Non-alcoholic Fatty Liver Disease (NAFLD) in Children NAFLD... · Non-alcoholic Fatty Liver Disease...
16
Pediatrics Grand Rounds 18 September 2009 University of Texas Health Science Center at San Antonio 1 Non-alcoholic Fatty Liver Disease (NAFLD) in Children Carisse Orsi, MD Pediatric Endocrine Fellow September 18, 2009 Goals and Objectives Define NAFLD Discuss the theories behind the pathophysiology of the disease Know how to diagnose NAFLD Understand the disease progression Discuss current studies for the treatment of fatty liver What is Non-Alcoholic Fatty Liver Disease (NAFLD)? A chronic liver condition characterized by: Hepatic fat accumulation (in the absence of ethanol abuse & other identifiable causes) Insulin resistance Frequently associated with impaired glucose intolerance or type 2 diabetes NAFLD Hepatic fat accumulation (steatosis) may range from simple steatosis Natural history poorly understood, no large long-term studies Non-Alcoholic Steatohepatitis (NASH) NASH is fat accumulation plus Necrosis inflammation Fibrosis May progress to portal hypertension and cirrhosis
Transcript of Non-alcoholic Fatty Liver Disease (NAFLD) in Children NAFLD... · Non-alcoholic Fatty Liver Disease...
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
1
Non-alcoholic Fatty Liver Disease (NAFLD)
in ChildrenCarisse Orsi, MD
Pediatric Endocrine FellowSeptember 18, 2009
Goals and Objectives
Define NAFLDDiscuss the theories behind the pathophysiology of the diseaseKnow how to diagnose NAFLDUnderstand the disease progressionDiscuss current studies for the treatment of fatty liver
What is Non-Alcoholic Fatty Liver Disease (NAFLD)?
A chronic liver condition characterized by:
Hepatic fat accumulation (in the absence of ethanol abuse & other identifiable causes)
Insulin resistance
Frequently associated with impaired glucose intolerance or type 2 diabetes
NAFLD
Hepatic fat accumulation (steatosis) may range from simple steatosis
Natural history poorly understood, no large long-term studies
Non-Alcoholic Steatohepatitis(NASH)
NASH is fat accumulation plusNecrosisinflammation Fibrosis
May progress to portal hypertension and cirrhosis
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
2
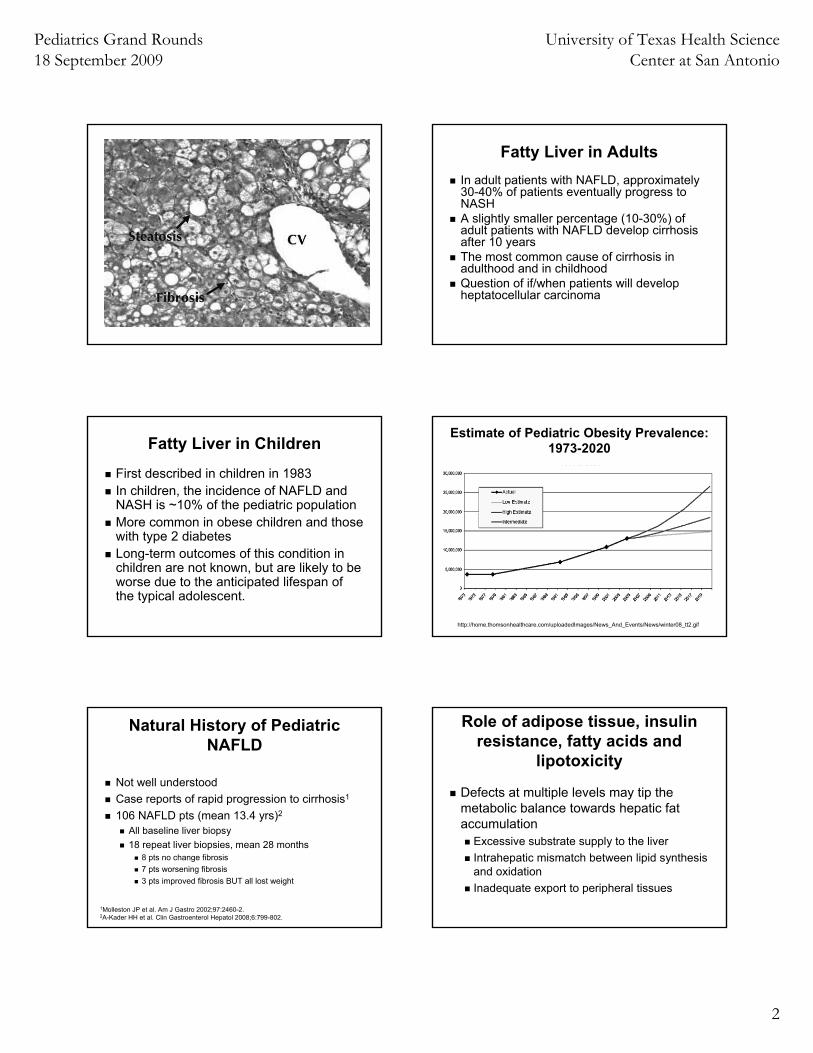
Fatty Liver in AdultsIn adult patients with NAFLD, approximately 30-40% of patients eventually progress to NASH A slightly smaller percentage (10-30%) of adult patients with NAFLD develop cirrhosis after 10 yearsThe most common cause of cirrhosis in adulthood and in childhoodQuestion of if/when patients will develop heptatocellular carcinoma
Fatty Liver in Children
First described in children in 1983In children, the incidence of NAFLD and NASH is ~10% of the pediatric population More common in obese children and those with type 2 diabetesLong-term outcomes of this condition in children are not known, but are likely to be worse due to the anticipated lifespan of the typical adolescent.
http://home.thomsonhealthcare.com/uploadedImages/News_And_Events/News/winter08_tt2.gif
Estimate of Pediatric Obesity Prevalence: 1973-2020
Natural History of Pediatric NAFLD
Not well understoodCase reports of rapid progression to cirrhosis1
106 NAFLD pts (mean 13.4 yrs)2
All baseline liver biopsy18 repeat liver biopsies, mean 28 months
8 pts no change fibrosis7 pts worsening fibrosis3 pts improved fibrosis BUT all lost weight
1Molleston JP et al. Am J Gastro 2002;97:2460-2.2A-Kader HH et al. Clin Gastroenterol Hepatol 2008;6:799-802.
