Thrombosis of prosthetic heart valves - shshe.org · Thrombosis of prosthetic heart valves Elona...
46
Thrombosis of prosthetic Thrombosis of prosthetic heart valves heart valves Elona Elona Dado Dado UHC UHC ” ” Mother Mother Tereza Tereza “ “ Service of Cardiac Surgery Service of Cardiac Surgery
Transcript of Thrombosis of prosthetic heart valves - shshe.org · Thrombosis of prosthetic heart valves Elona...

Thrombosis of prosthetic Thrombosis of prosthetic heart valvesheart valves
ElonaElona DadoDado
UHC UHC ”” Mother Mother TerezaTereza ““Service of Cardiac SurgeryService of Cardiac Surgery

Case 1Case 1
►►V.B a 54 year old woman, was hospitalized V.B a 54 year old woman, was hospitalized in our service of cardiac surgery.in our service of cardiac surgery.
►►Diagnosis Diagnosis : Rheumatic : Rheumatic ValvularValvular Heart Heart Disease . Severe Disease . Severe mitralmitral stenosisstenosis. Moderate . Moderate mitralmitral regurgitation. CHF regurgitation. CHF --NYHA III NYHA III functional class. Sinus rhythm.functional class. Sinus rhythm.
►►Surgical interventionSurgical intervention was performed : was performed : MitralMitral valve replacement with mechanical valve replacement with mechanical prosthetic valve prosthetic valve SJM Nr 27SJM Nr 27..

Postoperative period
►► Day twoDay two-- Uneventful. Sinus rhythm . Stable Uneventful. Sinus rhythm . Stable hemodinamichemodinamic status. status.
►► TTE examinationTTE examination : Maximal and mean : Maximal and mean prosthetic pressure gradients prosthetic pressure gradients 8 mmHg and 48 mmHg and 4mmHgmmHg respectively.respectively.
►► Day three Day three -- Complicated with Complicated with A.FibA.Fib and transient and transient cerebral ischemic attack.cerebral ischemic attack.
►► Anticoagulation level was Anticoagulation level was subtherapeuticsubtherapeutic ::INR 1.9INR 1.9..
..

Postoperative period
Day four : Day four : Sinus rhythmSinus rhythm was spontaneously was spontaneously reverted . No reverted . No dyspneadyspnea , stable , stable hemodinamicshemodinamics, , prosthetic sound present. prosthetic sound present. Normal neurological Normal neurological examinationexamination
TEE examination was performedTEE examination was performedTEE revealed a homogeneous ,soft mass , not TEE revealed a homogeneous ,soft mass , not pedunculatedpedunculated ,located at valve strut at LAA level. ,located at valve strut at LAA level. Dimensions : length 2,3cm area 2,1 cm2. No Dimensions : length 2,3cm area 2,1 cm2. No obstruction ,no increase in mean prosthetic obstruction ,no increase in mean prosthetic gradient (4 mm Hg). No tricuspid regurgitation.gradient (4 mm Hg). No tricuspid regurgitation.
TEE ITEE I

TEE diagnosisTEE diagnosis
Non obstructive prosthetic thrombosisNon obstructive prosthetic thrombosis
Therapeutic decisionTherapeutic decisionAccording to ESC guidelines (2007) on the According to ESC guidelines (2007) on the management of management of valvularvalvular heart disease heart disease surgerysurgery is is recommended for large ( > 10 mm) nonrecommended for large ( > 10 mm) non--obstructive prosthetic thrombosis complicated by obstructive prosthetic thrombosis complicated by embolism ( Class II a, level of evidence C) and embolism ( Class II a, level of evidence C) and medical therapymedical therapy in cases of small thrombosis in cases of small thrombosis (< 10 mm) (< 10 mm)

Therapeutic decisionTherapeutic decision
Considering Considering ►► Surgical risk of Surgical risk of reinterventionreintervention
(early postoperative period)(early postoperative period)►► Sub therapeutic anticoagulation level ( INR 1.9)Sub therapeutic anticoagulation level ( INR 1.9)►► Thrombus characteristicsThrombus characteristics-- fresh thrombusfresh thrombus►► Spontaneous reversion of sinus rhythm without Spontaneous reversion of sinus rhythm without
any further embolic complicationany further embolic complicationwe thought that would be mindful to switch to we thought that would be mindful to switch to
medical treatment : medical treatment : HEPARIN + AspirinHEPARIN + Aspirin

