Thesis Tugba Aydin final
28
Causes of high prevalence of Type 2 Diabetes in Turkish and Moroccan people in relation to migration Tuğba Aydın -A systematic literature research-
-
Upload
tugba-aydin -
Category
Documents
-
view
48 -
download
0
Transcript of Thesis Tugba Aydin final

Causes of high prevalence of Type 2 Diabetes in Turkish and Moroccan people
in relation to migration
Tuğba Aydın
- A s y s t e m a t i c l i t e r a t u r e r e s e a r c h -
2
L I T E R A T U R E T H E S I S
Prepared by: Tuğba Aydın, 2007991
Student: Management, Entrepreneurship and Policy analysis in Health and Life
Sciences
Specialization: Management and entrepreneurship
Version: Final
Date: 29th of August 2016
Supervisor:
Dr. C.W.M. Dedding
Faculty of Earth and Life Sciences, VU
De Boelelaan 1105 1081 HV Amsterdam
Room: U-538

3
SUMMARY
Introduction: Diabetes Mellitus is a chronic illness and indicates a deregulated amount of
glucose in the blood of the patient for a prolonged period and is an increasing problem
worldwide. In the Netherlands, 834.100 persons live with Diabetes each day, and this amount is
increasing with approximately 52.700 new cases per year. Several studies stated that
immigrants from Morocco and Turkey are more likely to be diagnosed with Type 2 Diabetes
than indigenous population. The prevalence among the approximately one million immigrants
of Turkish and Moroccan origin in the Netherlands is 3 to 6 times higher than among natives.
More insight about the factors leading to higher prevalence of Type 2 Diabetes among these
immigrant groups, could help to prevent the high amount of Diabetes among Turkish and
Moroccan groups and the high health costs. For this purpose, this thesis sets out the reasons of
the high prevalence of Turkish and Moroccan immigrants and examines the effect of migration
on Type 2 Diabetes. Hence, the research question is defined as: ‘What are the explanations in the literature for the high prevalence of Diabetes Type 2 among Turkish and Moroccan migrants in the Netherlands?’ Methods: A systematic literature research was performed. Two databases are consulted:
PubMed and Scopus. After entering the search term in the databases, the articles are first
analysed on the title and abstract. Thereafter a full text analysis was done. The following search
term is inserted in both databases: (Diabetes Mellitus Type 2 OR Type 2 Diabetes OR non insulin dependent Diabetes OR Type II Diabetes) AND (immigrants OR Turkish OR Turks OR Moroccan OR Morocco) AND (Netherlands). After the accessible full text filter, Scopus gave 145 accessible full
text hits, where PubMed identified 203 full texts that are free accessible for VU students. In the
end, in total 22 articles are included in this thesis. Results: This research found several reasons for the high prevalence of Type 2 Diabetes among
Turkish and Moroccan immigrants. Turkish and Moroccan immigrants have a deviated lipid
profile and non-fasting plasma glucose, high amount of obesity, lower socio economic status,
hypertension and genetics that set them in a high-risk profile of developing Type 2 Diabetes.
Also cultural habits such as diet and physical inactivity can play a role in the higher prevalence.
Discussion and conclusion: Several studies suggest that Turkish and Moroccan immigrants
adopt a more western diet when they migrate to Europe, and this diet change seems to
adversely affect their risk of developing Diabetes. An adopted westernized diet can lead to
obesity, which is strongly associated with the prevalence of Diabetes among Turkish
immigrants. Both in the western countries as in Turkey and Morocco, an increasing trend of
obesity is seen and described as a predictor of Type 2 Diabetes. Nevertheless, obesity seems to
increase as migrants get wealthier and urbanized, suggesting that migration amplifies the effect
of obesity on Diabetes, as this research also found that there is a significant difference in the
prevalence of obesity and Type 2 Diabetes in rural or urban areas. Taking in consideration that
largely amount of immigrants are migrated from rural area in Turkey and Morocco to urban
area in the Netherlands, migration could have a large effect on the high prevalence of Type 2
Diabetes among Turkish and Moroccan immigrants. Genetic factors may play a role in the

4
higher prevalence of Diabetes among Turkish and Moroccan immigrants, since some genes
seem to have a stronger association with Diabetes for Moroccans than for natives. The
management of lifestyle by controlling the diet and the physical activity among Moroccans
seemed challenging, meaning that culture plays a great role in the development of Type 2
Diabetes.
This review found that both immigration as well as ethnicity could account for the higher
prevalence of Type 2 Diabetes among Turkish and Moroccan immigrants in the Netherlands.
Migration can have a large effect on lifestyle and psychosocial aspects, but also ethnicity can be
an independent factor of the development of Type 2 Diabetes.

5
CONTENTS
1.INTRODUCTION.............................................................................................................................61.1.RESEARCHOBJECTIVEANDRESEARCHQUESTION.........................................................................................7
2.THEORETICALBACKGROUND......................................................................................................92.1.MODELSABOUTPOSSIBLECAUSESOFTYPE2DIABETES................................................................................92.2.SUB-QUESTIONS..................................................................................................................................11
3.METHODS.....................................................................................................................................123.1.INCLUSIONANDEXCLUSIONCRITERIA......................................................................................................123.2.DATABASEANDSELECTION....................................................................................................................12
4.RESULTS.......................................................................................................................................144.1.TYPE2DIABETESAMONGTURKSLIVINGINTURKEY...................................................................................144.2.TYPE2DIABETESAMONGMOROCCANSLIVINGINMOROCCO.....................................................................164.3.CAUSESOFHIGHPREVALENCEOFTYPE2DIABETESAMONGTURKISHIMMIGRANTS........................................174.4.CAUSESOFHIGHPREVALENCEOFTYPE2DIABETESAMONGMOROCCANIMMIGRANTS...................................19
5.DISCUSSIONANDCONCLUSION..................................................................................................225.1.FACTORSRELATEDTOMIGRATION..........................................................................................................225.2.FACTORSRELATEDTOETHNICITY............................................................................................................235.3.FACTORSWHICHARENOTCLEARLYRELATEDTOEITHERIMMIGRATIONORETHNICITY.......................................245.4.STRENGTHSANDLIMITATIONS...............................................................................................................245.5.CONCLUSION......................................................................................................................................25
REFERENCES....................................................................................................................................26

6
1.INTRODUCTION
Diabetes Mellitus (DM) is a chronic illness and indicates a deregulated amount of glucose in the
blood of the patient for a prolonged period (Adriaanse et al., 2008). This is mainly due to either
the pancreas is unable to produce enough insulin, also called Type 1 Diabetes, or the body is
unable to respond properly to the produced insulin, called Type 2 Diabetes (Shoback et al.,
2011). Insulin is essential to convert absorbed glucose in the liver into glycogen or triglycerides.
Worldwide, it is estimated that 415 million people are suffering from Diabetes Mellitus in 2015
(IDF, 2015), of which Diabetes Type 2 count for 90% of these cases (Shi and Hu, 2014). This
means that 8,3% of the adult population worldwide is affected, both man as woman in an equal
amount (Vos et al., 2012). The huge impact of Diabetes is increasing, as it is expected that the
number of people suffering from this disease will rise to 592 million within 20 years (IDF 2015).
In the Netherlands, 834.100 persons live with Diabetes each day, and this amount is increasing
with approximately 52.700 new cases per year (Diabetesfonds, 2016). In addition, 250.000 people
are at high risk to get Diabetes (NDF, 2010), which sets this disease to an increasing health
problem in the Netherlands.
Diabetes can have severe consequences if it is left undiagnosed or untreated, such as serious co-
morbidities, low quality of life, and high costs in health care (Adriaanse et al., 2008; Kleefstra et
al., 2008). Serious comorbidities that often accompany Diabetes are depression (Chen, 2013),
cardio vascular diseases, obesity (Ali et al., 2010, Schram et al., 2009), diabetic retinopathy and
chronic kidney failures (WHO, 2013). Comorbidities are an important predictor of early deaths
in Diabetes patients (Landman et al., 2010). The high prevalence and the increasing incidence in
combination with co-morbidities in Diabetes results in high costs in the health care. According
to the RIVM, the cost of care for Diabetes patients totalled 1.0 billion euros in 2007 (Luijben and
Kommer, 2010). That equals to 1.4% of total health care costs in the Netherlands. The largest
share of the costs (58%) is spent on drugs and medical devices (Baan et al., 2005).
Important risk factors for developing Type 2 Diabetes are obesity (Hartemink et al., 2006),
abdominal fat, lack of physical activity and dietary factors (Dabelea et al., 1998; Wei et al., 2003).
While both types of Diabetes are influenced by genetic predisposition, genetic factors seem to
play a larger role in Type 1 Diabetes than Type 2 Diabetes (Maher et al., 2008). Type 2 Diabetes
is also influenced by environmental, cultural and social factors (Summerson et al., 1992;
Uitewaal et al., 2002; Weijers et al., 1998). For this reason, several researchers have reported
differences between ethnic groups affected by Type 2 Diabetes (Chaturvedi et al., 1996; Jenum et
al., 2012). Many researches have described this for ethnic minority groups of South Asian or
Black African origin who are living in West-European countries (Agyemang et al., 2002; Burden
et al., 2000; Magnus et al., 1997). However, there are fewer studies about other large ethnic

