TheEffectofMediumChainTriglyceridesonTimetoNutritional...
10
Clinical Study TheEffectofMediumChainTriglyceridesonTimetoNutritional Ketosis and Symptoms of Keto-Induction in Healthy Adults: A Randomised Controlled Clinical Trial CliffJ.dC.Harvey , 1 GrantM.Schofield, 1 MicallaWilliden, 1 andJosephA.McQuillan 2,3 1 Human Potential Centre, AUT University, Auckland, New Zealand 2 Health, Sport and Human Performance, University of Waikato, Hamilton, New Zealand 3 Sports Performance Research Institute New Zealand, AUT University, Auckland, New Zealand Correspondence should be addressed to Cliff J. d C. Harvey; cliff@hpn.ac.nz Received 14 February 2018; Accepted 26 April 2018; Published 22 May 2018 Academic Editor: C. S. Johnston Copyright © 2018 Cliff J. d C. Harvey et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Medium chain triglycerides (MCTs) are ketogenic and might reduce adverse effects of keto-induction and improve time to ketosis and the tolerability of very low carbohydrate diets. is study investigates whether MCT supplementation improves time to nutritional ketosis (NK), mood, and symptoms of keto-induction. We compared changes in beta-hydroxybutyrate (BOHB), blood glucose, symptoms of keto-induction, and mood disturbance, in 28 healthy adults prescribed a ketogenic diet, randomised to receive either 30 ml of MCT, or sunflower oil as a control, three times per day, for 20 days. e primary outcome measured was the achievement of NK (≥0.5mmol·L −1 BOHB). Participants also completed a daily Profile of Mood States and keto-induction symptom questionnaire. MCT resulted in higher BOHB at all time points and faster time to NK, a result that failed to reach significance. Symptoms of keto-induction resulted from both diets, with a greater magnitude in the control group, except for abdominal pain, which occurred with greater frequency and severity in the MCT-supplemented diet. ere was a possibly beneficial effect on symptoms by MCT, but the effect on mood was unclear. Based on these results, MCTs increase BOHB compared with LCTand reduce symptoms of keto-induction. It is unclear whether MCTs significantly improve mood or time to NK. e trial was registered by the Australia New Zealand Clinical Trial Registry ACTRN12616001099415. 1. Introduction Very-low-carbohydrate ketogenic diets (VLCKDs) appear to offer specific benefits for health conditions ranging from neurological disorders, cancer, and obesity, diabetes, and other metabolic conditions [1–11]. A restriction of carbo- hydrate, either by fasting or by restricting dietary carbohy- drate, results in reduced insulin levels, thereby reducing lipogenesis, fat accumulation, and glycogen reserves. Long- chain fatty acids derived from common dietary lipids are almost always bound to albumin and are unable to cross the blood-brain barrier for use as fuel. us, when glycogen reserves become insufficient to supply the glucose re- quirement of the central nervous system (CNS), and for fat oxidation, an alternative fuel is required. During carbohydrate restriction, acetoacetate accumulates and is converted into acetone and beta-hydroxybutyrate (BOHB), leading to the presence of these ketones in the blood and urine (ketonaemia and ketonuria, resp.) and in the breath. Ketone bodies are utilised by tissue as a source of energy, with acetoacetate, the primary ketone body, and BOHB, not technically a ketone body (as the ketone moiety has been reduced to a hydroxyl group), functions as the primary fuel during ketosis resulting in two molecules of acetyl-CoA which enter the Krebs cycle. In ketosis, blood glucose (BG) levels stay within normal physiological limits due to the creation of glucose from glucogenic amino acids and via the liberation of glycerol during fatty acid oxidation. Nutritional ketosis (NK) results from VLCKDs, as com- pared to starvation ketosis seen in fasting, and pathological Hindawi Journal of Nutrition and Metabolism Volume 2018, Article ID 2630565, 9 pages https://doi.org/10.1155/2018/2630565
Transcript of TheEffectofMediumChainTriglyceridesonTimetoNutritional...

Clinical StudyThe Effect of Medium Chain Triglycerides on Time to NutritionalKetosis and Symptoms of Keto-Induction in Healthy AdultsA Randomised Controlled Clinical Trial
Cliff J d C Harvey 1 Grant M Schofield1 Micalla Williden1 and Joseph A McQuillan23
1Human Potential Centre AUT University Auckland New Zealand2Health Sport and Human Performance University of Waikato Hamilton New Zealand3Sports Performance Research Institute New Zealand AUT University Auckland New Zealand
Correspondence should be addressed to Cliff J d C Harvey cliffhpnacnz
Received 14 February 2018 Accepted 26 April 2018 Published 22 May 2018
Academic Editor C S Johnston
Copyright copy 2018 Cliff J d C Harvey et al )is is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Medium chain triglycerides (MCTs) are ketogenic and might reduce adverse effects of keto-induction and improve time to ketosisand the tolerability of very low carbohydrate diets )is study investigates whether MCT supplementation improves time tonutritional ketosis (NK) mood and symptoms of keto-inductionWe compared changes in beta-hydroxybutyrate (BOHB) bloodglucose symptoms of keto-induction and mood disturbance in 28 healthy adults prescribed a ketogenic diet randomised toreceive either 30ml of MCT or sunflower oil as a control three times per day for 20 days)e primary outcomemeasured was theachievement of NK (ge05mmolmiddotLminus1 BOHB) Participants also completed a daily Profile of Mood States and keto-inductionsymptom questionnaire MCT resulted in higher BOHB at all time points and faster time to NK a result that failed to reachsignificance Symptoms of keto-induction resulted from both diets with a greater magnitude in the control group except forabdominal pain which occurred with greater frequency and severity in the MCT-supplemented diet )ere was a possiblybeneficial effect on symptoms by MCT but the effect on mood was unclear Based on these results MCTs increase BOHBcompared with LCTand reduce symptoms of keto-induction It is unclear whether MCTs significantly improve mood or time toNK )e trial was registered by the Australia New Zealand Clinical Trial Registry ACTRN12616001099415
1 Introduction
Very-low-carbohydrate ketogenic diets (VLCKDs) appear tooffer specific benefits for health conditions ranging fromneurological disorders cancer and obesity diabetes andother metabolic conditions [1ndash11] A restriction of carbo-hydrate either by fasting or by restricting dietary carbohy-drate results in reduced insulin levels thereby reducinglipogenesis fat accumulation and glycogen reserves Long-chain fatty acids derived from common dietary lipids arealmost always bound to albumin and are unable to cross theblood-brain barrier for use as fuel )us when glycogenreserves become insufficient to supply the glucose re-quirement of the central nervous system (CNS) and for fatoxidation an alternative fuel is required During carbohydrate
restriction acetoacetate accumulates and is converted intoacetone and beta-hydroxybutyrate (BOHB) leading to thepresence of these ketones in the blood and urine (ketonaemiaand ketonuria resp) and in the breath Ketone bodies areutilised by tissue as a source of energy with acetoacetate theprimary ketone body and BOHB not technically a ketonebody (as the ketone moiety has been reduced to a hydroxylgroup) functions as the primary fuel during ketosis resultingin two molecules of acetyl-CoA which enter the Krebs cycleIn ketosis blood glucose (BG) levels stay within normalphysiological limits due to the creation of glucose fromglucogenic amino acids and via the liberation of glycerolduring fatty acid oxidation
Nutritional ketosis (NK) results from VLCKDs as com-pared to starvation ketosis seen in fasting and pathological
HindawiJournal of Nutrition and MetabolismVolume 2018 Article ID 2630565 9 pageshttpsdoiorg10115520182630565
ketosis such as the diabetic ketoacidosis results from un-controlled Type 1 diabetes [12] Both starvation or fastingketosis and nutritional ketosis result from evolutionary ad-aptations that allowed humans to survive in the absence ofcarbohydrate foods and thus glucose provision [13] Nutri-tional ketosis allows for the maintenance of ketosis withoutstarvation and so NK allows for the maintenance of ketosisfor longer than would be achievable with fasted ketosisVLCKDs typically result in BOHB levels of ge05mmolmiddotLminus1[14] and this level has been used as a cutoff point for entryinto NK [15] Adaptation to NK when transitioning froma standard higher carbohydrate diet to a VLCKD can causevarious short-term adverse effects [16] )ese effects ofldquoketo-inductionrdquo are constipation headache halitosismuscle cramps diarrhoea general weakness and rash [17])ese occur due to increased natriuresis kaliuresis anddiuresis in response to lowered insulin levels [18ndash21] greatestbetween days 1 and 4 of a fast or ketogenic diet [18] Transientreductions in glucose provision to the brain have been ob-served between days 1 and 3 with BG normalising after dayfour [22] while constipation and other gastrointestinal effectsresult from reduced food volume increased fat intake orreduced fibre intake [23 24] Difficulties with adherence toketogenic diets have been noted [3 17] but few studiesspecifically describe early adverse symptoms associated withketo-induction
Ketogenic diets typically contain a 3 1 to 4 1 ratio oflipids to nonlipid macronutrients or at least 75 of caloriescoming from lipids very low carbohydrates (often less than50 g) and low-to-moderate amounts of protein )e 4 1 lipidto nonlipid ratio ketogenic diet pioneered at Johns HopkinsUniversity Hospital [25 26] is now commonly used to induceketosis and is referred to as a ldquoclassicrdquo or ldquostandardrdquo ketogenicdiet Huttenlocher and colleagues first demonstrated thatdiets containing 60ndash75 of calories from lipids induce NK ifthey include a high proportion of medium chain triglycerides(MCTs) [27] A VLCKD with 60 of calories derived fromMCTs a three-fold greater intake of carbohydrate (18versus 6) and a sim50 (7 versus 10) increase in proteininduced NK with little clinical difference in BOHB levelswhen compared to a standard ketogenic diet [28] Unlikelong-chain triglycerides (LCTs) MCTs do not require theactions of bile normicellar-chylomicron-mediated absorptioninto the lymphatics and instead are diffused into the hepaticportal vein and preferentially converted into bio-availableketone bodies in the liver Moreover dietary MCTs promoteketonaemia and ketogenesis in both animals [29 30] andhumans [31]