Therapeutic resultTherapeutic result
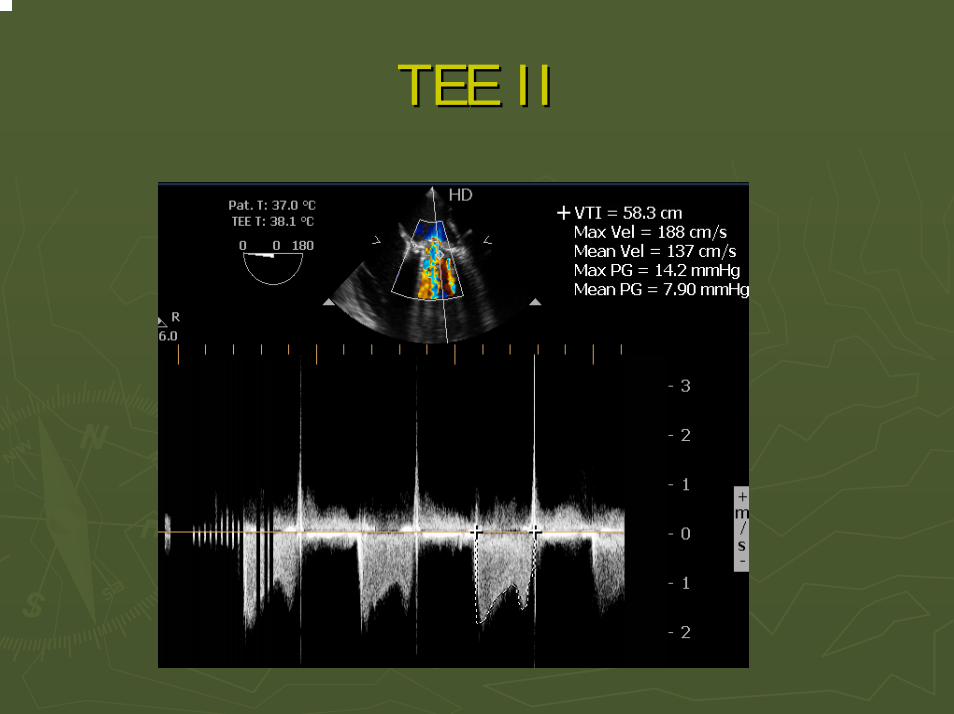
►► After one week of medical treatment (Heparin I/v After one week of medical treatment (Heparin I/v + Aspirin 100mg/d) another TEE was performed.+ Aspirin 100mg/d) another TEE was performed.
►► The response to heparin treatment was The response to heparin treatment was considered as considered as thromboliticthrombolitic successsuccess ( based on ( based on reduction about 75% in thrombus area) and reduction about 75% in thrombus area) and clinical successclinical success ( no minor or major ( no minor or major complications occurred, stable clinical status) complications occurred, stable clinical status)
TEE IITEE II

TEE ITEE I

TEE ITEE I

TEE IITEE II

Therapeutic result Therapeutic result
►►Heparin treatment was continued for Heparin treatment was continued for another week and another week and CumadinCumadin treatment was treatment was initiated ( initiated ( CumadinCumadin + Aspirin 100mg). INR + Aspirin 100mg). INR level of 3.5 was achieved .level of 3.5 was achieved .
►►After two weeks another TEE examination After two weeks another TEE examination was performed. Thrombus totally was performed. Thrombus totally disappeared .disappeared .
TEE IIITEE III..

Therapeutic resultTherapeutic result--follow upfollow up
9 9 mthsmths after dismissal, follow up after dismissal, follow up resulted in a very good clinical condition resulted in a very good clinical condition –– NYHA class I and normal prosthetic NYHA class I and normal prosthetic function in function in echocardiographicechocardiographicexamination. examination.

