Thyroid Ct Scan
11
AJR:187, November 2006 1349 AJR 2006; 187:1349–1356 0361–803X/06/1875–1349 © American Roentgen Ray Society M E D I C A L I M A G I N G A C E N T U R Y O F M E D I C A L I M A G I N G A C E N T U R Y O F Shetty et al. CT of Incidental Thyroid Lesions Head and Neck Imaging • Original Research Significance of Incidental Thyroid Lesions Detected on CT: Correlation Among CT, Sonography, and Pathology Sanjay K. Shetty 1,2 Michael M. Maher 1 Peter F. Hahn 1 Elkan F. Halpern 1 Suzanne L. Aquino 1 Shetty SK, Maher MM, Hahn PF, Halpern EF, Aquino SL Keywords: CT, head and neck imaging, sonography, thyroid gland DOI:10.2214/AJR.05.0468 Received March 17, 2005; accepted after revision October 10, 2005. 1 Department of Radiology, Massachusetts General Hospital, FND 214, 55 Fruit St., Boston, MA 02114. 2 Present address: Department of Radiology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., Boston, MA 02215. Address correspondence to S. K. Shetty ([email protected]). OBJECTIVE. The purpose of our study was to determine the prevalence of malignancy in incidental abnormalities of the thyroid gland detected on CT and to determine the relative accu- racy of characterizing these abnormalities on CT as compared with sonography and pathology. MATERIALS AND METHODS. We searched our department’s computerized clinical database for all thoracic and cervical CT scans in which a new abnormality was incidentally iden- tified in the thyroid gland from 1998–2001. Two hundred thirty patients with abnormal findings in the gland on CT subsequently underwent thyroid sonography, and 118 of the 230 patients un- derwent a diagnostic biopsy or resection. CT and sonographic images were directly reviewed to identify imaging features of each thyroid abnormality, including the location, size, appearance, and presence or absence of calcifications. Associations were evaluated using Fisher’s exact test of significance and the Student’s t test. The overall rate of malignant and potentially malignant lesions among these incidental abnormalities of the thyroid gland was calculated. RESULTS. CT findings matched the sonographic characterization in 122 patients (53.0%), correctly identified the dominant nodule but missed multinodularity in 69 (30.0%) patients, and underestimated the number of nodules in 24 (10.4%) patients. CT overestimated the number of nodules in 5 (2.2%) patients and was false-positive for lesions in 10 patients (4.3%). Ninety- one patients with a single or dominant nodule on CT had pathologic correlation: 7 nodules were malignant, 17 showed malignant potential, and 67 were benign. Of 27 patients with multinod- ular or enlarged thyroid glands on CT and histopathologic correlation, 2 lesions were malignant and 25 benign. The presence of punctate calcifications on CT significantly correlated to the presence of microcalcifications on sonography (p < 0.02). Benign nodules were significantly smaller (mean, 2.16 ± 1.01 cm; range, 0.6–4.5 cm) than malignant and potentially malignant nodules (mean, 2.79 ± 0.99 cm; range, 0.7–4.6 cm) (p = 0.01). Patients 35 years or younger who had a thyroid lesion on CT were more likely to have malignancy (p < 0.01). Overall, among incidentally detected lesions of the thyroid gland, there was at least a 3.9% rate of ma- lignancy (95% CI: 1.8–7.3%) and 7.4% rate of malignant potential (95% CI: 4.4–11.6%). CONCLUSION. There is at least an 11.3% prevalence of malignant or potentially malig- nant lesions among incidental thyroid abnormalities detected on CT. Patients 35 years or younger who have incidental abnormalities have a significantly greater rate of malignancy. No CT feature reliably distinguishes benign from malignant lesions in the thyroid gland. CT un- derestimates the number of nodules relative to sonography, which suggests that sonography is a useful adjunctive test after the incidental detection of a thyroid abnormality on CT. ncidental abnormalities of the thyroid gland are commonly en- countered by the radiologist, at a rate of 16% on cross-sectional imaging and 27% on sonography [1, 2]. Clinically detected thyroid nodules, includ- ing those detected on physical examination or because of patient symptoms, are benign in most patients (90–95%) [3]. The inciden- tally detected lesions of the thyroid found initially on cross-sectional imaging are a distinct and clinically silent group the sig- nificance of which is uncertain. The radiol- ogist encountering one of these lesions may use several strategies, ranging from recom- mending further imaging and clinical evalu- ation for every lesion to ignoring every le- sion. An appropriate management algorithm requires knowledge of the imaging and de- mographic features that may predict malig- nancy and the proportion of these lesions that may be malignant. I Downloaded from www.ajronline.org by 202.67.42.16 on 11/21/13 from IP address 202.67.42.16. Copyright ARRS. For personal use only; all rights reserved
-
Upload
aqsha-ramadhanisa -
Category
Documents
-
view
64 -
download
2
description
jurnal
Transcript of Thyroid Ct Scan
AJR:187, November 2006 1349
AJR 2006; 187:1349–1356
0361–803X/06/1875–1349
© American Roentgen Ray Society
M E D I C A L I M A G I N G
A C E N T U R Y O F
M E D I C A L I M A G I N G
A C E N T U R Y O F
Shetty et al.CT of Incidental Thyroid Lesions
H e a d a n d N e c k I m ag i n g • O r i g i n a l R e s e a rc h
Significance of Incidental Thyroid Lesions Detected on CT: Correlation Among CT, Sonography, and Pathology
Sanjay K. Shetty1,2
Michael M. Maher1
Peter F. Hahn1
Elkan F. Halpern1
Suzanne L. Aquino1
Shetty SK, Maher MM, Hahn PF, Halpern EF, Aquino SL
Keywords: CT, head and neck imaging, sonography, thyroid gland
DOI:10.2214/AJR.05.0468
Received March 17, 2005; accepted after revision October 10, 2005.
1Department of Radiology, Massachusetts General Hospital, FND 214, 55 Fruit St., Boston, MA 02114.
2Present address: Department of Radiology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., Boston, MA 02215. Address correspondence to S. K. Shetty ([email protected]).
OBJECTIVE. The purpose of our study was to determine the prevalence of malignancy inincidental abnormalities of the thyroid gland detected on CT and to determine the relative accu-racy of characterizing these abnormalities on CT as compared with sonography and pathology.
MATERIALS AND METHODS. We searched our department’s computerized clinicaldatabase for all thoracic and cervical CT scans in which a new abnormality was incidentally iden-tified in the thyroid gland from 1998–2001. Two hundred thirty patients with abnormal findingsin the gland on CT subsequently underwent thyroid sonography, and 118 of the 230 patients un-derwent a diagnostic biopsy or resection. CT and sonographic images were directly reviewed toidentify imaging features of each thyroid abnormality, including the location, size, appearance,and presence or absence of calcifications. Associations were evaluated using Fisher’s exact testof significance and the Student’s t test. The overall rate of malignant and potentially malignantlesions among these incidental abnormalities of the thyroid gland was calculated.
RESULTS. CT findings matched the sonographic characterization in 122 patients (53.0%),correctly identified the dominant nodule but missed multinodularity in 69 (30.0%) patients, andunderestimated the number of nodules in 24 (10.4%) patients. CT overestimated the numberof nodules in 5 (2.2%) patients and was false-positive for lesions in 10 patients (4.3%). Ninety-one patients with a single or dominant nodule on CT had pathologic correlation: 7 nodules weremalignant, 17 showed malignant potential, and 67 were benign. Of 27 patients with multinod-ular or enlarged thyroid glands on CT and histopathologic correlation, 2 lesions were malignantand 25 benign. The presence of punctate calcifications on CT significantly correlated to thepresence of microcalcifications on sonography (p < 0.02). Benign nodules were significantlysmaller (mean, 2.16 ± 1.01 cm; range, 0.6–4.5 cm) than malignant and potentially malignantnodules (mean, 2.79 ± 0.99 cm; range, 0.7–4.6 cm) (p = 0.01). Patients 35 years or youngerwho had a thyroid lesion on CT were more likely to have malignancy (p < 0.01). Overall,among incidentally detected lesions of the thyroid gland, there was at least a 3.9% rate of ma-lignancy (95% CI: 1.8–7.3%) and 7.4% rate of malignant potential (95% CI: 4.4–11.6%).
