
Tier 2 UPenn Case Log
49
Tier 2 ECC at MJR-VHUP Case Log Abigail Schmidt Matthew J. Ryan Veterinary Hospital at University of Pennsylvania Philadelphia, PA
-
Upload
abbsiegail -
Category
Education
-
view
237 -
download
1
Transcript of Tier 2 UPenn Case Log

Tier 2 ECC at MJR-VHUPCase Log
Abigail Schmidt
Matthew J. Ryan Veterinary Hospital
at University of Pennsylvania
Philadelphia, PA

MJR-VHUP Emergency Service
Incoming/Presenting Complaint BoardTreatment Area: Table 1

MJR-VHUP Emergency Service
Treatment Area: all 3 tables visibleCrash Cart & FAST scanner
**Hospital renovations construction began during my externship; entrance and lobby waiting were first areas to change in appearance, and therefore are not pictured

MJR-VHUP Emergency Service
Treatment Area cages
Oxygen cages
Hemotology Lab Area
Microscopic Analysis & Urinalysis Lab Area
Doctors’/Nurses’ Station

Case 1 “Socks”• Signalment: 10 yo MC Maine Coon Cat, 6.8 kg
• Presenting Complaint: 24 hr history of lethargy, inappetance, and ataxia. Presented to us at 8PM in evening.
O took to RDVM previous night, bloods were run then: Mild hyperalbuminemia (4.0), hyperglycemia (210), hypokalemia (2.8)No other abnormalities found on PE. RDVM sent home.
• Investigations & Results
–Physical Exam; Neurological Exam• BAR, T – 99.5, HR – 215, Grade 3 left systolic murmur heard, RR – 132
MM – pale pink and moist, CRT <2s• Neuro: Menace +, Palpebral +, Facial +, PLR +; all facial nerves intact.
While observing walk, P frequently lost balance and flipped over as FL slid underneath him. P’s gait was abnormal; wiggled back and forth to be ambulatory, but also circled a lot, in inconsistent directions.
–NOVA baseline bloodwork:
• other than a mild dehydration, all previous abnormalities were normal
–BP on each limb • RF – 158 mmHg, RH – 170 mmHg, LF – 170 mmHg, LH – 174 mmHg
–Urine toxin screen: Negative


Case 1 “Socks”
• Treatment– IV Plasmalyte fluids administered at 2.5ml/kg/hr rate – 15 ml/hr overnight
–Overnight, continued to monitor HR, RR, mentation, neurologic reflexes, & BPs in each limb
–By morning, seemed slightly more alert, but still very unsteady when tried to walk. Recommended MRI and possibly a spinal tap, for continued investigations with neurology service to look for potential cause of his symptoms. Differentials included: herniated IVDD, blood thrombus/stroke, infectious/inflammatory disease, and neoplasia.
–O declined offer due to finances.
• Outcome–Advised to monitor at home for progression of
clinical signs. Due to unsteadiness on feet, recommended to restrict Socks to a room without access to stairs for high furniture to prevent him from injuring himself from a fall, etc. If he did wellat home, advised a recheck with neurology service in 1-2 weeks, but sooner if not.
–Medications TGH: • Prednisolone steroid (3 mg/mL) – Tapering dose
instructions: Give 1 mL BID PO for 7 days, then decreased to 1 mL SID for 7 days, then decreased dose to 1 mL EOD for 7 days.
• Clindamycin (25 mg/mL) – Give 2.5 mL BID PO until gone.

Case 2 “Mittens”• Signalment: 2 yo FS Domestic Shorthaired Cat, 3.6 kg
• Presenting Complaint: Straining to urinate, hematuriaMittens was adopted off the streets from being a stray at 9 mos of age. She was spayed, vaccinated, and dewormed at this time. O moved two and a half months ago. Mittens was stressed initially, but quickly became acclimated to new surroundings. Two weeks ago, O got a new kitten. Kitten has been very curious and constantly following Mittens around, including in the litter box. O had 2 littler boxes for them initially, but has taken the 2nd box away now. O first noticed Mittens was going to litter box more frequently ~1 week ago. Mittens has been hiding more and eating/drinking less since kitten was brought into the home. O offered less wet food due to not wanting to waste it with Mittens less interested/eating less at the moment. Yesterday, noticed she was straining on the carpet. However P has had zero accidents. P is not passing much urine. Tonight when P strained, drops of blood seen coming from back end, at which point O brought to MJR-VHUP.
• Investigations & Results–Physical Exam
• QAR, T – 101.6, HR – 250, RR – 42, MM – pink and tacky, CRT <2 s; Slightly tense/painful on abdominal palpation
–Free catch Urine Sediment (passed during Mittens’ PE)• Urine Sediment: Struvite crystals seen (a normal finding in feline urine), but no sign of bacteria
with Diff-Quik stain–Dx: Idiopathic cystitis, stress-related
• Treatment–Buprenorphine (0.3 mg/mL): 0.1 mL q 8 hrs for pain–Diet: Recommended to offer increased amounts of water and wet food

Case 2 “Mittens”• Outcome
– Explained to O in great detail the process of Feline Lower Urinary Tract Disease (FLUTD). Idiopathic cystitis (non-infectious inflammation of the urinary bladder) is the most common cause of FLUTD. Other causes include bladder stones, urinary infection, and cancer. The most common idiopathic cause according to veterinary literature is due to stress in the environment.
– Gave O recommendations of changes that could be made at home to alleviate Mittens’ stress. Explained they were likely associated with the introduction of the new kitten and it’s refusal to give Mittens’ free space.
– Allow more space between food bowls: at the moment, they are set up next to each other. Each cat has its own bowl, but Mittens does not have privacy to eat. This could be a huge help to Mittens, as she isn’t used to sharing.
– Litter boxes: best to have (n+1, n=number of cats in the house) litter boxes available in the apartment. While understandable that where O lives is small, would be best to have at least 2 litter boxes, one for each cat so that Mittens has options.
– “Escape place”: Give Mittens a place to go to and hide where the kitten can’t get to her, for the time being, until she acclimates better to having the kitten around and in her space.
– Give Buprenorphine pain meds for the next few days and ease stress elements to environment, and issue should resolve itself in time, as no bacteria/infectious/traumatic source evident for the cause.
– Mittens was discharged with instructions to follow-up with rDVM

Case 3 “Blanca”• Signalment: 8 yo FS Domestic Shorthaired Cat, 6.8 kg
• Presenting Complaint: Vomiting overnight and unresponsive to voice and touch this morning
Blanca has a history of hepatic lipidosis (clinical symptoms of anorexia and constipation first developed ~1 month ago) and bilateral chronic renal disease with nephrolithiasis. An esophagostomy tube was first placed when she was presented with these signs at that time. She has consistently re-presented for varying related clinical symptoms, weekly to bi-weekly since developing these problems, never fully returning to her normal self according to O.
• Investigations & Results
–Physical Exam• QAR, HR – 244, RR and temperature wnl, MM – pale pink, slightly tacky, CRT <2 sec, BCS 8/9• No murmurs, arrhythmias, or abnormal lung sounds heard on auscultation of heart and
lungs• Abdomen soft and non-painful on palpation• E-tube still in place, opening clean and evidence of good healing apparent
–Flex-4 Chemistry: Creat, BUN, Potassium, Alk Phos• Creatinine mildly elevated (2.4 mg/dl – same as values from previous visits)• Kidney values stable with previous visits, indicating current status of renal disease is no
worse and previously diagnosed partial blockage nephrolith has not progressed to cause a complete blockage. Continued monitoring and imaging via ultrasound is recommended.

