Thrombosis Ppt
47
Thrombosis Thrombosis
Transcript of Thrombosis Ppt
ThrombosisThrombosis
ThrombosisThrombosis is the process involved in the formation of a is the process involved in the formation of a fibrin blood clot. Both platelets and a series of coagulant fibrin blood clot. Both platelets and a series of coagulant proteins (clotting factors) contribute to clot formation. proteins (clotting factors) contribute to clot formation.
An An embolusembolus is a small part of a clot that breaks off and is a small part of a clot that breaks off and travels to another part of the vascular system. Damage is travels to another part of the vascular system. Damage is
caused when the embolus becomes trapped in a small caused when the embolus becomes trapped in a small vessel, causing occlusion and leading to ischemia or vessel, causing occlusion and leading to ischemia or
infarction of the surrounding tissue. infarction of the surrounding tissue.
Normal clot formation maintains the integrity of the Normal clot formation maintains the integrity of the vasculature in response to injury, but pathological clotting vasculature in response to injury, but pathological clotting can occur in many clinical settings. Abnormal thrombotic can occur in many clinical settings. Abnormal thrombotic
events include deep venous thrombosis (DVT) and its events include deep venous thrombosis (DVT) and its primary complication, pulmonary embolism (PE), as well primary complication, pulmonary embolism (PE), as well
as stroke and other systemic manifestations of as stroke and other systemic manifestations of embolization of clots that form within the heart. embolization of clots that form within the heart.
Anticoagulant drug therapy is aimed at preventing Anticoagulant drug therapy is aimed at preventing pathological clot formation in patients at risk and at pathological clot formation in patients at risk and at
preventing clot extension and/or embolization in patients preventing clot extension and/or embolization in patients
who have developed thrombosis.who have developed thrombosis.
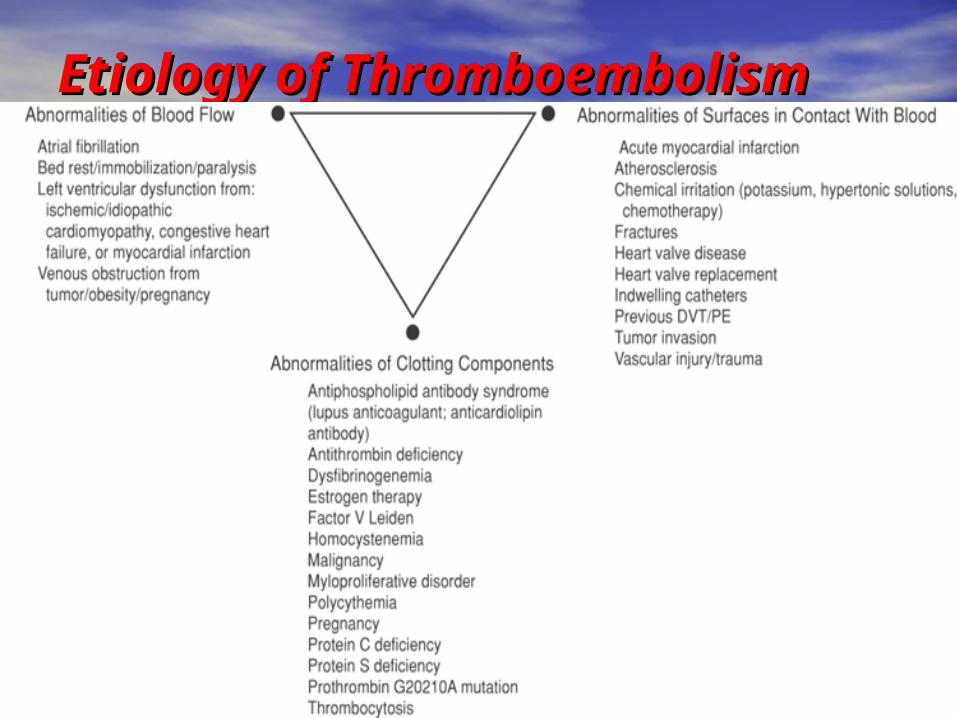
Etiology of Etiology of ThromboembolismThromboembolism
Clot FormationClot FormationThe intact endothelial lining of blood vessels normally The intact endothelial lining of blood vessels normally repels platelets and inhibits clot formation through repels platelets and inhibits clot formation through secretion of numerous inhibitory substances. Damage to secretion of numerous inhibitory substances. Damage to the endothelium leads to exposure of circulating blood to the endothelium leads to exposure of circulating blood to subendothelial substances, and this results in a complex subendothelial substances, and this results in a complex series of events, including platelet adhesion activation, series of events, including platelet adhesion activation, and aggregation, followed by activation of the clotting and aggregation, followed by activation of the clotting cascade. These events result in formation of a fibrin clot.cascade. These events result in formation of a fibrin clot.Platelet Adhesion, Activation, and AggregationPlatelet Adhesion, Activation, and AggregationEndothelial damage leads to exposure of blood to Endothelial damage leads to exposure of blood to subendothelial collagen and phospholipids, resulting in subendothelial collagen and phospholipids, resulting in platelet adhesion to the surface. von Willebrand factor platelet adhesion to the surface. von Willebrand factor serves as the binding ligand for platelet adhesion, via the serves as the binding ligand for platelet adhesion, via the glycoprotein I (GPI) receptor on the platelet surface. glycoprotein I (GPI) receptor on the platelet surface. Adhered platelets become activated and release Adhered platelets become activated and release numerous compounds, including adenosine diphosphate numerous compounds, including adenosine diphosphate and thromboxane A2, which stimulate platelet and thromboxane A2, which stimulate platelet aggregation. Fibrinogen serves as the binding ligand for aggregation. Fibrinogen serves as the binding ligand for platelet aggregation, via the GPIIb/IIIa receptor on the platelet aggregation, via the GPIIb/IIIa receptor on the platelet surface.platelet surface.
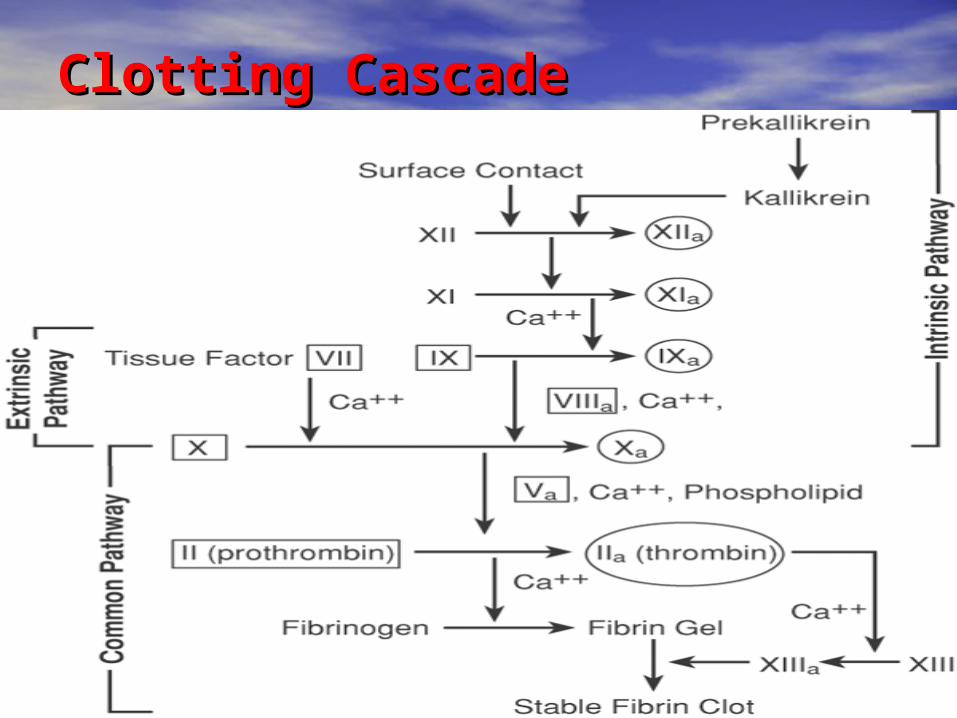
Clotting CascadeClotting Cascade
Pathological ThrombiPathological Thrombi Arterial thrombiArterial thrombi are composed primarily of platelets, are composed primarily of platelets, although they also contain fibrin and occasional although they also contain fibrin and occasional leukocytes. Arterial thrombi generally occur in areas of leukocytes. Arterial thrombi generally occur in areas of rapid blood flow (i.e., arteries) and are typically initiated rapid blood flow (i.e., arteries) and are typically initiated by spontaneous or mechanical rupture of atherosclerotic by spontaneous or mechanical rupture of atherosclerotic plaques. plaques.
Venous Venous thrombi are found primarily in the venous thrombi are found primarily in the venous circulation and are composed almost entirely of fibrin and circulation and are composed almost entirely of fibrin and erythrocytes. Venous thrombi have a small platelet head erythrocytes. Venous thrombi have a small platelet head and generally form in response to either venous stasis or and generally form in response to either venous stasis or vascular injury after surgery or trauma. The areas of vascular injury after surgery or trauma. The areas of stasis prevent dilution of activated coagulation factors by stasis prevent dilution of activated coagulation factors by normal blood flow.normal blood flow.
The selection of an antithrombotic agent may be The selection of an antithrombotic agent may be influenced by the type of thrombus to be treated. influenced by the type of thrombus to be treated. Fibrinolytic agents are used for rapid dissolution of Fibrinolytic agents are used for rapid dissolution of thromboemboli, most notably during myocardial infarction thromboemboli, most notably during myocardial infarction (MI).(MI).

