Therapy for NAFLD “Are we there...
34
Therapy for NAFLD “Are we getting there?” Sanjay Bhagani Royal Free London/UCL
Transcript of Therapy for NAFLD “Are we there...

Therapy for NAFLD “Are we getting there?”
Sanjay Bhagani
Royal Free London/UCL

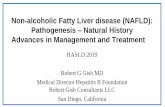
What is NAFLD ?
Steatosis/inflammation
Cirrhosis
Fibrosis
Steatosis
• Non-Alcoholic Fatty Liver Disease
• Wide disease range from simple steatosis to cirrhosis
Steatosis NASH Cirrhosis
12-40% 15%

Kotronen, Arterioscler Thromb Vasc Biol 2008
NAFLD: Potential consequences
HCC

NASH is the Subtype of NAFLD
that Primarily Progresses
NAFL
Stable
Liver Failure
NAFLD
Cirrhosis
10-15%
NASH
Death
40-60%
20-30%
HCC (Annual incidence
2%)
65-75%
Stable
Ludwig 1980; Diehl 1988; Lee 1989; Powell 1990; Bacon 1994; Matteoni 1999; Angulo 1999; Caldwell 1999; Ponawala 2000; Contos 2001;
Ong 2001; Bugianesi 2002; Ratziu 2002; Harrisson 2003; Marchesini 2003; Younossi 2004; Fassio 2004; Sanyal 2004; Ong 2005; Adams 2005;
Ong 2006; Rafiq 2008; Stepanova 2010; Younossi 2012.
NASH progressive in a sub-set of patients

Fibrosis stage is predictive of survival
229 biopsy-proven NAFLD, FU 26 yrs 619 biopsy-proven NAFLD, FU 12.6 yrs
F>2
F<3
Controls
F0
F1
F2-F3
F4
Angulo P et al. Gastroenterology 2015 Ekstedt M et al. Hepatology 2015
Cause of death: cardiovascular 38-43%, cancer 19%, cirrhosis 4-8% HCC 1-5%
Independent predictors: fibrosis, diabetes, tobacco, statin use

NASH
Apoptosis
Inflammation
Cirrhosis
HCC
Fibrosis
Metabolic
abnormality
Hepatic Fat
The molecular engine that drives disease progression
Adapted from Arun Sanyal, NASH Symposium Paris June 2015

Appropriate End-points for therapeutics in NAFLD
• Early phase trials – Populations with NASH or at high-risk of NASH
– Primary end-points based on mechanism of drug tested; e.g. reduction in hepatic fat by MR-Proton Density Fat Fraction, CAP
• Phase 3 studies – Biopsy proven NASH (NAS score >2) with F2+ fibrosis
– Primary End-point • Complete resolution of steatohepatitis and no worsening of
fibrosis
• At least one point improvement in Fibrosis score with no worsening of steatohepatitis

Therapeutics for NASH
• Metabolic abnormalities
• Cell-stress/apoptosis and inflammation
• Antifibrotics
• Gut-Liver axis

NASH – multiple potential targets
Banini & Sanyal, Curr. Opin. Gastroenterol. 2017

What works and what doesn’t work – data to date…
• Diet/exercise – 5% weight loss improves steatosis – 7% improvement in inflammation – >10% for improvement in fibrosis
• Insulin sensitising agents – Glitazones/Metformin – ?effective in pre-diabetics/T2DM
• Anti-lipid therapies – Fibrates, statins may improve lipids BUT no/little effect on
hepatic inflammation/fibrosis
• Anti-oxidants – Vitamin E works (but risk of Prostate cancer??)

Other/upcoming agents for ‘metabolic’ targets

OCA)
•Semisynthetic bile acid analog (6α-ethyl-chenodeoxycholic acid) 100
times more potent than chenodeoxycholic acid in binding farnesoid X
receptor
• Treatment with OCA has been associated with – Improved insulin
sensitivity
– Reductions in markers of liver inflammation and fibrosis
– Reductions in triglyceride levels
– Dose-related weight loss
– OCA was generally well tolerated; adverse effects were similar across
treatment groups
– Increases in LDL and reductions in HDL
Mudaliar S, et al. Gastroenterology. 2013;145:574-582.
Obetichocolic Acid (OCA)

