 2009). Even though clinical data is scarce, an important characteristic of BLM is its required activation for repair of DNA double-strand breaks, inducible by intercalating agents such as MMC (Langland et al, 2002). Accordingly, a knock-down of BLM in cell lines sensitizes these cells to cisplatin and camptothecin, indicating again the importance BLM in chemotherapeutic response and its possible clinical relevance (Mao et al, 2010).

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
188
In order to further characterize the role of BLM, RNA knockdown experiments in association with investigation of DNA repair proteins could be the next step. Another approach includes proteomics specifically targeting low-abundance nuclear proteins in order to determine the role of BLM in the development of resistance to cross-linking agents such as MMC in CRC cell lines. The results generated by proteomics should then subsequently be validated in a well-defined CRS and HIPEC cohort from an expert HIPEC centre. The ultimate clinical goal is to be able to differentiate between responders and non-responders to MMC. Non-responders could then be treated with an alternative intraperitoneal compound. We conclude that MMC sensitivity in CRC is associated with BLM expression. We are the first to have found a possible predictive biomarker for PM with CRC and suggest further validation of BLM as a biomarker for treatment stratification prior to CRS and HIPEC.

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
189
9
References1. Auerbach AD (2009) Fanconi anemia and its
diagnosis Mutat Res 668: 4-10.2. Bijnsdorp IV, Kruyt FA, Fukushima M, Smid K,
Gokoel S, Peters GJ (2010) Molecular mechanism underlying the synergistic interaction between trifluorothymidine and the epidermal growth factor receptor inhibitor erlotinib in human colorectal cancer cell lines Cancer Sci 101: 440-7.
3. Bischof O, Kim SH, Irving J, Beresten S, Ellis NA, Campisi J (2001) Regulation and localization of the Bloom syndrome protein in response to DNA damage J Cell Biol 153: 367-80.
4. Bretcha-Boix P, Farre-Alegre J, Sureda M, Dussan C, Perez Ruixo JJ, Brugarolas Masllorens A (2010) Cytoreductive surgery and perioperative intraperitoneal chemotherapy in patients with peritoneal carcinomatosis of colonic origin: outcomes after 7 years’ experience of a new centre for peritoneal surface malignancies Clin Transl Oncol 12: 437-42.
5. Cao C, Yan TD, Black D, Morris DL (2009) A systematic review and meta-analysis of cytoreductive surgery with perioperative intraperitoneal chemotherapy for peritoneal carcinomatosis of colorectal origin Ann Surg Oncol 16: 2152-65.
6. Cerretani D, Nencini C, Urso R, Giorgi G, Marrelli D, De Stefano A, Pinto E, Cioppa T, Nastri G, Roviello F (2005) Pharmacokinetics of mitomycin C after resection of peritoneal carcinomatosis and intraperitoneal chemohyperthermic perfusion J Chemother 17: 668-73.
7. Chen Y, Poon RY (2008) The multiple checkpoint functions of CHK1 and CHK2 in maintenance of genome stability Front Biosci 13: 5016-29.
8. Chua TC, Esquivel J, Pelz JO, Morris DL (2012a) Summary of current therapeutic options for peritoneal metastases from colorectal cancer J Surg Oncol.
9. Chua TC, Pelz JO, Morris DL (2012b) Surgery for colorectal peritoneal carcinomatosis Scand J Gastroenterol 47: 277-85.
10. Colavito S, Prakash R, Sung P (2010) Promotion and regulation of homologous recombination by DNA helicases Methods 51: 329-35.
11. Cummings J, Spanswick VJ, Tomasz M, Smyth JF (1998) Enzymology of mitomycin C metabolic activation in tumour tissue: implications for enzyme-directed bioreductive drug development Biochem Pharmacol 56: 405-14.
12. D’andrea AD, Grompe M (2003) The Fanconi anaemia/BRCA pathway Nat Rev Cancer 3: 23-34.
13. Davalos AR, Kaminker P, Hansen RK, Campisi J (2004) ATR and ATM-dependent movement of BLM helicase during replication stress ensures optimal ATM activation and 53BP1 focus formation Cell Cycle 3: 1579-86.
14. De Cuba EM, Kwakman R, Knol DL, Bonjer HJ, Meijer GA, Te Velde EA (2013) Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases: Systematic review of all literature and meta-analysis of observational studies Cancer Treat Rev 39: 321-7.
15. De Cuba EM, Kwakman R, Van Egmond M, Bosch LJ, Bonjer HJ, Meijer GA, Te Velde EA (2012) Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : Future possibilities for personalised treatment by use of biomarkers Virchows Arch.
16. Elias D, Quenet F, Goere D (2012) Current status and future directions in the treatment of peritoneal dissemination from colorectal carcinoma Surg Oncol Clin N Am 21: 611-23.
17. Ellis NA, Groden J, Ye TZ, Straughen J, Lennon DJ, Ciocci S, Proytcheva M, German J (1995) The Bloom’s syndrome gene product is homologous to RecQ helicases Cell 83: 655-66.
18. Ferrer M, De Winter JP, Mastenbroek DC, Curiel DT, Gerritsen WR, Giaccone G, Kruyt FA (2004) Chemosensitizing tumor cells by targeting the Fanconi anemia pathway with an adenovirus overexpressing dominant-negative FANCA Cancer Gene Ther 11: 539-46.
19. Fitzsimmons SA, Workman P, Grever M, Paull K, Camalier R, Lewis AD (1996) Reductase enzyme expression across the National Cancer Institute Tumor cell line panel: correlation with sensitivity to mitomycin C and EO9 J Natl Cancer Inst 88: 259-69.
20. Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, Barone R, Yonemura Y, Cavaliere F, Quenet F, Gutman M, Tentes AA, Lorimier
21. G, Bernard JL, Bereder JM, Porcheron J, Gomez-Portilla A, Shen P, Deraco M, Rat P (2004) Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study J Clin Oncol 22: 3284-92.
22. Gomes IM, Santos CR, Maia CJ (2014) Expression of STEAP1 and STEAP1B in prostate cell lines, and the putative regulation of STEAP1 by post-transcriptional and post-translational mechanisms Genes Cancer 5: 142-51.

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
190
23. Karow JK, Chakraverty RK, Hickson ID (1997) The Bloom’s syndrome gene product is a 3’-5’ DNA helicase J Biol Chem 272: 30611-4.
24. Kim H, D’andrea AD (2012) Regulation of DNA cross-link repair by the Fanconi anemia/BRCA pathway Genes Dev 26: 1393-408.
25. Kitagawa R, Kastan MB (2005) The ATM-dependent DNA damage signaling pathway Cold Spring Harb Symp Quant Biol 70: 99-109.
26. Kusamura S, Dominique E, Baratti D, Younan R, Deraco M (2008) Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy J Surg Oncol 98: 247-52.
27. Langland G, Elliott J, Li Y, Creaney J, Dixon K, Groden J (2002) The BLM helicase is necessary for normal DNA double-strand break repair Cancer Res 62: 2766-70.
28. Lao VV, Welcsh P, Luo Y, Carter KT, Dzieciatkowski S, Dintzis S, Meza J, Sarvetnick NE, Monnat RJ, Jr., Loeb LA, Grady WM (2013) Altered RECQ Helicase Expression in Sporadic Primary Colorectal Cancers Transl Oncol 6: 458-69.
29. Liu G, Yang D, Sun Y, Shmulevich I, Xue F, Sood AK, Zhang W (2012) Differing clinical impact of BRCA1 and BRCA2 mutations in serous ovarian cancer Pharmacogenomics 13: 1523-35.
30. Mao FJ, Sidorova JM, Lauper JM, Emond MJ, Monnat RJ (2010) The human WRN and BLM RecQ helicases differentially regulate cell proliferation and survival after chemotherapeutic DNA damage Cancer Res 70: 6548-55.
31. Misra V, Klamut HJ, Rauth AM (2002) Expression of the prodrug-activating enzyme DT-diaphorase via Ad5 delivery to human colon carcinoma cells in vitro Cancer Gene Ther 9: 209-17.
32. Mizumoto A, Canbay E, Hirano M, Takao N, Matsuda T, Ichinose M, Yonemura Y (2012) Morbidity and Mortality Outcomes of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy at a Single Institution in Japan Gastroenterol Res Pract 2012: 836425.
33. Nimonkar AV, Genschel J, Kinoshita E, Polaczek P, Campbell JL, Wyman C, Modrich P, Kowalczykowski SC (2011) BLM-DNA2-RPA-MRN and EXO1-BLM-RPA-MRN constitute two DNA end resection machineries for human DNA break repair Genes Dev 25: 350-62.
34. Oostra AB, Nieuwint AW, Joenje H, De Winter JP (2012) Diagnosis of fanconi anemia: chromosomal breakage analysis Anemia 2012: 238731.
35. Phillips RM, Burger AM, Loadman PM, Jarrett CM, Swaine DJ, Fiebig HH (2000) Predicting tumor responses to mitomycin C on the basis of DT-diaphorase activity or drug metabolism by tumor homogenates: implications for enzyme-directed bioreductive drug development Cancer Res 60: 6384-90.
36. Pichierri P, Franchitto A, Rosselli F (2004) BLM and the FANC proteins collaborate in a common pathway in response to stalled replication forks EMBO J 23: 3154-63.
37. Plumb JA, Workman P (1994) Unusually marked hypoxic sensitization to indoloquinone EO9 and mitomycin C in a human colon-tumour cell line that lacks DT-diaphorase activity Int J Cancer 56: 134-9.
38. Rouers A, Laurent S, Detroz B, Meurisse M (2006) Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis: higher complication rate for oxaliplatin compared to Mitomycin C Acta Chir Belg 106: 302-6.
39. Sengupta S, Linke SP, Pedeux R, Yang Q, Farnsworth J, Garfield SH, Valerie K, Shay JW, Ellis NA, Wasylyk B, Harris CC (2003) BLM helicase-dependent transport of p53 to sites of stalled DNA replication forks modulates homologous recombination EMBO J 22: 1210-22.
40. Sharp SY, Kelland LR, Valenti MR, Brunton LA, Hobbs S, Workman P (2000) Establishment of an isogenic human colon tumor model for NQO1 gene expression: application to investigate the role of DT-diaphorase in bioreductive drug activation in vitro and in vivo Mol Pharmacol 58: 1146-55.
41. Sitzmann JV, Wiebke EA (2013) Risk-reducing appendectomy and the elimination of BRCA1-associated intraperitoneal cancer JAMA Surg 148: 285-91; discussion 291.
42. Smyth GK, Michaud J, Scott HS (2005) Use of within-array replicate spots for assessing differential expression in microarray experiments Bioinformatics 21: 2067-75.
43. Suzuki H, Seki M, Kobayashi T, Kawabe Y, Kaneko H, Kondo N, Harata M, Mizuno S, Masuko T, Enomoto T (2001) The N-terminal internal region of BLM is required for the formation of dots/rod-like structures which are associated with SUMO-1 Biochem Biophys Res Commun 286: 322-7.
44. Szybalski W, Iyer VN (1964) Crosslinking of DNA by Enzymatically or Chemically Activated Mitomycins and Porfiromycins, Bifunctionally “Alkylating” Antibiotics Fed Proc 23: 946-57.

Tailoring HIPEC with MMC for PM of CRC | Chapter 9
191
9
45. Takemura H, Rao VA, Sordet O, Furuta T, Miao ZH, Meng L, Zhang H, Pommier Y (2006) Defective Mre11-dependent activation of Chk2 by ataxia telangiectasia mutated in colorectal carcinoma cells in response to replication-dependent DNA double strand breaks J Biol Chem 281: 30814-23.
46. Van Der Speeten K, Stuart OA, Sugarbaker PH (2009) Pharmacokinetics and pharmacodynamics of perioperative cancer chemotherapy in peritoneal surface malignancy Cancer J 15: 216-24.
47. Van Ruth S, Verwaal VJ, Zoetmulder FA (2003) Pharmacokinetics of intraperitoneal mitomycin C Surg Oncol Clin N Am 12: 771-80.
48. Verwaal VJ, Bruin S, Boot H, Van Slooten G, Van Tinteren H (2008) 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer Ann Surg Oncol 15: 2426-32.
49. Wang Y, Cortez D, Yazdi P, Neff N, Elledge SJ, Qin J (2000) BASC, a super complex of BRCA1-associated proteins involved in the recognition and repair of aberrant DNA structures Genes Dev 14: 927-39.
50. Whitehead RH, Jones JK, Gabriel A, Lukies RE (1987) A new colon carcinoma cell line (LIM1863) that grows as organoids with spontaneous differentiation into crypt-like structures in vitro Cancer Res 47: 2683-9.
51. Zhang F, Ma J, Wu J, Ye L, Cai H, Xia B, Yu X (2009) PALB2 links BRCA1 and BRCA2 in the DNA-damage response Curr Biol 19: 524-9.

Chapter 9 | Tailoring HIPEC with MMC for PM of CRC
192
Supplementary table and figure
Supplementary table 1: Genes of which mRNA levels in cell lines were analysed to correlate to sensitivity levels. P<0.05 was considered significant. Only BLM (P=0.01) and BRCA2 (P=0.02) showed significant correlation to clustered sensitivity to MMC
FA-BRCA pathway Gene mRNA product P
FANCA nsFANCB nsFANCC nsFANCD2 ns FANCE nsFANCF nsFANCG nsFANCI nsFANCL nsFANCM nsPALB2 nsBRIP1 nsBRCA2 0.02BTBD12/SLX4 nsMUS-81 nsRAD51C nsBLM 0.01ERCC1 ns
ATM-ATR pathway Gene mRNA product P
ATM nsRAD17 nsRAD9A nsRAD50 nsCHK1 ns CHK2 nsH2AX ns53BP1 nsp53 nsMDC1 nsSMC1A nsSMC1B nsATRIP nsMRE11 nsSTAG2 ns
MMC enzyme activation pathway Gene mRNA product
P
NQO1 nsPOR nsXDH nsCYB5R1 ns
SW1389
HCT15
VU1131-0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 ≥10
percen
tageofcellswith
breaks
Numberofchromosomalbreakspercell
FANCD2
Supplementary figure 1: Determination of FA-BRCA pathway functionality. A. Chromosomal breakage assay outcome showing number of chromosomal breaks after 48 hours exposure to 50nM MMC. Control lines VU1131-T2 (positive control) and corrected VU1131-T2-8+FANCC (negative control) evidently show breaks and respectively no breaks. No colorectal cell lines show clear signs of chromosomal breakage. None of the cell lines showed any breaks under normal growth conditions. B. Western blotting for FANCD2 on SW48 cell lysate. A clear double band indicates the presence of FANCD2. After induction with hydroxyurea (HU), the second band becomes more intense, indicating an active monoubiquitination of the FANCD2 protein. Vinculin loading control is shown at the bottom

Chapter 10Prognostic value of BRAF and
KRAS mutation status in stage II and III microsatellite instable colon cancers
E. M. V. de Cuba*P. Snaebjornsson*D. A. M. HeidemanN. C. T. van GriekenL. J. W. BoschR. J. A. FijnemanE. BeltH. BrilH. B. A. C. StockmannE. HooijbergC. J. A. PuntM. KoopmanI. D. NagtegaalV. H. M. CoupéB. CarvalhoG. A. Meijer*Both authors contributed equally to this manuscript
Int J Cancer. 2016 Mar 1;138(5):1139-45

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
194
Abstract
Background: Microsatellite instability (MSI) has been associated with favourable survival in early stage colorectal cancer (CRC) compared to microsatellite stable (MSS) CRC. The BRAF V600E mutation has been associated with worse survival in MSS CRC. This mutation occurs in 40% of MSI CRC and it is unclear whether it confers worse survival in this setting. The prognostic value of KRAS mutations in both MSS and MSI CRC remains unclear.
Methods: We examined the effect of BRAF and KRAS mutations on survival in stage II and III MSI colon cancer patients. BRAF exon 15 and KRAS exon 2-3 mutation status was assessed in 143 stage II (n=85) and III (n=58) MSI colon cancers by high resolution melting analysis and sequencing. The relation between mutation status and cancer-specific (CSS) and overall survival (OS) was analysed using Kaplan-Meier and Cox regression analysis.
Results: BRAF V600E mutations were observed in 51% (n=73) and KRAS mutations in 16% of cases (n=23). Patients with double wild-type cancers (dWT; i.e. BRAF and KRAS wild-type) had a highly favourable survival with 5-year CSS of 93% (95% CI 84-100%), while patients with cancers harbouring mutations in either BRAF or KRAS, had 5-year CSS of 76% (95% CI 67-85%). In the subgroup of stage II patients with dWT cancers no cancer-specific deaths were observed. On multivariate analysis, mutation in either BRAF or KRAS vs. dWT remained significantly prognostic.
Conclusions: Mutations in BRAF as well as KRAS should be analysed when considering these genes as prognostic markers in MSI colon cancers.