Pharmacology of Antithrombotic AgentsPharmacology of Antithrombotic AgentsHeparinHeparinHeparin is a rapid-acting anticoagulant that is Heparin is a rapid-acting anticoagulant that is administered parenterally. Standard heparin administered parenterally. Standard heparin (unfractionated heparin [UFH]) obtained from (unfractionated heparin [UFH]) obtained from bovine lung or porcine intestinal mucosa. The bovine lung or porcine intestinal mucosa. The action of heparin is facilitated by its binding to action of heparin is facilitated by its binding to the naturally circulating anticoagulant the naturally circulating anticoagulant antithrombin (AT). The heparin–AT complex antithrombin (AT). The heparin–AT complex attaches to and irreversibly inactivates factor IIa attaches to and irreversibly inactivates factor IIa (thrombin) and factor Xa, as well as activated (thrombin) and factor Xa, as well as activated factors IX, XI, and XII .Approximately one-third of factors IX, XI, and XII .Approximately one-third of the molecules present in UFH bind to AT and the molecules present in UFH bind to AT and provide the anticoagulant properties of heparin. provide the anticoagulant properties of heparin. The remaining two-thirds of the heparin The remaining two-thirds of the heparin molecules bind to plasma proteins and to molecules bind to plasma proteins and to endothelial cells, and limit its bioavailability.endothelial cells, and limit its bioavailability.
In cases of acute DVT or PE, the clotting cascade has In cases of acute DVT or PE, the clotting cascade has been activated, generating abnormal quantities of been activated, generating abnormal quantities of thrombin and fibrin. In these situations, thrombin must be thrombin and fibrin. In these situations, thrombin must be inactivated directly, a process that may require relatively inactivated directly, a process that may require relatively large doses of heparin. However, when the clotting large doses of heparin. However, when the clotting cascade is in a normal balance, it is possible to indirectly cascade is in a normal balance, it is possible to indirectly inactivate thrombin with smaller heparin doses by inactivate thrombin with smaller heparin doses by complexing factor Xa. Because of the amplification effect complexing factor Xa. Because of the amplification effect of the clotting cascade, inactivation of relatively small of the clotting cascade, inactivation of relatively small amounts of factor Xa indirectly prevents the production of amounts of factor Xa indirectly prevents the production of large quantities of thrombin. This phenomenon is the large quantities of thrombin. This phenomenon is the basis for low-dose heparin prophylaxis after surgery or in basis for low-dose heparin prophylaxis after surgery or in cases of prolonged bed rest or immobilization.cases of prolonged bed rest or immobilization.Heparin may be administered intravenously (IV) by Heparin may be administered intravenously (IV) by continuous infusion, or subcutaneously (SC), although its continuous infusion, or subcutaneously (SC), although its bioavailability is significantly reduced by SC bioavailability is significantly reduced by SC administration. Intramuscular administration should be administration. Intramuscular administration should be avoided because of the potential for hematoma avoided because of the potential for hematoma formation.formation.
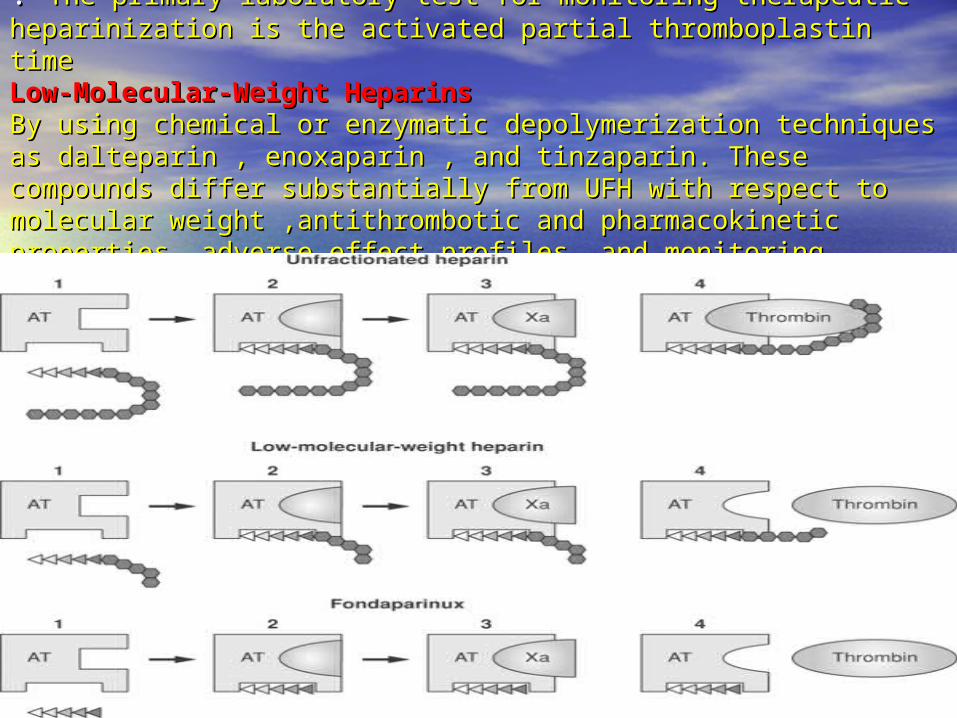
. . The primary laboratory test for monitoring therapeutic The primary laboratory test for monitoring therapeutic heparinization is the activated partial thromboplastin time heparinization is the activated partial thromboplastin time Low-Molecular-Weight HeparinsLow-Molecular-Weight HeparinsBy using chemical or enzymatic depolymerization techniques as By using chemical or enzymatic depolymerization techniques as dalteparin , enoxaparin , and tinzaparin. These compounds differ dalteparin , enoxaparin , and tinzaparin. These compounds differ substantially from UFH with respect to molecular substantially from UFH with respect to molecular weight ,antithrombotic and pharmacokinetic properties, adverse weight ,antithrombotic and pharmacokinetic properties, adverse effect profiles, and monitoring requirements .effect profiles, and monitoring requirements .
. . In general, these compounds are administered In general, these compounds are administered subcutaneously every 12 to 24 hours at fixed doses. subcutaneously every 12 to 24 hours at fixed doses. FondaparinuxFondaparinuxFondaparinux is a selective indirect factor Xa inhibitor. Fondaparinux is a selective indirect factor Xa inhibitor. This agent has a long elimination half-life, allowing for This agent has a long elimination half-life, allowing for once-daily SC administration at a fixed dose without the once-daily SC administration at a fixed dose without the need for routine coagulation monitoring.need for routine coagulation monitoring.
Direct Thrombin InhibitorsDirect Thrombin InhibitorsArgatroban, lepirudin , and bivalirudinArgatroban, lepirudin , and bivalirudin are direct are direct thrombin inhibitors that are used as alternative thrombin inhibitors that are used as alternative anticoagulants in patients with heparin-induced anticoagulants in patients with heparin-induced thrombocytopenia.. These agents are administered by thrombocytopenia.. These agents are administered by continuous infusion and require aPTT monitoring for continuous infusion and require aPTT monitoring for appropriate dosing adjustments. Bivalirudin is also used in appropriate dosing adjustments. Bivalirudin is also used in patients undergoing percutaneous coronary intervention. patients undergoing percutaneous coronary intervention. This agent appears to be associated with a lower rate of This agent appears to be associated with a lower rate of hemorrhagic complications than UFH and may reduce the hemorrhagic complications than UFH and may reduce the need for concurrent therapy with glycoprotein IIb/IIIa need for concurrent therapy with glycoprotein IIb/IIIa receptor antagonistsreceptor antagonists
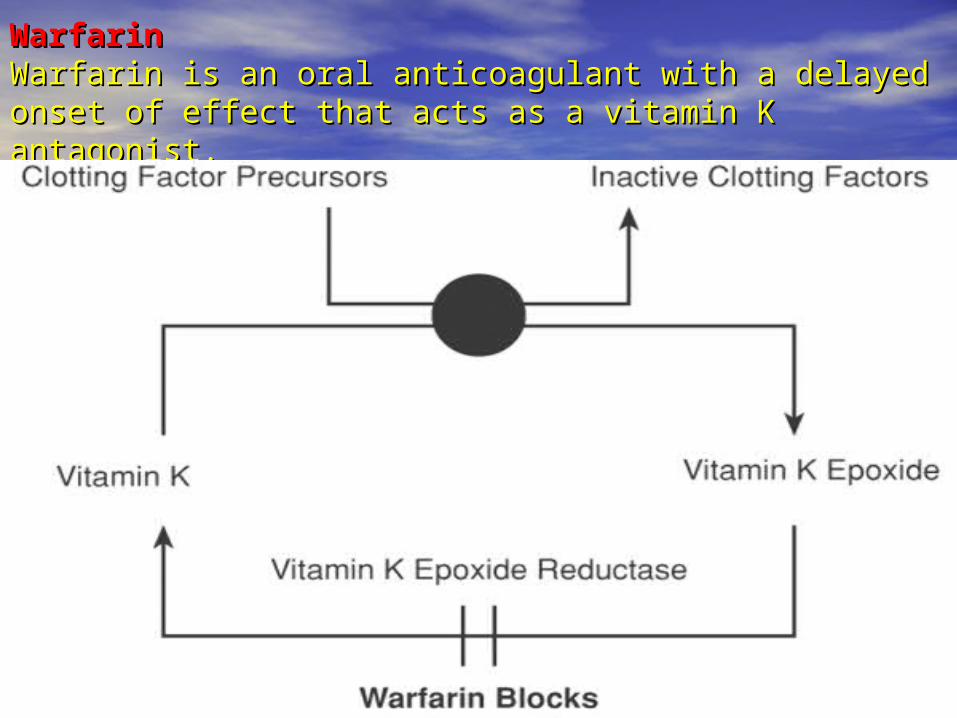
WarfarinWarfarinWarfarin is an oral anticoagulant with a delayed onset of Warfarin is an oral anticoagulant with a delayed onset of effect that acts as a vitamin K antagonist.effect that acts as a vitamin K antagonist.
