
The therapist’s responsibility: a systemic approach to...
20
Joumul of Family Therapy (1983) 5: 199 218 The therapist’s responsibility: a systemic approach to mobilizing family creativity Hugh Jenkins* and Michael Donnellyt Three techniques, sculpting, geneograms, and family drawing are considered within a systemic approach to therapy. Frequently, emphasis is laid on either the activity of the therapist or the behaviour of the family in treatment. We focus on ways in which the therapist draws on the clients’ creativity, relying fo this on a correct assessment of their ‘language’ or ‘idiom’. Certain assumptions are proposed, and case illustrations are used in their support. Our approach is that any material, or apparently no material, produced when using these techniques represents essential information which can be turned to therapeutic advantage by means of positive reframing. Although a framework within which to practise is viewed as essential, a ‘game-plan’ will almost certainly result in sterility and impasses in therapy. Therapist flexibility, it is proposed, is a prerequisite for creativity. We prefer to label resistance to treatment as failure by the therapist to recognize the clients’ needs. Introduction In a radio dramatization of War and Peace, one of the characters re- flected: ‘I am beginning to realize the total impossibility of changing another’s convictions with words.’$ This paper deals with some alter- natives to words as the main vehicle in psychotherapeutic treatment. Psychotherapy is, among other things, to do with language, and the attempts to reconcile the language of treatment with the language of distress.Impassesin therapy may result from the therap& failing to recognize the language or idiom of the client. And just as people in distress Received 14 July 1981; revised version received 8 June 1982. * Department of Children, Maudsley Hospital, Denmark Hill, London SE3 8AZ. t Gloucester House, Southmead Hospital, Bristol, BSlO 5NB. $ B.B.C. Radio 4, 15 July 1978. (Formerlyat The Young People’s Unit, Velindre Road, Cardiff, CF4 7JG.) 199 0163-4445/83/030199 +20$03.00/0 0 1983 The Association for Family Therapy
Transcript of The therapist’s responsibility: a systemic approach to...

Joumul of Family Therapy (1983) 5: 199 218
The therapist’s responsibility: a systemic approach to mobilizing family creativity
Hugh Jenkins* and Michael Donnellyt
Three techniques, sculpting, geneograms, and family drawing are considered within a systemic approach to therapy. Frequently, emphasis is laid on either the activity of the therapist or the behaviour of the family in treatment. We focus on ways in which the therapist draws on the clients’ creativity, relying for this on a correct assessment of their ‘language’ or ‘idiom’. Certain assumptions are proposed, and case illustrations are used in their support. Our approach is that any material, or apparently no material, produced when using these techniques represents essential information which can be turned to therapeutic advantage by means of positive reframing. Although a framework within which to practise is viewed as essential, a ‘game-plan’ will almost certainly result in sterility and impasses in therapy. Therapist flexibility, it is proposed, is a prerequisite for creativity. We prefer to label resistance to treatment as failure by the therapist to recognize the clients’ needs.
Introduction
In a radio dramatization of War and Peace, one of the characters re- flected: ‘I am beginning to realize the total impossibility of changing another’s convictions with words.’$ This paper deals with some alter- natives to words as the main vehicle in psychotherapeutic treatment.
Psychotherapy is, among other things, to do with language, and the attempts to reconcile the language of treatment with the language of distress. Impasses in therapy may result from the therap& failing to recognize the language or idiom of the client. And just as people in distress
Received 14 July 1981; revised version received 8 June 1982. * Department of Children, Maudsley Hospital, Denmark Hill, London SE3 8AZ.
t Gloucester House, Southmead Hospital, Bristol, BSlO 5NB. $ B.B.C. Radio 4, 15 July 1978.
(Formerly at The Young People’s Unit, Velindre Road, Cardiff, CF4 7JG.)
199 0163-4445/83/030199 +20$03.00/0 0 1983 The Association for Family Therapy
200 H. Jenkins and M . Donnelly
may resort to time-honoured but unsuccessful solutions to their problems, so too therapy can founder because only a limited range of time-honoured therapeutic alternatives are employed. The therapist needs to be able to offer the family in treatment a wider range of responses to familiar problems. It is this act of creative encounter, this ‘bringing into being’ (May, 1972) whether through sculpting, geneograms or family drawing that can activate the potential in families to explore, share, and change. The importance of ‘encounter’ (May, 1972) especially in relation to material generated by the family itself should not be underestimated, and is the primary focus of this paper.
Misunderstandings in human relationships can arise out of a failure by the parties concerned to respond to the salient component of the message. The girl who weakly resists the amorous advances of her admirer may well be disappointed when he desists. His response would be to the verbal, digital component of the message, and not to the more ambiguous analogic paramessages (Grinder and Bandler, 1976) of the submissive eye- closing and unassertive tone of voice in which the verbal injunction ‘No’ is given. At times, it may only be possible to communicate allegorically or analogically that which would be unacceptable if stated explicitly, as Freud (1 922) recognized in his pioneeringwork on the meaning of dreams.
Our focus is to consider ways of directing the attention of families to the products of their own creativity, so that learning takes place both at inter- personal and individual levels, and that in either case, learning is systems oriented. The techniques described do not rely for their impact on the spoken word, in the belief that words can be a barrier to, just as much as a vehicle for clear communication. However, any attempt to communicate via one ‘language’ a process which relies for its impact on another, can only approximate to the reality as experienced in the moment. When as here, the focus is on action techniques, the discrepancy will be considerable. Any attempt to confuse, the two ‘languages’, digital and analogic would result in a confusion of conceptual levels (Watzlawick et al., 1967), running counter to the physiological reality of our two brains (Watzlawick, 1978) and the two modes of communication that they repre- sent.
Some observers have labelled as resistant to treatment those patients who do not improve within the framework of the therapy offered (Davis and Oskerson, 1978). Others have commented in psychoanalytic terms on non-verbal techniques used to detour defences and to find ways around the rituals and habitual responses of the family (Wadeson, 1980; Kwiatkowska, 1971) but this differs from proposing that one of the responsibilities for therapists is to ‘focus on mobilizing the great supportive
Mobilizing family creativity 201
and therapeutic potential of the family itself (Skynner, 1976). In order to achieve this goal, the therapist must be able to discern ways in which verbal communications can be modified, amplified, or disqualified, by non-verbal or paraverbal communicational sequences (Breunlin, 1979; Scheflen, 1972; Grinder and Bandler, 1976). ‘At any point in anyrelation- ship, or set of relationships, touch, proximity, posture, gesture, facial expression, eye movements, direction of gaze, all play a central part in a communication gestalt that continuously influences, maintains and regulates interactional processes’ (Cade, 1975). The therapist can mobilize this knowledge in his use of interventions while remainingwary of being so seduced by technique that the family’s needs are ignored (Bodin and Ferber, 1972). Techniques are means to ends (Dale, 1981), to be used as integral adjuncts to the process and aims of treatment.