FLINT Phase 2 Trial Design The Farnesoid X Receptor Ligand Obeticholic Acid (OCA) in NASH Treatment
(OCA vs. Placebo for 72 Weeks N=283)
Fibrosis Improvement &
No worsening of Steatohepatitis
Lipid Parameters Measured
5 0
**
Total
cholesterol
Triglycerides
LDL
HDL
4 0
4 3 %
% o
f R
es
po
nd
ers
OCA
Pla
OCA
Pla
OCA
Pla
OCA
Pla
3 0
Baseline
190
197
112
111
42
44
196
178
2 0
Δ Baseline -
72 wks
+6*
-7*
+9*
-8*
-1*
+1*
-20
-7
2 1 %
1 0
Δ Baseline -
96 wks
-12
-8
-12
-12
+1
+1
-3
0
0
P la c e bo O be tic holic Ac id
Pruritus higher in OCA group (23% vs 6%) 1 dc’d OCA
Other AEs were similar to placebo and most SAE unrelated to therapy
Brent A Neuschwander-Tetri, et al. Lancet. 2014.

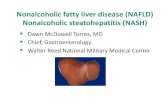
45%
61%
53%
46%
35%
22%
12%
21%
38% 35%
31%
19%
13% 13%
0%
10%
20%
30%
40%
50%
60%
70%
PrimaryEndpoint
Steatosis LobularInflammation
Ballooning Fibrosis NASHresolution
PortalInflammation
% of Patients with Improvement OCA Pbo
FLINT: Primary and Secondary Histological Endpoints
P=0.0002 P=0.001 P=0.006 P=0.03 P=0.004 P=0.08 P=0.90
• LDL-C increased • pruritus
Neueschwander-Tetri BA et al. Lancet 2014

Elafibranor (GFT505): mechanism of action

Placebo
(n = 92)
Elafibranor 80 mg (n = 93)
Elafibranor 120 mg (n = 89)
p (120 mg vs placebo)
Primary endpoint* 17 % 23 % 21 % 0,28
ITT analysis
Placebo
(n = 76)
Elafibranor 80 mg (n = 83)
Elafibranor 120 mg (n = 75)
p (120 mg vs placebo)
Primary endpoint* 11 % 20 % 20 % 0,018
Post hoc analysis in NAS ≥ 4
16
One year elafibranor vs. placebo in NASH
*Reversal of NASH without worsening of fibrosis
Ratziu et al, Gastroenterology 2016




Cell-stress/apoptosis and inflammation inhibitors

GS-4997 Alone (Apoptosis Signal-regulating Kinase (ASK-
1) Inhibitor) or in
Combination with Simtuzumab—Phase II Trial
• Phase 2, Randomized, Open Label Study Evaluating the Safety,
Tolerability, and Efficacy of GS-4997 Alone or in Combination With
Simtuzumab in NASH and Fibrosis Stages F2-F3
• Intervention:
– Arm A: GS-4997 6 mg QD+SIM 125 mg SQ weekly for 24 wks
– Arm B: GS-4997 18 mg QD+SIM 125 mg SQ weekly for 24 wks
– Arm C: SIM 125 mg SQ weekly for 24 weeks
• NASH with F2-F3
• Primary Outcomes:
– Adverse event of GS-4997 (Treatment-emergent SAE, worsening AST & ALT)
– Percent who prematurely discontinuation due to AE
ClinicalTrials.gov. NCT02466516. https://www.clinicaltrials.gov/ct2/show/NCT02279524.

GS-4997, an inhibitor of apoptosis signal-regulating kinase (ASK1), alone or in combination with Simtuzumab - results
Loomba R et al, AASLD 2016
43 37
3
30 30
7
20 20 20
0
20
40
60
80
100
18 mg ± SIM 6 mg ± SIM SIM
Perc
ent
of
Sub
ject
s
Fibrosis Improvement
Fibrosis Improvement
without NASH Worsening *
13/30 8/27 2/10 11/30 8/27 2/10
Progression to Cirrhosis
1/30 2/27
2/10
• GS4997 (2 doses) + Sim vs Sim alone • 2:2:1:1:1 randomization, Stratified by diabetes • NASH, NAS ≥ 5, F2-3

Reproduced from Xu et al. Biomolecules 2015;5(3):1563—1579. © 2015 by the authors; licensee MDPI, Basel, Switzerland.
Taken from an open access article distributed under the terms and conditions of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0/).
®
11
CCR2 and CCR5 Promote Obesity-Induced
Inflammation and Insulin Resistance