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
195
10
Introduction
Colorectal cancer (CRC) is both clinically and biologically a heterogeneous disease. Microsatellite instability (MSI) occurs in 15% of CRC and results from a genetic or epigenetic defect in DNA mismatch repair (MMR), occurring sporadically (12%) or due to Lynch syndrome (3%). These cancers are more frequently right sided and often show poor differentiation, increased mucin formation and lymphocytic infiltration.1
The crucial RAS-RAF-MEK-ERK signal transduction pathway is affected in both MSS and MSI CRC, and can be constitutively activated by mutations in KRAS or BRAF. BRAF V600E mutations in exon 15 occur in about 7% of MSS CRC and in 40% within the MSI subgroup. In MSI CRC, BRAF mutations are closely linked to sporadic disease, and rarely occur (1.4%) in Lynch syndrome CRC.2,3 KRAS exon 2 and 3 mutations are found in approximately 35% of MSS CRC and variably (6-30%) in MSI CRC, 4-6 with frequencies up to 40% in Lynch syndrome associated CRC.7 Co-occurrence of BRAF and KRAS mutations in CRC is an extremely rare event.8
MSI confers good survival in stage II CRC compared to MSS9,10, while in stage III the risk differences are limited.9-12 In stage IV CRC, however, MSI paradoxically confers worse survival than MSS CRC.13,14 MSI is found in 15-20% of stage II cancers, 7-13% in stage III and 3-8% of stage IV cancers.9,14,15 Based on the stepwise change in the frequency and prognostic impact of MSI cancers it can be hypothesized that a subset of poor survival MSI cancers exists that progress to higher stages, while the majority of MSI cancers show a low rate of progression.
BRAF mutation and inconsistently KRAS mutations have been associated with worse survival in stage II and III MSS CRC.16,17 The prognostic effect and clinical significance of both BRAF and KRAS mutations in stage II and III MSI CRC is currently unclear.1,16 BRAF mutation correlates strongly with older age16 and previous studies have mostly analysed its prognostic effect in MSI cancers univariately using overall survival (Supplementary Information Table 1). Also, despite BRAF and KRAS mutations being mutually exclusive and having complementary roles in the RAS-RAF-MEK-ERK signal transduction pathway, the prognostic effect of these mutations compared to double wild-type cancers (dWT; i.e. BRAF and KRAS wild-type) has rarely been studied in MSI cancers before. Therefore, in the present study, we set out to analyse the prognostic importance of BRAF and KRAS mutations in stage II and III MSI colon cancers.

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
196
Materials and Methods
In total, 143 MSI cancer samples from patients diagnosed between 1987 and 2008 with stage II and III MSI colon cancers were collected. Rectal cancers were not included in the study. MSI testing was performed according to standard procedures using MSI Multiplex System Version 1.2, Promega, Madison, WI, USA, as described previously.18 In a single institution cohort of patients with stage II and III colon cancer, 65 out of 332 had a MSI cancer.18 Furthermore, 20 patients out of 196 stage II and III CRC patients from an immunotherapy trial were included.19 Finally, 58 stage II and III archival MSI cases from VU University Medical Center were included. Clinicopathological variables collected included date of diagnosis, age at diagnosis, gender, tumour location (right colon: caecum, ascending, hepatic flexure, transverse; left colon: descending, sigmoid, rectosigmoid), TNM stage, histological type, grade of differentiation, administration of adjuvant chemotherapy, date of death and cause of death (colon cancer-related or -unrelated). Collection, storage and use of patient derived tissue and data were performed either under informed consent, or alternatively in compliance with the “Code for Proper Secondary Use of Human Tissue in The Netherlands”.20
In case of synchronous primary colon cancers (n=7), the most advanced cancer was selected for analysis when this information was available. None of the patients had received neoadjuvant therapy. DNA isolation, MSI testing, high resolution melting and sequencing for BRAF (exon 15 that includes the V600E mutation) and KRAS (exon 2 and 3 that include codons 12/13 and 59/61, respectively) were performed according to diagnostic standards.18,21
The end of the surveillance period was April 1 2014. Death from colon cancer (cancer-specific survival, CSS) was the main end-point. CSS was determined from the date of diagnosis to either the date of colon cancer related death or censorship. Patients were censored at the date of the last known doctor’s visit or at the date of death if patients died of unknown cause or other causes than colon cancer. Overall survival (OS) was calculated to facilitate comparison with previous studies.
Chi Square statistics were calculated for identification of associations between qualitative variables. Five-year CSS and OS rates were obtained by means of Kaplan-Meier analysis. Survival curves were compared using the log-rank test. The Cox’s proportional hazards regression model was used to study the association between survival and the clinicopathological variables in uni- and multivariate analyses. Hazard ratios (HR) were estimated with corresponding 95% confidence intervals (CI) and p-values. Uni- and multivariate analyses were carried out for stage II and III combined and stage-stratified.

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
197
10
Stepwise backward variable elimination was performed with a probability of entry p=0.05 and probability of removal p=0.10. patients’ age was categorized in quartiles because of a nonlinear relationship with CSS and OS. Input variables for multivariate analysis were: age, gender, tumour stage, tumour location, histological type, grade of differentiation and BRAF/KRAS mutation status. All statistical tests were two-sided. P≤ 0.05 was considered to indicate a significant difference. All analyses were carried out using SPSS 20.0 software [IBM Corporation].
Results
The prevalence of BRAF and KRAS mutations are presented in Table 1. BRAF and KRAS mutations were observed in 51% (n=73) and 16% (n=23) of cases, respectively, and were mutually exclusive. BRAF mutations all comprised V600E. KRAS mutations occurred mostly in exon 2 (total n=20; codon 12, n=13; codon 13, n=6; both codon 12 and 13, n=1) and only rarely in exon 3 (total n=3; codon 59, n=2; codon 61, n=1). KRAS mutation status could not be determined in 4% of cases (n=5), which were BRAF WT. In 29% of cases (n=42) both BRAF and KRAS were WT (dWT).BRAF mutation status was associated with higher age (p<0.01). Median age at diagnosis of patients with BRAF mutated cancers was 73 years (IQR 66-79), 64 years (IQR 47-80) for KRAS mutated cancers, and 60 years (IQR 46-74) for dWT cancers. Other parameters that were also associated with the presence of BRAF mutation were female gender (p<0.01), less frequent administration of adjuvant chemotherapy (p=0.01) and tumour location in the right colon (p=0.05). KRAS mutation status did not correlate significantly with other variables. Neither BRAF nor KRAS mutation status correlated with stage, histological type or grade of differentiation.
Survival dataMedian follow-up time was 6.4 years (IQR, 4.3-9.2). No patients were lost to follow-up. In total 55 deaths occurred (38%), 24 (44%) were colon cancer-related, and 29 patients (53%) died from other causes, while for 2 (2%) the cause of death was unknown. The last cancer-specific death occurred 4.7 years after diagnosis (median 2.3 years, IQR 1.2-3.2). The 5-year CSS and OS for stage II and III combined were 82% (95% CI 76-87%) and 71% (95% CI 64-79%), respectively. The 5-year CSS was 89% (95% CI 82-96%) in stage II and 72% (95% CI 60-84%) in stage III. The 5-year OS rates in stage II and III were 75% (95% CI 66-85%) and 65% (95% CI 53-78%), respectively.

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
198
Table 1: Patient and MSI tumour characteristics
valueTotal BRAF WT/mut. P-value KRAS WT/mut. P-value
N (%), n=143 N (%), n=143 N (%), n= 1381
Mutation status 70 (49) / 73(51) 115 (83) / 23 (17)GenderMaleFemale
62 (43) 81 (57)
41 (66) / 21 (34)29 (36) / 52 (64)
<0.01 47 (80) / 12 (20)68 (86) / 11 (14)
0.4
Age30-5758-6869-7879-93
36 (25)36 (25)38 (27)33 (23)
30 (83) / 6 (17)17 (47) / 19 (53)10 (26) / 28 (74)13 (39) / 20 (61)
<0.01 23 (72) / 9 (28)30 (86) / 5 (14)36 (95) / 2 (5)26 (79) / 7 (21)
0.07
Tumour LocationRight ColonLeft ColonColon NOS
114 (80)27 (19)2 (1)
51 (45) / 63 (55)18 (67) / 9 (33)1 (50) / 1 (50)
0.052 94 (85) / 17 (15)20 (77) / 6 (23)1 (100) / 0 (0)
0.42
Histological TypeAdenocarcinoma NOSMucinous Adenocarcinoma
93 (65)50 (35)
46 (50) / 47 (51)24 (48) / 26 (52)
1.0 77 (84) / 15 (16)38 (83) / 8 (17)
0.1
Grade of differentiationWell/moderatePoorUnknown
95 (66)45 (32)3 (2)
49 (52) / 46 (48)20 (44) / 25 (56)1 (33) / 2 (67)
0.52 75 (82) / 17 (19)38 (88) / 5 (12)2 (67) / 1 (33)
0.52
StageIIIII
85 (59)58 (41)
42 (49) / 43 (51)28 (48) / 30 (52)
1.0 68 (85) / 12 (15)47 (81) / 11 (19)
0.6
Adjuvant ChemotherapyNoYes Unknown
90 (63)36 (25)17 (12)
37 (41) / 53 (59)24 (67) / 12 (33)9 (53) / 8 (47)
0.012 76 (84) / 14 (16)25 (74) / 9 (27)14 (100) / 0 (0)
0.22
1 KRAS mutation status could not be determined in 5 cases. WT, wild-type; mut., mutation; NOS, not otherwise specified.2 Cases with missing value not included in chi-square test.
Univariate analysis
Compared to dWT cancers (5-year CSS 93%, 95% CI 84-100%), mutations in BRAF or KRAS were associated with a worse 5-year CSS of resp. 76% (95% CI 66-86%) and 77% (95% CI 59-95%), also showing similar HR of 3.61 (95% CI 1.05-12.39) and 3.46 (95% CI 0.83-14.49), respectively (Figure 1a; Table 2). For KRAS this was not statistically significant, which may well be explained by the low frequency of KRAS mutations in MSI colon cancers, which translates into a lower statistical power. Because of similar HR of BRAF and KRAS mutations vs. dWT, the mutual exclusivity of these mutations and their complementary roles in the RAS-RAF-MEK-ERK pathway, cases with either BRAF or

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
199
10
KRAS mutation were combined for further analysis. Patients with either BRAF or KRAS mutated tumours showed a significantly worse CSS compared to those with dWT tumours with 5-year CSS of 76% (95% CI 67-85%) and HR 3.57 (95% CI 1.07-11.98, p=0.04).
Figure 1. Kaplan-Meier graphs depicting cancer-specific survival (CSS) and overall survival (OS) of MSI colon cancer patients according to BRAF and KRAS mutation status in stage II and III (A, B) (n=143), stage II (C,D) (n=85) and stage III (E, F) (n=58). In each graph univariate hazard ratios (95% CI) and log rank pvalues. Since patients with stage II dWT cancers did not experience cancer-specific death the univariate Cox analysis could not be performed. WT, wild-type; dWT, double wild-type; HR, hazard ratio; U, univariate.

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
200
Tabl
e 2:
Can
cer-s
peci
fic su
rviv
al a
naly
sis f
or st
age
II a
nd II
I MSI
col
on c
ance
r pat
ient
s
Vari
able
Cat
egor
ies
Dea
ths
per
nr.
5-ye
ar
CSS
(%)
Uni
vari
ate
HR
(9
5% C
I)U
niva
riat
e C
ox p
-val
ueM
ulti-
vari
ate
HR
(9
5% C
I)M
ulti-
vari
ate
p-va
lue
Age
0-58
59
-68
69-7
8 ≥7
9
3/36
6/36
8/38
5/33
86 83 78 82
1.00
(ref
)1.
18 (0
.36-
3.88
)1.
62 (0
.53-
4.96
)1.
40 (0
.41-
4.85
)
0.8
Gen
der
Mal
e Fe
mal
e8/
6216
/81
87 791.
00 (r
ef)
1.68
(0.7
2-3.
92)
0.2
Stag
e (U
ICC
/AJC
C)
II
III
9/85
15/5
889 72
1.00
(ref
)2.
62 (1
.14-
5.98
)0.
022.
55
(1.1
1-5.
86)
0.03
Adj
uvan
t Che
mot
hera
py1
No
Yes
Mis
sing
12/9
09/
363/
17
85 741.
00 (r
ef)
1.88
(0.7
9-4.
47)
0.2
Tum
our L
ocat
ion
Left
Col
on
Rig
ht C
olon
C
olon
NO
S
5/27
19/1
140/
2
80 821.
00 (r
ef)
0.90
(0.3
4-2.
41)
0.8
His
tolo
gica
l Typ
e A
deno
carc
inom
a N
OS
Muc
inou
s ade
noca
rc.
12/9
312
/50
86 761.
00 (r
ef)
1.80
(0.8
1-4.
00)
0.2
2.13
(0
.95-
4.76
)0.
07
Gra
de o
f diff
eren
tiatio
nM
oder
ate/
wel
lPo
orU
nkno
wn3
19/9
55/
450/
3
78 881.
00 (r
ef)
0.53
(0.2
0-1.
42)
0.2
BRAF
mut
atio
n st
atus
2W
ild-ty
pe
(dW
T or
KRA
S m
utat
ion)
BRAF
mut
atio
n
8/70
16/7
3
88 76
1.00
(ref
)
2.18
(0.9
3-5.
09)
0.07
KRA
S m
utat
ion
stat
us2
Wild
-type
(d
WT
or B
RAF
mut
atio
n)K
RAS
mut
atio
nU
nkno
wn3
19/1
15
5/23
0/5
82 77
1.00
(ref
)
1.35
(0.5
1-3.
62)
0.5

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
201
10
Tabl
e 2:
Con
tinue
d
Vari
able
Cat
egor
ies
Dea
ths
per
nr.
5-ye
ar
CSS
(%)
Uni
vari
ate
HR
(9
5% C
I)U
niva
riat
e C
ox p
-val
ueM
ulti-
vari
ate
HR
(9
5% C
I)M
ulti-
vari
ate
p-va
lue
BRAF
and
KRA
S m
utat
ion
sepa
rate
ly v
s. dW
T2D
oubl
e w
ild-ty
peBR
AF m
utat
ion
KRA
S m
utat
ion
Unk
now
n3
3/42
16/7
35/
230/
5
93 76 77
1.00
(ref
)3.
61 (1
.05-
12.3
9)3.
46 (0
.83-
14.4
9)
0.1
Eith
er B
RAF
or K
RAS
mut
atio
n vs
. dW
TD
oubl
e w
ild-ty
peBR
AF o
r KRA
S m
ut.
Unk
now
n3
3/42
21/9
60/
5
93 761.
00 (r
ef)
3.57
(1.0
7-11
.98)
0.04
3.
65
(1.0
9-12
.44)
0.04
Inpu
t for
mul
tivar
iate
ana
lysi
s: A
ge, g
ende
r, st
age,
tum
our l
ocat
ion,
his
tolo
gica
l typ
e, g
rade
of d
iffer
entia
tion,
eith
er B
RA
F or
KR
AS
mut
atio
n vs
. dW
T. 1
33 o
ut o
f 143
pat
ient
s w
ere
avai
labl
e fo
r the
mul
tivar
iate
ana
lysi
s; 9
cas
es w
ere
excl
uded
due
to a
mis
sing
val
ue (t
umou
r loc
atio
n, g
rade
of
diffe
rent
iatio
n an
d K
RA
S m
utat
ion
stat
us) a
nd 1
cas
e w
as e
xclu
ded
due
to c
enso
ring
befo
re fi
rst c
ance
r spe
cific
eve
nt. U
sing
stag
e, h
isto
logi
cal t
ype
and
eith
er B
RA
F or
KR
AS
mut
atio
n vs
. dW
T as
the
only
inpu
t var
iabl
es g
ave
the
sam
e re
sults
.1 N
ot in
clud
ed in
the
mul
tivar
iate
ana
lysi
s due
to n
umbe
r of m
issi
ng v
alue
s.2 N
ot in
clud
ed in
the
mul
tivar
iate
ana
lyse
s.3 C
ateg
orie
s with
unk
now
n va
lues
wer
e no
t inc
lude
d in
the
surv
ival
ana
lyse
s.

