The Shoulder Book - thetherapyweb.com · The Shoulder Book Study Text. Contents Articles ... The...
25
PDF generated using the open source mwlib toolkit. See http://code.pediapress.com/ for more information. PDF generated at: Wed, 04 Sep 2013 07:57:03 UTC The Shoulder Book Study Text
Transcript of The Shoulder Book - thetherapyweb.com · The Shoulder Book Study Text. Contents Articles ... The...

PDF generated using the open source mwlib toolkit. See http://code.pediapress.com/ for more information.PDF generated at: Wed, 04 Sep 2013 07:57:03 UTC
The Shoulder BookStudy Text

ContentsArticles
Shoulder 1Glenohumeral joint 7Rotator cuff 11
ReferencesArticle Sources and Contributors 21Image Sources, Licenses and Contributors 22
Article LicensesLicense 23

Shoulder 1
Shoulder
Shoulder
Diagram of the human shoulder joint
Capsule of shoulder-joint (distended). Anterior aspect.
Latin articulatio humeri
Gray's subject #81 313 [1]
MeSH Shoulder [2]
The human shoulder is made up of three bones: the clavicle (collarbone), the scapula (shoulder blade), and thehumerus (upper arm bone) as well as associated muscles, ligaments and tendons. The articulations between the bonesof the shoulder make up the shoulder joints. "Shoulder joint" typically refers to the glenohumeral joint, which is themajor joint of the "shoulder," but can more broadly include the acromioclavicular joint. In human anatomy, theshoulder joint comprises the part of the body where the humerus attaches to the scapula, the head sitting in theglenoid fossa.[3] The shoulder is the group of structures in the region of the joint.[4]
There are two kinds of cartilage in the joint. The first type is the white cartilage on the ends of the bones (calledarticular cartilage) which allows the bones to glide and move on each other. When this type of cartilage starts to wearout (a process called arthritis), the joint becomes painful and stiff. The labrum is a second kind of cartilage in theshoulder which is distinctly different from the articular cartilage. This cartilage is more fibrous or rigid than thecartilage on the ends of the ball and socket. Also, this cartilage is also found only around the socket where it isattached.[5]
The shoulder must be mobile enough for the wide range actions of the arms and hands, but also stable enough toallow for actions such as lifting, pushing and pulling. The compromise between mobility and stability results in alarge number of shoulder problems not faced by other joints such as the hip.

Shoulder 2
Human anatomy
JointsThere are three joints of the shoulder: The glenohumeral, acromioclavicular, and the sternoclavicular joints.
Glenohumeral joint
The glenohumeral joint is the main joint of the shoulder and the generic term "shoulder joint" usually refers to it. It isa ball and socket joint that allows the arm to rotate in a circular fashion or to hinge out and up away from the body. Itis formed by the articulation between the head of the humerus and the lateral scapula (specifically-the glenoid fossaof the scapula). The "ball" of the joint is the rounded, medial anterior surface of the humerus and the "socket" isformed by the glenoid fossa, the dish-shaped portion of the lateral scapula. The shallowness of the fossa andrelatively loose connections between the shoulder and the rest of the body allows the arm to have tremendousmobility, at the expense of being much easier to dislocate than most other joints in the body. Approximately its 4 to 1disproportion between the large head of the humerus and the shallow glenoid cavity.
Anatomical studies of the shoulder by Leonardo daVinci c.1510
The capsule is a soft tissue envelope that encircles theglenohumeral joint and attaches to the scapula, humerus, and headof the biceps. It is lined by a thin, smooth synovial membrane.This capsule is strengthened by the coracohumeral ligament whichattaches the coracoid process of the scapula to the greater tubercleof the humerus. There are also three other ligaments attaching thelesser tubercle of the humerus to lateral scapula and arecollectively called the glenohumeral ligaments.
There is also a ligament called semicirculare humeri which is atransversal band between the posterior sides of the tuberculumminus and majus of the humerus. This band is one of the mostimportant strengthening ligaments of the joint capsule. Theshoulder is a vital joint and critical for movement.
Sternoclavicular joint
The sternoclavicular occurs at the medial end of the clavicle withthe manubrium or top most portion of the sternum. The clavicle istriangular and rounded and the manubrium is convex; the twobones articulate. The joint consists of a tight capsule and completeintra-articular disc which ensures stability of the joint. Thecostoclavicular ligament is the main limitation to movement, therefore, the main stabilizer of the joint. Afibrocartilaginous disc present at the joint increases the range of movement. Sternoclavicular dislocation is rare,[6]
however it can be caused by direct trauma.

Shoulder 3
MovementsThe muscles and joints of the shoulder allow it to move through a remarkable range of motion, making it one of themost mobile joints in the human body. The shoulder can abduct, adduct (such as during the shoulder fly), rotate, beraised in front of and behind the torso and move through a full 360° in the sagittal plane. This tremendous range ofmotion also makes the shoulder extremely unstable, far more prone to dislocation and injury than other joints [7]
The following describes the terms used for different movements of the shoulder:[8]
Name Description Muscles
Scapular retraction[] (aka scapularadduction)
The scapula is moved posteriorly and medially along the back,moving the arm and shoulder joint posteriorly. Retracting bothscapulae gives a sensation of "squeezing the shoulder bladestogether."
rhomboideus major, minor, and trapezius
Scapularprotraction
[] (akascapular abduction)
The opposite motion of scapular retraction. The scapula is movedanteriorly and laterally along the back, moving the arm and shoulderjoint anteriorly. If both scapulae are protracted, the scapulae areseparated and the pectoralis major muscles are squeezed together.
serratus anterior (prime mover), pectoralis minor andmajor
Scapular elevation [] The scapula is raised in a shrugging motion. levator scapulae, the upper fibers of the trapezius
Scapular depression[]
The scapula is lowered from elevation. The scapulae may bedepressed so that the angle formed by the neck and shoulders isobtuse, giving the appearance of "slumped" shoulders.
pectoralis minor, lower fibers of the trapezius,subclavius, latissimus dorsi
Arm abduction [] Arm abduction occurs when the arms are held at the sides, parallel tothe length of the torso, and are then raised in the plane of the torso.This movement may be broken down into two parts: True abductionof the arm, which takes the humerus from parallel to the spine toperpendicular; and upward rotation of the scapula, which raises thehumerus above the shoulders until it points straight upwards.
True abduction: supraspinatus (first 15 degrees),deltoid; Upward rotation: trapezius, serratus anterior
Arm adduction [] Arm adduction is the opposite motion of arm abduction. It can bebroken down into two parts: downward rotation of the scapula andtrue adduction of the arm.
Downward rotation: pectoralis minor, pectoralismajor, subclavius, latissimus dorsi (same as scapulardepression, with pec major replacing lower fibers oftrapezius); True Adduction: same as downwardrotation with addition of teres major and the lowestfibers of the deltoid
Arm flexion [] The humerus is rotated out of the plane of the torso so that it pointsforward (anteriorly).
pectoralis major, coracobrachialis, biceps brachii,anterior fibers of deltoid.
Arm extension [] The humerus is rotated out of the plane of the torso so that it pointsbackwards (posteriorly)
latissimus dorsi and teres major, long head of triceps,posterior fibers of the deltoid
Medial rotation ofthe arm []
Medial rotation of the arm is most easily observed when the elbow isheld at a 90-degree angle and the fingers are extended so they areparallel to the ground. Medial rotation occurs when the arm is rotatedat the shoulder so that the fingers change from pointing straightforward to pointing across the body.
subscapularis, latissimus dorsi, teres major,pectoralis major, anterior fibers of deltoid
Lateral rotation ofthe arm[]
The opposite of medial rotation of the arm. infraspinatus and teres minor, posterior fibers ofdeltoid
Armcircumduction
[]Movement of the shoulder in a circular motion so that if the elbowand fingers are fully extended the subject draws a circle in the airlateral to the body. In circumduction, the arm is not lifted aboveparallel to the ground so that "circle" that is drawn is flattened on top.
pectoralis major, subscapularis, coracobrachialis,biceps brachii, supraspinatus, deltoid, latissimusdorsi, teres major and minor, infraspinatus, longhead of triceps
The scapula is lowered from elevation. The scapulae may be depressed so that the angle formed by the neck andshoulders is obtuse, giving the appearance of "slumped" shoulders. Arm abduction occurs when the arms are held at

