Titrating Insulin to Glycemic Target Judy Bowen, MD CIM Rotation September, 2006.
12
Titrating Insulin to Glycemic Target Judy Bowen, MD CIM Rotation September, 2006
-
Upload
stewart-kelley -
Category
Documents
-
view
212 -
download
0
Transcript of Titrating Insulin to Glycemic Target Judy Bowen, MD CIM Rotation September, 2006.

Titrating Insulin to Glycemic Target
Judy Bowen, MD
CIM Rotation
September, 2006

Case 1
• Mrs. G, 46 y.o. was diagnosed with Type 2 DM diagnosed 5 years ago (initially treated with diet and exercise, then glipizide XL 5 mg BID and metformin 1,000 mg BID) has these Hgb A1c values q 3 months over the past year:
• 5.8%• 6.3%• 7.4%• 7.8%

Case 1, continued
• Her BMI is 33, BP is 126/72, micro-albumin is 9 on lisinopril 10 mg, LDL is 89 on Lipitor 10 mg. She takes 81 mg ASA daily. Her eye exam is up-to-date and normal. Monofilament exam is normal. Your exam is normal except for her obesity.
• Her fasting a.m. CBGs are 140-180• What do you recommend?

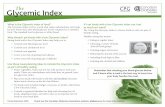
Schematic of 24-hour glucose profile
0
100
200
6 a.m. noon 6 p.m 12 a.m. 6 a.m.
Riddle M. AJM, 2004; 116:3S-9S

Initiating basal insulin therapy
• Add basal insulin therapy– Start with 10 units insulin in most patients– Use either NPH or glargine (both work)– NPH q HS, glargine either q HS or q AM– Glargine was associated with less nocturnal
hypoglycemia (Riddle et al, Diabetes Care, 2003; 26:3080-3086)
• Continue with oral agents
• Consider adverse effects

Treat-To-Target• Goal: near normal fasting CBGs (~100 mg/dl)
• Adjust dose weekly – based on average of two previous fasting CGBs
• Titration:– If CBG >/= 180, increase insulin by 8 units– If CBG 140-180, increase insulin by 6 units– If CBG 120-140, increase insulin by 4 units– If CBG 100-120, increase insulin by 2 units
• No increase if any hypoglycemia (CBG < 72) with or without symptoms

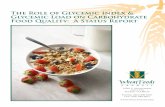
Relationship of A1c to CBG
4%5%
6%7%
8%9%
10%
65100135170205240275

Relationship of A1c to CBG
4%5%
6%7%
8%9%
10%
65100135170205240275

Case 1, continued
• Mrs. G agrees to start bedtime glargine 10 units, and feels confident she can titrate using the “Treat to Target” instructions with RN follow up. Over the next 3 weeks, she achieves fasting CBGs in the 100-120 range with 20 units glargine at bedtime, and no symptoms of hypoglycemia. Her follow up Hgb A1c 3 months after starting insulin is 6.5%

Case 2
• Mr. M, a 65 year-old patient with Type 2 DM for 10 years is on metformin 1,000 mg BID and insulin:– NPH q a.m. 30 units + Regular 10 units
– NPH q p.m. (supper) 25 units + Regular 15 units
• His fasting CBGs are in the 120’s but his Hgb A1c is now 8.0%. He wants better control.
• What do you recommend?

Switching to Basal/Prandial Insulin• To switch to glargine
– Add up his current total insulin dose (80 units)
– Reduce by 20% (64 units)
– Give half as glargine (32 units)
– Titrate using fasting CBGs and ‘treat-to-target’
• To add lispro/aspart– (Onset is 5-15 min, peak is 30-90 min, duration is 3.5 –
5 hours)
– Send to Diabetes Education to learn carb counting
– Give remaining “half” of total dose based on meals:
• 10 + 10 + 12 depending on carb load

Pearls
• Insulin therapy is associated with weight gain• Glargine doesn’t last 24 hours in every patient
(nor is NPH predictable)• We usually wait too long to start insulin in Type 2
patients • Early insulin therapy may be associated with
better daytime prandial secretion from native pancreas
• Finger sticks are more painful than insulin shots