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
202
As expected, tumour stage was also prognostic, with stage III showing worse CSS as compared to stage II (HR 2.62, 95% CI, 1.14-5.98; p=0.02). After stratifying for stage, cancers with either BRAF or KRAS mutation status were associated with worse CSS in stage II (log rank p=0.03; Figure 1c), but not in stage III (Figure 1e; p=0.3). None of the stage II patients with dWT cancers experienced colon cancer related death.When using OS as an end-point, BRAF or KRAS mutation status did not predict outcome in any of the analyses (Figure 1b, 1d and 1f). Of all the variables only patient´s age predicted overall survival with the oldest age group demonstrating shorter survival compared to the reference age category (p=0.01).
Multivariate analysis
On multivariate CSS analysis either BRAF or KRAS mutation vs. dWT (p=0.04), tumour stage (p=0.03) and mucinous phenotype (p=0.07) were maintained in the final model (Table 2).Using OS as an end-point, higher patients’ age (p<0.01) and grade of differentiation (p=0.03) significantly conferred worse survival, overruling all other variables, including BRAF and KRAS mutation status.
Discussion
In the present study, with 143 stage II and III MSI colon cancer patients, BRAF and KRAS mutations were found in 51% and 16% of cases, respectively, which compares to previous reports. The concomitant evaluation of both BRAF and KRAS mutation in MSI colon cancer provides useful prognostic information beyond evaluation of either variable separately. Most notably, patients with dWT cancers had a highly favourable survival with 5-year CSS of 93% (95% CI 84-100%) compared to patients with either BRAF or KRAS mutated cancers (5-year CSS 76%, 95% CI 67-85%). In the subgroup of stage II patients with dWT cancers no cancer-specific deaths were observed. On multivariate analysis mutation in either BRAF or KRAS vs. dWT remained significantly prognostic (Table 2). In contrast to CSS, BRAF or KRAS mutation status vs. dWT did not demonstrate significant prognostic value on OS, although a tendency toward worse survival was observed in case mutations in these genes were present. However, since BRAF mutations are associated with older age, OS may not be the optimal endpoint for addressing this question in early stage colon cancer. Therefore CSS was chosen as the main endpoint in this study.Several studies have presented data on the prognostic impact of BRAF mutation status in stage II and/or III MSI CRC (Supplementary Information Table 1).5,6,11,22-26 Some of these studies demonstrated a tendency toward worse survival for patients with a BRAF mutation in MSI cancers, although only one of these studies found BRAF mutation status to be significantly prognostic.22

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
203
10
Of the studies that included patients with stage I through IV MSI CRC (Supplementary Information Table 1)2,27-33 only one reported BRAF to be significantly prognostic.29 Studies specifically on metastatic CRC have related the presence of BRAF mutation with worse survival within the MSI subset of CRC.13,14,34
Except for one study,32 previous studies have not found KRAS mutation status to have prognostic impact in the MSI subset of CRC.4,6,11,24 Importantly however, none of these studies analyzed the prognostic impact of KRAS mutated cancers versus dWT cancers.
In comparison to previous studies, the current study’s design has certain advantages. First, unlike many previous studies (see Supporting Information Table 1) we used CSS and corrected multivariately for confounders, most notably patients’ age. This is crucial due to the strong correlation of BRAF mutation with age. In concordance with previous literature, mutation in either BRAF or KRAS vs. dWT lost its prognostic significance in the current study when overall survival was used as an end-point. Second, we compared either BRAF or KRAS mutated cancers to dWT cancers in our survival analyses. This approach has been used previously for colorectal cancers but has rarely been applied when analyzing MSI tumors separately. This approach is logical, from a biological standpoint, considering that these mutations are mutually exclusive and are active in the same oncogenic pathway. Thus, we were able to show that either BRAF or KRAS mutations, compared to dWT cancers, actually carry hazard ratios of similar caliber. It is thus not surprising that when KRAS mutated cancers are compared to KRAS wild-type cancers such an analysis is likely to demonstrate lack of prognostic impact since the wild-type category includes the more common BRAF mutated cancers. Third, previous literature that includes solely stage II and III cancers is quite limited. Because of relative rarity of MSI CRC many previous studies on the subject have therefore included stage I through stage IV cancers (Supporting Information Table 1). The major drawback of this approach is that stage IV MSI-cancers confer poor prognosis compared to MSS cancers.13,14 Narrowing the survival analysis down to clinically more homogenous groups is appropriate since significantly prognostic impact in a subgroup may drive the results of the survival analysis.
Chemotherapeutic options are limited for MSI cancers since studies have indicated that MSI cancers are less sensitive to 5-FU, which is the backbone of current chemotherapeutic regimens in CRC.1 This means that other systemic treatment options need to be explored for patients with MSI cancers. The combined high frequency of BRAF and KRAS mutations, 68% in the present study, emphasises the importance of the activation of the RAS-RAF-MEK-ERK signal transduction pathway in MSI cancers. This pathway is targetable at various levels using drugs such as EGFR and BRAF inhibitors, as well as drugs that target

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
204
this pathway more downstream like MEK inhibitors. Trials using various combinations of inhibitors of this pathway in metastatic CRC are on going. Such drugs may also become suitable treatment options in the adjuvant setting. It remains to be determined to what extent and how this important signal transduction pathway is activated in BRAF and KRAS dWT MSI cancers.
The present study showed that mucinous adenocarcinoma was borderline significantly associated with worse survival compared to conventional adenocarcinoma on multivariate analysis. As a novel observation, we found no difference in CSS between well/moderately and poorly differentiated MSI cancers. This is of interest because grade of differentiation has generally been associated with survival in CRC 35, although in those studies MSI was not distinguished from MSS. We also found no difference of survival between right and left colon cancers, as reported recently.12
The main limitation of the present study is potential bias inherent to its retrospective design. For this reason the effect of adjuvant chemotherapy could not be assessed. Furthermore, since the patients were diagnosed in 1987 through 2008 the chemotherapeutic regimens are likely to have varied. These most likely included 5-FU monotherapy, which may have a negative impact on survival. In addition, the data on high-risk factors in stage II CRC were incomplete and thus not taken along in the analysis.
In conclusion, BRAF and KRAS mutations show together a high prevalence in stage II and III MSI colon cancer and, when combined, are associated with poor survival compared to dWT cancers, which status confers an excellent cancer-specific survival. The concomitant evaluation of both BRAF and KRAS mutation in MSI colon cancers therefore provides useful prognostic information beyond evaluation of either variable alone.

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
205
10
References1. Sinicrope FA, Sargent DJ. Molecular Pathways:
Microsatellite Instability in Colorectal Cancer: Prognostic, Predictive, and Therapeutic Implications. Clin Cancer Res 2012;18:1506–12.
2. Phipps AI, Buchanan DD, Makar KW, Burnett-Hartman AN, Coghill AE, Passarelli MN, Baron JA, Ahnen DJ, Win AK, Potter JD, Newcomb PA. BRAF Mutation Status and Survival after Colorectal Cancer Diagnosis According to Patient and Tumor Characteristics. Cancer Epidemiol Biomarkers Prev 2012;21:1792–8.
3. Parsons MT, Buchanan DD, Thompson B, Young JP, Spurdle AB. Correlation of tumour BRAF mutations and MLH1 methylation with germline mismatch repair (MMR) gene mutation status: a literature review assessing utility of tumour features for MMR variant classification. J Med Genet 2012;49:151–7.
4. Nash GM, Gimbel M, Cohen AM, Zeng Z-S, Ndubuisi MI, Nathanson DR, Ott J, Barany F, Paty PB. KRAS Mutation and Microsatellite Instability: Two Genetic Markers of Early Tumor Development That Influence the Prognosis of Colorectal Cancer. Ann Surg Oncol 2010;17:416–24.
5. Farina-Sarasqueta A, van Lijnschoten G, Moerland E, Creemers GJ, Lemmens VEPP, Rutten HJT, van den Brule AJC. The BRAF V600E mutation is an independent prognostic factor for survival in stage II and stage III colon cancer patients. Ann Oncol 2010;21:2396–402.
6. Roth AD, Tejpar S, Delorenzi M, Yan P, Fiocca R, Klingbiel D, Dietrich D, Biesmans B, Bodoky G, Barone C, Aranda E, Nordlinger B, et al. Prognostic Role of KRAS and BRAF in Stage II and III Resected Colon Cancer: Results of the Translational Study on the PETACC-3, EORTC 40993, SAKK 60-00 Trial. J Clin Oncol 2010;28:466–74.
7. Oliveira C. Distinct patterns of KRAS mutations in colorectal carcinomas according to germline mismatch repair defects and hMLH1 methylation status. Hum Mol Genet 2004;13:2303–11.
8. Sahin IH, Kazmi SMA, Yorio JT, Bhadkamkar NA, Kee BK, Garrett CR. Rare Though Not Mutually Exclusive: A Report of Three Cases of Concomitant KRAS and BRAF Mutation and a Review of the Literature. J Cancer 2013;4:320–2.
9. Merok MA, Ahlquist T, Royrvik EC, Tufteland KF, Hektoen M, Sjo OH, Mala T, Svindland A, Lothe RA, Nesbakken A. Microsatellite instability has a positive prognostic impact on stage II colorectal cancer after complete resection: results from a large, consecutive Norwegian series. Ann Oncol 2013;24:1274–82.
10. Sargent DJ, Shi Q, Yothers G, Tejpar S, Bertagnolli MM, Thibodeau SN, Andre T, Labianca R, Gallinger S, Hamilton SR, Monges G, Pogue-Geile KL, et al. Prognostic impact of deficient mismatch repair (dMMR) in 7,803 stage II/III colon cancer (CC) patients (pts): A pooled individual pt data analysis of 17 adjuvant trials in the ACCENT database. J Clin Oncol [Abstract] 2014;32:3507.
11. Sinicrope FA, Mahoney MR, Smyrk TC, Thibodeau SN, Warren RS, Bertagnolli MM, Nelson GD, Goldberg RM, Sargent DJ, Alberts SR. Prognostic Impact of Deficient DNA Mismatch Repair in Patients With Stage III Colon Cancer From a Randomized Trial of FOLFOX-Based Adjuvant Chemotherapy. J Clin Oncol 2013;31:3664–72.
12. Klingbiel D, Saridaki Z, Roth AD, Bosman FT, Delorenzi M, Tejpar S. Prognosis of stage II and III colon cancer treated with adjuvant 5-fluorouracil or FOLFIRI in relation to microsatellite status: results of the PETACC-3 trial. Ann Oncol 2015;26:126–32.
13. Tran B, Kopetz S, Tie J, Gibbs P, Jiang Z-Q, Lieu CH, Agarwal A, Maru DM, Sieber O, Desai J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011;117:4623–32.
14. Venderbosch S, Nagtegaal ID, Maughan TS, Smith CG, Cheadle JP, Fisher D, Kaplan R, Quirke P, Seymour MT, Richman SD, Meijer GA, Ylstra B, et al. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FOCUS Studies. Clin Cancer Res 2014; 15;20:5322–30.
15. Hoffmeister M, Blaker H, Kloor M, Roth W, Toth C, Herpel E, Frank B, Schirmacher P, Chang-Claude J, Brenner H. Body Mass Index and Microsatellite Instability in Colorectal Cancer: A Population-based Study. Cancer Epidemiol Biomarkers Prev 2013;22:2303–11.
16. Thiel A, Ristimäki A. Toward a Molecular Classification of Colorectal Cancer: The Role of BRAF. Front Oncol 2013;3:281.
17. Lee D-W, Kim KJ, Han S-W, Lee HJ, Rhee YY, Bae JM, Cho N-Y, Lee K-H, Kim T-Y, Oh D-Y, Im S-A, Bang Y-J, et al. KRAS mutation is associated with worse prognosis in stage III or high-risk stage II colon cancer patients treated with adjuvant FOLFOX. Ann Surg Oncol 2015;22:187–94.