Case 3 “Blanca”• Treatment
–Cerenia injection given SQ for treatment of nausea and emesis (likely secondary to kidney disease)–Continue medications from before as previously indicated:
• Ondansetron (4mg tablets): Crust one tablet and mix with water, give through E-tube every 8 hours.• Omeprazole (10mg/ml solution): Give 0.7ml on an empty stomach through the E-tube every 24
hours.• Ursodiol (50mg/ml solution): Give 1.4ml through E-tube every 24 hours.• Buprenorphine (0.3ml/ml solution): Give 0.2ml under the tongue every 12 hours as needed for
pain.–Potential causes of lethargy and weakness may be due to kidney disease, pain, and vagal
stimulation. Recommended giving her the Buprenorphine for pain associated with trying to pass a kidney stone (as O had been given medication before, but not thought P was in pain, so did not give the med), to modulate any potential pain. O informed this might help improve her behavior, activity level, and may even reduce vomiting. O also told that was also possible that she suffered a vagal event due to overdistension, so recommended to continue spacing out her feedings and monitor for further episodes.
–FEEDING: Recommended to continue current feeding regimen (water blended with Hill’s z/d diet, fed 4 times per day), making sure to give small breaks during feeding. In addition, recommended to continue with the increased water intake (20ml warm water four times per day), making sure to give this at least 1 hour before or after feeding.
• Outcome–Recommended Blanca see internist for a recheck in 3 days to assess nephroliths and renal health status
with ultrasound imaging–Blanca represented to MJRVHUP 3 times more following this visit for continued vomiting and straining to
urinate. Her O grew progressively concerned about her quality of life and made the decision to euthanize 10 days after this particular visit took place.

Case 4 “Rudolph”• Signalment: 13 yo MC Miniature Schnauzer dog, 11.9 kg
• Presenting Complaint: Respiratory distress, difficulty breathing (referral)First noticed P to be acting differently 2 days ago; he was lethargic and reluctant to eat. He began to show
difficulty breathing the day prior to presenting. The morning he presented to MJR-VHUP, his respiratory efforts were further increased, he vomited bile, had diarrhea, and had an accident in the house. P was taken to rDVM, and radiographs were taken, which showed abnormal lung fields. He was then referred to MJR-VHUP.
• Investigations & Results–Physical Exam
• DAR, HR – 160, in respiratory distress with RR – 80, lung sounds harsh dorsally and decreased in the right cranial field
• Femoral pulses were moderate in quality; very tense on abdominal palpation. • Right lower eyelid = small mass; large soft SQ masses on chest and in inguinal area
–FAST Thoracic U/S: Pleural fluid seen in the right cranioventral field–Thoracocentesis: hemorrhagic effusion (PCV 15%, TS 5.0 g/dl) drained from RHS thorax (~30 mL)–Thoracic Radiographs: pleural fluid (greater on RHS than LHS), large lung mass in R caudal lung lobe–Prothrombin Time (PT): normal measurement of clotting time
• Treatment–Thoracocentesis & Oxygen Cage Therapy (RR decreased to 68, P became more BAR, able to stand &
walk around)–Cerenia injection given to treat nausea due to retching whilst in hospital

Case 4 “Rudolph”• Outcome
–Large tumor determined to be present in Rudolph’s right caudal lung lobe. The mass was the cause for the leaking, bloody fluid found in his chest. The exact nature of mass was unknown without further diagnostics, however most likely differential was neoplasia.
–Concerns at that point included:
(1) blood loss into his chest, (2) respiratory distress due to the fluid in his chest, (3) spread of the cancer, and (4) loss of his lung tissue to the tumor, with his most acute concern being his respiratory distress, due the fluid in his chest cavity preventing his lungs from expanding and being able to fully inflate properly. Rudolph is unable to support himself outside of oxygen and his blood oxygenation is at dangerously low levels.
–Recommended hospitalization and stabilization treatment (with oxygen therapy and blood transfusions, if necessary), and workup for spread of his tumor. If no other evidence of cancer is found, the treatment of choice would be surgical removal of that lung lobe, which would likely require further advanced imaging (such as a CT scan).
–If pursuing treatment not possible, then recommended humane euthanasia.
–O did not wish to pursue treatment and demanded to take Rudolph home. Expressed concern that Rudolph would continue to bleed at home and be unable to breathe effectively. Advised O to monitor P for signs of worsening respiratory distress (increased RR, agitation, panting, cyanosis) and to have him re-evaluated by a vet for another chest tap and oxygen stabilization or euthanasia if he continued to be in distress, or his present signs worsened.
–He was discharged against medical advice (AMA) with the recommendation to pursue further treatment, or euthanize promptly.

Case 5 “Chloe”• Signalment: 3 yo FS Mixed breed dog, 5.95 kg
• Presenting Complaint: Ibuprofen (Advil Liqui-gels) Ingestion (plausible toxicity)P suspected to have ingested up to 3 capsules (@200 mg/capsule) between 07:00 and 14:30, but may also have chewed 1-2 more. P vomited multiple times at home and en route to MJR-VHUP. P has no other significant health history.
• Investigations & Results
–Physical Exam• BAR, T – 102.3, HR – 132, RR – 36, no murmurs or arrhythmias noted on auscultation of heart and
lungs; MM pink and moist, CRT <2 sec, good hydration status• Abdomen soft and non-painful; no masses palpated• Rectal: soft stool, NAD noted
–NOVA• Assessed Chloe's acid-base status and minimal important electrolytes; all values wnl.
–Complete Blood Count• All RBC, WBC, and platelet counts wnl
–Biochemistry Profile• All electrolytes, proteins, glucose, liver, and kidney values wnl
–Urinalysis• Normal; USG wnl, no blood, proteins, or glucose present in urine, no evidence of kidney damage.
–Flex-4 (BUN, creatinine, sodium, potassium) - serial rechecks • Her kidney values and electrolytes were monitored closely during her stay. Her kidney values
(BUN and creatinine) remained normal. Her sodium and potassium levels were slightly increased 2 days after admission to hospital, but these resolved with a change in fluid therapy (see treatment).

Case 5 “Chloe”• Treatment
–Chloe's toxic dose fell somewhere between gastrointestinal and renal toxicity. She had known gastrointestinal side effects (vomiting with specks of blood) of ibuprofen toxicity.
–Hospitalized for fluid diuresis and continued supportive care, with transfer to Internal Medicine
–IV catheter placed on arrival and placed on high rate IV fluids; food withheld
–Started on anti-nausea medication (Cerenia) and anti-acids Famotidine (25 mcg q 8 hrs) and Pantoprazole(6mg q 24 hrs)
–Started on activated charcoal (q 6 hours) to bind any residual ibuprofen still present in GI tract due to hepato-recycling
–Sucralfate (0.5g q 8 hrs) to coat any ulcerations in stomach
–Chloe vomited once overnight in ER prior to Int Med transfer; some blood specks noted
• Outcome
–Chloe remained hospitalized for 48-72 hrs following admission to allow for treatment of ibuprofen recirculation (24-48 hrs) with fluid diuresis and continued supportive care
–She received multiple doses of activated charcoal and supportive medications for possible gastric ulceration. Her kidney values were closely monitored and showed no evidence of kidney damage.
–Discharged with instructions to continue gastro-protectant medications at home
• Misoprostol (100 mcg): Give ¼ tablet PO TID til gone.
• Omeprazole (10 mg/mL suspension): Give 0.6 mL PO SID til gone.
• Sucralfate (1g): Give ½ tablet dissolved in slurry PO TID til gone. Separate from other medications by 2 hrs.
–Recommended rechecking renal values and USG in 1 week with rDVM
–Chloe’s prognosis for NSAID toxicity, due to being treated appropriately, is very good