Focus of paper
We propose that there are in therapy two primary, although comple- mentary modes of activity. Both are present in any piece of therapeutic behaviour, although one will always predominate. They are identified as (l), therapist-oriented activities, and (2), client-oriented activities.
(1) Therapist-oriented activities may be seen to have two components, being(i) where the therapist personally engages in bringing about changes as a direct result of his interventions and his creativity, where he is pri- marily a choreographer, not a participant (Minuchin, 1974; Street and Treacher, 1980); and being (ii) where the therapist actively engages himself through techniques such as coaching, doubling, rble reversal, or even to the extent of enacting the part of a family member who may not be physically present in the session. In (ii), the therapist becomes more overtly a participant in the family scenario that he is attempting to change. Both components draw explicitly on the therapist’s own creativity and resources. Not only does the therapist initiate, but he remains central in focusing attention on the family, or on some part of it.
(2) Client-oriented activities differ in emphasis. The therapist as catalyst emphasizes family members’ inherent ability to initiate the thera- peutic material, drawing on their own creativity and resources, producing their own shared material from which they work, being guided by the therapist who is accordingly less central. The therapist’s creativity lies in calling on the potentials dormant in the family, commenting on or re- framing what they have manifestly produced.
This paper focuses on those activities that we have identified as primarily client-oriented. When the family is actively involved in the pro-
202 H . Jenkins and M . Donnelly
cess of treatment and senses an investment in its success or failure, it more readily works towards successful outcome (Haley, 1980). In those families where engagement appears particularly difficult, the attempt to place more emphasis on client-oriented activities may result in greater commit- ment by the family, since these activities tend to be more concrete, relying less for their impact on sophisticated intellectual processes. The three activities discussed are sculpting, geneograms, and family drawing. This is a conservative list, with many alternatives (Satir, 1972) open to the creative therapist. Whichever techniques are chosen, they need to be ‘with the whole family system and the overall goal for the system in mind, either to clarify the nature of the system, or to produce change in it’ (Schaverien, 1978).
Assumptions
Certain assumptions about the systemic use of client-oriented techniques underpin our thinking in this context, which we see as assisting treatment. They are; systems advantages, therapist advantages, and family advan- tages. These are summarized in the following way.
Systems advantages (i) Learning is systems-oriented, for family and therapist;
(ii) an action orientation allows family and therapist to ‘see how it is’; (iii) the process of task enactment highlights system functions; (iv) system ‘rules’ are more easily broken.
Therapist advantages ( i ) The therapist mobilizes family resources and more readily stimu-
lates motivation; (ii) any response, including an apparently nil response, provides material for therapeutic intervention.
Family advantages (i) Events and attitudes can be experienced and shared simultaneously;
(ii) any family member may well have been permitted to complete his statement for the first time; (iii) family members have an opportunity to experience other members’ views of reality, possibly also for the first time.
This analysis of advantages primarily serves the purpose of identifying different facets of a composite whole. Such divisions as do exist are con- ceptual abstractions whose aim is to help clarify the components of thera- peutic activity, and not to attempt a process of reification. The remainder

Mobilizing family creativity 203
of this paper aims to demonstrate the uses and complementary nature of sculpting, geneograms, and family drawing in the light of these assumptions.
Family sculpting
Family therapy borrows freely from many sources, one being psycho- drama. We learn from psychodrama the importance of warming up to a new situation. Unless the individual or family is able to experience the familiar in a new light, there will be little chance of change, for therapy involves the introduction of flexibility into people’s problem-solving patterns. ‘In systems terms, what commonly happens is that a family breaks a rule of its own system . . . while in a state of spontaneity’ (Schaverien, 1978). In family sculpting, the space between people and their physical postures become a part of the statement about relation- ships. Physical changes can then be used to represent visible shifts in relationships (Duhl et al., 1973; Walrond-Skinner, 1976) with be- havioural change capable of being carried over into the daily life of the family as the aim of such interventions. Interpersonal communication becomes more direct, and new opportunities for solving interpersonal conflicts are opened up (Papp et al., 1973). A statement about relation- ships and feelings, previously only partially perceived, through sculpting, or ‘spatialization’ Uefferson, 1978) can have great impact. It allows all members of a family to participate as sculptors in a manner appropriate to their age. The very young can be included in the sculpts of others; it may be significant who holds the baby, and young children can be engaged by such questions as: ‘Where would you like to sit for a good cuddle?’ or ‘Where do you go if you are unhappy?’ The issue is never about ‘right’ or ‘wrong’, but about how each member sees family relationships at that time. Individual statements cannot be denied, and however painful or difficult the tableau that emerges, family members must needs experience their own part in the overall whole.
All sculpts provide potential therapeutic material, and there is a sense in which a sculpt cannot fail. An apparently nil response will provide material, although all responses will also be influenced by the degree to which the therapist is comfortable with the medium:
. . . therapists to whom spatialization is a familiar tool realise that apparent failure may not be failure at all; sometimes use of a technique that produces no apparent response is, in fact, a significant part of a ‘softening up’ process. New insights are not always easy for clients to adopt; old ‘defences’ do not necessarily melt away at the first assault Uefferson, 1978).
204 H . Jenkins and M . Donnelly
The following illustrations from treatment demonstrate some of these points.
Case illustration l
Experience with the ‘P,’ family provides an example of a family sculpt where at the time much remained unresolved, (Jefferson, 1978). The part of the family in treatment by a co-therapy team were, father, mother, and the youngest of six children, Hilary, a girl in her mid-teens. She had been referred initially because of non-attendance at school to a child guidance setting, where one of the authors, H. J . , worked for one session a week. She spent most of her time on her own, rarely going out or mixing with people beyond her immediate family. When she did venture out, i t was invariably with another family member, and most frequently with her mother. During the third session the therapists felt that they were struggling. As words continued to fail, the family were asked to sculpt their current situation in turn, in order to help both them and the therapists, who con- fessed to feeling stuck. Mother’s view, and then father’s view were sculpted. In father’s sculpt, the three members were placed in three corners, as far away from each other as possible. Again the therapists felt stuck. Where now? There was no possibility of physical contact, nor of direct communication. Hilary was asked where she thought members would be in five years’ time. She thought she would be involved in more outside activities, and that by then her mother would have the interest of more grandchildren. She and her mother were then placed facing towards the outside of the group, signifying different and wider interests. She was asked where her father would be. She would not say or commit herself to anything at all. Her father was left in limbo. In fact, at the time he was unemployed, diabetic, and it seemed, an emotionally peripheral figure.