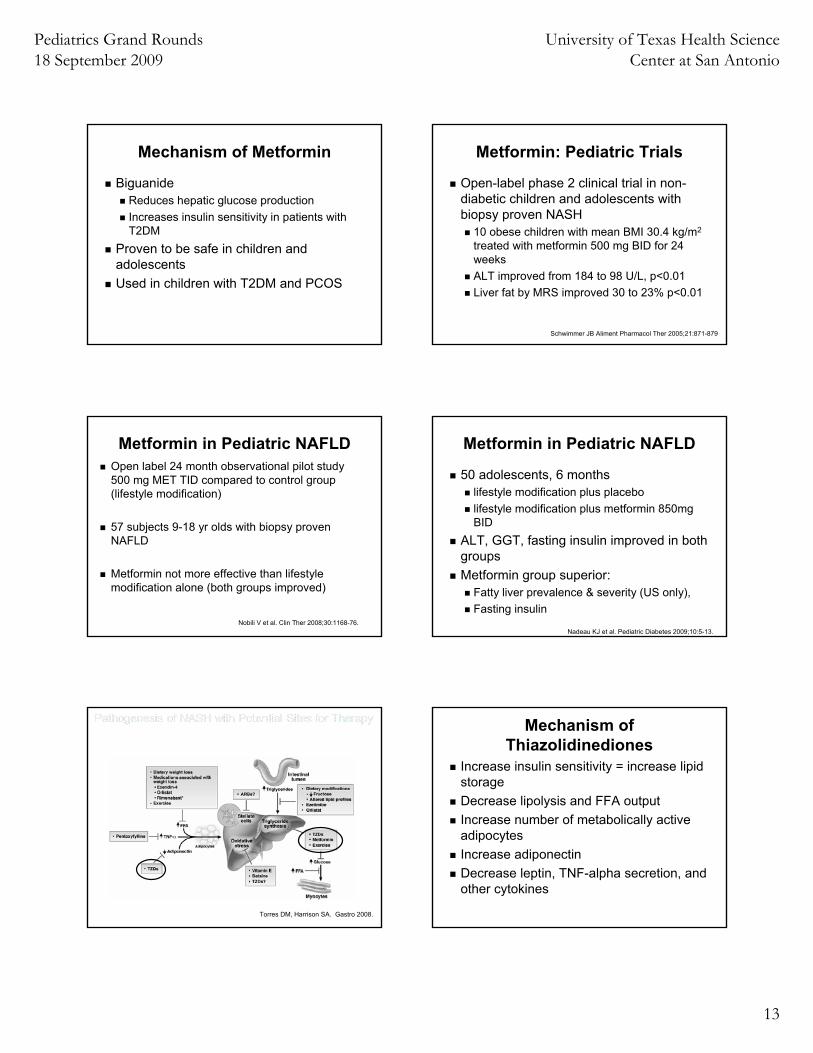
Role of adipose tissue, insulin resistance, fatty acids and
lipotoxicity
Defects at multiple levels may tip the metabolic balance towards hepatic fat accumulation
Excessive substrate supply to the liverIntrahepatic mismatch between lipid synthesis and oxidationInadequate export to peripheral tissues
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
3
Copyright ©2008 The Endocrine Society
Marchesini, G. et al. J Clin Endocrinol Metab 2008;93:s74-s80
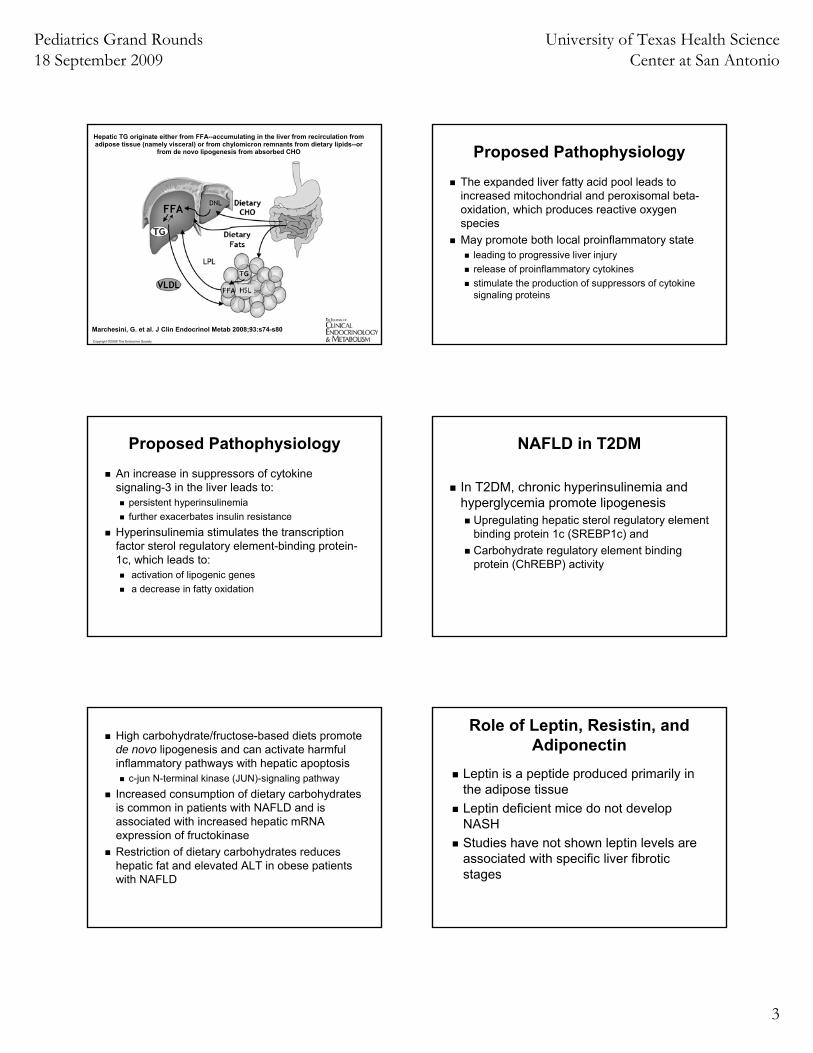
Hepatic TG originate either from FFA--accumulating in the liver from recirculation from adipose tissue (namely visceral) or from chylomicron remnants from dietary lipids--or
from de novo lipogenesis from absorbed CHO Proposed Pathophysiology
The expanded liver fatty acid pool leads to increased mitochondrial and peroxisomal beta-oxidation, which produces reactive oxygen speciesMay promote both local proinflammatory state
leading to progressive liver injury release of proinflammatory cytokinesstimulate the production of suppressors of cytokine signaling proteins
Proposed Pathophysiology
An increase in suppressors of cytokine signaling-3 in the liver leads to:
persistent hyperinsulinemiafurther exacerbates insulin resistance
Hyperinsulinemia stimulates the transcription factor sterol regulatory element-binding protein-1c, which leads to:
activation of lipogenic genes a decrease in fatty oxidation
NAFLD in T2DM
In T2DM, chronic hyperinsulinemia and hyperglycemia promote lipogenesis
Upregulating hepatic sterol regulatory element binding protein 1c (SREBP1c) andCarbohydrate regulatory element binding protein (ChREBP) activity
High carbohydrate/fructose-based diets promote de novo lipogenesis and can activate harmful inflammatory pathways with hepatic apoptosis
c-jun N-terminal kinase (JUN)-signaling pathwayIncreased consumption of dietary carbohydrates is common in patients with NAFLD and is associated with increased hepatic mRNA expression of fructokinaseRestriction of dietary carbohydrates reduces hepatic fat and elevated ALT in obese patients with NAFLD
Role of Leptin, Resistin, and Adiponectin
Leptin is a peptide produced primarily in the adipose tissueLeptin deficient mice do not develop NASHStudies have not shown leptin levels are associated with specific liver fibrotic stages
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
4
Resistin
An adipose-derived proteinOverexpression of resistin in mouse models led to glucose intolerance, hyperinsulinemia, and impaired suppression of free fatty acids levels High resistin levels have been associated with hepatic steatosis
Adiponectin
Hormone secreted exclusively by adipose tissueProduces beneficial effects on lipid metabolism, enhancing lipid clearance from plasma and beta-oxidation of fatty acids in muscleDirect anti-inflammatory effects, suppressing TNF-alpha production in the liverAppears to be protective against NASH
Proposed Progression from Adipose tissue to NASH
Step 1: Adipose tissue insulin resistance, provides lipotoxic environment that supplies liver with FFA and compensatory hyperinsulinemia that stimulates lipogenesisStep 2: Development of hepatic steatosisand of a lipid pool from where lipid-derived toxic metabolites may activate inflammatory pathways
Step 3: Progression from simple steatosisto active necroinflammation depends on the ability of the liver to adapt to longstanding triglyceride accumulation
Failure leads to FFA-induced lipotoxicity with mitochondrial dysfunction, endoplasmic reticulum stress, reactive oxygen species (ROS) formation, and chronic necroinflammation
Step 4: Fibrosis, chronic activation of hepatic stellate cells in a poorly understood cross-talk of Kupffer cells with hepatocytes
Who gets NAFLD?