CONCLUSION. There is at least an 11.3% prevalence of malignant or potentially malig-nant lesions among incidental thyroid abnormalities detected on CT. Patients 35 years oryounger who have incidental abnormalities have a significantly greater rate of malignancy. NoCT feature reliably distinguishes benign from malignant lesions in the thyroid gland. CT un-derestimates the number of nodules relative to sonography, which suggests that sonography isa useful adjunctive test after the incidental detection of a thyroid abnormality on CT.
ncidental abnormalities of thethyroid gland are commonly en-countered by the radiologist, at arate of 16% on cross-sectional
imaging and 27% on sonography [1, 2].Clinically detected thyroid nodules, includ-ing those detected on physical examinationor because of patient symptoms, are benignin most patients (90–95%) [3]. The inciden-tally detected lesions of the thyroid foundinitially on cross-sectional imaging are a
distinct and clinically silent group the sig-nificance of which is uncertain. The radiol-ogist encountering one of these lesions mayuse several strategies, ranging from recom-mending further imaging and clinical evalu-ation for every lesion to ignoring every le-sion. An appropriate management algorithmrequires knowledge of the imaging and de-mographic features that may predict malig-nancy and the proportion of these lesionsthat may be malignant.
I
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

Shetty et al.
1350 AJR:187, November 2006
The purpose of this study was to determinethe prevalence of malignancy in these inci-dental abnormalities of the thyroid gland de-tected on CT and to correlate CT with sonog-raphy and pathology results to determine ifany CT appearance distinguishes malignantfrom benign lesions.
Materials and MethodsThis study was approved by our institution’s hu-
man subjects research committee and was con-ducted in a manner compliant with the Health In-surance Portability and Accountability Act of 1996(HIPAA). We searched our department’s computer-ized clinical database for all thoracic and cervicalCT scans in which a new abnormality was inciden-tally identified in the thyroid gland from 1998 to2001. A second list of all diagnostic thyroid sono-graphic examinations was then created, includingexaminations from 1998 to 2001 inclusive, plus thefirst 6 months of 2002. A list of patients whose firstthyroid sonographic examination was scheduled af-ter the CT was then extracted from the combinationof both lists, yielding 358 patients. One hundredtwenty-eight patients were excluded because theinitial CT was prompted by a suspected abnormal-ity of the thyroid gland or because the requisition ora detailed chart review revealed a history of thyroiddisease, thyroid cancer, or surgery. This yielded afinal study population of 230 patients (159 womenand 71 men; mean age, 64.5 ± 14.1 years; range,29–94 years).
All CT examinations were performed withHiSpeed or LightSpeed scanners (GE Healthcare).Scans were obtained at 2.5- to 5-mm collimationthroughout the neck or thorax with or without con-trast administration. In contrast-enhanced studies,100 mL of nonionic contrast medium was adminis-tered IV using a power injector. Sonography of thethyroid gland was performed after CT, with a meandelay of 97 days (range, 0–1,167 days) between thetwo examinations. Sonography was performed witha Logiq sonography machine (GE Healthcare) us-ing a high-frequency linear transducer.
Image AnalysisAll CT and sonography studies were retrospec-
tively reviewed by a radiologist who was blinded tothe results of the other imaging technique and of pa-thology. CT was reviewed on a PACS workstation(IMPAX RS 3000 1K review station, AGFA Techni-cal Imaging Systems). On CT, each thyroid glandwas characterized as having a single nodule, multi-ple nodules with or without a dominant nodule, ordiffuse enlargement with or without a dominant nod-ule. The dominant lesion in each thyroid gland wasfurther assessed for size (maximum axial dimen-sion), location, density (qualitatively in relation to
normal thyroid parenchyma and quantitatively usinga region of interest centered in the lesion), the pres-ence or absence of calcification, margins, and con-sistency (i.e., homogeneous vs heterogeneous).
The sonographic features of the entire gland andthe dominant nodule were similarly reviewed on aPACS workstation. The appearance of the entiregland was characterized as enlarged, heterogeneouswithout a dominant nodule, multinodular, singlenodule, or normal. When a dominant nodule waspresent, multiple imaging features were noted, in-cluding size, location, solid versus cystic appear-ance, homogeneity versus heterogeneity, echoge-nicity relative to thyroid parenchyma, nature of themargins, and the presence or absence of microcal-cifications. Doppler flow characteristics were re-corded in only a small fraction of sonographic stud-ies and were therefore not included in the analysis.
Pathologic correlation was available in 118 pa-tients. Tissue samples were obtained through surgery,percutaneous fine-needle aspiration, or percutaneouscore needle biopsy. Particular attention was paid tothe location of the biopsy or surgical specimen to en-sure that the pathologic results were derived from thesame lesion identified on imaging. Lesions were des-ignated as benign (macrofollicular adenoma, mixedbut predominantly macrofollicular, colloid cyst, oradenomatous goiter), malignant (carcinoma or lym-phoma), or potentially malignant (microfollicular ormixed but predominantly microfollicular) [4–6]. Le-sions with nondiagnostic biopsy results were catego-rized as not having pathologic correlation unless asubsequent biopsy was diagnostic.
Data AnalysisStatistical analysis of the results was performed
with commercially available statistical software(SPSS version 11.0). The Fisher’s exact test wasused for the following analyses: to determine if anyfeature on CT correlated with sonographic find-ings, to determine if any feature on CT correlatedwith benign or malignant pathology, and to deter-mine if patient demographics (i.e., sex or age) cor-responded to malignancy. A two-tailed p value ofless than 0.05 was considered significant. Signifi-cant associations between two means (as in the caseof nodule size) was assessed using the Student’s ttest of two samples with unequal variance (het-eroscedastic). The overall percentage of malignantor potentially malignant lesions among these inci-dentally detected thyroid abnormalities was thencalculated, using as a denominator for the calcula-tion the total study population of 230 patients.
ResultsCT Appearance of Incidental Abnormalities
On CT, of 230 patients, 141 patients had asingle dominant nodule, 24 had a multinodu-
lar gland with a single dominant nodule, 43had a multinodular gland without a dominantnodule, 5 patients had a diffusely enlargedgland with a dominant nodule, and 17 had adiffusely enlarged gland without a dominantnodule (Table 1).
Dominant nodules were seen on CT in 170patients, distributed evenly between lobes (left,right, and isthmus: 84, 83, and 3, respectively)but more commonly in the lower pole (lower,
TABLE 1: CT Features of Incidentally Detected Thyroid Lesions
Appearance No. (%)
Thyroid gland (n = 230 patients)
Enlarged with dominant nodule 5 (2.2)
Enlarged without dominant nodule 17 (7.4)
Multinodular with dominant nodule 24 (10.4)
Multinodular without dominant nodule
43 (18.7)
Single dominant nodule 141 (61.3)
Dominant nodule (n = 170 nodules)
Location (lobe)
Left 84 (49.4)
Right 83 (48.8)
Isthmus 3 (1.8)
Location (within lobe)
Lower 93 (54.7)
Middle 60 (35.3)
Upper 12 (7.1)
Isthmus 3 (1.8)
Entire lobe 2 (1.2)
Punctuate calcifications
Present 21 (12.4)
Absent 149 (87.6)
Density (relative to thyroid parenchyma)
Hypodense 71 (41.8)
Isodense 28 (16.5)
Hyperdense 13 (7.6)
Heterogeneous 56 (32.9)
Densely calcified 2 (1.2)
Margins
Well circumscribed 162 (95.3)
Ill defined 8 (4.7)
Size
Average (cm) 2.09
Range (cm) 0.4–4.6
Density
Range (H) 2–221
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
CT of Incidental Thyroid Lesions
AJR:187, November 2006 1351
middle, and upper: 93, 60, and 12, with 3 in theisthmus and 2 involving the entire lobe). OnCT, the average size in the axial plane of thedominant nodule was 2.09 ± 1.02 cm (range,0.4–4.6 cm). In terms of relative density of thedominant nodule, 71 nodules were hypodense,28 were isodense, 13 were hyperdense, 56were heterogeneous, and 2 were calcified.Twenty-one nodules (12.4%) had punctate cal-cifications visible on CT (Table 1).