®
NCT02217475
18
HEP DART 2015
CENTAUR: NASH with Fibrosis Phase 2b Study
Global study
289 subjects enrolled
Key eligibility criteria
Biopsy diagnosis of
NASH with fibrosis
Enriched for patients
with
— T2DM
— High BMI with
>1 criteria of metabolic syndrome
— Bridging fibrosis
and/or definite NASH
Random
izati
on 1
:1
CVC 150 mg
CVC 150 mg
CVC 150 mg
Placebo
1:1
Placebo
(Year 2)
Primary endpoint
2-point improvement in NAS
without worsening of fibrosis)
Key secondary
endpoint
Resolution of NASH without
worsening of fibrosis
Other endpoints
Change in fibrosis stage
Collagen morphometry
α-SMA, CK-18
Validated fibrosis scores
Noninvasive imaging and
biomarkers
Kidney function
Final biopsy
Final
Analysis
Primary
Analysis
(Year 1)
Baseline
Primary endpoint biopsy
Screening biopsy

6%
10% 8%
20%
0%
5%
10%
15%
20%
25%
Complete Resolution of NASH ANDNo Worsening of Fibrosis
Improvement in Fibrosis Stage ANDNo Worsening of NASH
CENTAUR: primary endpoint not met but key secondary endpoint on fibrosis improvement met
19% 16%
0%
5%
10%
15%
20%
25%
≥2-point Improvement in NAS AND No Worsening of Fibrosis
Placebo (N=144) CVC (N=145)
PRIMARY ENDPOINT SECONDARY ENDPOINTS
P< 0.02
Sanyal A et al, AASLD 2016

Antifibrotics





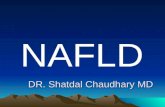
NAFLD Pipeline
CONFIDENTIAL
Drug/company (MoA)
FDA Fast Track for NASH
Breakthrough designation
NASH* landscape: Segmentation by company
Sources: pipeline databases, company websites, competitive intelligence analysis.
Preclinical: only selected projects to reach clinical development in 2016 are shown. More than one mode of action may be applicable for a given drug.
*NASH compounds only. Projects with only NAFLD patients are not considered
● INT-767/Intercept
● PRX-106/Protalix
● GRI-0621/GRI Bio
● RTU-1096/Sucampo
● Solithromycin/Cempra
● VLX103/Verlyx
● IMM-124-E/Immuron
● NP-201 program/NGM/Merck
● DUR-928/Durect
● BMS-986171/BMS
● VK-2809/Viking ● Aramchol/Galmed
● AZD4076/AZ
● Elafibranor/Genfit
● GS-4997/Gilead
● BMS-986036/BMS
● NGM-282/NGM
● LY-3202328/Lilly
● GS-0976/Gilead Nimbus
● NC-101/Naia
● KBP-042/Nordic Bioscience
● A4250/Albireo
● MSDC-0602/Octeta
● ZGN-839/Zagfen
● Semaglutide/Novo
● NGM313/NGM Bio
● VK-0214/Ligand
● RYI-018/Ruiyi
● FXR/Allergan/Akarna
● EDP-305/Enanta
● LJN452/Novartis/NIBR
● GS-9674/Gilead
● Obeticholic acid/Intercept
● GKT831/GenKyotex
● Simtuzumab/Gilead
● Emricasan/Conatus
● Cenicriviroc/Allergan/Tobira
● GR-MD-02/Galectin
● ND-L02-s0201/Nitto Denko
● MN-001/MediciNova
● JKB-121/Taiwan J Pharma
● Bertilimumab/Immune Therapeutics
● TEV-45478/Teva
● PXS-4728/BI
● MGL-3196/Madrigal
● IONIS-DGAT2Rx/Ionis
● FG-3019/FibroGen
● BOT-191/BiOrion
● IVA-337/Inventiva
● saroglitazar/Zydus
● Volixibat/Shire
● DS-102/Afimmune
● DRX-065/DeuteRx
●MT-3995/Mitsubishi
● LMB-763/Novartis
● UD-014/Ube
X
X
X
X
X
X
X
X X
X
X
X
X
X
X
Interaction with company in progress
Not available for partnering
Covered by internal program
X Declined or MoA
not interesting
Lipid metabolism
Anti-inflammatory
Glucose
metabolism
Antifibrotic
Oxidative stress
Immunomodulatory
Other
Phase II Phase IIb Phase IIa Phase I Preclinical

Future markets….

Targeted therapies for NAFLD
• A better understanding of the pathaphysiology
• Biomarker development for prediction of progression, inflammation and fibrosis
• Imaging/sonographic modalities

Acknowledgements
• Patrick Ingiliz
• Manolis Tsotchasiz
• Maud Lemoine
• Laurent Sefarty
• Zobair Yaunossi