Case 2Case 2►► F.B a 42 years old woman was hospitalized in F.B a 42 years old woman was hospitalized in
our service with the our service with the diagnosis diagnosis : : Suspected Suspected prosthesis valve thrombosis. Threatening prosthesis valve thrombosis. Threatening inferior limb ischemia.inferior limb ischemia.
History:History:►► MitralMitral valve valve replacementreplacement with mechanical with mechanical
monoleafletmonoleaflet ( Medtronic) ( Medtronic) prosthesisprosthesis 16 years 16 years ago.ago.
►► Two years agoTwo years ago-- transient transient cerebral ischemiccerebral ischemicattack, attack, peripheral embolicperipheral embolic events with events with subsequent bilateral lower limb ischemia. ABI subsequent bilateral lower limb ischemia. ABI dexterdexter and sinister 0.6 and 0.7 respectivelyand sinister 0.6 and 0.7 respectively
►► Not regular follow up. Poor pt complianceNot regular follow up. Poor pt compliance

Case 2Case 2
►► Before 4 months she was Before 4 months she was diagnoseddiagnosed for for large obstructive prosthetic valve large obstructive prosthetic valve thrombus, NYHA functional class III thrombus, NYHA functional class III symptomssymptoms , and was , and was operated on operated on emergencyemergency (large thrombus + (large thrombus + pannuspannuswas found).was found).
►►Sub therapeutic anticoagulation level in Sub therapeutic anticoagulation level in admission.admission.

Case 2Case 2
This time clinical and laboratory This time clinical and laboratory examination revealedexamination revealed ::Again Again subtherapeuticsubtherapeutic anticoagulationanticoagulation in in admission.admission.Absence of bilateral femoral and Absence of bilateral femoral and poplitealpopliteal
pulsespulses..No No dyspneadyspnea at restat rest, , no no orthopneaorthopnea, , nono
tachipneatachipnea. . Prosthetic valve sound presentProsthetic valve sound present. . No heart murmurs. Normal breath sounds. Normal No heart murmurs. Normal breath sounds. Normal BP. BP. Rhythmic heart soundsRhythmic heart soundsParoxysticParoxystic A.FibA.Fib

Case 2Case 2►► AngioAngio CT of aortaCT of aorta , , iliac and lower limb iliac and lower limb
arteries:arteries: Total aortic (at bifurcation level ) and Total aortic (at bifurcation level ) and iliac ( origin) occlusioniliac ( origin) occlusion
►► TTE examinationTTE examination ::Increase in prosthetic pressure gradients (Increase in prosthetic pressure gradients (mean mean gradient 14 mm gradient 14 mm HgHg).Suspected).Suspected thromboticthrombotic mass. mass. No tricuspid regurgitation.No tricuspid regurgitation.
►► TEE examination TEE examination ::PVT PVT -- soft mobile obstructive thrombisoft mobile obstructive thrombi..Considering Considering thromboticthrombotic burdenburden and and motilitymotility, and , and the previous peripheral the previous peripheral embolismembolism cardiac surgery cardiac surgery was indicated was indicated
( class ( class IIaIIa recommendation .ACC/AHA guidelines 2006)recommendation .ACC/AHA guidelines 2006)

TEE ITEE I

Timing of cardiac surgeryTiming of cardiac surgery
Acute threatening lower limb ischemia Acute threatening lower limb ischemia urged the need of emergent vascular urged the need of emergent vascular interventionintervention. . We had to We had to evaluateevaluate the risks of the risks of cardiac surgerycardiac surgeryin such a complex situation : critical inferior limb in such a complex situation : critical inferior limb ischemia, reischemia, re--operation (for the third time, last operation (for the third time, last intervention 4 intervention 4 mthsmths ago), absence of cardiac ago), absence of cardiac symptoms at rest.symptoms at rest.After informing the pts of her actual clinical status After informing the pts of her actual clinical status and risks the decision for and risks the decision for vascular surgery prior vascular surgery prior to cardiac surgery was made . to cardiac surgery was made .