Correlation of CT and SonographyAn abnormality of the thyroid gland on
CT correlated with an abnormality on subse-quent sonography in 220 patients (95.7%).CT matched the sonographic characteriza-tion in 122 cases (53.0%), correctly identi-fied the dominant nodule but missed multi-nodularity in 69 (30.0%) patients, and
underestimated the number of nodules in 24(10.4%) patients. CT overestimated thenumber of nodules in 5 (2.2%) patients. Inthe remaining 10 patients (4.3%), the thyroidgland was normal on sonography.
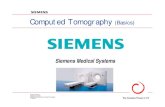
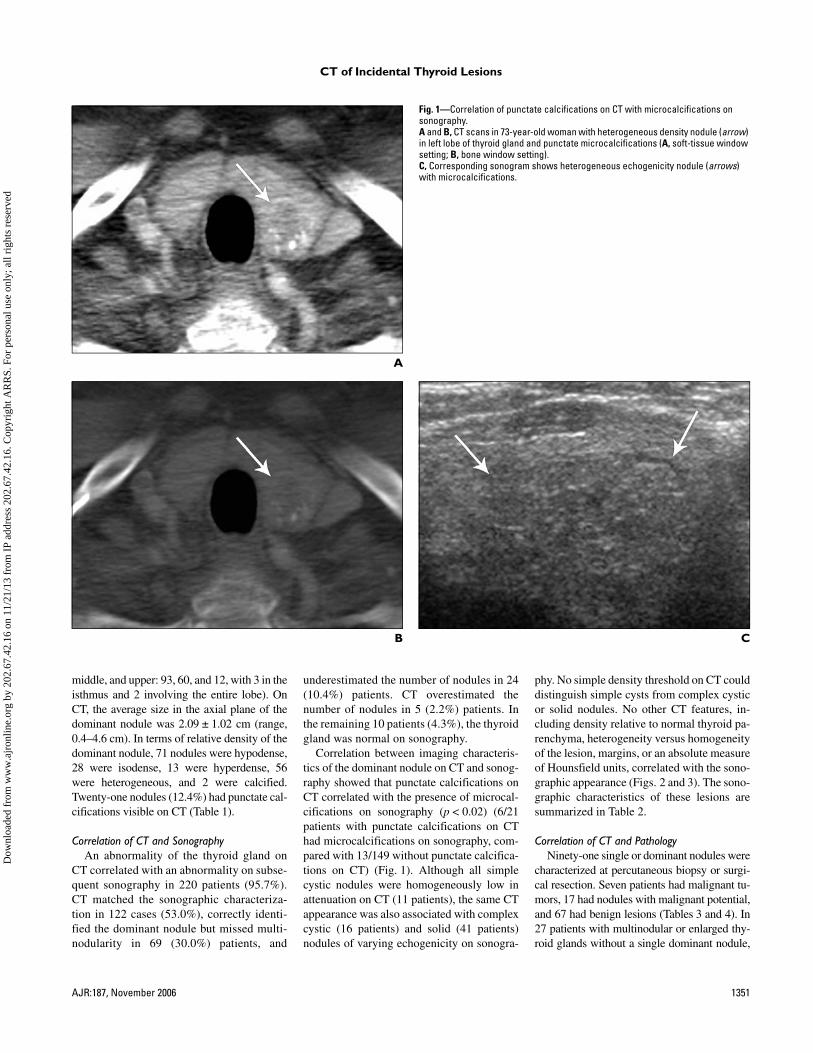
Correlation between imaging characteris-tics of the dominant nodule on CT and sonog-raphy showed that punctate calcifications onCT correlated with the presence of microcal-cifications on sonography (p < 0.02) (6/21patients with punctate calcifications on CThad microcalcifications on sonography, com-pared with 13/149 without punctate calcifica-tions on CT) (Fig. 1). Although all simplecystic nodules were homogeneously low inattenuation on CT (11 patients), the same CTappearance was also associated with complexcystic (16 patients) and solid (41 patients)nodules of varying echogenicity on sonogra-
phy. No simple density threshold on CT coulddistinguish simple cysts from complex cysticor solid nodules. No other CT features, in-cluding density relative to normal thyroid pa-renchyma, heterogeneity versus homogeneityof the lesion, margins, or an absolute measureof Hounsfield units, correlated with the sono-graphic appearance (Figs. 2 and 3). The sono-graphic characteristics of these lesions aresummarized in Table 2.
Correlation of CT and PathologyNinety-one single or dominant nodules were
characterized at percutaneous biopsy or surgi-cal resection. Seven patients had malignant tu-mors, 17 had nodules with malignant potential,and 67 had benign lesions (Tables 3 and 4). In27 patients with multinodular or enlarged thy-roid glands without a single dominant nodule,
A
Fig. 1—Correlation of punctate calcifications on CT with microcalcifications on sonography.A and B, CT scans in 73-year-old woman with heterogeneous density nodule (arrow) in left lobe of thyroid gland and punctate microcalcifications (A, soft-tissue window setting; B, bone window setting).C, Corresponding sonogram shows heterogeneous echogenicity nodule (arrows) with microcalcifications.
B C
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
Shetty et al.
1352 AJR:187, November 2006
pathology findings were benign in 25 patientsand malignant in two patients (Table 3).
Benign nodules (67 nodules; mean,2.16 ± 1.01 cm; range, 0.6–4.5 cm) were sig-nificantly smaller (p = 0.01) than malignantand potentially malignant nodules (23 nod-ules; mean, 2.79 ± 0.99 cm; range, 0.7–4.6cm). Nodules greater than 2.5 cm were morelikely to be malignant or potentially malig-nant (p = 0.03), with a sensitivity of 62.5%(15/24 malignant or potentially malignant
nodules were > 2.5 cm) and specificity of64.1% (43/67 benign nodules were ≤ 2.5 cm).
Other than size, no CT feature (of either theentire gland or of the dominant nodule) sig-nificantly correlated with benign or malignanthistopathologic results (Figs. 2 and 3). Nosignificant correlation was seen between ma-lignancy and the presence of punctate calcifi-cations in the lesion on CT (p = 0.72) (3/24malignant or potentially malignant nodulesand 7/67 benign nodules showed punctate cal-
A
B
C
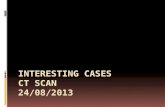
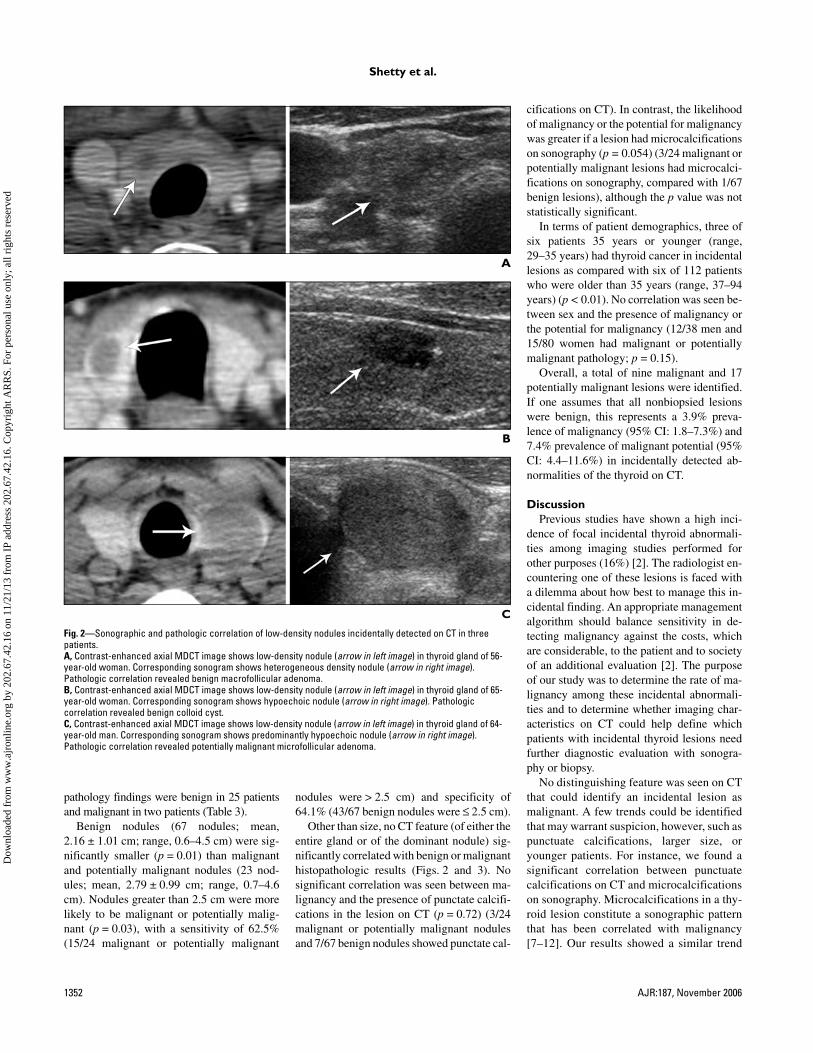
Fig. 2—Sonographic and pathologic correlation of low-density nodules incidentally detected on CT in three patients. A, Contrast-enhanced axial MDCT image shows low-density nodule (arrow in left image) in thyroid gland of 56-year-old woman. Corresponding sonogram shows heterogeneous density nodule (arrow in right image). Pathologic correlation revealed benign macrofollicular adenoma.B, Contrast-enhanced axial MDCT image shows low-density nodule (arrow in left image) in thyroid gland of 65-year-old woman. Corresponding sonogram shows hypoechoic nodule (arrow in right image). Pathologic correlation revealed benign colloid cyst.C, Contrast-enhanced axial MDCT image shows low-density nodule (arrow in left image) in thyroid gland of 64-year-old man. Corresponding sonogram shows predominantly hypoechoic nodule (arrow in right image). Pathologic correlation revealed potentially malignant microfollicular adenoma.