New themes were raised for the family and therapists, some of which were not tackled at that point. But new dimensions of father/daughter conflict and diffi- culties which seemed to mirror some of the marital dilemmas were brought forcibly into the session and the subsequent treatment in a way that hours of talking might have failed to achieve. Subsequently Hilary became a day-patient and finally, in order to deal more forcibly with separation and independence issues, she became an in-patient in an adolescent unit for a short while. The turning point for her appeared to be when she was helped in the active realization that she did not have to be responsible for the lack of emotional involvement between her parents, but had a separate life to lead. She left the unit no longer the phobic person when first seen in out-patient treatment. A card received from her eight months after discharge while she was involved in a Youth Opportunities Programme finished: ’Thanks for helping me to be able to go out and about again without a second thought about going. I don’t know where I would be without (everybody’s) help.’ She now has a permanent job, and other news indicates that her parents too are less ‘phobic’ about each other, and that all concerned have been freed in some degree from the frozen isolation of the initial sculpt. That
Mobilizing family creativity 205
sculpt allowed family members to make explicit their relationships that had long remained covert, including a family ‘rule’ that no one should acknowledge the fact. Hilary’s anger towards her father (on behalf of her mother?), was then visible, and from a now clear position of mutual isolation it became easier for the therapists to plan strategies that could deal with this.
Case illustration 2 Material of a different order arose from a sculpt with the ‘S.’ family, who in this session were, the stepfather, the mother, and her thirteen-year-old son, Simon. The therapist, H.J., noticed how the family almost huddled together when they came to their appointments. Simon said this was how the family always was. They were asked to sculpt their family relationships. It was not the content of each person’s sculpt that highlighted a family theme, since there were large areas of agreement, but the process of the sculpting itself. Repeatedly Simon managed to take over and to rearrange the two adults so that neither of them was able to complete an individual statement. The therapist became aware that this was part of the overall family interaction pattern. At this point it was possible to intervene more effectively in the light of this information, to support the adults in their struggle to retain some authority, and to help them support each other more appropriately. Part of the process was to facilitate more disengagement between the mother and Simon, and validate the stepfather’s r61e. It also meant excluding Simon physically from parts of subsequent sessions, in the face of dire threats about what he would do to himself because he was now being treated more firmly and consistently. In this instance the manner of the family’s interaction in the sculpt was systemically more important than the individual final statements. Sculpting can help family members to see how it is for themselves, and in relation to others. As people broaden their range of experience, so they can extend the repertoire of behaviours open to them. ‘It is the rigid, repetitive sequence of a narrow range that defines pathology’ (Haley, 1976). At the same time that the repertoire of behaviours is extended, so the family’s unspoken rules that their members shall be as they always have been will be challenged. The important issue revolves around how much challenging will be useful to the family.
I t is not stress itself that needs to be analyzed, but the degree of stress any parti- cular system can accommodate in order to thrive. Stress is a given and serves as a propeller in moving a system into action. In the old homeostatic model, stress is seen as deviant . . . something for the system to fend off. In a morphogenic systems model, stress is seen as an important variable for moving a system into action (Freeman, 1976).
Provided the therapist ensures that the family’s threshold to stress is not exceeded, he will be harnessing a force for change that originates within the family.
206 H. Jenkins and M . Donnelly
Family sculpting techniques have broader applications than those of the immediate treatment setting. Our contention is that the same tech- niques can be used in training professionals to better understand their own professional helping networks (Jenkins, 1977), and to understand the ‘reality’ of a family’s needs by recreating their scenario and the influencing factors of the therapist’s inputs in academic training settings (Simmonds and Brummer, 1980). Although considerable space has been devoted to the creative potential of family sculpting, many of the general themes raised apply equally to the use of geneograms and family drawing.
Family geneograms
In the same way that a family sculpting experience provides new informa- tion about family relationships, and new perspectives on old information, so too the judicious use of geneograms (Lieberman, 1979a, b ) may provide a context marker when working with clients individually, or with the whole family group present. Work with ‘individuals’ is wholly consistent in family therapy practice when this is viewed as an orientation for treatment (Haley, 1976). Just as absent members can be brought into a family by other members taking their part or by using chairs to represent them in a sculpt, so too the geneogram can powerfully bring absent members and past generations into the current therapeutic process. We might categorize these two techniques as predominantly three-dimensional (sculpting) and predominantly longitudinal (geneograms), while sharing the common aims of identifying family structure, of finding out who is important, of tuning into repetitive family themes or transgenerational scenarios, and of introducing alternative ways of perceiving and behaving for the participants.
Families transmit ritual themes or scripts from generation to generation (Palazzoli et al., 1977) and have ways of knowing about past and current events while not knowing clearly how this is so (Byng-Hall, 1973). Family members are often unclear about how they themselves fit into the overall picture, and what that family picture really is. In general, it is important to establish at some point a minimum network of information concerning the three generations of grandparents, parents, and children, whether it is an individual or family group which is physically present. The potential complexity of even so few people is enormous, where a system of eight people involves the possibility of fifty-six different triangular relationships (Haley, 1967). The geneogram is a useful way of gaining information which can involve all family members. It is available from session to session, when new information can be added, thereby helping to provide
Mobilizing family creativity 207
continuity to the therapeutic process. John Byng-Hall* says that he also finds it useful to bring the geneogram out as a way of re-engaging family members in a joint task when some form of unhelpful polarization has occurred during therapy.
A geneogram may be constructed early on in therapy, both to help establish baseline information, and to speed up the engagement of family members in the therapeutic process, or at a later stage when therapy has become blocked. Frequently, family discussion is sparked off, or strong feelings aroused, so that the geneogram is put on one side as the therapist helps the family deal with the particular issue. There are no set rules about how to construct a geneogram, but it helps if the therapist is consistent in using defined conventions. He must also be flexible enough to accom- modate to the structure of the family. Some of the impact of a geneogram comes from its apparent simplicity in representing relationships and events. Sometimes the material looks stark, and therapist and family may be pitched into the middle of re-awakened grief as events re-unfold in the session. At other times there is a feeling of relief for members who ‘see’ things for the first time. Whatever the response, family members will go away with material to think about independently of the use that the therapist makes of it in the session. Equally, the family may not be able to make, and the therapist not succeed in making such a medium fit for them, at which point the therapist’s creativity lies in opening up other avenues in order to elicit and use the same required information. Such was the case in the following illustration.
