Thyroid dysfunction in children with autism spectrum ...iliadneuro.com/pdf/Frye_Thyroid.pdf ·...
13
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/313778826 Thyroid dysfunction in children with autism spectrum disorder is associated with folate receptor alpha... Article in Journal of Neuroendocrinology · February 2017 DOI: 10.1111/jne.12461 CITATIONS 0 READS 63 11 authors, including: Some of the authors of this publication are also working on these related projects: Intracellular processing and transport of cobalamins View project Stephen Gregory Kahler University of Arkansas for Medical Sciences 108 PUBLICATIONS 2,938 CITATIONS SEE PROFILE Stepan Melnyk University of Arkansas for Medical Sciences 82 PUBLICATIONS 4,047 CITATIONS SEE PROFILE Jeffrey M Sequeira State University of New York Downstate Medi… 66 PUBLICATIONS 1,299 CITATIONS SEE PROFILE Edward V Quadros State University of New York Downstate Medi… 132 PUBLICATIONS 2,478 CITATIONS SEE PROFILE All content following this page was uploaded by Edward V Quadros on 24 March 2017. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are added to the original document and are linked to publications on ResearchGate, letting you access and read them immediately.
Transcript of Thyroid dysfunction in children with autism spectrum ...iliadneuro.com/pdf/Frye_Thyroid.pdf ·...

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/313778826
Thyroiddysfunctioninchildrenwithautismspectrumdisorderisassociatedwithfolatereceptoralpha...
ArticleinJournalofNeuroendocrinology·February2017
DOI:10.1111/jne.12461
CITATIONS
0
READS
63
11authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
IntracellularprocessingandtransportofcobalaminsViewproject
StephenGregoryKahler
UniversityofArkansasforMedicalSciences
108PUBLICATIONS2,938CITATIONS
SEEPROFILE
StepanMelnyk
UniversityofArkansasforMedicalSciences
82PUBLICATIONS4,047CITATIONS
SEEPROFILE
JeffreyMSequeira
StateUniversityofNewYorkDownstateMedi…
66PUBLICATIONS1,299CITATIONS
SEEPROFILE
EdwardVQuadros
StateUniversityofNewYorkDownstateMedi…
132PUBLICATIONS2,478CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyEdwardVQuadroson24March2017.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblueareaddedtotheoriginaldocumentandarelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.

Journal of Neuroendocrinology. 2017;29:1–12. wileyonlinelibrary.com/journal/jne | 1 of 12© 2017 British Society for Neuroendocrinology
Received:14November2015 | Revised:7February2017 | Accepted:9February2017DOI: 10.1111/jne.12461
O R I G I N A L A R T I C L E
Thyroid dysfunction in children with autism spectrum disorder is associated with folate receptor α autoimmune disorder
R. E. Frye1 | R. Wynne1 | S. Rose1 | J. Slattery1 | L. Delhey1 | M. Tippett1 | S. G. Kahler1 | S. C. Bennuri1 | S. Melnyk1 | J. M. Sequeira2 | E. V. Quadros2
1DepartmentofPediatrics,ArkansasChildren’sResearchInstitute,UniversityofArkansasforMedicalSciences,LittleRock,AR,USA2DepartmentofMedicine,StateUniversityofNewYork–DownstateMedicalCenter,Brooklyn,NY,USA
CorrespondenceRichardE.Frye,ArkansasChildren’sResearchInstitute,LittleRock,AR,USA.Email:[email protected]
Funding informationArkansasBiosciencesInstitute,AutismResearchInstitute;JaneBotsfordJohnsonFoundationandAutismSpeaks,Grant/AwardNumber:#8202;UniversityofMarylandBrainandTissueBank
Folatereceptorα(FRα)autoantibodies(FRAAs)areprevalentinautismspectrumdis-order(ASD).FRAAsdisruptfolatetransportacrosstheblood-brainbarrierbybindingtotheFRα.ThyroiddysfunctionisfrequentlyfoundinchildrenwithASD.Wemeas-uredblockingandbindingFRAAsandthyroid-stimulatinghormone(TSH),freethyrox-ine (T4) (FT4), total triiodothyronine (T3) (TT3), reverse T3 (rT3), thyroid-releasinghormone(TRH)andothermetabolitesin87childrenwithASD,84ofwhomalsoun-derwentbehaviourandcognition testingand in42ofwhomFRAAs,TSHandFT4weremeasuredattwotimepoints.TobetterunderstandthesignificanceoftheFRα in relationtothyroiddevelopment,weexaminedFRαexpressiononprenatalandpost-natalthyroid.TSH,TT3andrT3wereabovethenormalrangein7%,33%and51%oftheparticipantsandTRHwasbelowthenormalrangein13%oftheparticipants.FT4was rarely outside the normal range. TSH concentration was positively and theFT4/TSH,TT3/TSHandrT3/TSHratioswereinverselyrelatedtoblockingFRAAti-tres.Onrepeatedmeasurements,changesinTSHandFT4/TSHratiowerefoundtocorrespondtochangesinblockingFRAAtitres.TSHandtheFT4/TSH,TT3/TSHandrT3/TSHratioswererelatedtoirritabilityontheAberrantBehaviorChecklistandsev-eralscalesoftheSocialResponsivenessScale(SRS),whereasTT3wasassociatedwithSRSsubscalesandTRHwasrelatedtoVinelandAdaptiveBehaviorScalesubscales.The thyroid showed significant FRα expression during the early prenatal period,althoughexpressiondecreased significantly in latergestationandpostnatal thyroidtissue.TheresultsofthepresentstudysuggestthatthyroiddysfunctioninASDmayberelatedtoblockingFRAA.ThehighexpressionofFRα intheearlyfoetalthyroidsuggeststhatfoetalandneonatalexposuretomaternalFRAAscouldaffectthedevel-opmentofthethyroidandmaycontributetothepathologyinASD.
K E Y W O R D S
autismspectrumdisorders,folatereceptorautoantibody,freeT4,thyroidfunction,thyroid-stimulatinghormone
1 | INTRODUCTION
Thereisincreasingrecognitionthatthyroiddysfunctionisassociatedwith neurological and psychiatric disease, including neurodevelop-mentaldisorderssuchasintellectualdisability1andautismspectrum
disorder (ASD),2-7 focal and generalised neurological abnormalities,8 aswellaspsychiatricmanifestationssuchaspsychosis,9,10panicat-tacks,11 anxiety disorders,11,12 bipolar disorder,13-15 depression12,14 andschizophrenia.16,17Inaddition,normalthyroidfunctionisessentialfornormalcognition.18However,theexactnatureoftherelationship

2 of 12 | FRYE YEet al
betweenthyroiddysfunctionandneurologicalandpsychiatricdiseaseisunclear.
EarlyuncontrolledtreatmentstudiessuggestedthatchildrenwithASDshowedapositiveclinicalresponsetotriiodothyronine(T3).2,19 Asmallcontrolledcross-overstudyfoundthatT3resultedinlimitedsymptomatic improvement in childrenwithASD, especially in thosewithalowerintellectualquotient.20Otherstudiesexaminingthyroidhormones have been inconsistent. A letter to editor in 1970 indi-cated a high rateof hypothyroidism (73%) in 62 childrenwithASDusingT3uptaketesting,21althoughtwoothersmallstudiescouldnotconfirmthyroiddysfunctioninASD,findingnodifferenceinthyroid-stimulating hormone (TSH), thyroxin (T4) or T3 between ASD andcontrolchildren.22,23OtherstudiessuggestthatASDhasbeenassoci-atedwithafamilyhistoryofautoimmunethyroiddisorders24andthatdeficiencies inthyroidfunctionmaybepresentbeforeoratbirth inchildrenwithASD.5,6Morerecentstudieshaveexaminedthyroidreg-ulationinthecontextofthehypothalamic-pituitary-axis(HPA)inASD.TSHatbaselineandfollowingthyrotrophin-releasinghormone(TRH)stimulationwaslowerin41Japaneseautisticboyscomparedtocon-trolswithmental retardation,minimal brain dysfunction and typicaldevelopment,suggestingabluntedHPAresponse.3DiurnalvariationinTSHlevelswasfoundtobelargerinyoungadultswithASDcom-paredtocontrols,againindicatingdifferencesinHPAfunction.4
OneofthereasonsforinconsistentfindingscouldbeexplainedifonlysubgroupsofchildrenwithASDhadabnormalthyroidfunction.A recent study reported that folate receptorα (FRα) autoantibodies(FRAA),whicharepresentinupto75%ofchildrenwithASD,25 may contribute to thyroiddysfunction inASD.7 In32childrenwithASD,thosepositivefortheblockingFRAAshadahigherTSHcomparedtothosenegative for theblockingFRAAs,and theblockingFRAAwasfoundtocorrelatepositivelywithTSH.7
TherelationshipbetweenthyroidfunctionandFRAAtitreswasin-vestigatedbecauseofthelikelihoodthatautoantibodiescouldbindtotheFRαonthethyroidandaffectitsfunctionasaresultofmonoclonalanti-bodiestothetwodifferentepitopesoftheglycosyl-phosphatidylinositollinked folate-bindingmembranegp38proteinbeing foundonnormalthyroidtissue26withlimitedfocalreactivityinsomestudies.27,28BindingofFRAAstothyroidcellscouldaffectthyroidfunctioninseveralways.WhenFRAAsbindtoepithelialcellsofthechoroidplexus29 theycandisruptFRαfunction,resultinginreducedtransportoffolateacrosstheblood-brainbarrierandcausingadisorderknownascerebralfolatedefi-ciencysyndrome.30Thus,itispossiblethatFRAAbindingonthethyroidcoulddecreasefolateentryintothyroidcells.Folateisnotaprominentcofactorinthesynthesisofthyroidhormones.However,tyrosine,whichisderivedfromphenylalanineusingphenylalaninehydroxylase,isessen-tial for theproductionof thyroidhormones. Importantly, anessentialcofactorforphenylalaninehydroxylaseistetrahydrobiopterin,whichisultimatelyderivedfromthefolatecycle.31-33
Alternatively, FRAAs binding to thyroid cells could activate theimmune system, resulting in inflammation. Additionally, the folatepathwayisintimatelyinterconnectedwithmethylationandredoxreg-ulationpathways,bothofwhichareabnormalinchildrenwithASD.34 Methylationregulatesgeneexpressionandenzymefunction,andso
alterations in methylation can affect cellular function. The reducedformofglutathione(GSH) isthemajor intracellularanti-oxidantthatnot only protects the cell from damage, but also regulates enzymefunction;thus,decreasedGSHcanresultinbothcellulardamageanddeficitsinenzymeactivity.