cifications on CT). In contrast, the likelihoodof malignancy or the potential for malignancywas greater if a lesion had microcalcificationson sonography (p = 0.054) (3/24 malignant orpotentially malignant lesions had microcalci-fications on sonography, compared with 1/67benign lesions), although the p value was notstatistically significant.
In terms of patient demographics, three ofsix patients 35 years or younger (range,29–35 years) had thyroid cancer in incidentallesions as compared with six of 112 patientswho were older than 35 years (range, 37–94years) (p < 0.01). No correlation was seen be-tween sex and the presence of malignancy orthe potential for malignancy (12/38 men and15/80 women had malignant or potentiallymalignant pathology; p = 0.15).
Overall, a total of nine malignant and 17potentially malignant lesions were identified.If one assumes that all nonbiopsied lesionswere benign, this represents a 3.9% preva-lence of malignancy (95% CI: 1.8–7.3%) and7.4% prevalence of malignant potential (95%CI: 4.4–11.6%) in incidentally detected ab-normalities of the thyroid on CT.
DiscussionPrevious studies have shown a high inci-
dence of focal incidental thyroid abnormali-ties among imaging studies performed forother purposes (16%) [2]. The radiologist en-countering one of these lesions is faced witha dilemma about how best to manage this in-cidental finding. An appropriate managementalgorithm should balance sensitivity in de-tecting malignancy against the costs, whichare considerable, to the patient and to societyof an additional evaluation [2]. The purposeof our study was to determine the rate of ma-lignancy among these incidental abnormali-ties and to determine whether imaging char-acteristics on CT could help define whichpatients with incidental thyroid lesions needfurther diagnostic evaluation with sonogra-phy or biopsy.
No distinguishing feature was seen on CTthat could identify an incidental lesion asmalignant. A few trends could be identifiedthat may warrant suspicion, however, such aspunctuate calcifications, larger size, oryounger patients. For instance, we found asignificant correlation between punctuatecalcifications on CT and microcalcificationson sonography. Microcalcifications in a thy-roid lesion constitute a sonographic patternthat has been correlated with malignancy[7–12]. Our results showed a similar trend
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
CT of Incidental Thyroid Lesions
AJR:187, November 2006 1353
A
B
C
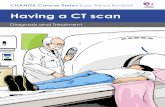
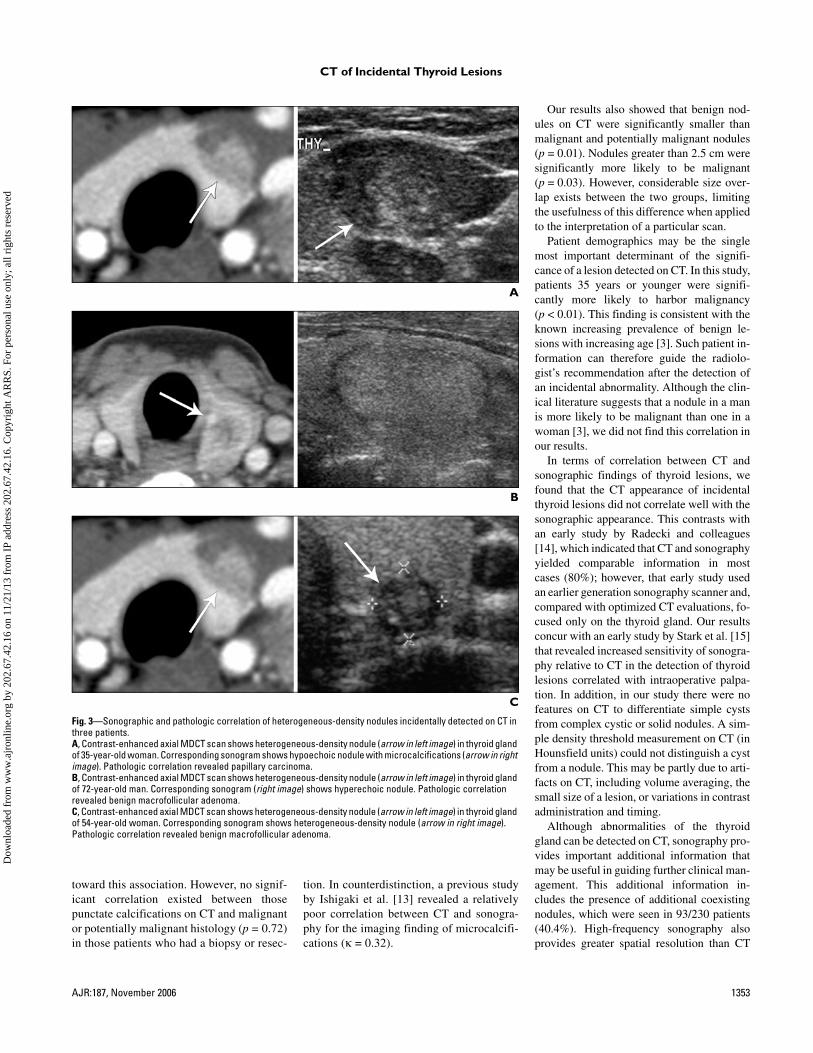
Fig. 3—Sonographic and pathologic correlation of heterogeneous-density nodules incidentally detected on CT in three patients.A, Contrast-enhanced axial MDCT scan shows heterogeneous-density nodule (arrow in left image) in thyroid gland of 35-year-old woman. Corresponding sonogram shows hypoechoic nodule with microcalcifications (arrow in right image). Pathologic correlation revealed papillary carcinoma.B, Contrast-enhanced axial MDCT scan shows heterogeneous-density nodule (arrow in left image) in thyroid gland of 72-year-old man. Corresponding sonogram (right image) shows hyperechoic nodule. Pathologic correlation revealed benign macrofollicular adenoma.C, Contrast-enhanced axial MDCT scan shows heterogeneous-density nodule (arrow in left image) in thyroid gland of 54-year-old woman. Corresponding sonogram shows heterogeneous-density nodule (arrow in right image). Pathologic correlation revealed benign macrofollicular adenoma.
toward this association. However, no signif-icant correlation existed between thosepunctate calcifications on CT and malignantor potentially malignant histology (p = 0.72)in those patients who had a biopsy or resec-
tion. In counterdistinction, a previous studyby Ishigaki et al. [13] revealed a relativelypoor correlation between CT and sonogra-phy for the imaging finding of microcalcifi-cations (κ = 0.32).
Our results also showed that benign nod-ules on CT were significantly smaller thanmalignant and potentially malignant nodules(p = 0.01). Nodules greater than 2.5 cm weresignificantly more likely to be malignant(p = 0.03). However, considerable size over-lap exists between the two groups, limitingthe usefulness of this difference when appliedto the interpretation of a particular scan.