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
206
18. Belt EJT, Velde te EA, Krijgsman O, Brosens RPM, Tijssen M, Essen HF, Stockmann HBAC, Bril H, Carvalho B, Ylstra B, Bonjer HJ, Meijer GA. High Lymph Node Yield is Related to Microsatellite Instability in Colon Cancer. Ann Surg Oncol 2012;19:1222–30.
19. de Weger VA, Turksma AW, Voorham QJM, Euler Z, Bril H, van den Eertwegh AJ, Bloemena E, Pinedo HM, Vermorken JB, van Tinteren H, Meijer GA, Hooijberg E. Clinical Effects of Adjuvant Active Specific Immunotherapy Differ between Patients with Microsatellite-Stable and Microsatellite-Instable Colon Cancer. Clin Cancer Res 2012;18:882–9.
20. Dutch Federation of Biomedical Scientific Societies. Code for proper secondary use of human tissue in the Netherlands. Available from: http://www.federa.org/ [cited 2014 Dec 23].
21. Heideman DAM, Lurkin I, Doeleman M, Smit EF, Verheul HM, Meijer GA, Snijders PJF, Thunnissen E, Zwarthoff EC. KRAS and BRAF Mutation Analysis in Routine Molecular Diagnostics: Comparison of Three Testing Methods on Formalin-Fixed Paraffin-Embedded Tumor-Derived DNA. J Mol Diagn 2012;14:247–55.
22. French AJ, Sargent DJ, Burgart LJ, Foster NR, Kabat BF, Goldberg R, Shepherd L, Windschitl HE, Thibodeau SN. Prognostic Significance of Defective Mismatch Repair and BRAF V600E in Patients with Colon Cancer. Clin Cancer Res 2008;14:3408–15.
23. Gavin PG, Colangelo LH, Fumagalli D, Tanaka N, Remillard MY, Yothers G, Kim C, Taniyama Y, Kim SI, Choi HJ, Blackmon NL, Lipchik C, et al. Mutation Profiling and Microsatellite Instability in Stage II and III Colon Cancer: An Assessment of Their Prognostic and Oxaliplatin Predictive Value. Clin Cancer Res 2012;18:6531–41.
24. Hutchins G, Southward K, Handley K, Magill L, Beaumont C, Stahlschmidt J, Richman S, Chambers P, Seymour M, Kerr D, Gray R, Quirke P. Value of Mismatch Repair, KRAS, and BRAF Mutations in Predicting Recurrence and Benefits From Chemotherapy in Colorectal Cancer. J Clin Oncol 2011;29:1261–70.
25. Ogino S, Shima K, Meyerhardt JA, McCleary NJ, Ng K, Hollis D, Saltz LB, Mayer RJ, Schaefer P, Whittom R, Hantel A, Benson AB, et al. Predictive and Prognostic Roles of BRAF Mutation in Stage III Colon Cancer: Results from Intergroup Trial CALGB 89803. Clin Cancer Res 2012;18:890–900.
26. Lin C-C, Lin J-K, Lin T-C, Chen W-S, Yang S-H, Wang H-S, Lan Y-T, Jiang J-K, Yang M-H, Chang S-C. The prognostic role of microsatellite instability, codon-specific KRAS, and BRAF mutations in colon cancer. J Surg Oncol 2014;110:451–7.
27. Maestro ML, Vidaurreta M, Sanz-Casla MT, Rafael S, Veganzones S, Martínez A, Aguilera C, Herranz MD, Cerdán J, Arroyo M. Role of the BRAF Mutations in the Microsatellite Instability Genetic Pathway in Sporadic Colorectal Cancer. Ann Surg Oncol 2007;14:1229–36.
28. Shaukat A, Arain M, Thaygarajan B, Bond JH, Sawhney M. Is BRAF Mutation Associated with Interval Colorectal Cancers? Dig Dis Sci 2010;55:2352–6.
29. Kalady MF, DeJulius KL, Sanchez JA, Jarrar A, Liu X, Manilich E, Skacel M, Church JM. BRAF Mutations in Colorectal Cancer Are Associated With Distinct Clinical Characteristics and Worse Prognosis. Dis Colon Rectum 2012;55:128–33.
30. Samowitz WS, Sweeney C, Herrick J, Albertsen H, Levin TR, Murtaugh MA, Wolff RK, Slattery ML. Poor survival associated with the BRAF V600E mutation in microsatellite-stable colon cancers. Cancer Res 2005;65:6063–9.
31. Lochhead P, Kuchiba A, Imamura Y, Liao X, Yamauchi M, Nishihara R, Qian ZR, Morikawa T, Shen J, Meyerhardt JA, Fuchs CS, Ogino S. Microsatellite instability and BRAF mutation testing in colorectal cancer prognostication. J Natl Cancer Inst 2013;105:1151–6.
32. Eklöf V, Wikberg ML, Edin S, Dahlin AM, Jonsson B-A, Öberg A, Rutegard J, Palmqvist R. The prognostic role of KRAS, BRAF, PIK3CA and PTEN in colorectal cancer. Br J Cancer 2013;108:2153–63.
33. Luey N, Toon CW, Sioson L, Clarkson A, Watson N, Cussigh C, Kedziora A, Pincott S, Pillinger S, Evans J, Percy J, Engel A, et al. A Further Investigation of Combined Mismatch Repair and BRAFV600E Mutation Specific Immunohistochemistry as a Predictor of Overall Survival in Colorectal Carcinoma. PLoS ONE 2014;9:e106105.
34. Goldstein J, Tran B, Ensor J, Gibbs P, Wong HL, Wong SF, Vilar E, Tie J, Broaddus R, Kopetz S, Desai J, Overman MJ. Multicenter retrospective analysis of metastatic colorectal cancer (CRC) with high-level microsatellite instability (MSI-H). Ann Oncol 2014;25:1032–8.
35. Compton CC, Fielding LP, Burgart LJ, Conley B, Cooper HS, Hamilton SR, Hammond ME, Henson DE, Hutter RV, Nagle RB, Nielsen ML, Sargent DJ, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000;124:979–94.

BRAF and KRAS in stage II, III MSI CRC | Chapter 10
207
10
Supp
lem
enta
ry ta
ble
Supp
lem
enta
ry ta
ble
1: P
revi
ous s
tudi
es o
n th
e pr
ogno
stic
impa
ct o
f BR
AF
mut
atio
n in
MSI
CR
C (s
tudi
es th
at in
clud
ed st
age
II a
nd II
I)
Aut
hor
(yea
r)N
r. of
M
SI p
atie
nts
Stag
eFr
eq. o
f BR
AF
m
utat
ion
(%)
Stat
istic
al te
stR
esul
ts
Fren
ch (2
008)
2213
4II
-III
62Lo
g ra
nk p
DFS
: p=0
.27
OS:
p=0
.006
Farin
a (2
010)
553
II-I
II55
Log
rank
pC
SS: N
S
Rot
h (2
010)
618
8II
-III
24Lo
g ra
nk p
RFS
: NS
OS:
NS
Gav
in (2
012)
2320
1II
-III
35U
niva
r. H
R (9
5% C
I)O
S: 1
.76
(0.8
8-3.
49),
p=0.
11
Hut
chin
s (20
11)24
156
120
I-II
I
II
I-II
I: 37
II: 4
2
Rel
ativ
e ris
k of
recu
rren
ce
(95%
CI)
I-II
I: 1.
09 (0
.42-
2.79
)
II: 0
.76
(0.2
0-2.
90)
Ogi
no (2
012)
2577
III
445-
year
surv
ival
Mul
tivar
.
BR
AF
WT:
RFS
74%
, DFS
74%
, OS
79%
BR
AF
Mut
.: R
FS 7
4%, D
FS 6
7%, O
S 66
%
The
BRAF
mut
ated
MSI
CR
C a
nd B
RAF
WT
MSI
C
RC
show
ed si
mila
r HR
and
95%
CI c
ompa
red
to
BRAF
wt M
SS (r
efer
ence
cat
egor
y).
Sini
crop
e (2
013)
1130
4II
I50
Uni
var.
HR
(95%
CI)
Mul
tivar
. HR
(95%
CI)
DFS
: 1.3
3 (0
.87-
2.04
), p=
0.19
DFS
: 1.5
8 (0
.88-
2.82
), p=
0.12
Sam
owitz
(200
5)30
83I-
IV52
Log
rank
pO
S: p
=0.8
9
Mae
stro
(200
7)27
49I-
IV18
Log
rank
pO
S: p
=1.0
0
Shau
kat (
2010
)2825
I-IV
68Lo
g ra
nk p
OS:
NS
Phip
ps (2
012)
229
7I-
IV42
Uni
var.
HR
(95%
CI)
OS:
1.1
7 (0
.75-
1.81
)C
SS: 0
.94
(0.4
4-2.
03)
Kal
ady
(201
2)29
76I-
IV38
Log
rank
pM
ultiv
ar. H
RO
S: p
=0.0
007
OS:
HR
2.7
, p=0
.012
Ek
lof (
2013
)3285
I-IV
53Lo
g ra
nk p
CSS
: NS

Chapter 10 | BRAF and KRAS in stage II, III MSI CRC
208
Supp
lem
enta
ry ta
ble
1: C
ontin
ued
Aut
hor
(yea
r)N
r. of
M
SI p
atie
nts
Stag
eFr
eq. o
f BR
AF
m
utat
ion
(%)
Stat
istic
al te
stR
esul
ts
Loch
head
(201
3)31
193
I-IV
52U
niva
r. H
R (9
5% C
I)M
ultiv
ar. H
R (9
5% C
I)U
niva
r. H
R (9
5% C
I)M
ultiv
ar. H
R (9
5% C
I)
OS:
1.3
7 (0
.87-
2.18
), p=
0.18
OS:
1.4
4 (0
.91-
2.30
), p=
0.12
CSS
: 1.7
1 (0
.72-
4.08
), p=
0.23
CSS
: 1.9
0 (0
.79-
4.57
), p=
0.15
Luey
(201
4)33
140
I-IV
77Lo
g ra
nk p
OS:
NS
Lin
(201
4)26
127
I-IV
21M
ultiv
ar. H
R (9
5% C
I)O
S: 1
.44
(0.9
6-2.
16),
p=0.
08

Summary and Future Perspectives


Summary and Future Perspectives |
211
General Summary
Metastatic disease (Stage IV) is present in approximately 20% of patients with colorectal cancer (CRC) at time of diagnosis. In the past, peritoneal metastases (PM) have been regarded as a condition only amenable to treatment with a palliative intent, due to the belief that the condition inevitably leads to a rapid demise of the patient. Surgical treatment of both hepatic and pulmonary metastases is the current standard of care for metastasized CRC, under the condition that these metastases can be radically resected in a safe manner. However, for a considerable time this approach was not regarded as feasible or desirable for patients with PM. Roughly 10-25% of CRC patients develop PM, of which 25% present with the peritoneum as the sole site of metastases. This observation led to the theory that PM are a form of localized spread, and thus amenable to a form of localized treatment, i.e. surgery. This prompted the subsequent development of a novel treatment during the eighties-early nineties, which consisted of an aggressive surgical approach, CytoReductive Surgery (CRS), combined with Hyperthermic IntraPEritoneal Chemotherapy (HIPEC). The introduction of this treatment modality was a game-changer in the treatment of PM, leading to five-year survival rates of up to 35-45% comparable to that after radical resection of liver metastases. Despite these improvements over the years, several important clinical needs still remain to be addressed. With a treatment related morbidity and mortality of respectively 10-20% and 1-5%, improved patient selection is paramount in reducing morbidity and mortality. Not only is it necessary to identify patients that could possibly be unfit for CRS and HIPEC, but also to select patients that will have the most advantage, i.e. best survival benefit, after treatment. Furthermore, the chemotherapy that is used in HIPEC is still based on the “one size fits all” principle, without biological stratification. Analogous to the initial treatment plan, i.e. the CRS and HIPEC procedure, the aftercare of these patients also requires further personalization. These patients have often undergone quite extensive gastro-intestinal surgery and are missing a key element in the containment of intra-abdominal infectious processes, the peritoneum. This makes this population different from other surgical patient populations undergoing stoma-reversal procedures, which could justify a different approach to patient counselling, the reversal procedure and aftercare. The studies in the present thesis aimed to provide more insight into a number of clinical challenges and their underlying biology as a first step towards developing possible solutions.This thesis is comprised of 10 studies in which we investigated several types of potential prognostic factors for treatment outcome in patients with peritoneal metastases of colorectal cancer. These include clinical, histopathological and molecular characteristics.

| Summary and Future Perspectives
212
Clinical Decision Making / Treatment Allocation
Chapter 2 provides a systematic review and meta-analysis of current literature in which we assessed the overall outcome after CRS and HIPEC in colorectal cancer (CRC) patients that present with concomitant peritoneal metastases (PM) and liver metastases (LM). There is no statistically significant difference in overall survival (pooled HR: 1.24 [95% CI: 0.90 – 1.60]) between patients with a combination of LM and PM and patients with isolated PM after CRS and HIPEC. In addition we found that patients with metastatic CRC to both peritoneum and liver show a tendency towards increased median overall survival after CRS and HIPEC combined with resection of liver metastases when compared to treatment with (modern) systemic chemotherapy alone.
Adequate aftercare of patients that have undergone CRS and HIPEC is crucial if they have been disease-free for an extended period of time. CRS and HIPEC has dramatically improved the survival in selected colorectal cancer patients with PM. Often during the CRS procedure, the risk of additional morbidity due to known complications accompanying a low-anastomosis is diminished by creating a colostomy. However, the morbidity and mortality associated with the reversal of the colostomy in this population is unknown. In chapter 3 we analysed the associations between four clinical and 10 treatment-related factors with the outcome of the reversal procedure. From two prospectively collected databases, we identified 21 patients out of 336 patients with a stoma who actively requested a reversal procedure. The reversal related morbidity observed in this cohort was 67%. Infectious complications were observed in 33% of the patients. In addition, we found that infectious complications after HIPEC were negatively correlated with the ultimate restoration of bowel continuity (P=0.05). It is thought that this is caused by a diminished capacity to contain intra-abdominal infectious complications after a complete peritonectomy procedure. The ultimate success-rate of the reversal procedure was 71%. Although the restoration of bowel continuity after CRS and HIPEC was successful in most patients, a relatively high complication rate was observed.
Molecular Approach – Possible Aids in Future Clinical Decision-Making
Uncovering the Biological Landscape of Peritoneal MetastasesAt present, the selection of patients for CRS and HIPEC is based on clinical parameters and intra-operative findings. Currently, patients with isolated PM with a Peritoneal Cancer Index (PCI) of lower than 20 or a simplified PCI score of less than five are deemed the most suitable candidates for this approach. Based on the hypothesis that underlying biological mechanisms drive the clinical behaviour of CRC PM, readouts of the disease biology, also