7
minority groups in West-Europe, such as Moroccans and Turks. They are the largest minority
groups in the Netherlands as Turks counts for 2,35 percent of the Dutch population, where
Moroccans counts for 2,23 percent (CBS, 2015).
An example of a study that investigated Diabetes in relation to Turkish or Moroccan
immigrants is published by Guell (2011). He stated that Turks who live in Germany are almost
twice as likely to suffer from Type 2 Diabetes as indigenous Germans (Guell, 2011). It is also
known that immigrant groups like the Moroccans or Turks living in the Netherlands show an
increased prevalence of Diabetes (Wändell et al., 2010). The prevalence among the
approximately one million immigrants of Turkish and Moroccan origin in the Netherlands is 3
to 6 times higher than among natives (Poortvliet et al, 2007). In addition, according to the risk
profile in the report of NDF (Dutch Diabetes Federation, 2010) being from Turkish origin is a
risk factor for Diabetes. These studies put the Turkish and Moroccan immigrant groups in an
extremely high-risk profile. However interventions directed to these groups and which takes
ethnicity into account are not sufficient, because they are mainly short termed or have
disappointing results (Looise et al., 2006).
Taking into account the many serious consequences of Diabetes and the increasing amount of
immigrants, it is important to investigate the factors leading to higher prevalence among
immigrants in the Netherlands in comparison with natives. Also the effect of migration on Type
2 Diabetes is important to investigate, as knowledge of all factors that possibly can lead to a
higher prevalence, could increase the effectiveness of interventions that take a patient’s
immigrant background into account. Interventions for better care adjusted for the needs of
immigrants could help to prevent the high amount of Diabetes among Turkish and Moroccan
groups, thereby decreasing early deaths and healthcare costs. For this purpose, this thesis sets
out the reasons of the high prevalence of these immigrants and examines the effect of migration
on Type 2 Diabetes.
1.1.Researchobjectiveandresearchquestion
The aim of this study is to perform a systemic literature research in order to set out the
explanations of the high prevalence of Type 2 Diabetes among Turkish and Moroccan
immigrants in the Netherlands, and to compare this prevalence to the prevalence in the
countries of origin. In addition this review will examine the effect of migration on the
prevalence of Type 2 Diabetes among Turkish and Moroccan immigrants living in the
Netherlands.
Hence, the research question is defined as:

8
What are the explanations in the literature for the high prevalence of Diabetes Type 2 among Turkish and Moroccan migrants in the Netherlands?

9
2.THEORETICALBACKGROUND
For the deeper understanding of the scope of this research, this section presents two models that
set out possible causes of Diabetes. Hence, the sub-questions of this research are formulated.
2.1.ModelsaboutpossiblecausesofType2Diabetes
Abate and colleagues (2003) divided the causes of Diabetes in two main factors: environmental
factors and genetic factors. In this model obesity is correlated with Diabetes and called
‘Diabesity’ (Abate et al., 2003). Figure 1 shows the different components of the model. Less
physical activity, extra calorie intake and an unhealthy diet composition can lead in time to
obesity. Stress and low socio economic status are also factors, which can in time cause obesity.
For example, socio-economic status can necessitate a person to cheap and unhealthy food. For
each kilogram of weight gain, it has been calculated that the risk for Diabetes increases by about
4.5% (Mokdad et al., 2001). In combination with the genetic factors that can lead to a high risk
for Diabetes, the calculated effect by Mokdad et al. (2001) can lead to beta-cell dysfunction and
insulin resistance, resulting in ‘Diabesity’ (Abate et al., 2003). Nevertheless, as mentioned in the
introduction, migration can play a possible important role in the high prevalence of Type 2
Diabetes among immigrants. Abate and co-workers have developed a model, which does not
take migration directly into account.
Figure1:interactionbetweenenvironmentalfactorsandgeneticfactors,leadingto'Diabesity'(Abateetal.,2003)

10
Misra and colleagues (2007) have developed a model to explain the effect of migration on
developing Diabetes. This model, Figure 2, focused on the interplay of multiple individual
factors that could determine the detrimentally metabolic changes and subsequently the high
prevalence of Diabetes type 2 in migrants.
According to this model, migration affects several factors. Firstly, lifestyle changes such as
decreased physical activity, changed (unhealthy) diet and smoking, can lead to metabolic
perturbations that subsequently can lead to Diabetes. Also psychosocial factors, such as cultural
alienation, low self-esteem (may be a result of trying to adapt to new environment, culture, and
language) and loss of support of for example family members can lead to metabolic
perturbations that can be a predictor of Diabetes (Misra et al., 2007). In addition race, a different
culture, low socioeconomic stratum, and lifestyle/habits of the migrants can lead to lifestyle
changes as well as to psychosocial factors that affect the metabolism negatively. Misra et al.
(2007) concluded that Diabetes can have multiple causal factors and that these factors interplay
with one another. Ethnicity (race) and culture are seen as central factors in this model that can
influence many other factors, as showed in the figure, and can even directly lead to metabolic
perturbations. Migration also seems to be an early predictor of Diabetes, as it influences many
other important factors that can cause Diabetes (Misra et al., 2007). This model and the model
introduced by Abate et al. (2003) include genetic factors as important factors in the development
of Diabetes, suggesting that certain ethnicities can be more vulnerable to Diabetes than others.
However, both models are not particularly focussed on Turkish and Moroccan immigrants
living in Western Europe. Therefore, this thesis is a review of literature focussing on Turkish
and Moroccan immigrants and takes the model of Misra et al. (2007) as base. Also, in order to
Figure2:interplayofmultiplefactors,whichmayleadtoDiabetes.SES=socioeconomicstratum,T2DM=Type2DiabetesMellitus(Misraetal,2007).

11
investigate the effect of migration on the high prevalence among Turkish and Moroccan
immigrants living in the Netherlands, it is also important to examine and compare the statistics
in the country of origin of these immigrants. The effect of migration can be derived from the
difference between people who have migrates and people who are still living in the country of
origin. If the data of immigrants and people from their country of origin are corresponding,
there is probably an effect of genetic predisposition and/ or culture. Differences in data likely
indicate an impact of migration.
2.2.Sub-questions
Hence, the following sub-questions are defined:
1. What is known in the literature about the prevalence of Type 2 Diabetes in countries of
origin: Turkey and Morocco?
2. How does migration influence the development of Type 2 Diabetes?