Case illustration 3
The family consists of John, his wife Maralyn, and the three children Marcia, sixteen, Helen, fifteen, and Martin, eleven. John was referred by his G.P. to a psychologist based in a Health Centre for individual psychotherapy. He had a history of anxiety and depression with obsessional and ritualistic features pre- dominating. He was described as ‘resistant’ to all forms of drug treatments, and had been told that his last option was to undergo a leucotomy. While an in-patient for assessment to see whether this was appropriate, he discharged himself saying he did not wish to have surgery and re-presented himself to his G.P. asking for some kind of psychotherapy.
The exact nature and extent of his obsessional symptoms had never really been determined, and some doubt had been expressed by previous clinicians as to whether he really experienced them, since no one had observed them directly. He claimed that they only happened at home, generally when he was doing domestic tasks, thereby preventing him from leaving the house.
* Workshop at the Annual Conference of the A.F.T.. Exeter 1978.
208 H. Jenkins and M . Donnelly
John was moody and irritable in the session, while Maralyn was cheerful and accepting of his elusive obsessions. He claimed that he did nothing about the house just in case he became obsessional, but would sit still all day reading, smoking, and making the occasional cup of coffee. Maralyn subtly encouraged this behaviour by always making sure that all the household tasks were done before she went to work. John had not worked for some years but stayed at home while his wife had become the breadwinner and established a social life away from the family, even going away on holiday with her colleagues without her husband. He claimed in defence of her behaviour that he did not go just in case he became obsessional and spoilt the holiday for her.
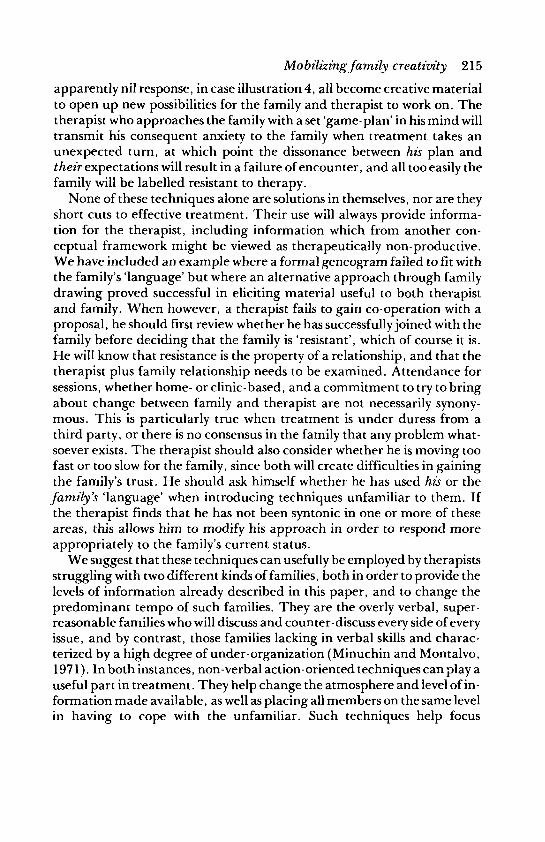
l . 2.
S ? m / M a r r ! d
(alcoholic) 1955)
I
6 l
D ,, (died at birth)
Morolyn John M. age 23
Morio Helen Martin
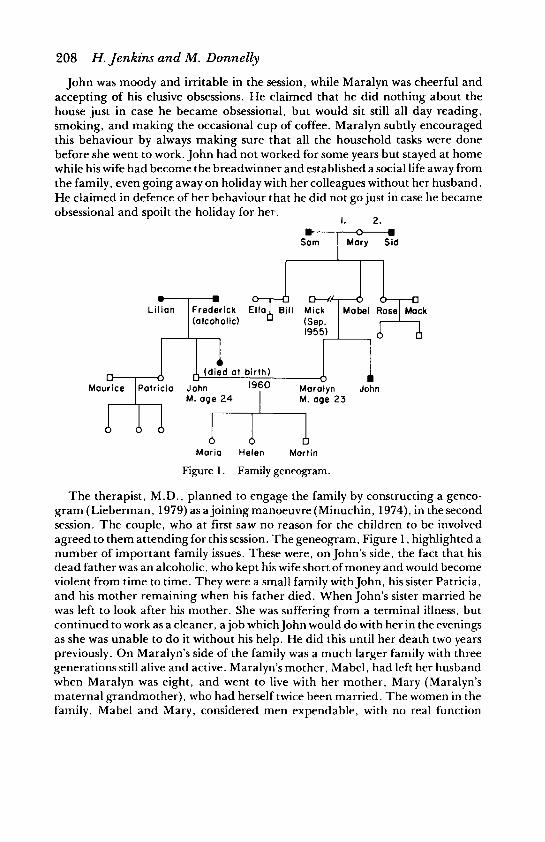
Figure 1 . Family geneogram.
The therapist, M.D., planned to engage the family by constructing a geneo- gram (Lieberman, 1979) as a joiningmanoeuvre (Minuchin, 1974), in the second session. The couple, who at first saw no reason for the children to be involved agreed to them attending for this session. The geneogram, Figure 1, highlighted a number of important family issues. These were, on John’s side, the fact that his dead father was an alcoholic, who kept his wife short of money and would become violent from time to time. They were a small family with John, his sister Patricia, and his mother remaining when his father died. When John’s sister married he was left to look after his mother. She was suffering from a terminal illness, but continued to work as a cleaner, a job which John would do with her in the evenings as she was unable to do it without his help. He did this until her death two years previously. On Maralyn’s side of the family was a much larger family with three generations still alive and active. Maralyn’s mother, Mabel, had left her husband when Maralyn was eight, and went to live with her mother, Mary (Maralyn’s maternal grandmother), who had herself twice been married. The women in the family, Mabel and Mary, considered men expendable, with no real function
Mobilizing family creativity 209
other than to earn money. There was a strong matriarchal input into this couple’s family system. John and Maralyn never went together to visit either of their families, with John especially describing difficulty in understanding her family.