Shoulder 4
the sides, parallel to the length of the torso, and are then raised in the plane of the torso. This movement may bebroken down into two parts: True abduction of the arm, which takes the humerus from parallel to the spine toperpendicular; and upward rotation of the scapula, which raises the humerus above the shoulders until it pointsstraight upwards.
Muscles
Major muscles
The muscles that are responsible for movement in the shoulder attach to the scapula, humerus, and clavicle. Themuscles that surround the shoulder form the shoulder cap and underarm.
Name Attachment Function
serratus anterior Originates on the surface of the upper eight ribs at theside of the chest and inserts along the entire anteriorlength of the medial border of the scapula.
It fixes the scapula into the thoracic wall and aids in rotationand abduction of the shoulders.
subclavius Located inferior to the clavicle, originating on the firstrib and inserting (penetrating) on the subclavian grooveof the clavicle.
It depresses the lateral clavicle and also acts to stabilize theclavicle.
pectoralis minor Arises from the third, fourth, and fifth ribs, near theircartilage and inserts into the medial border and uppersurface of the coracoid process of the scapula.
This muscle aids in respiration, medially rotates the scapula,protracts the scapula, and also draws the scapula inferiorly.
sternocleidomastoid Attaches to the sternum (sterno-), the clavicle (cleido-),and the mastoid process of the temporal bone of theskull.
Most of its actions flex and rotate the head. In regards to theshoulder, however, it also aids in respiration by elevating thesternoclavicular joint when the head is fixed.
levator scapulae Arises from the transverse processes of the first fourcervical vertebrae and inserts into the medial border ofthe scapula.
It is capable of rotating the scapula downward and elevatingthe scapula.
rhomboid major andrhomboid minor (worktogether)
They arise from the spinous processes of the thoracicvertebrae T1 to T5 as well as from the spinous processesof the seventh cervical. They insert on the medial borderof the scapula, from about the level of the scapular spineto the scapula's inferior angle.
They are responsible for downward rotation of the scapulawith the levator scapulae, as well as adduction of the scapula.
trapezius Arises from the occipital bone, the ligamentum nuchae,the spinous process of the seventh cervical, and thespinous processes of all the thoracic vertebrae, and fromthe corresponding portion of the supraspinal ligament. Itinserts on the lateral clavicle, the acromion process, andinto the spine of the scapula.
Different portions of the fibers perform different actions on thescapula: depression, upward rotation, elevation, andadductions.
deltoid, anterior fibers Arises from the anterior border and upper surface of thelateral third of the clavicle.
The anterior fibres are involved in shoulder abduction whenthe shoulder is externally rotated. The anterior deltoid is weakin strict transverse flexion but assists the pectoralis majorduring shoulder transverse flexion / shoulder flexion (elbowslightly inferior to shoulders).
deltoid, middle fibers Arises from the lateral margin and upper surface of theacromion.
The middle fibres are involved in shoulder abduction when theshoulder is internally rotated, are involved in shoulder flexionwhen the shoulder is internally rotated, and are involved inshoulder transverse abduction (shoulder externally rotated) --but are not utilized significantly during strict transverseextension (shoulder internally rotated).

Shoulder 5
deltoid, posterior fibers Arises from the lower lip of the posterior border of thespine of the scapula, as far back as the triangular surfaceat its medial end.
The posterior fibres are strongly involved in transverseextension particularly since the latissimus dorsi muscle is veryweak in strict transverse extension. The posterior deltoid isalso the primary shoulder hyperextensor.
Rotator cuff
The rotator cuff is an anatomical term given to the group of muscles and their tendons that act to stabilize theshoulder. It is composed of the tendons and muscles (supraspinatus, infraspinatus, teres minor and subscapularis)that hold the head of the humerus (ball) in the glenoid fossa (socket).Two filmy sac-like structures called bursae permit smooth gliding between bone, muscle, and tendon. They cushionand protect the rotator cuff from the bony arch of the acromion.
Medical problemsShoulder problems including pain, are one of the more common reasons for physician visits for musculoskeletalsymptoms. The shoulder is the most movable joint in the body. However, it is an unstable joint because of the rangeof motion allowed. This instability increases the likelihood of joint injury, often leading to a degenerative process inwhich tissues break down and no longer function well. Major injuries to the shoulder include rotator cuff tear andbone fractures of one or more of the bones of the shoulder.Shoulder fractures include:•• Clavicle fracture•• Scapular fracture• Proximal humerus fracture
Evolutionary variationTetrapod forelimb are characterised by a high degree of mobility in the shoulder-thorax connection. Lacking of asolid skeletal connection between the shoulder girdle and the vertebral column, the forelimb's attachment to the trunkis instead mainly controlled by serratus lateralis and levator scapulae. Depending on locomotor style, a bone connectthe shoulder girdle to the trunk in some animals; the coracoid bone in reptiles and birds, and the clavicle in primatesand bats; but cursorial mammals lack this bone. In primates, the shoulder shows characteristics the differs from othermammals, including a well developed clavicle, a dorsally shifted scapula with prominent acromion and spine, and ahumerus featuring a straight shaft and a spherical head. [9]