Therapeutic decisionTherapeutic decision
►► Vascular surgeryVascular surgery --Aortic and iliac artery Aortic and iliac artery thrombectomithrombectomi -- revealed fresh and organizedrevealed fresh and organizedthrombi thrombi at aortic bifurcation level and at both at aortic bifurcation level and at both iliac arteries. Reversion of femoral pulses and of iliac arteries. Reversion of femoral pulses and of the previous ABI (0.5/0.7)the previous ABI (0.5/0.7)
►► Meanwhile the pt was under treatment with Meanwhile the pt was under treatment with intravenous Heparinintravenous Heparin ..
Stable cardiac situation. Stable cardiac situation. CordaronCordaron to maintain to maintain stable sinus rhythmstable sinus rhythm

Therapeutic decisionTherapeutic decision
►► TTE and TEE examinationTTE and TEE examination was performed to was performed to reevaluate prosthetic status before taking the reevaluate prosthetic status before taking the next step next step -- cardiac surgerycardiac surgery..
Examination resultsExamination results::Diminished thrombus size , decrease in Diminished thrombus size , decrease in
prosthetic pressure gradient (8 mm Hg).prosthetic pressure gradient (8 mm Hg).
TEE IITEE II

TEE IITEE II
TEE IITEE II

Therapeutic decisionTherapeutic decision
Was cardiac surgery still recommendable?Was cardiac surgery still recommendable?►► Small clot burden. Small clot burden. ►► NYHA class INYHA class I--II symptoms. Stable sinus rhythmII symptoms. Stable sinus rhythm►► Proven partial Proven partial hemodynamichemodynamic success of heparin success of heparin
treatment without clinical complications.treatment without clinical complications.
But highly mobile But highly mobile thromboticthrombotic mass with an evident mass with an evident risk of risk of embolisationembolisation..

Therapeutic decisionTherapeutic decision
We decided to continue treatment with I/V We decided to continue treatment with I/V Heparin Heparin and and Aspirin 100mgAspirin 100mg
(Recommendation class (Recommendation class IIbIIb, ACC/AHA , ACC/AHA guidelines 2006) for two weeks followed by guidelines 2006) for two weeks followed by CumadineCumadine + + AspirineAspirine aiming to achieve INR aiming to achieve INR levels near 3.5!levels near 3.5!

Therapeutic resultTherapeutic result--follow upfollow up
►►TEE IIITEE III : Normal prosthetic function. Total : Normal prosthetic function. Total thrombus thrombus lysislysis..
►►HemodynamicHemodynamic and clinical success:and clinical success:NYHA I functional class , no major or minor NYHA I functional class , no major or minor complications.complications.
TEE IIITEE III

DiscussionDiscussion
►► Prosthetic valve thrombosis (Prosthetic valve thrombosis (PVT)isPVT)is a rare but a rare but serious complication , most often encountered serious complication , most often encountered with with mechanical prosthesismechanical prosthesis..
►► Significant mortality and morbidity warrants Significant mortality and morbidity warrants rapid diagnostic evaluation.rapid diagnostic evaluation.
►► Variability in clinical presentation makes the Variability in clinical presentation makes the diagnosis challenging.diagnosis challenging.
►► The main diagnostic procedures include : The main diagnostic procedures include : echocardiography echocardiography ––transsthoracictranssthoracic and and transoesophagealtransoesophageal ; ; cinefluoroscopycinefluoroscopy

DiscussionDiscussion►► The incidence of The incidence of obstructive PVTobstructive PVT for for
mechanical valves varies between 03mechanical valves varies between 03--1.3% 1.3% patient years.patient years.
►► NonNon--obstructiveobstructive PVT is a relatively frequent PVT is a relatively frequent finding in the finding in the postoperative periodpostoperative period --reported incidence 10% (in earlier studies up reported incidence 10% (in earlier studies up to 12.5to 12.5--15%)15%)
►► PVT incidence in the first postoperative year PVT incidence in the first postoperative year is 24 %, 2is 24 %, 2--4 years 15% with a subsequent 4 years 15% with a subsequent decrease thereafter.decrease thereafter.
►► ThrombembolicThrombembolic complications occur at a rate complications occur at a rate of 0.7of 0.7--6 % patient years.6 % patient years.