ObeseMetabolic syndromeT2DMAcanthosis nigricansMales > femalesHispanics > Caucasians > AA
San Diego Study
The largest study that has been undertaken on adolescents and NASH in a retrospective autopsy-based evaluation
Performed on 742 children between 2 to 19 years of age Died traumatically (motor vehicle accidents, accidents, homicide or suicide) Individuals were excluded if they had any factors that would potentially influence liver histology (ie. recent inpatient hospital stay or a positive alcohol or drug toxicology screen)
Schwimmer JB, et al. Pediatrics 2006
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
5
San Diego StudyIn this unique group of previously healthy children, 9.6% had evidence of fatty infiltration of the liver as assessed by liver histology Fatty liver disease was more prevalent among those who were older, overweight, and known associations with insulin resistanceFatty liver was also more common in males (10.5 % versus 7.4% in females) and Hispanics (11.8% versus 1.5% in Blacks and 8.6% in non-Hispanic whites)
Schwimmer JB, et al. Pediatrics 2006
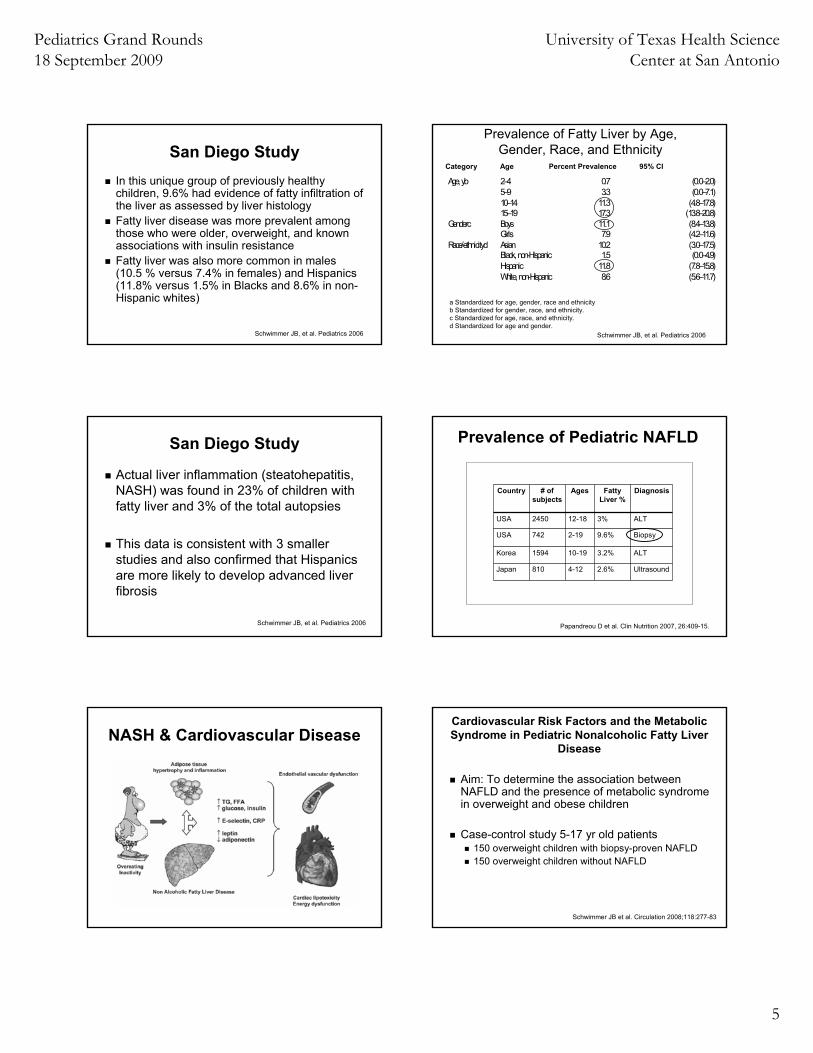
Age, yb 2–4 0.7 (0.0–2.0)5–9 3.3 (0.0–7.1)10–14 11.3 (4.8–17.8)15–19 17.3 (13.8–20.8)
Genderc Boys 11.1 (8.4–13.8)Girls 7.9 (4.2–11.6)
Race/ethnicityd Asian 10.2 (3.0–17.5)Black, non-Hispanic 1.5 (0.0–4.9)Hispanic 11.8 (7.8–15.8)White, non-Hispanic 8.6 (5.6–11.7)
a Standardized for age, gender, race and ethnicity b Standardized for gender, race, and ethnicity. c Standardized for age, race, and ethnicity. d Standardized for age and gender.
Prevalence of Fatty Liver by Age, Gender, Race, and Ethnicity
Schwimmer JB, et al. Pediatrics 2006
Category Age Percent Prevalence 95% CI
San Diego Study
Actual liver inflammation (steatohepatitis, NASH) was found in 23% of children with fatty liver and 3% of the total autopsies
This data is consistent with 3 smaller studies and also confirmed that Hispanics are more likely to develop advanced liver fibrosis
Schwimmer JB, et al. Pediatrics 2006
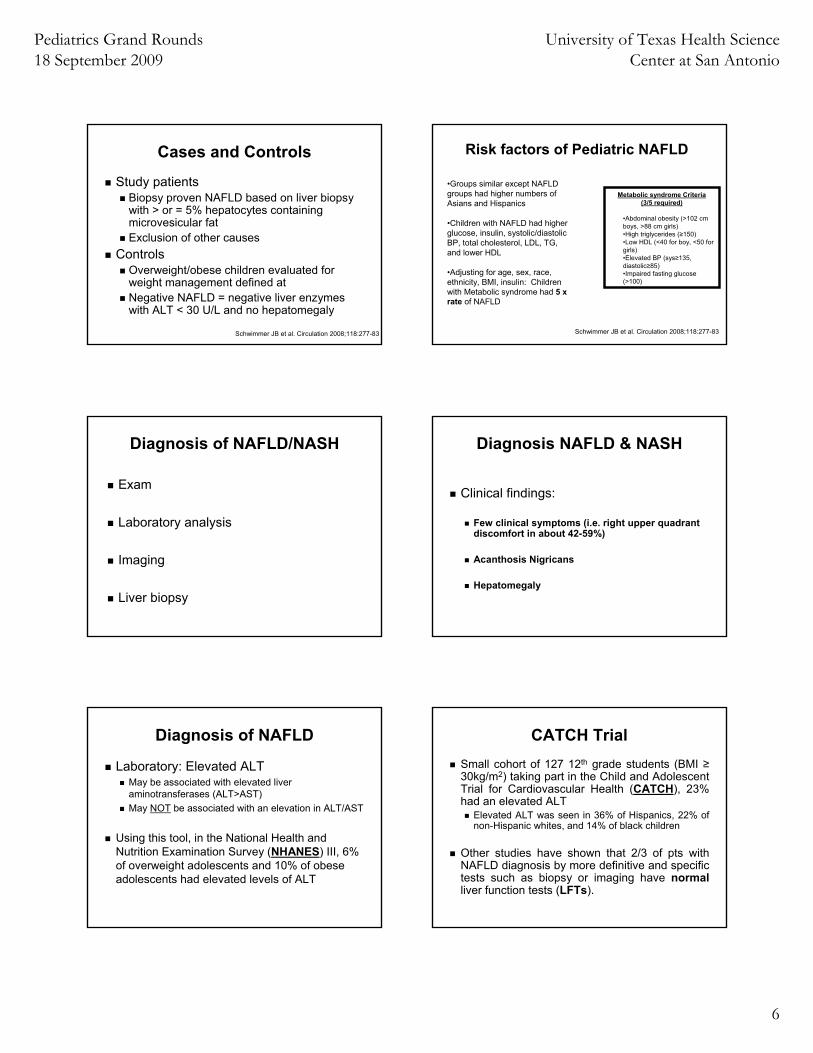
Prevalence of Pediatric NAFLD
Papandreou D et al. Clin Nutrition 2007, 26:409-15.