Patient demographics may be the singlemost important determinant of the signifi-cance of a lesion detected on CT. In this study,patients 35 years or younger were signifi-cantly more likely to harbor malignancy(p < 0.01). This finding is consistent with theknown increasing prevalence of benign le-sions with increasing age [3]. Such patient in-formation can therefore guide the radiolo-gist’s recommendation after the detection ofan incidental abnormality. Although the clin-ical literature suggests that a nodule in a manis more likely to be malignant than one in awoman [3], we did not find this correlation inour results.
In terms of correlation between CT andsonographic findings of thyroid lesions, wefound that the CT appearance of incidentalthyroid lesions did not correlate well with thesonographic appearance. This contrasts withan early study by Radecki and colleagues[14], which indicated that CT and sonographyyielded comparable information in mostcases (80%); however, that early study usedan earlier generation sonography scanner and,compared with optimized CT evaluations, fo-cused only on the thyroid gland. Our resultsconcur with an early study by Stark et al. [15]that revealed increased sensitivity of sonogra-phy relative to CT in the detection of thyroidlesions correlated with intraoperative palpa-tion. In addition, in our study there were nofeatures on CT to differentiate simple cystsfrom complex cystic or solid nodules. A sim-ple density threshold measurement on CT (inHounsfield units) could not distinguish a cystfrom a nodule. This may be partly due to arti-facts on CT, including volume averaging, thesmall size of a lesion, or variations in contrastadministration and timing.
Although abnormalities of the thyroidgland can be detected on CT, sonography pro-vides important additional information thatmay be useful in guiding further clinical man-agement. This additional information in-cludes the presence of additional coexistingnodules, which were seen in 93/230 patients(40.4%). High-frequency sonography alsoprovides greater spatial resolution than CT
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
Shetty et al.
1354 AJR:187, November 2006
and affords improved evaluation of nodule ar-chitecture and consistency. Current manage-ment of multinodular glands, although stilldebated, emphasizes that the decision shouldbe based on the sonographic features of eachnodule [16]. Therefore, knowledge of addi-tional nodules may influence the decision tobiopsy. Our findings are concordant with pre-viously published data that suggest thatsonography is preferable for the evaluation ofsolid-component homogeneity [13]. In addi-tion, published recommendations suggest thatsimple cystic lesions do not require biopsy [3,16]. In a small minority of patients (10 pa-tients), the subsequent sonographic examina-tion showed normal findings; in those cases,the apparent CT abnormality was either in-correctly characterized as an abnormality onCT (because of an adjacent structure or mis-interpretation of a contour irregularity as anodule) or inaccessible to sonography (be-cause of a substernal location).
Sonography also provides better accuracythan CT in measuring lesions in the thyroidgland. The overall trend of increasing concernfor malignancy in larger lesions is echoed in theSociety of Radiologists in Ultrasound (SRU)consensus statement on thyroid nodules [16],which uses a graded threshold for considerationof thyroid nodules based on size and sono-graphic characteristics. Using this scheme, thesmallest nodules (≥ 1.0 cm) require a strongsonographic feature of malignancy (microcal-cifications), whereas larger lesions (≥ 2.0 cm)can have less concerning features (mixed solidand cystic or predominantly cystic) to considerbiopsy. The absence of a distinct size thresholdto differentiate benign from malignant, as wellthe possibility of malignancy in lesions evensmaller than 1.0 cm, is consistent with a studyby Papini et al. [17] in which an equal fre-quency of malignancy was observed in nodulesgreater than and those less than 10 mm as mea-sured on sonography.
In our calculation of the overall rate of ma-lignant and potentially malignant lesions, weassumed that all nonbiopsied lesions were be-nign, and we used the total number of patientsin the series as a denominator in the calculationof the prevalence of malignancy among inci-dental thyroid lesions. This method counteredthe potential bias of considering only lesionsthat were biopsied, which would have likelyrepresented a highly selected group with amuch greater expectation of malignancy. Infact, many of the patients who did not undergobiopsy may have been lost to follow-up or hadan evaluation elsewhere; those patients werecounted as having benign lesions, although aportion of them may have harbored malignantor potentially malignant lesions. This possibil-ity suggests that our calculation may underes-timate the true prevalence of malignant orpotentially malignant lesions among the inci-dentally detected abnormalities of the thyroidgland detected on CT.
Despite the assumption made in our calcu-lation, we identified a surprisingly high num-ber of malignant or potentially malignant le-sions among incidental abnormalities initiallydetected on CT. This relatively high fractionnecessitates careful consideration of furtherimaging or evaluation in all patients in whomincidental lesions are detected. The presence ofmalignancy in two patients with apparent mul-tifocal abnormalities of the thyroid gland onCT further indicates that even a multinodulargland necessitates further evaluation [17]. Therate of malignant and potentially malignant le-sions stands in distinction to the complete ab-
sence of malignant or potentially malignant le-sions in the series described by Yousem et al.[2], although their series included pathologiccorrelation in only four of 36 patients. In con-trast, previous studies of “incidental” lesions ofthe thyroid on sonography have actually beenbased on selected referral populations initiallyreferred for a finding on sonography; thosestudies have revealed malignancy rates of 12%[18] and 28.8% [12].
Our study has several limitations based pri-marily on its retrospective design. It is impos-sible to draw conclusions about patients who
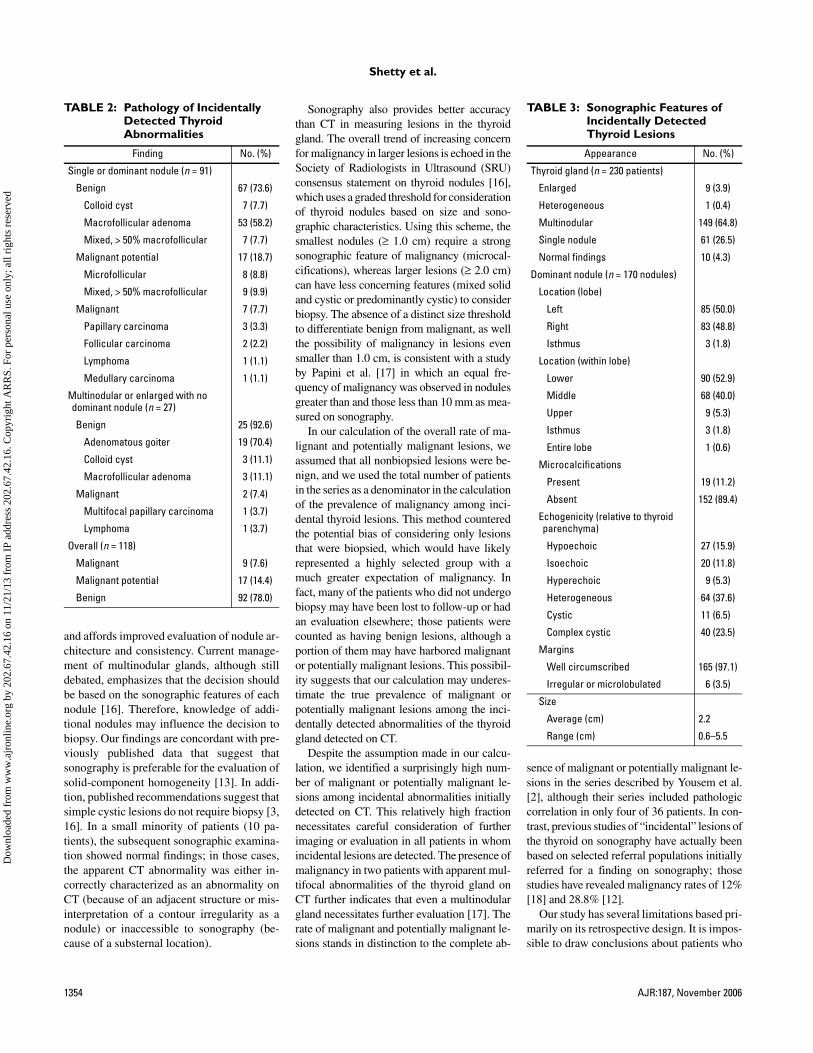
TABLE 2: Pathology of Incidentally Detected Thyroid Abnormalities
Finding No. (%)
Single or dominant nodule (n = 91)
Benign 67 (73.6)
Colloid cyst 7 (7.7)
Macrofollicular adenoma 53 (58.2)
Mixed, > 50% macrofollicular 7 (7.7)
Malignant potential 17 (18.7)
Microfollicular 8 (8.8)
Mixed, > 50% macrofollicular 9 (9.9)
Malignant 7 (7.7)
Papillary carcinoma 3 (3.3)
Follicular carcinoma 2 (2.2)
Lymphoma 1 (1.1)
Medullary carcinoma 1 (1.1)
Multinodular or enlarged with no dominant nodule (n = 27)
Benign 25 (92.6)
Adenomatous goiter 19 (70.4)
Colloid cyst 3 (11.1)
Macrofollicular adenoma 3 (11.1)
Malignant 2 (7.4)
Multifocal papillary carcinoma 1 (3.7)
Lymphoma 1 (3.7)
Overall (n = 118)
Malignant 9 (7.6)
Malignant potential 17 (14.4)
Benign 92 (78.0)
TABLE 3: Sonographic Features of Incidentally Detected Thyroid Lesions
Appearance No. (%)
Thyroid gland (n = 230 patients)
Enlarged 9 (3.9)
Heterogeneous 1 (0.4)
Multinodular 149 (64.8)
Single nodule 61 (26.5)
Normal findings 10 (4.3)
Dominant nodule (n = 170 nodules)
Location (lobe)
Left 85 (50.0)
Right 83 (48.8)
Isthmus 3 (1.8)
Location (within lobe)
Lower 90 (52.9)
Middle 68 (40.0)
Upper 9 (5.3)
Isthmus 3 (1.8)
Entire lobe 1 (0.6)
Microcalcifications
Present 19 (11.2)
Absent 152 (89.4)
Echogenicity (relative to thyroid parenchyma)
Hypoechoic 27 (15.9)
Isoechoic 20 (11.8)
Hyperechoic 9 (5.3)
Heterogeneous 64 (37.6)
Cystic 11 (6.5)
Complex cystic 40 (23.5)
Margins
Well circumscribed 165 (97.1)
Irregular or microlobulated 6 (3.5)
Size
Average (cm) 2.2
Range (cm) 0.6–5.5
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

CT of Incidental Thyroid Lesions
AJR:187, November 2006 1355
may have had incidental lesions seen on CTwho did not (for any reason) receive furtherevaluation with sonography, because thesepatients were not included in the study popu-lation. The inclusion of only patients who un-derwent subsequent sonography may have in-troduced a bias because the clinical factorsthat led to the referral for subsequent sonog-raphy have not been included in the evalua-tion. However, it has been routine practice atour institution to refer all patients with an in-cidental lesion of the thyroid gland for a ded-icated sonographic examination of the thyroidgland, thereby reducing the magnitude of thisselection bias in our study population.