Based on existing evidence MCT supplementation is de-monstrably ketogenic [29ndash31] increases BOHB in a linearand dose-dependent manner [32ndash36] and allows the achieve-ment of ketosis with lower amounts of lipids (and concomi-tantly higher levels of protein and carbohydrate) [28 37 38]However there is a paucity of research considering the rolethat MCTs may play in inducing ketosis more rapidly ina ketogenic diet with a 4 1 lipid to nonlipid ratio or inimproving symptoms of keto-induction and mood NK isdefined by the magnitude of ketonaemia (specificallyge05mmolmiddotLminus1 of BOHB) and symptoms of keto-induction
occur during the transition from a standard diet (withlimited ketone expression in the blood) and the achievementof NK )erefore it is likely that the use of MCTs resultingin ketonaemia and ketogenesis could reduce time to NKand symptoms of keto-induction )ese symptoms are likelyto relate at least in part to the transition from a glucosedominant fuel system to one in which BOHB becomesa primary fuel source Further by reducing the time to NKcompliance to a VLCKD could be improved Likewisemitigation of symptoms of keto-induction is likely to resultin improved adherence to the diet
)e aim of the present study therefore was to inves-tigate in a randomised double-blind placebo-controlledtrial whether MCTs reduce time to nutritional ketosis andsymptoms of keto-induction andmood in a classic ketogenicdiet )e primary outcome measured was the time takento achieve NK Secondary outcomes were symptoms andmood
2 Materials and Methods
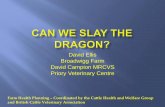
Twenty-eight participants (2 males 26 females ageplusmn SD35plusmn 4 y) (Table 1) were recruited between the 18th and 19thof October 2015 and gave written informed consent toparticipate in this randomised double-blinded placebo-controlled study Participants were required to be non-obese (lt30 BMI) not diagnosed as diabetic not currentlynor previously following a ketogenic diet and not a client ofany of the researchers in clinical practice )e study tookplace between the 2nd and 21st of November 2015 Col-lection of data and analysis was performed at AUT HumanPotential Centre Auckland New Zealand (Figure 1)
Participants were prescribed a ketogenic diet with a 4 1lipid to nonlipid ratio Males were allocated a diet containing2200 kcalmiddotdayminus1 and females 1800 kcalmiddotdayminus1 each equating to80 calories from fat (including supplemental oils) 13 to17 from protein and 3 to 6 from carbohydrate Minordifferences in carbohydrate and protein were due to the useof a protein intake of 14 gmiddotkgminus1 bmmiddotdayminus1 (population meansfor male and female resp) consistent with InternationalSociety of Sports Nutrition (ISSN) guidelines for optimalprotein intake for performance [39] Participants wererandomised to receive either an MCT supplement con-taining 65 caprylic acid (C 8) and 35 capric acid (C 10)triglycerides (Amtrade NZ limited) or a long chain tri-glyceride (sunflower) oil (Home Brand) 30ml three times
Table 1 Demographic characteristics of participants
MCT LCTGender (MF) 111 110Age (years) mean (range) 40 (33 to 47) 40 (32 to 48)
Ethnicity (n)
European (5)
European (11)NZ Maori (2)
Pacific Island (3)Chinese (1)
Other Asian (1)MCT medium chain triglyceride LCT long-chain triglyceride M maleF female
2 Journal of Nutrition and Metabolism
per day for 20 days While MCTs are essentially nontoxic[40] Ivy et al observed that 100 of participants in theirstudy experienced gastric distress (cramping and diarrhoea)with dosages of 50 and 60 g MCT with only small GI effectsnoted at 30 g [41] We used this dosage (30 g) as it was mostlikely to elicit an effect without unduly exposing participantsto adverse effects arising from MCT ingestion For ouranalysis we considered the day in which each participantachieved ge05mmolmiddotLminus1 BOHB as the time at which theyhad achieved NK We proposed this threshold for NK(ge05mmolmiddotLminus1) based on the level of BOHB observed inthose following a VLCKD[14] and as used as a cutoff pointfor ketosis by Guerci and colleagues [15]
Participants were provided with a ldquoFreeStyle Neordquoblood-prick ketometerglucometer (Abbott Industries) andwere required to use the device to measure and record fastedBOHB and BG daily upon waking Participants were alsoinstructed to complete a questionnaire including a keto-induction symptoms questionnaire (Symptom-Q) andProfile of Mood States-Short Form (POMS-SF) )e Profileof Mood States is a questionnaire commonly used to de-termine the overall mood state of study participants [42]Saya Shacham developed a shortened 37 question version ofthis form with correlation coefficients between the short andoriginal scales all above 95 indicating the suitability of thisshortened form for estimating mood )e symptoms ques-tionnaire was developed by one of the authors (d C Harvey)based on symptoms commonly observed in previous studiesof ketogenic diets )e questionnaire asked ldquoIn the past 24hours to what extent have you experienced the following
symptomsrdquo answered on a Likert scale of (1) not at all(2) mild (3) moderate (4) severe and (5) intolerable forthe following symptomseffects headache constipationdiarrhoea stomach or intestinal pain intestinal bloatinghalitosis (bad breath) muscle cramps muscle weakness skinrash and difficulty concentrating
An AUT University staff member who was not involvedin data collection randomised participants using a simplerandomisation technique of coin flipping to generatea treatment sequence into two groups ldquoArdquo and ldquoBrdquo andlabelled the supplemental oils ldquoArdquo or ldquoBrdquo for distribution andblinding and retained the blinding key )e primary re-searcher was unblinded to the supplement-oil key only afterdata analysis had been completed
Participants were instructed to contact the primary andtertiary researchers for any assistance during the study du-ration CH is a registered clinical nutritionist with the NewZealand Clinical Nutrition Association and MW is a regis-tered nutritionist with the Nutrition Society of New Zealand)e research was conducted in accordance with AUT ethicalguidelines Ethics approval was provided by the AUT Uni-versity Ethics Committee (approval number 15317)
21 StatisticalAnalyses Magnitude-based inferences (MBIs)were used to compare the observed measures (BOHB BGSymptoms-Q and POMS-SF) Pairwise comparisons weremade between each of the 19 time points for control (LCT)and experimental (MCT) trials for all using a customisedanalysis spreadsheet [43] Pairwise comparisons were also
Allocated to LCT intervention (n = 14)
Did not receive allocated intervention(n = 0)
Received allocated intervention (n = 14)(i)(ii)
Allocated to MCT intervention (n = 14)Received allocated intervention (n = 14)Did not receive allocated intervention(n = 0)
(i)(ii)
Analysed (n = 12)Excluded from analysis (n = 0)(i)
Allocation
Analysis
Follow-up
Analysed (n = 11)Excluded from analysis (n = 0)(i)
Assessed for eligibility (n = 59)Enrollment
Excluded (n = 31)Not meeting inclusion criteria (n = 22)Declined to participate (n = 9)Other reasons (n = 0)
(i)(ii)
(iii)
Randomized (n = 28)
Lost to follow-up (n = 0)Discontinued intervention (n = 2) due to
gastrointestinal distress
Lost to follow-up (n = 0)Discontinued intervention (n = 3) due to light-headedness and inability to concentrate (n = 1)
extreme hunger (n = 1) unreported (n = 1)
Figure 1 CONSORT flow diagram showing recruitment and retention of study participants
Journal of Nutrition and Metabolism 3
made between observed measures relative to respectivebaseline values for each group Data for BOHB and BGcomparisons were log transformed for analysis to reducebias arising from nonuniformity of error and subsequentlyback transformed to obtain changes in means and varia-tions as factors Raw data were used for comparisons be-tween groups for Symptoms-Q and POMS-SF results )esum of symptoms scores (Symptoms-Q) and total mooddisturbance score (TMDS) of the POMS-SF were used foranalysis Total mood disturbance score (TMDS) of thePOMS-SF was calculated by subtracting positive mooditems from negative mood items [44] To make inferencesabout true (population) values of the effect on BOHBSymptoms-Q and POMS of MCT relative to LCT theuncertainty in the effect was expressed as 90 confidencelimits and as likelihoods that the true value of the effectrepresents substantial change (harm or benefit) An effectwas deemed to be unclear if its confidence interval over-lapped the thresholds for substantiveness that is if theeffect could be substantially positive and negative [45] )esmallest worthwhile change for between-group means forall blood and perceptual measures was calculated as 02 ofthe between-subject SD [45] Inferences were based onthreshold chances of harm of a difference between groupsof 05 and benefit of 25 To determine the likelihood ofclinical effects the default values and qualitative terms wereset at lt05 most unlikely 05 to 5 very unlikely 5 to25 unlikely 25 to 75 possibly 75 to 95 likely 95 to995 very likely and gt995most likely Effect sizes (ESs)were calculated using Cohens d with an ES of lt02 con-sidered trivial gt02 small gt06 moderate gt12 large andgt20 very large [45]
Time to NK comparison between LCT and MCT groupswas made using a KaplanndashMeier survival analysis for time toevent [46] )e ldquoeventrdquo analysed was the first recorded in-stance of NK (ge05mmolmiddotLminus1 BOHB) for each participantand a log-rank test determined the significance of thesurvival analysis data [46]
Finally correlations were considered between BOHBand glucose BOHB and symptoms (Symptom-Q) andBOHB and mood (POMS) Correlations were considered tobe trivial rlt 01 smallgt 01 moderategt 03 largegt 05 verylargegt 07 nearly perfectgt 09 or perfect 1 [47] Statisticalsignificance of survival analyses correlations and additionalanalyses was determined by a p value of le005
3 Results
A total of five participants withdrew during the data col-lection periodmdashtwo from the MCT group (illness andgastrointestinal discomfort) and three from the LCT group(one due to extreme hunger one unreported and a third dueto light-headedness and inability to concentrate) )eremaining participantsrsquo (n 23) self-reported adherence tosupplementation was 97 (combined) for both treatmentgroups )irty-two (7) of BOHB measures failed to berecorded due to technical or operator error with the mea-surement device Mean imputation analysis was used toadjust for the missing measures [48]
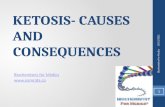