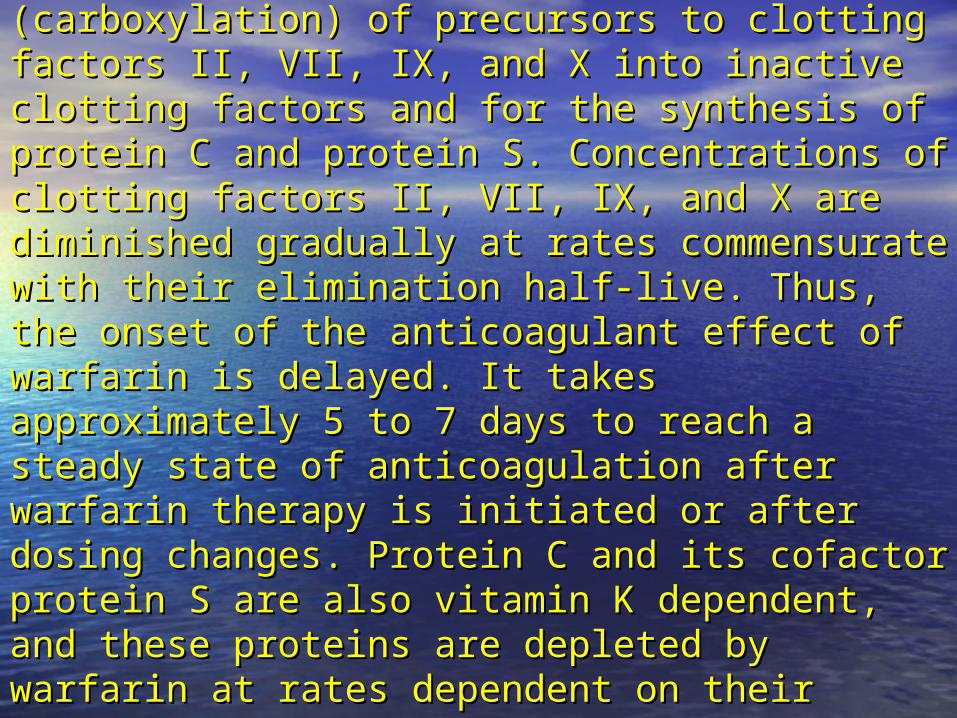
Vitamin K is essential for the conversion Vitamin K is essential for the conversion (carboxylation) of precursors to clotting factors II, (carboxylation) of precursors to clotting factors II, VII, IX, and X into inactive clotting factors and for VII, IX, and X into inactive clotting factors and for the synthesis of protein C and protein S. the synthesis of protein C and protein S. Concentrations of clotting factors II, VII, IX, and X Concentrations of clotting factors II, VII, IX, and X are diminished gradually at rates commensurate are diminished gradually at rates commensurate with their elimination half-live. Thus, the onset of with their elimination half-live. Thus, the onset of the anticoagulant effect of warfarin is delayed. It the anticoagulant effect of warfarin is delayed. It takes approximately 5 to 7 days to reach a takes approximately 5 to 7 days to reach a steady state of anticoagulation after warfarin steady state of anticoagulation after warfarin therapy is initiated or after dosing changes. therapy is initiated or after dosing changes. Protein C and its cofactor protein S are also Protein C and its cofactor protein S are also vitamin K dependent, and these proteins are vitamin K dependent, and these proteins are depleted by warfarin at rates dependent on their depleted by warfarin at rates dependent on their elimination half-lives.elimination half-lives.
Warfarin is rapidly and completely absorbed in the upper Warfarin is rapidly and completely absorbed in the upper gastrointestinal (GI) tract by passive diffusion . It is gastrointestinal (GI) tract by passive diffusion . It is approximately 99% bound to serum albumin. The volume approximately 99% bound to serum albumin. The volume of distribution (Vd) for warfarin is 12.5% of body weight.. of distribution (Vd) for warfarin is 12.5% of body weight.. The primary laboratory test for monitoring warfarin The primary laboratory test for monitoring warfarin therapy is the prothrombin time (PT).therapy is the prothrombin time (PT).Warfarin is administered orally as a racemic mixture Warfarin is administered orally as a racemic mixture containing equal parts of the enantiomers R(+)-warfarin containing equal parts of the enantiomers R(+)-warfarin and S(–)-warfarin. The S(–)-isomer is 2.7 to 3.8 times more and S(–)-warfarin. The S(–)-isomer is 2.7 to 3.8 times more potent as an anticoagulant than the R(+)-isomer, has a potent as an anticoagulant than the R(+)-isomer, has a longer elimination half-life, and is primarily metabolized longer elimination half-life, and is primarily metabolized by cytochrome P450 (CYP)-2C9. Comparatively, R(+)-by cytochrome P450 (CYP)-2C9. Comparatively, R(+)-warfarin is metabolized by primarily by CYP1A2 and warfarin is metabolized by primarily by CYP1A2 and CYP3A4. Many drugs interact with warfarin by CYP3A4. Many drugs interact with warfarin by stereoselectively inhibiting the metabolism of either the stereoselectively inhibiting the metabolism of either the R(+)-isomer or the S(–)-isomer. Genetic expression of R(+)-isomer or the S(–)-isomer. Genetic expression of CYP2C9 influences the rate of metabolism of warfarin and CYP2C9 influences the rate of metabolism of warfarin and thus impacts dosing requirements to meet a particular thus impacts dosing requirements to meet a particular therapeutic endtherapeutic end
Tests Used to Monitor Antithrombotic TherapyTests Used to Monitor Antithrombotic TherapyBefore the initiation of antithrombotic therapy,The Before the initiation of antithrombotic therapy,The clinician should obtain a baseline platelet count and clinician should obtain a baseline platelet count and hematocrit (Hct), as well as evaluate the baseline hematocrit (Hct), as well as evaluate the baseline integrity of the extrinsic and intrinsic coagulation integrity of the extrinsic and intrinsic coagulation pathways with PT and aPTT, the tests used to monitor pathways with PT and aPTT, the tests used to monitor warfarin and heparin, respectively.warfarin and heparin, respectively.
Prothrombin Time/International Normalized RatioProthrombin Time/International Normalized RatioThe PT is prolonged by deficiencies of clotting factors II, V, The PT is prolonged by deficiencies of clotting factors II, V, VII, and X, as well as by low levels of fibrinogen and very VII, and X, as well as by low levels of fibrinogen and very high levels of heparin. It reflects alterations in the high levels of heparin. It reflects alterations in the extrinsic and common pathways of the clotting cascade, extrinsic and common pathways of the clotting cascade, but not in the intrinsic system. The PT is measured by but not in the intrinsic system. The PT is measured by adding calcium and tissue thromboplastin to a sample of adding calcium and tissue thromboplastin to a sample of plasma from which platelets have been removed by plasma from which platelets have been removed by centrifugation. The time to clot formation is detected by centrifugation. The time to clot formation is detected by automated instruments using light-scattering techniques automated instruments using light-scattering techniques that measure optical density. The mean normal PT is that measure optical density. The mean normal PT is
approximately 12 seconds approximately 12 seconds ..
The thromboplastins used in PT monitoring are extracted The thromboplastins used in PT monitoring are extracted from various tissue sources by a number of techniques from various tissue sources by a number of techniques and prepared for commercial use as reagents.and prepared for commercial use as reagents. Unfortunately, thromboplastins are not standardized Unfortunately, thromboplastins are not standardized among manufacturers or among batches of reagent among manufacturers or among batches of reagent produced by the same manufacturer, leading to produced by the same manufacturer, leading to significant variability in PT results for anticoagulated significant variability in PT results for anticoagulated patients. patients. To standardize PT results, the WHO developed a system To standardize PT results, the WHO developed a system by which all commercially available thromboplastins are by which all commercially available thromboplastins are compared with an international reference thromboplastin compared with an international reference thromboplastin and then assigned an International Sensitivity Index (ISI). and then assigned an International Sensitivity Index (ISI). This value is used to mathematically convert PT to the This value is used to mathematically convert PT to the international normalized ratio (INR) by exponentially international normalized ratio (INR) by exponentially multiplying the PT ratio to the power of the ISI of the multiplying the PT ratio to the power of the ISI of the thromboplastin being used in the laboratory to measure thromboplastin being used in the laboratory to measure the test (INR = [PT patient/PT mean normal]ISI). The ISI of the test (INR = [PT patient/PT mean normal]ISI). The ISI of the international reference thromboplastin is 1.0.the international reference thromboplastin is 1.0.
INR is the internationally recognized standard for INR is the internationally recognized standard for monitoring warfarin therapy. Regular-intensity monitoring warfarin therapy. Regular-intensity therapy is defined as dosing warfarin to reach a therapy is defined as dosing warfarin to reach a goal INR of 2.5 (range, 2.0–3.0) and is appropriate goal INR of 2.5 (range, 2.0–3.0) and is appropriate for most settings that require the prevention for most settings that require the prevention and/or treatment of thromboembolic disease. and/or treatment of thromboembolic disease. High-intensity therapy is used in mechanical High-intensity therapy is used in mechanical valve replacement and certain situations of valve replacement and certain situations of thromboembolic recurrence, despite adequate thromboembolic recurrence, despite adequate anticoagulation, and is defined as dosing warfarin anticoagulation, and is defined as dosing warfarin to reach a goal INR of 3.0 (range, 2.5–3.5).to reach a goal INR of 3.0 (range, 2.5–3.5).