Althoughthepreviousstudy7onlyexaminedtherelationshipbe-tweenFRAAsandTSH, inthepresentstudy,freeT4(FT4), totalT3(TT3),reverseT3(rT3)andTRHwerealsoexamined.WehypothesisethatFRAAsmaybedisruptingtheHPAbybluntingthesensitivityofthethyroidtoTSHor,inotherwords,makingthethyroidresistanttotheeffectsofTSH.ThiswouldresultinahigherTSHconcentrationtoproduce aparticular thyroidhormone concentration.Quantitatively,suchaneffectshouldbedetectablebymeasuringtheratioofathy-roidhormonetoTSHanddeterminingwhetherthisratioisalteredbyFRAAs.WeinvestigatedthisbyexaminingtherelationshipsbetweenFRAAsandTSH,FT4,TT3,rT3,TRHandtheratioofthyroidhormones(FT4/TT3/rT3) toTSH. Inaddition,wedeterminedwhethermarkersofglutathioneandmethylationandbloodconcentrationsoffolatearerelatedtothyroidfunctionaimingtoensurethatthesephysiologicalprocessesarenotconfoundersinthethyroidfunction-FRAAsrelation-ship.Wealsoexaminedtherelationshipbetweenthyroidfunctionandbehaviourandcognition.
Lastly,wealso investigatedthedevelopmental timingofthepo-tential relationship between FRAAs and thyroid function. Becausethyroid metabolism is critical prenatally35,36 and some mothers ofchildrenwithASDarepositiveforFRAAs,25,37weexaminedthede-velopmentalaspectoftheFRαonbothfoetalandpost-natalthyroidtissuetodeterminewhethertheFRαismoresignificantlyrepresentedduringa specificdevelopmental timeperiod.Wealsoexamined thechangeinFRAAs,TSHandFT4overa12-weekperiodduringaclinicaltrial.38Theaimwas todeterminewhetherFRAAsandthyroid func-tionchangetogether,insupportofthenotionthatFRAAsandthyroidfunctionaredynamicallylinked.
2 | MATERIALS AND METHODS
Eighty-seven children with ASD (mean±SD age 6years10months±3years1month)andtwelvetypicallydevelopingcontrols(mean±SD age 8years 2months±5years 2months) participated inthepresentstudy.ControlswereusedtoobtainmeasuresofnormalFT4andTSHinthesamepopulation,independentofestablishedcon-trolranges.ThesamplesusedinthepresentstudywereobtainedfromtworesearchprotocolsapprovedbytheInstitutionalReviewBoardattheUniversityofArkansasforMedicalScience(LittleRock,AR,USA).Forbothstudies,written informedconsentwasobtained frompar-entsofparticipants;participantassentwaswaived.Forbothstudies,fastingbloodsamplesbeforebreakfastwererequiredasoneofthefirstproceduresafterconsent.Theinclusionandexclusioncriteriare-mainedbroad,aimingtoincludearepresentativesampleofchildrenwithidiopathicASD.
AdiagnosisofASDwasrequiredforentryintothestudy.Adiagno-siswasdefinedbyoneofthefollowing:(i)agold-standarddiagnostic

| 3 of 12FRYE YEet al
instrument such as the Autism Diagnostic Observation Scheduleand/orAutismDiagnosticInterview-Revised(ADI-R); (ii)theStateofArkansas diagnostic standard, defined as agreement of a physician,psychologist and speech therapist; and/or (iii) Diagnostic StatisticalManual diagnosis by a physician along with standardised validatedquestionnairesanddiagnosisconfirmationbytheprincipalinvestiga-tor(R.E.Frye).ReconfirmationofthediagnosisusingtheADI-Rbyanindependentresearchreliableraterwasrequestedforaportionofpar-ticipantstoconfirmthatthecriteriausedforincludingtheparticipantswasequivalenttothisgold-standardinstrument.39
Excludedfromthestudywerethosechildrenonmedicationinter-feringwiththyroidfunction,includingthyroidsupplements,steroids,β-blockers, antipsychoticsand lithium,aswell aschildrenwithwell-definedgeneticsyndromes.
2.1 | Folate autoantibody assay
Approximately 1mL of serumwas collected and sent to the labo-ratoryofDrEdwardQuadrosat theStateUniversityofNewYork,Downstate(Brooklyn,NY,USA).Theassayforboththeblockingandbinding FRAAs has been described previously.30,40 Blocking FRAAswereexpressedaspmoloffolicacidblockedfrombindingtoFRαpermLofserum,andbindingFRAAswereexpressedaspmolofimmuno-globulin(Ig)GantibodypermLofserum.
2.2 | Thyroid function assays
PlasmaTSH,FT4,TT3,TRH, rT3andcortisolweremeasuredusingenzyme-linkedimmunosorbentassay(ELISA)kitsinaccordancewiththe manufacturer’s instructions (ab1000660, ab108686, ab108685from Abcam, Cambridge, MA, USA; CEA839Hu from Cloud-CloneCorp, Houston, TX, USA; MBS2510365 from MyBioSource, SanDiego, CA, USA; 11-CORHU-E01 from ALPCO, Salem, NH, USA).TSH,TT3andFT4were interpretedusingtheNationalAcademyofClinical Biochemistry standard for children.41 TSH reference rangewas0.4-5.0mIU/L, FT4 reference rangewas9-20pmol/L andTT3referencerangewas80-180ng/dL.BecausetheFT4toTSHratioisknowntobelogdistributed,thethyroidhormone(FT4,TT3,rT3)toTSHratioswerelog-transformedbeforeanalysis.41NormativevaluesforTRH,rT3andcortisolwereobtainedfromthemanufacturersasbeingintherange35.7-167.8pg/mL,2.4-45.8ng/dLand7-25μg/dL,respectively.Cortisolwasmeasuredbecausethyroidhormonescanbemodulatedbycortisol.
2.2.1 | Immunohistochemical analysis of FRα expression in the thyroid
Foetalthyroidtissuefrom15,17,18,19and20weeksoldfoetusespreservedinformalinwereobtainedfromtheUniversityofMarylandBrainandTissueBank,whichisaBrainandTissueRepositoryoftheNIHNeuroBioBank.Thesewereembedded inparaffinandsections(6 μm thick)were cut. Thyroid sections from a 5-month-old infant,3-year-old child and a 27-year-old adult were purchased from US
Biomax Inc. (Rockville, MD, USA). All sections were deparaffinisedandincubatedwith100μLofgoatserumfor1hourfollowedbyin-cubationwith a 1:500 dilution of rabbit antihumanFRα in 100 μLof goat serumovernight. The sectionswerewashed and incubatedwith a1:600dilutionof goat anti rabbit IgG-peroxidase conjugate(VectorLaboratories, Inc.,Burlingame,CA,USA) for1hour,washedandincubatedwithdiaminobenzidineasthechromagen.Thesectionswerestainedwithhaematoxalin(VectorLaboratories,Inc.)tovisualisethenuclei.