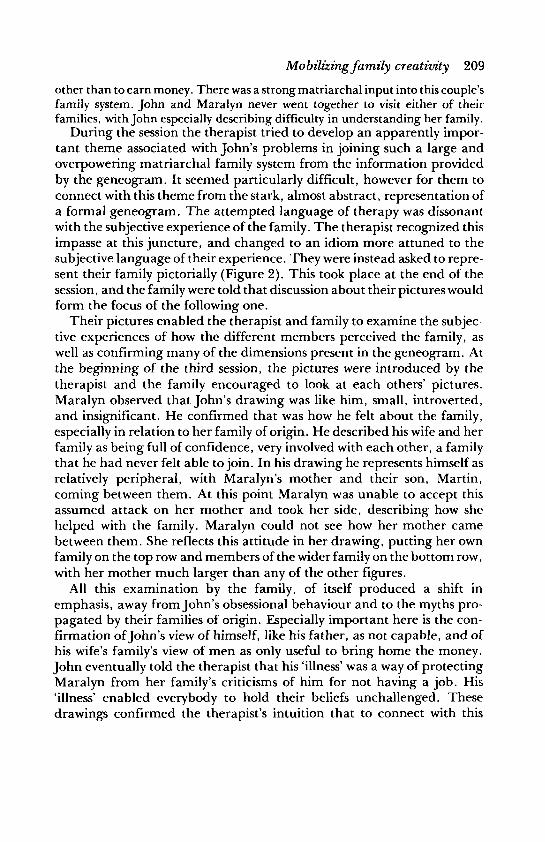
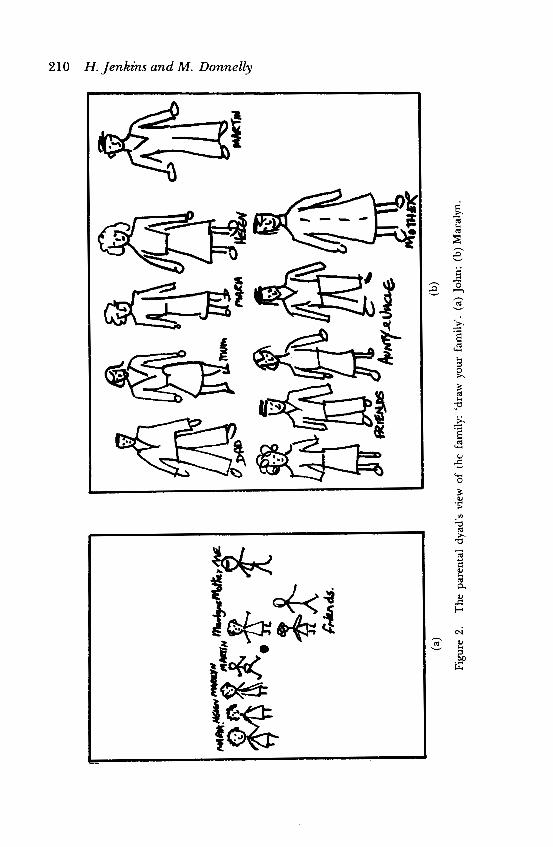
During the session the therapist tried to develop an apparently impor- tant theme associated with John’s problems in joining such a large and overpowering matriarchal family system from the information provided by the geneogram. It seemed particularly difficult, however for them to connect with this theme from the stark, almost abstract, representation of a formal geneogram. The attempted language of therapy was dissonant with the subjective experience of the family. The therapist recognized this impasse at this juncture, and changed to an idiom more attuned to the subjective language of their experience. They were instead asked to repre- sent their family pictorially (Figure 2). This took place at the end of the session, and the family were told that discussion about their pictures would form the focus of the following one.
Their pictures enabled the therapist and family to examine the subjec- tive experiences of how the different members perceived the family, as well as confirming many of the dimensions present in the geneogram. At the beginning of the third session, the pictures were introduced by the therapist and the family encouraged to look at each others’ pictures. Maralyn observed that John’s drawing was like him, small, introverted, and insignificant. He confirmed that was how he felt about the family, especially in relation to her family of origin. He described his wife and her family as being full of confidence, very involved with each other, a family that he had never felt able to join. In his drawing he represents himself as relatively peripheral, with Maralyn’s mother and their son, Martin, coming between them. At this point Maralyn was unable to accept this assumed attack on her mother and took her side, describing how she helped with the family. Maralyn could not see how her mother came between them. She reflects this attitude in her drawing, putting her own family on the top row and members of the wider family on the bottom row, with her mother much larger than any of the other figures.
All this examination by the family, of itself produced a shift in emphasis, away from John’s obsessional behaviour and to the myths pro- pagated by their families of origin. Especially important here is the con- firmation of John’s view of himself, like his father, as not capable, and of his wife’s family’s view of men as only useful to bring home the money. John eventually told the therapist that his ‘illness’ was a way of protecting Maralyn from her family’s criticisms of him for not having a job. His ‘illness’ enabled everybody to hold their beliefs unchallenged. These drawings confirmed the therapist’s intuition that to connect with this
210 H. Jenkins and M . Donnelly
h e
h
v
Mobilizing family creativity 21 1
family’s reality, a ‘language’ of a different order was necessary. It could well have been a family sculpt, but in this instance, the drawing seemed to operate in the space between a formal geneogram and such a possible concrete non-verbal enactment.
Family drawing
The use of drawing and pictorial representation has a well-established r6le within other therapeutic modes, and has great potential for family work, but is largely undeveloped in the U.K. so far. One of the main areas of development has been in ways of engaging children in the therapeutic pro- cess (Guttman, 1975; Muller, 1966; Kwiatkowska, 1971), while other practitioners have developed techniques for use with couples (Kwiat- kowska, 1967; Bing, 1970) and with couples’ groups (Wadeson, 1980). Some have placed an emphasis on the diagnostic nature of the drawing process in revealing either ‘core problems’ (Sherr and Hicks, 1973), or in establishing an evaluation of the family (Kwiatkowska, 1971; Muller, 1966; Zierer et al., 1966). Some work has been undertaken with multi- family therapy (Wadeson, 1976), where two or three families are seen at the same time. There is also an interesting description of the use of art with respect to families being seen within a Multiple Impact Therapy frame- work (Kraft and Austin, 1966). In a different context, Feinstein (1981) uses historical drawing as part of a family reconstruction process.
As a general rule, art therapists have adapted their existing skills and heritage to fit within the theoretical orientations and practical methods used in the particular agencies where they work. This has produced a ten- dency for therapists to develop particular skills to meet individual needs, while having no overall theoretical philosophy emerging with respect to art and family therapy that would justify its use as a separate therapeutic modality. Within a systems theory approach, family drawing serves the same purpose as other action techniques. That is, it is aimed at the whole family system, either to clarify the nature of the system, or to produce change in it.