31 Effects on Beta-Hydroxybutyrate Supplementing MCTresulted in consistently higher blood levels of BOHB in ourcohort of healthy adults relative to LCT treatment withhigher BOHB at all time points in the MCTgroup (Figure 2)While clinically trivial effects were observed for days oneto six between-group effects for days seven to 19 wereclear for MCT relative to LCT (Table 2) )e magnitude ofthese effects was 02plusmn 07 mmolmiddotLminus1 (days 1 to 6) and 08plusmn07 mmolmiddotLminus1 (days 7 to 19)
)ere was also a very likely negative effect of BOHB onglucose in both groups )at is higher BOHB levels resultedin lower glucose levels )is was further indicated by a verylarge significant inverse relationship of glucose to BOHBfor both MCT (r minus070 p 00005) and LCT groups(r minus078 p 000003)
32 Time to Nutritional Ketosis Overall time to ketosis wasmore rapid with MCTsupplementation )e achievement ofNK within the first three days was higher with MCT versusLCT (17 versus 0 on day one and 33 versus 18 on daytwo) (Figure 3) and the mean time to NK was one dayshorter with MCT supplementation but any observed dif-ferences between LCT and MCT for time to NK failed toreach significance (p 030)
33 Symptoms of Keto-Induction Supplementation withMCT versus control resulted in lower symptoms associatedwith keto-induction with the mean sum of symptom scoreslower in the MCT group across all time points except fordays 16 18 and 19 (Figure 4)
Effects of MCTon the change in symptoms from baselinewere possibly beneficial for days 4 6 9 to 11 and 13 to 15 buton all other days effects were unclear relative to LCTImprovements in symptom scores from the preceding dayindicated a possibly beneficial effect of MCTon 11 of 19 days)ere was an unclear effect of BOHB as a predictor ofsymptoms for MCT relative to LCT (Table 2) However
00
05
10
15
20
25
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
BOH
B (m
mol
Lndash1
)
Day numberLCTMCT
Figure 2 Mean BOHB for MCT versus LCT supplementationError bars represent SE from the mean
4 Journal of Nutrition and Metabolism
Tabl
e2
Standardise
deffects
formeandifferences
(LCTminusMCT)
inmoo
dstateBO
HB
andbloo
dglucosefordays
1to
19
Dayrarr
Baselin
e1
23
45
67
89
1011
1213
1415
1617
1819
∆symptom
sfrom
baselin
e
Standard
difference
inmeans
minus008
019minus0
27minus0
02minus0
17
000
003minus0
28minus0
24minus0
22
015minus0
12minus0
26minus0
36
023
009
079
067
086
CL90
plusmn086
099
066
070
067
083
077
074
072
066
070
076
075
074
089
083
065
070
066
Clin
ical
inference
+minus
+
+
+
∆symptom
sby
day
Standard
difference
means
006minus0
16minus0
03minus0
24
034minus0
24
038minus0
10minus0
26minus0
37
036
031minus0
18minus0
19minus0
15
060minus0
26
030
006
CL90
plusmn085
067
049
067
054
049
050
056
053
073
062
064
050
043
064
060
068
048
041
Clin
ical
inference
+
+
+
+
+
∆PO
MSfrom
baselin
eStandard
difference
inmeans
046
026
065
035
062
040
034
071
011
023
033
028
045
054
044
034
048
064
061
CL90
plusmn071
077
080
077
061
080
090
084
084
083
084
079
086
080
073
060
086
080
021
Clin
ical
Inference
∆PO
MSby
day
046minus0
20
025minus0
17
027minus0
22minus0
06
037minus0
60
012
010minus0
06
017
009minus0
10minus0
10
015
016minus0
03
CL90
plusmn071
035
037
041
059
062
038
057
030
047
035
043
033
027
058
035
063
027
023
Clin
ical
Inference
+
+
+
++
+minusminusminus
+
minusminus
BOHB
Difference
inmeans
asafactor
116
124
116
106
100
104
148
190
187
245
191
185
231
184
176
206
167
193
171
116
CL90
times∕divide
175
171
161
168
174
179
189
179
190
191
171
176
169
182
186
201
198
190
197
175
Non
clinical
inference
++
+++
++++
+++
Glucose
Difference
inmeans
asafactor
094
099
099
098
100
098
096
095
103
093
088
104
085
100
098
094
094
093
101
094
CL90
times∕divide
111
114
109
110
108
110
111
110
111
109
111
109
126
110
111
107
107
107
108
111
Non
clinical
inference
+
++minusminus
+++
minus
+++
Standardise
deffectsform
eanchanges(LC
TminusMCT)
inSymptom
-QandPO
MS-TM
DSford
ays1
to19
relativ
eto
baselin
emeasuresa
ndford
ay-to-daychangesClin
icalinferences
basedon
thresholdchanceso
fharm
andbenefit
of25and05
Non
clinicalinferencesbasedon
thresholdchanceso
f5forsub
stantia
lmagnitudesPo
sitiveo
rclin
icallybeneficial++
+very
likely++
likely+po
ssiblyunclearnegativeo
rno
tclin
ically
beneficialminus
possiblyminusminus
likelyminusminusminus
very
likely
Journal of Nutrition and Metabolism 5
there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

ketosis such as the diabetic ketoacidosis results from un-controlled Type 1 diabetes [12] Both starvation or fastingketosis and nutritional ketosis result from evolutionary ad-aptations that allowed humans to survive in the absence ofcarbohydrate foods and thus glucose provision [13] Nutri-tional ketosis allows for the maintenance of ketosis withoutstarvation and so NK allows for the maintenance of ketosisfor longer than would be achievable with fasted ketosisVLCKDs typically result in BOHB levels of ge05mmolmiddotLminus1[14] and this level has been used as a cutoff point for entryinto NK [15] Adaptation to NK when transitioning froma standard higher carbohydrate diet to a VLCKD can causevarious short-term adverse effects [16] )ese effects ofldquoketo-inductionrdquo are constipation headache halitosismuscle cramps diarrhoea general weakness and rash [17])ese occur due to increased natriuresis kaliuresis anddiuresis in response to lowered insulin levels [18ndash21] greatestbetween days 1 and 4 of a fast or ketogenic diet [18] Transientreductions in glucose provision to the brain have been ob-served between days 1 and 3 with BG normalising after dayfour [22] while constipation and other gastrointestinal effectsresult from reduced food volume increased fat intake orreduced fibre intake [23 24] Difficulties with adherence toketogenic diets have been noted [3 17] but few studiesspecifically describe early adverse symptoms associated withketo-induction
Ketogenic diets typically contain a 3 1 to 4 1 ratio oflipids to nonlipid macronutrients or at least 75 of caloriescoming from lipids very low carbohydrates (often less than50 g) and low-to-moderate amounts of protein )e 4 1 lipidto nonlipid ratio ketogenic diet pioneered at Johns HopkinsUniversity Hospital [25 26] is now commonly used to induceketosis and is referred to as a ldquoclassicrdquo or ldquostandardrdquo ketogenicdiet Huttenlocher and colleagues first demonstrated thatdiets containing 60ndash75 of calories from lipids induce NK ifthey include a high proportion of medium chain triglycerides(MCTs) [27] A VLCKD with 60 of calories derived fromMCTs a three-fold greater intake of carbohydrate (18versus 6) and a sim50 (7 versus 10) increase in proteininduced NK with little clinical difference in BOHB levelswhen compared to a standard ketogenic diet [28] Unlikelong-chain triglycerides (LCTs) MCTs do not require theactions of bile normicellar-chylomicron-mediated absorptioninto the lymphatics and instead are diffused into the hepaticportal vein and preferentially converted into bio-availableketone bodies in the liver Moreover dietary MCTs promoteketonaemia and ketogenesis in both animals [29 30] andhumans [31]
Based on existing evidence MCT supplementation is de-monstrably ketogenic [29ndash31] increases BOHB in a linearand dose-dependent manner [32ndash36] and allows the achieve-ment of ketosis with lower amounts of lipids (and concomi-tantly higher levels of protein and carbohydrate) [28 37 38]However there is a paucity of research considering the rolethat MCTs may play in inducing ketosis more rapidly ina ketogenic diet with a 4 1 lipid to nonlipid ratio or inimproving symptoms of keto-induction and mood NK isdefined by the magnitude of ketonaemia (specificallyge05mmolmiddotLminus1 of BOHB) and symptoms of keto-induction
occur during the transition from a standard diet (withlimited ketone expression in the blood) and the achievementof NK )erefore it is likely that the use of MCTs resultingin ketonaemia and ketogenesis could reduce time to NKand symptoms of keto-induction )ese symptoms are likelyto relate at least in part to the transition from a glucosedominant fuel system to one in which BOHB becomesa primary fuel source Further by reducing the time to NKcompliance to a VLCKD could be improved Likewisemitigation of symptoms of keto-induction is likely to resultin improved adherence to the diet
)e aim of the present study therefore was to inves-tigate in a randomised double-blind placebo-controlledtrial whether MCTs reduce time to nutritional ketosis andsymptoms of keto-induction andmood in a classic ketogenicdiet )e primary outcome measured was the time takento achieve NK Secondary outcomes were symptoms andmood
2 Materials and Methods
Twenty-eight participants (2 males 26 females ageplusmn SD35plusmn 4 y) (Table 1) were recruited between the 18th and 19thof October 2015 and gave written informed consent toparticipate in this randomised double-blinded placebo-controlled study Participants were required to be non-obese (lt30 BMI) not diagnosed as diabetic not currentlynor previously following a ketogenic diet and not a client ofany of the researchers in clinical practice )e study tookplace between the 2nd and 21st of November 2015 Col-lection of data and analysis was performed at AUT HumanPotential Centre Auckland New Zealand (Figure 1)
Participants were prescribed a ketogenic diet with a 4 1lipid to nonlipid ratio Males were allocated a diet containing2200 kcalmiddotdayminus1 and females 1800 kcalmiddotdayminus1 each equating to80 calories from fat (including supplemental oils) 13 to17 from protein and 3 to 6 from carbohydrate Minordifferences in carbohydrate and protein were due to the useof a protein intake of 14 gmiddotkgminus1 bmmiddotdayminus1 (population meansfor male and female resp) consistent with InternationalSociety of Sports Nutrition (ISSN) guidelines for optimalprotein intake for performance [39] Participants wererandomised to receive either an MCT supplement con-taining 65 caprylic acid (C 8) and 35 capric acid (C 10)triglycerides (Amtrade NZ limited) or a long chain tri-glyceride (sunflower) oil (Home Brand) 30ml three times
Table 1 Demographic characteristics of participants
MCT LCTGender (MF) 111 110Age (years) mean (range) 40 (33 to 47) 40 (32 to 48)
Ethnicity (n)
European (5)
European (11)NZ Maori (2)
Pacific Island (3)Chinese (1)
Other Asian (1)MCT medium chain triglyceride LCT long-chain triglyceride M maleF female
2 Journal of Nutrition and Metabolism
per day for 20 days While MCTs are essentially nontoxic[40] Ivy et al observed that 100 of participants in theirstudy experienced gastric distress (cramping and diarrhoea)with dosages of 50 and 60 g MCT with only small GI effectsnoted at 30 g [41] We used this dosage (30 g) as it was mostlikely to elicit an effect without unduly exposing participantsto adverse effects arising from MCT ingestion For ouranalysis we considered the day in which each participantachieved ge05mmolmiddotLminus1 BOHB as the time at which theyhad achieved NK We proposed this threshold for NK(ge05mmolmiddotLminus1) based on the level of BOHB observed inthose following a VLCKD[14] and as used as a cutoff pointfor ketosis by Guerci and colleagues [15]