Thepolyclonalantiserumusedwaspreparedby immunisingrab-bits with affinity purified FRα from human epidermoid carcinomaKBcellsconditionedtogrowinlowfolatethatup-regulatesFRαex-pression.42Thepurityoftheantigenwascheckedbysodiumdodecylsulphate-polyacrylamidegel electrophoresis.The titreof theantise-rumwascheckedbydirect immunoprecipitationof 3HPGA-FRα and byELISAandthespecificityoftheantiserumwascheckedbyblockingthetitrewithexcesspurifiedFRα.ThespecificityofimmunostainingwasestablishedbyabsorbingouttheantibodyontoFRα-sepharosematrixandbyblockingofimmunostainingwhentheantiserumispre-incubatedwithaten-foldmolarexcessofpurifiedFRα.
2.3 | Redox, methylation, immune and vitamin biomarkers
Redoxandmethylationpotentialwasmeasuredbythefreereduced-to-oxidised glutathione redox ratio (GSH/GSSG) and SAM to SAHratio(SAM/SAH),respectively.Fastingblood(4mL)wascollectedintoanethylenediaminetetraceticacid-Vacutainertube,chilledoniceandcentrifuged at 1500g for 15minutes at 4°C. Plasmawas stored at−80°Candanalysedbyhigh-performanceliquidchromatographywithelectrochemicaldetectionwithin2weeksofcollectionasdescribedpreviously.43PlasmatotalfolateandvitaminB12wasmeasuredusingaSimulTRAC-SNBRadioassayKit(cataloguenumber06B264806;MPDiagnostics,SantaAna,CA,USA).
2.4 | Cognitive and behavioural assessments
The Preschool Language Scale-4 and two versions of the ClinicalEvaluationsofLanguageFundamentalswereusedtoassesslanguageability.38 Both instruments provide a standardised core languagescore,thusprovidinganindexoflanguageabilityindependentoftheinstrument used. For each participant, themost ability appropriateinstrumentwasused toprevent floor and ceiling effects. Languagetestingwasavailableon84participants.
Adaptive behaviour was assessed using the Vineland AdaptiveBehaviorScales(2ndedition),InterviewEdition,SurveyForm(VABS),an instrument that has demonstrated good reliability andvalidity.44 Standardisedscoresforsummaryscalesexaminedwerecommunica-tion,dailylivingskills,socialskills,motorskillsandadaptivebehaviourcomposite.VABStestingwasavailableon84participants.
TheAberrantBehaviorChecklist(ABC)wasdesignedtomeasuredisruptivebehavioursinindividualswithdevelopmentaldisabilities.45 TheABChasbeenshowntohaveconvergentanddivergentvalidity

4 of 12 | FRYE YEet al
inASD46 andhasbeenused inmultipleautismclinical trials.47ABCscoreswereavailableon82participants.
The Social Responsiveness Scale (SRS)measures the severity ofsocialskilldeficits.48Ithasbeenvalidatedandshowntobereliableandtohavegoodcorrespondencetothegold-standardADI-R,atthesametimeasbeingmoretimeefficientandcosteffective.49SRSscoreswereavailableon81participants.
2.5 | Folinic acid treatment
Forty-twoparticipantswerepartofadouble-blind,placebo-controlledtrialontheeffectoffolinicacidonchildrenwithASD.38Inthesepar-ticipants, FRAA titres,TSHandT4weremeasuredprior to startingtreatmentandattheendof12weeksoftreatmentwitheitherhigh-dosefolinicacid(2mg/kg/dayintwodivideddoses;maximum50mg/day)orplaceboinmostoftheparticipantsinthetrial.
2.6 | Statistical analysis
The ‘glm’and ‘glimmix’procedureofSAS,version9.1 (SASInstituteInc.,Cary,NC,USA)wereused for the cross-sectional analysis andrepeated-measuresanalysis,respectively,andatwo-tailedαof0.05wasused.WedichotomisedblockingandbindingFRAAstatussepa-rately,aswellas theoverallFRAAstatus (positivevsnegative).Wealsoexaminedtherelationshipbetweenthyroidhormonesandblock-ingandbindingFRAAtitresseparately.Amixed-modelwasusedforthe repeatedmeasures analysiswith theparticipant variable as therandom-effect.
3 | RESULTS
3.1 | Participants
Participantswererecruitedfromourresearchregistry(40%),autismclinic(23%),communityadvertisementandsocialmedia(10%),word-of-mouth (15%)andphysician referrals (13%).Thebasicparticipantcharacteristics did not differ across the FRAA status (Table1). Allparticipantsevaluatedbyan independentresearchreliableraterex-ceededthethresholdforautismdiagnosis.
3.2 | Overall thyroid function
FortheoverallASDpopulation,themean±SDTSHconcentrationwas2.76±1.82mIU/L(range0.63-11.55mIU/L)andwasbelowandabovethestandardreferencerangein0%and7%ofASDparticipants,re-spectively,andnodifferentfromcontrols(4.14±2.13mIU/L).
For the overall ASD population, FT4 concentration was14.38±2.27pmol/L (range 8.66-21.12pmol/L) and was below andabove thestandard reference range in1%and2%ofASDchildren,respectively, and slightly higher than controls (13.77±3.00pmol/L)(F1,94=5.19,P=.03).
FortheoverallASDpopulation,theFT4/TSHratiowas0.78±0.26andwasnotsignificantlydifferentfromcontrols(0.56±0.29).
TT3 concentration was 170.5±24.4ng/dL (range 117.4-224.6 ng/dL)andwasabnormallylowandhighin0%and33%oftheASDchildren, respectively,using thestandard reference range.TheTT3/TSHratiowas1.86±0.28(range1.12-2.50).
rT3 concentrationwas 49.8±13.5ng/dL (range 28.8-95.3ng/dL)andwasabnormallylowandhighin0%and51%oftheASDchildren,respectively,usingthemanufacturer’sreferencerange.TherT3/TSHratiowas1.32±0.28(range0.65-1.92).
Thyroid-releasing hormone concentrationwas 61.0±24.0pg/mL(range19.7-127.9pg/mL) andwasabnormally lowandhigh in13%and 0%of theASD children, respectively, using themanufacturer’sreferencerange
Thyroidhormoneswerenotsignificantlycorrelatedwithcortisollevels.
3.3 | Thyroid function and folate- related metabolism
FT4wasrelatedtotheSAM/SAHratio,anindexofmethylationab-normalities, such that a higher SAM/SAH ratio (bettermethylation)wasrelatedtoalowerFT4(F1,84=8.30,P=.005).TSHwasfoundtobepositivelyrelatedtotheglutathioneredoxratio,suchthathigher(bet-ter)glutathioneredoxratiowasrelatedtohigherTSHconcentrations(F1,84=4.48,P=.05).
Noneoftheotherthyroidfunctionmeasureswerelinearlyrelatedtoglutathione,SAM/SAH,folateorB12.
3.4 | Thyroid function and folate receptor α autoantibodies
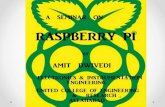
Thyroid-stimulatinghormonewassignificantlyhigher inparticipantspositive(3.94±2.94mIU/L)fortheblockingFRAAcomparedtothosenegative (2.49±1.38mIU/L) for the blocking FRAA (F1,83=10.85,P=.001) and the TSH concentration was found to increase as theblockingFRAAtitresincreased(F1,84=7.85,P=.006)(Figure1A).
Participants who were positive for the blocking FRAA demon-strateda lowerFT4/TSHratio(0.66±0.30)comparedtoparticipantsnegativefortheblockingFRAA(0.82±0.25)(F1,83=6.12,P=.02). In ad-dition,theblockingFRAAtitredemonstratedaninverserelationshipwiththeT4/TSHratio(F1,84=5.27,P=.02)(Figure1B).
Participants who were positive for the blocking FRAA demon-strateda lowerTT3/TSHratio(1.71±0.32)comparedtoparticipantsnegativefortheblockingFRAA(1.90±0.27)(F1,83=6.09,P=.02). In ad-dition,theblockingFRAAtitredemonstratedaninverserelationshipwiththeTT3/TSHratio(F1,84=7.58,P<0.01(Figure1C).
Participants who were positive for the blocking FRAA demon-strateda lower rT3/TSH ratio (1.36±0.27) compared toparticipantsnegativefortheblockingFRAA(1.67±0.28)(F1,83=6.09,P=.02). In ad-dition,theblockingFRAAtitredemonstratedaninverserelationshipwiththerT3/TSHratio(F1,84=4.95,P=.03)(Figure1D).
Thyroid-stimulatinghormoneandtheratiosofthyroidhormones(FT4,TT3,rT3)toTSHwerenotsignificantlydifferentacrosspositivevsnegativebindingFRAAparticipants,norweretheysignificantlylin-earlyrelatedtobindingFRAAtitres.