A second source of potential bias is the de-pendence on the initial CT interpretation to de-tect an abnormality of the thyroid gland; cer-tainly, a number of incidental lesions wereprobably not detected during the initial inter-pretation and therefore were not included inour analysis; one might hypothesize that thesemissed lesions tended to be smaller, located atthe periphery of the gland, or isodense relativeto the thyroid gland. It is difficult to say howthe exclusion of these missed lesions might af-fect the final result. In addition, the study pop-ulation was older and more likely to have con-current health problems than the generalpopulation because all were being imaged forother reasons. However, our study group prob-ably represents a population that might be en-countered in any large metropolitan setting.
Definitive surgical excision was not avail-able in all cases, either because patients werelost to follow-up, refused surgery, or pursued
subsequent treatment at a different institution.So as not to bias our results by excludingthese patients entirely, the category of “poten-tially malignant” was applied to microfollic-ular or predominantly microfollicular lesionswithout definite surgical excision. Althoughthe diagnosis and management of these le-sions are debated in the clinical literature[4–6], the current standard is to recommendresection of hypofunctioning or eufunction-ing microfollicular lesions because the possi-bility of follicular carcinoma can be excludedonly through the evaluation of architecturalchanges such as vascular or capsular invasion.
The incidental nodules of the thyroid weredetected on CT performed for a variety of rea-sons. This entailed the use of different scan-ning parameters, including differing fields ofview and slice thicknesses. These parametersmay have altered the ability to accurately mea-sure thyroid nodules. Contrast enhancementwas also variable: Some studies were unen-hanced and others used variable delays be-tween contrast injection and imaging. Al-though previous studies have shown improvedcontrast between thyroid lesions and normalgland parenchyma on unenhanced or late-phase contrast-enhanced studies (relative toearly-phase contrast enhancement) [13], it re-mains to be determined whether the enhance-ment characteristics of a lesion (which werenot assessed in our study) may prove useful inthe differentiation of incidental thyroid lesions.
In conclusion, a relatively high number ofthyroid abnormalities are incidentally de-tected on CT that are malignant or potentially
malignant. The clinical literature indicatesthat most palpable thyroid nodules are benign(90–95%) [3, 19]. However, in our study, wefound a 3.9% prevalence of malignancy (95%CI: 1.8–7.3%) and a 7.4% prevalence of ma-lignant potential (95% CI: 4.4–11.6%) amongincidental lesions of the thyroid gland. Con-sidered as a group, these findings yield anoverall rate of 11.3% for malignant or poten-tially malignant lesions among incidentallydetected thyroid lesions on CT.
Unfortunately, we did not find any distinctCT feature that invariably distinguishes benignfrom malignant lesions when correlated tosonographic appearance or histopathology. Pa-tient demographics may be the most useful toolfor the radiologist because patients 35 years oryounger were significantly more likely to har-bor malignancy in an incidental thyroid glandabnormality. CT tends to underestimate thetrue number of nodules and cannot reliably dis-tinguish cystic from solid nodules; the adjunc-tive information afforded by the sonographyexamination suggests that evaluation withsonography should be performed after detec-tion of an incidental abnormality of the thyroidon CT. Although sampling of these incidentallesions may be necessary on the basis of the re-sults of the subsequently performed sono-graphic or clinical evaluation, referring a pa-tient for sampling based on the CT findingsalone would be imprudent and premature, par-ticularly when a noninvasive examination(sonography) is readily available that can pro-vide useful adjunctive information that will in-form the decision to pursue biopsy. Our results
TABLE 4: Correlation of Pathology and CT Imaging Features in 91 Dominant Nodules
Pathology No.
Size (cm) Punctate Calcifications
Density (H) Density (by No. of Nodules)Margins (by No. of
Nodules)
Average Range Average Range Hypo Iso Hyper Hetero WC ID
Malignant
Papillary cancer 3 2.37 1.5–2.8 0 55.7 21–100 1 1 0 1 3 0
Follicular cancer 2 3.65 3.3–4.0 0 94 49–145 0 0 0 2 1 1
Lymphoma 1 3.40 NA 1 38 NA 0 0 0 1 1 0
Medullary 1 2.70 NA 1 18 NA 0 0 0 1 1 0
Malignant potential
Microfollicular 9 2.71 0.7–4.6 0 54.3 32–109 6 0 0 3 8 1
> 50% Microfollicular 8 2.76 1.9–3.8 1 70.4 23–165 3 0 1 4 8 0
Benign
Colloid cyst 7 2.29 0.8–3.2 0 49.7 5–130 3 0 0 4 7 0
Macrofollicular 53 2.08 0.6–4.5 7 71.5 3–163 17 10 4 22 51 2
> 50% Macrofollicular 7 2.74 0.8–4.2 0 51.6 10–74 3 0 0 4 7 0
Total 91 33 11 5 42
Note—Hypo = hypodense, Iso = isodense, Hyper = hyperdense, Hetero = heterogeneous, WC = well-circumscribed, ID = ill-defined, NA = not applicable.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

Shetty et al.
1356 AJR:187, November 2006
suggest that every incidental abnormality ofthe thyroid detected on CT deserves additionalclinical or imaging evaluation to exclude thepossibility of malignancy. The optimal form ofthis subsequent evaluation, from the perspec-tive of both patient care and cost-effectiveness,should be the subject of future study.
References1. Brander A, Viikinkoski P, Nickels J, Kivisaari L.