Participants were provided with a ldquoFreeStyle Neordquoblood-prick ketometerglucometer (Abbott Industries) andwere required to use the device to measure and record fastedBOHB and BG daily upon waking Participants were alsoinstructed to complete a questionnaire including a keto-induction symptoms questionnaire (Symptom-Q) andProfile of Mood States-Short Form (POMS-SF) )e Profileof Mood States is a questionnaire commonly used to de-termine the overall mood state of study participants [42]Saya Shacham developed a shortened 37 question version ofthis form with correlation coefficients between the short andoriginal scales all above 95 indicating the suitability of thisshortened form for estimating mood )e symptoms ques-tionnaire was developed by one of the authors (d C Harvey)based on symptoms commonly observed in previous studiesof ketogenic diets )e questionnaire asked ldquoIn the past 24hours to what extent have you experienced the following
symptomsrdquo answered on a Likert scale of (1) not at all(2) mild (3) moderate (4) severe and (5) intolerable forthe following symptomseffects headache constipationdiarrhoea stomach or intestinal pain intestinal bloatinghalitosis (bad breath) muscle cramps muscle weakness skinrash and difficulty concentrating
An AUT University staff member who was not involvedin data collection randomised participants using a simplerandomisation technique of coin flipping to generatea treatment sequence into two groups ldquoArdquo and ldquoBrdquo andlabelled the supplemental oils ldquoArdquo or ldquoBrdquo for distribution andblinding and retained the blinding key )e primary re-searcher was unblinded to the supplement-oil key only afterdata analysis had been completed
Participants were instructed to contact the primary andtertiary researchers for any assistance during the study du-ration CH is a registered clinical nutritionist with the NewZealand Clinical Nutrition Association and MW is a regis-tered nutritionist with the Nutrition Society of New Zealand)e research was conducted in accordance with AUT ethicalguidelines Ethics approval was provided by the AUT Uni-versity Ethics Committee (approval number 15317)
21 StatisticalAnalyses Magnitude-based inferences (MBIs)were used to compare the observed measures (BOHB BGSymptoms-Q and POMS-SF) Pairwise comparisons weremade between each of the 19 time points for control (LCT)and experimental (MCT) trials for all using a customisedanalysis spreadsheet [43] Pairwise comparisons were also
Allocated to LCT intervention (n = 14)
Did not receive allocated intervention(n = 0)
Received allocated intervention (n = 14)(i)(ii)
Allocated to MCT intervention (n = 14)Received allocated intervention (n = 14)Did not receive allocated intervention(n = 0)
(i)(ii)
Analysed (n = 12)Excluded from analysis (n = 0)(i)
Allocation
Analysis
Follow-up
Analysed (n = 11)Excluded from analysis (n = 0)(i)
Assessed for eligibility (n = 59)Enrollment
Excluded (n = 31)Not meeting inclusion criteria (n = 22)Declined to participate (n = 9)Other reasons (n = 0)
(i)(ii)
(iii)
Randomized (n = 28)
Lost to follow-up (n = 0)Discontinued intervention (n = 2) due to
gastrointestinal distress
Lost to follow-up (n = 0)Discontinued intervention (n = 3) due to light-headedness and inability to concentrate (n = 1)
extreme hunger (n = 1) unreported (n = 1)
Figure 1 CONSORT flow diagram showing recruitment and retention of study participants
Journal of Nutrition and Metabolism 3
made between observed measures relative to respectivebaseline values for each group Data for BOHB and BGcomparisons were log transformed for analysis to reducebias arising from nonuniformity of error and subsequentlyback transformed to obtain changes in means and varia-tions as factors Raw data were used for comparisons be-tween groups for Symptoms-Q and POMS-SF results )esum of symptoms scores (Symptoms-Q) and total mooddisturbance score (TMDS) of the POMS-SF were used foranalysis Total mood disturbance score (TMDS) of thePOMS-SF was calculated by subtracting positive mooditems from negative mood items [44] To make inferencesabout true (population) values of the effect on BOHBSymptoms-Q and POMS of MCT relative to LCT theuncertainty in the effect was expressed as 90 confidencelimits and as likelihoods that the true value of the effectrepresents substantial change (harm or benefit) An effectwas deemed to be unclear if its confidence interval over-lapped the thresholds for substantiveness that is if theeffect could be substantially positive and negative [45] )esmallest worthwhile change for between-group means forall blood and perceptual measures was calculated as 02 ofthe between-subject SD [45] Inferences were based onthreshold chances of harm of a difference between groupsof 05 and benefit of 25 To determine the likelihood ofclinical effects the default values and qualitative terms wereset at lt05 most unlikely 05 to 5 very unlikely 5 to25 unlikely 25 to 75 possibly 75 to 95 likely 95 to995 very likely and gt995most likely Effect sizes (ESs)were calculated using Cohens d with an ES of lt02 con-sidered trivial gt02 small gt06 moderate gt12 large andgt20 very large [45]
Time to NK comparison between LCT and MCT groupswas made using a KaplanndashMeier survival analysis for time toevent [46] )e ldquoeventrdquo analysed was the first recorded in-stance of NK (ge05mmolmiddotLminus1 BOHB) for each participantand a log-rank test determined the significance of thesurvival analysis data [46]
Finally correlations were considered between BOHBand glucose BOHB and symptoms (Symptom-Q) andBOHB and mood (POMS) Correlations were considered tobe trivial rlt 01 smallgt 01 moderategt 03 largegt 05 verylargegt 07 nearly perfectgt 09 or perfect 1 [47] Statisticalsignificance of survival analyses correlations and additionalanalyses was determined by a p value of le005
3 Results
A total of five participants withdrew during the data col-lection periodmdashtwo from the MCT group (illness andgastrointestinal discomfort) and three from the LCT group(one due to extreme hunger one unreported and a third dueto light-headedness and inability to concentrate) )eremaining participantsrsquo (n 23) self-reported adherence tosupplementation was 97 (combined) for both treatmentgroups )irty-two (7) of BOHB measures failed to berecorded due to technical or operator error with the mea-surement device Mean imputation analysis was used toadjust for the missing measures [48]
31 Effects on Beta-Hydroxybutyrate Supplementing MCTresulted in consistently higher blood levels of BOHB in ourcohort of healthy adults relative to LCT treatment withhigher BOHB at all time points in the MCTgroup (Figure 2)While clinically trivial effects were observed for days oneto six between-group effects for days seven to 19 wereclear for MCT relative to LCT (Table 2) )e magnitude ofthese effects was 02plusmn 07 mmolmiddotLminus1 (days 1 to 6) and 08plusmn07 mmolmiddotLminus1 (days 7 to 19)
)ere was also a very likely negative effect of BOHB onglucose in both groups )at is higher BOHB levels resultedin lower glucose levels )is was further indicated by a verylarge significant inverse relationship of glucose to BOHBfor both MCT (r minus070 p 00005) and LCT groups(r minus078 p 000003)
32 Time to Nutritional Ketosis Overall time to ketosis wasmore rapid with MCTsupplementation )e achievement ofNK within the first three days was higher with MCT versusLCT (17 versus 0 on day one and 33 versus 18 on daytwo) (Figure 3) and the mean time to NK was one dayshorter with MCT supplementation but any observed dif-ferences between LCT and MCT for time to NK failed toreach significance (p 030)
33 Symptoms of Keto-Induction Supplementation withMCT versus control resulted in lower symptoms associatedwith keto-induction with the mean sum of symptom scoreslower in the MCT group across all time points except fordays 16 18 and 19 (Figure 4)
Effects of MCTon the change in symptoms from baselinewere possibly beneficial for days 4 6 9 to 11 and 13 to 15 buton all other days effects were unclear relative to LCTImprovements in symptom scores from the preceding dayindicated a possibly beneficial effect of MCTon 11 of 19 days)ere was an unclear effect of BOHB as a predictor ofsymptoms for MCT relative to LCT (Table 2) However
00
05
10
15
20
25
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
BOH
B (m
mol
Lndash1
)
Day numberLCTMCT
Figure 2 Mean BOHB for MCT versus LCT supplementationError bars represent SE from the mean
4 Journal of Nutrition and Metabolism
Tabl
e2
Standardise
deffects
formeandifferences
(LCTminusMCT)
inmoo
dstateBO
HB
andbloo
dglucosefordays
1to
19
Dayrarr
Baselin
e1
23
45
67
89
1011
1213
1415
1617
1819
∆symptom
sfrom
baselin
e
Standard
difference
inmeans
minus008
019minus0
27minus0
02minus0
17
000
003minus0
28minus0
24minus0
22
015minus0
12minus0
26minus0
36
023
009
079
067
086
CL90
plusmn086
099
066
070
067
083
077
074
072
066
070
076
075
074
089
083
065
070
066
Clin
ical
inference
+minus
+
+
+
∆symptom
sby
day
Standard
difference
means
006minus0
16minus0
03minus0
24
034minus0
24
038minus0
10minus0
26minus0
37
036
031minus0
18minus0
19minus0
15
060minus0
26
030
006
CL90
plusmn085
067
049
067
054
049
050
056
053
073
062
064
050
043
064
060
068
048
041
Clin
ical
inference
+
+
+
+
+
∆PO
MSfrom
baselin
eStandard
difference
inmeans
046
026
065
035
062
040
034
071
011
023
033
028
045
054
044
034
048
064
061
CL90
plusmn071
077
080
077
061
080
090
084
084
083
084
079
086
080
073
060
086
080
021
Clin
ical
Inference
∆PO
MSby
day
046minus0
20
025minus0
17
027minus0
22minus0
06
037minus0
60
012
010minus0
06
017
009minus0
10minus0
10
015
016minus0
03
CL90
plusmn071
035
037
041
059
062
038
057
030
047
035
043
033
027
058
035
063
027
023
Clin
ical
Inference
+
+
+
++
+minusminusminus
+
minusminus
BOHB
Difference
inmeans
asafactor
116
124
116
106
100
104
148
190
187
245
191
185
231
184
176
206
167
193
171
116
CL90
times∕divide
175
171
161
168
174
179
189
179
190
191
171
176
169
182
186
201
198
190
197
175
Non
clinical
inference
++
+++
++++
+++
Glucose
Difference
inmeans
asafactor
094
099
099
098
100
098
096
095
103
093
088
104
085
100
098
094
094
093
101
094
CL90
times∕divide
111
114
109
110
108
110
111
110
111
109
111
109
126
110
111
107
107
107
108
111
Non
clinical
inference
+
++minusminus
+++
minus
+++
Standardise
deffectsform
eanchanges(LC
TminusMCT)
inSymptom
-QandPO
MS-TM
DSford
ays1
to19