| 5 of 12FRYE YEet al
TABLE 1 Demographicandclinicalcharacteristicsbyfolatereceptorαautoantibodygroups
Variable FRAA negative (n=35) FRAA positive (n=52)
Age(years,months),mean±SD 6years10months±3years6months 6years11months±2years11months
Males,n(%) 28(80%) 42(81%)
Vinelandadaptivebehaviourcomposite,mean(SD) 64.2 (11.7) 64.8 (9.8)
TSH(mIU/L) 2.44(1.36) 3.00(2.06)
HighTSH(<0.4mIU/L) 2(5%) 5(9%)
LowTSH(>5.0mIU/L) 0(0%) 0(0%)
FreeT4(pmol/L) 14.47 (1.92) 14.33(2.51)
HighT4(<9pmol/L) 0(0%) 2(4%)
LowT4(>20pmol/L) 0(0%) 1(2%)
FreeT4toTSHratio(log-transformed) 0.84 (0.26) 0.75 (0.27)
TotalT3(ng/dL) 170.41 (25.1) 170.5 (24.2)
HighT3(>180ng/dL) 0(0%) 0(0%)
LowT3(<80ng/dL) 13(37%) 16(31%)
TotalT3toTSHratio(log-transformed) 1.91 (0.28) 1.73(0.23)
ReverseT3(ng/dL) 48.9(8.3) 57.9(23.4)
HighrT3(>45.77ng/dL) 0(0%) 0(0%)
LowrT3(<2.39ng/dL) 20(57%) 24(46%)
ReserveT4toTSHratio(logtransformed) 1.36(0.27) 1.18 (0.22)
Thyroid-releasinghormone(pg/mL) 65.6 (24.6) 50.4 (16.2)
HighTRH(>167.8pg/mL) 3(9%) 8(15%)
LowTRH(<35.7pg/mL) 0% 0%
Cortisol(μg/dL) 18.45 (8.9) 20.4(13.0)
Folate(ng/mL)(normal5-21) 16.9(3.9) 18.0 (4.5)
B12(pg/mL)(normal200-900) 786(395) 1313(1391)
Languagetesting,n(%)
PreschoolLanguageScales 13(37%) 16(30%)
Clinicalevaluationoflanguagefundamentals2 14(40%) 17(32%)
Clinicalevaluationoflanguagefundamentals4 7(20%) 20(38%)
Diagnosticdocumentation,n(%)
Autismdiagnosticobservationschedule 18(51%) 25(47%)
3Practitioneragreement 27(77%) 35(66%)
Singlepractitionerwithstandardisedquestionnaires 5(14%) 13(25%)
Autismdiagnosticinterview-revised
Participatedinconfirmationtesting,n(%) 28(80%) 41(77%)
Socialinteractionscore,mean±SD(range) 21.57±5.41(10-30) 22.68±4.85(11-30)
Communicationscore:verbal,mean±SD(range) 16.67±4.24(10-24) 19.38±3.67(7-25)
Communicationscore:nonverbal,mean±SD(range) 12.69±2.36(7-14) 13.07±1.53(9-14)
Restricted&repetitiveplayscore,mean±SD(range) 5.79±1.83(2-10) 5.95±2.47(2-12)
Summaryscore,mean±SD(range) 4.43±0.92(2-5) 4.39±0.89(2-5)
Medications(concurrenttreatments),n(%)
Melatonin 15(43%) 11(21%)
Allergy/asthmamedications 11(31%) 11(21%)
Gastrointestinalmedications 11(31%) 9(17%)
α-Adrenergicagonists 6(17%) 10(19%)
Stimulant 6(17%) 8(15%)
(Continues)

6 of 12 | FRYE YEet al
Thyroid-releasinghormone,FT4,T3andrT3werenotsignificantlydifferentacrossFRAAgroups,norweretheysignificantlylinearlyre-latedtoblockingorblindingFRAAtitres.
3.5 | Relationship between thyroid function and behavior and cognition
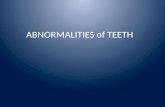
HigherTSHwasrelatedtolower(better)ABCIrritability(F1,80=5.94,P=.02)(Figure2A)andSRSAwareness(F1,79=5.01,P=.03)(Figure2B),Cognition (F1,79=5.97, P=.03) (Figure2C), Motivation (F1,79=4.46,P=.04) (Figure2D), Mannerisms (F1,79=6.87, P=.01) (Figure2E) andTotalscore(F1,79=5.72,P=.02)(Figure2F).
A higher FT4/TSH ratio was related to higher (worse) ABCIrritability(F1,80=7.56,P=.01)(Figure2G)andHyperactivity(F1,80=5.29,P=.02) (Figure2H)andSRSAwareness(F1,79=4.70,P=.03) (Figure2I),Cognition (F1,79=5.82,P=.02) (Figure2J),Communication (F1,79=4.00,P=.05) (Figure2K), Motivation (F1,79=4.89, P=.03) (Figure2l),Mannerisms(F1,79=5.35,P=.02)(Figure2M)andTotalscore(F1,79=5.61,P=.02)(Figure2N).
HigherT3wasrelatedtohigher(worse)SRSCognition(F1,79=4.83,P=.03) (Figure2O), Motivation (F1,79=6.98, P=.01) (Figure2P),
Mannerisms(F1,79=4.55,P=.04)(Figure2q)andTotalscore(F1,79=5.14,P=.03)(Figure2R).
AhigherTT3/TSHratiowasrelatedtohigher(worse)ABCIrritability(F1,80=8.40,P=.005)(Figure2S)andSRSAwareness(F1,79=6.45,P=.01) (Figure2T),Cognition(F1,79=6.87,P=.01)(Figure2U),Communication(F1,79=3.83, P=.05) (Figure2V), Motivation (F1,79=4.90, P=.03)(Figure2W), Mannerisms (F1,79=6.35, P=.01) (Figure2X) and Totalscore(F1,79=7.50,P<.01)(Figure2Y).
AhigherrT3/TSHratiowasrelatedtohigher(worse)ABCIrritability(F1,80=10.26, P=.002) (Figure2AA) and SRS Awareness (F1,79=5.14,P=.03) (Figure2AB), Cognition (F1,79=4.35, P=.04) (Figure2AC) andTotalscore(F1,79=5.30,P=.02)(Figure2AD).
HigherTRHwasrelatedtolower(worse)VABSDailyLivingSkills(F1,82=5.36, P=.02) (Figure2AE) and Social Skills (F1,82=4.25, P=.04) (Figure2AF).
3.6 | Repeated thyroid and autoantibody measurements
Forty-twoparticipantswerepartofaclinicaltrialinwhichtheywereblindlyrandomisedtoreceiveeitherplaceboorhigh-dosefolinicacid
Variable FRAA negative (n=35) FRAA positive (n=52)
Anti-epilepticmedication 1(3%) 7(13%)
Selectiveserotoninreuptakeinhibitors 0(0%) 7(13%)
Antimicrobialmedications 2(6%) 3(6%)
Immunomodulatorymedications 1(3%) 2(4%)
Otherpsychotropicmedications 0(0%) 1(2%)
Supplements(concurrenttreatments),n(%)
Multivitamin 14(40%) 16(30%)
Minerals 5(14%) 11(21%)
Fattyacids 4(11%) 9(17%)
VitaminB12 1(3%) 10(19%)
OtherBvitamins 2(6%) 8(15%)
Folate 4(11%) 6(11%)
Otherantioxidants 2(6%) 7(13%)
Carnitine 2(6%) 6(11%)
Othervitamins 4(11%) 4(8%)
CoenzymeQ10 2(6%) 3(6%)
Othersupplements 0(0%) 2(4%)
Aminoacids 0(0%) 1(2%)
Comorbidmedicalconditions,n(%)
Allergicdisorders 15(43%) 21(40%)
Gastrointestinaldisorders 14(40%) 22(42%)
Neurologicaldisorders 6(17%) 17(32%)
Nondiagnosticcopynumbervariants 8(23%) 15(28%)
Psychiatricdisorders 2(6%) 15(28%)
Immuneabnormality 6(17%) 9(17%)
FRAA,folatereceptorαautoantibody;T3,triiodothyronine;T4,thyroxine;TRH,thyroid-releasinghormone;TSH,thyroid-stimulatinghormone.
TABLE 1 (Continued)

| 7 of 12FRYE YEet al
andhadboththyroidfunctionandFRAAmeasuredatthebeginningandendofthetrial.Thisallowedustoexaminethecorrespondencebetweenthechange inthyroidfunctionandFRAAtitresandtode-terminewhetherhigh-dosefolinicacidhadanysystematiceffectonthyroidfunction.
ThechangeinTSHandFT4/TSHratio(butnotFT4)wassignifi-cantly related to the change in blockingFRAA, but not thebindingFRAA.ThechangeinTSHhadapositiverelationshipwiththeblockingFRAAtitres(F1,40=6.22,P=.02)(Figure3A),whereasthechangeintheFT4/TSHratiohadaninverserelationshiptotheblockingFRAAtitres(F1,40=4.39,P=.04) (Figure3B). NeitherTSH and FT4, nor FT4/TSHratioswererelatedtowhetherornotthepatientreceivedhigh-dosefolinicacidorplacebo.