12
3.METHODS
In this section, the methods that were used to achieve the research objective are described in
detail. A systematic review was conducted from which the results are presented in a flow
diagram.
3.1.Inclusionandexclusioncriteria
The inclusion and exclusion criteria are contentious very important, since these criteria
determine the scope and the validity of the results (Meline, 2006). Both criteria are summarized
in Table 1. Since this research focuses on Type 2 Diabetes, articles investigating other types of
Diabetes are excluded. Also articles that were not related to ethnicity are excluded. Publications
that studied the epidemiology of Type 2 Diabetes among immigrants are included. Articles that
studied Turkish or Moroccan migrant Diabetes patients in other European countries were also
included, since they are likely comparable to the Netherlands. Furthermore, in order to avoid
out-dated data, only publications from 1999 until 2016 are included.
Inclusion criteria Exclusion criteria Diabetes Mellitus Type 2 Not Diabetes Mellitus Type 2
Ethnicity Not ethnicity related studies
Immigrants Not English or Dutch publications
Publication date: 1999- 2016
English and Dutch publications
Epidemiology: morbidity, prevalence, incidence
Table 1: Inclusion and exclusion criteria.
3.2.Databaseandselection
In order to increase the amount of usable literature that is available about the research topic,
two databases, PubMed and Scopus, are consulted. The search was done in May and June 2016.
The process of selecting studies for systematic review has several layers. In this study, the
selection of literature was based on three steps. After entering the key words in the databases,
the first step was to analyse the title and the abstract of the hits. The following search term is
inserted in both databases: (Diabetes Mellitus Type 2 OR Type 2 Diabetes OR non insulin dependent Diabetes OR Type II Diabetes) AND (immigrants OR Turkish OR Turks OR Moroccan OR Morocco) AND (Netherlands).
Based on the inclusion and exclusion criteria, a first selection was made based on the title of the
articles. In the second step, the accessibility of the article was considered, since some articles
were not accessible with the institutional access and therefore could not be taken into account in
this study. After the accessible full text filter, Scopus gave 145 accessible full text hits, where

13
PubMed identified 203 full texts that are free accessible for VU students. These hits are sieved
by the inclusion and exclusion criteria as identified in Table 1, which was the third step (article
selection by full text screening). At the end, many articles are excluded due to the accessibility
or the scope of the articles that was not corresponding with the scope of this research after
reading the full text.
Screen
ing
Includ
ed
Eligibility
Iden
tification
Recordsafterduplicatesremovedandfreefulltextscreened(n=203PubMed&n=103
Scopus)
Full-textarticlesassessedforeligibility(n=306)
Full-textarticlesexcluded(n=276)
Studiesincludedn=22
Table1:Databasessearchandstudiesincluded
Recordsidentifiedthroughdatabasesearching(PubMed)
(n=568)
Additionalrecordsidentifiedthroughothersources(Scopus)
(n=330)

14
4.RESULTS
The first section of this section describes literature about the data of the country of origin of
Turkish immigrants, where the second section describes this for Moroccan population. The
third and last section sets out the literature found about the causes of the high prevalence of
Type 2 Diabetes among Turkish and Moroccan people who have migrated to Western countries.
In this way the influence of migration on the high prevalence of Turkish and Moroccan
immigrants can be examined. Each section will elaborate the included studies explaining that
particular topic of the section.
4.1.Type2DiabetesamongTurkslivinginTurkey
This section sets out the literature found with regard to Type 2 Diabetes in Turks living in
Turkey in order to compare these data with that on Turkish immigrants, to investigate the effect
of migration on Diabetes. Four studies about this topic met the inclusion criteria and are
included in the analysis. These studies are listed in the next table. Author(s), year
Aim(s) Study characteristics
Onat et al., 2006 The statistics (incidence, predictors and
outcomes) of T2D in Turkey. Cross-sectional study.
Misra and Ganda, 2007 Impact of migration on adiposity and
T2D in several ethnic groups. Meta-analysis
Porsch-Ozcurumez et al., 1999
Comparison of cholesterol level and lipid
profile of Turkish people living in
Germany with Turkish sedentees in
Turkey.
Geissen study. 480 Turkish immigrants
living in Germany.
Satman et al., 2002 Diabetes and risk characteristics in
Turkey. Prevalence of T2D and impaired
glucose tolerance among Turkish people
living in Turkey and assessment of the
relation between glucose intolerance of
these people and the lifestyle and
physical risk factors.
Cross sectional study. 4.788 people who
were aged above the 20.
The studies that are found investigated whether the prevalence of Type 2 Diabetes is also high
in Turkey, and possible causes of a higher prevalence. Onat and colleagues (2006) investigated
in their cross-sectional study the incidence, prevalence, predictors, and outcomes of Diabetes
Type 2 in Turkey. For this purpose, they evaluated 3401 participants prospectively. Based on
their data, they estimated that 11% (2,90 million) of Turkish people in Turkey who are 35 years
or older are suffering from Diabetes. They also concluded that there are approximately 300.000
annual incidences of Diabetes. This study revealed that age, hypertension, abdominal obesity,

15
and low HDL cholesterol in men were significant predictors of Diabetes. Subsequently, Diabetes
was an independent predictor of cardiovascular diseases, fatal as well as non-fatal. These data
can mean that immigration is not the only cause of the large number of Diabetic Turkish
immigrants (Onat et al., 2006).
Misra and Ganda (2007) reviewed studies on the impact of migration on adiposity (severe or
morbid overweight) and Type 2 Diabetes in several ethnic groups, including South Asians,
Hispanics, Chinese, Japanese, and Turks. They indicated that the risk for Type 2 Diabetes
escalated with the gradient of obesity at migrants like Hispanics, Chinese and South Asians, as
they became more affluent and urbanized, indicating an important role of environmental
factors. They also suggest that nutrition, physical inactivity, gene-environment interaction,
stress, and other factors such as ethnic susceptibility are playing a role in developing Type 2
Diabetes among immigrants (Misra and Ganda (2007).
Misra and Ganda referred also to a study of Porsch-Ozcurumez et al. (1999). They concluded
that Turks who have lived for at least 10 years in Germany have a higher cholesterol
concentration than their relatives in Turkey, suggesting that migration has affected their
cholesterol level negatively (Misra & Ganda, 2007). The study of Porsch-Ozcurumez et al. (1999,
as cited in Misra & Ganda, 2007) included 480 Turkish immigrants living in Germany. It is
showed that the total cholesterol level of these Turkish immigrants was comparable with other
Western countries, however significantly higher than people living in Turkey. The HDL-
cholesterol concentrations were however low and corresponding with people in Turkey who
were not physically active. Based on these data, it seems that the lipid profile Turkish
immigrants in Germany are ‘westernizing’ and they are therefore more likely to develop Type 2
Diabetes and cardiovascular diseases (Porsch-Ozcurumez et al., 1999).
Satman et al. (2002) did a cross-sectional study on Diabetes and risk characteristics in Turkey
and included 4.788 people who were aged above 20. They investigated the prevalence of
Diabetes and impaired glucose tolerance among Turkish people living in Turkey and assessed
the relation between glucose intolerance and lifestyle and physical risk factors. They found that
the overall prevalence of Diabetes was 7,2% and glucose intolerance was 6,7%, however less
frequent in men than women. People who were living in rural areas also had Diabetes or
glucose intolerance less frequently than people who were living in urban areas. There was also
a high prevalence of hypertension and obesity, respectively 29% and 22%, which were more
common in women. Taking into account that this research also concluded that the prevalence of
Diabetes increased with higher BMI, this is a serious disease in Turkey (Satman et al., 2002).
16
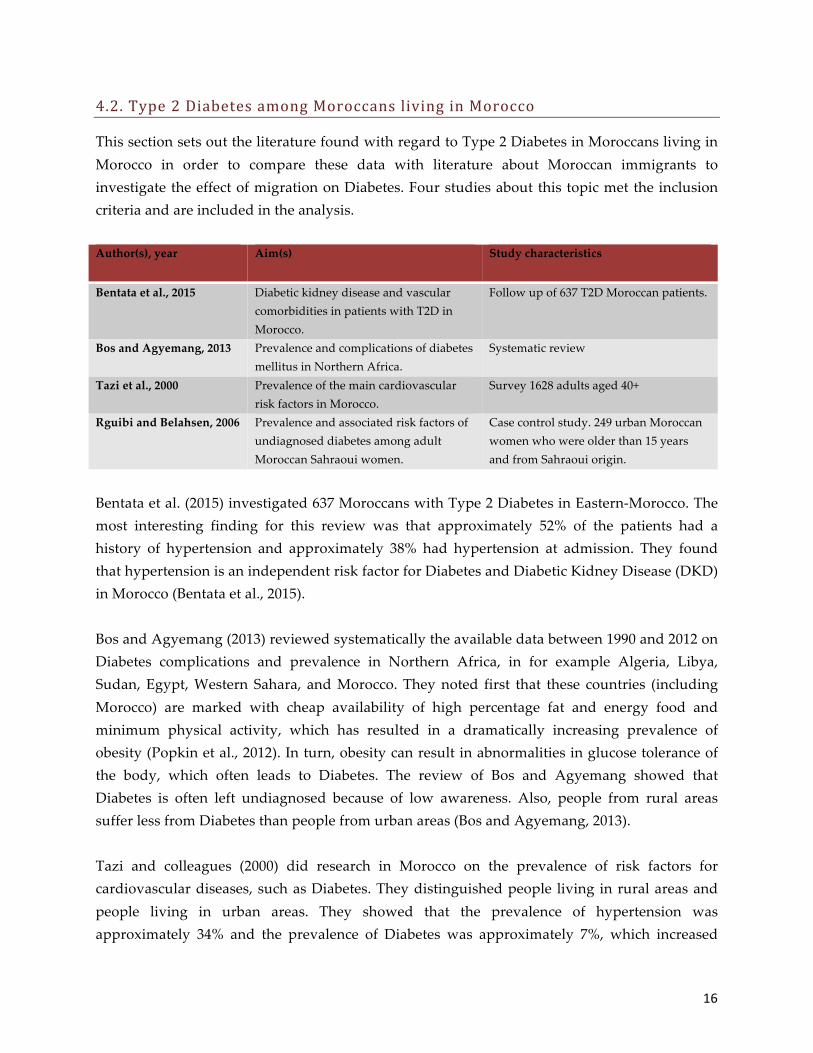
4.2.Type2DiabetesamongMoroccanslivinginMorocco
This section sets out the literature found with regard to Type 2 Diabetes in Moroccans living in
Morocco in order to compare these data with literature about Moroccan immigrants to
investigate the effect of migration on Diabetes. Four studies about this topic met the inclusion
criteria and are included in the analysis. Author(s), year
Aim(s) Study characteristics
Bentata et al., 2015 Diabetic kidney disease and vascular
comorbidities in patients with T2D in
Morocco.
Follow up of 637 T2D Moroccan patients.
Bos and Agyemang, 2013 Prevalence and complications of diabetes
mellitus in Northern Africa.
Systematic review
Tazi et al., 2000 Prevalence of the main cardiovascular
risk factors in Morocco. Survey 1628 adults aged 40+
Rguibi and Belahsen, 2006 Prevalence and associated risk factors of
undiagnosed diabetes among adult
Moroccan Sahraoui women.
Case control study. 249 urban Moroccan
women who were older than 15 years
and from Sahraoui origin.
Bentata et al. (2015) investigated 637 Moroccans with Type 2 Diabetes in Eastern-Morocco. The
most interesting finding for this review was that approximately 52% of the patients had a
history of hypertension and approximately 38% had hypertension at admission. They found
that hypertension is an independent risk factor for Diabetes and Diabetic Kidney Disease (DKD)
in Morocco (Bentata et al., 2015).
Bos and Agyemang (2013) reviewed systematically the available data between 1990 and 2012 on
Diabetes complications and prevalence in Northern Africa, in for example Algeria, Libya,
Sudan, Egypt, Western Sahara, and Morocco. They noted first that these countries (including
Morocco) are marked with cheap availability of high percentage fat and energy food and
minimum physical activity, which has resulted in a dramatically increasing prevalence of
obesity (Popkin et al., 2012). In turn, obesity can result in abnormalities in glucose tolerance of
the body, which often leads to Diabetes. The review of Bos and Agyemang showed that
Diabetes is often left undiagnosed because of low awareness. Also, people from rural areas
suffer less from Diabetes than people from urban areas (Bos and Agyemang, 2013).
Tazi and colleagues (2000) did research in Morocco on the prevalence of risk factors for
cardiovascular diseases, such as Diabetes. They distinguished people living in rural areas and
people living in urban areas. They showed that the prevalence of hypertension was
approximately 34% and the prevalence of Diabetes was approximately 7%, which increased