Shoulder 6
Additional images
The left shoulder and acromioclavicular joints, and the properligaments of the scapula
Instrumented shoulder endoprosthesis, with a 9-channel telemetry transmitter to measure six loadcomponents in vivo. (cut model)
References[1] http:/ / education. yahoo. com/ reference/ gray/ subjects/ subject?id=81#p313[2] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?mode=& term=Shoulder[7][7] Scientific Keys Volume I, The Key Muscles of Hatha Yoga, Ray Long MD FRCSC, Third Edition, pg. 174
http:/ / www. prlog. org/12015359-acromioclavicular-arthritis-by-dr-les-bailey-phddoacopmapta-int-part-dr-les-bailey. html• Video of the shoulder carriage in motion (http:/ / chrisevans3d. com/ research. htm)• NIH (article includes text from this source) (http:/ / www. niams. nih. gov/ hi/ topics/ shoulderprobs/ shoulderqa.
htm)• University of Michigan Medical School module on movements of the shoulder, arm, forearm, and hand (http:/ /
www. med. umich. edu/ lrc/ coursepages/ M1/ anatomy2010/ html/ modules/ upper_limb_module/upper_limb_01. html)

Glenohumeral joint 7
Glenohumeral joint
Glenohumeral joint
The right shoulder and Glenohumeral joint
Latin Articulatio humeri
Gray's subject #82 315 [1]
MeSH Glenohumeral+Joint [2]
The glenohumeral joint, (from ancient Greek glene, eyeball, puppet, doll + -oid, 'form of', + Latin humerus,shoulder) or shoulder joint, is a multiaxial synovial ball and socket joint and involves articulation between theglenoid fossa of the scapula (shoulder blade) and the head of the humerus (upper arm bone). Due to the very limitedinterface of the humerus and scapula, it is the most mobile joint of the human body.
MovementsThe glenoid fossa is shallow and contains the glenoid labrum which deepens it and aids in stability. With 120degrees of unassisted flexion, the glenohumeral joint is the most mobile joint in the body.Scapulohumeral rhythm helps to achieve further range of movement. The Scapulohumeral rhythm is the movementof the scapula across the thoracic cage in relation to the humerus. This movement can be compromised by anythingthat changes the position of the scapula. This could be an imbalance in the muscles that hold the scapula in placewhich are the upper and lower trapezius. This imbalance could cause a forward head carriage which in turn canaffect the range of movements of the shoulder.The rotator cuff muscles of the shoulder produce a high tensile force, and help to pull the head of the humerus intothe glenoid fossa.
Movements of the shoulder joint.[3]
Movement Muscles Origin Insertion
Flexion(150°–170°)
Anterior fibers of deltoid Clavicle Middle of lateral surface ofshaft of humerus
Clavicular part ofpectoralis major
Clavicle Lateral lip of bicipital grooveof humerus
Long head of bicepsbrachii
Supraglenoid tubercle of scapula Tuberosity of radius, Deepfascia of forearm
Short head of bicepsbrachii
Coracoid process of scapula
Coracobrachialis Coracoid process Medial aspect of shaft ofhumerus
Glenohumeral joint 8
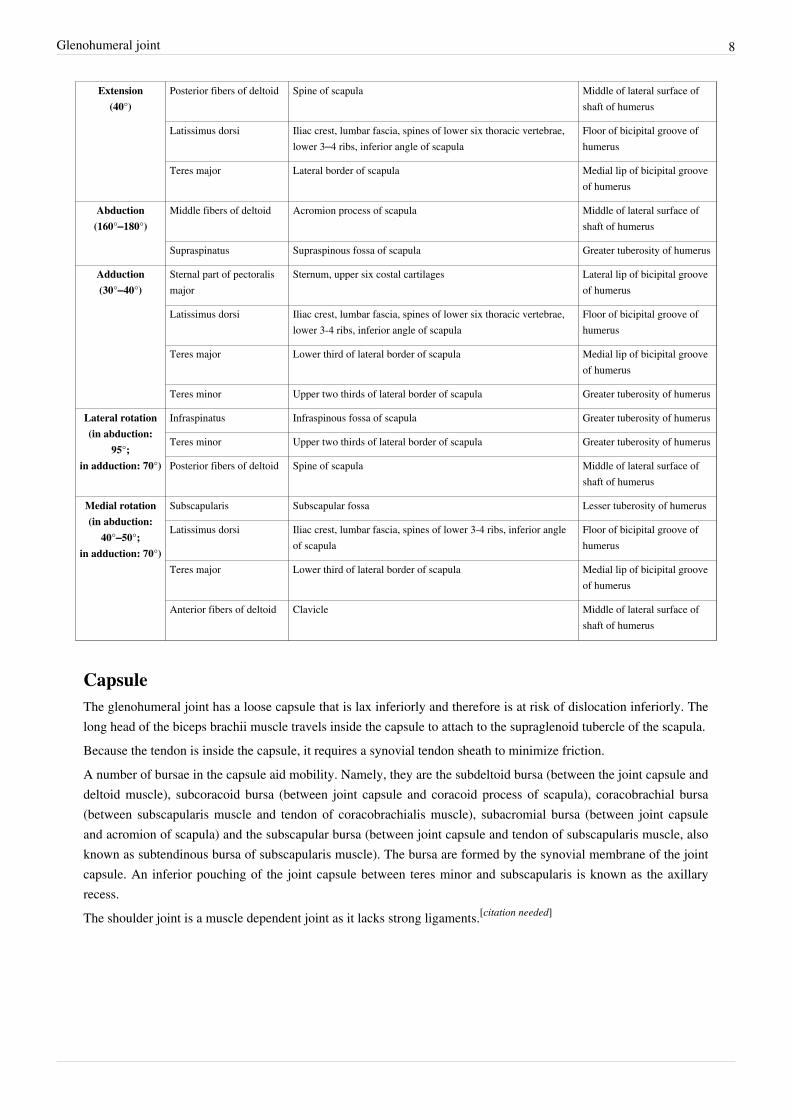
Extension(40°)
Posterior fibers of deltoid Spine of scapula Middle of lateral surface ofshaft of humerus
Latissimus dorsi Iliac crest, lumbar fascia, spines of lower six thoracic vertebrae,lower 3–4 ribs, inferior angle of scapula
Floor of bicipital groove ofhumerus
Teres major Lateral border of scapula Medial lip of bicipital grooveof humerus
Abduction(160°–180°)
Middle fibers of deltoid Acromion process of scapula Middle of lateral surface ofshaft of humerus
Supraspinatus Supraspinous fossa of scapula Greater tuberosity of humerus
Adduction(30°–40°)
Sternal part of pectoralismajor
Sternum, upper six costal cartilages Lateral lip of bicipital grooveof humerus
Latissimus dorsi Iliac crest, lumbar fascia, spines of lower six thoracic vertebrae,lower 3-4 ribs, inferior angle of scapula
Floor of bicipital groove ofhumerus
Teres major Lower third of lateral border of scapula Medial lip of bicipital grooveof humerus
Teres minor Upper two thirds of lateral border of scapula Greater tuberosity of humerus
Lateral rotation(in abduction:
95°;in adduction: 70°)
Infraspinatus Infraspinous fossa of scapula Greater tuberosity of humerus
Teres minor Upper two thirds of lateral border of scapula Greater tuberosity of humerus
Posterior fibers of deltoid Spine of scapula Middle of lateral surface ofshaft of humerus
Medial rotation(in abduction:
40°–50°;in adduction: 70°)
Subscapularis Subscapular fossa Lesser tuberosity of humerus
Latissimus dorsi Iliac crest, lumbar fascia, spines of lower 3-4 ribs, inferior angleof scapula
Floor of bicipital groove ofhumerus
Teres major Lower third of lateral border of scapula Medial lip of bicipital grooveof humerus
Anterior fibers of deltoid Clavicle Middle of lateral surface ofshaft of humerus
CapsuleThe glenohumeral joint has a loose capsule that is lax inferiorly and therefore is at risk of dislocation inferiorly. Thelong head of the biceps brachii muscle travels inside the capsule to attach to the supraglenoid tubercle of the scapula.Because the tendon is inside the capsule, it requires a synovial tendon sheath to minimize friction.A number of bursae in the capsule aid mobility. Namely, they are the subdeltoid bursa (between the joint capsule anddeltoid muscle), subcoracoid bursa (between joint capsule and coracoid process of scapula), coracobrachial bursa(between subscapularis muscle and tendon of coracobrachialis muscle), subacromial bursa (between joint capsuleand acromion of scapula) and the subscapular bursa (between joint capsule and tendon of subscapularis muscle, alsoknown as subtendinous bursa of subscapularis muscle). The bursa are formed by the synovial membrane of the jointcapsule. An inferior pouching of the joint capsule between teres minor and subscapularis is known as the axillaryrecess.The shoulder joint is a muscle dependent joint as it lacks strong ligaments.[citation needed]