Activated Partial Thromboplastin TimeActivated Partial Thromboplastin TimeThe aPTT reflects alterations in the intrinsic pathway of The aPTT reflects alterations in the intrinsic pathway of the clotting cascade and is used to monitor heparin the clotting cascade and is used to monitor heparin therapy. Mean normal values vary among reagents, but therapy. Mean normal values vary among reagents, but typically fall between 24 and 36 seconds. Heparinization typically fall between 24 and 36 seconds. Heparinization to prolong the aPTT to 1.5 to 2.5 times the mean normal to prolong the aPTT to 1.5 to 2.5 times the mean normal value historically was considered adequate to prevent value historically was considered adequate to prevent propagation or extension of thrombuspropagation or extension of thrombus
Deep Venous ThrombosisDeep Venous ThrombosisClinical PresentationClinical PresentationSigns and SymptomsSigns and Symptoms1-One of the most reliable, although nonspecific, physical 1-One of the most reliable, although nonspecific, physical findings of DVT is unilateral leg swelling that often isfindings of DVT is unilateral leg swelling that often isaccompanied by warmth and local tenderness or pain.accompanied by warmth and local tenderness or pain.A tender, cordlike entity caused by venous obstruction A tender, cordlike entity caused by venous obstruction can sometimes be palpated in the affected area.can sometimes be palpated in the affected area.2- Discoloration of the affected limb, including pallor from 2- Discoloration of the affected limb, including pallor from arterial spasm, cyanosis from venous obstruction, or a arterial spasm, cyanosis from venous obstruction, or a reddish color from perivascular inflammation, may also reddish color from perivascular inflammation, may also occur. occur. 3-The presence or absence of a positive Homans' sign 3-The presence or absence of a positive Homans' sign (pain behind the knee or calf on dorsiflexion of the foot) is (pain behind the knee or calf on dorsiflexion of the foot) is rarely helpful in making the diagnosis because it is rarely helpful in making the diagnosis because it is present in only about 30% of patients with DVT. Many present in only about 30% of patients with DVT. Many patients (>50%) can present with asymptomatic disease, patients (>50%) can present with asymptomatic disease, Because symptoms of DVT are nonspecific, the diagnosis Because symptoms of DVT are nonspecific, the diagnosis must be confirmed by objective testing.must be confirmed by objective testing.
Risk FactorsRisk FactorsThe diagnosisThe diagnosis of DVT depends not only on the presenting of DVT depends not only on the presenting signs and symptoms, but also on the presence of risk signs and symptoms, but also on the presence of risk factors.. It is common for more than one risk factor to be factors.. It is common for more than one risk factor to be present in patients who develop DVT, and these factors present in patients who develop DVT, and these factors are cumulative in their effectare cumulative in their effect..DiagnosisDiagnosisDiagnostic strategies should include an assessment of Diagnostic strategies should include an assessment of pretest clinical probability (clinical suspicion), D-dimer pretest clinical probability (clinical suspicion), D-dimer assay (an evaluation of the presence of fibrin degradation assay (an evaluation of the presence of fibrin degradation products, indicative of clot formation), and noninvasive products, indicative of clot formation), and noninvasive imaging tests.imaging tests.Despite its limitations as a single diagnostic tool, clinical Despite its limitations as a single diagnostic tool, clinical assessment can improve the diagnostic accuracy of assessment can improve the diagnostic accuracy of noninvasive testing. noninvasive testing. A clinical prediction rule, takes into account signs, A clinical prediction rule, takes into account signs, symptoms, and risk factors to categorize patients as symptoms, and risk factors to categorize patients as being at low, intermediate, or high probability of having a being at low, intermediate, or high probability of having a DVTDVT
The most common noninvasive test is The most common noninvasive test is 1-duplex scanning, 1-duplex scanning, 2-leg scanning 2-leg scanning 3-Doppler ultrasonography 3-Doppler ultrasonography 4- Venography (radiographic visualization of the 4- Venography (radiographic visualization of the involved vessels with injection of radiocontrast involved vessels with injection of radiocontrast material), an invasive diagnostic test, is the most material), an invasive diagnostic test, is the most sensitive and specific method for diagnosis of sensitive and specific method for diagnosis of DVTDVT
TreatmentTreatmentBaseline InformationBaseline InformationIn addition to assessing the integrity of the In addition to assessing the integrity of the clotting process with platelet count, Hct, PT, and clotting process with platelet count, Hct, PT, and aPTT, the patient's baseline renal function should aPTT, the patient's baseline renal function should also be evaluated and documented because also be evaluated and documented because some anticoagulants are renally eliminatedsome anticoagulants are renally eliminated. . Initiation of TherapyInitiation of TherapyPrompt and optimal anticoagulant therapy is Prompt and optimal anticoagulant therapy is indicated to minimize thrombus extension and its indicated to minimize thrombus extension and its vascular complications, as well as to prevent PE. vascular complications, as well as to prevent PE. Treatment options include IV UFH therapy Treatment options include IV UFH therapy initiated with a loading dose followed by a initiated with a loading dose followed by a continuous infusion, adjusted-dose SC UFH, or continuous infusion, adjusted-dose SC UFH, or LMWH or fondaparinux administered by SC LMWH or fondaparinux administered by SC injection.injection.
HeparinHeparinLoading DoseLoading DoseA loading dose of heparin is required for several reasons. A loading dose of heparin is required for several reasons. Although many clinicians historically used standardized Although many clinicians historically used standardized doses of heparin for initiation of therapy (e.g., 5,000-U doses of heparin for initiation of therapy (e.g., 5,000-U loading dose; 1,000-U/hour maintenance dose), this loading dose; 1,000-U/hour maintenance dose), this approach can result in significant delays in reaching a approach can result in significant delays in reaching a therapeutic intensity of anticoagulation. Body weight therapeutic intensity of anticoagulation. Body weight represents the most reliable predictor of heparin dosing represents the most reliable predictor of heparin dosing requirement. For nonobese patients, the use of the actual requirement. For nonobese patients, the use of the actual body weight is recommended to calculate the initial UFH body weight is recommended to calculate the initial UFH dose. In obese patients, the use of the actual body weight dose. In obese patients, the use of the actual body weight is controversial, and the use of an adjusted-dosing weight is controversial, and the use of an adjusted-dosing weight is recommended by some experts.is recommended by some experts. Initial heparin loading doses of 70 to 100 U/kg followed Initial heparin loading doses of 70 to 100 U/kg followed by an infusion rate of 15 to 25 U/kg/hour are commonly by an infusion rate of 15 to 25 U/kg/hour are commonly recommended. Selection of the lower or upper dosage recommended. Selection of the lower or upper dosage range is guided by the severity of the patient's symptoms range is guided by the severity of the patient's symptoms and his or her potential sensitivity to adverse effects.and his or her potential sensitivity to adverse effects.
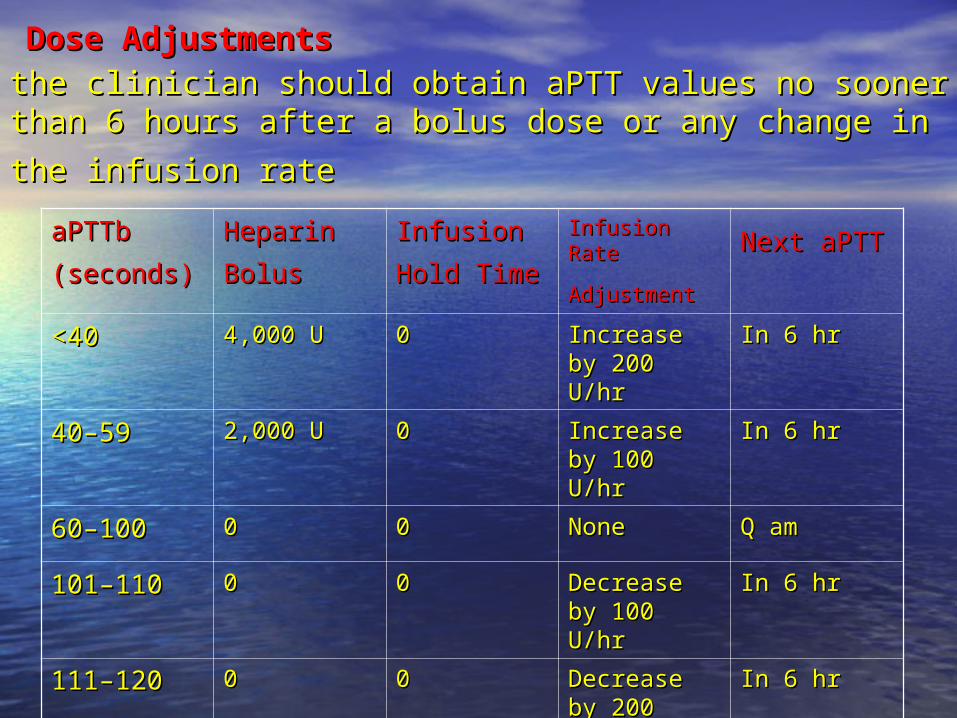
Dose AdjustmentsDose Adjustments the clinician should obtain aPTT values no sooner than 6 the clinician should obtain aPTT values no sooner than 6 hours after a bolus dose or any change in the infusion hours after a bolus dose or any change in the infusion
raterate aPTTb aPTTb
(seconds)(seconds) Heparin Heparin
BolusBolus Infusion Infusion
Hold TimeHold Time Infusion Rate Infusion Rate
AdjustmentAdjustment Next aPTTNext aPTT
<40 <40 4,000 U 4,000 U 00 Increase by Increase by 200 U/hr200 U/hr
In 6 hrIn 6 hr
40–59 40–59 2,000 U 2,000 U 00 Increase by Increase by 100 U/hr 100 U/hr
In 6 hrIn 6 hr
60–10060–100 00 00 None None Q am Q am
101–110 101–110 00 00 Decrease by Decrease by 100 U/hr 100 U/hr
In 6 hrIn 6 hr
111–120111–120 00 00 Decrease by Decrease by 200 U/hr 200 U/hr
In 6 hrIn 6 hr
>120>120 00 30 min. 30 min. Decrease by Decrease by 200 U/hr 200 U/hr
In 6 hrIn 6 hr
Therapeutic MonitoringTherapeutic Monitoring the aPTT should be measured routinely to the aPTT should be measured routinely to guide subsequent dosing adjustments. The guide subsequent dosing adjustments. The aPTT should be evaluated no sooner than 6 aPTT should be evaluated no sooner than 6 hours after the loading dose or after any hours after the loading dose or after any changes in infusion rate, . If dosing is changes in infusion rate, . If dosing is stable, the aPTT should be evaluated once stable, the aPTT should be evaluated once
daily daily Additional monitoring include evaluation for Additional monitoring include evaluation for potential adverse reactions and possible potential adverse reactions and possible therapeutic failure. Hct and platelet count should therapeutic failure. Hct and platelet count should be checked every 1 to 2 days,examined for signs be checked every 1 to 2 days,examined for signs of bleeding, as well as for signs and symptoms of bleeding, as well as for signs and symptoms associated with thrombus extension and PE.associated with thrombus extension and PE.