Country # of subjects
Ages Fatty Liver %
Diagnosis
USA 2450 12-18 3% ALT
USA 742 2-19 9.6% Biopsy
Korea 1594 10-19 3.2% ALT
Japan 810 4-12 2.6% Ultrasound
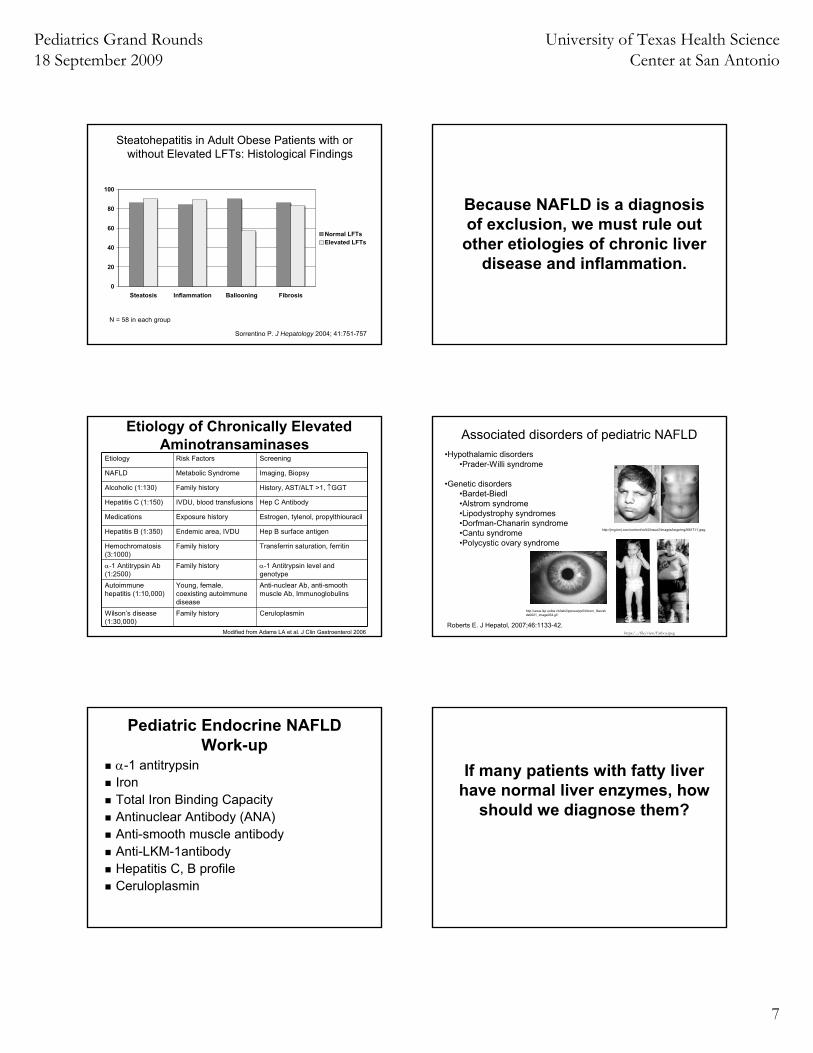
NASH & Cardiovascular DiseaseCardiovascular Risk Factors and the Metabolic Syndrome in Pediatric Nonalcoholic Fatty Liver
Disease
Aim: To determine the association between NAFLD and the presence of metabolic syndrome in overweight and obese children
Case-control study 5-17 yr old patients150 overweight children with biopsy-proven NAFLD 150 overweight children without NAFLD
Schwimmer JB et al. Circulation 2008;118:277-83
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
6
Cases and Controls
Study patientsBiopsy proven NAFLD based on liver biopsy with > or = 5% hepatocytes containing microvesicular fatExclusion of other causes
Controls Overweight/obese children evaluated for weight management defined at Negative NAFLD = negative liver enzymes with ALT < 30 U/L and no hepatomegaly
Schwimmer JB et al. Circulation 2008;118:277-83
Risk factors of Pediatric NAFLD
•Groups similar except NAFLD groups had higher numbers of Asians and Hispanics
•Children with NAFLD had higher glucose, insulin, systolic/diastolic BP, total cholesterol, LDL, TG, and lower HDL
•Adjusting for age, sex, race, ethnicity, BMI, insulin: Children with Metabolic syndrome had 5 x rate of NAFLD
Schwimmer JB et al. Circulation 2008;118:277-83
Metabolic syndrome Criteria (3/5 required)
•Abdominal obesity (>102 cm boys, >88 cm girls)•High triglycerides (≥150)•Low HDL (<40 for boy, <50 for girls)•Elevated BP (sys≥135, diastolic≥85)•Impaired fasting glucose (>100)
Diagnosis of NAFLD/NASH
Exam
Laboratory analysis
Imaging
Liver biopsy
Diagnosis NAFLD & NASH
Clinical findings:
Few clinical symptoms (i.e. right upper quadrant discomfort in about 42-59%)
Acanthosis Nigricans
Hepatomegaly
Diagnosis of NAFLD
Laboratory: Elevated ALTMay be associated with elevated liver aminotransferases (ALT>AST)May NOT be associated with an elevation in ALT/AST
Using this tool, in the National Health and Nutrition Examination Survey (NHANES) III, 6% of overweight adolescents and 10% of obese adolescents had elevated levels of ALT
CATCH TrialSmall cohort of 127 12th grade students (BMI ≥30kg/m2) taking part in the Child and Adolescent Trial for Cardiovascular Health (CATCH), 23% had an elevated ALT
Elevated ALT was seen in 36% of Hispanics, 22% of non-Hispanic whites, and 14% of black children
Other studies have shown that 2/3 of pts with NAFLD diagnosis by more definitive and specific tests such as biopsy or imaging have normalliver function tests (LFTs).
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
7
Steatohepatitis in Adult Obese Patients with or without Elevated LFTs: Histological Findings
0
20
40
60
80
100
Steatosis Inflammation Ballooning Fibrosis
Normal LFTsElevated LFTs
N = 58 in each group
Sorrentino P. J Hepatology 2004; 41:751-757
Because NAFLD is a diagnosis of exclusion, we must rule out
other etiologies of chronic liver disease and inflammation.
Etiology of Chronically Elevated Aminotransaminases
Etiology Risk Factors Screening
NAFLD Metabolic Syndrome Imaging, Biopsy
Alcoholic (1:130) Family history History, AST/ALT >1, ↑GGT
Hepatitis C (1:150) IVDU, blood transfusions Hep C Antibody
Medications Exposure history Estrogen, tylenol, propylthiouracil
Hepatitis B (1:350) Endemic area, IVDU Hep B surface antigen
Hemochromatosis(3:1000)
Family history Transferrin saturation, ferritin
α-1 Antitrypsin Ab(1:2500)
Family history α-1 Antitrypsin level and genotype
Autoimmune hepatitis (1:10,000)
Young, female, coexisting autoimmune disease
Anti-nuclear Ab, anti-smooth muscle Ab, Immunoglobulins
Wilson’s disease (1:30,000)
Family history Ceruloplasmin
Modified from Adams LA et al. J Clin Gastroenterol 2006
Associated disorders of pediatric NAFLD•Hypothalamic disorders
•Prader-Willi syndrome
•Genetic disorders•Bardet-Biedl•Alstrom syndrome•Lipodystrophy syndromes•Dorfman-Chanarin syndrome•Cantu syndrome•Polycystic ovary syndrome
Roberts E. J Hepatol, 2007;46:1133-42.
http://jmg.bmj.com/content/vol42/issue2/images/large/mg26617.f1.jpeg
https:/.../file/view/Fatboy.jpeg
http://www.ikp.unibe.ch/lab2/ppnew/pp5/inborn_files/slide0021_image034.gif
QuickTime™ and a decompressor
are needed to see this picture.
Pediatric Endocrine NAFLD Work-up
α-1 antitrypsinIronTotal Iron Binding CapacityAntinuclear Antibody (ANA)Anti-smooth muscle antibodyAnti-LKM-1antibodyHepatitis C, B profileCeruloplasmin
If many patients with fatty liver have normal liver enzymes, how
should we diagnose them?
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
8
Imaging NAFLD/NASH
Ultrasound
Computed Tomography (CT)
MRI and spectroscopy
Diagnosis by UltrasoundIn adults, ultrasound of the liver is 60-94% sensitive and 73-95% specific for the diagnosis of liver fat when compared to liver histology With >30% fatty infiltration, sensitivity of ultrasound is 80% With 10-19% fatty infiltration, sensitivity of ultrasound is 55%Sensitivity and specificity of ultrasound decrease due to the presence of morbid obesity to 49% and 75%, respectively
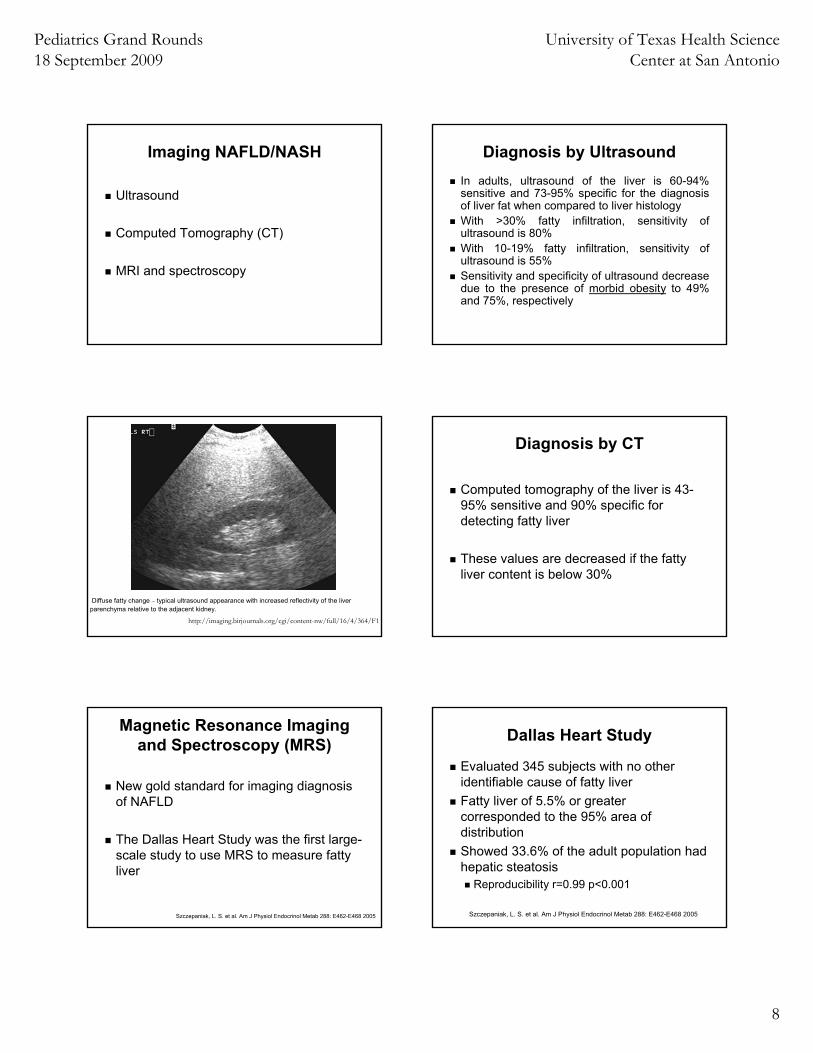
Diffuse fatty change – typical ultrasound appearance with increased reflectivity of the liver parenchyma relative to the adjacent kidney.