Thyroid gland: US screening in a random adult pop-
ulation. Radiology 1991; 181:683–687
2. Yousem DM, Huang T, Loevner LA, Langlotz
CP. Clinical and economic impact of incidental
thyroid lesions found with CT and MR. AJNR
1997; 18:1423–1428
3. Hegedus L. Clinical practice: the thyroid nodule. N
Engl J Med 2004; 351:1764–1771
4. Carpi A, Nicolini A, Sagripanti A, Righi C, Fabris
FM, Di Coscio G. Large-needle aspiration biopsy
for the preoperative selection of palpable thyroid
nodules diagnosed by fine-needle aspiration as a
microfollicular nodule or suspected cancer. Am J
Clin Pathol 2000; 113:872–877
5. Barbaro D, Simi U, Lopane P, et al. Thyroid nodules
with microfollicular findings reported on fine-nee-
dle aspiration: invariably surgical treatment? En-
docr Pract 2001; 7:352–357
6. Carpi A, Nicolini A, Righi C, Romani R, Di Coscio
G. Large needle aspiration biopsy results of palpa-
ble thyroid nodules diagnosed by fine-needle aspi-
ration as a microfollicular nodule with atypical cells
or suspected cancer. Biomed Pharmacother 2004;
58:351–355
7. Pombo F, Rodriguez E, Cao JI, Martinez-Isla C.
Cervical lymph node metastases of medullary thy-
roid carcinoma: CT findings. Eur Radiol 1997;
7:99–101
8. Peccin S, de Castsro JA, Furlanetto TW, Furtado AP,
Brasil BA, Czepielewski MA. Ultrasonography: is
it useful in the diagnosis of cancer in thyroid nod-
ules? J Endocrinol Invest 2002; 25:39–43
9. Kim EK, Park CS, Chung WY, et al. New sono-
graphic criteria for recommending fine-needle as-
piration biopsy of nonpalpable solid nodules of the
thyroid. AJR 2002; 178:687–691
10. Takashima S, Fukuda H, Nomura N, Kishimoto H,
Kim T, Kobayashi T. Thyroid nodules: re-evalua-
tion with ultrasound. J Clin Ultrasound 1995;
23:179–184
11. Iannuccilli JD, Cronan JJ, Monchik JM. Risk for
malignancy of thyroid nodules as assessed by sono-
graphic criteria: the need for biopsy. J Ultrasound
Med 2004; 23:1455–1464
12. Kang HW, No JH, Chung JH, et al. Prevalence, clin-
ical, and ultrasonographic characteristics of thyroid
incidentalomas. Thyroid 2004; 14:29–33
13. Ishigaki S, Shimamoto K, Satake H, et al. Multi-
slice CT of thyroid nodules: comparison with ultra-
sonography. Radiat Med 2004; 22:346–353
14. Radecki PD, Arger PH, Arenson RL, et al. Thyroid
imaging: comparison of high-resolution real-time
ultrasound and computed tomography. Radiology
1984; 153:145–147
15. Stark DD, Clark OH, Gooding GAW, Moss AA.
High-resolution ultrasonography and computed to-
mography of thyroid lesions in patients with hyper-
parathyroidism. Surgery 1983; 94:863–868
16. Frates MC. Society of Radiologists in Ultrasound
Web site. Consensus Conference on Management of
Thyroid Nodules (preliminary report), 2004. Avail-
able at: www.sru.org. Accessed August 2004
17. Papini E, Guglielmi R, Bianchini A, et al. Risk of
malignancy in nonpalpable thyroid nodules: predic-
tive value of ultrasound and color-Doppler features.
J Clin Endocrinol Metab 2002; 87:1941–1946
18. Nam-Goong IS, Kim HY, Gong G, et al. Ultra-
sonography-guided fine-needle aspiration of thy-
roid incidentaloma: correlation with pathological
findings. Clin Endocrinol (Oxf) 2004; 60:21–28
19. Lawrence W Jr, Kaplan BJ. Diagnosis and manage-
ment of patients with thyroid nodules. J Surg Oncol
2002; 80:157–170
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

This article has been cited by:
1. Miriam Ruesseler, Anna Schill, Thomas Lehnert, Hendrik Wyen, Sebastian Wutzler, Ingo Marzi, Felix Walcher. 2013. Incidentalfindings in patients with multiple injuries. Journal of Trauma and Acute Care Surgery 75:5, 848-853. [CrossRef]
2. Michael K. Malone, Jonathan Zagzag, Jennifer B. Ogilvie, Kepal N. Patel, Keith S. Heller. 2013. Thyroid Cancers Detected byImaging Are Not Necessarily Small or Early Stage. Thyroid 130913071028003. [CrossRef]
3. Zhi-Jiang Han, Yan-Yan Shu, Xu-Feng Lai, Wen-Hui Chen. 2013. Value of computed tomography in determining the natureof papillary thyroid microcarcinomas: evaluation of the computed tomographic characteristics. Clinical Imaging 37:4, 664-668.[CrossRef]
4. Andreas M. Darr, Thomas Opfermann, Tobias Niksch, Dominik Driesch, Robert J. Marlowe, Martin Freesmeyer. 2013. Low-Activity 124I-PET/Low-Dose CT Versus 99mTc-Pertechnetate Planar Scintigraphy or 99mTc-Pertechnetate Single-PhotonEmission Computed Tomography of the Thyroid. Clinical Nuclear Medicine 1. [CrossRef]
5. X. V. Nguyen, K. Roy Choudhury, J. D. Eastwood, G. H. Lyman, R. M. Esclamado, J. D. Werner, J. K. Hoang. 2013.Incidental Thyroid Nodules on CT: Evaluation of 2 Risk-Categorization Methods for Work-Up of Nodules. American Journalof Neuroradiology . [CrossRef]
6. Sebastian R. Aspinall, Sarah G.S. Ong, Michael S.J. Wilson, Thomas W.J. Lennard. 2013. How shall we manage the incidentallyfound thyroid nodule?. The Surgeon 11:2, 96-104. [CrossRef]
7. Jeong Hyun Lee, Yoshimi Anzai. 2013. Imaging of Thyroid and Parathyroid Glands. Seminars in Roentgenology 48:1, 87-104.[CrossRef]
8. Teresa R. Kroeker, Gavin le Nobel, Mazin Merdad, Jeremy L. Freeman. 2013. Outcomes of incidentally discovered thyroid nodulesreferred to a high-volume head and neck surgeon. Head & Neck n/a-n/a. [CrossRef]
9. Jong Hoo Lee, Sun Young Jeong, Yee Hyung Kim. 2013. Clinical significance of incidental thyroid nodules identified on low-dose CT for lung cancer screening. Multidisciplinary Respiratory Medicine 8:1, 56. [CrossRef]
10. J. Tramalloni, J.L. Wémeau. 2012. Consensus français sur la prise en charge du nodule thyroïdien : ce que le radiologue doitconnaître. EMC - Radiologie et imagerie médicale - Cardiovasculaire - Thoracique - Cervicale 7:4, 1-18. [CrossRef]
11. Jenny K. Hoang, Phillip Raduazo, David M. Yousem, James D. Eastwood. 2012. What to Do With Incidental Thyroid Noduleson Imaging? An Approach for the Radiologist. Seminars in Ultrasound, CT and MRI 33:2, 150-157. [CrossRef]
12. Che-Wei Wu, Gianlorenzo Dionigi, Ka-Wo Lee, Pi-Jung Hsiao, Ming-Chen Paul Shin, Kuo-Bow Tsai, Feng-Yu Chiang. 2012.Calcifications in thyroid nodules identified on preoperative computed tomography: Patterns and clinical significance. Surgery 151:3,464-470. [CrossRef]
13. Judy Jin, Christopher R. McHenry. 2012. Thyroid incidentaloma. Best Practice & Research Clinical Endocrinology & Metabolism26:1, 83-96. [CrossRef]
14. Leslie Eisenbud Quint, Kuanwong Watcharotone, James D. Myles, Larry D. Gruppen, Patricia B. Mullan. 2011. IncidentalFindings at Chest CT. Academic Radiology 18:12, 1500-1506. [CrossRef]
15. Monzer M. Abu-Yousef, Joshua H. Larson, David M. Kuehn, Andrew S. Wu, Archana T. Laroia. 2011. Safety of Ultrasound-Guided Fine Needle Aspiration Biopsy of Neck Lesions in Patients Taking Antithrombotic/Anticoagulant Medications. UltrasoundQuarterly 27:3, 157-159. [CrossRef]
16. J.-L. Wémeau, J.-L. Sadoul, M. d’Herbomez, H. Monpeyssen, J. Tramalloni, E. Leteurtre, F. Borson-Chazot, P. Caron, B.Carnaille, J. Léger, C. Do, M. Klein, I. Raingeard, R. Desailloud, L. Leenhardt. 2011. Guidelines of the French society ofendocrinology for the management of thyroid nodules. Annales d'Endocrinologie 72:4, 251-281. [CrossRef]
17. Jing Gao, Jonathan Kazam, Elias KazamMultimodality Imaging and Aspiration Biopsy Guidance in the Perioperative Managementof Thyroid Carcinoma 117-132. [CrossRef]
18. Michael K. Atalay, Ethan A. Prince, Catherine A. Pearson, Kevin J. Chang. 2011. The Prevalence and Clinical Significance ofNoncardiac Findings on Cardiac MRI. American Journal of Roentgenology 196:4, W387-W393. [Abstract] [Full Text] [PDF][PDF Plus]
19. Sameer Ahmed, Karen M. Horton, R. Brooke Jeffrey, Jr., Sheila Sheth, Elliot K. Fishman. 2010. Incidental Thyroid Noduleson Chest CT: Review of the Literature and Management Suggestions. American Journal of Roentgenology 195:5, 1066-1071.[Abstract] [Full Text] [PDF] [PDF Plus]
20. Matthew C. Miller. 2010. The Patient with a Thyroid Nodule. Medical Clinics of North America 94:5, 1003-1015. [CrossRef]21. N. G. Iyer, Ashok R. Shaha, Carl E. Silver, Kenneth O. Devaney, Alessandra Rinaldo, Phillip K. Pellitteri, Alfio Ferlito. 2010.