Duration of TherapDuration of TherapAdherence of a thrombus to the vessel wall and Adherence of a thrombus to the vessel wall and subsequent endothelialization usually takes 7 to 10 days. subsequent endothelialization usually takes 7 to 10 days. However, anticoagulation therapy must generally However, anticoagulation therapy must generally continue for 3 to 6 months to prevent recurrent continue for 3 to 6 months to prevent recurrent thrombosis. Warfarin is preferred for this long-term thrombosis. Warfarin is preferred for this long-term anticoagulation because it can be administered orally, anticoagulation because it can be administered orally, and it is generally initiated on the same day as heparin. and it is generally initiated on the same day as heparin. The long elimination half-life of warfarin and the long The long elimination half-life of warfarin and the long elimination half-lives of clotting factors II and X elimination half-lives of clotting factors II and X necessitate a prolonged period of overlap between necessitate a prolonged period of overlap between warfarin and heparin. Heparin is, therefore, continued for warfarin and heparin. Heparin is, therefore, continued for ≥5 days and until the INR is >2 and stable. Heparin ≥5 days and until the INR is >2 and stable. Heparin therapy should not be discontinued before at least 5 days therapy should not be discontinued before at least 5 days even if the INR is therapeutic before then because of the even if the INR is therapeutic before then because of the time required for adequate elimination of factors II and X time required for adequate elimination of factors II and X by warfarin and the time required to reach its full by warfarin and the time required to reach its full antithrombotic potential. Shortening the duration of antithrombotic potential. Shortening the duration of heparin therapy is associated with an increased risk of heparin therapy is associated with an increased risk of recurrent thrombosis.recurrent thrombosis.
Adverse EffectsAdverse Effects1-1-Thrombocytopenia induced by heparin has two distinct Thrombocytopenia induced by heparin has two distinct presentations.presentations.A- A- Heparin-associated thrombocytopenia (HAT)Heparin-associated thrombocytopenia (HAT) occurs as occurs as a direct effect of heparin on platelet function, causing a direct effect of heparin on platelet function, causing transient platelet sequestration and clumping with transient platelet sequestration and clumping with reductions in platelet count, but usually remaining reductions in platelet count, but usually remaining >100,000/mm3. This reversible form of thrombocytopenia >100,000/mm3. This reversible form of thrombocytopenia occurs within the first several days of heparin therapy. occurs within the first several days of heparin therapy. Patients remain asymptomatic, and platelet counts return Patients remain asymptomatic, and platelet counts return to normal even when heparin therapy is continuedto normal even when heparin therapy is continuedB-Reductions in platelet count of >50% from baseline B-Reductions in platelet count of >50% from baseline suggest the development of heparin-induced suggest the development of heparin-induced thrombocytopenia (HIT),thrombocytopenia (HIT), a more severe immune-mediated a more severe immune-mediated reaction with a typical delay in onset of 5 to 14 days after reaction with a typical delay in onset of 5 to 14 days after the initiation of heparin therapy. In contrast, “immediate-the initiation of heparin therapy. In contrast, “immediate-onset” HIT can occur rapidly (within 24 hours of UFH onset” HIT can occur rapidly (within 24 hours of UFH initiation) in patients previously exposed to heparin.initiation) in patients previously exposed to heparin.
The overall incidence of HIT is <3%-6% . HIT occurs more The overall incidence of HIT is <3%-6% . HIT occurs more frequently with bovine lung heparin than with heparin frequently with bovine lung heparin than with heparin derived from porcine gut mucosa, and also with prolonged derived from porcine gut mucosa, and also with prolonged IV UFH use versus SC UFH. Despite its low incidence, HIT IV UFH use versus SC UFH. Despite its low incidence, HIT is a life-threatening condition with high morbidity and is a life-threatening condition with high morbidity and mortality. Platelet aggregation secondary to HIT can lead mortality. Platelet aggregation secondary to HIT can lead to significant venous and arterial thrombosis, as well as to significant venous and arterial thrombosis, as well as thromboembolic stroke, acute MI, skin necrosis, and thromboembolic stroke, acute MI, skin necrosis, and thrombosis of other major arteries.thrombosis of other major arteries.
In patients who develop HIT, heparin therapy should be In patients who develop HIT, heparin therapy should be stopped immediately, and treatment with an alternative stopped immediately, and treatment with an alternative anticoagulant should be initiated. Although associated anticoagulant should be initiated. Although associated with a lower risk of HIT (<1%) than UFH, LMWH products with a lower risk of HIT (<1%) than UFH, LMWH products are contraindicated in patients with HIT because of a high are contraindicated in patients with HIT because of a high incidence of immunologic cross-reactivity with heparin.incidence of immunologic cross-reactivity with heparin.
HemorrhageHemorrhageBleeding is the most common adverse effect associated with Bleeding is the most common adverse effect associated with heparin.The most common sites for heparin-associated bleeding are heparin.The most common sites for heparin-associated bleeding are soft tissues, the GI and urinary tracts, the nose, and the oral pharynx.soft tissues, the GI and urinary tracts, the nose, and the oral pharynx.
In addition to length of therapy, many factors influence the risk of In addition to length of therapy, many factors influence the risk of bleeding during heparinization, including advanced age, serious bleeding during heparinization, including advanced age, serious comorbid illnesses (heart disease, renal insufficiency, hepatic comorbid illnesses (heart disease, renal insufficiency, hepatic dysfunction, cerebrovascular disease, malignancy, and severe dysfunction, cerebrovascular disease, malignancy, and severe anemia), and concomitant antithrombotic .Soft tissue bleeding anemia), and concomitant antithrombotic .Soft tissue bleeding commonly occurs at sites of recent surgery or trauma. Although an commonly occurs at sites of recent surgery or trauma. Although an elevated aPTT has historically been considered a risk factor for elevated aPTT has historically been considered a risk factor for bleeding complications, several investigators have been unable to bleeding complications, several investigators have been unable to substantiate a relationship between supratherapeutic aPTT values substantiate a relationship between supratherapeutic aPTT values and hemorrhagic effects. In addition, bleeding episodes can occur and hemorrhagic effects. In addition, bleeding episodes can occur when coagulation test results are within the therapeutic range. These when coagulation test results are within the therapeutic range. These conflicting results may be explained in part by the influence of conflicting results may be explained in part by the influence of additional risk factors for bleeding and by the effect of heparin on additional risk factors for bleeding and by the effect of heparin on platelet function and vascular permeability.platelet function and vascular permeability.
He should be questioned and examined for the presence of nose He should be questioned and examined for the presence of nose bleeding (epistaxis), increased tendency to bruise (ecchymosis), bleeding (epistaxis), increased tendency to bruise (ecchymosis), bright red blood in the stool (hematochezia), black or tarry stool bright red blood in the stool (hematochezia), black or tarry stool (melena), or coughing up of blood (hemoptysis).(melena), or coughing up of blood (hemoptysis).
OsteoporosisOsteoporosisThe development of osteoporosis has been associated The development of osteoporosis has been associated with administration of >20,000 U/day of heparin for 6 with administration of >20,000 U/day of heparin for 6 months or longer. Various mechanisms have been months or longer. Various mechanisms have been suggested, but the underlying pathophysiology of this suggested, but the underlying pathophysiology of this rare adverse effect remains unclear. Affected patients rare adverse effect remains unclear. Affected patients may present with bone pain and/or radiographic findings may present with bone pain and/or radiographic findings suggestive of fractures. suggestive of fractures.