17
with age. The prevalence of obesity was also remarkably high in females and people living in
urban areas (Tazi et al., 2000).
Rguibi and Belahsen (2006) examined the prevalence and the related risk factors of undiagnosed
Diabetes among 249 urban Moroccan women who were older than 15 years and from Moroccan
origin. Diabetes was more common among women who were older, obese, had hypertension, or
had a genetic inheritance. The prevalence of undiagnosed diabetes was 6.4%, which probably
results from the high unawareness among Moroccan women, although they are from the city.
4.3.CausesofhighprevalenceofType2DiabetesamongTurkishimmigrants
This section sets out the literature found with regard to factors that can lead for high prevalence
of Type 2 Diabetes among Turkish immigrants living in Western Europe, in particular in the
Netherlands. Seven studies about this topic met the inclusion criteria and are included in the
analysis. These studies are listed in the next table.
Author(s), year
Aim(s) Study characteristics
Uitewaal et al., 2002, Testing the mean fasting glucose levels between Turkish and Dutch T2D patients.
Retrospective cohort study in 17 GPs. 106 Turkish and 90 Dutch T2D patients. Two year follow up.
Uitewaal et al., 2004 Comparison prevalence of cardiovascular risk factors for coronary heart disease and diabetes between Dutch and Turkish T2D patients.
Cross sectional study, 294 Dutch and 147 Turkish patients
Arslan et al., 2014 The association of single nucleotide polymorphism -19, -44 and -63 in the Calpain-10 gene and Type 2 Diabetes in Turkish population.
93 healthy participants and 118 T2D patients
Gonen et al., 2012 The relation of SNPs in ATP sensitive potassium channels (in Beta cells of the pancreas) with the mechanism of glucose-stimulated insulin secretion in Turkish Diabetics.
Screening of 169 T2D patients and 119 healthy patients.
Onat et al., 2009 Association between levels of C-III apoliprotein and Diabetes in Turkish people.
Cohort study of 800 participants followed up 4 years.
Onat et al., 2010 Association between levels of A-I apoliprotein and Diabetes in Turkish people.
Cohort study of more than 2000 people. Followed up 7 years.
Ujcic- Voortman et al., 2009 Diabetes prevalence and risk factors among ethnic minorities
Health survey. 375 Turkish, 314 Moroccan and 417 Dutch individuals aged 18–70 years. Participants underwent a physical examination and a health interview.
Uitewaal and colleagues have published several articles on the topic Diabetes and in particular
among Turkish immigrants. In one article from 2002 they performed a retrospective cohort
study in 17 general health practices. 106 Turkish Type 2 Diabetes patients and 90 Dutch patients
were followed for two years. They concluded that a significant number of Turkish patients had

18
a higher mean non-fasting plasma glucose level than Dutch patients (respectively 12.9 and 10.8
mmol/l) during the two-year follow-up. This means that Turkish immigrants compared to the
indigenous Dutch people are more likely to develop Diabetes, as they have significantly high
risk for higher mean non-fasting plasma glucose levels, which is a predictor of Diabetes
(Uitewaal et al., 2002).
In another study Uitewaal et al. (2004) compared the prevalence of cardiovascular risk factors
for coronary heart disease between Dutch and Turkish immigrants Diabetes Type 2 patients.
They performed a cross-sectional study using databases from three studies on Diabetes Type 2
and compared 294 Dutch to 147 Turkish Diabetes patients. One of the interesting finding in this
study was the significantly lower HDL-cholesterol of Turkish males patients (0,94mmol/l) in
comparison with Dutch males (1,08 mmol/l). The lower HDL, the higher the risk for Diabetes
and cardio vascular diseases, suggesting that lower HDL-cholesterol may be one of the reasons
for the higher prevalence of Diabetes among Turkish immigrants (Uitewaal et al., 2004).
Ujcic-Voortman et al., (2009) did a health survey to investigate the prevalence of Type 2
Diabetes among Turkish and Moroccan immigrants in Amsterdam. 375 Turkish, 314 Moroccan
and 417 Dutch individuals aged between 18 and 70 years were included. A physical
examination was done and a health interview was conducted. They found that the prevalence of
Type 2 Diabetes in the population living in Amsterdam was significantly higher in Turkish
immigrants (5.6%) and Moroccan immigrants (8.0%) when it was compared to Dutch
individuals (3.1%). They concluded that these differences in prevalence could be partly
explained by the lower socioeconomic status and higher frequency of obesity among these
ethnic minorities. The typical age of onset of diabetes in both Turks and Moroccans is
respectively one and two decades younger than in the indigenous population, suggesting that
lifestyle factors such as socio economic status or ethnicity (which can set the migrants at higher
risk for obesity) can play a role in the high prevalence of Type 2 Diabetes among immigrants
(Ujcic-Voortman et al., 2009).
Genetic factors may also play a role in the higher prevalence of Diabetes among Turkish
immigrants. For example, Arslan and colleagues (2014) investigated the association of single
nucleotide polymorphism -19, -44 and -63 in the Calpain-10 gene and Type 2 Diabetes in 211
Turkish participants, of which 93 were healthy and 118 were diagnosed with Type 2 Diabetes.
They found no significant differences in the genotype and allele distribution of single
nucleotide polymorphism between the Diabetic patients and healthy participants, but the
frequencies of 121 haplotype and the 122/121 haplotype combination were significantly higher
in Diabetic patients than in controls. This research suggests therefore that 121 haplotype and
122/121 haplotype combination of SNP-19, -44 and -63 in the Calpain-10 gene can be associated
with the development of Type 2 Diabetes among Turkish people (Arslan et al., 2014).