Summary and Future Perspectives |
213
known as biomarkers, might improve and refine the identification of suitable patients. In addition, these markers could potentially include so-called drugable targets. Relatively little is known about the biology of peritoneal spread of CRC. In chapter 4, we provide an overview of molecules associated with peritoneal dissemination and explore the clinical possibilities of these candidate biomarkers. In a series of over 100 studies on PM published between 1990 and 2010, IGF-1, HIF1α, VEGF, EGFR and ITGB1 emerge as the most interesting candidates for possible clinical application. Even though these promising candidate biomarkers have been identified, all of these require extensive further validation prior to clinical application. According to the proposed model seen in chapter 4 (figure 1), tumour cell adhesion is a key step in peritoneal dissemination. In chapter 5 we have provided an overview of the functional importance of adhesion molecules in peritoneal dissemination. Most importantly, targeting adhesion molecules might be able to prevent tumour cell adhesion to the peritoneal surface and tumour outgrowth in patients at high risk for peritoneal dissemination. The most studied molecules in tumour cell adhesion were found to be integrin α2β1, CD44s and MUC16. Furthermore, L1CAM, EpCAM, MUC1, sLex and Lex, chemokine receptors, Betaig-H3 and uPAR may have a role in this process. Based on current literature the blood group antigens and MUC16 are the most promising prognostic biomarkers in the context of colorectal PM. We feel that advancing the studies on the diagnostic and possible therapeutic value of adhesion molecules seems a promising and logical approach to optimizing and personalizing treatment of patients presenting with PM of CRC. In chapter 4, attachment is considered a key step in the dissemination process of intra-abdominal tumour cells. In addition to attachment, angiogenesis, i.e. the formation of new blood vessels, is crucial for tumour growth beyond 150-200 micrometres from the nearest blood vessel and thus for the progression of micrometastases to macrometastases. Angiogenesis depends on, among other things, complex interactions between several cell types and extracellular matrix components. Even though the exact interactions required for this process are not fully understood, several studies suggest a role for the attachment molecule Versican (VCAN). VCAN mediated angiogenesis possibly depends upon interaction with vascular endothelial growth factor (VEGF). In chapter 6, we analysed the expression of one attachment molecule, VCAN and VEGF and their relation to overall survival after CRS and HIPEC with curative intent. Our study shows that high stromal VCAN expression was associated with high microvessel density (MVD) and higher T-stage, but with improved resection outcome. Epithelial VCAN was associated with MVD and with a more complete resection macroscopically. In multivariate analysis, simplified PCI, VEGF expression levels, age, VCAN expression levels and lymph node status were all associated with overall survival after treatment with CRS and HIPEC. The

| Summary and Future Perspectives
214
possible role of VEGF as a predictor of worse outcome supports the rationale for (neo-)adjuvant anti-VEGF based therapy in this particular group of metastasized CRC patients. Furthermore, epithelial VCAN seems to be indicative for good outcome in CRC patients with PM. One possible mechanism by which epithelial VCAN positively influences patient outcome might be related to tumour cell responses to chemotherapy. The potential influence of VCAN in tumour response to chemotherapy in this context further emphasizes the importance of the systematic analysis of interactions between cancer cells and their environment, in this case the peritoneal surface, in order to identify possible mechanisms contributing to drug sensitivity.
In chapter 4 several promising biomarkers were identified that are potential candidates for more refined identification of suitable patients. Angiogenesis can not only be driven by the interaction between VCAN and VEGF, but possibly also by the activation of alternative pathways. In chapter 7 we investigated the presence of the angiogenesis related markers; HIF1a, SDF1, CXCR4, VEGF and MVD and whether or not these have prognostic implications in patients with PM of CRC undergoing CRS and HIPEC. Multivariate analysis showed an independent association between PCI, resection outcome and VEGF expression with OS after treatment. We conclude that not only could VEGF levels serve as a prognostic tool, but also that addition of anti-VEGF antibody therapies, i.e. Bevacizumab, could be of added value in this subgroup of metastatic colorectal cancer patients. Our study adds to the evidence that the possibility of combining the aggressive surgical approach, CRS & HIPEC, with the systemic administration of anti-VEGF forms a very interesting and viable avenue for the further improvement of survival in this particular population of metastatic CRC patients.
Other than the fact that PM and LM differ from location, to date little is known about possible biological differences between these two metastatic niches. To uncover possible differences between PM and LM, we have investigated the individual and combined prognostic value of HIF1a, GLUT1 and VEGF in a multi-institutional cohort of patients with resected colorectal cancer liver metastasis.
In the majority of CRC patient with LM, resection appears not to be curative, despite its curative intent. Overexpression of HIF1a, GLUT1 and VEGF has been associated with tumour progression and poor prognosis of CRC patients in general. In chapter 8 we found that high GLUT1 expression was associated with good prognosis, particularly in patients treated with systemic therapy. High VEGF expression was associated with poor prognosis, particularly in patients not treated with systemic therapy. Thus, at present, no differences in marker expression profiles have been found for HIF1a and VEGF between LM and PM.

Summary and Future Perspectives |
215
In LM, assessment of GLUT1 levels on top of VEGFA expression may improve outcome by selecting patients eligible for resection and, furthermore, selecting patients highly expressing both VEGFA and GLUT1 as best candidates for additional systemic treatment.
Tailoring Chemotherapeutic RegimentsHIPEC consists of intra-peritoneal lavage with Mitomycin C (MMC) in order to eliminate minimal residual disease after cytoreduction. During surgery it is impossible to determine the extent of microscopic disease left behind. In order to eliminate these cancerous cells that are either still attached to the peritoneal surface or free floating in the abdomen, the surgical team administers hyperthermic intra-peritoneal MMC. MMC is the drug of choice because of the direct cytotoxicity and the tissue penetrance of only one to two mm. This is thought to cause minimal systemic side effects, while still eliminating minimal residual disease after cytoreduction. After cytoreduction and HIPEC, a subset of patients were observed to have decreased survival, despite a low PCI and a favourable resection outcome, giving rise to our hypothesis that these patients might respond differently to MMC. In chapter 9, we studied multiple markers to predict treatment response to MMC in patients receiving HIPEC for PM of CRC in order to ultimately tailor the treatment and subsequently improve survival after cytoreduction and HIPEC. MMC functions by intercalating or cross-linking DNA, thus creating DNA damage, which disrupts DNA replication. There are two proposed mechanisms by which a cancer cell can become resistant to the effects of MMC. Activation of MMC is required in order for it to function. Another way for these malignant cells to overcome this MMC-induced damage is simply to repair it by activation of either the Fanconi Anaemia-BRCA (FA-BRCA) pathway or the ATM-ATR pathway. In this study, MMC sensitivity was determined for 12 CRC cell lines and correlated to mRNA expression of 37 genes related to the Fanconi Anaemia (FA)-BRCA pathway, ATM-ATR pathway and enzymatic activation of MMC. In addition, the functionality of the FA-BRCA pathway in these cell lines was assessed using a chromosomal breakage assay and Western Blot for key protein FANCD2. Briefly, the number of chromosomal breaks corresponds with the functionality of the FA-BRCA pathway. For example, cells with a non-functional FA-BRCA pathway display more than 10 breaks per cell. An additional step in assessing the activity of this pathway is assessing the presence of FANCD2 protein. FANCD2 is monoubiquitinated in case of DNA damage, which results in the activation of DNA repair mechanisms. High sensitivity for MMC correlated with a low Bloom syndrome (BLM) and BRCA2 at mRNA expression level. However, FA-BRCA pathway functionality demonstrated no correlation to MMC sensitivity. BLM was further analysed by staining for the corresponding protein with immunohistochemistry on both the CRC cell lines and patient derived material. In cell lines, weak intensity staining of BLM by IHC

| Summary and Future Perspectives
216
correlated with high sensitivity to MMC. Subsequently, low BLM protein expression was significantly associated with an improved survival in patients after CRS and HIPEC.Ultimately, low BLM levels were found to be associated with high MMC sensitivity and an improved survival after HIPEC. These findings indicate a possible role for BLM in the prediction of MMC sensitivity in CRS and HIPEC patients and certainly warrant further investigation prior to implementation in a clinical setting.
Microsatellite instable (MSI) CRC has been described to preferentially metastasize to the peritoneal surface. MSI tumours tend to have a worse prognosis in late stage disease, probably because the tumours are less sensitive to regiments containing 5-FU. Paradoxically, this phenotype has been associated with favourable survival in early stage CRC compared to microsatellite stable (MSS) CRC. BRAF mutation has been associated with worse survival in MSS CRC. This mutation occurs in 40% of MSI CRC and it is unclear whether it confers worse survival in this setting. In chapter 10, we investigated the effect of BRAF and KRAS mutations on survival in both stage II and III MSI colon cancer patients. BRAF mutations were observed in 51% and KRAS mutations in 16% of the included patients. Patients with double wild-type cancers had a highly favourable survival with 5-year cancer-specific survival (CSS) of 93%, while patients with cancers harbouring mutations in either BRAF or KRAS, had 5-year CSS of 76%. Multivariate analysis showed that a mutation in either BRAF or KRAS versus double wild-type tumours remained significantly prognostic. In the future, it would be interesting to assess the percentage of MSI tumours in patients presenting with PM and study the possible effect of this phenotype on the survival of patients after CRS and HIPEC. In conclusion, mutations in BRAF as well as KRAS should be analysed when considering these genes as prognostic markers in MSI colon cancers. Patients with BRAF or KRAS mutant CRC could therefore potentially benefit from adjuvant therapy, which evidently should be tuned to the specific biology underlying these tumours.
Conclusions and Future Perspectives
The studies presented in this thesis have improved our understanding of both clinical and molecular factors affecting the entire clinical course of Cytoreductive surgery (CRS) and Hyperthermic IntraPeritoneal Chemotherapy (HIPEC) patients – from diagnosis to aftercare.
CRS and HIPEC is an aggressive combination with considerable treatment related morbidity and mortality. Therefore, further development of strategies to aid in clinical decision-making is fundamental for the improvement and evolution of this approach. From

Summary and Future Perspectives |
217
a clinical point of view, we gained insight into possible inclusion of patients with liver metastases for CRS and HIPEC. In addition, we described the negative effect of infectious complications after HIPEC on the success of bowel continuity restoration long after the initial surgical procedure. This finding will aid in the counselling of CRS and HIPEC patients who are actively requesting bowel restoration. In addition to our clinical findings, we found very promising molecular markers of prognosis after CRS and HIPEC and of Mitomycin C (MMC) sensitivity. Furthermore, we have explored possible biomarkers for cancer-specific survival after primary resection of Microsatellite Instable (MSI) CRC, which have been described to preferentially metastasize to the peritoneal surface and to be less sensitive to regiments containing 5-FU. Advancing our understanding of the molecular basis of this undeniably complex process will be challenging, but ultimately very rewarding. These biomarkers have the potential to be powerful allies in the treatment of our patients by further enabling the treatment team to tailor this aggressive, but effective modality based on disease biology to better suit the needs of the individual patient.
The future
The need for additional tools in aid of continuous refinement of both patient selection and the treatment itself is critical in improving the outcome for our patients. From a clinical viewpoint future efforts should focus on uncovering additional clinical patient selection criteria. Not only to identify patients that will have the best outcome after CRS and HIPEC, but also to try to identify the patients deemed excellent candidates for this combined approach but alas intra-operatively are found to be unsuitable. Continuing efforts from our group and collaborators are currently focussed on indentifying clinicopathological factors that can be assessed pre-operatively. Firstly, by means of an extensive systematic review and meta-analysis of all published data to date. The available tools, at present, rely heavily on intraoperative findings. Preoperative patient selection is preferential, because it allows for a more patient-centred approach with increased information, less morbidity and early referral for systemic therapy. In addition, with the growing stress on our healthcare system, both on specialized personnel and finances, it would be more desirable to be able to identify patients who are not suitable for this approach beforehand, i.e. preoperatively, in order to minimize the burden on hospital resources. Last, but certainly not least, we feel it would aid in avoiding the uncertainty, and thus emotional burden on the patient, that accompanies an approach based on largely intra-operative findings. To achieve this the combination of the growing amount of clinical data available worldwide from expert centres is the key to unlocking a robust clinical profile we can utilize for optimal patient counselling and care.
A profile or selection algorithm based on solely clinical data is an excellent starting

| Summary and Future Perspectives
218
point, however adding specific biomarkers to the diagnostic and work-up trajectory could greatly improve the chances of creating a more reproducible and sound profile on which to adequately select patients for this type of combined treatment modality. A multimodal approach in the truest sense of the word.
Our future preclinical work will focus on further tailoring the treatment, based on the patient’s individual tumour characteristics. Ideally, future efforts to uncover additional molecular markers in PM of CRC would be undertaken with the aid of high-throughput methods, such as next-generation sequencing either as a stand-alone technique or combined with a proteomic approach on a well-defined, large patient cohort from the Dutch Peritoneal Oncology Group (DPOG) and international affiliated organisations. The findings should subsequently be validated by for example immunohistochemistry and functional assays. Furthermore, we are looking forward to the design of clinical studies in the future to further investigate the findings with respect to MMC sensitivity. The addition of anti-VEGF and other (targeted) therapies to the treatment arsenal for patients who develop PM of CRC should also be further studied, with a special focus on patients deemed inoperable who are subsequently treated neo-adjuvantly.
The omics-revolution in medicine is moving forward at a very high speed, facilitating the development of new trial designs where patients are included based on the biology of their disease, as well as to enable earlier read out of end-points (e.g. ctDNA), which enables real-time reaction in the inclusion of patients and ultimately implement cutting-edge medicine in the clinic faster. With the further development and careful implementation of molecularly driven medicine in oncology, the question is not if, but when these techniques will be implemented in this category of CRC patients, i.e. specifically those with peritoneal metastases. In the future, the use of combined clinical and molecular prognostic and predictive markers will lead to true patient centred, tailored medicine in peritoneal metastases of colorectal cancer. Cooperation between expert centres, not only nationally, but internationally will be of vital importance in order to provide improved treatment and care for our patients at the fastest pace possible.

Nederlandse Samenvatting


Nederlandse Samenvatting |
221
Nederlandse samenvatting
Bij 20% van de colorectaal carcinoom (CRC) patiënten wordt bij initiële diagnose uitgezaaide ziekte vastgesteld. Van deze patiënten ontwikkeld ca. 25% uitzaaiingen naar het buikvlies, oftewel peritoneaal metastasen (PM), hetzij geïsoleerd of in combinatie met andere uitzaaiingen, naar bijvoorbeeld de lever. In het verleden werden PM beschouwd als incurabele ziekte en werd de patiënt in kwestie verwezen voor palliatieve chemotherapie. Tegenwoordig is chirurgische behandeling van zowel lever- als long metastasen de gouden standaard, onder voorwaarde dat de metastasen in hun totaliteit, veilig chirurgisch kunnen worden verwijderd. Jaren werd er gedacht dat deze aanpak niet adequaat zou zijn voor het behandelen van PM. Echter, is er een subgroep van CRC patiënten die zich uitsluitend met PM presenteren, wat leidde tot de hypothese dat dit toch een lokale vorm van verspreiding van de ziekte betreft en dus wellicht wel adequaat chirurgisch zou kunnen worden benaderd. Deze gedachte heeft geleid tot de ontwikkeling van een nieuwe behandelingsvorm in de jaren tachtig-negentig, wat bestond uit een chirurgische aanpak gecombineerd met hypertherme, dus verwarmde, intra-peritoneale chemotherapie. De behandeling staat heden ten dage beter bekend als cytoreductieve chirurgie (CRS) en hyperthermic intraperitoneal chemotherapy, oftewel HIPEC. De introductie van deze behandeling kan worden bestempeld als revolutionair in de behandeling van patiënten met uitzaaiingen naar het peritoneum. Na behandeling met CRS en HIPEC werden 5-jaars overlevingspercentages van 35-45% gemeld, wat vergelijkbaar is met de 5-jaars overleving na curatieve resectie van levermetastasen. Ondanks de geboekte vooruitgang zijn er nog verscheidene klinische behoeften welke geadresseerd dienen te worden in deze bijzondere populatie patiënten. De behandelingsgerelateerde morbiditeit en mortaliteit bedraagt respectievelijk 10-20% en 1-5%. Gezien het majeure chirurgie betreft met een hoog percentage behandelingsgerelateerde complicaties, is het van levensbelang de patiënten selectie te verbeteren ter reductie van morbiditeit en mortaliteit. Het is hiervoor niet alleen belangrijk patiënten te excluderen die wellicht niet geschikt zijn voor deze behandelingsstrategie, maar het is cruciaal om juist de patiënten die het meeste baat hebben bij deze behandelingsvorm tijdig te identificeren. Bovendien is de chemotherapie welke gebruikt wordt tijdens de behandeling nog altijd gebaseerd op een zogenaamde “one-size fits all” principe, zonder additionele stratificatie/selectie gebaseerd op de biologie van de tumor.
Overeenkomstig de initiële behandelingsstrategie van deze populatie CRC patiënten, behoeft ook de nazorg een gemodificeerde aanpak. Deze patiënten hebben vaak zeer uitgebreide chirurgie ondergaan en missen, als onderdeel van de behandeling, een essentieel onderdeel wat een grote rol speelt in het bedwingen van eventuele intra-abdominale infecties, namelijk het peritoneum.