Case 6 “Kelly”• Signalment: 9 yo FS Beagle dog, 18.0 kg
• Presenting Complaint: Coughing and a mass in her neck (Hx of mass for ~1 month, no change in size until FNA’d previous day at rDVM; doubled in size overnight, referral)
• Investigations & Results
–Physical Exam
• BAR, occasional dry cough and retch. TPR wnl. Serous discharge OU. Cough present on palpation of neck region. Soft SQ mass (~2 cm diameter) palpable in ventral cranial cervical region, surrounded by significant soft tissue swelling and a larger (~5cm x 3cm) firm, SQ swelling in her caudal neck, in the region of her thoracic inlet. No abnormalities heard on auscultation of heart and lungs. Tense on abdominal palpation, but no masses or organomegaly appreciated. 2 small nodules with an area of ulceration were found on the left side of her vulva. No enlargement of peripheral lymph nodes found.
–Coagulation Panel
• Elevated D-Dimer (0.48 ug/ml; <0.2 ug/ml normal) and decreased platelets (<177 x 10 ^3/ul; clumping); many platelets clumps present on platelet morphology assessment; Slightly hemolyzed sample. PT (@7.3 sec) & PTT (@10.9 sec) within normal reference ranges. No RBC fragments seen.
• Treatment
–Medication TGH: Hycodan (5 mg tablets) – give 1/2 tablet PO SID-QID as needed to control coughing
Case 6 “Kelly”• Outcome
–At this point, nature of neck mass was unknown. Differentials included neoplasia, inflammation, infection, and hemorrhage. Of these, the most likely possibility was neoplastic (cancerous), and further diagnostics (i.e. biopsy, imaging) with oncology specialists were required to determine if it was benign or malignant. Cancerous differentials included thyroid tumors (adenoma or carcinoma), subcutaneous or cutaneous masses (MCT, hemangiosarcoma, lipoma). More advanced imaging such as CT or ultrasound were also considered to be beneficial for complete interpretation. If definitive treatment such as surgery or radiotherapy was pursued for Kelly, this imaging is of critical importance.
–Kelly was not in immediate danger of respiratory difficulty at this visit. Coagulation parameters were pending at time of discharge.
–Discharged with instructions to continue to monitor for evidence of difficulty breathing, worsening cough, worsening gagging/retching, or increased pain or discomfort
–Advised to return on Monday for admission appointment with transfer to comprehensive oncology department
• Follow Up
–Coagulation parameters returned with abnormal results; Kelly was to return for institution of treatment for clotting problems.
–Comprehensive oncology diagnosed Kelly with bilateral thyroid carcinoma, and her Os elected for bilateral thyroidectomy (with parathyroids) excision procedure. She has continued to receive chemotherapy treatment in the form of Carboplatin injections.
–Complications associated with her treatment thus far have been minimal and include hypocalcemia and skin trunk pyoderma.

Case 7 “Saffron”• Signalment: 8 yo FS Goldendoodle dog, 20.0 kg
• Presenting Complaint: Pericardial effusion (referral)Saffron presented to her rDVM yesterday following a collapse while on a walk. Bloodwork, a urinalysis, and radiographs were run at rDVM, which showed elevated renal values, evidence of infection, and unremarkable findings, respectively. P was hospitalized with fluid and antibiotic therapy. Repeat bloodwork and rads were taken today: elevated renal values resolved, but rads showed evidence of suspected pericardial effusion. Referred to MJR-VHUP.
Saffron has hx of luxating patella sx in 2008. She is treated with soloxine for hypothyroidism. She has not been on heartworm prevention for the past couple years (recommendations by holistic vet), but has consistently tested negative for HW.
• Investigations & Results
–Physical Exam
• BAR, T – 101.4, HR – 108, RR – 38, MM – pink and moist, CRT <2 sec
• CVS: Arrhythmia and slightly muffled heart sounds noted on cardiac auscultation; pulses strong & synchronous with occasional pulse deficits. Lungs ausculted normally with normal resp. effort. Jugular veins distended.
• Abdomen soft, non-distended and non-painful. Several movable skin masses noted on chest.

Case 7 “Saffron”• Investigations & Results (Continued)
–ECG: frequent VPCs noted with intermittent accelerated idiopathic ventricular rhythm and ventricular tachycardia
–Focused Thoracic Ultrasound: Mild pleural effusion and mild pericardial effusion noted
–Blood Pressure: Initially elevated (160-230 mmHg), but normalized following transfer to Cardiology service and pericardiocentesis treatment
–Venous Blood gas: unremarkable
–PCV/TS: 35%/6.0 mg/dl
Transferred to Cardiology Service
–Echocardiogram: Revealed a mass associated with her R atrium; small amount of pericardial effusion, and tamponade
–Abdominal Ultrasound: Several small nodules within the spleen. Thrombus visible in one of blood vessels going to spleen. Remainder of organs appeared normal.
–Thoracic Radiographs: No overt evidence of metastasis
–Dx: (1) Pericardial effusion and tamponade - resolved with treatment
(2) Right atrial mass - r/o hemangiosarcoma vs other
(3) Azotemia - resolved, r/o due to tamponade vs pyelonephritis vs other
(4) Historical: Pyuria - r/o UTI

• Treatment–Lidocaine: 2 boluses used to treat intermittent cardiac ventricular arrhythmias; arrhythmias improved.
–Light sedation & Pericardiocentesis: 75 mLs fluid removed from pericardial sac without complication and submitted for cytology. Cytology revealed hemorrhagic effusion with reactive mesothelial cells. No evidence of neoplastic cells seen, however if lesion is poorly exfoliative, effusion cytology may not be sensitive enough to detect neoplastic cells.No microorganisms or atypical cells were identified.
–Hospitalized for supportive care, maintained on iV fluids and antibiotics overnight to treat her suspected UTI; she had occasional VPCs, but her overall rate and rhythm improved and she did well overnight. Brief repeat echo showed no recurrence of pericardial effusion. She transferred to Cardiology service on 14/9/14.
• Outcome–Despite tumor type being unknown, recommended to pursue treatment for suspect hemangiosarcoma. Os
educated on benefits of surgery versus chemotherapy, with goal of sx being to remove pericardium and prevent recurrence of tamponade (most acutely life threatening presenting sign). Biopsy of mass could be performed during sx, but not considered safe due to location and potentially high blood supply. O notified that sx most effective in conjunction with chemo. O informed that even if all tx options pursued, hemangiosarcoma does not carry a good long-term prognosis.
–Saffron’s O did consult with Soft Tissue Sx and elected to have thoracoscopic pericardectomy on 23/9/14. They did not pursue chemotherapy at that time.
–On 26/10/14 Saffron represented for evaluation of labored breathing and 800mL of sanguinous fluid was removed from right pleural space. Following procedure P breathing more easily, but O told that humane euthanasia was reasonable consideration, as unknown how long P had before fluid could re-accumulate. O took her home at that time.
Case 7 “Saffron”

Case 8 “Sasha”• Signalment: 4 yo FS French Mastiff dog, 40.0 kg
• Presenting Complaint: GDV (referral) –First showed signs of bloat and abdominal distension this morning.
Last night she ate well and then ran about in yard outside for 20-30 minutes. She was fine when O went to bed. O took to rDVM upon noticing belly bloat, and they instructed to rush her to MJR-VHUP for treatment of GDV.
• Investigations & Results
–Physical Exam
• QAR, slightly depressed; T – 100.0, HR – tachycardic @172, RR –28, MM – pk & tacky, CRT <2 sec
• Abdomen is distended beyond limits of ribcage; is noticeably uncomfortable from the distension
• Mild seromucoid discharge OU; small lower lid mass OS
• Pulses are moderate in quality
–Abdominal radiographs
• Revealed a large, gas-distended stomach; pylorus on the R, so appeared to be in correct position. SI also distended with gas.
–Extended Database
• Evidence of poor perfusion (lactate 9.1 mg/dl) and dehydration