19
Gonen and colleagues (2012) investigated genetic factors related to Diabetes. They found that
ATP sensitive potassium channels (in Beta cells of the pancreas) are related with the mechanism
of glucose-stimulated insulin secretion. These channels are genetically coded by ABCC8 and
KCNJ11 genes. Single nucleotide polymorphisms (little changes in the genetic design) are
associated with defects in insulin secretion in Type 2 Diabetes. To investigate whether this is the
case in Turkish Diabetics, they screened 169 patients and 119 healthy participants. Indeed, they
noticed that ABCC8 exons 16 and 31 increased the likeability of Diabetes and KCNJ11 E23K
decreased the insulin secretion, suggesting that genetic factors can play a role in the prevalence
of Diabetes among Turkish people (Gonen et al., 2012).
Onat et al. (2009; 2010) performed two studies on the association between apoliprotein A-I and
apoliprotein C-III and Diabetes. More than 2000 people were followed up for approximately 7
years, showing that higher serum apoliprotein A-I levels doubled the risk for incident Diabetes
among Turkish people, above the effects of aging and low HDL-cholesterol (Onat et al., 2010).
Another study investigated whether apoliprotein C-III predicts Type 2 Diabetes in nearly 800
participants who were followed up 4 years (Onat et al., 2009). Dysfunctional HDL apoliprotein
C-III was a stronger predictor of Type 2 Diabetes than the girth of the waist among Turkish
people (Onat et al., 2009). Another study from 2008 concluded that prehypertension doubles in
average the risk for Diabetes and serves as a predictive factor for Diabetes in Turks (Onat et al.,
2008).
4.4.CausesofhighprevalenceofType2DiabetesamongMoroccanimmigrants
This section sets out the studies found with regard to explanations for the prevalence of Type 2
Diabetes among Moroccan immigrants living in West-Europe. Seven studies met the inclusion
criteria and are included in the analysis. These studies are listed in the next table.
Author(s), year
Aim(s) Study characteristics
Riffi et al., 2002, Testing the mean fasting glucose levels between Moroccan and Belgian T2D patients.
Retrospective cohort study. 96 Moroccans and 62 Belgian T2D patients
Sayad et al., 2009 Relation of diet habits of Moroccan people and Diabetes
Prospective study via questionnaire. 150 subjects with Diabetes duration of +-12,5 years.
El Achhab et al., 2009 The link of ENPP1 K121Q polymorphism with Type 2 Diabetes and obesity among Moroccan people.
Case-control study. 350 women T2D patients and 153 men. 285 healthy women and 127 men (all aged 40 years or older).
Sefri et al., 2014 Analysis of the link between polymorphism of TNF promoter gene and T2D in Moroccan people.
Case-control 307 patients and 244 healthy people.
Benrahma et al., 2012 The association between the C677T and A1298C polymorphisms of the MTHFR gene with Type 2 Diabetes and its complications.
Case control study of nearly 300 Diabetic patient and approximately 250 controls.
Cauchi et al., 2007 The association between TCF7L2 genes with Meta-analysis.

20
Type 2 Diabetes. Benrahma et al., 2011 Familial aggregation of T2D in Moroccan
people. Cohort study232 Moroccan T2D patients were included
A study of Riffi, Devrouy and Vijver from 2012 compared 62 Belgian and 96 Moroccan Diabetic
(type 2) patients, living in Belgium. They concluded that the mean fasting plasma glucose,
which is an indicator for Diabetes, were significantly higher in the Moroccan patients when
compared to mean fasting plasma glucose of the Belgian patients (respectively 186 and 142
mg/dL). That means that the Moroccan patients have a 31% higher amount of fasting plasma
glucose. Moreover, mean HbA1c was also significantly higher in the Moroccan patients
compared to the Belgian patients (respectively 8,7% and 7,6%), suggesting that these factors
could be a reason for the higher prevalence of Diabetes among Moroccan immigrants compared
to the Belgian population (Riffi et al., 2012).
Sayad, Ridouane and Essaadouni (2009) investigated the relationship between diet habits of
Moroccan patients in Morocco with Type 2 Diabetes and Type 2 Diabetes. They included 150
subjects (mean age 58 years and Diabetes duration 12,5 years in average) in their prospective
study, where they collected information through a questionnaire. They found that 61,3% of the
respondents had too high HbA1c, which means that the Diabetes control was insufficient. The
respondents were also characterized by a high amount of obesity (64%), a high frequency of
hypertension (68%) and also high lipid abnormalities (61,3%), and irregular and low levels of
physical activity. The authors also mentioned that the food mainly eaten by the Moroccan
population such as couscous and potatoes has a high glycaemic index and lipid (use of olives
and olive oil in the preparation of a meal). The management of lifestyle by controlling the diet
and the physical activity among Moroccans appeared to be challenging, suggesting that culture
plays a large role in the development and the high prevalence of Type 2 Diabetes among
Moroccan people (Sayad et al., 2009).
Besides the mean fasting glucose, diet habits, low physical activity and culture of Moroccan
immigrants, genetic factors may also play a role in the development of Diabetes among
Moroccan immigrants. For example, El Achhab and colleagues (2009) investigated the link of
ENPP1 (known of insulin down-regulation) K121Q polymorphism with Type 2 Diabetes and
obesity among Moroccan people. Diabetic patients consisted of 350 women and 153 men, while
non-Diabetics consisted of 285 women and 127 men (all aged 40 years or older). This case-
control study, which investigated the genetic factor of Diabetes and related obesity found that
the polymorphism K121Q can be associated with Type 2 Diabetes in Moroccan patients in the
presence of obesity (El Achhab et al, 2009).

21
Sefri et al. (2014) also published an article about the genetic factors. They analysed in their study
the link between polymorphism of TNF promoter gene and Type 2 Diabetes in Moroccans.
They included 307 Diabetic patients and 244 healthy controls. They found that the allele -308A
is linked with Type 2 Diabetes. Their results thus suggest that the -308A polymorphism is a
strong genetic risk factor for Type 2 Diabetes among Moroccan people (Sefri et al., 2014).
Benrahma et al. (2012) also studied the effect of genetics among Moroccans by investigating the
association between the C677T and A1298C polymorphisms of the MTHFR gene with Type 2
Diabetes and its complications. They performed a case control study with nearly 300 Moroccan
Diabetic patients and approximately 250 Moroccan controls and concluded that an evident link
is showed by their study between the MTHFR C677T polymorphism and Diabetes in Moroccan
patients (Benrahma et al., 2012). Cauchi and colleagues (2007) conducted a meta-analysis on the
association between TCF7L2 genes with Type 2 Diabetes in Moroccan and Austrian subjects,
with and without diabetes (406 Moroccan controls and 504 Moroccan Diabetics; 1074 Austrian
controls and 486 Austrian Diabetics). They concluded that, compared to any other gene variants
previously confirmed by meta-analysis, TCF7L2 can be distinguished by its tremendous
reproducibility of relationship with Type 2 Diabetes among Moroccans.
Benrahma and colleagues (2001) give another reason for the high prevalence of Diabetes among
Moroccan immigrants. They studied familial aggregation of Type 2 Diabetes in Moroccan
immigrants. 232 participants were included and 50% of the participants reported at least one
relative with Diabetes. Twenty-four percent of the participants had one parent or both parents
diagnosed with Diabetes. Mothers had Diabetes more frequently than fathers. The authors
argue that these results suggest that Diabetes is possibly transmitted maternally within the
Moroccan population (Benrahma et al., 2001). An explanation for this effect is not given.