Our experience Our experience ►► During the time period of 2001During the time period of 2001--2007 , 2007 , 480 480 mitralmitral
valve replacements with prosthetic valve were valve replacements with prosthetic valve were performed in our service: performed in our service: 407 407 bileafletbileaflet (SJM) , (SJM) , 6767monoleafletmonoleaflet ( 35 ( 35 SorinSorin, 32 , 32 CarbomedixCarbomedix) and ) and 6 6 bioproshtesisbioproshtesis..
►► 9 emergent re9 emergent re--operations because PVToperations because PVT(0.01%).(0.01%).3 cases with 3 cases with bileafletbileaflet PVT ( SJM), 6 cases with PVT ( SJM), 6 cases with monoleafletmonoleaflet PVT( 4 PVT( 4 SorinSorin, 2 Medtronic). In , 2 Medtronic). In six casessix casesthrombus and thrombus and pannuspannus was found. was found. In In ––hospital hospital mortality of PVT remortality of PVT re--operations was 0operations was 0. In our . In our experience experience subtherapeuticsubtherapeutic anticoagulation is anticoagulation is found to be the found to be the most powerful predictor of PVT most powerful predictor of PVT and and thrombembolicthrombembolic complicationscomplications..

Our experienceOur experience
►►Heparin was proven successful in three Heparin was proven successful in three other cases of Left other cases of Left atrialatrial thrombosis in our thrombosis in our service: service: 2 cases with LAA thrombi2 cases with LAA thrombi1 with 1 with interatrialinteratrial septum aneurysm thrombiseptum aneurysm thrombi

DiagnosisDiagnosis--echocardiographyechocardiography
TransthoracicTransthoracic echocardiographyechocardiography►► TransvalvularTransvalvular flow gradientflow gradient►►Inspection of the prosthesisInspection of the prosthesis
( Class I recommendation, level of evidence B; ACC/AHA ( Class I recommendation, level of evidence B; ACC/AHA valve disease guidelines 2006)valve disease guidelines 2006)

DiagnosisDiagnosis--echocardiographyechocardiography
TransoesophagealTransoesophageal echocardiographyechocardiography
TEE is currently the test of choice forTEE is currently the test of choice for►► diagnosisdiagnosis►► guiding the therapeutic strategyguiding the therapeutic strategy: :
thrombus burdenthrombus burden►► assessing the treatment efficacyassessing the treatment efficacy
(Class I recommendation, level of evidence B; ACC/AHA (Class I recommendation, level of evidence B; ACC/AHA valve disease guidelines 2006)valve disease guidelines 2006)

TreatmentTreatment
Although surgical treatment is usually Although surgical treatment is usually preferred in cases of obstructive PVT preferred in cases of obstructive PVT optimal treatment remains controversialoptimal treatment remains controversial
Different therapeutic modalities availableDifferent therapeutic modalities available►►SurgerySurgery►►Heparin treatmentHeparin treatment►►FibrinolisisFibrinolisis
TreatmentTreatment
Choice betweenChoice between surgery surgery and and medicalmedicaltreatmenttreatment is influenced by:is influenced by:
►► presence of presence of valvularvalvular obstructionobstruction►► valve location (leftvalve location (left--or right sided)or right sided)►► thrombus sizethrombus size►► clinical statusclinical status
TreatmentTreatment
►►First successful First successful thrombolyticthrombolytic treatment of a treatment of a thrombosedthrombosed StarrStarr--Edwards prosthesis in Edwards prosthesis in tricuspid position was reported by tricuspid position was reported by LuluagaLuluagaet al in 1971.et al in 1971.
►►Since than Since than thrombolyticthrombolytic therapy has therapy has emerged as an alternative to reemerged as an alternative to re--operation.operation.
►►Case reports and series vary widely in the Case reports and series vary widely in the mortality and morbidity rate associated with mortality and morbidity rate associated with thrombosis , more than in rate of success.thrombosis , more than in rate of success.