http://imaging.birjournals.org/cgi/content-nw/full/16/4/364/F1
Diagnosis by CT
Computed tomography of the liver is 43-95% sensitive and 90% specific for detecting fatty liver
These values are decreased if the fatty liver content is below 30%
Magnetic Resonance Imaging and Spectroscopy (MRS)
New gold standard for imaging diagnosis of NAFLD
The Dallas Heart Study was the first large-scale study to use MRS to measure fatty liver
Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab 288: E462-E468 2005
Dallas Heart Study
Evaluated 345 subjects with no other identifiable cause of fatty liverFatty liver of 5.5% or greater corresponded to the 95% area of distributionShowed 33.6% of the adult population had hepatic steatosis
Reproducibility r=0.99 p<0.001
Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab 288: E462-E468 2005
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
9
Copyright ©2005 American Physiological Society
Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab 288: E462-E468 2005
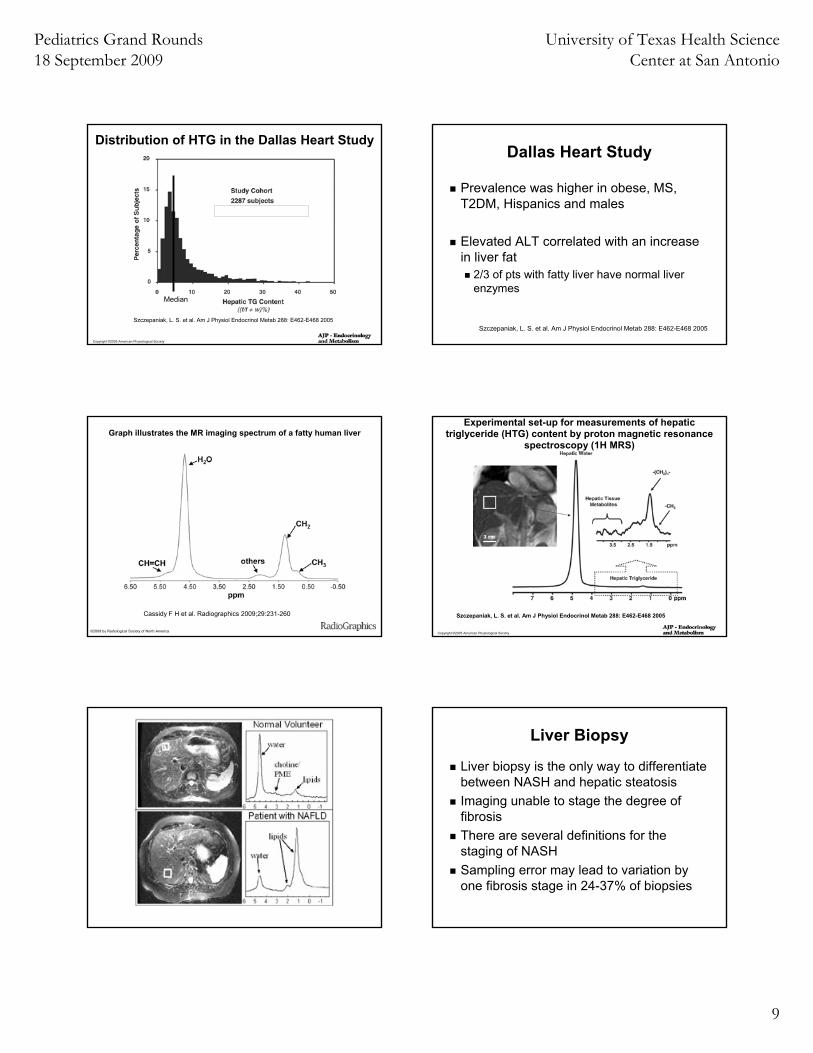
Distribution of HTG in the Dallas Heart Study
|
Median
Dallas Heart Study
Prevalence was higher in obese, MS, T2DM, Hispanics and males
Elevated ALT correlated with an increase in liver fat
2/3 of pts with fatty liver have normal liver enzymes
Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab 288: E462-E468 2005
Graph illustrates the MR imaging spectrum of a fatty human liver
Cassidy F H et al. Radiographics 2009;29:231-260
©2009 by Radiological Society of North America Copyright ©2005 American Physiological Society
Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab 288: E462-E468 2005
Experimental set-up for measurements of hepatic triglyceride (HTG) content by proton magnetic resonance
spectroscopy (1H MRS)
Liver Biopsy
Liver biopsy is the only way to differentiate between NASH and hepatic steatosisImaging unable to stage the degree of fibrosisThere are several definitions for the staging of NASHSampling error may lead to variation by one fibrosis stage in 24-37% of biopsies
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
10
Staging of NASH
Pediatric NASH is often histopathologicallydifferent than adult NASH in the degree of and location of fat, inflammation and fibrosis
Typical adult pattern of NASH includes macrovesicular steatosis, lobular inflammation and ballooning degeneration
Pediatric NASH
Portal inflammation (70%) and portal fibrosis (60%) was present in biopsiesTypical adult pattern termed Type 1Type 2: Steatosis with portal inflammation and/or fibrosis
Without perisinusoidal fibrosis or evidence of ballooning degeneration
Type 1 and Type 2 NASHDistinct clinical and demographic differences between children with type 1 and type 2 histologyThis is suggestive of important pathophysiological differences between adult and pediatric NASHChildren with type 2 are
youngergreater severity of obesitymale > female
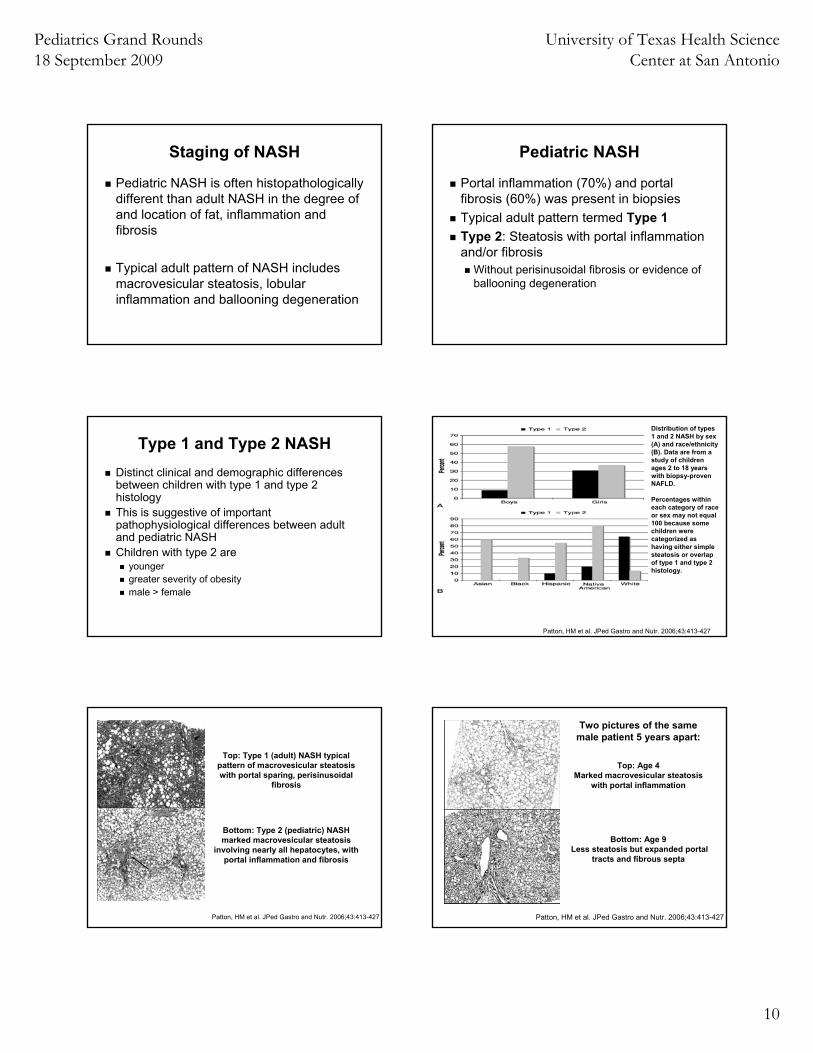
Distribution of types 1 and 2 NASH by sex (A) and race/ethnicity (B). Data are from a study of children ages 2 to 18 years with biopsy-proven NAFLD.