22
5.DISCUSSIONANDCONCLUSION
The aim of this study was to perform a systemic review in order to set out the factors that play a
role in the high prevalence of Diabetes Type 2 among Turkish and Moroccan immigrants in the
Netherlands, and to examine the effect of migration on the prevalence of Diabetes Type 2.
Hence, the research question was defined as: ‘What are the explanations in the literature for the
high prevalence of Type 2 Diabetes among Turkish and Moroccan migrants in the
Netherlands?’
In this section, the results of the previous chapter are discussed. The reasons for the high
prevalence of Type 2 Diabetes among Turkish and Moroccan immigrants and the prevalence of
Type 2 Diabetes in their countries of origins are discussed. By comparing the data of the
immigrants and people living in the country of origin of the Turkish of Moroccan immigrants,
the effect of migration is examined. The results of this research are compared with the model of
Misra et al. (2007), which explained the relation between migration and Type 2 Diabetes.
Besides that, the strengths and limitations of this study are described. At the end, conclusions of
this research are drawn.
5.1.Factorsrelatedtomigration
Many factors that can play a role in the high prevalence of Type 2 Diabetes among Turkish and
Moroccan immigrants are set out in this research. Differences found between Turkish or
Moroccan immigrants and Turks living in Turkey or Moroccans living in Morocco likely point
to an effect of migration on the prevalence of Type 2 Diabetes. Nevertheless only some factors,
found in this research, can be assigned to migration.
Several studies suggest that Turkish and Moroccan immigrants adopt a more western diet when
they migrate to Europe, and this diet change seems to adversely affect their risk of developing
diabetes. For example, Turkish and Moroccan immigrants have cholesterol levels similar to
those of other Western countries and were remarkably higher than that of Turks and Moroccans
in their home country (Misra and Ganda, 2007; Porsch-Ozcurumez et al., 1999; Tazi et al., 2000).
In addition both Turkish and Moroccan immigrants have lower HDL levels compared to the
indigenous people (Uitewaal et al., 2004; Riffi et al., 2012). An adopted westernized diet can lead
to obesity, which is strongly associated with the prevalence of Diabetes among Turkish
immigrants. Both in the western countries as in Turkey and Morocco, an increasing trend of
obesity is seen and described as a predictor of Type 2 Diabetes (Bos and Agyemang, 2013;
Misra and Ganda, 2007; Onat et al., 2006; Satman et al., 2002;). Nevertheless, obesity seems to
increase as migrants get wealthier and urbanized, suggesting that migration amplifies the effect
of obesity on Diabetes, as this research also found that there is a significant difference in the

23
prevalence of obesity and Type 2 Diabetes in rural or urban areas (Bos and Agyemang, 2013;
Satman et al., 2002). Taking in consideration that largely amount of immigrants are migrated
from rural area in Turkey and Morocco to urban area in Western Europe, migration could have
a large effect on the high prevalence of Type 2 Diabetes among Turkish and Moroccan
immigrants. Also, lower socio economic status of both Moroccan as Turkish immigrants, as they
are migrated from rural areas from the country of origin, can lead to a higher prevalence of
Diabetes in comparison with natives (Ujcic-Voortman et al., 2009). Age is several times
mentioned as a factor of development of Diabetes among immigrants (Onat 2006; Rguibi &
Belahsen, 2006; Tazi et al., 2000). The higher prevalence of Type 2 Diabetes among immigrants
can also be explained by age, because first generation immigrants from Turkey and Morocco in
the Netherlands are aging (RIVM, 2011).
5.2.Factorsrelatedtoethnicity
Some factors that are found in this research, which are related with Type 2 Diabetes, cannot be
assigned to migration. Examples of these factors are genetic predisposition and culture.
Genetic factors may play a role in the higher prevalence of Diabetes among Turkish immigrants,
such as single nucleotide polymorphisms (SNPs), which are associated with defects in insulin
secretion in Type 2 Diabetes (Arslan et al., 2014; Gonen et al., 2012) and higher levels of
apoliprotein A-I and apoliprotein C-III (Onat et al., 2008). Also other polymorphisms are found
in Moroccans (Benrahma et al., 2012; Sefri et al., 2014). Furthermore, TCF7L2 gene seems to have
a stronger association with Diabetes for Moroccans than for Austrians (Cauchi et al., 2007).
Besides, dysfunctional HDL apoliprotein C-III was a stronger predictor of Type 2 Diabetes than
the girth of the waist among Turkish people (Onat et al., 2009), suggesting that genetics may
play a larger role than obesity. Obesity can also be due to genetics in Moroccan people (El
Achhab et al, 2009).
Culture is a factor that is mentioned several times as a cause of Diabetes among Turkish and
Moroccan immigrants. For example, the management of lifestyle by controlling the diet and the
physical activity among Moroccans seemed challenging, meaning that culture plays a great role
in the development of Type 2 Diabetes (Sayad et al., 2009). It is shown that 61,3% of Moroccan
diabetes patients had too high HbA1c, which means that the Diabetes control was insufficient
(Sayad et al., 2009). Also, cheap availability of high percentage fat and energy food in Morocco
and minimum physical activity (Bos & Agyemang, 2013; Sayad et al., 2009) is a part of the
Moroccan culture and can lead to high prevalence of Type 2 Diabetes, suggesting that these
factors are not due to migration, as Moroccans living in Morocco have also Diabetes that are
possibly caused by cultural factors.
24
Several factors are the same for immigrants as for their counterparts in their home country,
suggesting the origin is either culture or genetics but not immigration. For example,
hypertension and obesity are both higher in Diabetic Turks and Moroccans in their home
country (Onat et al., 2006; Satman et al., 2002; Bentata et al., 2015; Sayad et al., 2009).
Furthermore, females seem to have more obesity in Morocco and Turkey (Satman et al., 2002;
Tazi et al., 2000) and more hypertension in Turkey (Satman et al., 2002), suggesting that gender
can play a role in the prevalence of Diabetes in Moroccans and Turks, unrelated to migration.
However, it is unclear whether this gender difference is due to culture or genetics.
5.3.Factorswhicharenotclearlyrelatedtoeitherimmigrationorethnicity
Some factors that can contribute to the high prevalence of Type 2 Diabetes among Turkish and
Moroccan immigrants are difficult to assign to migration or ethnicity. For example literature
showed that Turkish and Moroccan immigrants, compared to the indigenous people, have
significantly high risk for higher mean non-fasting plasma glucose levels, which is a predictor of
Diabetes (Uitewaal et al., 2002; Riffi et al., 2012). It is also shown in the literature that Diabetes is
possibly transmitted maternally within the Moroccan population (Benrahma et al., 2011). An
explanation for this effect is not given but it can be both due to the cultural influence through
the mother as well as genetic factors.
Many factors that explain the high prevalence of Type 2 Diabetes among Turkish and Moroccan
immigrants, found in this research seem to correspond with the model of Misra et al., (2007). In
that model (showed in chapter 2) Type 2 Diabetes is caused by metabolic perturbations, resulted
from either migration related factors as ethnicity related factors. Interestingly, not all factors
that are discussed in the model of Misra et al. (2007) are found in this research, such as the effect
of smoking and stress on the prevalence of Type 2 Diabetes. Also ‘low self-esteem’ and ‘loss of
support’, which are subdivided under ‘psycho-social factors’ in the model, are not found in the
literature about Turkish and Moroccan immigrants, creating a gap in the literature.
5.4.Strengthsandlimitations
Some strengths and limitations of this systemic review about the reasons of Type 2 Diabetes
with regard to the migration of Moroccan and Turkish ethnic minorities have to be mentioned.
First of all, this review gave more insight about the high prevalence of Moroccan and Turkish
immigrants, the situation in the country of origin and the effect of migration on Type 2
Diabetes. The amount of literature about in particular Moroccan and Turkish immigrants living
in the Netherlands is small. An increased understanding about this subject is important because
these groups of immigrants show a significantly higher prevalence in comparison with the
native population and they are increasing in amount. This research contributes to the