relativ
eto
baselin
emeasuresa
ndford
ay-to-daychangesClin
icalinferences
basedon
thresholdchanceso
fharm
andbenefit
of25and05
Non
clinicalinferencesbasedon
thresholdchanceso
f5forsub
stantia
lmagnitudesPo
sitiveo
rclin
icallybeneficial++
+very
likely++
likely+po
ssiblyunclearnegativeo
rno
tclin
ically
beneficialminus
possiblyminusminus
likelyminusminusminus
very
likely
Journal of Nutrition and Metabolism 5
there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

per day for 20 days While MCTs are essentially nontoxic[40] Ivy et al observed that 100 of participants in theirstudy experienced gastric distress (cramping and diarrhoea)with dosages of 50 and 60 g MCT with only small GI effectsnoted at 30 g [41] We used this dosage (30 g) as it was mostlikely to elicit an effect without unduly exposing participantsto adverse effects arising from MCT ingestion For ouranalysis we considered the day in which each participantachieved ge05mmolmiddotLminus1 BOHB as the time at which theyhad achieved NK We proposed this threshold for NK(ge05mmolmiddotLminus1) based on the level of BOHB observed inthose following a VLCKD[14] and as used as a cutoff pointfor ketosis by Guerci and colleagues [15]
Participants were provided with a ldquoFreeStyle Neordquoblood-prick ketometerglucometer (Abbott Industries) andwere required to use the device to measure and record fastedBOHB and BG daily upon waking Participants were alsoinstructed to complete a questionnaire including a keto-induction symptoms questionnaire (Symptom-Q) andProfile of Mood States-Short Form (POMS-SF) )e Profileof Mood States is a questionnaire commonly used to de-termine the overall mood state of study participants [42]Saya Shacham developed a shortened 37 question version ofthis form with correlation coefficients between the short andoriginal scales all above 95 indicating the suitability of thisshortened form for estimating mood )e symptoms ques-tionnaire was developed by one of the authors (d C Harvey)based on symptoms commonly observed in previous studiesof ketogenic diets )e questionnaire asked ldquoIn the past 24hours to what extent have you experienced the following
symptomsrdquo answered on a Likert scale of (1) not at all(2) mild (3) moderate (4) severe and (5) intolerable forthe following symptomseffects headache constipationdiarrhoea stomach or intestinal pain intestinal bloatinghalitosis (bad breath) muscle cramps muscle weakness skinrash and difficulty concentrating
An AUT University staff member who was not involvedin data collection randomised participants using a simplerandomisation technique of coin flipping to generatea treatment sequence into two groups ldquoArdquo and ldquoBrdquo andlabelled the supplemental oils ldquoArdquo or ldquoBrdquo for distribution andblinding and retained the blinding key )e primary re-searcher was unblinded to the supplement-oil key only afterdata analysis had been completed
Participants were instructed to contact the primary andtertiary researchers for any assistance during the study du-ration CH is a registered clinical nutritionist with the NewZealand Clinical Nutrition Association and MW is a regis-tered nutritionist with the Nutrition Society of New Zealand)e research was conducted in accordance with AUT ethicalguidelines Ethics approval was provided by the AUT Uni-versity Ethics Committee (approval number 15317)
21 StatisticalAnalyses Magnitude-based inferences (MBIs)were used to compare the observed measures (BOHB BGSymptoms-Q and POMS-SF) Pairwise comparisons weremade between each of the 19 time points for control (LCT)and experimental (MCT) trials for all using a customisedanalysis spreadsheet [43] Pairwise comparisons were also
Allocated to LCT intervention (n = 14)
Did not receive allocated intervention(n = 0)
Received allocated intervention (n = 14)(i)(ii)
Allocated to MCT intervention (n = 14)Received allocated intervention (n = 14)Did not receive allocated intervention(n = 0)
(i)(ii)
Analysed (n = 12)Excluded from analysis (n = 0)(i)
Allocation
Analysis
Follow-up
Analysed (n = 11)Excluded from analysis (n = 0)(i)
Assessed for eligibility (n = 59)Enrollment
Excluded (n = 31)Not meeting inclusion criteria (n = 22)Declined to participate (n = 9)Other reasons (n = 0)
(i)(ii)
(iii)
Randomized (n = 28)
Lost to follow-up (n = 0)Discontinued intervention (n = 2) due to
gastrointestinal distress
Lost to follow-up (n = 0)Discontinued intervention (n = 3) due to light-headedness and inability to concentrate (n = 1)
extreme hunger (n = 1) unreported (n = 1)
Figure 1 CONSORT flow diagram showing recruitment and retention of study participants
Journal of Nutrition and Metabolism 3
made between observed measures relative to respectivebaseline values for each group Data for BOHB and BGcomparisons were log transformed for analysis to reducebias arising from nonuniformity of error and subsequentlyback transformed to obtain changes in means and varia-tions as factors Raw data were used for comparisons be-tween groups for Symptoms-Q and POMS-SF results )esum of symptoms scores (Symptoms-Q) and total mooddisturbance score (TMDS) of the POMS-SF were used foranalysis Total mood disturbance score (TMDS) of thePOMS-SF was calculated by subtracting positive mooditems from negative mood items [44] To make inferencesabout true (population) values of the effect on BOHBSymptoms-Q and POMS of MCT relative to LCT theuncertainty in the effect was expressed as 90 confidencelimits and as likelihoods that the true value of the effectrepresents substantial change (harm or benefit) An effectwas deemed to be unclear if its confidence interval over-lapped the thresholds for substantiveness that is if theeffect could be substantially positive and negative [45] )esmallest worthwhile change for between-group means forall blood and perceptual measures was calculated as 02 ofthe between-subject SD [45] Inferences were based onthreshold chances of harm of a difference between groupsof 05 and benefit of 25 To determine the likelihood ofclinical effects the default values and qualitative terms wereset at lt05 most unlikely 05 to 5 very unlikely 5 to25 unlikely 25 to 75 possibly 75 to 95 likely 95 to995 very likely and gt995most likely Effect sizes (ESs)were calculated using Cohens d with an ES of lt02 con-sidered trivial gt02 small gt06 moderate gt12 large andgt20 very large [45]
Time to NK comparison between LCT and MCT groupswas made using a KaplanndashMeier survival analysis for time toevent [46] )e ldquoeventrdquo analysed was the first recorded in-stance of NK (ge05mmolmiddotLminus1 BOHB) for each participantand a log-rank test determined the significance of thesurvival analysis data [46]
Finally correlations were considered between BOHBand glucose BOHB and symptoms (Symptom-Q) andBOHB and mood (POMS) Correlations were considered tobe trivial rlt 01 smallgt 01 moderategt 03 largegt 05 verylargegt 07 nearly perfectgt 09 or perfect 1 [47] Statisticalsignificance of survival analyses correlations and additionalanalyses was determined by a p value of le005
3 Results
A total of five participants withdrew during the data col-lection periodmdashtwo from the MCT group (illness andgastrointestinal discomfort) and three from the LCT group(one due to extreme hunger one unreported and a third dueto light-headedness and inability to concentrate) )eremaining participantsrsquo (n 23) self-reported adherence tosupplementation was 97 (combined) for both treatmentgroups )irty-two (7) of BOHB measures failed to berecorded due to technical or operator error with the mea-surement device Mean imputation analysis was used toadjust for the missing measures [48]
31 Effects on Beta-Hydroxybutyrate Supplementing MCTresulted in consistently higher blood levels of BOHB in ourcohort of healthy adults relative to LCT treatment withhigher BOHB at all time points in the MCTgroup (Figure 2)While clinically trivial effects were observed for days oneto six between-group effects for days seven to 19 wereclear for MCT relative to LCT (Table 2) )e magnitude ofthese effects was 02plusmn 07 mmolmiddotLminus1 (days 1 to 6) and 08plusmn07 mmolmiddotLminus1 (days 7 to 19)
)ere was also a very likely negative effect of BOHB onglucose in both groups )at is higher BOHB levels resultedin lower glucose levels )is was further indicated by a verylarge significant inverse relationship of glucose to BOHBfor both MCT (r minus070 p 00005) and LCT groups(r minus078 p 000003)
32 Time to Nutritional Ketosis Overall time to ketosis wasmore rapid with MCTsupplementation )e achievement ofNK within the first three days was higher with MCT versusLCT (17 versus 0 on day one and 33 versus 18 on daytwo) (Figure 3) and the mean time to NK was one dayshorter with MCT supplementation but any observed dif-ferences between LCT and MCT for time to NK failed toreach significance (p 030)
33 Symptoms of Keto-Induction Supplementation withMCT versus control resulted in lower symptoms associatedwith keto-induction with the mean sum of symptom scoreslower in the MCT group across all time points except fordays 16 18 and 19 (Figure 4)
Effects of MCTon the change in symptoms from baselinewere possibly beneficial for days 4 6 9 to 11 and 13 to 15 buton all other days effects were unclear relative to LCTImprovements in symptom scores from the preceding dayindicated a possibly beneficial effect of MCTon 11 of 19 days)ere was an unclear effect of BOHB as a predictor ofsymptoms for MCT relative to LCT (Table 2) However
00
05
10
15
20
25
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
BOH
B (m
mol
Lndash1
)
Day numberLCTMCT
Figure 2 Mean BOHB for MCT versus LCT supplementationError bars represent SE from the mean
4 Journal of Nutrition and Metabolism
Tabl
e2
Standardise
deffects
formeandifferences
(LCTminusMCT)
inmoo
dstateBO
HB
andbloo
dglucosefordays
1to
19
Dayrarr
Baselin
e1
23
45
67
89
1011
1213
1415
1617
1819
∆symptom
sfrom
baselin
e
Standard
difference
inmeans
minus008
019minus0
27minus0
02minus0
17
000
003minus0
28minus0
24minus0
22
015minus0
12minus0
26minus0
36
023
009
079
067
086
CL90
plusmn086
099
066
070
067
083
077
074
072
066
070
076
075
074
089
083
065
070
066
Clin
ical
inference
+minus
+
+
+
∆symptom
sby
day
Standard
difference
means
006minus0
16minus0
03minus0
24
034minus0
24
038minus0
10minus0
26minus0
37
036
031minus0
18minus0
19minus0
15
060minus0
26
030
006
CL90
plusmn085
067
049
067
054
049
050
056
053
073
062
064
050
043
064
060
068
048
041
Clin
ical
inference
+
+
+
+
+
∆PO
MSfrom
baselin
eStandard
difference
inmeans
046
026
065
035
062
040
034
071
011
023
033
028
045
054
044
034
048
064
061
CL90
plusmn071
077
080
077
061
080
090
084
084
083
084
079
086
080
073
060
086
080
021
Clin
ical
Inference