• Treatment
–Gastric decompression with oro-grastric tubing: Tube passed with moderate difficulty; approximately 20-30 mLbrown fluid removed
–Plasmalyte Fluid Bolus: 2 L fluid bolus given to help alleviate dehydration
• Outcome
–Following gastric decompression with oro-gastric tube, P appeared less distended with gas and was able to drink some water without any vomiting or retching. This suggests she may not have a GDV, but it is by no means a definitive test. As it is unclear if P suffered from gastric dilation, or GDV, discussed with O that GDV requires emergency surgical correction. Based on her xrays, P either has a full 360 degree twist, or just bloat. Due to being unclear, discussed with O option of doing exploratory surgery. O declined due to financial reasons.
–Dx: Gastric Dilation (tentative)
–Recommended to continue to monitor Sasha for worsening distension of abdomen, retching or vomiting, lethargy, pain, or dullness. Instructed to have her re-evaluated immediately if become concerned.
–Discharged with instructions to purchase OTC medications Pepcid AC (famotidine) and Maalox (Aluminum hydroxide, magnesium hydroxide, simethicone), as well as recommendations to have a gastropexy surgery performed, to change feeding regime to have more frequent, smaller meals throughout the day, and to limit activity immediately following eating/drinking
–Sasha represented to MJR-CHUP the following day with continued lethargy and 2 episodes of bright red urine, suspected to contain blood. Further diagnostics confirmed hemoabdomen with thrombocytopenia and tentative splenic torsion diagnosis. O elected for euthanasia due to severe financial constraints.
Case 8 “Sasha”
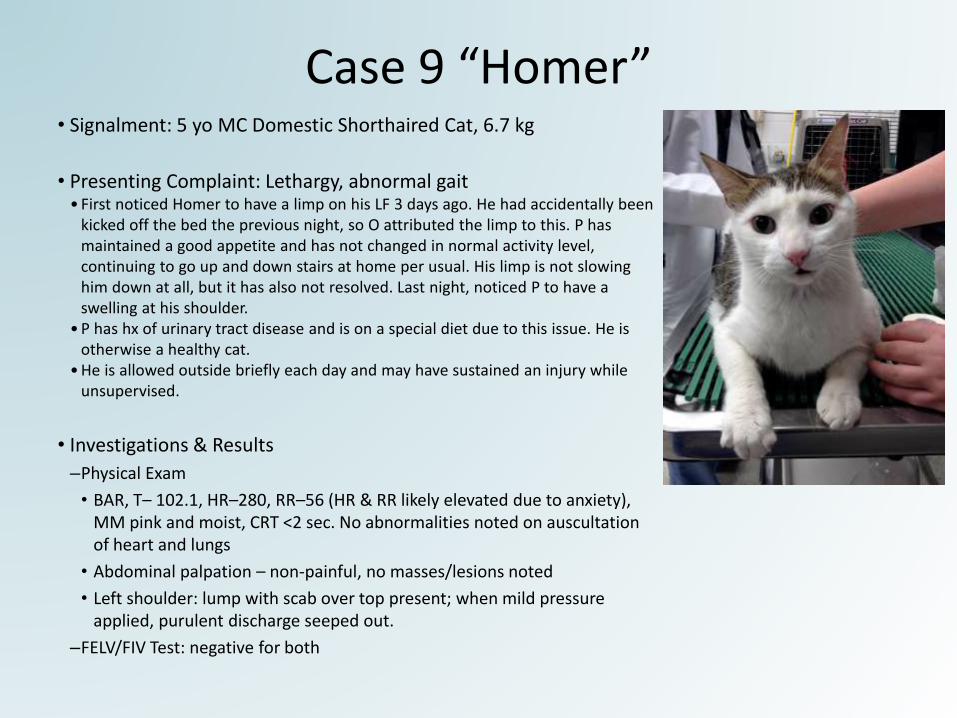
Case 9 “Homer”• Signalment: 5 yo MC Domestic Shorthaired Cat, 6.7 kg
• Presenting Complaint: Lethargy, abnormal gait• First noticed Homer to have a limp on his LF 3 days ago. He had accidentally been
kicked off the bed the previous night, so O attributed the limp to this. P has maintained a good appetite and has not changed in normal activity level, continuing to go up and down stairs at home per usual. His limp is not slowing him down at all, but it has also not resolved. Last night, noticed P to have a swelling at his shoulder.
• P has hx of urinary tract disease and is on a special diet due to this issue. He is otherwise a healthy cat.
• He is allowed outside briefly each day and may have sustained an injury while unsupervised.
• Investigations & Results
–Physical Exam
• BAR, T– 102.1, HR–280, RR–56 (HR & RR likely elevated due to anxiety), MM pink and moist, CRT <2 sec. No abnormalities noted on auscultation of heart and lungs
• Abdominal palpation – non-painful, no masses/lesions noted
• Left shoulder: lump with scab over top present; when mild pressure applied, purulent discharge seeped out.
–FELV/FIV Test: negative for both

Case 9 “Homer”• Treatment–Dx: Abscess (Left shoulder)
–Abscess Cleaning & Repair: P was sedated and area over his abscess was clipped. A scalpel was used to open abscess and the area was thoroughly flushed out with sterile saline. A moderate amount of pus was removed and some firmer, deep tissue was palpated, consistent with fibrosis. There was minimal pocketing, so a drain was not placed. The wound was left open for drainage. Two additional small cuts were seen in the area consistent with a bite wound, but these were not full-thickness cuts and appeared to be healing well.
–Rabies Vaccine: administered SQ in RH limb
• Outcome–Discharged with instructions to monitor wound for worsening signs of swelling, heat,
pus, blood, pain, or further opening of the wound. If any of these seen, recommended to seek re-evaluation by a veterinarian.
–Sent home with:
• E-collar: to be kept on at ALL TIMES during recovery to prevent P form licking at or opening wound.
• Medications:
–Buprenorphine (0.3 mg/mL) – 0.2 mL to be given transmucosally (under tongue/side of cheek) q 8-12 hrs as needed for pain
–Clavamox (62.5 mg/mL) – 1.5 mL to be given PO q 12 hrs for 14 days (antibiotic)
–Recommended to have Homer rechecked in 10-14 days to confirm wound has healed well and no new purulent material has developed

Case 10 “Panther”• Signalment: 15 yo MC Domestic Shorthaired Cat, 5.75 kg
• Presenting Complaint: Decreased appetite and vomiting Panther is a diabetic cat. He first developed a change in appetite in June (~3 months ago) when he was boarded at his rDVM clinic while his Os were on vacation. He continued to have a sporadic appetite after his Os return. Over the past 2 days, his appetite decreased significantly. He did not receive his normal insulin dose yesterday morning due to inappetance. He vomited after his evening meal. He last received insulin (2U Lantus) at 8PM last night. This morning his Os found 3 more green-tinged vomit piles, at which point they brought him to MJR-VHUP.
Panther has been diabetic for 5 years now, and was managed on oral medications until 2 years ago when he began to receive insulin injections. His normal routine involves receiving 2U Lantus injectable insulin BID. He has had one other diabetes-related hospitalization for a hypoglycemic complication 2 years ago.
• Investigations & Results–Physical Exam
• QAR, resistant to examination. TPR – wnl, MM pink and slightly tacky, CRT <2 sec
• Moderate skin turgor suggesting moderate dehydration; coat unkempt
• Heart and lungs auscult normally, however he was very vocal during examination
• OD abnormal & discolored with signs of corneal ulcer
• Abdomen tense and slightly painful on palpation
• Investigations & Results (Continued)
–NOVA x2
• Day 1: Gluc 231 mg/dL (65-112 mg/dL), Lactate 3.1 mmol/L (0.5-2 mmol/L), PCV 35%, TP 9.6 g/dL
• Day 2: Gluc 246 mg/dL, Lactate 1.0 mmol/L, PCV 25%, TP 7.1 g/dL
–Ketones: negative
–Complete Blood Count: Mild toxic change to white blood cells
–Blood Chemistry
• Glucose 216 mg/dL, Ca+ 13.0 mg/dl (9.1-11.2), K+ 5.6 mmol/L (3.5-4.8), ALT 211 U/L (33-152), AST 52 U/L (1-37), Alk. Phos. 92 U/L (22-87)
–Snap PLI: Abnormal
–Urinalysis: 4+ Glucose, Ketone negative, USG: 1.024
• Treatment
– IVF to correct hydration and electrolytes (Hartmann’s)
–Buprenorphine (0.01 mg/kg) given IV for pain
–Timentin (50 mg/kg) and Metronidazole (7.5 mg/kg) given IV
–Cerenia (1 mg/kg) and Pantoprazole (1 mg/kg) given to treat nausea and decrease acidity of the stomach
–Erythromycin topical ointment to treat OD
– Insulin Therapy: 0.1U/kg of Regular insulin given if Panther’s BG >250 mg/dL
Case 10 “Panther”