25
knowledge about Type 2 Diabetes and these immigrants, which is important to set up or adjust
the healthcare in order to prevent the disease and decrease the healthcare costs.
A limitation of this research was the small number of studies on this topic. It is also remarkable
that the research syntax in used databases has mainly found articles of the same first author and
mostly same co-workers, like Uitewaal and colleagues. This is strengths and limitation at the
same time, as the writers are very experienced in the topic Diabetes and ethnicity, but may also
be researcher biased. Besides that, since PubMed is a biomedical database, a lot of literature
about genetics is found and included in this research. At last, the search in this research was
limited to articles in English. And only articles that were reachable with a student account for
Pubmed and guest account for Scopus are used.
5.5.Conclusion
This study investigated the explanations in the literature for the high prevalence of Diabetes
Type 2 among Turkish and Moroccan migrants in the Netherlands? The first sub question
focussed on the knowledge in the literature about the prevalence of Type 2 Diabetes in
countries of origin of these migrants, Turkey and Morocco. The second sub-question focussed
on the influence of migration on the development of Type 2 Diabetes.
This review found that both immigration as well as ethnicity could account for the higher
prevalence of Type 2 Diabetes among Turkish and Moroccan immigrants in the Netherlands.
Diabetes also seems to be a challenging health problem in Turkey and Morocco, suggesting that
Diabetes among Turks and Moroccans is not only due to migration. ‘Westernizing’ of lifestyle
or genetic factors could play a role. Many lifestyle habits or cultural influences such as dietary
factors of Turkish and Moroccan minorities are also seen in the country of origin. Nevertheless,
many immigrants are migrated from rural areas and living in urban areas in the host countries.
Also in the country of origin is seen that rural areas are less affected by Diabetes. Migration into
urban areas is associated with increases in obesity. Diabetes has a very convincing and strong
relation with obesity, which set the ethnic minorities at a higher risk, since they can adopt an
unhealthy lifestyle and have less physical activity, especially in urban areas. Moreover, some
alterations in genetic codes seem to be important in the development of Diabetes among
Turkish and Moroccan immigrants. This is in concordance with the model published by Misra
and colleagues (2007), showed in chapter 2. They noticed that migration could have a large
effect on lifestyle and psychosocial aspects, but also ethnicity can be an independent factor of
the development of Type 2 Diabetes. However, a gap in literature was found, since articles
about smoking and stress in particular for Turkish and Moroccan immigrants were not found in
this research.

26
REFERENCES
- ADA, American Diabetes Association, Type 2 Diabetes in Children and Adolescents, Pediatrics 2000;105;671
- Adriaanse MC, Pouwer F, Dekker JM, Nijpels G, Stehouwer CD, Heine RJ, et al.Diabetes-related symptom
distress in association with glucose metabolism and comorbidity: the Hoorn Study. Diabetes Care, 2008; 31(12):
2268-70.
- Agyemang C, Bhopal RS. Is the blood pressure of South Asian adults in the UK higher or lower than that in
European white adults~ A review of cross-sectional data. J Human Hypertens 2002; 16: 739-51.
- Arslan E, Acik L, Gunaltili G, Ayvaz G, Altinova AE1, Arslan M. The effect of calpain-10 gene polymorphism on
the development of type 2 diabetes mellitus in a Turkish population. Endokrynol Pol. 2014;65(2):90-5.
- Attridge M, Creamer J, Ramsden M, Cannings-John R, Hawthorne K. Culturally appropriate health education
for people in ethnic minority groups with type 2 diabetes mellitus. Cochrane Database of Systematic Reviews
2014, Issue 9.
- Benrahma H, Abidi O, Melouk L, Ajjemami M, Rouba H, Chadli A, Oudghiri M, Farouqui A, Barakat A.
Association of the C677T polymorphism in the human methylenetetrahydrofolate reductase (MTHFR) gene
with the genetic predisposition for type 2 diabetes mellitus in a Moroccan population. Genet Test Mol
Biomarkers. 2012 May;16(5):383-7.
- Benrahma H., Arfa I, Charif M, Bounaceur S, Eloualid A, Boulouiz R, Nahili H, Abidi O, Rouba H et al.Maternal
Effect and Familial Aggregation in a Type 2 Diabetic Moroccan Population.Journal of Community Health.
December 2011, Volume 36, Issue 6, pp 943-948
- Bentata Y, Chemlal A, Karimi I, El Alaoui F, Haddiya I, Abouqal R. Diabetic kidney disease and vascular
comorbidities in patients with type 2 diabetes mellitus in a developing country. Saudi J Kidney Dis Transpl.
2015 Sep;26(5):1035-43.
- Bos M. and Agyemang C. (2013) “Prevalence and complications of diabetes mellitus in Northern Africa, a
systematic review,” BMC Public Health, vol. 13, no. 1, article 387.
- Burden AC. Blood pressure control and cardiovascular risk in patients of Indo-Asian and African-Caribbean
descent. Int JClin Pract 1998; 52 (6): 388·94. Brancati FL, Kao WH, Folsom AR, Watson RL, Szklo M. Incident
type 2 Diabetes mellitus in African·American and white adults: the Atherosclerosis Risk in Communities Study.
2000; 283 :2253-9.
- Cauchi S, El Achhab Y, Choquet H, Dina C, Krempler F, Weitgasser R, Nejjari C, Patsch W, Chikri M, Meyre D,
Froguel P. TCF7L2 is reproducibly associated with type 2 diabetes in various ethnic groups: a global meta-
analysis. J Mol Med (Berl). 2007 Jul;85(7):777-82.
- CBS (2014), statline, Bevolking; kerncijfers augustus 2014
- Chaturvedi N, Jarrett J, Morrish N, Keen H, Fuller JH. Differences in mortality and morbidity in African
Caribbean and European people with non-insulin-dependent Diabetes mellitus: result of 20-year follow-up of a
London cohort of a multinational study. BM) 1996; 313: 848-52.
- Chen B, Zhang X, Xu X, Lv X, Yao L, Huang X, Guo X, Liu B, Li Q, Cui C.Pak J Med Sci. 2013 Sep;29(5):1147-52.
Diabetes education improves depressive state in newly diagnosed patients with type 2 Diabetes.
- Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ.Increasing prevalence of Type II
Diabetes in American Indian children. Diabetologia 1998; 41(8): 904-10.
- Diabetesfonds.nl/over-diabetes/diabetes-in-het-algemeen/diabetes-in-cijfers, retrieved 24 June 2016
- El Achhab Y., Meyre D., Bouatia-Naji N., Berraho M., Deweirder M., Vatin V., et al. Association of the ENPP1
K121Q polymorphism with type 2 diabetes and obesity in the Moroccan population. Diabetes Metab, 35 (1)
(2009), pp. 37–42
- Gonen MS, Arikoglu H, Erkoc Kaya D, Ozdemir H, Ipekci SH, Arslan A, Kayis SA, Gogebakan B. Effects of
single nucleotide polymorphisms in K(ATP) channel genes on type 2 diabetes in a Turkish population. Arch
Med Res. 2012 May;43(4):317-23.
- Guell C. (2011) Diabetes management as a Turkish family affair: chronic illness as a social experience. Annals of
Human Biology, Vol. 38, No. 4: Pages 438-444
- Hartemink N, Boshuizen HC, Nagelkerke NJ, Jacobs MA, van Houwelingen HC.Combining risk estimates from
observational studies with different exposure cutpoints: a meta-analysis on body mass index and Diabetes type
2. Am J Epidemiol 2006b; 163(11): 1042-52
- Jenum, A.K., Diep, L.M., Holmboe-Ottesen, G., Holme, I.M.K., Kumar, B.N., Birkeland, K.I.,"Diabetes