∆PO
MSby
day
046minus0
20
025minus0
17
027minus0
22minus0
06
037minus0
60
012
010minus0
06
017
009minus0
10minus0
10
015
016minus0
03
CL90
plusmn071
035
037
041
059
062
038
057
030
047
035
043
033
027
058
035
063
027
023
Clin
ical
Inference
+
+
+
++
+minusminusminus
+
minusminus
BOHB
Difference
inmeans
asafactor
116
124
116
106
100
104
148
190
187
245
191
185
231
184
176
206
167
193
171
116
CL90
times∕divide
175
171
161
168
174
179
189
179
190
191
171
176
169
182
186
201
198
190
197
175
Non
clinical
inference
++
+++
++++
+++
Glucose
Difference
inmeans
asafactor
094
099
099
098
100
098
096
095
103
093
088
104
085
100
098
094
094
093
101
094
CL90
times∕divide
111
114
109
110
108
110
111
110
111
109
111
109
126
110
111
107
107
107
108
111
Non
clinical
inference
+
++minusminus
+++
minus
+++
Standardise
deffectsform
eanchanges(LC
TminusMCT)
inSymptom
-QandPO
MS-TM
DSford
ays1
to19
relativ
eto
baselin
emeasuresa
ndford
ay-to-daychangesClin
icalinferences
basedon
thresholdchanceso
fharm
andbenefit
of25and05
Non
clinicalinferencesbasedon
thresholdchanceso
f5forsub
stantia
lmagnitudesPo
sitiveo
rclin
icallybeneficial++
+very
likely++
likely+po
ssiblyunclearnegativeo
rno
tclin
ically
beneficialminus
possiblyminusminus
likelyminusminusminus
very
likely
Journal of Nutrition and Metabolism 5
there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

made between observed measures relative to respectivebaseline values for each group Data for BOHB and BGcomparisons were log transformed for analysis to reducebias arising from nonuniformity of error and subsequentlyback transformed to obtain changes in means and varia-tions as factors Raw data were used for comparisons be-tween groups for Symptoms-Q and POMS-SF results )esum of symptoms scores (Symptoms-Q) and total mooddisturbance score (TMDS) of the POMS-SF were used foranalysis Total mood disturbance score (TMDS) of thePOMS-SF was calculated by subtracting positive mooditems from negative mood items [44] To make inferencesabout true (population) values of the effect on BOHBSymptoms-Q and POMS of MCT relative to LCT theuncertainty in the effect was expressed as 90 confidencelimits and as likelihoods that the true value of the effectrepresents substantial change (harm or benefit) An effectwas deemed to be unclear if its confidence interval over-lapped the thresholds for substantiveness that is if theeffect could be substantially positive and negative [45] )esmallest worthwhile change for between-group means forall blood and perceptual measures was calculated as 02 ofthe between-subject SD [45] Inferences were based onthreshold chances of harm of a difference between groupsof 05 and benefit of 25 To determine the likelihood ofclinical effects the default values and qualitative terms wereset at lt05 most unlikely 05 to 5 very unlikely 5 to25 unlikely 25 to 75 possibly 75 to 95 likely 95 to995 very likely and gt995most likely Effect sizes (ESs)were calculated using Cohens d with an ES of lt02 con-sidered trivial gt02 small gt06 moderate gt12 large andgt20 very large [45]
Time to NK comparison between LCT and MCT groupswas made using a KaplanndashMeier survival analysis for time toevent [46] )e ldquoeventrdquo analysed was the first recorded in-stance of NK (ge05mmolmiddotLminus1 BOHB) for each participantand a log-rank test determined the significance of thesurvival analysis data [46]
Finally correlations were considered between BOHBand glucose BOHB and symptoms (Symptom-Q) andBOHB and mood (POMS) Correlations were considered tobe trivial rlt 01 smallgt 01 moderategt 03 largegt 05 verylargegt 07 nearly perfectgt 09 or perfect 1 [47] Statisticalsignificance of survival analyses correlations and additionalanalyses was determined by a p value of le005
3 Results
A total of five participants withdrew during the data col-lection periodmdashtwo from the MCT group (illness andgastrointestinal discomfort) and three from the LCT group(one due to extreme hunger one unreported and a third dueto light-headedness and inability to concentrate) )eremaining participantsrsquo (n 23) self-reported adherence tosupplementation was 97 (combined) for both treatmentgroups )irty-two (7) of BOHB measures failed to berecorded due to technical or operator error with the mea-surement device Mean imputation analysis was used toadjust for the missing measures [48]
31 Effects on Beta-Hydroxybutyrate Supplementing MCTresulted in consistently higher blood levels of BOHB in ourcohort of healthy adults relative to LCT treatment withhigher BOHB at all time points in the MCTgroup (Figure 2)While clinically trivial effects were observed for days oneto six between-group effects for days seven to 19 wereclear for MCT relative to LCT (Table 2) )e magnitude ofthese effects was 02plusmn 07 mmolmiddotLminus1 (days 1 to 6) and 08plusmn07 mmolmiddotLminus1 (days 7 to 19)
)ere was also a very likely negative effect of BOHB onglucose in both groups )at is higher BOHB levels resultedin lower glucose levels )is was further indicated by a verylarge significant inverse relationship of glucose to BOHBfor both MCT (r minus070 p 00005) and LCT groups(r minus078 p 000003)
32 Time to Nutritional Ketosis Overall time to ketosis wasmore rapid with MCTsupplementation )e achievement ofNK within the first three days was higher with MCT versusLCT (17 versus 0 on day one and 33 versus 18 on daytwo) (Figure 3) and the mean time to NK was one dayshorter with MCT supplementation but any observed dif-ferences between LCT and MCT for time to NK failed toreach significance (p 030)
33 Symptoms of Keto-Induction Supplementation withMCT versus control resulted in lower symptoms associatedwith keto-induction with the mean sum of symptom scoreslower in the MCT group across all time points except fordays 16 18 and 19 (Figure 4)
Effects of MCTon the change in symptoms from baselinewere possibly beneficial for days 4 6 9 to 11 and 13 to 15 buton all other days effects were unclear relative to LCTImprovements in symptom scores from the preceding dayindicated a possibly beneficial effect of MCTon 11 of 19 days)ere was an unclear effect of BOHB as a predictor ofsymptoms for MCT relative to LCT (Table 2) However
00
05
10
15
20
25
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
BOH
B (m
mol
Lndash1
)
Day numberLCTMCT
Figure 2 Mean BOHB for MCT versus LCT supplementationError bars represent SE from the mean
4 Journal of Nutrition and Metabolism
Tabl
e2
Standardise
deffects
formeandifferences
(LCTminusMCT)
inmoo
dstateBO
HB
andbloo
dglucosefordays
1to
19
Dayrarr
Baselin
e1
23
45
67
89
1011
1213
1415
1617
1819
∆symptom
sfrom
baselin
e
Standard
difference
inmeans
minus008
019minus0
27minus0
02minus0
17
000
003minus0
28minus0
24minus0
22
015minus0
12minus0
26minus0
36
023
009
079
067
086
CL90
plusmn086
099
066
070
067
083
077
074
072
066
070
076
075
074
089
083
065
070
066
Clin
ical
inference
+minus
+
+
+
∆symptom
sby
day
Standard
difference
means
006minus0
16minus0
03minus0
24
034minus0
24
038minus0
10minus0
26minus0
37
036
031minus0
18minus0
19minus0
15
060minus0
26
030
006
CL90
plusmn085
067
049
067
054
049
050
056
053
073
062
064
050
043
064
060
068
048
041
Clin
ical
inference
+
+
+
+
+
∆PO
MSfrom
baselin
eStandard
difference
inmeans
046
026
065
035
062
040
034
071
011
023
033
028
045
054
044
034
048
064
061
CL90
plusmn071
077
080
077
061
080
090
084
084
083
084
079
086
080
073
060
086
080
021
Clin
ical
Inference
∆PO
MSby
day
046minus0
20
025minus0
17
027minus0
22minus0
06
037minus0
60
012
010minus0
06
017
009minus0
10minus0
10
015
016minus0
03
CL90
plusmn071
035
037
041
059
062
038
057
030
047
035
043
033
027
058
035
063
027
023
Clin
ical
Inference
+
+
+
++
+minusminusminus
+
minusminus
BOHB
Difference
inmeans
asafactor
116
124
116
106
100
104
148
190
187
245
191
185
231
184
176
206
167
193
171
116
CL90
times∕divide
175
171
161
168
174
179
189
179
190
191
171
176
169
182
186
201
198
190
197
175
Non
clinical
inference
++
+++
++++
+++
Glucose
Difference
inmeans
asafactor
094
099
099
098
100
098
096
095
103
093
088
104
085
100
098
094
094
093
101
094
CL90
times∕divide
111
114
109
110
108
110
111
110
111
109
111
109
126
110
111
107
107
107
108
111
Non
clinical
inference
+
++minusminus
+++
minus
+++
Standardise
deffectsform
eanchanges(LC
TminusMCT)
inSymptom
-QandPO
MS-TM
DSford
ays1
to19
relativ
eto
baselin
emeasuresa
ndford
ay-to-daychangesClin
icalinferences
basedon
thresholdchanceso
fharm
andbenefit
of25and05
Non
clinicalinferencesbasedon
thresholdchanceso
f5forsub
stantia
lmagnitudesPo
sitiveo
rclin
icallybeneficial++
+very
likely++
likely+po
ssiblyunclearnegativeo
rno
tclin
ically
beneficialminus
possiblyminusminus
likelyminusminusminus
very
likely
Journal of Nutrition and Metabolism 5
there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Tabl
e2
Standardise
deffects
formeandifferences
(LCTminusMCT)
inmoo
dstateBO
HB
andbloo
dglucosefordays
1to
19
Dayrarr
Baselin
e1
23
45
67
89
1011
1213
1415
1617
1819
∆symptom
sfrom
baselin
e
Standard
difference
inmeans
minus008
019minus0
27minus0
02minus0
17
000
003minus0
28minus0
24minus0
22
015minus0
12minus0
26minus0
36
023
009
079
067
086
CL90
plusmn086
099
066
070
067
083
077
074
072
066
070
076
075
074
089
083
065
070
066
Clin
ical
inference
+minus
+
+
+
∆symptom
sby
day
Standard
difference
means
006minus0
16minus0
03minus0
24
034minus0
24
038minus0
10minus0
26minus0
37
036
031minus0
18minus0
19minus0
15
060minus0
26
030
006
CL90
plusmn085
067
049
067
054
049
050
056
053
073
062
064
050
043
064
060
068
048
041
Clin
ical
inference
+
+
+
+
+
∆PO
MSfrom
baselin
eStandard
difference
inmeans
046
026
065
035
062
040
034
071
011
023
033
028
045
054
044
034
048
064
061
CL90
plusmn071
077
080
077
061
080
090
084
084
083
084
079
086
080
073
060
086
080
021
Clin
ical
Inference
∆PO
MSby
day
046minus0
20
025minus0
17
027minus0
22minus0
06
037minus0
60
012
010minus0
06
017
009minus0
10minus0
10
015
016minus0
03
CL90
plusmn071
035
037
041
059
062
038
057
030
047
035
043
033
027
058
035
063
027
023
Clin
ical
Inference
+
+
+
++
+minusminusminus
+
minusminus
BOHB
Difference
inmeans
asafactor
116
124
116
106
100
104
148
190
187
245
191
185
231
184
176
206
167
193
171
116
CL90
times∕divide
175
171
161
168
174
179
189
179
190
191
171
176
169
182
186
201
198
190
197
175
Non
clinical
inference
++
+++
++++
+++
Glucose
Difference
inmeans
asafactor
094
099
099
098
100
098
096
095
103
093
088
104
085
100
098
094
094
093
101
094
CL90
times∕divide
111
114
109
110
108
110
111
110
111
109
111
109
126
110
111
107
107
107
108
111
Non
clinical
inference
+
++minusminus
+++
minus
+++
Standardise
deffectsform
eanchanges(LC
TminusMCT)
inSymptom
-QandPO
MS-TM
DSford
ays1
to19
relativ
eto
baselin
emeasuresa
ndford
ay-to-daychangesClin