• Outcome–Panther remained stable overnight. His blood glucose was monitored every 4 hours. It remained around 150-250 mg/dL,
and he was given a dose of insulin twice during his ES stay. He had a good appetite and ate canned Hill's I/D. He did not vomiting at all during his stay.
–Based on his bloodwork having elevated liver enzymes in conjunction with his history of decreased appetite and vomiting, it was recommended that Panther remain hospitalized for further diagnostics (abdominal ultrasound with or without biopsies of the abnormal organs) and treatments to make sure his condition did not deteriorate. Possible differentials included: inflammatory – pancreatitis, hepatitis, cholangitis; infectious – bacteria or virus; or neoplastic – lymphoma. Due to his being negative for ketones, the vomiting and decreased appetite were not felt to be attributed to his diabetes.
–His 2nd day bloodwork showed he was no longer dehydrated, however he as hemodilute and slightly anemic. While not symptomatic for his anemia, it was recommended to have continued monitoring.
–Os declined further investigations due to finances, Panther’s fractious demeanor in the hospital, and his age.
–Panther was discharged with instructions to monitor for vomiting, diarrhea, lethargy, inappetance, weakness, collapse, polyphagia, PU/PD, and weight loss. They were also instructed to monitor his eye for any increase in squinting, redness, or discharge.
Medications TGH: Clavamox(62.5 mg/mL) – Give 1.25 mLs PO q 12 hrs x 10 days; Metronidazole (50 mg tab) – Give 1 tablet PO q 12 hrs; Buprenorphine (0.3 mg/mL) – Give 0.2 mLs TM q 12 hr for pain; Omeprazole (10 mg/mL) – Give 0.5 mLs PO q24 hrs; Erythromycin Ophthalmic Ointment (0.5%) – Apply ¼ inch strip in OD q 8 hr.
Continue to give Panther his insulin as previously prescribed. Noted that his dose may need adjusting depending on his appetite. Recommended to give Panther 1U instead of 2U when he does not eat, and to consult a vet when making changes to his insulin regimen. Advised to see a vet for re-evaluation in 24-48 hrs.
–24/11/14: P represented to MJR-VHUP for 2 day history of decreased appetite and abnormal gait. He had an abnormal mental status, was dull and weak. His PE had several neuro abnormalities and he was hypoglycemic on bloodwork, with anemia and elevated renal parameters. An abdominal FAST scan revealed a very large, vascular mass associated with his pancreas. O not interested in pursuing diagnostics/treatment to determine if mass benign vs malignant, etc; do not feel is in Panther’s best interest. O opted for humane euthanasia.
Case 10 “Panther”
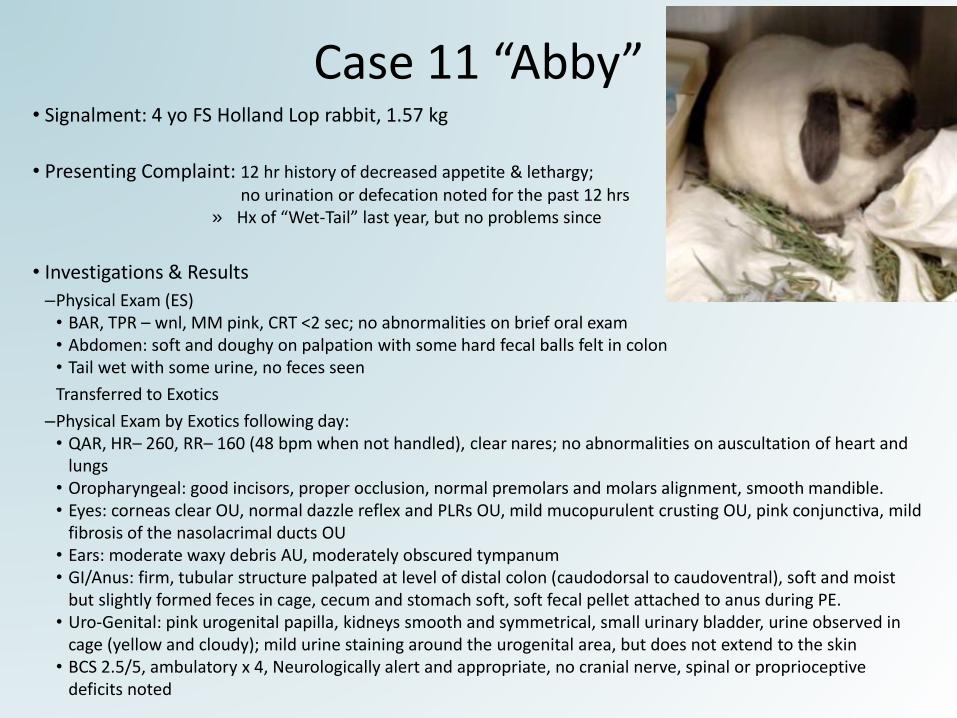
Case 11 “Abby”• Signalment: 4 yo FS Holland Lop rabbit, 1.57 kg
• Presenting Complaint: 12 hr history of decreased appetite & lethargy; no urination or defecation noted for the past 12 hrs
» Hx of “Wet-Tail” last year, but no problems since
• Investigations & Results
–Physical Exam (ES)• BAR, TPR – wnl, MM pink, CRT <2 sec; no abnormalities on brief oral exam• Abdomen: soft and doughy on palpation with some hard fecal balls felt in colon• Tail wet with some urine, no feces seen
Transferred to Exotics
–Physical Exam by Exotics following day:• QAR, HR– 260, RR– 160 (48 bpm when not handled), clear nares; no abnormalities on auscultation of heart and
lungs• Oropharyngeal: good incisors, proper occlusion, normal premolars and molars alignment, smooth mandible. • Eyes: corneas clear OU, normal dazzle reflex and PLRs OU, mild mucopurulent crusting OU, pink conjunctiva, mild
fibrosis of the nasolacrimal ducts OU • Ears: moderate waxy debris AU, moderately obscured tympanum • GI/Anus: firm, tubular structure palpated at level of distal colon (caudodorsal to caudoventral), soft and moist
but slightly formed feces in cage, cecum and stomach soft, soft fecal pellet attached to anus during PE. • Uro-Genital: pink urogenital papilla, kidneys smooth and symmetrical, small urinary bladder, urine observed in
cage (yellow and cloudy); mild urine staining around the urogenital area, but does not extend to the skin• BCS 2.5/5, ambulatory x 4, Neurologically alert and appropriate, no cranial nerve, spinal or proprioceptive
deficits noted

• Investigations & Results (Continued)–Bloodwork - CBC/PCV/TS/Chemistry
• Mild non-regenerative anemia. No peripheral lymphocytosis (which can be seen with lymphoma).
–Urinalysis
• Free catch collection, Cloudy yellow in color, USG: 1.008, pH: 8.0, Blood: 4+; repeated q 6hr and USG, blood presence, and pH values changed throughout
• Transient hematuria (r/o cystitis, pyelonephritis, vaginitis, or hematochezia/melena). Isosthenuria (r/o iatrogenic diuresisvs renal disease vs UTI vs other). pH 6.5 urine r/o metabolic acidosis.
–Abdominal Ultrasound
• Descending colon (small colon) mass with mass partially obstructing the fecal output - r/o neoplasia, i.e. lymphoma, carcinoma. Inflammatory condition/mural fibrosis, granulomatous thickening other non-neoplastic causes cannot be ruled out. Mildly inflamed mesentery is present around it. Scant peritoneal effusion - may be normal amount for species although is subjectively slightly more than usual.
• Colonic cancer most likely differential, but cannot r/o infectious/inflammatory process that is partially obstructing fecal output in the colon; unable to obtain FNA at this time as mass too thin for attempt to get sample. Biopsy preferable for determining nature of mass.
• Treatment–Dx: GI stasis, secondary to colonic mass (suspect underlying infectious/inflammatory/neoplastic cause)
–SQ Fluids: 40 mL/kg given q 8 hrs
–Buprenorphine: 0.03mg/kg SQ q8, decreased to 0.01 mg/kg q8 following transfer from ES to Exotics
–Diet: Critical Care feedings of 20 mL/kg q 6 hr
–Metronidazole: 15 mg/kg PO q 12 hr
–Metacam: 0.5 mg/kg PO q 12 hr
• Outcome: discharged after 48 hrs of hospitalization and support care. Sent home on medications: Metronidazole (50 mg/mL) – give 0.49 mLs PO q 12 hrs for 2 weeks; Metacam (1.5 mg/mL) – Give 0.54 mLs PO q 12 hr for 2 weeks. Advised to return 7 days to monitor her progress and recheck bloodwork for renal values. If worsening signs of GI stasis noted at home, seek veterinary care sooner.
Case 11 “Abby”