Glenohumeral joint 9
Ligaments• Superior, middle and inferior glenohumeral ligaments•• Coracohumeral ligament•• Transverse humeral ligament
Nerve Supply•• suprascapular nerve•• axillary nerve•• lateral pectoral nerve
Blood SupplyThe glenohumeral joint is supplied with blood by branches of the anterior and posterior circumflex humeral andsuprascapular arteries.
PathologyThe capsule can become inflamed and stiff, with abnormal bands of tissue (adhesions) growing between the jointsurfaces, causing pain and restricting movement of the shoulder, a condition known as frozen shoulder or adhesivecapsulitis.
Additional images
Cross-section ofshoulder joint cavity
Diagram of the humanshoulder joint
The left shoulder andacromioclavicular
joints, and the properligaments of the
scapula.
coracohumeral ligament ofGlenohumeral joint
articular capsule of glenohumeraljoint
glenohumeral ligaments ofglenohumeral joint
cartilage of glenohumeral joint synovial membrane ofglenohumeral joint

Glenohumeral joint 10
articular capsule of glenohumeraljoint
References[1] http:/ / education. yahoo. com/ reference/ gray/ subjects/ subject?id=82#p315[2] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?mode=& term=Glenohumeral+ Joint
External links• Overview at brown.edu (http:/ / biomed. brown. edu/ Courses/ BI108/ BI108_2004_Groups/ Group01/ bioghj.
htm)• Overview at ouhsc.edu (http:/ / moon. ouhsc. edu/ dthompso/ namics/ gh. htm)• SUNY Figs 10:03-12 (http:/ / ect. downstate. edu/ courseware/ haonline/ figs/ l10/ 100312. htm)• Diagram at yess.uk.com (http:/ / www. yess. uk. com/ patient_information/ anatomy/ )

Rotator cuff 11
Rotator cuff
Rotator cuff
Muscles on the dorsum of the scapula, and the Triceps brachii.
The scapular and circumflex arteries.
In anatomy, the rotator cuff (sometimes incorrectly called a "rotator cup", "rotor cuff", or rotary cup[1]) is a groupof muscles and their tendons that act to stabilize the shoulder. The four muscles of the rotator cuff are over half ofthe seven scapulohumeral muscles.
FunctionThe rotator cuff muscles are important in shoulder movements and in maintaining glenohumeral joint (shoulderjoint) stability.[] These muscles arise from the scapula and connect to the head of the humerus, forming a cuff at theshoulder joint. They hold the head of the humerus in the small and shallow glenoid fossa of the scapula. Theglenohumeral joint has been analogously described as a golf ball (head of the humerus) sitting on a golf tee (glenoidfossa).[2]
During abduction of the arm, moving it outward and away from the trunk, the rotator cuff compresses theglenohumeral joint, a term known as concavity compression, in order to allow the large deltoid muscle to furtherelevate the arm. In other words, without the rotator cuff, the humeral head would ride up partially out of the glenoidfossa, lessening the efficiency of the deltoid muscle. The anterior and posterior directions of the glenoid fossa aremore susceptible to shear force perturbations as the glenoid fossa is not as deep relative to the superior and inferiordirections. The rotator cuff's contributions to concavity compression and stability vary according to their stiffnessand the direction of the force they apply upon the joint.