27
susceptibility in ethnic minority groups from Turkey, Vietnam, Sri Lanka and Pakistan compared with
Norwegians - The association with adiposity is strongest for ethnic minority women",2012,"BMC Public
Health","12","1", 150,"","",,16,"
- Kleefstra N, Landman GW, Houweling ST, Ubink-Veltmaat LJ, Logtenberg SJ, Meyboom-de Jong B, et
al.Predicton of mortality in type 2 Diabetes from health-related quality of life (ZODIAC-4). Diabetes Care, 2008;
31(5): 932-3.
- Landman GW, Hateren KJ van, Kleefstra N, Groenier KH, Gans RO, Bilo HJ.Health-related quality of life and
mortality in a general and elderly population of patients with type 2 Diabetes (ZODIAC-18). Diabetes Care,
2010; 33(11): 2378-82.
- Looise BJ, Poel F, van der Bos V (2006) Diabeteseducatie in Nederland-state of art van methoden en materialen.
Nationaal Instituut voor Gezondheidsbevordering en Ziektepreventei (NIGZ)
- Luijben AHP, Kommer GJ Tijd en toekomst. Deelrapport van de VTV 2010 Van gezond naar beter. RIVM-
rapport nr. 270061008. Bilthoven: RIVM,2010.
- Magnus MH. Cardiovascular health among African-Americans: a review of the health status, risk reduction,
and intervention strategies. Am JHealth Promot 1991; 5: 282-90. Cappuccio FP. Ethnicity and cardiovascular
risk: variations in people of African ancestry and South Asian origin. JHum Hypertens 1997; 11:571-6.
- Maher B .Personal genomes: The case of the missing heritability. Nature 2008c; 456(7218): 18-21
- Meline T (2006). Selecting studies for systematic review: inclusion and exclusion criteria. Contemp Issues in
Commun Sci Disord; 33: 21–27.
- Misra A., Ganda O.P. (2007) Migration and its impact on adiposity and type 2 Diabetes Nutrition, 23(9), pp. 696-
708.
- Mokdad A.H., Bowman B.A., Ford E.S., Vinicor F.,. Marks J.S, Koplan J.P. The continuing epidemics of obesity
and Diabetes in the United States. AMA, Journal of the American Medical Association, 286 (2001), pp. 1995-200
- Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks JS: Prevalence of obesity, Diabetes,
and obesity-related health risk factors, 2001. JAMA 2003, 289:76-79.
- NDF, Rapport Routeplanner Diabetes preventie, 2010
- Onat A, Hergenç G, Ayhan E, Uğur M, Kaya H, Tuncer M, Can G. Serum apolipoprotein C-III in high-density
lipoprotein: a key diabetogenic risk factor in Turks. Diabet Med. 2009 Oct;26(10):981-8.
- Onat A, Hergenç G, Bulur S, Uğur M, Küçükdurmaz Z, Can G. The paradox of high apolipoprotein A-I levels
independently predicting incident type-2 diabetes among Turks. Int J Cardiol. 2010 Jun 25;142(1):72-9.
- Onat A, Yazici M, Can G, Kaya Z, Bulur S, Hergenç G. Predictive value of prehypertension for metabolic
syndrome, diabetes, and coronary heart disease among Turks. Am J Hypertens. 2008 Aug;21(8):890-5.
- Onat A., Hergenc G., Uyarel H., Can G., Ozhan H. (2006). Prevalence, incidence, predictors and outcome of
Type 2 Diabetes in Turkey. The Anatolian Journal of Cardiology 2006; 6: 314-21
- Poortvliet MC, Schrijvers CTM, Baan CA. Diabetes in Nederland. RIVM-Rapport 260322001. RIVM, Bilthoven,
2007. QUI-databank. H-MIS (Minimale Interventiestrategie Stoppen-met-roken voor de huisartsenpraktijk)
2007.
- Popkin BM, Adair LS, Shu Wen NG: 2012. Global nutrition transition and the pandemic of obesity in developing
countries. Nutr Rev. 70 (1): 3-21.
- Porsch-Ozcurumez M., Bilgin Y., Wollny M., Gediz A., Arat A., Karatay E., et al. Prevalence of risk factors of
coronary heart disease in Turks living in Germany: the Giessen Study. Atherosclerosis, 144 (1999), pp. 185�198
- Rguibi M, Belahsen R. Prevalence and associated risk factors of undiagnosed diabetes among adult Moroccan
Sahraoui women. Public Health Nutr, 9 (6) (2006), pp. 722�727.
- Riffi A., Devrouy D., van de Vijver E., A comparison between Moroccan and Belgian type-2 diabetic patients.
Acta Clin Belg. 2012 Jul-Aug;67(4):246-9.
- RIVM, Sanderse C, Verweij A, Beer J. Migratie: Wat waren de belangrijkste ontwikkelingen in het verleden? In:
Volksgezondheid Toekomst Verkenning, Nationaal Kompas Volksgezondheid. Bilthoven: RIVM,
<http://www.nationaalkompas.nl> Nationaal Kompas Volksgezondheid\Bevolking\Migratie, 21 september
2011.
- Satman I, Yilmaz T, Sengül A, , Salman S, Salman F, Uygur S., Bastar I, Tütüncü Y, Sargin M, Dinççag N,
Karsidag K, Kalaça S, Özcan C, King H. Population-Based Study of Diabetes and Risk Characteristics in Turkey
Results of the Turkish Diabetes Epidemiology Study. Diabetes Care September 2002 vol. 25 no. 9 1551-1556.
- Sayad N.O., Ridouane S., Essaadouni L.Diet habits of type 2 diabetic patients living at Marrakech, Morocco.
Médecine des Maladies Métaboliques. Volume 3, Issue 5, November 2009, Pages 544–547.

28
- Schram MT, Baan CA, Pouwer F.Depression and quality of life in patients with Diabetes: a sysemiatic review
from the European depression in Diabetes (EDID) research consortium. Curr Diabetes Rev, 2009; 5(2): 112-9.
- Sefri H, Benrahma H, Charoute H, Lakbakbi el Yaagoubi F, Rouba H, Lyoussi B, Nourlil J, Abidi O, Barakat A.
TNF A -308G>A polymorphism in Moroccan patients with type 2 diabetes mellitus: a case-control study and
meta-analysis. Mol Biol Rep. 2014 Sep;41(9):5805-11.
- Shi, Y. Hu, F.B. (2014). "The global implications of diabetes and cancer". The Lancet 383 (9933): 1947–8.
- Shoback, edited by David G. Gardner, Dolores (2011). "Chapter 17". Greenspan's basic & clinical endocrinology
(9th ed.). New York: McGraw-Hill Medical. ISBN 0-07-162243-8.
- Summerson JH, Konen JC, Dignan MB. Racial differences in lipid and lipoprotein levels in Diabetes.
Metabolism.1992; 41:851-5.
- Tazi M. A., Abir-Khalil S., Chaouki N. et al., “Prevalence of the main cardiovascular risk factors in Morocco:
results of a National Survey, 2000,” Journal of Hypertension, vol. 21, no. 5, pp. 897–903, 2003.
- Uitewaal P.J.M, Voorham A.J.J., Bruijnzeels M.A., Berghout A., Bernsen R.M.D., Trienekens P.H., Hoes A.W.,
Thomas S., (2005) No clear effect of diabetes education on glycaemic control for Turkish type 2 diabetes
patients: a controlled experiment in general practice. Neth J Med 63, 428–434.
- Uitewaal P.J.M., A.N. Goudswaard, L.J. Ubnik-Veltmaat, M.A. Bruijnzeels, A.W. Hoes, S. Thomas.
Cardiovascular risk factors in Turkish immigrants with type 2 Diabetes mellitus: comparison with Dutch
patients. Eur. J. Epidemiol., 19 (2004), pp. 923–929
- Uitewaal PJM, Bruijnzeels MA, Bernsen, Voorham AJJ, Hoes AW, Thomas S. Diabetes care in Dutch general
practice: differences between Turkish immigrants and Dutch patients Eur. J. Public Health, 14 (2004), pp. 15–18.
- Ujcic-Voortman Joanne K. , Schram Miranda T. , Jacobs-van der Bruggen Monique A. , Verhoeff Arnoud
P., Baan Caroline A. Diabetes prevalence and risk factors among ethnic minorities The European Journal of
Public HealthOct 2009,19(5)511-515
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans
V, et al. (2012). "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a
systematic analysis for the Global Burden of Disease Study 2010.". Lancet 380 (9859): 2163–96.
- Wändell PE, Carlsson A, Steiner KH. CurrDiabetes Prevalence of Diabetes among immigrants in the Nordic
countries.Rev. 2010 Mar;6(2):126-33.
- Wei JN, Sung FC, Lin CC, Lin RS, Chiang CC, Chuang LM.National surveillance for type 2 Diabetes mellitus in
Taiwanese children. JAMA, 2003; 290(10): 1345-50.
- Weijers RNM, Bekedam DJ, Oosting H. The prevalence of type 2 Diabetes and gestational Diabetes mellitus in
an inner city multi-ethnic population. Eur J Epidemioll998; 14: 693-9.
- WHO (2013). Diabetes Fact sheet N°312". October 2013. Retrieved 25 June 2016.
- WHO(2016), Global report on Diabetes. www.who.int/Diabetes/global-report/en/ Geneva, 2016