HyperkalemiaHyperkalemiaAlthough rare, hyperkalemia has been attributed to Although rare, hyperkalemia has been attributed to heparin-induced inhibition of aldosterone synthesis, heparin-induced inhibition of aldosterone synthesis, appears to be reversible after discontinuation of appears to be reversible after discontinuation of heparin.Patients with diabetes or renal failure may be at heparin.Patients with diabetes or renal failure may be at
greatest riskgreatest risk..
Hypersensitivity ReactionsHypersensitivity ReactionsOther rarely occurring adverse effects associated with Other rarely occurring adverse effects associated with heparin include generalized hypersensitivity reactions, heparin include generalized hypersensitivity reactions, such as urticaria, chills, fever, rash, rhinitis, conjunctivitis, such as urticaria, chills, fever, rash, rhinitis, conjunctivitis, asthma, and angioedema, and a reversible temporal asthma, and angioedema, and a reversible temporal alopeciaalopecia..
Adjusted-Dose Subcutaneous AdministrationAdjusted-Dose Subcutaneous AdministrationThe most common strategy for treatment of venous The most common strategy for treatment of venous thrombosis in hospitalized patients without IV access is thrombosis in hospitalized patients without IV access is the use of SC LMWH . Another alternative is SC the use of SC LMWH . Another alternative is SC administration of unfractionated heparin with adjustment administration of unfractionated heparin with adjustment of dosing to maintain a therapeutic aPTT.Typically, SC of dosing to maintain a therapeutic aPTT.Typically, SC heparin is administered at 12-hour intervals, and aPTT is heparin is administered at 12-hour intervals, and aPTT is monitored at the mid-dosing interval (i.e., 6 hours after a monitored at the mid-dosing interval (i.e., 6 hours after a dose). dose).
Heparin Protocol for Adjusted-Dose Subcutaneous Heparin Protocol for Adjusted-Dose Subcutaneous AdministrationAdministrationaa1-Initial therapy with adjusted-dose SC heparin 1-Initial therapy with adjusted-dose SC heparin *Give SC heparin 240 U/kg STAT. *Give SC heparin 240 U/kg STAT. *Check first aPTT 6 hours after first dose. *Check first aPTT 6 hours after first dose.
*Adjust dosing per chart below.*Adjust dosing per chart below. 2-Conversion from continuous infusion heparin to 2-Conversion from continuous infusion heparin to adjusted-dose SC heparin adjusted-dose SC heparin *Calculate total 24-hour heparin requirement necessary *Calculate total 24-hour heparin requirement necessary to maintain therapeutic aPTT. to maintain therapeutic aPTT. *Divide 24-hour heparin requirement by 2 and increase *Divide 24-hour heparin requirement by 2 and increase this dose by an additional 10%–20% to determine initial Q this dose by an additional 10%–20% to determine initial Q 12 hours SC dosing requirement. 12 hours SC dosing requirement. *Discontinue IV heparin and administer initial Q 12 hr SC *Discontinue IV heparin and administer initial Q 12 hr SC dose within 1 hr. dose within 1 hr. *Check first aPTT 6 hr after first dose. *Check first aPTT 6 hr after first dose.
*Adjust dosing per chart below.*Adjust dosing per chart below.
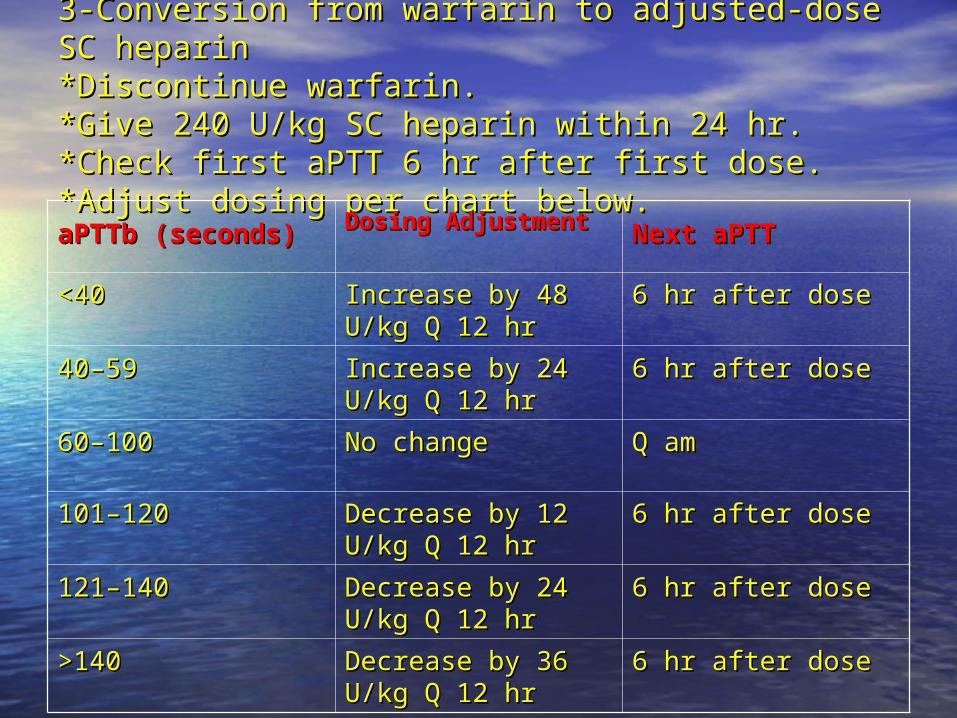
3-Conversion from warfarin to adjusted-dose SC 3-Conversion from warfarin to adjusted-dose SC heparin heparin *Discontinue warfarin. *Discontinue warfarin. *Give 240 U/kg SC heparin within 24 hr. *Give 240 U/kg SC heparin within 24 hr. *Check first aPTT 6 hr after first dose. *Check first aPTT 6 hr after first dose. *Adjust dosing per chart below.*Adjust dosing per chart below.aPTTb (seconds)aPTTb (seconds) Dosing AdjustmentDosing Adjustment Next aPTTNext aPTT
<40 <40 Increase by 48 U/kg Increase by 48 U/kg Q 12 hr Q 12 hr
6 hr after dose 6 hr after dose
40–59 40–59 Increase by 24 U/kg Increase by 24 U/kg Q 12 hr Q 12 hr
6 hr after dose 6 hr after dose
60–100 60–100 No change No change Q amQ am
101–120 101–120 Decrease by 12 Decrease by 12 U/kg Q 12 hr U/kg Q 12 hr
6 hr after dose 6 hr after dose
121–140 121–140 Decrease by 24 Decrease by 24 U/kg Q 12 hr U/kg Q 12 hr
6 hr after dose 6 hr after dose
>140 >140 Decrease by 36 Decrease by 36 U/kg Q 12 hr U/kg Q 12 hr
6 hr after dose 6 hr after dose
More recent data support the efficacy of weight based SC More recent data support the efficacy of weight based SC UFH (initial dose of 333 U/kg followed by 250 U/kg every UFH (initial dose of 333 U/kg followed by 250 U/kg every 12 hours) 12 hours) without routine aPTT monitoringwithout routine aPTT monitoring for the for the treatment oftreatment of acute VTE. acute VTE. Reversal of EffectReversal of EffectHeparin should be discontinued immediately, and Heparin should be discontinued immediately, and treatment should include maintenance of fluid volume treatment should include maintenance of fluid volume and replacement of clotting factors with whole blood, and replacement of clotting factors with whole blood, fresh frozen plasma, or clotting factor concentrates. If fresh frozen plasma, or clotting factor concentrates. If hemorrhage had not been present and the only hemorrhage had not been present and the only manifestation of overdose had been a prolonged aPTT, manifestation of overdose had been a prolonged aPTT, administration of heparin simply could have been administration of heparin simply could have been discontinued, permitting the effects to clear within a few discontinued, permitting the effects to clear within a few hours.hours.
Protamine can be used to neutralize heparin by forming Protamine can be used to neutralize heparin by forming an inactive protamine–heparin complex.Protamine has a an inactive protamine–heparin complex.Protamine has a rapid onset of action, with effects lasting about 2 hours. rapid onset of action, with effects lasting about 2 hours. Protamine sulfate is infused slowly over 3 to 5 minutes, as Protamine sulfate is infused slowly over 3 to 5 minutes, as a 1% solution at a dose of 1 mg for each 100 U of heparin a 1% solution at a dose of 1 mg for each 100 U of heparin administered, but only if it is given within 30 minutes of administered, but only if it is given within 30 minutes of discontinuation of heparin administration. The maximum discontinuation of heparin administration. The maximum single recommended dose of protamine is 50 mg, but single recommended dose of protamine is 50 mg, but doses may be repeated if bleeding persists. If protamine doses may be repeated if bleeding persists. If protamine therapy is delayed, dosing should be based on the therapy is delayed, dosing should be based on the estimated amount of heparin remaining, taking into estimated amount of heparin remaining, taking into consideration the elimination half-life of heparin. consideration the elimination half-life of heparin. Response to protamine therapy can be assessed by a Response to protamine therapy can be assessed by a return of the aPTT to baseline. Adverse effects associated return of the aPTT to baseline. Adverse effects associated with protamine include systemic hypotension secondary with protamine include systemic hypotension secondary to rapid administration; anaphylaxis characterized by to rapid administration; anaphylaxis characterized by edema, bronchospasm, and cardiovascular collapse; and edema, bronchospasm, and cardiovascular collapse; and catastrophic pulmonary vasoconstrictioncatastrophic pulmonary vasoconstriction
Low-Molecular-Weight HeparinLow-Molecular-Weight HeparinLMWH results in fewer deaths, major hemorrhages, and LMWH results in fewer deaths, major hemorrhages, and recurrent VTE when compared to UFH, not require aPTT recurrent VTE when compared to UFH, not require aPTT monitoring. Based on these advantages, outpatient use of monitoring. Based on these advantages, outpatient use of LMWH has become the most common approach to LMWH has become the most common approach to treatment of uncomplicated DVT. The synthetic treatment of uncomplicated DVT. The synthetic pentasaccharide, fondaparinux, can be considered as an pentasaccharide, fondaparinux, can be considered as an alternative treatment option to the LMWHs as it has been alternative treatment option to the LMWHs as it has been shown to be as effective and safe as LMWH in the shown to be as effective and safe as LMWH in the treatment of DVT. Fondaparinux has the benefit that, to treatment of DVT. Fondaparinux has the benefit that, to date, HIT has not been associated with its date, HIT has not been associated with its use.Contraindications to home treatment of DVT include a use.Contraindications to home treatment of DVT include a pre-existing condition that requires hospitalization, pre-existing condition that requires hospitalization, clinical symptoms of PE and/or hemodynamic instability, clinical symptoms of PE and/or hemodynamic instability, recent or active bleeding, and end-stage renal disease.recent or active bleeding, and end-stage renal disease.In addition, hemorrhage and recurrent VTE are less likely In addition, hemorrhage and recurrent VTE are less likely to occur with twice-daily dosing of LMWH as compared to to occur with twice-daily dosing of LMWH as compared to once-daily dosing, thus raising further controversy around once-daily dosing, thus raising further controversy around the routine use of once-daily dosing.the routine use of once-daily dosing.