Thyroid incidentalomas: to treat or not to treat. European Archives of Oto-Rhino-Laryngology 267:7, 1019-1026. [CrossRef]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
22. Emmanuel Atta Agaba. 2010. Primary Cavernous Hemangioma of the Thyroid Gland. Southern Medical Journal 103:7, 601.[CrossRef]
23. Nina D. Baier, Mukesh G. Harisinghani, Peter R. Mueller. 2010. Reply. American Journal of Roentgenology 194:5, 1403-1403.[Citation] [Full Text] [PDF] [PDF Plus]
24. Ferris M. Hall. 2010. Biopsy of Thyroid Nodules. American Journal of Roentgenology 194:5, 1403-1403. [Citation] [Full Text][PDF] [PDF Plus]
25. L. J. Layfield, E. S. Cibas, Z. Baloch. 2010. Thyroid fine needle aspiration cytology: a review of the National Cancer Institutestate of the science symposium. Cytopathology 21:2, 75-85. [CrossRef]
26. Edmund S. Cibas. 2010. Fine-Needle Aspiration in the Work-Up of Thyroid Nodules. Otolaryngologic Clinics of North America43:2, 257-271. [CrossRef]
27. Koichiro Kaneko, Koichiro Abe, Shingo Baba, Yoshitaka Tanabe, Hidetake Yabuuchi, Masamitsu Hatakenaka, Masayuki Sasaki,Hiroshi Honda. 2010. Can calcification predict 131I accumulation on metastatic lymph nodes in papillary thyroid carcinomapatients receiving 131I therapy? Comparison of CT, 131I WBS and 18F-FDG PET/CT. European Radiology 20:2, 477-483.[CrossRef]
28. L. E. Ginsberg. 2010. "If Clinically Indicated:" Is It?. Radiology 254:2, 324-325. [CrossRef]29. A.G. Osborn. 2010. Partially Cystic Thyroid Nodules on Ultrasound: Probability of Malignancy and Sonographic Differentiation.
Yearbook of Diagnostic Radiology 2010, 346-348. [CrossRef]30. Arturs Ozolins, Zenons Narbuts, Ilze Strumfa, Peteris Prieditis, Janis Gardovskis. 2010. Diagnosis and Management of the Thyroid
Nodules. Acta Chirurgica Latviensis 10:2. . [CrossRef]31. Philip Shie, Roberto Cardarelli, Kelly Sprawls, Kimberly G. Fulda, Alan Taur. 2009. Systematic review: prevalence of malignant
incidental thyroid nodules identified on fluorine-18 fluorodeoxyglucose positron emission tomography. Nuclear MedicineCommunications 30:9, 742-748. [CrossRef]
32. Tyler W. Barrett, Michelle Schierling, Chuan Zhou, J. Drew Colfax, Stephan Russ, Paige Conatser, Penny Lancaster, KeithWrenn. 2009. Prevalence of incidental findings in trauma patients detected by computed tomography imaging. The AmericanJournal of Emergency Medicine 27:4, 428-435. [CrossRef]
33. S Bastin, MJ Bolland, MS Croxson. 2009. Role of ultrasound in the assessment of nodular thyroid disease. Journal of MedicalImaging and Radiation Oncology 53:2, 177-187. [CrossRef]
34. Judy Jin, Scott M. Wilhelm, Christopher R. McHenry. 2009. Incidental thyroid nodule: patterns of diagnosis and rate ofmalignancy. The American Journal of Surgery 197:3, 320-324. [CrossRef]
35. Stavros Tsantis, Nikos Dimitropoulos, Dionisis Cavouras, George Nikiforidis. 2009. Morphological and wavelet features towardssonographic thyroid nodules evaluation. Computerized Medical Imaging and Graphics 33:2, 91-99. [CrossRef]
36. Scott M. Wilhelm. 2008. Utility of I-123 thyroid uptake scan in incidental thyroid nodules: An old test with a new role. Surgery144:4, 511-517. [CrossRef]
37. Dae Young Yoon, Suk Ki Chang, Chul Soon Choi, Eun Joo Yun, Young Lan Seo, Eun Suk Nam, Sung Jin Cho, Young-Soo Rho,Hwoe Young Ahn. 2008. The Prevalence and Significance of Incidental Thyroid Nodules Identified on Computed Tomography.Journal of Computer Assisted Tomography 32:5, 810-815. [CrossRef]
38. James I. Cohen, Kelli D. Salter. 2008. Thyroid Disorders: Evaluation and Management of Thyroid Nodules. Oral and MaxillofacialSurgery Clinics of North America 20:3, 431-443. [CrossRef]
39. Jenny Gough, David Scott-Coombes, F. Fausto Palazzo. 2008. Thyroid Incidentaloma: An Evidence-based Assessment ofManagement Strategy. World Journal of Surgery 32:7, 1264-1268. [CrossRef]
40. Edmund S. Cibas, Erik K. Alexander, Carol B. Benson, Pedro Patricio de Agustín, Gerard M. Doherty, William C. Faquin,William D. Middleton, Theodore Miller, Stephen S. Raab, Matthew L. White, Susan J. Mandel. 2008. Indications for thyroidFNA and pre-FNA requirements: A synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of theScience Conference. Diagnostic Cytopathology 36:6, 390-399. [CrossRef]
41. Jin Young Kwak, Eun-Kyung Kim, Ji Hyun Youk, Min Jung Kim, Eun Ju Son, Seon Hyeong Choi, Ki Keun Oh. 2008.Extrathyroid Extension of Well-Differentiated Papillary Thyroid Microcarcinoma on US. Thyroid 18:6, 609-614. [CrossRef]
42. Derek G. Lohan, Anderanik Tomasian, Roya Saleh, Mayil Krishnam, J. Paul Finn. 2008. Hypervascular Thyroid Nodules onTime-Resolved MR Angiography at 3 T: Radiologic–Pathologic Correlation. American Journal of Roentgenology 190:4, W255-W260. [Abstract] [Full Text] [PDF] [PDF Plus]
43. T. Le Corroller, P. Champsaur, G. Moulin. 2008. Radioanatomie du cou. EMC - Radiologie et imagerie médicale - Cardiovasculaire- Thoracique - Cervicale 3:1, 1-20. [CrossRef]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
44. Scott M. Wilhelm, Ann V. Robinson, Smitha S. Krishnamurthi, Harry L. Reynolds. 2007. Evaluation and management ofincidental thyroid nodules in patients with another primary malignancy. Surgery 142:4, 581-587. [CrossRef]
45. H. Dralle. 2007. Inzidentalome der Schilddrüse. Der Chirurg 78:8, 677-686. [CrossRef]46. A.G. Osborn. 2007. Significance of Incidental Thyroid Lesions Detected on CT: Correlation Among CT, Sonography, and
Pathology. Yearbook of Diagnostic Radiology 2007, 357-359. [CrossRef]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 2
02.6
7.42
.16
on 1
1/21
/13
from
IP
addr
ess
202.
67.4
2.16
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved