Thrombosis Canada Clinical Tools Perioperative Management ...
61
Thrombosis Canada Clinical Tools Perioperative Management of Anticoagulants Antithrombotic Use in Atrial Fibrillation Dr. Benjamin Bell, MD FRCPC Staff General Internist North York General Hospital Lecturer, University of Toronto Executive Member, Thrombosis Canada Dr. Pascal Bastien, MD FRCPC Head, Division of General Internal Medicine North York General Hospital Lecturer, University of Toronto Member, Thrombosis Canada
Transcript of Thrombosis Canada Clinical Tools Perioperative Management ...

Thrombosis Canada Clinical Tools
Perioperative Management of AnticoagulantsAntithrombotic Use in Atrial Fibrillation
Dr. Benjamin Bell, MD FRCPCStaff General Internist
North York General HospitalLecturer, University of TorontoExecutive Member, Thrombosis Canada
Dr. Pascal Bastien, MD FRCPCHead, Division of General Internal Medicine
North York General HospitalLecturer, University of TorontoMember, Thrombosis Canada

Faculty/Presenter Disclosure
• Faculty: Dr. Benjamin Bell• Relationships with commercial interests:*
– Grants/Research Support: N/A– Speakers Bureau/Honoraria: Bayer– Advisory Boards: Bristol Meyers Squibb/Pfizer and Sanofi Aventis – Consulting Fees: N/A– Other: N/A

Faculty/Presenter Disclosure
• Faculty: Dr. Pascal Bastien• Relationships with commercial interests:*
– Grants/Research Support: N/A– Speakers Bureau/Honoraria: Bayer– Advisory Boards: Sanofi Aventis – Consulting Fees: N/A– Other: N/A

Disclosure of Commercial Support• This program has received financial support from Alexion Canada, Leo
Pharma, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Covidien, Novartis, Octapharma, BMS/Pfizer Alliance, Pfizer Canada Injectables, Aspen Pharmacare and Sanofi in the form of an Unrestricted Educational Grant
• This program has not received in-kind support from any commercial organization
• Potential for conflict(s) of interest:– Thrombosis Canada developed a free clinical app that will be discussed
in this program

Mitigating Potential Bias
• No commercial or other non-commercial organization have had any input to the content of this program
• No commercial or other non-commercial organization have been present at or privy to any discussions, meetings, or other activities related to the content of this program

Stroke Prevention in Atrial Fibrillation
Dr. Pascal Bastien, MD FRCPCHead, Division of General
Internal MedicineNorth York General Hospital
Lecturer, University of TorontoMember, Thrombosis Canada

Objectives
• Review updated CCS algorithm from 2014 Atrial Fibrillation guidelines
• Describe the complementary roles of NOACs and warfarin in stroke prevention in atrial fibrillation
• Showcase a safe, effective and prompt strategy to assist in the choice and dosing of antithrombotics for atrial fibrillation

Atrial Fibrillation Scope of Problem
• AF is responsible for a 5‐ to 7‐fold increase in stroke risk
• 350,000 Canadians have AF• Prevalence of AF increases with age
– 0.5% in patients 55‐59 yo– 10% in patients ≥ 80 yo
• Almost all patients with AF should be anticoagulated

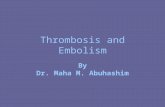
Projected Number of Adults with AF in USA between 1995 and 2050
Go AS, et al. JAMA. 2001;285(18):2370–2375.

CCS Guidelines for AF Stroke Prevention
CHADS2 CHA2DS2‐VASc CCS algorithm

Case 1
• 36 yo woman, otherwise healthy, complaining of palpitations
• She undergoes a 48h Holter and is found to have symptomatic paroxysms of AF
• Rate vs. rhythm control• Stroke prophylaxis

Rate vs. Rhythm Control

Audience Poll: What antithrombotic agent would you recommend for this woman?A. WarfarinB. DabigatranC. AspirinD. None
A. B. C. D.
0% 0%0%0%
10
Stroke Prophylaxis

Is there an app for that?

Take Home Point 1
• Not all patients with AF need to receive antithrombotic therapy
• Female sex alone is not sufficient to justify antithrombotic therapy in AF

Case 2
• 54 yo man, current smoker, with history CAD but no CHADS risk factors
• A routine ECG incidentally shows AF at 94 bpm
• Rate vs. rhythm control• Stroke prophylaxis

Is there an app for that?

Take Home Point 2
• Aspirin is an appropriate antithrombotic agent in a select group of patients.
• Vascular disease alone is not sufficient to justify OAC in AF (in contrast to ESC guidelines)

Case 3
• 75 year old man with diabetic nephropathy and ESRD on dialysis (guidelines suggest that warfarin is favored if GFR<30).

Is there an app for that?

Take Home Point 3
• Warfarin remains the agent of choice for AF in a number of circumstances– CrCl < 30cc/min *– AF with rheumatic mitral stenosis– Poor medication adherence (although failure to undergo blood testing favors NOAC)
– In association with another indication for warfarin• eg. mechanical valve, LV thrombus

Case 4
• 85 yo man with hypertension, diabetes, CKD (CrCl 55) and atrial fibrillation. His weight is 60kg.

Audience Poll: Most appropriate agent for stroke prevention*A. Dabigatran 150 mg BIDB. Dabigatran 110 mg BIDC. Rivaroxaban 20 mg ODD. Rivaroxaban 15 mg ODE. Apixaban 5 mg BIDF. Apixaban 2.5 mg BIDG. Warfarin
A. B. C. D. E. F. G.
0% 0% 0% 0%0%0%0%
10
*there’s more than 1 right choice!

Patient has risk factor for stroke
Estimate CrCl
<30 mL/min
30‐49 mL/min
>50 mL/min
Elderly and/or risk
factors forbleeding
Age <75 years
Age 75‐80 years
Age >80 years
110mg BID 150mg BID 150mg BID 110mg BID 110mg BID150mg BID
Contra‐indicated
One other risk factor
for bleeding
Dabigatran
Recommended dose
Dose can be considered
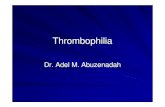
Canadian Dosing Recommendations for Stroke Prevention in AF

Canadian Dosing Recommendations for Stroke Prevention in AF
Patient has risk factor for
stroke
Estimate CrCl
30‐49 mL/min
>50 mL/min
20 mg OD15 mg OD
<30 mL/min
Not recommended
Rivaroxaban
Recommended dose*Rivaroxaban 15mg and 20mg should be taken with food

Canadian Dosing Recommendations for Stroke Prevention in AF
Recommended dose
Apixaban
Patient has risk factor for stroke
Estimate CrCl
≥25 mL/min
5 mg BID2.5 mg BID
<15 mL/min
Not recommended
Check Age Check Weight
Check Serum Creatinine
≥ 80 years ≤ 60 kg≥ 133
micromol/L
If ≥ 2 features
If ≤ 1 features
≥15 ‐24
mL/min
No dosing recommendation can be made*
* In patients with eCrCL 15 ‐ 24 mL/min, no dosing recommendation can be made as clinical data are very limited

Is there an app for that?

Take Home Point 4
• NOACs are considered first line over warfarin, in most patients, but require appropriate dosing.

Perioperative Management of Anticoagulants
November 2014Benjamin Bell, MD FRCPC
Staff General Internist, North York General HospitalExecutive Member, Thrombosis Canada

Objectives
• Develop an evidence‐based approach to the perioperative management of anticoagulants
• Accurately risk stratify patients• Bleeding risk associated with procedure• Thrombotic risk associated with indication
• Introduce online, point of care tools and apps

Case• Dentist calls• 81 year old male patient needs a few teeth pulled
• On rivaroxaban 15 mg daily• AF, hypertension, diabetes, CKD (eGFR 35mL/min)
• Dentist wants to know how to manage anticoagulant

Audience Poll: Your Advice?A. Discontinue
rivaroxaban 5 days before procedure
B. Discontinue rivaroxaban 2 days before procedure
C. Continue rivaroxaban
A. B. C.
0% 0%0%
10

Recommended risk assessment algorithm1. What is the
procedural risk of bleeding?
2. What is the patient’s risk of thrombosis?
3. Which antithrombotic agent is/are being used and what is its half‐life?
Surgicalbleeding risk
Patientthrombosis risk

Guidelines

Is there an app for that?

Recommended risk assessment algorithm1. What is the
procedural risk of bleeding?
2. What is the patient’s risk of thrombosis?
3. Which antithrombotic agent is/are being used and what is its half‐life?
Surgicalbleeding risk
Patientthrombosis risk

Procedural risk of bleeding
• Low
• Moderate (2 day risk of major bleed 0‐2%)
• High (2 day risk of major bleed 2‐4%)
Continue antithrombotic
Hold antithrombotic
Hold antithrombotic

Procedural risk of bleedingModerate risk procedures(2‐day risk of major bleed 0%‐2%)• Cholecystectomy• Abdominal hysterectomy
• Carpal tunnel repair
• Knee/hip replacement and shoulder/foot/hand surgery and arthroscopy
• Dilatation and curettage
• Skin cancer excision
• Abdominal hernia repair
• Axillary node dissection
• Hydrocele repair• Noncataract eye surgery
• Noncoronary angiography
• Bronchoscopy ±biopsy
• Cutaneous and bladder/prostate/ thyroid/breast/lymph node biopsies
High risk procedures(2‐day risk of major bleed 2%‐4%)• Any major operation (duration > 45 minutes)
• Any procedure involving neuraxial anesthesia
• Heart valve replacement
• Coronary artery bypass
• Abdominal aortic aneurysm repair
• Neurosurgical/urologic/head and neck/abdominal/breast cancer surgery
• Laminectomy• TURP• Kidney biopsy• Polypectomy, variceal treatment, biliary sphincterectomy, pneumatic dilatation
• PEG placement• Endoscopically guided fine‐needle aspiration
• Vascular surgery• Bilateral knee replacement
Blood. 2012;120(15):2954‐2962

Very low risk procedures• Minor dental procedures
• Conservation work• Prosthodontics• Scaling/polishing• Extractions (single and multiple)
• Endodontics• Minor dermatologic procedures
• Skin biopsy• Excisions
• Cataract extraction• Endoscopy withoutadvanced therapeutic procedures (eg. polypectomy)

Managing bleeding
• Local hemostatic measures• Ensure INR in therapeutic range• Avoidance of NSAID for postoperative pain control• Dental procedures
• Use of tranexamic mouthwash (5cc before procedure and QID x 2 days following procedure)

What about warfarin?
• Same approach!

Take home points
• There is no need to hold anticoagulation (including NOACs) for procedures associated low bleeding risk
• Avoid NSAIDs for analgesia
• Local hemostatic measures will manage bleeding

Case• 78 F severe OA• Scheduled for L TKA next week
• Seen in the preoperative clinic by an internist last week
• Mechanical mitral valve for severe MS
• AF, HTN, CKD (CrCl~45mL/min)
• On warfarin 3.5 mg OD, amlodipine 5 mg OD
• Doesn’t trust whatever the “hospital doctor” said and wants your advice for warfarin

Recommended risk assessment algorithm1. What is the
procedural risk of bleeding?
2. What is the patient’s risk of thrombosis?
3. Which antithrombotic agent is/are being used and what is its half‐life?
Surgicalbleeding risk
Patientthrombosis risk

Is there an app for that?

Risk of thrombosis
• Must be considered when anticoagulants are to be held
• Low
• Moderate
• High
No bridging therapy
Consider bridging therapy
Bridging therapy indicated

Risk of thrombosis

Bridging
Time in subtherapeutic range
Time
Degree ofanticoagulation
Warfarin held Intervention
x
x
x

Bridging
Time
Degree ofanticoagulation
Intervention
Time in subtherapeutic range
Warfarin held
x
x
x

Intervention
Time
Degree ofanticoagulation
Bridging
Warfarin held

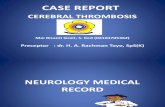
Sample Bridging ProtocolDay Warfarin LMWH
‐6 ✔ X
‐5 X X
‐4 X X
‐3 X ✔
‐2 X ✔
‐1 X ✔*
Surgery X X
+1 ✔ ✔**
+2 ✔ ✔**
+3 ✔ ✔***
* Use half daily dose** If high bleeding risk, hold, or use prophylactic dose LMWH
*** Continue LMWH until INR in therapeutic range

Take home points
• Anticoagulants must be held for patients undergoing moderate/high bleeding risk procedures
• Bridging with LMWH should be considered for patients at moderate/high risk for thrombosis

Case: but what about the NOACs?• 76 M new BRBPR, Fe deficiency anemia
• Scheduled for colonoscopy with polypectomy expected
• AF, HTN, previous stroke, diabetic CHF, CKD (CrCl~38mL/min)
• On rivaroxaban 15 mg daily, amlodipine 5 mg, Lasix 60 mg, ramipril 10 mg, metformin 1 g BID, sitagliptin 100 mg
• GI on vacation until day before procedure, lost instructions

Recommended risk assessment algorithm1. What is the
procedural risk of bleeding?
2. What is the patient’s risk of thrombosis?
3. Which antithrombotic agent is/are being used and what is its half‐life?
Surgicalbleeding risk
Patientthrombosis risk

Is there an app for that?

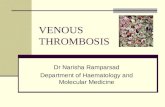
Drug pharmacology
Drug Renal clearance
c‐max t ½ CrCl >50 t ½ CrCl 30‐50
Dabigatran 80% 2h 14h 18h
Rivaroxaban 33% 4h 8h 9h
Apixaban 25% 4h 7h 17h
Dalteparin 70% 4h 2‐5h 4‐8h
Blood. 2012;120(15):2954‐2962

Bridging
Time
Degree ofanticoagulation
NOAC held
Intervention
Time in subtherapeutic range

How long to hold the drug?
Blood. 2012;120(15):2954‐2962

Take home points
• Bridging anticoagulation is virtually never indicated for patients treated with a NOAC
• Duration off the drug depends on patient renal function and surgical bleeding risk

Take home points• Do not withhold anticoagulants for low bleeding risk procedures
• Bridging recommended for patients at high thromboembolic risk undergoing moderate/high bleed risk procedures who are anticoagulated with warfarin
• Bridging is not necessary for patients anticoagulated with NOACs
• Duration of cessation of NOAC depends on agent, renal function and surgical bleeding risk … so use an app to make appropriate recommendations