Percentages within each category of race or sex may not equal 100 because some children were categorized as having either simple steatosis or overlap of type 1 and type 2 histology.
Patton, HM et al. JPed Gastro and Nutr. 2006;43:413-427
Top: Type 1 (adult) NASH typical pattern of macrovesicular steatosiswith portal sparing, perisinusoidal
fibrosis
Bottom: Type 2 (pediatric) NASH marked macrovesicular steatosis
involving nearly all hepatocytes, with portal inflammation and fibrosis
Patton, HM et al. JPed Gastro and Nutr. 2006;43:413-427
Two pictures of the same male patient 5 years apart:
Top: Age 4Marked macrovesicular steatosis
with portal inflammation
Bottom: Age 9Less steatosis but expanded portal
tracts and fibrous septa
Patton, HM et al. JPed Gastro and Nutr. 2006;43:413-427

Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
11
Elevated LFTS
Pediatric NAFLD Algorithm
Rule out other causes of fatty
liver
Consider Liver Biopsy
NASH
▪Reduce daily caloric intake ▪Exercise
Consider: ▪Clinical treatment trials vs.
intensive diet and exercise
Consider Imaging
Risk factors for Fatty Liver:•Insulin resistance•Obesity•Diabetes
Recheck liver enzymesAfter 3 months
LFTs increasing
NAFLD
What are the treatments options for pediatric patients with NAFLD?
Pediatric NAFLD Ongoing Research
132 studies for “fatty liver treatment”7 studies ongoing for “pediatric fatty liver”
Drugs under investigationAcarbose (pilot study)XenicalMetformin
Other trialsLow glycemic diet vs low fat diet
Torres DM, Harrison SA. Gastro 2008.
Treatment Options
In a 12-month double-blinded placebo study on 90 children with NAFLD
Subjects were placed on a balanced caloric dietPhysical exercise Either placebo or Vitamin E 600 IU/day and Vitamin C 500 mg/day.
Diet and exercise alone was better than antioxidant therapy
Nobili, V. et al. Aliment Pharmocol Ther.2006;24(11):1553-1561.
Trial of Lifestyle Modification & Antioxidant Therapy for Pediatric NAFLD
•53 patients followed for 24 months •Diet & increased physical activity counseling plus placebo OR Vit E 600 IU/day & Vit C 500 mg/day
Placebo Baseline
Placebo 2 year
p Vit E + C Baseline
Vit E + C 2 year
p P*
BMI 26.8 23.7 <0.001 24.9 21.2 <0.001 0.4
ALT 63 34 <0.001 71 40 <0.001 0.6
AST 49 34 <0.001 44 32 <0.001 0.6
Chol 156 132 <0.001 167 127 <0.001 0.02
Trig 89 62 <0.001 87 67 <0.001 0.8
Gluc 87 75 <0.001 83 72 <0.001 0.6
NAS 4 2 <0.001 4 2 <0.001 0.06
Nobili V et al. Hepatology 2008;48:119-128.
P*=intergroup p, NAS=NAFLD activity score on liver biopsy
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
12
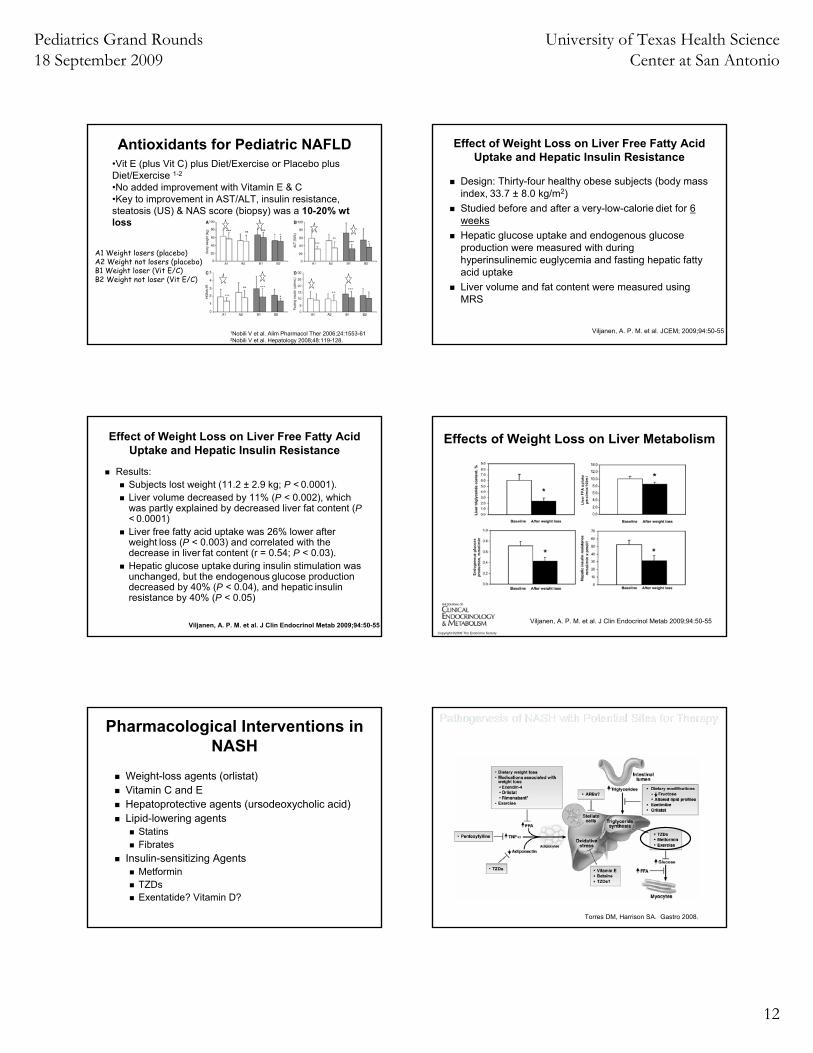
Antioxidants for Pediatric NAFLD•Vit E (plus Vit C) plus Diet/Exercise or Placebo plus Diet/Exercise 1-2
•No added improvement with Vitamin E & C•Key to improvement in AST/ALT, insulin resistance, steatosis (US) & NAS score (biopsy) was a 10-20% wt loss
1Nobili V et al. Alim Pharmacol Ther 2006;24:1553-612Nobili V et al. Hepatology 2008;48:119-128.