3.7 | FRα expression in the thyroid
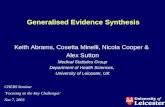
ToexaminethedevelopmentalaspectoftheFRαwithrespecttothy-roiddevelopment,FRαexpressionwasmeasuredonthethyroidglandduringvariousagesoflife.Figure4showsthatFRαishighlyexpressedat15and17weeksofgestation,whereasFRαisnotexpressedinthefoetaltissueat18,19or20weeksofgestation,norwasitexpressedinthe5-monthpostpartumthyroidtissue,suggestingthatFRαexpressionisonlypresentinearlygestationandlostinlatergestationasthethy-roidmatures.Wehavealsoexaminedthyroidfroma3-year-oldchildanda27-year-oldadultandfoundnoFRαexpression(datanotshown).
4 | DISCUSSION
BothblockingandbindingFRAAsareconsideredtohavepathologicalconsequencesinASDbecausetheybindtotheFRαwheretheycaninterferewithfunctionoftheFRαandreducethetransportationoffolate intothecentralnervoussystem25andtheymayalsoactivatetheimmunesystem.50TherearereportsoftheFRαbeingexpressedonnormalthyroidtissue,26althoughsometimesonlytoalimitedex-tent.27,28 In the present study, we investigated the significance ofFRAAsinconjunctionwiththyroidfunction inchildrenwithASDtofollow-up on our previous report.7We also examined FRα expres-siononthethyroidtissueatdifferentstagesofhumandevelopment.Severalinterestingrelationshipswereidentified.
AutismspectrumdisorderchildrenpositiveforblockingFRAAshadhigherTSHand lowerFT4/TSH,TT3/TSHand rT3/TSH ratios thanthosenegativeforblockingFRAAs.Additionally,blockingFRAAtitreswerelinearlyrelatedtoTSHconcentrationsandFT4/TSH,TT3/TSHandrT3/TSHratios.Furthermore,whenweexaminedthechangesinFRAAtitresandthyroidfunction(TSH,FT4)overa12-weekperiod,wefoundastrongrelationshipbetweenachangeinblocking(butnotbinding)FRAAtitresandachangeintheTSHandFT4/TSHratio,con-sistentwiththecross-sectiondata.TheblockingFRAAdidnotappeartohavesignificantinfluenceonFT4,TT3orrT3specifically.
ItappearsthattheblockingFRAAhasaninfluenceonTSHandtheFT4/TSH,TT3/TSHandrT3/TSHratiosbyincreasingtheTSHrelative
F IGURE 1 Inchildrenwithautismspectrumdisorderhigherblockingfolatereceptorαautoantibody(FRAA)titresareassociatedwith(A)higherthyroid-stimulatinghormone(TSH),(B)lowerthyroxine(T4)toTSHratio,(C)lowertotaltriiodothyronine(T3)toTSHratioand(D)lowerreserveT3toTSHratio
12
8
TSH
(mIU
/L)
Free
T4
to T
SH r
atio
(log
tra
nsfo
rmed
)
4
00 0.5 1 1.5
1.5
1.0
0.5
0.0
Tota
l T3
to T
SH r
atio
(log
tra
nsfo
rmed
)
1.5
1.0
2.5
2.0
Reve
rse
T3 t
o TS
H r
atio
(log
tra
nsfo
rmed
)
1.5
0.5
1.0
2.0
Blocking autoantibody titre (pmol/L)0 0.5 1 1.5Blocking autoantibody titre (pmol/L)
0 0.5 1 1.5Blocking autoantibody titre (pmol/L)
0 0.5 1 1.5Blocking autoantibody titre (pmol/L)
(A) (B)
(C) (D)

8 of 12 | FRYE YEet al
totheproductionofthyroidhormones.ThissuggeststhattheeffectoftheblockingFRAAonthyroidfunctionmayoccuratthelevelofthethyroidbymakingthethyroidlesssensitivetoTSHoralteringthesen-sitivityoftheHPA.Specifically,alowerFT4/TSH,TT3/TSH,rT3/TSHratioswouldsuggestthatahigherTSHconcentrationisneededforthe
productionof thyroidhormones, implyingadecreasedsensitivityofthethyroidorHPA.TheideathatchildrenwithASDmayhavediffer-encesinHPAdynamicsand/orthyroidsensitivitytoTSHisconsistentwithbothresearchandclinicalstudies.Studieshaveshownabluntedpituitary response toTRHstimulation inASDboys3and thediurnal
F IGURE 2 Therelationshipbetweenthyroidfunctionandbehaviourinchildrenwithautismspectrumdisorder.Higherthyroid-stimulatinghormone(TSH)wasassociatedwithlower(better)(A)AberrantBehaviorChecklist(ABC)Irritability,(B)SocialResponsivenessScale(SRS)Awareness,(C)SRSCognition,(D)SRSMotivation,(E)SRSMannerisms(F)SRSTotalScore;Higherfreethyroxine(T4)toTSHratiowasassociatedwithhigher(worse)(G)ABCIrritability,(H)ABCHyperactivity,(I)SRSAwareness,(J)SRSCognition,(K)SRSCommunication,(I)SRSMotivation,(M)SRSMannerismsand(N)SRSTotalScore;HighertotalT3wasassociatedwithhigher(worse)(O)SRSCognition,(P)SRSMotivation,(Q)SRSMannerismsand(R)SRSTotalScore.Highertotaltriiodothyronine(T3)toTSHratiowasassociatedwithhigher(worse)(S)ABCIrritability,(T)SRSAwareness,(U)SRSCognition,(V)SRSCommunication,(W)SRSMotivation,(X)SRSMannerismsand(Y)SRSTotalScore;HigherreverseT3toTSHratiowasassociatedwithhigher(worse)(AA)ABCIrritability,(AB)SRSAwareness,(AD)SRSCognition,and(AD)SRSTotalScore;HigherThyroidReleasingHormonewasrelatedtoworse(lower)(AE)VABSDailyLivingSkillsand(AF)VABSSocialSkills
50
40
30
20
10
00 4
TSH (mIU/L)8 12
ABC
Irrit
abili
ty (r
aw s
core
)
0 4TSH (mIU/L)
8 12
100
80
60
40
SRS
Aw
aren
ess
(T s
core
)
0 4TSH (mIU/L)
8 12
100
80
60
40
SRS
Cog
nitio
n (T
sco
re)
0 4TSH (mIU/L)
8 12
100
80
60
40
SRS
Mot
ivat
ion
(T s
core
)
0 4TSH (mIU/L)
8 12
100
80
60
40
SRS
Man
neris
ms
(T s
core
)
0 4TSH (mIU/L)
8 12
100
80
60
40
SRS
Tota
l (T
scor
e)
50
40
30
20
10
00 0.5
Free T4 to TSH ratio1 1.5
ABC
Irrit
abili
ty (r
aw s
core
)
50
40
30
20
10
0
ABC
Hyp
erac
tivity
(raw
sco
re)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Aw
aren
ess
(T s
core
)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Cog
nitio
n (T
sco
re)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Coo
mun
icat
ion
(T s
core
)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Mot
ivat
ion
(T s
core
)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Man
neris
ms
(T s
core
)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40
SRS
Tota
l (T
scor
e)
0 0.5Free T4 to TSH ratio
1 1.5
100
80
60
40100 150 200 250
SRS
Cog
nitio
n (T
sco
re)
Total T3 (ng/dL)100 150 200 250
Total T3 (ng/dL)
100
80
60
40
SRS
Mot
ivat
ion
(T s
core
)
100 150 200 250Total T3 (ng/dL)
100
80
60
40
SRS
Man
neris
ms
(T s
core
)
100
80
60
40
SRS
Tota
l (T
scor
e)
100 150 200 250Total T3 (ng/dL)
Total T3 to TSH ratio
50
40
30
20
10
01 1.5 2 2.5
ABC
Irrit
abili
ty (r
aw s
core
)
100
80
60
40
SRS
Aw
aren
ess
(T s
core
)
Total T3 to TSH ratio1 1.5 2 2.5
100
80
60
40
SRS
Cog
nitio
n (T
sco
re)
Total T3 to TSH ratio1 1.5 2 2.5
100
80
60
40
SRS
Coo
mun
icat
ion
(T s
core
)
Total T3 to TSH ratio1 1.5 2 2.5
100
80
60
40
SRS
Mot
ivat
ion
(T s
core
)
Total T3 to TSH ratio1 1.5 2 2.5
100
80
60
40
SRS
Mot
ivat
ion
(T s
core
)
Total T3 to TSH ratio1 1.5 2 2.5
100
80
60
40
SRS
Tota
l (T
scor
e)
Total T3 to TSH ratio1 1.5 2 2.5
50
40
30
20
10
00.5 1
Reverse T3 to TSH ratio1.5 2
ABC
Irrit
abili
ty (r
aw s
core
)
100
80
60
40
SRS
Aw
aren
ess
(T s
core
)
0.5 1Reverse T3 to TSH ratio
1.5 2
100
80
60
40
SRS
Cog
nitio
n (T
sco
re)
0.5 1Reverse T3 to TSH ratio
1.5 2
100
80
60
40
SRS
Tota
l (T
scor
e)
0.5 1Reverse T3 to TSH ratio
1.5 2
0 50 100 150
100
80
60
40Dai
ly L
ivin
g Sk
ills
(Sca
led
Scor
e)
Thyroid-releasing hormone (pg/mL)
100
80
60
40
Soci
al S
kills
(Sca
led
Scor
e)
0 50Thyroid-releasing hormone (pg/mL)
100 150
(A) (B) (C) (D) (E) (F)
(G) (H) (I) (J) (K) (L) (M) (N)
(S) (T) (U) (V)
(AA) (AB)
(AE) (AF)
(AC) (AD)
(W) (X) (Y)
(O) (P) (Q) (R)
F IGURE 3 Changein(A)thyroid-stimulatinghormone(TSH)and(B)thefreethyroxine(T4)toTSHratioisassociatedwithachangeintheblockingfolatereceptorαautoantibody
5 0.2
–0.2
–0.6
–1.0
4
3
2
1Cha
nge
in T
SH
Cha
nge
in T
4 to
TSH
rat
io
0
–1–1.0 –0.5
Change in blocking autoantibody0.0 0.5 1.0 1.5 –1.0 –0.5
Change in blocking autoantibody0.0 0.5 1.0 1.5
(A) (B)

| 9 of 12FRYE YEet al
variationofTSHappearstobelargerinyoungadultswithASD.4TRHconcentrationswerenotrelatedtoblockingFRAAtitres,whichsug-geststhattheeffectisatthelevelofthethyroidandnotthepituitary.