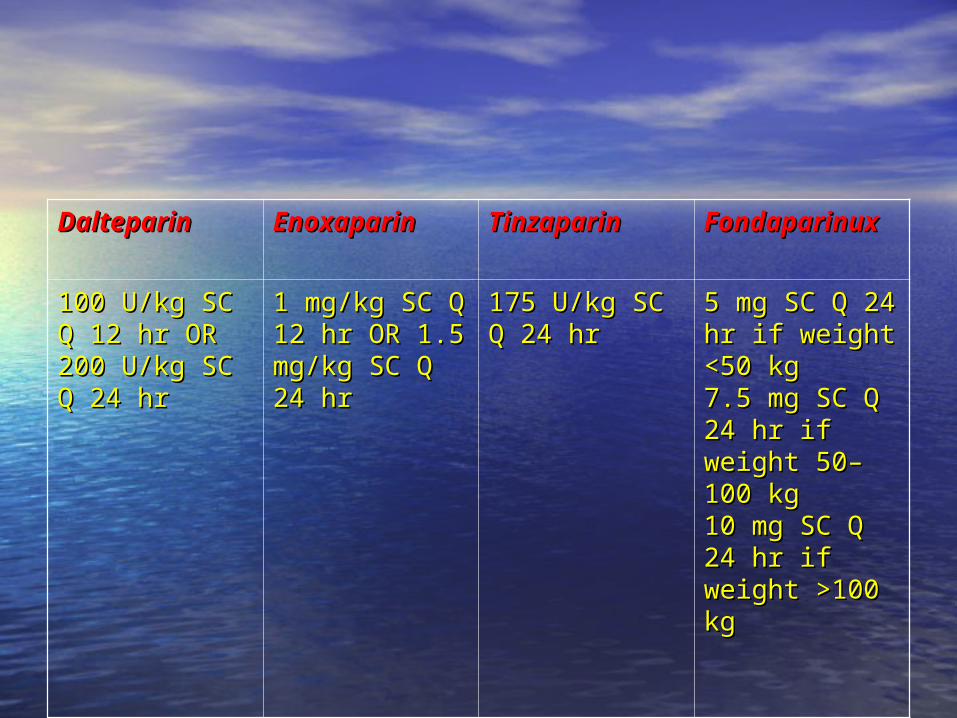
DalteparinDalteparin EnoxaparinEnoxaparin TinzaparinTinzaparin FondaparinuFondaparinuxx
100 U/kg SC Q 100 U/kg SC Q 12 hr OR 200 12 hr OR 200 U/kg SC Q 24 U/kg SC Q 24 hrhr
1 mg/kg SC Q 1 mg/kg SC Q 12 hr OR 1.5 12 hr OR 1.5 mg/kg SC Q mg/kg SC Q 24 hr24 hr
175 U/kg SC Q 175 U/kg SC Q 24 hr 24 hr
5 mg SC Q 24 5 mg SC Q 24 hr if weight hr if weight <50 kg<50 kg7.5 mg SC Q 7.5 mg SC Q 24 hr if weight 24 hr if weight 50–100 kg50–100 kg10 mg SC Q 10 mg SC Q 24 hr if weight 24 hr if weight >100 kg>100 kg
PreventionPreventionSurgical procedures represent a significant risk factor for Surgical procedures represent a significant risk factor for DVT formation. All hospitalized patients, including both DVT formation. All hospitalized patients, including both surgical and nonsurgical patients, should be stratified for surgical and nonsurgical patients, should be stratified for risk of DVT based on the presence of various risk factor as risk of DVT based on the presence of various risk factor as age (older than 40 years) ,obesity, peripheral vascular age (older than 40 years) ,obesity, peripheral vascular disease, and probable postoperative immobilization). disease, and probable postoperative immobilization). Nonpharmacologic MeasuresNonpharmacologic MeasuresMechanical interventions aimed at preventing venous Mechanical interventions aimed at preventing venous stasis and increasing venous return include the use of stasis and increasing venous return include the use of elastic compression stockings, as well as leg elevation, elastic compression stockings, as well as leg elevation, leg exercises, and early postoperative ambulation. leg exercises, and early postoperative ambulation. Pharmacologic MeasuresPharmacologic MeasuresFixed, low-dose unfractionated heparin (LDUFH), Fixed, low-dose unfractionated heparin (LDUFH), administered as 5,000 U SC Q 8 to 12 hr depending on administered as 5,000 U SC Q 8 to 12 hr depending on the indication, is an inexpensive and effective the indication, is an inexpensive and effective pharmacologic approach to DVT prevention in the setting pharmacologic approach to DVT prevention in the setting of venous stasis, in medical patients, or after certain of venous stasis, in medical patients, or after certain surgical procedures.surgical procedures.
Because low-dose heparin inactivates factor Xa Because low-dose heparin inactivates factor Xa without a direct effect on factor IIa, the aPTT is without a direct effect on factor IIa, the aPTT is not prolonged, and therefore, aPTT monitoring is not prolonged, and therefore, aPTT monitoring is unnecessary. Bleeding complications are unnecessary. Bleeding complications are minimized using this dosing regimen. minimized using this dosing regimen. Fixed-dose SC LMWH and fondaparinux are Fixed-dose SC LMWH and fondaparinux are alternative approaches for preventing DVT. alternative approaches for preventing DVT. Enoxaparin 30 mg SC Q 12 hr or 40 mg SC once Enoxaparin 30 mg SC Q 12 hr or 40 mg SC once daily, dalteparin 2,500 to 5,000 IU SC once daily, daily, dalteparin 2,500 to 5,000 IU SC once daily, and fondaparinux 2.5 mg SC once daily are and fondaparinux 2.5 mg SC once daily are effective strategies, The first dose should be effective strategies, The first dose should be administered several hours preoperatively, and administered several hours preoperatively, and dosing should continue postoperatively until she dosing should continue postoperatively until she
is fully ambulatory. is fully ambulatory.
Fixed-dose SC LMWH and fondaparinux are Fixed-dose SC LMWH and fondaparinux are alternative approaches for preventing DVT. alternative approaches for preventing DVT. Enoxaparin 30 mg SC Q 12 hr or 40 mg SC once Enoxaparin 30 mg SC Q 12 hr or 40 mg SC once daily, dalteparin 2,500 to 5,000 IU SC once daily, daily, dalteparin 2,500 to 5,000 IU SC once daily, and fondaparinux 2.5 mg SC once daily are and fondaparinux 2.5 mg SC once daily are effective strategies, The first dose should be effective strategies, The first dose should be administered several hours preoperatively, and administered several hours preoperatively, and dosing should continue postoperatively until she dosing should continue postoperatively until she is fully ambulatory.is fully ambulatory.
Pulmonary EmbolismPulmonary EmbolismClinical PresentationClinical PresentationSigns and SymptomsSigns and SymptomsThe clinical diagnosis of PE is often difficult to The clinical diagnosis of PE is often difficult to make because of the nonspecificity of symptoms. make because of the nonspecificity of symptoms. The most commonly observed subjective The most commonly observed subjective symptoms are dyspnea, pleuritic chest pain, symptoms are dyspnea, pleuritic chest pain, anxiety or a feeling of impending doom, and anxiety or a feeling of impending doom, and cough. Hemoptysis occurs occasionally. The cough. Hemoptysis occurs occasionally. The objective signs most commonly observed are objective signs most commonly observed are tachypnea at a rate of ≥20 breaths/minute, tachypnea at a rate of ≥20 breaths/minute, tachycardia of ≥100 beats/minute. DVT precedes tachycardia of ≥100 beats/minute. DVT precedes PE in 80% or more of patients.PE in 80% or more of patients.

