Torsion testis final
12
Dr Arun Gupta Director imaging Dr Rakhee gupta Dr R K S Gandhi Dr Vinayak Mittal Dr Ritesh Mahajan TORSION TESTIS
-
Upload
ritesh-mahajan -
Category
Health & Medicine
-
view
1.565 -
download
5
description
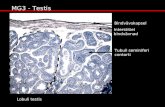
Urogenital ultrasound series : torsion testis
Transcript of Torsion testis final

Dr Arun Gupta Director imaging
Dr Rakhee gupta Dr R K S Gandhi Dr Vinayak Mittal Dr Ritesh Mahajan
TORSION TESTIS

TORSION TESTIS
Torsion is more common in boys than in men, and itrepresents only 20% of the acute scrotal pathologic
phenomena in postpubertal males. However, prompt diagnosis is necessary because torsion
requires immediate surgery to preserve the testis. Acute Sub-Acute Chronic ------------------ Intra- VaginalExtra -Vaginal
NORMAL TORSION

The tunica vaginalis does not completely surround the testis and epididymis, which are attached to the posteriorscrotal wall .
Bell-clapper anomaly. The tunica vaginalis completely surrounds the testis, epididymis,and part of the spermatic cord, predisposing to torsion.
Intravaginal torsion. Bell-clapper anomaly with complete torsion of the spermatic cord, compromising the blood supply to the testis.
Extravaginal torsion in a neonate. Tunica vaginalis is in normal position, but abnormal motility allows rotation of the testis, epididymis, and spermatic cord.

NORMAL ORIENTATION OF THE RT SIDE
TESTIS IS APPRECIATED
AND
CHANGE IN THE LONG AXIS OF THE LEFT SIDE TESTIS
IS SEQUEL TO TORSION
( BELL CLAPPER MORPHOLOGY) .
NORMAL TORSION SEQUAEL

COMPARISON BETWEEN NORMAL
AND ISCHEMIC TESTIS .
NORMAL RT TESTIS HAS MIDLEVEL ECHOES OF THE PARENCHYMA WITH SLOW FLOW VASCULARITY .
HYPOECHOIC / HETEROGENOUS ECHOGENECITY OF LEFT TESTIS ( EARLY TORSION).
HYPERECHOIC ECOPATTERN CAN BE SEEN WITH INFARCTION / HAEMORRHAGE ALSO NORMAL
TESTIS
TORSION SEQUAEL
NORMAL INTRAPARENCHYMAL
VASCULARITY

CORD TESTIS EPIDYDIMIS COMPLEX
1. EPIDYDIMIS may be enlarged and can not
be appreciated as separate from the
cord leading to formation of
CORD / EPIDYDIMIS COMPLEX.
2. EXTRATESTICULAR MASS CAN BE SEQUAEL TO
HAEMORRGAE IN EPIDYDIMIS /
TUNICA VAGINALIS

Circumferential swirl of the vessels is appreciated proximal to the torison site . Distal to the swirl there
is no color fill .
TORSION KNOT The spermatic cord immediately proximal to the testis and epididymis is twisted, causing a
characteristic torsion knot or “whirlpool pattern” of concentric layers.

HIGH RESISTANCE ARTERIAL FLOW IS APPRECIATED JUST PROXIMAL TO THE TORISON SITE
REACTIONARY INCREASE IN THE THICKNESS OF THE SCROTAL SUBCUTIS PLANE WTH INCREASED VASCULARITY OF THE PARATESTICULAR TISSUES ( DARTOS FASCIA )

TORSION TESTIS
In torsion,blood flow is absent in the affected testicle or significantly less than in the normal, contralateral testicle.
NO BLOOD FLOW IS APPRECIATED IN THE EPIDYDIMIS /TESTIS COMPLEX DISTAL TO SWIRL OF BLOOD FLOW REPRESENTING THE TORSION SITE
TORSION KNOT

POST ORCHIDOPEXY IMAGES BOTH TESTIS HAVE NEAR
NORMAL COMPARABLE ECHOPATTERN

Potential pitfalls ….while diagnosing torsion
PARTIAL TORSION : Torsion of at least 540 degrees is necessary for complete arterial occlusion .With partial torsion of 360 degrees, or less, arterial flow may still occur, but venous outflow is often obstructed causing diminished diastolic arterial flow on spectralDoppler examination.
TORSION/DETORSION :If spontaneous detorsion occurs, flow
within the affected testis may be normal, or it may be increased and mimic orchitis. Spontaneous detorsion rarely occurs and leaves a segmental testicular infarction.
ISCHEMIA FROM ORCHITIS :Segmental testicular infarction
may also occur with Henoch-Schönlein purpura or with orchitis . Orchitis may also cause global ischemia of the testis and mimic torsion.

REFERENCE
DIAGNOSTICULTRASOUNDFOURTH EDITIONCarol M. Rumack, MD, FACRJ. William Charboneau, MD, FACRDeborah Levine, MD, FACR