Case illustration 4
Family drawing with the ‘ H family illustrates some of the ways that drawing within a systems approach can be used in therapy. Mr and Mrs H. were married in 1950, and had two children, Valerie aged twenty-seven, and Kevin, aged seventeen. At the time the family came into treatment, Valerie had married and moved a considerable distance from her family of origin, and was not included in the family sessions. The reason the family were in therapy was that Kevin had to
212 H. Jenkins and M . Donnelly be placed on probation on the condition that he receive some form of psychiatric care.
There were a number of events that precipitated this family into crisis. The family home was burgled and L1200 worth of goods were taken. This event prompted a ‘nervous breakdown’ in Mrs H., and a few days later Kevin committed his first offence. In a single day he took and drove away three motorcycles which he claimed to be test driving. He was disqualified for three months and fined. He immediately paid his fine out of his own savings. When he regained his licence three months later, he took and drove away three cars on two separate days. He was unable to explain any of these events.
During the first session it transpired that Mrs H. was very angry at her husband for being passive, both at home and in their marital relationship. They each com- plained of living separate lives, while at the same time uniting to label Kevin as a ‘slow starter’, who had difficulty in communicating. Whenever he tried, they would interrupt him.
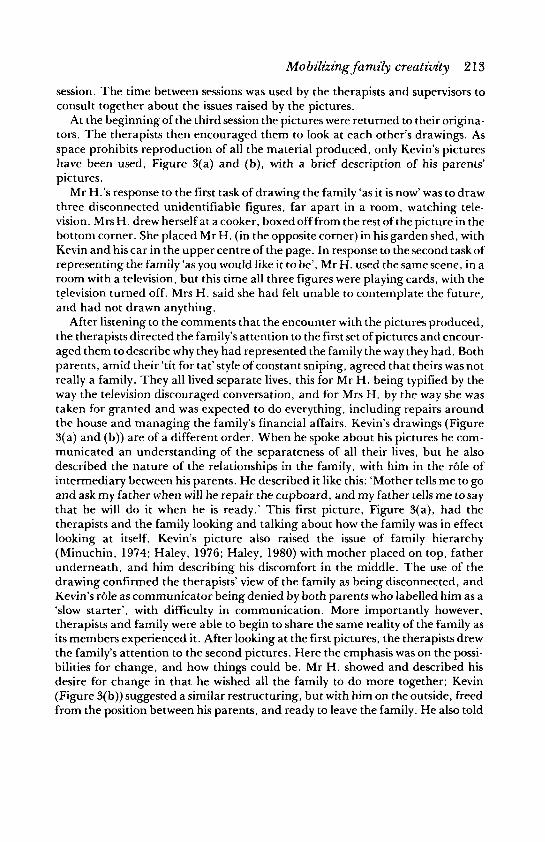
The drawing task was introduced near the end of the second session, with the therapists asserting that this was usual at this point in therapy. Each member was given a drawing board with two pieces of paper, and a range of coloured wax crayons. They were encouraged to view this activity as one in which they could begin to help themselves with their problem. The therapists then asked them to ‘represent with the materials’ (not to draw, nor to imply that this was art) their family ‘as it is now’. When this had been done, the therapists asked them to use the second piece of paper to represent their family as they ‘would like it to be’. The family was neither encouraged to look, nor not to look at each other’s pictures at the time. The completion of the task signalled the end of the session, with the family being clearly told that their pictures would provide the basis of the next
I
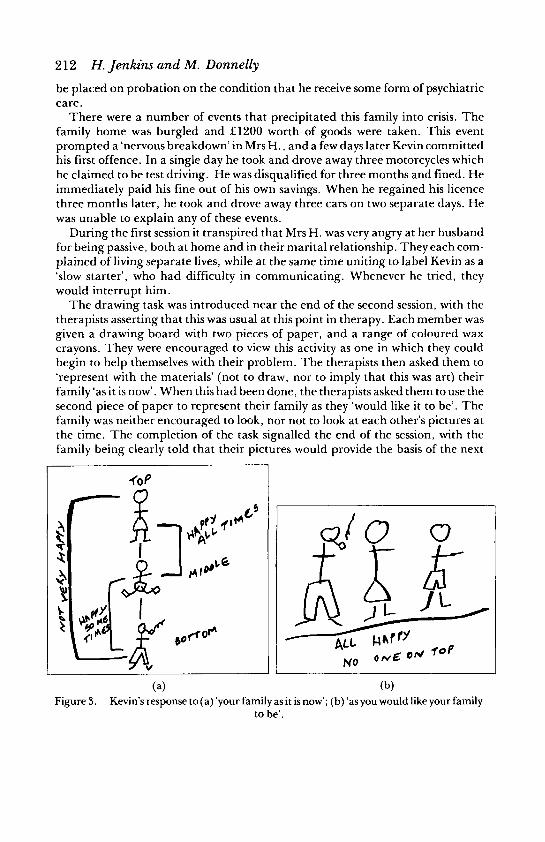
(a) (b) Figure 3. Kevin’s response to (a) ‘your family as it is now’; (b) ‘as you would like your family
to be’.
Mobilizing family creativity 2 13
session. The time between sessions was used by the therapists and supervisors to consult together about the issues raised by the pictures.
At the beginning of the third session the pictures were returned to their origina- tors. The therapists then encouraged them to look at each other’s drawings. As space prohibits reproduction of all the material produced, only Kevin’s pictures have been used, Figure 3(a) and (b), with a brief description of his parents’ pictures.
Mr H.’s response to the first task of drawing the family ‘as it is now’ was to draw three disconnected unidentifiable figures, far apart in a room, watching tele- vision. Mrs H. drew herself at a cooker, boxed off from the rest of the picture in the bottom corner. She placed Mr H. (in the opposite corner) in his garden shed, with Kevin and his car in the upper centre of the page. In response to the second task of representing the family ‘as you would like it to be’, Mr H. used the same scene, in a room with a television, but this time all three figures were playing cards, with the television turned off. Mrs H. said she had felt unable to contemplate the future, and had not drawn anything.