| Nederlandse Samenvatting
222
Met het in kaart brengen van deze verscheidene klinische behoeften, beoogden wij meer inzicht te krijgen in zowel klinische als biologische processen als eerste stap richting de ontwikkeling van oplossingen voor deze vraagstukken. Tevens is het continu verbeteren van dergelijke processen een zeer belangrijk doel op zich. In dit proefschrift bespreek ik verschillende mogelijke factoren die van invloed zijn op de behandelingsuitkomst van patiënten met uitzaaiingen naar het buikvlies van CRC. Het betreffen zowel klinische als histopathologische en moleculaire kenmerken.
Klinische besluitvorming / Selectie voor behandeling
Hoofdstuk 2 van dit proefschrift bestaat uit een systematische review en meta-analyse, waarbij er is gekeken naar de overleving na CRS & HIPEC bij patiënten met een combinatie van PM en lever metastasen. Naar aanleiding van ons onderzoek konden wij concluderen dat er geen statistisch significante overlevingsverschil kon worden aangetoond tussen patiënten met alleen PM en patiënten met zowel PM als lever metastasen na behandeling middels HIPEC (pooled HR: 1.24 [95% BI: 0.90 – 1.60]). Tevens werd een tendens waargenomen bij patiënten met zowel PM als lever metastasen richting betere overleving na CRS en HIPEC in combinatie met resectie van de levermetastase(n) in vergelijking met na behandeling met (moderne) systemische chemotherapie.
Adequate, aan de specifieke behoeften van deze patiëntenpopulatie, aangepaste nazorg is essentieel wanneer patiënten voor langere tijd ziekte-vrij zijn. CRS en HIPEC heeft de overleving van een selectie van patiënten met PM van CRC significant verbeterd. Soms wordt er tijdens de operatie, om complicaties van een zogenaamde “lage naad” te voorkomen, een colostoma aangelegd. De morbiditeit en mortaliteit die gepaard gaan met het opheffen van een colostoma is in deze populatie patiënten echter niet bekend. In hoofdstuk 3 hebben we ons derhalve gefocust op de associatie tussen vier klinische en 10 behandelings- of operatie gerelateerde factoren en de uitkomst, c.q. complicaties na het opheffen van de stoma. 21 van de 336 patiënten met een colostoma hebben uiteindelijk verzocht deze op te heffen. Het percentage patiënten die hierbij een complicatie kreeg bedroeg 67%, waarbij in 33% er sprake was van een complicatie van infectieuze aard. Er werd ook een associatie gezien tussen infectieuze complicaties en een verminderde kans op succesvolle opheffing van het colostoma wat betekent dat er dus een verminderde kans is op adequate continuïteitsherstel (p=0.05). De theorie die hieraan te grondslag ligt is dat dit veroorzaakt wordt door een verminderd vermogen tot het indammen van intra-abdominale infectieuze complicaties na een complete peritonectomie, wat een standaard onderdeel is van de behandeling middels CRS en HIPEC.

Nederlandse Samenvatting |
223
De uiteindelijke succespercentage gezien in ons cohort, bedroeg 71%. Concluderend kunnen wij stellen dat het succespercentage van het opheffen van een stoma in deze populatie vrij hoog is, echter gaat deze wel gepaard met een relatief hoge kans op complicaties.
Een Moleculaire Aanpak – Hulpmiddelen voor Klinische Besluitvorming in de Toekomst
De huidige selectie van patiënten voor CRS en HIPEC is gebaseerd op klinische parameters en intra-operatieve bevindingen. In de praktijk betekent dit dat patiënten met een “Peritoneal Cancer Index”, oftewel PCI van minder dan twintig of een vereenvoudigde PCI van minder dan 5 worden beschouwd als de meest ideale kandidaten voor deze behandelingsmodaliteit. Gebaseerd op de hypothese dat onderliggende biologische processen of mechanismen het klinisch beloop voor een belangrijk deel bepalen, zouden zogenaamde biomarkers (moleculen) een belangrijke rol kunnen gaan spelen in de verfijning en verbetering van de patiënten selectie. Een bijkomend voordeel is dat zich onder deze moleculen wellicht ook zogenaamde “drugable targets” bevinden. Dit zijn moleculen waar reeds bekende therapieën op kunnen aangrijpen, om zo het behandelingsarsenaal uit te breiden in de hoop op een betere uitkomst voor deze patiënten.
Er is relatief weinig bekend over de biologische processen die ten grondslag liggen aan intra-abdominale verspreiding van CRC. Hoofdstuk 4 bestaat uit een overzicht van moleculen waarvan bekend is dat die mogelijk een rol spelen in het disseminatieproces wat zich intra-abdominaal afspeelt. Ook wordt er in dit hoofdstuk gekeken naar de mogelijkheden qua klinische toepasbaarheid van deze moleculen of biomarkers. In een serie van meer dan 100 studies naar PM welke zijn gepubliceerd tussen 1990 en 2010, bleken IGF-1, HIF1α, VEGF, EGFR en ITGB1 de meest interessante kandidaten voor eventuele klinische toepassing. Ofschoon deze kandidaten als zeer interessant worden bestempeld behoeven ze verdere validatie alvorens er überhaupt sprake kan zijn van een introductie in de kliniek. Volgens het model besproken in hoofdstuk 4, is de adhesie van tumorcellen aan het peritoneale oppervlak een van de cruciale stappen in het disseminatie proces. In hoofdstuk 5 geven wij een overzicht van de meest onderzochte en functioneel belangrijke adhesie moleculen. Theoretisch zou het blokkeren van deze moleculen een belangrijke doorbraak kunnen zijn in de preventie van PM. Het idee is dat door de blokkade van deze stap men in staat zou zijn om de adhesie van tumorcellen aan het peritoneaal oppervlak te voorkomen, waardoor er uiteindelijk ook geen uitgroei kan plaatsvinden bij patiënten die risico lopen hierop. De meest onderzochte moleculen in deze context waren integrine α2β1, CD44s en MUC16. Verder zouden L1CAM, EpCAM, MUC1, sLex en Lex, chemokine receptoren, Betaig-H3 en uPAR hier ook mogelijk een belangrijke rol in spelen. Op basis van de meest

| Nederlandse Samenvatting
224
recente literatuur zouden de bloedgroep antigenen en MUC16 de meest veelbelovende biomarkers zijn bij het colorectaal carcinoom. Het verder uitbouwen van onze kennis van de diagnostische en mogelijke therapeutische waarde van deze moleculen lijkt een veelbelovende en vooral logische stap in de optimalisatie en personalisatie van de behandeling van patiënten met PM van CRC. Naast adhesie, lijkt angiogenese een belangrijke rol te spelen in de vorming van PM. Angiogenese is vaatnieuwvorming, een proces wat van cruciaal belang is in de groei en ontwikkeling van tumor op meer dan 150-200 micrometer verwijderd van de dichtstbijzijnde bloedvat en dus van het uitgroeien van een micrometastase (niet te zien met het blote oog) tot een macrometastase. Angiogenese is afhankelijk van o.a. complexe interacties tussen verscheidene celtypen en het zogenaamde extracellulaire matrix. Tot op heden is het exacte proces niet ontrafeld, maar lijkt er een belangrijke rol te zijn voor de adhesiemolecuul VCAN hierin. Het wordt gesuggereerd dat VCAN gemedieerde angiogenese, oftewel vaatnieuwvorming, afhankelijk is van de interactie tussen VCAN en Vascular Endothelial Growth Factor (VEGF). In hoofdstuk 6 hebben wij de relatie tussen expressie van beide eiwitten en de uitkomst na CRS en HIPEC geanalyseerd. Onze studie toonde dat hoge expressie van VCAN eiwit in het tumor stroma geassocieerd is met een hogere vaatdichtheid (MVD), hoger T-stadium, maar ook met een hogere kans op een macroscopisch radicale resectie. De mate van VCAN expressie door de tumorcellen was ook geassocieerd met een hogere MVD en een hogere kans op een macroscopisch radicale resectie. Bij multivariate analyse werd een associatie aangetoond tussen vereenvoudigde PCI score, de mate van expressie van VEGF, leeftijd, mate van expressie van VCAN, de status van de lymfklieren (wel of geen metastasen) en de overleving na CRS en HIPEC. De mogelijke rol van VEGF in het voorspellen van de uitkomst na CRS en HIPEC ondersteund, theoretisch, de gedachte dat deze patiënten in aanmerking zouden kunnen komen voor (neo-)adjuvante behandeling met anti-VEGF therapieën. Een andere interessante bevinding is dat epitheliale expressie van het VCAN eiwit geassocieerd is met een relatief goede uitkomst na CRS en HIPEC. Een theorie is dat de epitheliale expressie van VCAN mogelijk gerelateerd is aan de gevoeligheid voor chemotherapie van de tumorcellen. De mogelijke invloed van VCAN expressie van tumorcellen en de gevoeligheid voor chemotherapeutica onderstreept in onze ogen het belang van verder, systematisch, onderzoek en daardoor beter inzicht in de complexe interacties tussen tumorcellen en hun omgeving, in dit geval het peritoneale oppervlak. Deze kennis kan vervolgens lijden tot de identificatie van mechanismen die bijdragen aan gevoeligheid voor chemotherapie in deze groep patiënten.
In hoofdstuk 4 hebben wij vanuit de literatuur verscheidene, veelbelovende biomarkers geïdentificeerd welke ingezet zouden kunnen worden in de verbetering van patiënten selectie. De hypothese luidt dan ook dat we deze biomarkers zouden kunnen gebruiken

Nederlandse Samenvatting |
225
voor dit doel in deze specifieke populatie van patiënten met gemetastaseerde ziekte. Zoals eerder gesteld is vaatnieuwvorming, oftewel angiogenese een belangrijke factor in de ontwikkeling van metastasen. In hoofdstuk 7 hebben we de expressie van verscheidene angiogenese gerelateerde eiwitten geanalyseerd, te weten; HIF1a, SDF1, CXCR4 en VEGF alsook de vaatdichtheid (MVD). Vervolgens hebben wij gekeken naar de relatie tussen de mate van expressie van deze eiwitten, de MVD en de prognose van CRS en HIPEC patiënten. Univariate analyse toonde dat een hoge PCI score, een macrosocpisch irradicale resectie en een hoge VEGF expressie gerelateerd waren aan een slechtere overleving na behandeling met CRS en HIPEC. Er werd geen associatie aangetoond tussen de mate van expressie van de overige eiwitten, MVD en overleving na behandeling. Ook bij multivariate analyse werd een onafhankelijke relatie aangetoond tussen PCI score, resectie uitkomst en mate van VEGF expressie en uitkomst na behandeling. Gezien de uitkomsten, concluderen wij dat VEGF mogelijk ingezet zou kunnen worden als prognostisch instrument. Hiernaast zou dit kunnen betekenen dat de behandeling van deze patiënten met anti-VEGF gebaseerde therapieën meerwaarde kan hebben in deze populatie patiënten. Onze studie draagt bij aan het idee dat juist de combinatie van deze chirurgische aanpak met een systemische benadering, in de vorm van o.a. anti-VEGF gebaseerde therapie, een zeer interessante invalshoek vormt voor het verder verbeteren van de overleving na behandeling middels CRS en HIPEC.
In de meerderheid van de patiënten met levermetastasen (LM) van CRC blijkt resectie uiteindelijk niet curatief te zijn, ondanks het feit dat deze behandeling in opzet wel curatief is. De overexpressie van de eiwitten HIF1a, GLUT1 en VEGF staan bekend als geassocieerd met tumor progressie en een slechtere prognose bij patiënten met CRC in het algemeen. In hoofdstuk 8 hebben wij zowel de individuele als gecombineerde prognostische waarde geanalyseerd van deze drie eiwitten in een multi-center cohort van patiënten met gereseceerde LM. Hoge expressie van GLUT-1 was geassocieerd met een slechtere prognose, met name in patiënten behandeld met systemische chemotherapie. Een hoge expressie van VEGF was ook geassocieerd met een slechtere prognose, echter in patiënten die niet waren behandeld met systemische chemotherapie. Derhalve, lijkt de beoordeling van zowel de mate van expressie van GLUT-1 als VEGF een waardevol instrument te zijn in de verbetering van de patiënten selectie voor resectie. Bovendien, zouden patiënten met een hoge expressie van beide eiwitten de beste kandidaten kunnen vormen voor additionele systemische chemotherapie.
Onderdeel van de HIPEC behandeling is een intra-peritoneale spoeling met chemotherapeutica, waaronder het middel Mitomycine C (MMC) om de microscopische rest-ziekte na resectie te elimineren. De MMC wordt voor toediening verwarmd. De keuze

| Nederlandse Samenvatting
226
voor MMC is tweeledig; Enerzijds is het middel direct cytotoxisch met een penetrantie in het weefsel van slechts een tot twee mm, wat als bijkomend voordeel heeft dat dit in theorie tot minder systemische bijwerkingen zou leiden terwijl het toch de microscopische ziekte attaqueert. Ondanks een lage PCI score en een macroscopisch radicale resectie werd toch gezien dat er een subgroep patiënten een slechtere overleving hadden na behandeling middels CRS en HIPEC. Hypothetisch zou dit kunnen liggen aan een verminderde gevoeligheid van de tumorcellen voor een deel van de behandeling, namelijk het chemotherapeuticum MMC. In hoofdstuk 9, hebben we multipele mogelijke markers voor respons op MMC geanalyseerd ten einde de behandeling toe te snijden op het profiel van de patiënt en zodoende de overleving te verbeteren voor deze subgroep. De werking van MMC berust op DNA-crosslinking, waarbij er DNA schade optreedt en als gevolg hiervan geen DNA replicatie meer kan plaatsvinden. Uiteindelijk leidt dit proces tot apoptose oftewel celdood. Er zijn twee mechanismen waardoor een tumorcel resistent kan worden voor MMC. 1) MMC dient geactiveerd te worden alvorens deze werkzaam is. Er zijn verschillende enzymen, reductases genoemd, die MMC kunnen activeren doormiddel van enzymatische reductie, waarvan DT-diaphorase de meest potente en meest onderzochte is. 2) Een andere wijze waarop dit plaats kan vinden is als de tumorcellen in staat zijn om de DNA schade te repareren, doormiddel van de activatie van de Fanconi Anaemia-BRCA (FA-BRCA) pathway of de ATM-ATR pathway, die beide de RAD51C kern foci reguleren die DNA herstel middels homologe recombinatie of nucleotide excision repair (NER) medieert. Voor onze studie hebben wij de MMC gevoeligheid bepaald van in totaal 12 CRC cellijnen en deze werd gecorreleerd aan de mRNA expressie van 37 genen die gerelateerd zijn aan zowel de Fanconi Anaemia (FA)-BRCA pathway, ATM-ATR pathway als de enzymatische activatie van MMC. Additioneel, functioneel onderzoek is gedaan in deze cellijnen naar de functionaliteit van de FA-BRCA pathway middels een chromosomale breuk en Western Blot voor het FANCD2 eiwit. Het aantal chromosomale breuken correspondeert met de functionaliteit van de FA-BRCA pathway. In cellen met een niet-functionele FA-BRCA pathway worden meer den 10 breuken per cel waargenomen. Een aanvullende stap in de analyse van de activiteit van deze pathway is het aantonen van het FANCD2 eiwit. FANCD2 wordt gemonoubiquitineerd indien er sprake is van DNA schade, wat leidt tot de activatie van DNA herstel mechanismen. Hoge sensitiviteit voor MMC correleerde in onze studie met een lage mRNA expressie van zowel Bloom syndrome protein (BLM) als BRCA2. Echter toonden de uitgevoerde functionele FA-BRCA assays/testen geen correlatie met MMC gevoeligheid. De verdere analyse van BLM werd gedaan middels immunohistochemische kleuringen voor het eiwit in zowel cellijnen als patiëntmateriaal. In de cellijnen correspondeerde een lage BLM expressie met een hoge sensitiviteit voor MMC. Vervolgens werd een significante