icalinferences
basedon
thresholdchanceso
fharm
andbenefit
of25and05
Non
clinicalinferencesbasedon
thresholdchanceso
f5forsub
stantia
lmagnitudesPo
sitiveo
rclin
icallybeneficial++
+very
likely++
likely+po
ssiblyunclearnegativeo
rno
tclin
ically
beneficialminus
possiblyminusminus
likelyminusminusminus
very
likely
Journal of Nutrition and Metabolism 5
there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

there was a large inverse correlation (rminus060) observedbetween BOHB and Symptoms-Q in the MCT group(p 0005) only We noted a small inverse correlationbetween BOHB and symptoms in LCT (r minus023) a resultthat failed to reach significance (p 030)
34 Mood Mood scores were improved at all time pointsfrom baseline in both groups with generally better mood
reported by the LCTgroup compared to theMCT As BOHBlevels increased reported mood improved in both groups)ere was a significant large inverse correlation betweenmean BOHB and mean POMS-TMDS in both the MCT(r minus070 p 00006) and LCT supplemented groups(r minus067 p 0001) (Figure 5) However the effect ofMCT relative to LCT on improvement in mood across alltime points was unclear (Table 2)
When considering changes relative to the precedingday there were approximately equal days of improvementin MCT versus LCT supplementation (nine and ten daysresp) A possible beneficial effect was observed across eightdays for MCT supplementation (Table 2) MCT supple-mentation provides very likely beneficial effects on TMDSwhen BOHB is a predictor A large correlation betweenglucose and TMDS in both MCT (r 050 p 002) andLCT (r 059 p 001) was also observed )ere wasa possibly beneficial effect from MCT supplementationwhen glucose was used as a predictor of mood We ob-served an association between mood scores and symptomscores across both groups (MCT r 061 p 0004 LCTr 063 p 0003)
4 Discussion
)is study was the first to assess the impact of MCTon timeto NK and symptoms of keto-induction and mood andwe believe the first to specifically describe symptoms of
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Pe
rcen
t sur
viva
l (
)Time to nutritional ketosis (days)
LCTMCTMedian
MCT (n = 12)LCT (n = 11)
Day In NK In NKd in NK
1 0 0 02 2 2 183 6 4 554 8 2 735 9 1 826 9 0 827 9 0 8211 10 1 9114
Not in NK
1195322211 10 0 91
In NK In NKd in NK
10 2 2 178 4 2 336 6 2 506 6 0 504 8 2 673 9 1 751 11 2 921 11 0 92
Not in NK
0 12 1 100
LCT = long chain triglyceride MCT = medium chain triglyceride NK = nutritional ketosis
Figure 3 KaplanndashMeier survival graph and relative percentages of participants achieving nutritional ketosis (NK)
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Sum
of s
ympt
om sc
ores
Day number
LCTMCT
Figure 4 Sum of symptoms of keto-induction scores Bars rep-resent SE from the mean
6 Journal of Nutrition and Metabolism
keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

keto-induction (keto-flu) within the first few days of a ke-togenic diet
Not surprisingly there was a clear and significant effectof MCT supplementation on BOHB levels relative to LCTcontrol MCTs are demonstrably ketogenic [29ndash31] and thiseffect was expected All MCT participants reached NK(ge05mmolmiddotLminus1) with one participant in the LCT groupfailing to reach NK A significant effect on time to NK wasnot demonstrated despite the MCT group (based on meanBOHB levels) achieving ketosis two days earlier on day 2versus day 4 for MCT and LCT respectively We wouldconsider an effect of MCT on time to NK to be likely due tothe demonstrable effect on ketogenesis and ketonaemiaresulting from MCT ingestion [29ndash31] It must also be notedthat this is likely to be a ldquotruerdquo effect that we observed as theparticipantsrsquo BOHB levels were tested when fasted in themorning and so increased BOHB cannot be solely explainedby transient ketonaemia resulting from MCT ingestion )iseffect is further indicated by the increased magnitude of thedifference in BOHB between MCT and LCT groups over thestudy course Studies with larger numbers of participants willbe required to test this hypothesis adequately
Symptoms initially worsened in response to both dietinterventions but these were ameliorated by day four forMCT and day five for LCT At this time point mean BOHBlevels were 08 and 09mmolmiddotLminus1 respectively )is resultmight suggest that the definition for NK of le05mmolmiddotLminus1 assuggested by Volek and Phinney [49] and previously used asa threshold for ketosis [15] is not sufficient as a functionalmeasure for ketosis We also considered that a higher entrypoint to NK could be 07mmolmiddotLminus1 based on the average ofthe BOHB readings on the day at which symptom scores hadreturned to baseline and the preceding day as the ques-tionnaire evaluated symptoms for the previous 24 hoursWith this hypothetical higher threshold for NK achieve-ment of NK was greater in the MCTgroup for the first threedays but this result was also not significant nor was theachievement of NK appreciably different after this time
Further exploration to define NK more appropriately tofunctional outcomes and to determine evidence-basedthresholds is warranted
Symptoms were reduced in the MCT group relative toLCT A possibly beneficial clinical effect was exhibited onsymptoms by MCTapplication across almost all time pointsand mean symptom scores returned to baseline a day earlierwith MCT supplementation While the effect of MCT whenBOHB levels were used as a predictor of symptoms wasunclear the large inverse correlation between BOHB andsymptoms in theMCTgroup not observed for LCT suggeststhat the increase in BOHB resulting from MCT supple-mentation results in improved symptoms of keto-induction)is result further suggests that there might be a thresholdlevel of BOHB required to mitigate some of the symptomsassociated with keto-induction and that the higher BOHBexhibited in the MCT group may have caused this reduc-tion in symptoms )is is a result that warrants furtherexploration Relative to the MCT group the LCT groupreported factor increases of 05 (p 001) 20 (p 001)17 (p 00004) and 23 (p 00004) for concentrationdifficulties muscle cramps intestinal bloating and con-stipation respectively Relative to LCT there was a 17 factorincrease in the incidence of abdominal pain with MCT(p 0003) )ere are known gastrointestinal effects fromingestion of MCTs [41] and in the amounts provided toparticipants it is possible that symptoms noted with a higherincidence in the MCT group especially diarrhoea andstomach pain resulted from the use of MCTs Abdominalpain halitosis and diarrhoea were in fact the most com-monly observed effects in the MCT group with only ab-dominal pain as noted reaching significance and halitosis(ldquoketone breathrdquo) observed similarly in both groups Reduceddosages of MCTs warrant further study to determine dose-dependent effects on symptoms and mood relative to control
Mood scores correlated with symptom scores but effectsof MCT on mood state were unclear Interestingly moodscores were typically more positive in MCT whereas im-provement from baseline was greater with LCTcompared toMCT Day-by-day improvements in mood were similarbetween MCT and LCT with some benefit from MCTsupplementation observed on several days (Table 2) It isunlikely that MCT would worsen mood independentlyexcept if resultant adverse effects (such as the stomach painnoted above) was sufficient to depress mood When BOHBwas considered as a predictor variable for mood there wasa likely beneficial effect from MCT supplementation
)ere were several limitations to this study Differencesin compliance may have resulted from the free-living natureof this study We did not adjust for exercise and activityalthough participants were advised to not change theircurrent exercise habits Standardised diets (both for maleand female) were provided per age- and gender-adjustedaverage requirements )us those participants that weremore active may have exhibited differing results for BOHBsymptoms and mood Additionally some participants ex-perienced occasional difficulty taking readings with theketometerglucometer resulting in several missed readingswhich could have influenced results
2
18
16
14
12
1
08
06
04
02
0
BOH
B
POMS-TMDSndash8 ndash6 ndash4 ndash2 0 2 4 6 8 10 12 14
MCTLCT
Figure 5 Mean BOHB compared to mean POMS-TMDS
Journal of Nutrition and Metabolism 7
Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Because of the preliminary and exploratory nature ofthis study we conducted many comparisons and hy-pothesis tests We recognise the potential for multiplicityA total of 114 pairwise comparisons were made with 28results or 25 reaching clinical significance Since it isexpected by chance that 5 of tests are expected to be falsepositives (or 6 results) our trial shows a clear excess ofpositive results over the number expected if chance werethe only explanation for them While it is not possible todistinguish which differences are true positives or nega-tives an excess of observed over expected suggests some ofthe significant differences are true Similarly in correla-tions 3 of 5 results were significant We also note thatmagnitude-based inferences are not based on p values andthus patterns of statistical significance with particularmeasures makes type-1 error less likely
Furthermore the numbers allocated to this study werelimited by budgetary constraints due to its exploratorynature and this is likely to have reduced the statistical powerof our results We conducted a retrospective power calcu-lation )e primary outcome of interest was the incidence ofnutritional ketosis )e true proportion who achieved NK atseven days was 90 in the MCTgroup and 70 in the LCTgroup therefore this study would have had 25 power todetect a significant difference in these proportions (alphalevel 5) assuming the data conforms to a chi-squaredistribution It is not surprising that we did not see a sta-tistically significant difference between the two groups in thesurvival analysis )e chance of a false-negative result underthese circumstances would be 75 We consider that despitethe relatively small numbers in the cohort the findings are ofconsiderable interest to both the scientific and lay com-munity as there has been little direct research on keto-induction and ldquoketo-flurdquo specifically We also recognisethe limitations of our convenience sample arising from thesnowball method of recruitment via our networks on a first-come basis as this led to an almost entirely female cohort
5 Conclusion