After listening to the comments that the encounter with the pictures produced, the therapists directed the family’s attention to the first set of pictures and encour- aged them to describe why they had represented the family the way they had. Both parents, amid their ‘tit for tat’style of constant sniping, agreed that theirs was not really a family. They all lived separate lives, this for Mr H. being typified by the way the television discouraged conversation, and for Mrs H. by the way she was taken for granted and was expected to do everything, including repairs around the house and managing the family’s financial affairs. Kevin’s drawings (Figure 3(a) and (b)) are of a different order. When he spoke about his pictures he com- municated an understanding of the separateness of all their lives, but he also described the nature of the relationships in the family, with him in the r61e of intermediary between his parents. He described it like this: ‘Mother tells me to go and ask my father when will he repair the cupboard, and my father tells me to say that he will do it when he is ready.’ This first picture, Figure 3(a), had the therapists and the family looking and talking about how the family was in effect looking at itself. Kevin’s picture also raised the issue of family hierarchy (Minuchin, 1974; Haley, 1976; Haley, 1980) with mother placed on top, father underneath, and him describing his discomfort in the middle. The use of the drawing confirmed the therapists’ view of the family as being disconnected, and Kevin’s r61e as communicator being denied by both parents who labelled him as a ‘slow starter’, with difficulty in communication. More importantly however, therapists and family were able to begin to share the same reality of the family as its members experienced it. After looking at the first pictures, the therapists drew the family’s attention to the second pictures. Here the emphasis was on the possi- bilities for change, and how things could be. Mr H. showed and described his desire for change in that he wished all the family to do more together; Kevin (Figure 3(b)) suggested a similar restructuring, but with him on the outside, freed from the position between his parents, and ready to leave the family. He also told

214 H . Jenkzns and M . Donnelly
the therapists that he had given his father a pipe, as mother needed someone strong to lean on. Implicit in Kevin’s drawings was a desire to shift from a denied complementary family structure to a more symmetrical one which would consider him as more adult.
Paradoxically, although Kevin’s pictures seem to be the most insightful of the family predicament, it was Mrs H.’s blank view of the future which actively challenged them. Her blank picture was carefully reframed as being a very honest response, one that must have taken great courage to describe the future in such a direct and uncompromising way. The therapists encouraged Mr and Mrs H. to discuss their future, and why she saw it as so blank. I t emerged from their dis- cussion that Mrs H. was unhappy with a future in which Kevin might be leaving home, when she would be left with ‘that man’. This produced valuable material for both the therapists and family. It enabled the therapists to focus on the parental dyad, and to allow Kevin the opportunity to free himself from the family system which sought to keep him as a dependent child. Here, the pictures enabled a previously silent or censored member of the family to have a voice. They high- lighted the areas where change was considered most possible, and they enabled the whole family to share the fears they all held as they began to deal with the developmental crisis it found itself in. Mrs H. drew attention by using the blank page to her fears of being left with her husband, and this now became the real family problem rather than Kevin’s earlier acting out behaviour.
Conclusion Clearly we have not covered, nor attempted to account for, all the thera- peutic possibilities of the range of interventions open to the therapist. Flexibility and the ability to respond intuitively to the client’s idiom are more important than the learning by rote of a limited range of well- rehearsed techniques. Any technique which is used out of context by the therapist will be experienced by the family as an emotional assault. Any system which feels itself to be under threat will respond in the most familiar way it knows in order to retain its integrity. At all times, and in varying degrees, therapy is about changing the system. It is a delicate task for the therapist to gauge the fine balance between being inducted into the family system, healthily stressing that system, and overloading its coping abilities. The more pathological and rigid the system, the greater will be its tendency to perceive threat to its wholeness.
Whether the therapist chooses sculpting, geneograms or family drawing, or any combination, a common theme seems to be his or her ability to take familiar or negative material, and to create an opportunity for the family to perceive itself differently. Hence, the process of a sculpt in case illustration 2 , the lack of immediate relevance for the family in the geneogram in case illustration 3, and the blank sheet of paper, that
Mobilizing family creativity 215
apparently nil response, in case illustration 4, all become creative material to open up new possibilities for the family and therapist to work on. The therapist who approaches the family with a set ‘game-plan’ in his mind will transmit his consequent anxiety to the family when treatment takes an unexpected turn, at which point the dissonance between his plan and their expectations will result in a failure of encounter, and all too easily the family will be labelled resistant to therapy.
None of these techniques alone are solutions in themselves, nor are they short cuts to effective treatment. Their use will always provide informa- tion for the therapist, including information which from another con- ceptual framework might be viewed as therapeutically non-productive. We have included an example where a formal geneogram failed to fit with the family’s ‘language’ but where an alternative approach through family drawing proved successful in eliciting material useful to both therapist and family. When however, a therapist fails to gain co-operation with a proposal, he should first review whether he has successfully joined with the family before deciding that the family is ‘resistant’, which of course it is. He will know that resistance is the property of a relationship, and that the therapist plus family relationship needs to be examined. Attendance for sessions, whether home- or clinic-based, and a commitment to try to bring about change between family and therapist are not necessarily synony- mous. This is particularly true when treatment is under duress from a third party, or there is no consensus in the family that any problem what- soever exists. The therapist should also consider whether he is moving too fast or too slow for the family, since both will create difficulties in gaining the family’s trust. He should ask himself whether he has used his or the family’s ‘language’ when introducing techniques unfamiliar to them. If the therapist finds that he has not been syntonic in one or more of these areas, this allows him to modify his approach in order to respond more appropriately to the family’s current status.
We suggest that these techniques can usefully be employed by therapists struggling with two different kinds of families, both in order to provide the levels of information already described in this paper, and to change the predominant tempo of such families. They are the overly verbal, super- reasonable families who will discuss and counter-discuss every side of every issue, and by contrast, those families lacking in verbal skills and charac- terized by a high degree of under-organization (Minuchin and Montalvo, 1971). In both instances, non-verbal action-oriented techniques can play a useful part in treatment. They help change the atmosphere and level of in- formation made available, as well as placing all members on the same level in having to cope with the unfamiliar. Such techniques help focus

216 H. Jenkins and M . Donnelly
attention on the minutiae of process, increasing the likelihood of creating therapeutic intensity. A primary gain in both instances is for the therapist to win back some leverage in order to workmore effectively with the family.
A number of themes have been considered in this paper which may help the therapist in his attempt to be useful to those who come, or are sent to him for help. In the interests of clarity, we have isolated and concentrated on certain activities which we identify as primarily client-oriented. In this we have also been faithful to the process of therapy, since we find increasingly in our work the usefulness of isolating and concentrating on specific issues as a way of encapsulating a wider reality, and of giving us something over which we can help the family change. The therapist should also be highly sensitive to the needs of his clients in order to help them generate the flexibility and the energy to solve their difficulties. To this end, the therapist becomes directly involved. In attempting to introduce flexibility into the lives of his clients, the therapist finds that he too must develop his own flexibility and willingness to experiment. When this takes place, we believe that it is possible for the ‘encounter’ we discussed at the beginning to be creative for all those involved. If the particular techniques we have described achieve this, they can justifiably be used in therapy.