TreatmentTreatment
Definition ofDefinition ofThrombolyticThrombolytic successsuccess : A reduction >75 % in : A reduction >75 % in
thrombus largest diameter.thrombus largest diameter.HemodinamicHemodinamic successsuccess : :
Complete Complete HemodinamicHemodinamic successsuccess : Return of : Return of the the transvalvulartransvalvular gradient in normal range.gradient in normal range.Partial Partial HemodynamicHemodynamic successsuccess : partial : partial improvement of the improvement of the transvalvulartransvalvular gradient gradient
Clinical successClinical success: : HemodynamicHemodynamic success without success without clinical complications.clinical complications.
TreatmentTreatment
ProPro--TEE registry results identified TEE registry results identified
►► thrombus size > 0.8 cm2thrombus size > 0.8 cm2
►► history of previous stroke history of previous stroke
as the major risks factors for complications of as the major risks factors for complications of lyticlytictreatmenttreatment
JACC 2004JACC 2004

International ProInternational Pro--TEE registry recommendations TEE registry recommendations Left sided obstructive thrombiLeft sided obstructive thrombi
Thrombus sizeThrombus size
Thrombus< 0.8cm2 Thrombus >0.8cm2Thrombus< 0.8cm2 Thrombus >0.8cm2
ThrombolysisThrombolysis Surgical Surgical vsvs lyticlytic risk risk
yes lower surgical risyes lower surgical risk nok no
thrombolysisthrombolysis surgery surgery

ProPro--TEE registry resultsTEE registry results
Relationship of thrombus area to overall complication and Relationship of thrombus area to overall complication and death rate . death rate . *p=.003*p=.003 **p <.0001 **p <.0001 øøpp=.016=.016

ProPro--TEE registry resultsTEE registry results
Incidence of complication and death rate according to theIncidence of complication and death rate according to thepresence and absence of the two risk factors ( RF) presence and absence of the two risk factors ( RF) thrombus areathrombus area and and previous strokeprevious stroke

TreatmentTreatmentNon obstructive leftNon obstructive left--sided PVTsided PVT
►► Large ( > 5 mm) thrombiLarge ( > 5 mm) thrombisurgerysurgery in case of failure to medical in case of failure to medical treatment ( treatment ( heparinheparin), particularly in the ), particularly in the presence of mobile and presence of mobile and pedunculatedpedunculatedthrombi. thrombi.
►► Small (< 5mm) thrombiSmall (< 5mm) thrombi--medical treatment:medical treatment:heparinheparin or or warfarinwarfarin plus 100mg aspirinplus 100mg aspirinHeparin treatment aloneHeparin treatment alone in pts with fresh in pts with fresh large mobile thrombi and large mobile thrombi and subtherapeuticsubtherapeuticanticoagulation has been demonstrated anticoagulation has been demonstrated successful in case reports successful in case reports
Heart 2007Heart 2007

TreatmentTreatment
Obstructive thrombiObstructive thrombiACC/AHA valve disease guidelines 2006:ACC/AHA valve disease guidelines 2006:Class :Class :IIaIIa , level of evidence : C, level of evidence : C1.1. Emergency operationEmergency operation is is reasonable reasonable for for
the following pts the following pts left sided PVTleft sided PVT..A.A. Pts with NYHA functional Pts with NYHA functional class IIIclass III--IV IV symptoms.symptoms.B .B . Pts with Pts with large clot burdenlarge clot burden
2.2. FibrinoliticFibrinolitic is reasonableis reasonable for for thrombosedthrombosedright sided prosthetic right sided prosthetic valve with NYHA valve with NYHA functional functional class IIIclass III--IV IV symptoms or symptoms or large clot large clot burdenburden

TreatmentTreatment
►► Class II BClass II B1.1. FibrinoliticFibrinolitic therapytherapy as a first as a first ––line treatmentline treatmentIn In left side PV Tleft side PV T for the following ptsfor the following ptsA.A. Pts with NYHA functional class Pts with NYHA functional class II--II symptoms II symptoms , ,
and a and a small clot burden small clot burden (level of evidence : B)(level of evidence : B)
B.B. Pts with NYHA Pts with NYHA class IIIclass III--IV IV symptoms and symptoms and a small a small clot burden if emergency surgery is of high risk or clot burden if emergency surgery is of high risk or not available not available (level of evidence : B)(level of evidence : B)

TreatmentTreatment
C . Pts with obstructive PVT , NYHA class III-IV and a large clot burden if emergency surgery is high risk or not available ( Level of evidence C )
2 . Intravenous heparin as an alternative to fibrinolitic therapy for pts in NYHA I-II and a small clot burden

ESC guidelines 2007

ESC guidelines 2007

Thank you for your attention