Nederlandse Samenvatting |
227
associatie waargenomen tussen een lage BLM expressie in het patiëntmateriaal en een betere uitkomst (overleving) na CRS en HIPEC. Concluderend kunnen wij stellen dat in onze studie een lage expressie van BLM geassocieerd was met een hogere sensitiviteit voor MMC en een betere overleving na CRS en HIPEC. Deze bevindingen ondersteunen de gedachte dat er een mogelijke rol is weggelegd voor BLM in de predictie van MMC gevoeligheid in CRS en HIPEC patiënten. Verder onderzoek is, op basis van deze gegevens, zeker geïndiceerd alvorens over te gaan naar een mogelijke klinische toepassing.
Het is beschreven dat de voorkeurslokalisatie voor metastasen van microsatelliet instabiele (MSI) CRC het peritoneum is. Echter is dit fenotype geassocieerd met een relatief gunstige prognose, vergeleken met microsatelliet stabiele (MSS) CRC. In MSS CRC is bekend dat een mutatie in het BRAF gen, om precies te zijn de V600E mutatie, geassocieerd is met een ongunstige prognose. Deze mutatie komt in ongeveer 40% van de MSI carcinomen voor, maar de klinische relevantie qua prognose hiervan in de MSI setting is onbekend. In hoofdstuk 10, hebben we het effect van zowel BRAF als KRAS mutaties op de overleving bestudeerd in stadium II en III patiënten met een MSI fenotype. BRAF V600E kwamen voor in 51% van de geïncludeerde patiënten en KRAS mutaties in 16%. Patiënten met tumoren zonder mutaties in beide genen, zogenaamde dubbel wild-type tumoren, hadden een buitengewoon goede prognose met een kanker specifieke 5-jaars overleving van 93%, alwaar patiënten met tumoren met een mutatie in BRAF of KRAS een 5-jaars kanker specifieke overleving toonden van 73%. Ook bij multivariate analyse was dit verschil significant. Mutaties in zowel BRAF als KRAS zouden samen geanalyseerd moeten worden in studies naar prognostische waarde van deze mutaties in MSI CRC. Patiënten met mutaties in een van deze twee genen zouden baat kunnen hebben bij adjuvante therapie, welke idealiter afgestemd dient te worden aan de specifieke biologische kenmerken van de tumor in kwestie.
Conclusie
In zijn algemeenheid hebben de studies waaruit dit proefschrift bestaat ons zeer waardevolle en bruikbare inzichten verschaft in zowel klinische als moleculair biologische processen en factoren die van invloed zijn op de gehele traject van de zorg en behandeling van patiënten met peritoneaal metastasen (PM) van het colorectaal carcinoom (CRC). Het is bekend dat CRS en HIPEC een vrij agressieve behandeling is met een relatief hoge behandelingsgerelateerde morbiditeit en mortaliteit. Daarom is het van groot belang om het werk voort te zetten ten einde meer inzicht te krijgen in deze klinische en moleculair biologische factoren die mogelijk van invloed zijn op het klinisch beloop. Deze kennis kan dan benut worden in de verbetering en “finetuning” van de klinische besluitvorming, welke zich mogelijkerwijs zal vertalen in een verbetering van de overleving na CRS en HIPEC.


List of Publications


List of Publications |
231
Ex-vivo Artifacts and Histopathological Pitfalls in the LungThunnissen E, Blaauwgeers HJ, de Cuba EM, Yick CY, Flieder DB.Arch Pathol Lab Med. 2016 Mar;140(3):212-20.
Versican and vascular endothelial growth factor expression levels in peritoneal metastases from colorectal cancer are associated with survival after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy.Sluiter NR, de Cuba EM, Kwakman R, Meijerink WJ, Delis-van Diemen PM, Coupé VM, Beliën JA, Meijer GA, de Hingh IH, Te Velde EA.Clin Exp Metastasis. 2016 Apr;33(4):297-307
Clinicopathological Parameters in Patient Selection for Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Cancer Metastases: A Meta-analysis.Kwakman R, Schrama AM, van Olmen JP, Otten RH, de Lange-de Klerk ES, de Cuba EM, Kazemier G, Te Velde EA.Ann Surg. 2016 Jan 7. Epub ahead of print
Angiogenesis-Related Markers and Prognosis After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Metastatic Colorectal Cancer.de Cuba EM, de Hingh IH, Sluiter NR, Kwakman R, Coupé VM, Beliën JA, Verwaal VJ, Meijerink WJ, Delis-van Diemen PM, Bonjer HJ, Meijer GA, Te Velde EA.Ann Surg Oncol. 2016 May;23(5):1601-8
A prognostic classifier for patients with colorectal cancer liver metastasis, based on AURKA, PTGS2 and MMP9.Goos JA, Coupé VM, van de Wiel MA, Diosdado B, Delis-Van Diemen PM, Hiemstra AC, de Cuba EM, Beliën JA, Menke-van der Houven van Oordt CW, Geldof AA, Meijer GA, Hoekstra OS, Fijneman RJ; DeCoDe PET Group.Oncotarget. 2016 Jan 12;7(2):2123-34.
Prognostic value of BRAF and KRAS mutation status in stage II and III microsatellite instable colon cancers.de Cuba EM*, Snaebjornsson P*, Heideman DA, van Grieken NC, Bosch LJ, Fijneman RJ, Belt E, Bril H, Stockmann HB, Hooijberg E, Punt CJ, Koopman M, Nagtegaal ID, Coupé VH, Carvalho B, Meijer GA.Int J Cancer. 2016 Mar 1;138(5):1139-45.

| List of Publications
232
Molecular biology of peritoneal carcinomatosisR Kwakman, NR Sluiter, EM de Cuba, EA te VeldeIntraperitoneal Cancer Therapy: Principles and Practice, 61 (Chapter in a book)
Tailoring heated intraperitoneal mitomycin C for peritoneal metastases originating from colorectal carcinoma: a translational approach to improve survival.Kwakman R*, de Cuba EM*, de Winter JP, de Hingh IH, Delis-van Diemen PM, Tijssen M, Rooimans MA, Krijgsman O, Carvalho B, Peters GJ, Bonjer HJ, Meijer GA, Te Velde EA.Br J Cancer. 2015 Mar 3;112(5):851-6.
Glucose Transporter 1 (SLC2A1) and Vascular Endothelial Growth Factor A (VEGFA) Predict Survival After Resection of Colorectal Cancer Liver Metastasis.Goos JA, de Cuba EM, Coupé VM, Diosdado B, Delis-Van Diemen PM, Karga C, Beliën JA, Oordt CW, Geldof AA, Meijer GA, Hoekstra OS, Fijneman RJ; DeCoDe PET Group.Ann Surg. 2016 Jan;263(1):138-45.
Morbidity associated with colostomy reversal after cytoreductive surgery and HIPEC.de Cuba EM, Verwaal VJ, de Hingh IH, van Mens LJ, Nienhuijs SW, Aalbers AG, Bonjer HJ, te Velde EA.Ann Surg Oncol. 2014 Mar;21(3):883-90.
Cytoreductive surgery and HIPEC for peritoneal metastases combined with curative treatment of colorectal liver metastases: Systematic review of all literature and meta-analysis of observational studies.de Cuba EM, Kwakman R, Knol DL, Bonjer HJ, Meijer GA, Te Velde EA.Cancer Treat Rev. 2013 Jun;39(4):321-7.
Understanding molecular mechanisms in peritoneal dissemination of colorectal cancer : future possibilities for personalised treatment by use of biomarkers.de Cuba EM, Kwakman R, van Egmond M, Bosch LJ, Bonjer HJ, Meijer GA, te Velde EA.Virchows Arch. 2012 Sep;461(3):231-43.
Randomized, blinded comparison of transgastric, transcolonic, and laparoscopic peritoneoscopy for the detection of peritoneal metastases in a human cadaver model.Voermans RP, van Berge Henegouwen MI, de Cuba E, van den Broek FJ, van Acker G, Timmer R, Fockens P.Gastrointest Endosc. 2010 Nov;72(5):1027-33.

Dankwoord


Dankwoord |
235
Dankwoord
“It takes a village to raise a child”….. Aan deze quote moet ik steevast denken als ik denk aan dit proefschrift. Zonder de hulp van velen was dit niet mogelijk geweest. Graag zou ik van de gelegenheid gebruik willen maken om enkele mensen, persoonlijk, te bedanken. Mezelf kennende zullen er hiaten zitten in mijn dankwoord. Ik hoop dat degene die ik op dit moment, onbedoeld, vergeet mij dit kunnen vergeven.
Allereerst zou ik de patiënten willen bedanken die dit onderzoek mogelijk hebben gemaakt. Mijn hoop is dat doormiddel van de nu opgedane kennis wij deze behandeling steeds verder kunnen ontwikkelen en verbeteren voor toekomstige patiënten.
Prof. dr. H.J. Bonjer, promotor. Beste professor Bonjer, wat is het een enorm voorrecht geweest om onderdeel te mogen zijn van uw “stal”! Uw “go getter” attitude is altijd een inspiratie geweest voor mij. Niets was onmogelijk en dat heeft u ons als jonge onderzoekers altijd goed ingepeperd tijdens onder andere de wekelijkse research meetings van de afdeling heelkunde. Meetings waarbij u steevast op het juiste moment kwam met ideeën en nieuwe invalshoeken waardoor iemand weer met hernieuwde enthousiasme verder kon. Ook het belang van teamwork is iets wat u ons allemaal heeft bijgebracht, getuige de fantastische sfeer tussen de arts-onderzoekers onderling en met de stafleden, wat alleen maar beter werd na de verhuizing naar de researchkamer op de 7e. Professor Bonjer, woorden schieten tekort. Zeer veel dank voor de mooie, vormende, leerzame tijd op uw afdeling. En last but certainly not least bedankt voor de gezelligheid en meerdere, fantastische ChirurgenCup dagen (Regio 1 rules!). Dat zijn herinneringen die ik altijd bij me zal dragen.
Prof. dr. G.A. Meijer, promotor. Beste Gerrit, wat heb ik een geweldige tijd gehad bij jou en de TP! Wie had ooit gedacht dat de jonge vrouw die ooit bij jullie begon op het lab op een gezamenlijk project met de afdeling heelkunde nu in opleiding zou zijn tot patholoog! Ik had het niet kunnen verzinnen ;) En dat dankzij je enthousiasme over alles wat je kon zien onder een microscoop en wat dat wellicht betekende voor het beloop van de ziekte. Er ging een wereld voor mij open! Gerrit, waar zal ik beginnen… Wat heb ik veel van jou geleerd. Niet alleen op wetenschappelijk vlak. Als ietwat ongeduldige wildebras heb ik van jou geleerd (iets beter ;)) de kalmte te bewaren, als je weer eens tegen mij zei “Rustig aan Erienne, het komt goed.” En warempel, het kwam ook altijd wel goed. Ondanks je zeer drukke agenda heb je ook altijd tijd weten te maken, zeker voor de soms hoognodige peptalks als ik het even niet zag zitten of voor een fantastische brainstormsessie waarna ik weer vol goede moed verder kon. Mijn tijd als onderzoeker bij jou en de TP heeft mij gevormd. Dat is van onschatbare waarde. Gerrit, bedankt voor alles!

| Dankwoord
236
dr. E.A. te Velde, co-promotor. Beste Lisette, ook aan jou heb ik heel veel te danken! Een gesprek eind 2009 tussen mij en toen nog arts-assistent heelkunde Kuhlmann op de artsenkamer van 6Noord aan de andere kant van de Amstel leidde tot een gesprek met jou, toen nog fellow, over de mogelijkheden voor een promotietraject aan de VU. And the rest, as they say, is history! Wat een avontuur. Van het opzetten van de HIPEC behandelingsteam en onderzoeksgroep in de VU, tot het schrijven van onze publicaties, het begeleiden van onze studenten en de gezellige congresbezoeken (Berlijn, Uppsala). En dan ook nog de heelkunde feesten en de ChirurgenCup! Zonder jou tomeloze enthousiasme waarmee je mensen moeiteloos leek mee te krijgen in onze plannen, je kritische blik en jou bezielende volharding had ik hier nu niet gestaan. Lisette, het was een voorrecht om je eerste promovendus te zijn en met jou samen te mogen werken. Heel veel dank voor de kans die je mij hebt gegeven wat uiteindelijk tot dit alles heeft mogen leiden. Op naar nog meer mooie projecten en de volgende promovendus afkomstig uit je groep!
Graag zou ik ook een woord van dank willen richten aan de leden van lees- en promotiecommissies. Beste dr. Ignace de Hingh, dr. Jeroen Meijerink, dr. Monique van Leerdam, Prof. dr. Geert Kazemier, Prof. dr. Iris Nagtegaal, Prof. dr. E. Voest en Prof. dr. Onno Kranenburg, hartelijk dank voor de tijd en moeite welke u besteed heeft aan het kritisch beoordelen van mijn proefschrift en het vertrouwen welke u heeft uitgesproken door zitting te willen nemen in mijn lees- en/of promotiecommissie.
dr. I.H.J.T. de Hingh. Beste Ignace, op een dag mocht ik langskomen in Eindhoven om met jou te praten over ons project en de plannen. Wat een hartelijke ontvangst hebben wij bij jou gehad en wat een fantastische eerste gesprekken zijn dat geweest. Jou enthousiasme werkt aanstekelijk! Ik ben je voor altijd dankbaar voor je vertrouwen in ons en je steun. Je hebt een enorme bijdrage geleverd aan mijn boekje. Ik ben je dan ook zeer erkentelijk dat je deel wilde uitmaken van mijn leescommissie.
dr. W.J.H.J. Meijerink. Beste Jeroen, heel veel dank voor het vertrouwen, je luisterend oor en je hulp toen ik het even nodig had. Ik wens jou en je groep heel veel succes met het voortzetten van de ontzettend mooie imaging projecten waar jullie met hart en ziel aan werken. Ook ben ook ontzettend blij dat je deel hebt willen uitmaken van mijn leescommissie.
dr. V.J. Verwaal. Beste dr. Verwaal, zeer veel dank voor uw inzet en hulp bij het opzetten van de HIPEC in het VUmc. Uw expertise en kritische blik hebben zeker een bijdrage geleverd aan het werk wat zowel klinisch, als wetenschappelijk verricht wordt bij ons in het VUmc.