Theeffectofthyroidhormonesonthebrainiscomplex,especiallyduringfoetalandneonataldevelopment.35,36FRαishighlyexpressedinfoetalthyroidtissueonlyearlyingestation,withnoobservableex-pressioninlategestationorpostnatalthyroidtissue.Thisisbasedonalimitednumberofthyroidsamplesandthereforethisfindingshouldbe considered preliminary. Exposure tomaternal FRAAs and folatedeficiency in uteromaycontributetopoordevelopmentoftheglandanddysfunction in later life.Thereportedhistologicaldatasuggeststhatthe influenceofFRAAscouldoccurduringfoetaldevelopment.BecauseseveralstudieshavedemonstratedthatmothersofchildrenpositiveforFRAAsalsoarepositiveforFRAAs,25,37itispossiblethatmaternalFRAAspresentduringgestationcoulddisruptthyroiddevel-opmentand/oralterthedevelopmentalexpressionoftheFRαonthethyroid.
There isevidencethatmaternalFRAAscandisruptfoetaldevel-opment.MaternalFRAAsresultinneurodevelopmentalabnormalitiesinrodentoffspring51andmaternalFRAAshavebeenlinkedtoneuraltubedefectsandsubfertilityinhumans,52aswellaspretermbirth.53ItispossiblethatdisruptionoffoetalthyroiddevelopmentbymaternalFRAAscouldhaveresultedinalteredregulationofthethyroidduringchildhood.However,thechangeinTSHwithchangeinFRAAdemon-stratedon repeatedmeasurements suggest thatFRAAsmayhaveamoredirecteffectonregulationofthethyroidduringchildhood.Forexample,itispossiblethatfoetalexposuretoFRAAsmayhavealtereddevelopmentalFRαexpressionsothattheFRαhasincreasedexpres-siononthethyroidduringchildhood.Examiningthyroidtissuefrom
children exposed to FRAAs during gestationwould help clarify thispossibility.However,toourknowledge,nosuchtissueisavailableatpresent.
Behaviourappearstoberelatedtothyroidfunction inASDchil-drensuchthathigherlevelsofTSHisassociatedwithbetterASDbe-haviouralcharacteristicsusingtheABCaswellastheSRSscales,aninstrument thathashighcorrespondencewithagold-standardASDassessment, theADI-R.TheFT4/TSH,TT3/TSHandrT3/TSHratiosalsoappeartobesimilarlyrelatedtoABCandSRSscales,suchthatalowerratio isassociatedwithbetteroverallbehaviour.Therelation-ship between thyroid hormones and behaviour should not be sur-prisingbecausethyroidhormonescanbothpositivelyandnegativelymodulateneurotransmittersystemsas,wellashaveadirecteffectongeneexpression.54However, theexactmechanismbywhichthyroidhormones influencebehaviourandcognition inASDremains to theclarified.
Thyroid-stimulatinghormoneisrelatedtobehavioureventhough,forthemostpart,itiswithinthenormalrangeinoursample,andbothTSHandtheFT4/TSHarerelatedtobehavioureventhoughtheyarenotsignificantlydifferentthanthecontrolvaluesinoursample.Thissuggests that theeffect is not related to absolute thyroidhormonelevelsbutrathertoHPAsensitivity,suchthatsomechildrenwithASDmaybemoresensitivetoasmallvariationinthyroidhormonelevels.Thiswould suggest that the relationship betweenTSH and thyroidhormonesproducedbythethyroid(ie,FT4,TT3,rT3)ismoreimport-ant that theabsoluteconcentrationsof thesehormones.This couldexplainwhysomestudieshavedemonstratednormalthyroidhormonelevels in childrenwithASD,22,23whereas others have showndiffer-encesindynamicchangesinthyroidhormonesinchildrenwithASD,
F IGURE 4 Folatereceptorαexpressioninthethyroidtissueduringembryonicdevelopmentandfollowingbirth.(A)Folatereceptorα expressioninthethyroidgland.Counterstainedsampleswithhaematoxylintovisualisenuclei.(B)Tissuestainedwithhaematoxilinandeosin.
15 weeks
(A)
50 µm
(B)
17 weeks 18 weeks 19 weeks 20 weeks 5 months after birth
50 µm 50 µm 50 µm 50 µm 50 µm
50 µm 50 µm 50 µm 50 µm 50 µm 50 µm

10 of 12 | FRYE YEet al
suchasabluntedresponsetoTRHstimulation3anddifferencesinthediurnalvariationofthyroidhormonelevels.4Thesedatasuggestthatsimply using normal ranges to interpret levels of thyroid hormonesinchildrenwithASDmaynotcapturesubtleabnormalitiesinthyroidfunction.
Severalpreliminaryclinicalstudiesthathavesuggestedafavour-able response to thyroidhormonesupplementation inchildrenwithASD2,19,20andanimalmodelshavedemonstratedanimprovementinASD behaviours with T4 supplementation.55 Although thyroid hor-monesupplementationwouldappeartobecountertoourbehaviouraldataandthefactthatTT3andrT3wasfoundtobeabovenormalinahighpercentageofchildrenwithASD,itispossiblethatsuchsupple-mentationcouldreducevariationsintheHPA,leadingtoamorestableregulationofthyroidhormones. Interestingly,clinicalstudies inASDindividuals show a positive effect of propranolol, amedication thatblockstheconversionofT4toT3,therebypotentiallyprovidingben-efit inthosewithhighTT3orrT3concentrations.Indeed,inindivid-ualswithASD,propranololhasbeenshowntoimprovelanguage,56,57 cognitive flexibility,58 working memory,59 facial scanning60 and be-haviour.61,62Lithium,amedicationthat inhibitsthyroidfunction,hasbeenshowntohavepositiveeffectonASDbehavioursinseveralclin-ical63-65andanimalstudies,66therebyalsoindicatingarelativeoverac-tivityofthethyroidastheculprit.
Thefindingsofthepresentstudycouldguidefutureresearchstud-ies aiming to better understand the importance of thyroid functioninASD,suchthattheclinical implicationsofthethyroid inASDcanbebetterunderstood.First,itdoesappearthatthereisarelationshipbetweenFRAAsandthethyroid,withFRAAsmostlikelyaffectingthesensitivityoftheHPA,probablyatthelevelofthethyroid.TherealsoappearstobearelativelyincreasedexpressionoftheFRαduringpre-nataldevelopment,suggestingthattheeffectsofFRAAsmaybemostsignificant before birth.Additionally, data reportedwithin the pres-entstudysuggestthatvariationsinthyroidfunctiondoindeedhaveaneffectonthebehaviourofchildrenwithASD,althoughtheexactmechanismforthisinfluenceinnotclear.WeconsiderthatitmightbewiseforfurtherresearchtoconcentrateontheHPAwithrespecttothethyroidandfocusonthedynamicchangesinthyroidhormonesatbaseline,aswellasontreatmentsthataffectthethyroid.