DiagnosisDiagnosisBecause the clinical signs and symptoms of PE are Because the clinical signs and symptoms of PE are difficult to distinguish from many other medical difficult to distinguish from many other medical conditions, further evaluation is necessary. Chest conditions, further evaluation is necessary. Chest radiograph, ECG, and arterial blood gas (alveolar-arterial radiograph, ECG, and arterial blood gas (alveolar-arterial oxygen gradient [A-a gradient]) abnormalities are often oxygen gradient [A-a gradient]) abnormalities are often present in patients with PE, but they are somewhat present in patients with PE, but they are somewhat nonspecific. Although pulmonary angiography has been nonspecific. Although pulmonary angiography has been considered the gold standard for diagnosis of PE, it is an considered the gold standard for diagnosis of PE, it is an invasive procedure that is expensive and technically invasive procedure that is expensive and technically difficult to perform. Noninvasive tests such as V/Q lung difficult to perform. Noninvasive tests such as V/Q lung scans and computed tomography (CT) scans are useful scans and computed tomography (CT) scans are useful and the most frequently used diagnostic procedures to and the most frequently used diagnostic procedures to document the presence of PE. document the presence of PE.
TreatmentTreatmentTreatment options for PE include IV UFH therapy initiated Treatment options for PE include IV UFH therapy initiated with a loading dose followed by a continuous infusion, or with a loading dose followed by a continuous infusion, or a LMWH or fondaparinux administered by SC injection. a LMWH or fondaparinux administered by SC injection. Monitoring of the aPTT would be used to adjust dosing to Monitoring of the aPTT would be used to adjust dosing to maintain treatment within the therapeutic range .maintain treatment within the therapeutic range .
The alternative to UFH for treatment of PE is the use of a The alternative to UFH for treatment of PE is the use of a SC LMWH or SC fondaparinux.ex:- fixed-dos enoxaparin 1 SC LMWH or SC fondaparinux.ex:- fixed-dos enoxaparin 1 mg/kg Q 12 hr). Generally, PE should not be treated on an mg/kg Q 12 hr). Generally, PE should not be treated on an outpatient basis. In this case, LMWH or fondaparinux outpatient basis. In this case, LMWH or fondaparinux would be used during the complete hospital course, or would be used during the complete hospital course, or only for partial outpatient therapy in selected lower-risk only for partial outpatient therapy in selected lower-risk and stable patients who may be discharged early.and stable patients who may be discharged early.
The use of thrombolytic therapy should be reserved for The use of thrombolytic therapy should be reserved for patients with acute massive embolism, who are patients with acute massive embolism, who are hemodynamically unstable (SBP <90 mmHg) and at low hemodynamically unstable (SBP <90 mmHg) and at low risk for bleeding.risk for bleeding.
WarfarinWarfarinEither heparin or LMWH/fondaparinux therapy should be continued Either heparin or LMWH/fondaparinux therapy should be continued for at least 5 days in the setting of PE, and until warfarin therapy is for at least 5 days in the setting of PE, and until warfarin therapy is therapeutic and stable. Warfarin should be started on the first day of therapeutic and stable. Warfarin should be started on the first day of hospitalization and continued for a minimum of 3 to 6 months or hospitalization and continued for a minimum of 3 to 6 months or longer.There are several reasons to overlap heparin and warfarin longer.There are several reasons to overlap heparin and warfarin therapy. The onset of warfarin activity depends not only on its therapy. The onset of warfarin activity depends not only on its inherent pharmacokinetic characteristics (half-life >36 hours), but inherent pharmacokinetic characteristics (half-life >36 hours), but also on the rate of elimination of circulating clotting factors that also on the rate of elimination of circulating clotting factors that correspond with their elimination half-lives. Initial increases in the INR correspond with their elimination half-lives. Initial increases in the INR reflect only reductions in factor VII activity, but full anticoagulation reflect only reductions in factor VII activity, but full anticoagulation with warfarin requires adequate suppression of factors II and X, which with warfarin requires adequate suppression of factors II and X, which have significantly longer elimination half-lives.have significantly longer elimination half-lives. In addition to suppressing the synthesis of the vitamin K–dependent In addition to suppressing the synthesis of the vitamin K–dependent clotting factors, warfarin also inhibits the formation of the naturally clotting factors, warfarin also inhibits the formation of the naturally occurring anticoagulant protein C and its cofactor, protein S. In occurring anticoagulant protein C and its cofactor, protein S. In patients with congenital protein C or protein S deficiency, initial patients with congenital protein C or protein S deficiency, initial warfarin therapy can suppress these proteins to concentrations that warfarin therapy can suppress these proteins to concentrations that may result in hypercoagulability with possible thrombus extension, may result in hypercoagulability with possible thrombus extension, unless concurrent heparin therapy provides adequate unless concurrent heparin therapy provides adequate anticoagulation.anticoagulation.Heparin therapy has been observed to prolong the INR, and warfarin Heparin therapy has been observed to prolong the INR, and warfarin can prolong the aPTT by several seconds.can prolong the aPTT by several seconds.
Initiation of TherapyInitiation of TherapyInitiation of warfarin dosing is complex because dosing Initiation of warfarin dosing is complex because dosing requirements vary significantly among individuals.Two requirements vary significantly among individuals.Two methods for initiation of warfarin therapy have been methods for initiation of warfarin therapy have been developed.developed.The average daily dosing method relies on an The average daily dosing method relies on an understanding that although dosing requirements for understanding that although dosing requirements for warfarin vary significantly among patients, an average warfarin vary significantly among patients, an average dosing requirement of 4 to 5 mg/day of warfarin is dosing requirement of 4 to 5 mg/day of warfarin is necessary to maintain an INR of 2.0 to 3.0.necessary to maintain an INR of 2.0 to 3.0. patients who may be more sensitive to the effects of patients who may be more sensitive to the effects of warfarin are expected to require lower dosages of warfarin are expected to require lower dosages of warfarin including(Age older than 75 years,Clinical warfarin including(Age older than 75 years,Clinical CHF,Clinical hyperthyroidism,Decreased oral CHF,Clinical hyperthyroidism,Decreased oral intake,Diarrhea,Drug–drug interactions,Elevated baseline intake,Diarrhea,Drug–drug interactions,Elevated baseline INR, End-stage renal disease, Fever, Hepatic INR, End-stage renal disease, Fever, Hepatic disease,Hypoalbuminemia,Malignancy,Malnutritionand disease,Hypoalbuminemia,Malignancy,Malnutritionand Postoperative status Postoperative status
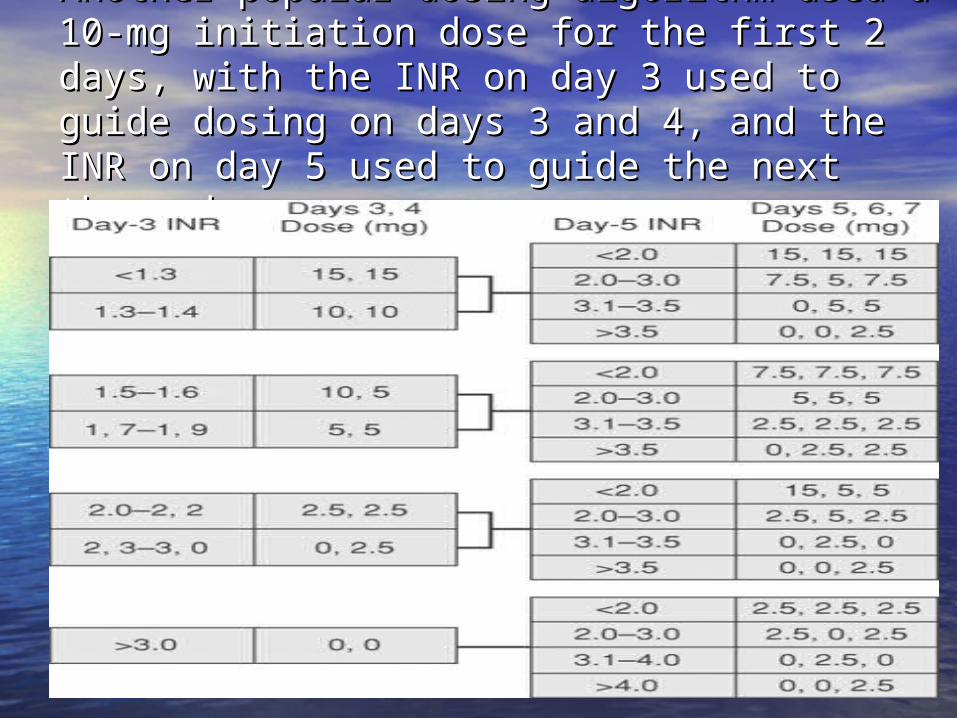
Another popular dosing algorithm used a 10-Another popular dosing algorithm used a 10-mg initiation dose for the first 2 days, with the mg initiation dose for the first 2 days, with the INR on day 3 used to guide dosing on days 3 INR on day 3 used to guide dosing on days 3 and 4, and the INR on day 5 used to guide the and 4, and the INR on day 5 used to guide the next three doses .next three doses .
The 10-mg initiation dose may lead to The 10-mg initiation dose may lead to overanticoagulation and heightened bleeding risk overanticoagulation and heightened bleeding risk in elderly and ill patients with multiple medical in elderly and ill patients with multiple medical problems.problems. Average daily dosing is often used to initiate Average daily dosing is often used to initiate therapy in ambulatory patients; in this case, the therapy in ambulatory patients; in this case, the first INR should be evaluated within 3 to 5 days of first INR should be evaluated within 3 to 5 days of initiation of warfarin therapy. In hospitalized initiation of warfarin therapy. In hospitalized patients, it is more common to evaluate the INR patients, it is more common to evaluate the INR daily during initiation of therapy.daily during initiation of therapy.