Rotator cuff 12
Muscles comprising rotator cuff
Muscle Origin on scapula Attachment on humerus Function Innervation
Supraspinatusmuscle
supraspinous fossa superior and middle facet of thegreater tuberosity
abducts the arm Suprascapular nerve (C5)
Infraspinatusmuscle
infraspinous fossa posterior facet of the greatertuberosity
externally rotates thearm
Suprascapular nerve (C5-C6)
Teres minormuscle
middle half of lateralborder
inferior facet of the greater tuberosity externally rotates thearm
Axillary nerve (C5)
Subscapularismuscle
subscapular fossa lesser tuberosity (60%) or humeralneck (40%)
internally rotates thehumerus
Upper and Lower subscapularnerve (C5-C6)
The supraspinatus muscle fans out in a horizontal band to insert on the superior and middle facets of the greatertubercle. The greater tubercle projects as the most lateral structure of the humeral head. Medial to this, in turn, is thelesser tuberosity of the humeral head. The subscapularis muscle origin is divided from the remainder of the rotatorcuff origins as it is deep to the scapula.
Injuries
Rotator cuff tearThe tendons at the ends of the rotator cuff muscles can become torn, leading to pain and restricted movement of thearm. A torn rotator cuff can occur following a trauma to the shoulder or it can occur through the "wear and tear" ontendons, most commonly the supraspinatus tendon found under the acromion.Rotator cuff injuries are commonly associated with motions that require repeated overhead motions or forcefulpulling motions. Such injuries are frequently sustained by athletes whose actions include making repetitive throws,athletes such as cheerleaders, baseball pitchers, softball pitchers, American football players (especiallyquarterbacks), weightlifters, especially powerlifters due to extreme weights used in the bench press, rugby players,volleyball players (due to their swinging motions)[citation needed], water polo players, rodeo team ropers, shot putthrowers (due to using poor technique)[citation needed], swimmers, boxers, kayakers, western martial artists, fastbowlers in cricket, tennis players (due to their service motion)[citation needed] and tenpin bowlers due to the repetitiveswinging motion of the arm with the weight of a bowling ball.This type of injury also commonly affects orchestra conductors, choral conductors, and drummers (due, again, toswinging motions).
Rotator cuff impingementA systematic review of relevant research found that the accuracy of the physical examination is low.[] TheHawkins-Kennedy test[3][] has a sensitivity of approximately 80% to 90% for detecting impingement. Theinfraspinatus and supraspinatus[4] tests have a specificity of 80% to 90%.[]
Treatment
Reduce pain and swelling
As with all muscle injuries, R.I.C.E. is an initial response to injury recommended by health providers:• Rest means ceasing movement of the affected area.• Icing uses ice to reduce inflammation.• Compression limits the swelling.

Rotator cuff 13
• Elevation involves placing the area higher to reduce inflammation and swelling.Cold compression therapy shoulder wraps facilitate the icing and compression of an otherwise difficult body area toice and compress.Depending on severity of symptoms, further imaging with radiograph, or MRI may be warranted to see if surgery oran underlying bone injury exists.
Posture and sleeping positions
Postures and sleeping positions may be modified to provide relief. But as your shoulder begins to heal, sleepingpositions may vary considerably.[]
Strengthening
The rotator cuff can be strengthened to rehabilitate shoulder injuries, and prevent future ones. There are differentexercises to target the individual rotator cuff muscles.
Description Beginning End
The most effective is the side-lying external rotation, which activates thesupraspinatus, subscapularis, infraspinatus and teres minor.
Lie on a bench sideways, with the affected arm next to the side and flexed about 90degrees at the elbow. Rotate the upper arm outward, keeping the elbow flexed and thearm close to the body, until the lower arm is perpendicular to the ceiling (see picture).For added resistance, use a dumbbell. Pace at two seconds out and four seconds back.
This is an excellent all-around shoulder exercise.
The propped external rotator targets the infraspinatus and teres minor.
Sit perpendicular to the dumbell with arm flexed at 90 degrees at the elbow, and theforearm resting parallel on the dumbell. Raise the dumbbell up until the forearmpoints up. Slowly lower the dumbbell and repeat, exercising both arms.
The posterior deltoid also aids in external rotation. Like the posterior deltoid, both theinfraspinatus and teres minor also contribute to transverse extension of the shoulder,such as during a bent over row to the chest. They can be trained in this way besidesisolating the external rotation action.
The lateral raise with internal rotation (LRIR) primarily targets the supraspinatus.
Grasping a dumbbell in each hand, internally rotate the arms so that the thumbs pointtowards the floor when extended (as if emptying a drink into a bin). Raise the armssideways, keeping the thumbs pointing downwards, until the dumbbells are just belowthe shoulders.
This exercise is sometimes called a lateral raise.
Strengthening the rotator cuff allows for increased loads in a variety of exercises. When weightlifters are unable toincrease the weight they can lift on a pushing exercise (such as the bench press or military press) for an extendedperiod of time, strengthening the rotator cuff can often allow them to begin making gains again. It also preventsfuture injuries to the glenohumeral joint, balancing the often-dominant internal rotators with stronger externalrotators. Finally, exercising the rotator cuff can lead to improved posture, as without exercise to the external rotator,the internal rotators can see a shortening, leading to tightness. This often manifests itself as rounded shoulders.Non-Operative TreatmentNon-operative treatment is often the first line of treatment for rotator cuff injuries. If the tendons are strained or tornless than 50%, they respond well to an aggressive non-operative approach. Non-operative measures can includephysical therapy, oral or injected medications, biologic augmentation such as PRP, ultrasound therapy, dry needling,and other modalities. It will often take 3 months to recover with non-operative measures.

Rotator cuff 14
Surgery
Even for full thickness rotator cuff tears, conservative care (i.e., non-surgical treatment) outcomes are usuallyreasonably good.[5] However, many patients still suffer disability and pain despite non-surgical therapies. Formassive tears of the rotator cuff, surgery has shown durable outcomes on 10 year follow-up.[6] However, the samestudy demonstrated ongoing and progressive fatty atrophy and repeat tears of the rotator cuff. Shen has shown thatMRI evidence of fatty atrophy in the rotator cuff prior to surgery is predicative of a poor surgical outcome.[7] If therotator cuff is completely torn, surgery is usually required to reattach the tendon to the bone.[8]
Surgery for the Rotator Cuff
Surgery for the rotator cuff can be for complete tears, or partial tears/strains that fail to get better. If a torn rotatorcuff goes untreated for too long, it may become un-repairable and so shoulder pain should not be ignored. Surgeryoften consists of removing damaged tissue and repairing the good tissue back to the bone. Bone spurs andinflammation (bursitis) is also removed to try to prevent re-tears. all arthroscopic rotator cuff repairs can fix mosttears through 4-5 small incisions. On occasion a patch needs to be placed on the rotator cuff tendons which requires alarger incision. Many times, the biceps tendon is damaged with rotator cuff tears and may also require bicepstenodesis surgery at the same time.
Rehab
The rehab for rotator cuff surgery falls into three basic categories; some damage to the tendons with surgeryconsisting of debridement, removing spurs and cleaning out inflammation, tears requiring repair with excellentquality tendon tissue, and tears requiring repair with poor quality tendon tissue. The first category, rehab consists ofearly active and passive range of motion exercises focused on maintaining range of motion for 4 weeks and thenstrengthening and return to sports from weeks 4-8. Repaired tendons with excellent quality will begin full passivemotion early, start active motion from weeks 4-8, strengthening from 8-12 and return to sports after 3–4 months.Repairs with poor tissue quality will have no motion early on, start passive motion after 2–4 weeks, active at 6–8weeks, strengthening at 4 months and return to sports at 6 months. Your doctor will guide you through therehabilitation process.
Imaging
Shoulder imagingThere are several ways to depict the structures of the shoulder, which consist of muscles, tendons, bones, cartilageand soft tissue. When deciding which medical imaging technique should be used, there are a couple of factors thatneed to be taken into account. Firstly, one has to consider the suspected clinical diagnosis. Together with theknowledge of the advantages and limitations of the various medical imaging techniques ( i.e. conventionalradiography, ultrasound, computer tomography and magnetic resonance), one has to make an informed decisionwhich technique would best suit the specific situation.Hodler et al. recommend to start scanning with conventional x-rays taken from at least two planes, since this methodgives a wide first impression and even has the chance of exposing any frequent shoulder pathologies, i.e.decompensated rotator cuff tears, tendinitis calcarea, dislocations, fractures, usures and/or osteophytes. Furthermore,x-rays are required for the planning of an optimal CT or MR image.[9]
Conventional x-rays and ultrasonography are the primary tools used to confirm a diagnosis of injuries sustained tothe rotator cuff. For extended clinical questions, imaging through Magnetic Resonance with or without intraarticularcontrast agent is indicated.The conventional invasive arthrography is now-a-days being replaced by the non-invasive MRI and US and is usedas an imaging reserve for patients who are contraindicated for MRI, for example pacemaker-carriers with an unclearand unsure ultrasonography.[10]