Case 12 “Dior”• Signalment: 7 yo MC Bichon Frise, 8.2 kg
• Presenting Complaint: Acutely down in hind limbs
• Investigations & Results
–Physical Exam
• BAR, T – 100.9, HR – 118, RR – 40, MM – pink and moist, CRT <2 sec
• Musculoskeletal
–Gait assessment: FLs placed normally; HLs dragged behind, unable to pick up feet, or move/place them to stand properly/have normal ambulatory motion
• Neuro:
–CPs: FLs +ve; HLs –ve
–Cutaneous skin sensation test: suggestive of a T3-L3 myelopathy
–HLs: Absent motor, questionable deep pain sensation
• Outcome–Recommended further diagnostics and discussed possible medical vs
surgical options to treat; O expressed concern over being able to provide adequate nursing care at home for a paralyzed dog. Given this, his guarded prognosis, and financial constraints, O elected for humane euthanasia.

Case 13 “Lola”• Signalment: 8 yo FS English Bulldog, 14.3 kg ( from 17.0 kg in July)
• Presenting Complaint: Sudden blindness (recurrence due to optic neuritis), decreased appetite, & lethargyLola is managed with Azathioprine for optic neuritis. She was diagnosed with pituitary dependent Hyperadrenocorticismin July, and is managed with Trilostane. Due to her waxing and waning appetite, she did not receive this medication consistently over the past few days. She was evaluated on 28/8 (DOP to ES 14/9). She has also been treated in the
past for calcinosis cutis and pyoderma with marbofloxacin.
• Investigations & Results– Physical Exam• At presentation P was depressed, but responsive. P appeared stressed and pulse ox
registered her to be at 90% saturation; she was placed in O2 cage.• After calming dow rest of PR performed: TPR – wnl, BCS 3/9• 3rd eyelids elevated, enophthalmus noted bilaterally. Menace and PLR were negative
OU, suggesting absence of vision.• Auscultation of heart & lungs: Increased bronchovesicular sounds bilaterally, with
referred upper airway sounds. No murmurs or arrhythmias.• Abdomen: pot-belly appearance, soft on palpation with no obvious pain/discomfort • Integument: generalized alopecia with calcinosis cutis lesions noted along dorsum;
raw, irritated superficial skin lesions along her sternum and lateral aspect of L elbow.
–NOVA: baseline E-lytes, acid/base status, and renal values found to be unremarkable
– Chest Radiographs: showed an increased interstitial pattern associated with the L Cr lung lobe and an alveolar pattern noted along the R middle lung lobe. Top Ddx include pneumonia (aspiration v. infectious), fibrosis, and chronic lower airway disease.

Case 13 “Lola”
• Treatment–Admitted and started on IVF therapy
• Cefotaxime and Clindamycin given for broad spectrum empirical antibiotic coverage to treat her suspect pneumonia (based on rads) and gastroprotectants.
–Oxygen cage therapy: remained oxygen dependent, so kept in O2 cage overnight
–Continued to have increased respiratory effort (with normal rate); mentally dull, but with no further neurological abnormalities
–During brief assessment in the morning, she decompensated rapidly and developed profound hypoxia. This further complicated with decreased chest excursions and was thought to be in respiratory fatigue/arrest due to being completely obtunded by this stage. She was immediately intubated and oral cavity suctioned due to excessive secretions. BP and HR were markedly low. CPR was provided in the form of administering atropine (IV) to improve HR, and multiple rapid infusions of crystalloid fluids (IV) to improve BP.
–Lola’s perfusion parameters remained progressively worse despite aggressive tx, which carried with it a poor prognosis. Septic shock was a high ddx due to her clinical picture and lack of response to tx. Cardiogenic, metabolic, upper airway disease, and other ddxs were not ruled out, and could have been contributing factors to her decline.
• Outcome–Os requested we keep her alive until they could get to the hospital to say goodbye. They then elected for
humane euthanasia.
Case 14 “Beulah”• Signalment: 8 yo FS Mixed breed dog, 16.7 kg
• Presenting Complaint: Chewed up inhalers/Albuterol ingestion toxicityO first discovered P got into inhalers upon getting home after being away for ~3 hrs; O discovered chewed inhaler canisters. For first 45 min after O got home, P seemed okay. O then noticed she was shaking, heart was racing, and she seemed overheated (panting a lot). O called ASCPA Poison Control (case #140116809), and then brought her to MJR-VHUP.
P has a hx of getting into things she shouldn’t, but never required hospitalization before. P also has hx of seizures, which are treated BID with a grain and a ¼ of Phenobarbital. Most recent seizure occurred yesterday, and she typically has a seizing episode once q 3 weeks.
• Investigations & Results–Physical Exam• BAR, HR – tachycardic @195, T&R – wnl, MM pink and moist,
CRT <2 sec; well-hydrated• No obvious signs of oral trauma/lesions/ulceration • Abdominal palpation: very tense, but non-painful
–NOVA• K+ low @3.02 mmol/L, Lactate elevated @5.5 mmol/L. • E-lytes continued to be monitored overnight, and normalized.
–Continuous ECG• Maintained on continuous ECG to monitor HR and rhythm. Despite being tachycardic, P had a normal rhythm
overnight. Around midnight P’s HR normalized and continued to be within normal range without medication administration.
–Blood Pressure: At presentation - 110 mmHg; monitored overnight and remained normal.

• Treatment
–Maintained on IVF overnight with continued ECG, BP, and baseline bloodwork monitoring
–Propanalol (beta-blocker) 0.2mg/kg administered IV in hopes of lowering her HR. She was given 3 initial boluses, and her HR was maintained in the normal range.
–Beulah ate and drank readily, with no other clinical symptoms developing. Her anti-seizure medications were continued as given at home.
• Outcome
–Discharged day following initial presentation with instructions to continue to monitor P at home for any signs of tremors, hyperactivity, vomiting, inappetance, hypersalivation, oral pain, or increased respiratory rate/effort. If any of these signs noted, seek veterinary care.
–Continue anti-seizure medications as previously prescribed at home.
–Advised that as long as Beulah does well at home, and none of aforementioned signs were noted, then there was no need for a recheck appointment for this toxicity.
Case 14 “Beulah”

Case 15 “Austin”
• Signalment: 14 yo M White Standard Poodle dog, 19.7 kg
• Presenting Complaint: Acute labored breathing and discomfortOs first noticed Austin not himself morning of presentation when he was acting anxious and uncomfortable. His breathing became very labored, and Os also noticed he was painful in his abdomen. At this point, he was brought to MJR-VHUP.
Austin has a history of GDV, which was resolved with gastropexy procedure 2 years ago. Current medications he is on include Famotidine and Simethicam due to this history. He also has a Grade II heart murmur, but has never needed medical treatment for his heart condition. He occasionally experiences episodes of coughing or diarrhea due to his sensitive stomach, but his appetite has continued to be healthy.
• Investigations & Results–Physical Exam• QAR, T – normal, HR – tachycardic @180, Grade II/VI systolic murmur with weak, but synchronous pulses,
RR – tachypneic @84, labored with slightly increased lung sounds, but no crackles or wheezes detected• MM moist, but appeared injected; Eyes – evidence of nuclear sclerosis, OS Ca+ deposits noted on cornea• Abdomen: tense and moderately painful on palpation • Genital: Both testes present in scrotum, L testicle more firm than R
–NOVA: no E-lyte abnormalities, but lactate elevated level, consistent with poor perfusion. –CBC: unremarkable; Biochemistry: mildly ed globulins; slightly ed liver enzyme (AST); Coagulation: NSF–Continuous ECG: Severely tachycardic at 200 bpm initially. Multifocal VPCs and supraventricular
tachyarrhythmias noted on ECG evaluation prior to medical intervention.