Inconclusion,thepresentstudyhashelpeddefinetheimportanceof thyroid function inASD and the effect of the FRAA on thyroidfunction inASD. It appears that foetal exposure toblockingFRAAscouldaffect thedevelopmentof the thyroid,potentiallymaking thethyroid less sensitive toTSH. TSH and the ratio of hormones pro-ducedbythethyroidtoTSHappeartoberelatedtoASDbehaviour,implicatingdysregulationoftheHPA,althoughtheexactsignificanceof thesefindingswill require furtherclinicalstudywith largerpopu-lations. Overall the present study highlights the importance of theFRAAsandthyroidfunction,bothtogetherandseparately,inASDandtheneedforfurtherclinicalstudiestobetterunderstandhowtargetedtherapeutic interventions can help improve the lives of individualswithASDandtheirfamilies.ThesefindingsmayalsobeapplicabletootherdisordersassociatedwithFRAAs,suchasschizophrenia67 and subfertility.68
ACKNOWLEDGEMENTS
The present study was supported, in part, by funding from theArkansas Biosciences Institute, Autism Research Institute, the JaneBotsfordJohnsonFoundationandAutismSpeaksgrant#8202.HumanfoetalthyroidtissuewasprovidedbytheUniversityofMarylandBrainandTissueBank,whichisaBrainandTissueRepositoryoftheNIHNeuroBioBank.
CONFLICT OF INTERESTS
DrsFryeandQuadros areon theScientificAdvisoryBoardof IliadNeurosciencesInc.(PlymouthMeeting,PA).Twooftheauthors(JMSandEVQ)areinventorsonaUSpatentforthedetectionofFRautoan-tibodiesissuedtotheResearchFoundationoftheStateUniversityofNewYork.Theotherauthorsdeclarethattheyhavenoconflictsofinterest.
AUTHOR CONTRIBUTIONS
REF, RW, SR, JS, LD,MT, SCB, SM, JMS and EVQ performed theresearch.REF,SR,JS,LDandEVQdesignedtheresearchstudy.REF,LDandEVQanalysedthedata.REF,SR,JS,LD,SGK,JMSandEVQwrotethepaper.
REFERENCES
1. BrownRS.Disordersof thethyroidgland in infancy,childhoodandadolescence. In:DeGrootLJ,ChrousosG,DunganK,FeingoldKR,GrossmanA,HershmanJM,etal.,eds.Endotext.SouthDartmouth,MA:MDText.com,Inc.;2000.
2. SherwinAC, Flach FF, Stokes PE. Treatment of psychoses in earlychildhood with trilodothyronine. Am J Psychiatry. 1958;115: 166-167.
3. Hashimoto T, Aihara R, Tayama M, Miyazaki M, Shirakawa Y,Kuroda Y. Reduced thyroid-stimulating hormone response tothyrotropin-releasinghormoneinautisticboys.Dev Med Child Neurol. 1991;33:313-319.
4. Nir I,MeirD,ZilberN,KnoblerH,HadjezJ, LernerY.Brief report:circadianmelatonin,thyroid-stimulatinghormone,prolactin,andcor-tisollevelsinserumofyoungadultswithautism.J Autism Dev Disord. 1995;25:641-654.
5. GillbergIC,GillbergC,KoppS.Hypothyroidismandautismspectrumdisorders.J Child Psychol Psychiatry.1992;33:531-542.
6. HoshikoS,GretherJK,WindhamGC,SmithD,FesselK.Arethyroidhormoneconcentrationsatbirthassociatedwithsubsequentautismdiagnosis?Autism Res.2011;4:456-463.
7. FryeRE,SequeiraJM,QuadrosEV,RossignolD.Folatereceptoralphaautoantibodiesmodulatethyroidfunctioninautismspectrumdisor-der. N Am J Med Sci.2014;7:53-56.
8. TamagnoG,FederspilG,MurialdoG.Clinicalanddiagnosticaspectsof encephalopathy associatedwith autoimmune thyroiddisease (orHashimoto’sencephalopathy).Intern Emerg Med.2006;1:15-23.
9. Griswold KS, Del Regno PA, Berger RC. Recognition and differ-ential diagnosis of psychosis in primary care. Am Fam Physician. 2015;91:856-863.
10. HazenEP,SherryNA,ParangiS,RabitoCA,SadowPM.CaserecordsoftheMassachusettsGeneralHospital.Case10-2015.A15-year-oldgirl with Graves’ disease and psychotic symptoms. N Engl J Med. 2015;372:1250-1258.

| 11 of 12FRYE YEet al
11. Bensenor IM,NunesMA, SanderDinizMF, Santos IS,BrunoniAR,LotufoPA.Subclinicalthyroiddysfunctionandpsychiatricdisorders:cross-sectionalresultsfromtheBrazilianStudyofAdultHealth(ELSA-Brasil).Clin Endocrinol (Oxf). 2015;Jan 12. doi: 10.1111/cen.12719.[Epubaheadofprint].
12. Bove KB,WattT,VogelA, et al.Anxiety and depression aremoreprevalentinpatientswithgraves’diseasethaninpatientswithnodu-largoitre.Eur Thyroid J.2014;3:173-178.
13. CoboJ,Gimenez-PalopO,PatroE,etal.Lackofconfirmationofthy-roidendophenotypeinBipolarDisorderTypeIandtheirfirst-degreerelatives.Psychoneuroendocrinology.2015;51:351-364.
14. DegnerD,HaustM,MellerJ,RutherE,ReulbachU.Associationbe-tweenautoimmunethyroiditisanddepressivedisorderinpsychiatricoutpatients.Eur Arch Psychiatry Clin Neurosci. 2015;265:67-72.
15. HuLY,ShenCC,HuYW,etal.Hyperthyroidismandriskforbipolardisor-ders:anationwidepopulation-basedstudy.PLoS ONE.2013;8:e73057.
16. BicikovaM,HamplR,HillM,RipovaD,MohrP,PutzZ.Neuro-andimmunomodulatorysteroidsandotherbiochemicalmarkersindrug-naiveschizophreniapatientsandtheeffectoftreatmentwithatypicalantipsychotics.Neuro Endocrinol Lett.2011;32:141-147.
17. EatonWW, ByrneM, EwaldH, et al.Association of schizophreniaandautoimmunediseases:linkageofDanishnationalregisters.Am J Psychiatry.2006;163:521-528.
18. RovetJF.The roleof thyroidhormones for braindevelopment andcognitivefunction.Endocr Dev.2014;26:26-43.
19. Campbell M, Hollander CS, Ferris S, Greene LW. Response tothyrotropin-releasing hormone stimulation in young psychotic chil-dren:apilotstudy.Psychoneuroendocrinology.1978;3:195-201.
20. CampbellM, SmallAM,HollanderCS, et al.A controlled crossoverstudyoftriiodothyronineinautisticchildren.J Autism Child Schizophr. 1978;8:371-381.
21. KhanAA.Thyroiddysfunction.Br Med J. 1970;4:495.22. Abbassi V, Linscheid T, ColemanM. Triiodothyronine (T3) concen-
tration and therapy in autistic children. J Autism Child Schizophr. 1978;8:383-387.
23. CohenDJ,YoungJG,LoweTL,HarcherikD.Thyroidhormoneinautis-ticchildren.J Autism Dev Disord. 1980;10:445-450.
24. Molloy CA, Morrow AL, Meinzen-Derr J, et al. Familial autoim-munethyroiddiseaseasariskfactorforregressioninchildrenwithAutism Spectrum Disorder: a CPEA Study. J Autism Dev Disord. 2006;36:317-324.
25. FryeRE,SequeiraJM,QuadrosEV,JamesSJ,RossignolDA.Cerebralfolate receptor autoantibodies in autism spectrum disorder. Mol Psychiatry.2013;18:369-381.
26. MantovaniLT,MiottiS,MenardS,etal.Folatebindingproteindis-tribution in normal tissues and biological fluids fromovarian carci-nomapatientsasdetectedbythemonoclonalantibodiesMOv18andMOv19. Eur J Cancer (Oxford, England: 1990).1994;30A:363-369.
27. Weitman SD,WeinbergAG, Coney LR, ZurawskiVR, Jennings DS,KamenBA.Cellularlocalizationofthefolatereceptor:potentialroleindrugtoxicityandfolatehomeostasis.Cancer Res. 1992;52:6708-6711.
28. WeitmanSD,LarkRH,ConeyLR,etal.Distributionofthefolatere-ceptorGP38 innormal andmalignant cell linesand tissues.Cancer Res.1992;52:3396-3401.
29. WollackJB,MakoriB,AhlawatS,etal.Characterizationoffolateup-takebychoroidplexusepithelialcellsinaratprimaryculturemodel.J Neurochem.2008;104:1494-1503.
30. RamaekersVT,RothenbergSP,SequeiraJM,etal.Autoantibodiestofolatereceptorsinthecerebralfolatedeficiencysyndrome.N Engl J Med.2005;352:1985-1991.