Rotator cuff 15
Conventional x-rays
a.-p.-projection 40° posterior oblique after Grashey
CR. shoulder x-ray, a.p.
The scapula should be positioned parallel to the x-ray film. The bodyhas to be rotated about 30 to 45 degrees towards the shoulder to beimaged, and the standing or sitting patient lets the arm hang.This method allows the diagnostician to judge:[10]
•• The joint gap and the vertical alignment towards the socket.The humerus head should be aligned in the neutral position andexternal rotation in a way towards the socket, that a fictive continuousline can be seen. This line is called Bandi line, otherwise known as theMénard-Shenton line. A discontinuous line alludes to a cranialdecentralization of the humerus head.[11]
Transaxillary projection
Transaxillary conventional radiography
The arm should be abduced 80 to 100 degrees at a precise definedscapular or frontal plane.This method allows the diagnostician to judge:[10]
•• The horizontal alignment of the humerus head in respect to thesocket, and the lateral clavicle in respect to the acromion.
•• Lesions of the anterior and posterior socket border or of thetuberculum minus.
•• The eventual non-closure of the acromial apophysis.•• The coraco-humeral interval

Rotator cuff 16
Transaxillary projection. Schematic drawing.After "Orthopedic radiology: a practical
approach; Adam Greenspan; ISBN0-7817-1589-X, 9780781715898"
Y-projection
Y-projection conventional radiography
The lateral contour of the shoulder should be positioned in front of thefilm in a way that the longitudinal axis of the scapula continues parallelto the path of the rays.This method allows the diagnostician to judge:[10]
•• The horizontal centralization of the humerus head and socket.•• The osseous margins of the coraco-acromial arch and hence the
supraspinatus outlet canal.•• The shape of the acromionThis Y-projection can be traced back to Wijnblath’s 1933 publishedcavitas-en-face projection.[12]
It must be pointed out that this projection has a low tolerance for errorsand accordingly needs proper execution.[10]
Ultrasound
There are several solid advantages of ultrasound. It is relatively cheap,does not emit any radiation, is accessible, is capable of visualizingtissue function in real time and allows to the performing of provocativemaneuvers in order to replicate the patient’s pain. Those apparentbenefits have helped ultrasound become a common initial choice forassessing tendons and soft tissues. Limitations include, for example,the high degree of operator dependence and the inability to define pathologies in bones. One also has to have anextensive anatomical knowledge of the examined region and keep an open mind to normal variations and artifactscreated during the scan.[13] Although musculo-skeletal ultrasound training, like medical training in general, is a lifelong process, Kissin et al.suggest that rheumatologists who taught themselves how to manipulate ultrasound can use it just as well asinternational musculo-skeletal ultrasound experts to diagnose common rheumatic conditions.[14] After the introduction of high-frequency transducers in the mid-eighties, ultrasound has become a conventional toolfor taking accurate and precise images of the shoulder to support diagnosis.[15][16][17][18][19] Adequate for the examination are high-resolution, high-frequency transducers with a transmission frequency of 5,
7.5 and 10 MHz. To improve the focus on structures close to the skin an additional „water start-up length“ is advisable. During the examination the patient is asked to be seated, the affected arm is then adducted and the elbow

Rotator cuff 17
is bent to 90 degrees. Slow and cautious passive lateral and/or medial rotations have the effect of being able tovisualize different sections of the shoulder. In order to also demonstrate those parts which are hidden under theacromion in the neutral position, a maximum medial rotation with hyperextension behind the back is required.[20] To avoid the different tendon echogenicities caused by different instrument settings, Middleton compared thetendon’s echogenicity with that of the deltoid muscle, which is still lege artis.[21][22] Usually the echogenicity compared to the deltoid muscle is homogeneous intensified without dorsal echo extinction.Variability with reduced or intensified[23] echo has also been found in healthy tendons. Bilateral comparison is veryhelpful when distinguishing and setting boundaries between physiological variants and a possible pathologicalfinding. Degenerative changes at the rotator cuff often are found on both sides of the body. Consequently unilateraldifferences rather point to a pathological source and bilateral changes rather to a physiological variation.[24] In addition, a dynamic examination can help to differentiate between an ultrasound artifact and a real pathology.[25] To accurately evaluate the echogenicity of an ultrasound, one has to take into account the physical laws of reflection,absorption and dispersion. It is at all times important to acknowledge that the structures in the joint of the shoulderare not aligned in the transversal, coronal or sagittal plane, and that therefore during imaging of the shoulder thetransducer head has to be hold perpendicularly or parallel to the structures of interest. Otherwise the appearingechogenicity may not be evaluated.[26] Orientation-aid for the longitudinal plane: As an aid to orientation, it is advisable to begin the examination with the delineation of the acromion, as it is easy topalpate and it has an identifiable echo extinction. To adjust the longitudinal plane image the way it is known in thex-rays and the physical examination, the acromion has to be visible at the image border.[26] Orientation-aid for the transversal plane: Again it is advantageous to start above the acromion and then move the transducer to the humerus. The acromionecho extinction disappears and the wheel-like figure with almost concentric projection of the deltoid muscle,supraspinatus muscle tendon and humeral head-outline turns up as soon as the transducer is directed perpendicularlyand parallel to the acromion edge. Using the anterior transversal plane one can depict the intraarticular part of thelong head of the biceps brachii muscle. Additionally one can use the posterior transversal plane to depict theintersection of the infraspinatus muscle tendon and the posterior edge of the fossa.[26]
usual longitudinal front vision usual longitudinal backvision
usual transversalside vision
supraspinatustendon
acromion of the left shoulder in the left half of the image and vice versa. (Inorder to explore the entire tendon the examiner must move the transducer fromventral to dorsal perpendicular at the acromion axis. Either through a maximalmedial rotation or an according position of the transducer it is possible to seethe supra- infraspinatus tendon intersection.)
ventral right shoulderin the right half of theimage and vice versa.
infraspinatustendon
scapula spine of the rightshoulder in the left halfof the image and viceversa.
Longitudinal ultra sonography of thesupraspinatus tendon
Transversal ultra sonography of thesupraspinatus tendon