MCTsupplementation improves BOHB levels relative to anLCT control and has a possible clinical application toreduce symptoms of keto-induction It is unclear at thistime whether MCTs significantly improve time to NK andmood but the large inverse correlation between BOHB andmood disturbance scores and the observed correlationbetween symptoms and mood suggest that in the context ofa VLCKD MCTsupplementation may also improve moodDue to the exploratory nature of this study large variationsbetween individual responses made many results unclearespecially concerning time to NK
More research with larger sample sizes is needed in thisarea to elucidate the role of MCTs in a classic ketogenic dietmore completely and to understand the variability betweenindividuals in their responses to ketogenic diets
Data Availability
Data are available upon request
Conflicts of Interest
)e authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
)e authors are grateful to the participants in this studyand to Amtrade NZ Limited and Mark Story who suppliedMCT oil for our use )e authors acknowledge the supportof our colleagues at the Human Potential Centre AUTUniversity and especially Caryn Zinn Simon)ornley andEric Helms who have provided advice for the directionand publication of our research All funding was providedby the Human Potential Centre of AUT University
References
[1] F Lefevre and N Aronson ldquoKetogenic diet for the treatmentof refractory epilepsy in children a systematic review ofefficacyrdquo Pediatrics vol 105 no 4 p e46 2000
[2] D L Keene ldquoA systematic review of the use of the ketogenicdiet in childhood epilepsyrdquo Pediatric Neurology vol 35 no 1pp 1ndash5 2006
[3] R G Levy P N Cooper P Giri and J Pulman KetogenicDiet and Other Dietary Treatments for Epilepsy )e CochraneLibrary London UK 2012
[4] C B Henderson F M Filloux S C Alder J L Lyon andD A Caplin ldquoEfficacy of the ketogenic diet as a treatmentoption for epilepsy meta-analysisrdquo Journal of Child Neu-rology vol 21 no 3 pp 193ndash198 2006
[5] E G Neal H Chaffe R H Schwartz et al ldquo)e ketogenic dietfor the treatment of childhood epilepsy a randomised con-trolled trialrdquo Lancet Neurology vol 7 no 6 pp 500ndash5062008
[6] A Paoli A Rubini J Volek and K Grimaldi ldquoBeyond weightloss a review of the therapeutic uses of very-low-carbohydrate(ketogenic) dietsrdquo European Journal of Clinical Nutritionvol 67 no 8 pp 789ndash796 2013
[7] P Sumithran and J Proietto ldquoKetogenic diets for weight lossa review of their principles safety and efficacyrdquo ObesityResearch and Clinical Practice vol 2 no 1 pp 1ndash13 2008
[8] M Maalouf J M Rho and M P Mattson ldquo)e neuro-protective properties of calorie restriction the ketogenic dietand ketone bodiesrdquo Brain Research Reviews vol 59 no 2pp 293ndash315 2009
[9] K Castro L S Faccioli D Baronio C Gottfried I S Perryand R dos Santos Riesgo ldquoEffect of a ketogenic diet on autismspectrum disorder a systematic reviewrdquo Research in AutismSpectrum Disorders vol 20 pp 31ndash38 2015
[10] K Varshneya C Carico A Ortega and C G Patil ldquo)eefficacy of ketogenic diet and associated hypoglycemia as anadjuvant therapy for high-grade gliomas a review of theliteraturerdquo Cureus vol 7 no 2 p e251 2015
[11] D Kulak and A J Polotsky ldquoShould the ketogenic diet beconsidered for enhancing fertilityrdquo Maturitas vol 74 no 1pp 10ndash13 2013
[12] H A Krebs ldquo)e regulation of the release of ketone bodies bythe liverrdquoAdvances in Enzyme Regulation vol 4 pp 339ndash3531966
[13] G F Cahill Jr ldquoFuel metabolism in starvationrdquo AnnualReview of Nutrition vol 26 no 1 pp 1ndash22 2006
8 Journal of Nutrition and Metabolism
[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

[14] A Gibson R Seimon C Lee et al ldquoDo ketogenic diets reallysuppress appetite A systematic review and meta-analysisrdquoObesity Reviews vol 16 no 1 pp 64ndash76 2015
[15] B Guerci M Benichou M Floriot et al ldquoAccuracy ofan electrochemical sensor for measuring capillary bloodketones by fingerstick samples during metabolic deteriorationafter continuous subcutaneous insulin infusion interruptionin type 1 diabetic patientsrdquo Diabetes Care vol 26 no 4pp 1137ndash1141 2003
[16] A L Hartman and E P Vining ldquoClinical aspects of theketogenic dietrdquo Epilepsia vol 48 no 1 pp 31ndash42 2007
[17] W S Yancy Jr M K Olsen J R Guyton R P Bakst andE C Westman ldquoA low-carbohydrate ketogenic diet versusa low-fat diet to treat obesity and hyperlipidemia a ran-domized controlled trialrdquo Annals of Internal Medicinevol 140 no 10 pp 769ndash777 2004
[18] G J Hamwi M C Mitchell R G Wieland F A Kruger andS S Schachner ldquoSodium and potassium metabolism duringstarvationrdquo American Journal of Clinical Nutrition vol 20no 8 pp 897ndash902 1967
[19] R A DeFronzo M Goldberg and Z S AGus ldquo)e effectsof glucose and insulin on renal electrolyte transportrdquo Journalof Clinical Investigation vol 58 no 1 p 83 1976
[20] R A DeFronzo ldquo)e effect of insulin on renal sodiummetabolismrdquo Diabetologia vol 21 no 3 pp 165ndash1711981
[21] S Tiwari S Riazi and C A Ecelbarger ldquoInsulinrsquos impact onrenal sodium transport and blood pressure in health obesityand diabetesrdquo American Journal of Physiology Renal Physi-ology vol 293 no 4 pp F974ndashF984 2007
[22] M P Harber S Schenk A L Barkan and J F HorowitzldquoAlterations in carbohydrate metabolism in response to short-term dietary carbohydrate restrictionrdquo American Journal ofPhysiology-Endocrinology vol 289 no 2 pp E306ndashE3122005
[23] H C Kang D E Chung D W Kim and H D Kim ldquoEarly-and late-onset complications of the ketogenic diet for intrac-table epilepsyrdquo Epilepsia vol 45 no 9 pp 1116ndash1123 2004
[24] H Chul Kang Y Joo Kim D Wook Kim and H Dong KimldquoEfficacy and safety of the ketogenic diet for intractablechildhood epilepsy Korean multicentric experiencerdquo Epi-lepsia vol 46 no 2 pp 272ndash279 2005
[25] S Livingstone ldquoComprehensive management of epilepsy ininfancy childhood and adolescencerdquo Archives of Disease inChildhood vol 47 no 255 p 842 1972
[26] S Livingston L L Pauli and I Pruce ldquoKetogenic diet intreatment of childhood epilepsyrdquo Developmental Medicineand Child Neurology vol 19 no 6 pp 833-834 1977
[27] P Huttenlocher AWilbourn and J Signore ldquoMedium-chaintriglycerides as a therapy for intractable childhood epilepsyrdquoNeurology vol 21 no 11 p 1097 1971
[28] P R Huttenlocher ldquoKetonemia and seizures metabolic andanticonvulsant effects of two ketogenic diets in childhoodepilepsyrdquo Pediatric Research vol 10 no 5 pp 536ndash540 1976
[29] A Bach H Schirardin A Weryha and M Bauer ldquoKetogenicresponse to medium-chain triglyceride load in the ratrdquoJournal of Nutrition vol 107 no 10 pp 1863ndash1870 1977
[30] Y Y Yeh and P Zee ldquoRelation of ketosis to metabolic changesinduced by acute medium-chain triglyceride feeding in ratsrdquoJournal of Nutrition vol 106 no 1 pp 58ndash67 1976
[31] M-P St-Onge R Ross W D Parsons and P J H JonesldquoMedium-chain triglycerides increase energy expenditure anddecrease adiposity in overweight menrdquo Obesity Researchvol 11 no 3 pp 395ndash402 2003
[32] L Sann P Divry Y Lasne and A Ruitton ldquoEffect of oral lipidadministration on glucose homeostasis in small-for-gestational-age infantsrdquo Acta Paediatrica Scandinavicavol 71 no 6 pp 923ndash927 1982
[33] P Y Wu J Edmond N Auestad S Rambathla J Bensonand T Picone ldquoMedium-chain triglycerides in infant for-mulas and their relation to plasma ketone body concentra-tionsrdquo Pediatric Research vol 20 no 4 pp 338ndash341 1986
[34] T B Seaton S L Welle M K Warenko and R G Campbellldquo)ermic effect of medium-chain and long-chain triglyceridesin manrdquo American Journal of Clinical Nutrition vol 44 no 5pp 630ndash634 1986
[35] J Decombaz M J Arnaud H Milon et al ldquoEnergy meta-bolism of medium-chain triglycerides versus carbohydratesduring exerciserdquo European Journal of Applied Physiology andOccupational Physiology vol 52 no 1 pp 9ndash14 1983
[36] M Krotkiewski ldquoValue of VLCD supplementation withmedium chain triglyceridesrdquo International Journal of Obesityvol 25 no 9 pp 1393ndash1400 2001
[37] R M Schwartz S Boyes and A Aynsley-Green ldquoMetaboliceffects of three ketogenic diets in the treatment of severeepilepsyrdquo Developmental Medicine and Child Neurologyvol 31 no 2 pp 152ndash160 1989
[38] E G Neal H Chaffe R H Schwartz et al ldquoA randomizedtrial of classical and medium-chain triglyceride ketogenicdiets in the treatment of childhood epilepsyrdquo Epilepsiavol 50 no 5 pp 1109ndash1117 2009
[39] B Campbell R B Kreider T Ziegenfuss et al ldquoInternationalSociety of Sports Nutrition position stand protein andexerciserdquo Journal of the International Society of SportsNutrition vol 4 no 1 p 8 2007
[40] K A Traul A Driedger D L Ingle and D Nakhasi ldquoReviewof the toxicologic properties of medium-chain triglyceridesrdquoFood and Chemical Toxicology vol 38 no 1 pp 79ndash98 2000
[41] J L Ivy D L Costill W J Fink and E Maglischo ldquoCon-tribution of medium and long chain triglyceride intake toenergy metabolism during prolonged exerciserdquo InternationalJournal of Sports Medicine vol 1 no 1 pp 15ndash20 1980
[42] D McNair M Lorr and L Droppleman Profile of MoodStates Manual Edits Educational and Industrial TestingService San Diego CA USA 1992
[43] W G Hopkins ldquoSpreadsheets for analysis of controlled trialswith adjustment for a subject characteristicrdquo Sportsciencevol 10 pp 46ndash50 2006
[44] S L Curran M A Andrykowski and J L Studts ldquoShort Formof the Profile of Mood States (POMS-SF) psychometric in-formationrdquo Psychological Assessment vol 7 no 1 pp 80ndash831995
[45] W G Hopkins ldquoHow to interpret changes in an athleticperformance testrdquo Sportscience vol 8 p 7 2004
[46] J T Rich J G Neely R C Paniello C C J VoelkerB Nussenbaum and E W Wang ldquoA practical guide tounderstanding Kaplan-Meier curvesrdquo Otolaryngology vol 143no 3 pp 331ndash336 2010
[47] W Hopkins New View of Statistics Effect Magnitudes 2002httpswwwsportsciorgresourcestatseffectmaghtml
[48] F E Harrell Jr Regression Modeling Strategies with Appli-cations to Linear Models Logistic and Ordinal Regression andSurvival Analysis Springer Berlin Germany 2015
[49] J S Volek and S D Phinney e Art and Science of LowCarbohydrate Living Beyond Obesity New York USA Be-yond Obesity 2013
Journal of Nutrition and Metabolism 9
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom









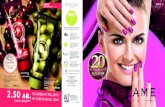



![Nutritional Ketosis Condition and Specific Ketogenic Diet ... · Ketosis can be induced when a ketogenic diet is followed for more than 3 days. This induced nutritional ketosis [23].](https://static.fdocuments.in/doc/165x107/5fc6fb73d71b24630f77a027/nutritional-ketosis-condition-and-specific-ketogenic-diet-ketosis-can-be-induced.jpg)