A1 Weight losers (placebo)A2 Weight not losers (placebo)B1 Weight loser (Vit E/C)B2 Weight not loser (Vit E/C)
Effect of Weight Loss on Liver Free Fatty Acid Uptake and Hepatic Insulin Resistance
Design: Thirty-four healthy obese subjects (body mass index, 33.7 ± 8.0 kg/m2)Studied before and after a very-low-calorie diet for 6 weeksHepatic glucose uptake and endogenous glucoseproduction were measured with duringhyperinsulinemic euglycemia and fasting hepatic fatty acid uptakeLiver volume and fat content were measured usingMRS
Viljanen, A. P. M. et al. JCEM; 2009;94:50-55
Effect of Weight Loss on Liver Free Fatty Acid Uptake and Hepatic Insulin Resistance
Results: Subjects lost weight (11.2 ± 2.9 kg; P < 0.0001). Liver volume decreased by 11% (P < 0.002), whichwas partly explained by decreased liver fat content (P< 0.0001)Liver free fatty acid uptake was 26% lower after weight loss (P < 0.003) and correlated with the decrease in liver fat content (r = 0.54; P < 0.03). Hepatic glucose uptake during insulin stimulation was unchanged, but the endogenous glucose production decreased by 40% (P < 0.04), and hepatic insulin resistance by 40% (P < 0.05)
Viljanen, A. P. M. et al. J Clin Endocrinol Metab 2009;94:50-55Copyright ©2009 The Endocrine Society
Viljanen, A. P. M. et al. J Clin Endocrinol Metab 2009;94:50-55
Effects of Weight Loss on Liver Metabolism
Pharmacological Interventions in NASH
Weight-loss agents (orlistat)Vitamin C and EHepatoprotective agents (ursodeoxycholic acid)Lipid-lowering agents
StatinsFibrates
Insulin-sensitizing AgentsMetforminTZDsExentatide? Vitamin D?
Torres DM, Harrison SA. Gastro 2008.
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
13
Mechanism of Metformin
BiguanideReduces hepatic glucose productionIncreases insulin sensitivity in patients with T2DM
Proven to be safe in children and adolescentsUsed in children with T2DM and PCOS
Metformin: Pediatric Trials
Open-label phase 2 clinical trial in non-diabetic children and adolescents with biopsy proven NASH
10 obese children with mean BMI 30.4 kg/m2
treated with metformin 500 mg BID for 24 weeksALT improved from 184 to 98 U/L, p<0.01Liver fat by MRS improved 30 to 23% p<0.01
Schwimmer JB Aliment Pharmacol Ther 2005;21:871-879
Metformin in Pediatric NAFLDOpen label 24 month observational pilot study 500 mg MET TID compared to control group (lifestyle modification)
57 subjects 9-18 yr olds with biopsy proven NAFLD
Metformin not more effective than lifestyle modification alone (both groups improved)
Nobili V et al. Clin Ther 2008;30:1168-76.
Metformin in Pediatric NAFLD
50 adolescents, 6 monthslifestyle modification plus placebo lifestyle modification plus metformin 850mg BID
ALT, GGT, fasting insulin improved in both groupsMetformin group superior:
Fatty liver prevalence & severity (US only),Fasting insulin
Nadeau KJ et al. Pediatric Diabetes 2009;10:5-13.
Torres DM, Harrison SA. Gastro 2008.
Mechanism of Thiazolidinediones
Increase insulin sensitivity = increase lipid storageDecrease lipolysis and FFA outputIncrease number of metabolically active adipocytesIncrease adiponectinDecrease leptin, TNF-alpha secretion, and other cytokines
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
14
UTHSCSA study on TZD55 adult pts randomly assigned to hypocaloricdiet with/without pioglitazonePerformed biopsy, MRS, OGTT
Improved glycemic controlImproved ALTDecreased hepatic contentNo change in fibrosis
Safety of TZDs in children not establishedOngoing trial of rosiglizatone in the T2DM TODAY trial
Belfort, R. et al. NEJM. 2006;355:2297-307.
Must Weigh Risks and Benefits
Benefits Risks- Adiponectin
- Hepatic insulin sensitivity
- Steatosis
- Necro-inflammation
- Cardiovascular risk
- Triglycerides w/avandia
- Bone Loss/Fracture
- Weight gain, peripheral fat
- Worsening of CHF
Incretins and Fatty Liver
Incretins are gastrointestinal hormones that enhance the postprandial insulin response. A synthetic form of exendin-4, exenatide, has been developed and undergone extensive clinical trialsExenatide is currently FDA approved for adults and children older than age 16 for treatment of T2DM in combination with sulfonylureas, metformin and/or thioglitazones
Incretins and Fatty LiverExenatide mechanism of action includes:
stimulates glucose-dependent pancreatic insulin secretion restores the first-phase insulin response (often lost in T2DM) suppresses glucagon secretion during periods of hyperglycemia decreases gastric emptying increases satiety
These effects lead to overall decreased insulin resistance and often weight loss
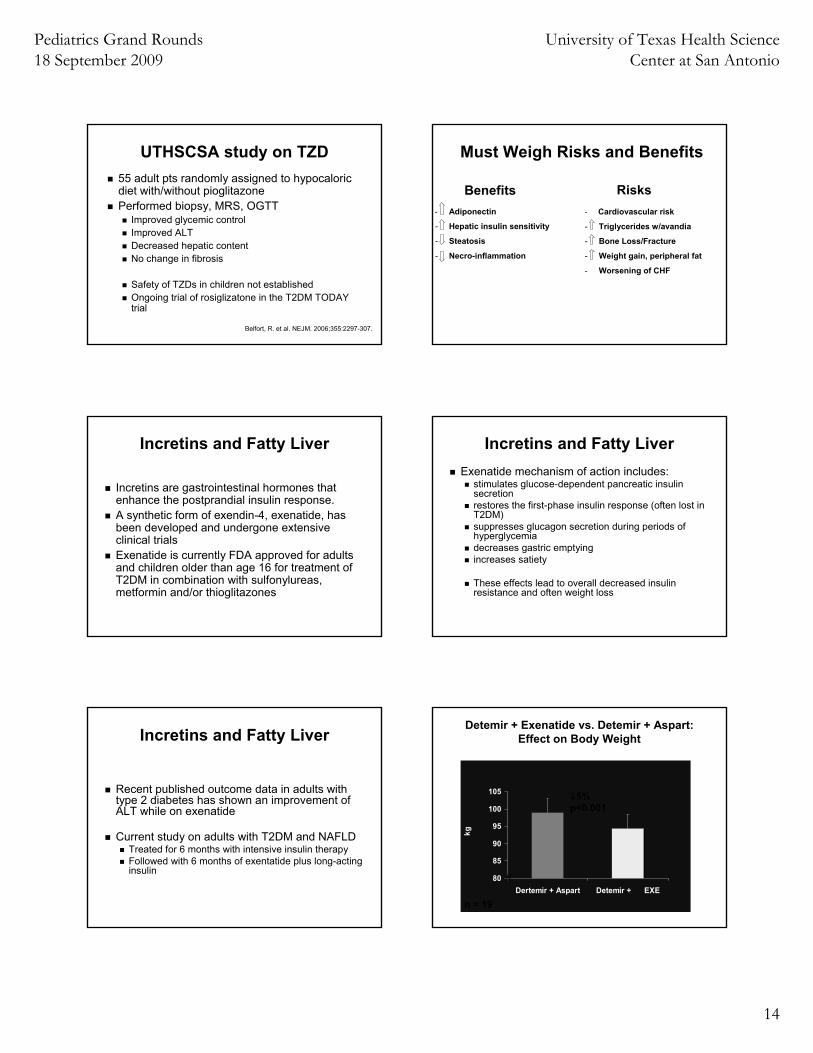
Incretins and Fatty Liver
Recent published outcome data in adults with type 2 diabetes has shown an improvement of ALT while on exenatide
Current study on adults with T2DM and NAFLDTreated for 6 months with intensive insulin therapyFollowed with 6 months of exentatide plus long-acting insulin
Detemir + Exenatide vs. Detemir + Aspart:Effect on Body Weight
80
85
90
95
100
105
Dertemir + Aspart Detemir + EXE
kg
n = 19
//
↓5%p<0.001
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
15
Detemir + Exenatide vs. Detemir + Aspart: Mixed Meal Results
40
90
140
190
240
290
6am
7am
8am
9am
10am
11am
12pm
Time
mg/
dL
Glucose Detemir + Aspart
Glucose Detemir + EXE
INS Detemir + Aspart
INS Detemir + EXE
⁄⁄
n = 19A1c: Pre-tx: 7.0±0.2 vs. Post-tx: 6.8±0.2
p<0.001
Glucose
Insulin
Mean 1st & 2nd Phase Insulin Secretion:Hyperglcemic Clamp
20
40
60
80
100
Mean 1st Phase Mean 2nd Phase
uU/m
L Detemir + AspartDetemir + EXE
⁄⁄
n = 19
↑ 53%p<0.05
↑ 47%p<0.05
Detemir + Exenatide vs. Detemir + Aspart: Effect on Liver Fat
5
6
7
8
9
10
11
Detemir + Aspart Detemir + EXE
% L
FAT
n = 19
↓27%p=0.04
⁄⁄
Vitamin D and Fatty Liver
Vitamin D is found in dietary sources such as fish, eggs, and fortified milk and is increased by sunlight exposure. Frequently found to be deficient in teens who have had suboptimal diets despite sun exposure. Its actions are well-recognized in their role in mineral homeostasis by regulation of calcium absorption from the gut and reabsorption in the kidney. More recently, Vitamin D is associated with autoimmune diseases, cancer, and Type 1 and Type 2 Diabetes.