Rotator cuff 18
MRIOrthopedics established early the MRI as the tool of choice for joint- and soft tissue-imaging, because itsnon-invasiveness, the lack of radiation exposure, multi planar slicing possibilities and the high soft tissuecontrast.[27]
The MR Imaging should provide joint details to the treating orthopedist, to help him diagnose and decide the nextappropriate therapeutic step. To examine the shoulder, the patient is lying and the concerned arm is in lateralrotation. For signal detection it is recommended to use a surface-coil. To find pathologies of the rotator cuff in thebasic diagnostic investigation, T2-weighted sequences with fat-suppression or STIR sequences have proven value. Ingeneral, the examination should occur in the following three main planes: axial, oblique coronal and sagittal.[28]
Most morphological changes and injuries are sustained to the supraspinatus tendon. Traumatic rotator cuff changesare often located antero-superior, meanwhile degenerative changes more likely are supero-posterior.[29]
Tendons are predominantly composed of dense collagen fiber bundles. Because of their extreme short T2-relaxationtime they appear typically signal-weak, respectively, dark. Degenerative changes, inflammations and also partial andcomplete tears cause loss of the original tendon structure. Fatty deposits, mucous degeneration and hemorrhages leadto an increased intratendinal T1-image. Edema formations, inflammatory changes and ruptures increase the signalsin a T2-weighted image.[28]
Magic angle artifact
MRI. Magic angle artifact.
Erickson et al. noticed and described a typical artifact and gave the phenomenon thename „magic angle“. The „magic angle“ describes a changed T2-relaxation timedepending on the spatial orientation of the tissue to the main magnetic field. If partsof the tendon are located at the area of the magic angle at 55 degrees to the mainmagnetic field, their T2-relaxation time gets influenced and the signal heavilyintensified. Unluckily these artifacts occupy similar areas where clinical relevantpathologies are found. To avoid a wrong diagnosis it is recommended to excludethis phenomenon in a case of doubt through a heavy T2-weighted sequence or anadditional fat-suppression at a proton weighted sequence.[30]
MRA
While using MRI, true lesions at the rotator interval region between the parts of thesupraspinatus and subscapularis are all but impossible to distinguish from normalsynovium and capsule.[31]
In 1999, Weishaupt D. et al. reached through two readers a significant bettervisibility of pully lesions at the rotator interval and the expected location of thereflection pulley of the long biceps and subscapularis tendon on parasagittal(reader1/reader2 sensitivity: 86%/100%; specificity: 90%/70%) and axial(reader1/reader2 sensitivity: 86%/93%; specificity: 90%/80%) MRA images.[32]
When examining the rotator cuff, the MRA has a couple of advantages compared tothe native MRI. Through a fat suppressed T2-weighted spin echo, MRA canreproduce an extreme high fat-water-contrast, which helps to detect water-depositswith better damage diagnosis in structurally changed collagen fiber bundles.[33]

Rotator cuff 19
Additional images
Diagram of the human shoulderjoint
Suprascapular and axillary nerves of rightside, seen from behind.
Thesuprascapular,axillary, andradial nerves.
References[1] Tnation article Push-Ups, Face Pulls, and Shrugs ...for Strong and Healthy Shoulders! (http:/ / www. t-nation. com/ free_online_article/
sports_body_training_performance_repair/ pushups_face_pulls_and_shrugs) by Bill Hartman and Mike Robertson: The rotator cuff, of course.(Or for those of you from Indiana, that would be your "rotary cup").
[3][3] (video)[4][4] (video)[9][9] Hodler J et al.. Gelenkdiagnostik mit bildgebenden Verfahren. Stuttgart [etc.]. G. Thieme. 1992. ISBN 3-13-780501-5[10] Hedtmann A et al.. Imaging in evaluating rotator cuff tears. Orthopade. 2007 Sep;36(9):796-809. - (http:/ / www. springerlink. com/ content/
26l346817932h383/ )[11][11] Bandi W (1981) Die Läsion der Rotatorenmanschette. Helv Chir Acta 48:537-549[12][12] Wijnbladh H (1933) Zur Röntgendiagnose von Schulterluxationen. Chirurg 5:702[13] Broadhurst NA. Musculoskeletal ultrasound - used to best advantage. Aust Fam Physician. 2007 Jun;36(6):430-2. - free article(http:/ / www.
racgp. org. au/ afp/ 200706/ 200706broadhurst. pdf)[14] Kissin et al.. Self-directed learning of basic musculo-skeletal ultrasound among rheumatologists in the United States. Arthritis Care Res
(Hoboken). 2010 Feb;62(2):155-60 - (http:/ / www3. interscience. wiley. com/ journal/ 123236784/ abstract)[15] Allen GM, Wilson DJ, Eur J Ultrasound. 2001 Oct;14(1):3-9. Review - (http:/ / linkinghub. elsevier. com/ retrieve/ pii/
S0929826601001409)[16] Middleton WD, Edelstein G, et al. Sonographic detection of rotator cuff tears. Ajr American Journal of Roentgenology.
1985a;144(2):349–53. free article(http:/ / www. ajronline. org/ cgi/ reprint/ 144/ 2/ 349)[17] Middleton WD, Reinus WR, et al. Ultrasonographic evaluation of the rotator cuff and biceps tendon. Journal of Bone and Joint Surgery
American Volume. 1986;68(3):440–50.[18] Crass JR, Craig EV, et al. Ultrasonography of rotator cuff tears: a review of 500 diagnostic studies. Jcu J Clin Ultrasound.
1988;16(5):313–27.[19] Mack LA, Gannon MK, et al. Sonographic evaluation of the rotator cuff. Accuracy in patients without prior surgery. Clinical Orthopaedics
and Related Research. 1988a;234:21–7.[20][20] Thelen M. et al.. Radiologische Diagnostik der Verletzungen von Knochen und Gelenken. Stuttgart [etc.]. Georg Thieme. 1993. ISBN
3-13-778701-7[21][21] Middleton WD. et al.. Ultrasonography of the rotator cuff: technique and normal anatomy. J Ultrasound Med.. 1984 Dec;3(12):549-51[22] Middleton WD. et al.. Pitfalls of rotator cuff sonography. AJR AM J Roentgenol. 1986 Mar;146(3):555-60 @Katthagen BD. et al..
Schultersonographie. Stuttgart. ISBN 3-13-719401-6 - free article(http:/ / www. ajronline. org/ cgi/ reprint/ 146/ 3/ 555)[23][23] crass 1984 @Katthagen BD. et al.. Schultersonographie. Stuttgart. ISBN 3-13-719401-6[24][24] Middleton WD. et al.. Pitfalls of rotator cuff sonography. AJR AM J Roentgenol. 1986 Mar;146(3):555-60[25][25] Hedtmann A. et al.. Atlas und Lehrbuch der Schultersonographie. Stuttgart. 1988@ Hodler J et al.. Gelenkdiagnostik mit bildgebenden
Verfahren. Stuttgart [etc.]. G. Thieme. 1992. ISBN 3-13-780501-5[26][26] Katthagen BD. et al.. Schultersonographie. Stuttgart. ISBN 3-13-719401-6[27] Trattnig S. et al.. High-field and ultrahigh-field magnetic resonance imaging: new possibilities for imaging joints. Z Rheumatol. 2006
Dec;65(8):681-7 - (http:/ / www. springerlink. com/ content/ 54r55191m43327j5/ )[28] Romaneehsen B. et al.. MR imaging of tendon diseases. Exemplified using the examples of rotator cuff, epicondylitis and achillodynia.
Orthopade. 2005 Jun;34(6):543-9 - (http:/ / www. springerlink. com/ content/ r60654q134376711/ )