References
BING, E. (1970) The conjoint family drawing. Family Process, 9: 173-194. BODIN, A. and FERBER, A. (1972) How to go beyond the use of language. In: A. Ferber,
M. Mendelsohnand A. Napier(Eds) TheBookofFamily Therapy, pp. 272-317. New York. Houghton Mifflin Co. Sentry Edition.
BREUNLIN, D. (1979) Nonverbal communication in family therapy. In: S. Walrond- Skinner (Ed.) Family and Marital Psychotherapy: a Cnizcal Approach, pp. 106--131. London. Routledge and Kegan Paul.
BYNG-HALL, J. (1973) Family myths as defence in conjoint family therapy. BrzizjhJournal of Medical Psychology, 46: 239-250.
CADE, B. (1975) Family sculpting. Proceedings of the Association f o r the Psychiatnc Study of Adolescents, Cardiff, pp. 53-57.
DALE, P. (1981) Family therapy and incomplete families.Jounml ofFamily Therapy, 3:
DAVIS, P. H. and OSHERSON, A. (1978) Modified techniques for therapy with inarticulate adolescents. American Journal of Psychotherapy, 32: 533-543.
DUHL, F. J., KANTOR, D. and DUHL, B. S. (1973) Learning, space, and action in family therapy: a primer of sculpture. In: D. A. Bloch (Ed.) Techniques of Family Psycho- therapy: a Przmer, pp. 47-63. New York. Grune and Stratton.
FEINSTEIN, H. M. (1981) Family therapy for the historian? The case of William James. Family Process, 20: 97-107.
3-19.
FREEMAN, D. S. (1976) The family as a system: fact or fantasy? Comprehensive Psychiatry, 17: 735-747.
Mo bilizing family creativity 2 17
FREUD, S. (1922) Introductory Lectures on Psychoanalyszi. London. George Allen and Unwin.
GRINDER, J. and BANDLER, R. (1976) The Structure of Magic, Vol. 11. Palo Alto. Science and Behavior Books.
GUTTMAN,-H. A. (1975) The child’s participation in conjoint family therapy. J o u m l of the American Academy of Child Psychiaty, 14: 490-499.
HALEY, J. (1967) Toward a theory of pathological systems. In: P. Watzlawick and J. H. Weakland (Eds) The Interactional View, pp. 31-48. New York. W. W. Norton and Co. 1977.
HALEY, J. (1976) Problem-Solwzkg Therapy. New York. Jmey Bass. HALEY, J. (1980) LeatziLg Home: the Therapy of Disturbed Young People. New York.
McCraw-Hill. JEFFERSON, C. (1 978) Some notes on the use of family sculpture in therapy. Family Process,
17: 69-76. JENKINS, H. (1977) Professionalsystemsin relationships tochild abuse. Proceedings oJSocial
Work Practice and Non-Accidental Injuy to Children, Welsh Office, pp. 27-31. KRAFT, A. and AUSTIN, V. (1966) Art therapy in the educational use of multiple impact
therapy. Psychiaty and Art, Proceedings of the 3Vth International Colloquium of Psychopathology of Expression, Washington D.C., pp. 106-115.
KWIATKOWSKA, H. Y. (1967) The use of families’ art productions for psychiatric evalua- tion. Bulletin oJArt Therapy, 6: 52-72.
KWIATKOWSKA, H. Y. (1971) Family art therapy and family art evaluation: indication and contraindication. In: J. Jakab (Ed.) hychia ty and Art, Vol. 3, pp. 138-151. Basel. Krager .
LIEBERMAN, S. (1979~) Transgenerational analysis: thegeneogram as a technique in family therapy. Journal of Family Therapy, 1: 51-64.
LIEBERMAN, S. (19796) Tramgenerational Family Therapy. London. Croom Helm. MAY, R. (1976) The Courage to Create. London. Collins. MINLJCHIN, S. (1974) Families and Family Therapy. London. Tavistock. MINUCHIN, S. and MONTALVO, B. (1971) Techniques for working with disorganized low
socioeconomic families. In: J. Haley (Ed.) Changing Families, pp. 202-211. New York. Grune and Stratton.
MULLER, E. F. (1966) Family group art therapy: treatment of choice for a specific case. Psychiaty and Art, Proceedings of the IVth International Colloquium-for Psycho- therapy of Expression, Washington D.C., pp. 132- 143.
PALAZZOLI, M. S. , BOSCOLO, L., CECCHIN, G. F. and PRATA, G. (1977) Family rituals: a powerful tool in family therapy. Family Process, 16: 445-453.
PAPP, P,, SILVERSTEIN, 0. and CARTER, E. (1973) Familysculptingin preventive work with ‘well families’. Family Process, 12: 197-212.
SATIR, V. (1972) Peoplemaking. Pal0 Alto. Science and Behavior Books. SCHAVERIEN, J. (1978) Psychodrama in family therapy. Unpublished paper, given at the
SCHEFLEN, A. E. (1972) Body Language and Social Order. Englewood Cliffs, N.J.
SHERR, C., and HICKS, H. (1973) Family drawings as a diagnostic and therapeutic tech- nique. Family Process, 12: 439-460.
SIMMONDS, J. and BRUMMER, N. (1980) The family sculpt as an educational experience: an exploration of appropriate professional involvement. J o u m l of Family Therapy, 2: 389-399.
Family Institute, Cardiff.
Prentice-Hall.
21 8 H . Jenkins and M . Donnelly
SKYNNER, A. C. R. (1976) Family and marital psychotherapy. British Journal of Hospital
STREET, E. and TREACHER, A. (1980) Microtraining and family therapy skills- towards a
WADFSON, H. (1976) The fluid family in multi-family art therapy. The American Journal
WADESON, H. (1980) Art Psychotherapy. New York, John Wiley. WALROND-SKINNER, S. (1976) Family Therapy: The Treatment of Natural Systems.
London. Routledge and Kegan Paul. WATZLAWICK, P. (1978) The Language of Change: Elements of Therapeutic Communi-
cation. New York. Basic Books. WArZLAWICK, P., BFAVIN,J. andJACKSON, D. (1967)PragmuticsofHuman Communica-
tion. A Study of Interactional Patterns, Pathologies and Paradoxes. New York. W. W. Norton and Co.
Medicine. March, 224-234.
possible synthesis. J o u m l of Family Therapy, 2: 243-257.
ofArt Therapy, 15: 115-118.


