• Investigations & Results (Continued)
–Abdominal U/S: A large R-sided liver mass noted, as well as a R craniodorsal abdominal mass of unknown origin. Several splenic nodules seen with scant amount of free abdominal effusion. Stomach was mildly dilated. Small cystic calculi and nodules seen within both testicles.
–Thoracic Radiographs: No evidence of metastatic disease in lungs. NSF noted in cardiovascular structures.
–Echocardiogram: Cardiac contractility and function appeared normal. Ventricles were smaller than normal, suggestive of hypovolemia.
–Blood Pressure: On presentation, was severely elevated at 220 mmHg. BP was monitored overnight and maintained within a normal range at 100 mmHg following fluid therapy.
• Treatment–Admitted for hospitalization overnight. While in ES, he received multiple boluses of crystalloid IV fluids. He
was maintained on IV fluids and pain medication overnight. Given his persistently elevated HR, also received Diltiazem, to which he responded well.
–He was transferred to Soft Tissue Surgery Service the following day on 9/16/14 for exploratory laporotomy. –GA & Ex Lap: Performed to determine extent of his abdominal disease and address the correctable problems.
Given the severity of his abdominal lesions (including two large splenic masses, a R liver lobe mass, and retroperitoneal mass surrounding the R kidney, R adrenal gland and both the vena cava and aorta. Os were contacted intra-operatively to discuss viable tx options and prognosis for Austin. In light of these findings, they elected to have Austin humanely euthanized on the operating table. A necropsy was not performed
Case 15 “Austin”

Case 16 “King Kong”• Signalment: 2 yo M Alapaha Blue-Blood Bulldog, 40.0 kg
• Presenting Complaint: Lameness of R Hind limb King Kong has been less active for the past month, and has been more reluctant to jump or run. Over the past week, his condition worsened, and he has an obvious RH lameness. His LH leg is much thicker and heavier muscled cf. RH leg. No change in appetite, and no vomiting or diarrhea have been noted.
• Investigations & Results–Physical Exam• BAR, calm, slightly overweight BCS 6/9. TPR – wnl; no murmurs, arrhythmias, or abnormal lung sounds heard on
auscultation of chest; MM pink and moist, CRT <2 sec• Musculoskeletal: obvious RH lameness; would hold up RH when initially stood up from rest• Orthopedic exam: R stifle instability (cranial tibial thrust and cranial drawer)
–Tentative diagnosis: ruptured cranial cruciate ligament of RH stifle
• Outcome: –Discussed medical versus surgical options for treating CCL rupture; O was adamant to go ahead with surgery–Discharged with instructions to restrict King Kong’s activity (strict rest: no running, jumping, or rough playing;
confine exercise to short leash walks to use the restroom) until his Orthopedic Surgery appointment, to arrange surgical correction. Offered NSAIDs to manage pain until surgery, however O declined the required pre-NSAID bloodwork and NSAIDs at this time.
–Advised to phone appt desk to arrange Orthopedic appt for radiographs and CCL rupture Sx, and to not give food to P after 10PM the night before his appt.
–Medication TGH: Tramadol (50 mg tablets) – Give 3 tabs PO q 8-12 hrs as needed for pain control
–Returned following day for appt with Ortho; Rads confirmed joint effusion and osteoarthritis consistent with CCL disease. Right stifle arthrotomy, TPLO, & partial meniscectomy procedures performed 17/9/14 (2 days following initial presentation) by Orthopedic Surgery Service.

Case 17 “Jake”• Signalment: 1 yo M Norwegian Dwarf rabbit, 1.35 kg
• Presenting Complaint: Ingestion of rodenticide poison (Brodifacoum toxicity)P first caused alarm when O heard him chewing on something abnormal; upon further investigation, discovered he had been chewing on a red rodenticide stick
• Investigations & Results–Physical Exam• BAR, T – 102.1, axillary T – 98.7, HR – 280, RR – 200 (all wnl); no murmurs or arrhythmias
heard on auscultation of heart; sniffing, no difficulty breathing, lungs clear on auscultation
• MM pink and moist, CRT <2 sec; both testicles present in scrotum, soft and non-painful• Abdomen soft and non-painful on palpation
• Treatment–Calculated that Jake had ingested a fair amount of rat poison; said poison
works by inhibiting Vitamin K production, necessary for blood clotting.–Vitamin K supplementation: SQ injection of Vitamin K1 (3 mg/kg) was
administered.
• Outcome–Discharged with instructions to monitor Jake closely for any signs of
bleeding which might include: bruising of the abdomen, red patches on his ears or in the sclera of his eyes. Monitor his gums for any red patches, or becoming white or pale.
–Also monitor Jake for lethargy, decreased appetite, decreased fecal production, difficulty breathing, or an increased respiratory effort.
– If any of these signs seen, please seek veterinary care ASAP

Case 17 “Jake”
• Outcome (Continued)
–Medications TGH: Continue to supplement Vitamin K for several weeks to prevent bleeding.
• Vitamin K1 25mg tablets: Give 1/4 tablet by mouth q 24 hours. Very important that Jake get this medication daily; 7 tablets dispensed, to treat for the following 28 days.
• Advised that Jake not have access to rat poison in the future, and to schedule a recheck appointment with the Exotics Service in 4 weeks time, once Jake had completed his Vitamin K medication.

Case 18 “Izzy”• Signalment: 6 mo FS Domestic Shorthaired cat, 3.6 kg
• Presenting Complaint: Vomiting and ingestion of ribbonFirst had an episode of vomiting last night following evening meal. P vomited again morning of presentation, and then continued to make retching noises. O then noticed that she had a piece of black ribbon hanging out of her mouth. O proceeded to tug on ribbon lightly, at which point it snapped. O then brought P to MJR-VHUP with ribbon in hand, worried that she might have more ribbon trapped within GIT. Time at which P ingested ribbon is unknown, as she has continued to have a normal appetite, but has not had any bowel movements. She has been less rambunctious at night when Os sleeping, but O had attributed that to her outgrowing kitten-hood. P was not noted to be lethargic prior to morning of presentation.
O first acquired P 2 months ago from local shelter; no medical issues since being adopted.
• Investigations & Results–Physical Exam• BAR, T – 101.8, HR – 204, RR – 44, MM pale pink and tacky, CRT <2 sec, moderate skin turgor • Chest and lungs auscult normally, no murmurs or arrhythmias, clear lung sounds; strong, synchronous pulses
• Abdomen: not tense on palpation, intestinal loops feel watery without distension
–NOVA: unremarkable; all values wnl–Abdominal U/S: No obvious foreign body or obstructive pattern revealed. No
long pieces of string were seen. Stomach had material present that could be food or small pieces of ribbon.