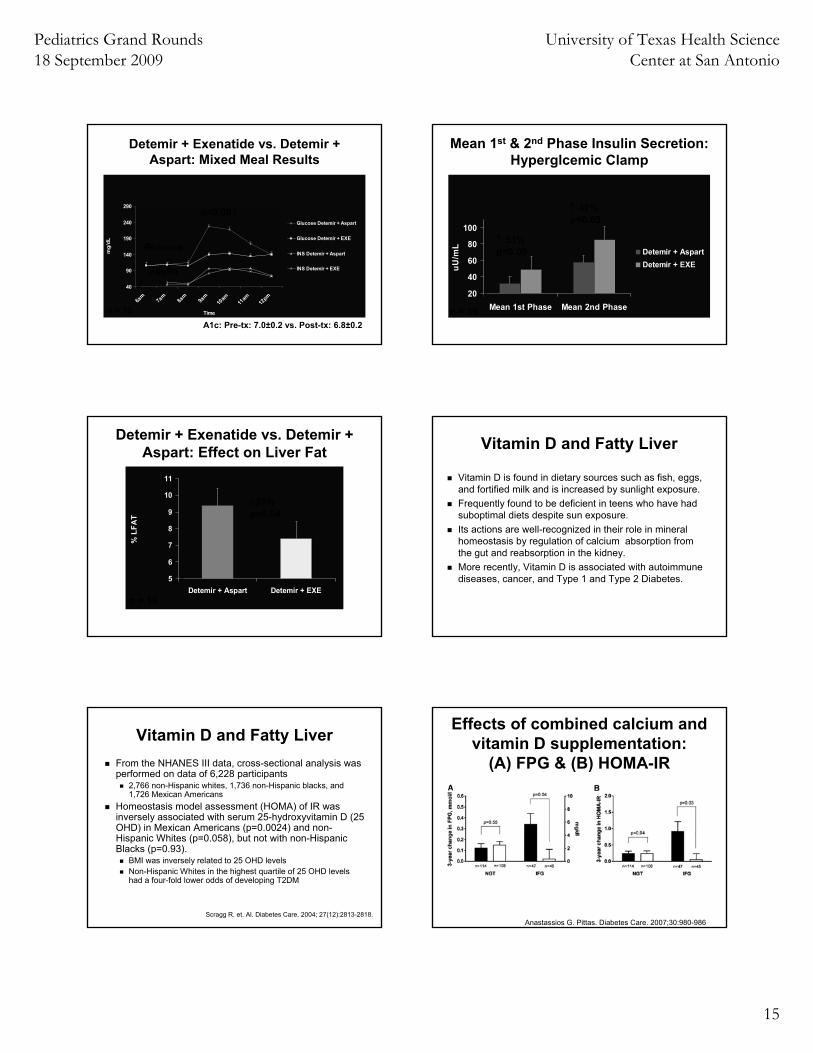
Vitamin D and Fatty LiverFrom the NHANES III data, cross-sectional analysis was performed on data of 6,228 participants
2,766 non-Hispanic whites, 1,736 non-Hispanic blacks, and 1,726 Mexican Americans
Homeostasis model assessment (HOMA) of IR was inversely associated with serum 25-hydroxyvitamin D (25 OHD) in Mexican Americans (p=0.0024) and non-Hispanic Whites (p=0.058), but not with non-Hispanic Blacks (p=0.93).
BMI was inversely related to 25 OHD levelsNon-Hispanic Whites in the highest quartile of 25 OHD levels had a four-fold lower odds of developing T2DM
Scragg R. et. Al. Diabetes Care. 2004; 27(12):2813-2818.Anastassios G. Pittas. Diabetes Care. 2007;30:980-986
Effects of combined calcium and vitamin D supplementation:
(A) FPG & (B) HOMA-IR
Pediatrics Grand Rounds 18 September 2009
University of Texas Health Science Center at San Antonio
16
Vitamin D and Fatty Liver
Cross-sectional analysis of 3577 adolescents from 2001-2004 NHANESMean 25 (OH)D level 24.8 ng/mL
W >MA>AAAssociated with weight and abdominal obesityAdjusting for age, gender, race, and BMI
25 (OH)D inversely associated with plasma glucose concentration
Reis, JP et. Al. Pediatrics. 124: e371-379, 2009
Vitamin D and Fatty LiverIn the cross-sectional analysis of 60 biopsy-proven NAFLD and 60 healthy control patients with comparable age, sex and BMI
NAFLD patients had lower serum 25 (OH)D (51.0 ± 22 vs. 74.5 ±15 nmol/L, p=0.001) when compared to healthy controls An inverse relationship exists between decreasing 25 (OH)D with increasing degree of liver histology (p <0.001) This linear association may suggest a dose-effect relationship
Ongoing trial here at our CHART center to observe if Vitamin D supplementation to physiologic levels has any effect on NAFLD in obese children between the ages of 10 and 17 who present with vitamin D deficiency
Targher G et al. Nut, Met & CV Diseases 17:517-524,2007
Summary
NAFLD is a comorbidity of obesity and diabetesWe do not know the progression of the disease but we do know in adults it can lead to cirrhosis and liver failureWe need to find ways to prevent or stall fatty liver
ReferencesAdams LA, et al. Diagnostic Evaluation of Nonalcoholic Fatty Liver Disease. J ClinGastroenterol. 2006;40:S34-S38.Anastassios G. Pittas. The Effects of Calcium and Vitamin D Supplementation on Blood Glucose and Markers of Inflammation in Nondiabetic Adults. Diabetes Care. 2007; 30:980-986.Belfort, R. et al. A Placebo-Controlled Trial of Pioglitazone in Subjects with Nonalcoholic Steatohepatitis. NEJM. 2006;355:2297-307.Chavez-Tapia NC, et al. Non-alcoholic fatty liver disease in pediatric populations. JPEM. 2007;20:1059-1073.Cusi, Kenneth. Nonalcoholic fatty liver disease in type 2 diabetes mellitus. Current Opinion in Endocrinology, Diabetes & Obesity. 2009, 16:141-149.Larry, L, Pioglitazone trial for NASH: results show promise. Gastroenterology, 2007; 132(3): 836-8.Marchesini, G et al. Obesity-Associated Liver Disease. JCEM. 2008; 93:S74-S80. Nobili, V. et al. Effect of Vitamin E on Aminotransferase Levels and Insulin Resistance in Children With Nonalcoholic Fatty Liver Disease. Aliment PharmocolTher. 2006;24(11):1553-1561.
ReferencesPatton, HM et al. Pediatric Nonalcoholic Fatty Liver Disease: A Critical Appraisal of Current Data and Implications for Future Research. Journal of Pediatric Gastroenterology and Nutrition. 2006;43:413-427.Reis, JP et al. Vitamin D Status and Cardiometabolic Risk Factors in the United States Adolescent Population. 2009;124:e371-379.Schwimmer, JB et al. A phase 2 clinical trial of metformin as a treatment for non-diabetic paediatric non-alcoholic steatohepatitis. Aliment Pharmacol Ther. 2005;21:871-879.Scragg R, Sowers M, Bell C. Serum 25-Hydroxyvitamin D, Diabetes, and Ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care. 2004; 27(12):2813-2818.Szczepaniak, L. S. et al. Am J Physiol Endocrinol Metab. 2005; 288: E462-E468.Targher G et al. Associations between serum 25-hydroxyvitamin D3 concentrations and liver histology in patients with non-alcoholic fatty liver disease. Nutrition, Metabolism & Cardiovascular Diseases 17:517-524,2007.