Dankwoord |
237
Prof. dr. M. van Egmond. Beste Marjolein, ook aan jou ben ik dank verschuldigd voor het delen van jou enorme kennis van de moleculaire biologie met mij. Zeker in mijn beginperiode. Heel fijn dat je de tijd hiervoor nam. Je drive en kennis zijn een inspiratiebron!
Prof. dr. J.P. de Winter†. Beste Johan, ondanks dat je er niet meer bent wilde ik ook jou bedanken voor wat je voor onze groep en voor mij hebt betekent. In de korte tijd dat ik je heb mogen meemaken, heb ik jou gekend als een zeer getalenteerde, en gedreven wetenschapper die tegelijkertijd zeer bescheiden overkwam. Johan, bedankt.
Prof. dr. G.J. Peters. Beste professor Peters, zeer veel dank voor al uw begeleiding bij de onmisbare chemosensitiviteitsproeven. Wat hebben Riom en ik een hoop geleerd tijdens onze afspraken met u.
dr. D.L. Knol en dr. V.J. Coupé, Beste Dirk en Veerle, wat had ik gedaan zonder jullie! Heel veel dank voor jullie tijd en expertise. En Veerle, heel veel dank voor het nakijken van al die powerpoints die wij met jou hebben gedeeld met alle statistische vragen die we maar konden bedenken ;) Het resultaat mag er wezen.
Ook aan de overige mede-auterus ben ik veel dank verschuldigd. Beste Simon Nienhuijs, Arend Aalbers, Martin Rooijmans, Daniëlle Heideman, Eric Belt, Herman Bril, Hein Stockmann, Jeroen Beliën, Eric Hooijberg, Professor Punt en Miriam Koopman, zeer veel dank voor jullie zeer gewaardeerde input en enthousiasme. Het was een waar genoegen om met jullie samen te mogen werken en van jullie te leren.
Pien Delis- van Diemen, paranimf. Lieve Pien, wat ben ik blij dat je naast me zal staan! Zonder jou, was het allemaal niet gelukt. Je hebt van een arts die niet eens kon pipetteren een “half-decent” plak, pipetteer, kweek en kleur OIO weten te maken en dat allemaal in een hele korte tijd! Jouw geduld en enthousiasme heb ik altijd enorm weten te waarderen. En het feit dat je een ontzettende lieverd bent des te meer! Wat een ontzettend fijne tijd hebben we gehad. Pien, it’s an honor and a privilege.
Riom Kwakman, paranimf. Lieve Riom, waar zal ik beginnen… Als eerste Honours-Programme “kuiken” werd je mij toevertrouwd op het Mitomycine C project. Wat heb ik in de loop der jaren veel aan jou gehad! Samen celkweken in het weekend, de grote plakmarathon onder leiding van Pien, het brainstormen onder genot van een kopje koffie, de etentjes met Nina en de gezelligheid. Kortom, we hebben een hoop leuke dingen samen mogen doen en meegemaakt! Onze inspanningen hebben zich inmiddels vertaald in een aantal zeer mooie publicaties, waar ik echt met een fantastisch gevoel op terugkijk. Riom,

| Dankwoord
238
veel dank dat je mij wilt bijstaan! Ik ben zeker dat we over niet al te lange tijd ook voor jou in de aula zullen zijn ;) Heel veel succes!
Ook ben ik dank verschuldigd aan meerdere studenten die op de een of andere wijze hebben bijgedragen aan het onderzoek; Leonieke van Mens, Anne Schrama en Josefien van Olmen. In het bijzonder ook veel dank aan onze tweede Honours-Programme studente Nina Sluiter, wie haar HP-traject fantastisch heeft afgerond! Lieve Nina, knap werk geleverd! Bedankt voor alles wat je hebt gedaan, de mooie figuren, statistiek brainstorm sessies en de gezelligheid. Heel veel succes met alles meissie. Gezien jouw tot nu toe opgedane kennis, kunde en je instelling twijfel ik niet dat het helemaal goed gaat komen Nina!
Pétur Snaebjornsson. Lieve Pétur, wat heb ik met veel plezier met jou samengewerkt. Je geduld, onuitputtelijke kennis, kundige blik en enthousiasme zijn een enorme stimulans geweest. Zeker nodig als het niet allemaal direct van een leien dakje gaat (het is immers onderzoek…). Bedankt voor je vriendschap Pétur, ik ben zo blij dat ik een geweldige promotie-maatje in jou heb gevonden. Ik ben dan ook zeer vereerd dat ik jou paranimf mag zijn. Zeg maar tegen Joost dat ook na deze “bevalling” een celebratory brunch in Amsterdam op zijn plaats is! ;)
Beste Remond en Beatriz. De twee rotsen in de branding voor elke AIOS van de TP. Allebei met een eigen stijl, maar beide op hun eigen manier warm in de begeleiding van de jonge enthousiastelingen. Bedankt voor de goede gesprekken, de aanmoediging en vooral de gezelligheid J Ook op jullie nieuwe plek gaan jullie zeker mooie resultaten boeken!
Aan de collega’s van de TP, de Tumor Genome Core Analysis Unit en de Moleculaire Pathologie ook veel dank! In het bijzonder: Mark (wat hadden we zonder jou gemoeten!), Mireille (bedankt voor alle hulp en praktische tips!), Marlies, Raffaëlla, Pauline (bedankt voor alles!), Josien (Fijn maatje voor in de late uren op CCA 1.10 ;)), Linda (moet nog altijd aan die woest aantrekkelijke man denken…), Sandra (roooooomie!), Evert(tje, toekomstige collega patholoog!), Annemieke, Florence (Flo), Mariska (zoveel energie, hoe doe je dat toch?!), Rinus (Uncle Q), Jeroen B, Meike, Jeroen(tje, Ajax!), Lisette (a.k.a. MirNa, Lysate), Marianne (het gevreesde zwarte boekje…), Anne (gezelligheidsmonster), George, Nicole (bedankt voor het zetje in de goede richting ;)), Oscar (gesprekken met jou gingen altijd de “foute kant” op!), Sjoerd, Jasmijn, Robert, Suzanne, Denise, Saskia, Lise, Wina, Bauke, Daoud, Paul, Francois, Dirk, Ilari, Renske, Leontine, Erik H., Annelies, Mariëtte en Maarten.

Dankwoord |
239
Lieve mede-onderzoekers van de heelkunde! Het is zover, eindelijk! Zonder jullie als o.a. sparring-partners en buddies was het een stuk onaangenamer geweest! Lieverds, bedankt! In het bijzonder wilde ik graag Dieuwertje, Marjolein, Martijn, Georgios, Nicole, Marieke, Saskia, Renske, Karin, Gabor, Max, Wouter, Joanna, Nikki, Kak Khee en Jennifer bedanken. Ook alle (oud) ANIOS, AIOS, Ilse, Wendy, Rita, Ron en stafleden van de afdeling Heelkunde wilde ik zeer hartelijk bedanken voor de mooie tijd en jullie oprechte interesse.
Mede (oud) AIOS van de pathologie: Evita (Snottebel), Teodora (TeoD, a.k.a. el madrino), Clifton (Patron!), David, Kimberly, Mariëlle, Mathilda (Buuf), Anna-Lena, Annefleure, Maartje, Emma W, Emma R, Max, Aart, Shaima, Kim, Lyan, Astrid, Mehrdad, Irene, Sara, Jolanda, Bego (Heaven!) en Edith bedankt voor alle gezelligheid! Een speciaal woord van dank aan de fotografen Jaap en Ron, voor hun hulp bij het maken en bewerken van het beeldmateriaal. Ook de analisten, in het bijzonder de analisten van de uitsnijkamer, immuno en BioBank wilde ik heel hartelijk bedanken voor hun bijdrage aan mijn onderzoek. Ook de pathologen, in het bijzonder Prof. dr. Paul van der Valk en Prof. dr. Elisabeth Bloemena, (oud) opleiders, wilde ik heel graag bedanken voor hun interesse en steun.
Aan het begin van elke tocht staan enkele mensen die je op een of andere wijze hebben geïnspireerd of gemotiveerd. In mijn geval waren dat op Aruba drs. J. Samuels, mw. P. Samuels-Zijlstra, drs. F. Ho-Kang-You en mw. Ho-Kang-You - Arends. Hier in Nederland heb ik mijn eerste voetstappen in de onderzoekswereld mogen zetten onder aanmoediging van en/of hoede van o.a. Prof. dr. Peeters, drs. Ben Saleem, dr. Paul Berger, dr. Rogier Voermans en Prof. dr. Fockens, waarvoor mijn eeuwige dank.
Prof. dr. R. Rojer en mw. J. Rojer-de Cuba, Lieve tio Robby en tante Jeanette, masha danki voor de inspiratie en interesse in mijn onderzoek. Ik prijs me rijk met familieleden zoals jullie.
Aan Diane, Nicole en Clarita; Shonnan, masha danki pa tur cos! Aunque nos no ta wak otro hopi, asina nos wak otro atrobe ta masha gezellig! Keda manda nos hopi potret di boso preciosidadnan. Jean-Jacques and Kelly, guys, no one can quite do a New Year’s Eve, or any party for that matter, like you! I always have such a blast, thank you for all the merriment!
“Las chulas” - Jeanelle, Darice en Gardenia. Ladies, masha masha masha danki voor alle gezelligheid and the sometimes much needed distraction. So much more than cousins!

| Dankwoord
240
Lieve Nicole en Daniëlle, wat had ik toch gedaan zonder jullie! Mijn 020 ladies. Aan jullie beide veel dank voor het altijd klaarstaan voor mij en de soms broodnodige afleiding in de vorm van feestjes, fantastische etentjes en cocktails :D Ook aan Marijke, Chantal, Merel, Maurice, Carien, Piet-Hein, Thomas en Danny veel dank voor de mooie tijd en fantastische herinneringen. Many more to come!
Oom Joop†, tante Sybilla, Vanja, Wytze, Kevin, Niklas*, Joop en Mieke, ook wel bekend als de Arubaanse tak van de Brattinga’s. Ook al zien we elkaar minder vaak dan ik graag zou willen, wil ik jullie heel erg hartelijk bedanken voor mijn “thuis” bij jullie. Zonder jullie was ik nooit teruggekomen uit Aruba en in Groningen gebleven in 2004 ;) Masha danki y un braza hopi duro y sunchi!
Lieve Roman, Lizet, Paul, Florien en Tessa, wat ben ik bevoorrecht met een schoonfamilie zoals jullie! Vanaf het eerste moment heb ik me altijd erg welkom gevoeld bij jullie. Inmiddels negen jaar, meerdere feestjes, etentjes, tripjes naar Wieleń, weekendjes weg naar-een-niet-nader-te-noemen-park en een gezamenlijke vakantie op Aruba verder is het gelukkig nog steeds zo J Jongens, Dziękuję bardzo!
De Brattinga Clan. Lieve Oma, Ben, Doayenne, Lynne, Lisette, Vera en Riki, bedankt voor de veilige thuishaven die jullie samen met mamma vormen voor mij, Kaye & co. Op tijden waarop het wat tegen zit, kan ik me altijd troosten met de gedachte dat het nog een x aantal maanden duurt voor ik me weer bij jullie, in het warmste nest wat iemand zich maar kan wensen, kan voegen op het zonnige pareltje in de Caribische zee wat wij thuis mogen noemen. Ik ben gezegend met een fantastische jeugd, waar ik goede herinneringen aan heb, mede dankzij jullie. Bedankt voor jullie liefde en steun. En ook voor de vele Happy Hours bij oma! :D
Ook dank aan de families, de Cuba, Solognier en Borowski voor het meeleven en steun deze afgelopen jaren. Ook al begreep niet iedereen helemaal waar ik mee bezig was, werd jullie frisse blik op de zaak en interesse zeer gewaardeerd!
Lieve pappa. Veel te vroeg ben je heengegaan. Ik had nog graag veel vaker naar je kwajongensverhalen van vroeger willen luisteren of gesprekken met je willen voeren over heden, verleden en toekomst op de veranda in Venezuela.

Dankwoord |
241
Lieve, kleine Kaye. Inmiddels niet zo klein meer en ook al bijna afgestudeerd als arts! Hopi proud dibo ruman! Wat is het een feest om een zusje te hebben zoals jij. Je bent een mooie, gezellige, vrolijke en enthousiaste verschijning. And smart as a whip too! Geen wonder dat Damiano je charmes niet kon weerstaan ;) Lieve D, welcome to the clan. Je bent een geweldige aanwinst J Kaye, geen haar op mijn hoofd die eraan twijfelt dat je het he-le-maal gaat redden. Volg je hart. Ik sta altijd achter je.
Lieve mamma. Mijn held en grote voorbeeld. Het harde werken en discipline hebben die kleine en ik niet van een vreemde! Ondanks dat je een drukke baan hebt heb je altijd, maar dan ook altijd tijd gemaakt voor ons. Wat zijn Kaye en ik bevoorrecht met een moeder zoals jij. Een sterke, onafhankelijke, doch zeer lieve en warme vrouw. Wat bewonder ik hoe je altijd alle ballen in de lucht weet te houden. Bedankt voor alle geduld, liefde en het feit dat je ons hebt grootgebracht met het idee dat we konden worden wat we maar wilden, mits we er vol voor gingen en bereid waren hard te werken. Niets is onmogelijk. Dit boekje bewijst ook maar weer dat mamma altijd gelijk heeft! ;)
Lieve Jan, dushi van me. Hier zijn we dan, 9 jaar na “ ’t Vaatje ” in Grunn. Ik had die negen fantastische jaren voor geen goud willen missen! Wat ben ik toch een bofkont met een echtgenoot zoals jij: intelligent, moedig, grappig, charmant EN lief! Ik ben erg trots op je en bewonder jou enorm, Jan. Bedankt voor al je steun dushi, zonder jou was ik er wellicht niet zonder kleerscheuren vanaf gekomen ;) Ik hoop dat wij nog jaren van elkaars gezelschap mogen genieten en nog meer leuke avonturen mogen beleven samen! Ik kijk er naar uit! Love you.


13653_DeCuba_OM_v1.indd 2 19-04-16 12:33

Towards Personalized Medicine in Treatment and Care of Patients
with Peritoneal Metastases of Colorectal Cancer
Erienne Marie-Luise Véronique de Cuba
Towards Personalized M
edicine in Treatment and C
are of Patients with Peritoneal M
etastases of Colorectal C
ancer Erienne de C
uba
INVITATION
voor het bijwonen vande openbare verdediging
van het proefschrift
Towards Personalized Medicine in Treatment
and Care of Patients with Peritoneal Metastases of Colorectal Cancer
door
Erienne Marie-Luise Véronique de Cuba
Donderdag, 9 juni 2016Om 13.45
In de aula van deVrije Universiteit
De Boelelaan 1105te Amsterdam
met aansluitend receptie
ParanimfenPien Delis-van Diemen
[email protected] Kwakman
Erienne de CubaHoutmankade 43 HS
1013 MR, [email protected]
Erienne Marie-Luise Véronique de Cuba was born on the 25th of October 1983 on the sunny island of Aruba as the eldest child in a family of four. After completing high school (VWO) in 2002 on the one happy island at the Colegio Arubano, she proceeded to study medicine in Groningen at the Rijksuniversiteit Groningen.
In December 2009 she completed her medical studies, during which she concluded several internships focussed on gastro-intestinal malignancies and a research project at the department of Gastroenterology and Hepatology of
the Academic Medical Center Amsterdam on the treatment of pancreatic pseudocysts after pancreatitis under the leadership of Prof.dr. P. Fockens.
She started her PhD in February 2010 on clinical and molecular profiling of patients presenting with peritoneal metastases of colorectal cancer under the guidance of dr. E.A. te Velde, prof.dr. H.J. Bonjer and prof.dr. G.A. Meijer. at the VU University Medical Center.
In the fall of 2013 she started her residency in surgical pathology at the VU Medical Center in Amsterdam under the supervision of prof.dr. E. Bloemena and prof.dr. P. van der Valk. The author currently resides with her husband in Amsterdam.
13653_DeCuba_OM_v1.indd 1 19-04-16 12:33