• Treatment– IV Fluids: started to treat dehydration whilst waiting for further diagnostics (U/S imaging) to have availability
–With the insignificant findings by U/S imaging of the abdomen, discussed hospitalization with IV Fluids versus IV medication vsoutpatient therapy. O felt comfortable taking her home and monitoring, and and agreed to bring P back if her signs continue.
– P received SQ fluids and injection of Cerenia for nausea prior to discharge
– Discharged with recommendations to carefully monitor for continued signs (vomiting, cessation of eating, lethargy, depression) at home – if any of these signs seen, advised to call or come in to be seen.
–Otherwise, instructed to only feed small amounts of food at a time for the next 24-48 hrs, gradually increasing the amount being fed over time. Recommended to keep P separated from other cat until certain she has recovered from this episode.
Case 18 “Izzy”

Case 19 “Jeter”• Signalment: 12 yo MC Yorkshire Terrier dog, 3.71 kg
• Presenting Complaint: Respiratory distress & tracheal collapse (referral)O first noticed Jeter was struggling to breathe and coughing more 2 nights ago. O treated with Benadryl at home, hoping to help him breathe better, but Benadryl had minimal effect. O took him to ER last night. He was placed in O2 and given Prednisone to help alleviate his symptoms. O then took him home AMA, before returning to rDVMwith P where he was again placed in O2 and chest rads were taken.
Jeter has a hx of tracheal collapse since Oct 2010, when chest images first taken. He has sporadic coughing episodes periodically, and they are more severe when he gets stressed or excited. Jeter has seasonal allergies.
• Investigations & Results–Physical Exam• BAR, very dyspneic. Quickly placed in O2 cage. Temp & HR wnl. No murmurs or arrhythmias heard on auscultation of heart.
Lung sounds harsh with referred upper airway noise. • Eyes: Bilateral nuclear sclerosis; remainder of PE unremarkable.
• Treatment– Jeter was comfortable in Oxygen cage, but would quickly deteriorate when taken outside of oxygen.
• Outcome–Recommended thoracic rads for further evaluation of the tracheal collapse and the lung parenchyma as initial diagnostics. –Recommended placing a trachel stent for treatment of tracheal collapse. Procedure would require P to be hospitalized in ES
overnight, then transferred to Intervential Radiology Department/Surgery Department in the morning. –Procedure would require P to have CBC/Chem, Chest Xrays, and Fluoroscopy performed on day of presentation. Then the
tracheoscopy, tracheal wash, and stent placement would be performed next day. – If tracheal stenting was not performed, medical management was offered. –Due to his severity of disease and concern for his quality of life, Os elected for humane euthanasia.

Case 20 “Louise”• Signalment: 6 mo FS Domestic Shorthaired cat, 3.32 kg
• Presenting Complaint: Permethrin toxicityO took Louise and pet dog to rDVM for regular check-ups and flea medication. rDVM gave O a topical flea medication (Advantix II) and told O could be used on both Louise and pet dog. O applied medication when got home from rDVM as instructed to both pets that evening (0.4mL K9 Advantix II to Louise). Shortly after O realized the topical flea medication had warning labels stating it was toxic to cats. O immediately gave Louise a bath with oatmeal shampoo 30 minutes after initial application. O monitored P for abnormal signs, stated that P was trembling and trying to lick at spot where applied med. P has seemed lethargic/depressed, but has still been interested in treats. No vomiting or diarrhea. O adopted Louise in mid-May at ~2 months of age. No prior health issues before this event.
• Investigations & Results–Physical Exam• BAR, HR – wnl, Temp & RR – elevated; heart and lungs auscult normally• PLR – slightly delayed, menace & palpebral reflexes +ve , but body was tremoring throughout exam • Abdomen: soft and non-painful
–NOVA• mild increase in BUN, likely secondary to mild dehydration
• Treatment– IV catheter placed; P given Robaxin (methocarbamol, a muscle relaxant) IV
to decrease muscle tremors. –Louise was kept overnight for continued supportive treatment and
monitoring. She had no significant tremoring overnight.

• Outcome
–Due to no further complications overnight, Louise was discharged the following morning
–Os instructed to monitor for further episodes of tremoring and lethargy at home. Advised that P may continue to be more quiet than usual for the next couple of days, but that this should resolve.
–Recommended to be cautious that in the future, and only apply products that are intended for use on cats from high quality manufacturers. Advised O to contact vet if have any questions – but common SAFE products for use in cats include: Advantage, Revolution, or Frontline for cats.
Case 20 “Louise”
Case 21 “Jake”• Signalment: 4 yo MC Bluetick Coonhound, 35.7 kg
• Presenting Complaint: Marijuana (THC) Ingestion ToxicityOs were out for ~5 hours this afternoon and when returned, found Jake on their bed laying in his own urine. He was awake, but unable to move around very much. The marijuana belonged to Os sister, and she estimated that Jake ingested 2 grams of marijuana. P has not had any vomiting or diarrhea since ingesting the substance. Jake had an episode of pancreatitis in January 2013. Otherwise, Jake has been a healthy dog.
• Investigations & Results–Physical Exam• Dull and minimally responsive, T – 101.3, HR – bradycardic @60, RR – 20, well-hydrated• Heart & lungs auscultated within normal limits; Eyes – glassy • Urogenital: incontinent, leaking urine; Recumbent and minimally responsive to agitation
–NOVA: Mild increase in K+, likely secondary to release from muscle contractions; otherwise unremarkable
• Treatment–Given the large dose Jake potentially ingested and how dull he
was as well, as the risk for aspiration pneumonia should he vomit, recommended monitoring P in the hospital overnight.
–Put on IV fluids to help flush out the toxins. –Periods of overstimulation and hyperexcitability were quickly
resolved with a low dose of Butorphanol.–Overnight, P remained dull and relatively poorly responsive;
recommended further monitoring and supportive care, and P continued to improve while in ES.
–P’s temperature was monitored closely. Overnight T dropped, and he required active warming. He improved gradually through the course of the day.

• Outcome
–Despite still being slightly dysphoric from the marijuana ingestion toxicity, Jake was discharged to his Os.
–Os were told he should still continue to improve over the next 24-48 hrs.
–Recommended to continue to monitor Jake closely at home for any signs of his status worsening, i.e. if he appears dull, disoriented, is vomiting, not eating, or otherwise ill. Should he show any of these signs, advised to seek veterinary care immediately.
–Provided that Jake continued to do well at home, instructed that there was no need for him to be re-evaluated.
Case 21 “Jake”

Case 22 “Samantha”• Signalment: 6 yo FS Mixed breed dog
• Presenting Complaint: Irritation & exposure of TPLO incision site of LH limbP chewed bandage off (repeat offender) to expose TPLO plate; MDR infection+
Samantha's initial TPLO sx on L HL took place ~3 weeks ago. The wound dehisced within the first week and surgery had to be performed again to clean out the wound. P came in yesterday (Friday) to Orthopedic Surgery service to revisit closure of her TPLO site following infection and complication from initial surgery and agitation of the site. There was not enough skin to effectively close the incision in surgery as hoped. It was elected to leave the site open, and to rebandage the L HL. P would have a recheck appointment Monday (in 2 days). O was out for 2 hours today and P managed to get to her bandage and again irritate the leg and the skin just above surgical site. Samantha is otherwise healthy and has been eating normally.
• Investigations & Results–Physical Exam• BAR, TPR – wnl, P is very excitable• L HL has areas of redness and irritation above her knee and at
uppermost region of TPLO bandage and surgical site.–Blood Pressure: normal @ 125 mmHg
• Treatment–Wound lavage and bandage change

Case 24 “Samantha”• Treatment (continued)–P was sedated with Dexdormitor (5mcg/kg IV) and Butorphanol
(0.2mg/kg IV). Her bandage was removed and her wound site evaluated. The surrounding skin looked mildly irritated, but the actual wound itself did not seem disturbed or overly inflamed.
–Granulation tissue still present; wound was flushed thoroughly with sterile saline, and a soft tissue bandage was reapplied. Samantha was given Antisedan to reverse sedation, and her recovery was uneventful.
• Outcome–Discharged following recovery from sedation with STRICT instructions to
keep E-collar on at ALL times to prevent her from licking at the incision site until time of suture removal.
–Advised to continue to monitor Samantha for signs of lethargy, inappetance, vomiting, diarrhea, pain, or recurrent L HL swelling. Recommend to have re-evaluated ASAP if these changes notes.
–Also advised to monitor bandage for dislodgement or strike through seepage, and if seen, to have her re-evaluated.
–Restrict activity as previously instructed for next 8-12 weeks. Absolutely no running, jumping, or playing, and confine her to a large crate when she is left unattended. Walk slowly on leash to urinate and defecate for 5-10 minsdaily.
–Meds TGH: Continue on Chloramphenicol and Tramadol as previously prescribed. O advised may restart Ps Rimadyl as previously prescribed for any associated inflammation/discomfort.

THANK YOU!
In short, I had a wonderful learning experience while externing at UPenn with their Emergency Service department. Thank you so much for this wonderful opportunity! I hope you enjoyed my presentation


