31. FryeRE.Centraltetrahydrobiopterinconcentrationinneurodevelop-mentaldisorders.Front Neurosci. 2010;4:52.
32. FryeRE,DeLatorreR,TaylorHB,etal.Metaboliceffectsofsaprop-terin treatment in autism spectrum disorder: a preliminary study.Transl Psychiatry.2013;3:e237.
33. Frye RE, Huffman LC, Elliott GR. Tetrahydrobiopterin as a noveltherapeutic intervention for autism. Neurotherapeutics. 2010;7: 241-249.
34. FryeRE,JamesSJ.Metabolicpathologyofautisminrelationtoredoxmetabolism.Biomark Med.2014;8:321-330.
35. BurrowGN,FisherDA,LarsenPR.Maternalandfetalthyroidfunc-tion.N Engl J Med.1994;331:1072-1078.
36. deEscobarGM,ObregonMJ,delReyFE.Maternalthyroidhormonesearly in pregnancy and fetal braindevelopment.Best Pract Res Clin Endocrinol Metab. 2004;18:225-248.
37. Ramaekers VT, Quadros EV, Sequeira JM. Role of folate recep-tor autoantibodies in infantile autism. Mol Psychiatry. 2013;18: 270-271.
38. Frye RE, Slattery J, Delhey L, et al. Folinic acid improves verbalcommunication in children with autism and language impairment:a randomized double-blind placebo-controlled trial.Mol Psychiatry. 2016;Oct18.doi:10.1038/mp.2016.168.[Epubaheadofprint].
39. FalkmerT,AndersonK,FalkmerM,HorlinC.Diagnosticproceduresinautismspectrumdisorders:asystematicliteraturereview.Eur Child Adolesc Psychiatry.2013;22:329-340.
40. MolloyAM,QuadrosEV,SequeiraJM,etal.Lackofassociationbe-tweenfolate-receptorautoantibodiesandneural-tubedefects.N Engl J Med.2009;361:152-160.
41. Demers LM, Spencer CA. Laboratorymedicine practice guidelines:laboratory support for thediagnosisandmonitoringof thyroiddis-ease.Clin Endocrinol (Oxf).2003;58:138-140.
42. SadasivanE,RegecA,RothenbergSP.Thehalf-lifeofthetranscriptencodingthefolatereceptoralphainKBcellsisreducedbycytosolicproteinsexpressedinfolate-repleteandnotinfolate-depletedcells.Gene. 2002;291:149-158.
43. MelnykS,PogribnaM,Pogribny I,HineRJ,JamesSJ.AnewHPLCmethodforthesimultaneousdeterminationofoxidizedandreducedplasma aminothiols using coulometric electrochemical detection. J Nutr Biochem. 1999;10:490-497.
44. SparrowS,CicchettiD,BallaD.VinelandAdaptiveBehaviorScales2nded.Bloomington,MN,USA:PearsonAssessments;2005.
45. AmanMG,SinghNN,StewartAW,FieldCJ.Theaberrantbehaviorchecklist:abehaviorratingscalefortheassessmentoftreatmentef-fects.Am J Ment Defic. 1985;89:485-491.
46. KaatAJ, Lecavalier L,AmanMG.Validity of the aberrant behaviorchecklist in children with autism spectrum disorder. J Autism Dev Disord.2014;44:1103-1116.
47. FryeRE,SlatteryJ,MacFabeDF,etal.Approaches tostudyingandmanipulating theentericmicrobiome to improveautismsymptoms.Microb Ecol Health Dis. 2015;26:26878.
48. Constantino JN. The Social Responsiveness Scale. Los Angeles, CA:WesternPsychologicalServices;2002.
49. MurrayMJ,MayesSD,SmithLA.Brief report:excellentagreementbetween two brief autism scales (Checklist for Autism SpectrumDisorderandSocialResponsivenessScale)completedindependentlybyparentsandtheAutismDiagnosticInterview-Revised.J Autism Dev Disord. 2011;41:1586-1590.
50. DesaiA, Sequeira JM,Quadros EV.Themetabolic basis for devel-opmental disorders due to defective folate transport. Biochimie. 2016;126:31-42.
51. SequeiraJM,DesaiA,Berrocal-ZaragozaMI,MurphyMM,Fernandez-BallartJD,QuadrosEV.Exposuretofolatereceptoralphaantibodiesduringgestationandweaning leads to severebehavioraldeficits inrats:apilotstudy.PLoS ONE. 2016;11:e0152249.
52. YangN,WangL,FinnellRH,etal.LevelsoffolatereceptorautoantibodiesinmaternalandcordbloodandriskofneuraltubedefectsinaChinesepopulation.Birth Defects Res A Clin Mol Teratol. 2016;106:685-695.
53. VoHD,SequeiraJM,QuadrosEV,SchwarzSM,PerenyiAR.Theroleoffolatereceptorautoantibodiesinpretermbirth.Nutrition (Burbank, Los Angeles County, Calif).2015;31:1224-1227.

12 of 12 | FRYE YEet al
54. BauerM,GoetzT, GlennT,WhybrowPC.The thyroid-brain inter-action in thyroid disorders and mood disorders. J Neuroendocrinol. 2008;20:1101-1114.
55. Tunc-OzcanE,UllmannTM,ShuklaPK,RedeiEE.Low-dosethyroxineattenuatesautism-associatedadverseeffectsoffetalalcoholinmaleoffspring’ssocialbehaviorandhippocampalgeneexpression.Alcohol Clin Exp Res.2013;37:1986-1995.
56. BeversdorfDQ,SaklayenS,HigginsKF,BodnerKE,KanneSM,ChristSE. Effect of propranolol on word fluency in autism. Cogn Behav Neurol. 2011;24:11-17.
57. NarayananA,WhiteCA,SaklayenS,etal.Effectofpropranololonfunctionalconnectivity inautismspectrumdisorder–apilotstudy.Brain Imaging Behav. 2010;4:189-197.
58. HechtPM,WillMJ,SchachtmanTR,WelbyLM,BeversdorfDQ.Beta-adrenergicantagonisteffectsonanovelcognitive flexibility task inrodents.Behav Brain Res. 2014;260:148-154.
59. Bodner KE, Beversdorf DQ, Saklayen SS, Christ SE. Noradrenergicmoderation ofworkingmemory impairments in adultswith autismspectrumdisorder.J Int Neuropsychol Soc. 2012;18:556-564.
60. ZamzowRM,ChristSE,SaklayenSS,etal.Effectofpropranololonfa-cialscanninginautismspectrumdisorder:apreliminaryinvestigation.J Clin Exp Neuropsychol.2014;36:431-445.
61. Deepmala,AgrawalM.Useofpropranololforhypersexualbehaviorinanadolescentwithautism.Ann Pharmacother.2014;48:1385-1388.
62. LuiselliJK,BlewP,KeaneJ,ThibadeauS,HolzmanT.Pharmacotherapyforsevereaggressioninachildwithautism:‘openlabel’evaluationofmultiplemedicationsonresponsefrequencyandintensityofbehav-ioralintervention.J Behav Ther Exp Psychiatry.2000;31:219-230.
63. KerbeshianJ,BurdL,FisherW.Lithiumcarbonateinthetreatmentoftwopatientswithinfantileautismandatypicalbipolarsymptomatol-ogy.J Clin Psychopharmacol. 1987;7:401-405.
64. SiegelM, Beresford CA, BunkerM, et al. Preliminary investigationof lithiumformooddisordersymptoms inchildrenandadolescentswith autism spectrum disorder. J Child Adolesc Psychopharmacol. 2014;24:399-402.
65. SteingardR,BiedermanJ.Lithiumresponsivemanic-likesymptomsintwoindividualswithautismandmentalretardation.J Am Acad Child Adolesc Psychiatry.1987;26:932-935.
66. WuX,BaiY,TanT,etal.Lithiumamelioratesautistic-likebehaviorsin-ducedbyneonatalisolationinrats.Front Behav Neurosci.2014;8:234.
67. RamaekersVT,ThonyB,SequeiraJM,etal.Folinicacidtreatmentforschizophrenia associated with folate receptor autoantibodies.Mol Genet Metab.2014;113:307-314.
68. Berrocal-ZaragozaMI, Fernandez-Ballart JD,MurphyMM, Cavalle-BusquetsP,SequeiraJM,QuadrosEV.Associationbetweenblockingfolatereceptorautoantibodiesandsubfertility.Fertil Steril. 2009;91(4 suppl):1518-1521.
How to cite this article:FryeRE,WynneR,RoseS,etal.Thyroiddysfunctioninchildrenwithautismspectrumdisorderisassociatedwithfolatereceptorαautoimmunedisorder.J Neuroendocrinol.2017:29:1-12.https://doi.org/10.1111/jne.12461
View publication statsView publication stats