Rotator cuff 20
[29][29] Nové-Josserand L, Gerber C, Walch G (1997) Lesions of the antero-superior rotator cuff. Lippincott-Raven, Philadelphia[30] Erickson SJ, Cox IH, Hyde JS, Car re ra GF, Strandt JA, Estkowski LD (1991) Effect of tendon orientation on MR imaging signal intensity:
a manifestation of the „magic angle“ phenomenon. Radiology 181:389–393[31] Seeger LL, Lubowitz J, Thomas BJ (1993) Case report 815: Tear of the rotator interval. Skeletal Radiol 22(8): 615–617[32] Weishaupt D, Zanetti M, Tanner A et al. (1999) Lesions of the reflection pulley of the long biceps tendon. MR arthrographic findings. Invest
Radiol 34: 463–469 @Hedtmann A. et al.. Imaging in evaluating rotator cuff tears. Orthopade. 2007 Sep;36(9):796-809 - (http:/ / www.springerlink. com/ content/ 26l346817932h383/ )
[33] Palmer WE, Brown JH, Rosenthal DI (1993) Rotator cuff: evaluation with fat-suppressed MR arthrography.Radiology 188:683–687
Article Sources and Contributors 21
Article Sources and ContributorsShoulder Source: http://en.wikipedia.org/w/index.php?oldid=564664668 Contributors: A Stop at Willoughby, Achowat, AdiJapan, Akamad, Akanemoto, Al tally, AnakngAraw, Arcadian,Auntof6, Badgettrg, Barzkar, Basharh, Beth ohara, Bhadani, Borgx, Bryan H Bell, COMPFUNK2, Carlos T. Blackburn, Chsf, Clark89, Clarkcj12, Conquerist, Darren Snoogy, Deathawk, Delldot,Diberri, Dictabeard, Dirkbenade, Discospinster, DoctorReiux, Drdrby, Drlesbailey, Drmies, Dura Mater, Dwst, EWikist, Ec5618, Edward, Eep², Enochlau, Eribro, Erics, Esowteric, Faigl.ladislav,Fama Clamosa, Fleagle11, GamingFreek101, GazMbe, Gdaniel111, Gdo01, Gjd001, Graichen, GregorB, Grylliade, Guanaco, Gurch, HDS, Hu12, Hughcharlesparker, Jahnavisatyan, Jfdwolff,Jim1138, Jncraton, Julesd, Kbh3rd, Keitei, LedgendGamer, LifeStar, LokiClock, LucasVB, M karzarj, MONGO, MW3915, Mac Davis, MacedonianBoy, Marek69, Massimo Macconi, Matsen,Maxim, Maxxicum, Mayoife, Mcstrother, Merlin-UK, Mgnbar, Mikael Häggström, Miquonranger03, Mjanja, Mulad, Myself0101, Narom, NellieBly, Newone, Ngoquangduong, Nitroshockwave,Nono64, Norden83, Nposs, Nurg, Nwbeeson, Nyttend, Ohnoitsjamie, Orthosurgeon, Oxymoron83, Palnatoke, Patiwat, Patrick, Patxi lurra, Pb30, PhilipBembridge, Piet Delport, Quadell,RDBrown, RSatUSZ, Rajkiandris, Ranveig, Raven in Orbit, Raygun man, Rebroad, Rivertorch, RockMFR, Romanm, Rpf, Saganaki-, Sardaukar Blackfang, Shobhitha, Snoyes, Symane,Termininja, The Anome, The Minister of War, The Rationalist, TheWama, Theone00, Thrissel, TimonyCrickets, Tobby72, Tristanb, Unyoyega, V.narsikar, Vchimpanzee, Vclaw, WLU,Whhalbert, Wi-king, Wireless Keyboard, Yekrats, Yidisheryid, 206 anonymous edits
Glenohumeral joint Source: http://en.wikipedia.org/w/index.php?oldid=570678297 Contributors: -Marcus-, AB, Ajp, Anatomist90, Arcadian, Barzkar, BirgitteSB, BruceBlaus, Daleee, DamianYerrick, Dr. ambitious, Drgarden, Drmies, Eleassar, Fama Clamosa, GameKeeper, GazMbe, Graham87, Groyolo, Guoguo12, Gurch, Hughcharlesparker, InvictaHOG, JakobSteenberg, Kasschei,KnightLago, LokiClock, Madhero88, Mandarax, Nono64, Nurg, Oliver Münz, Pearle, Petruss, Prsephone1674, RSatUSZ, Raven in Orbit, Robert.Allen, Root4(one), Saltanat ebli, Sandr0,Savabubble, Shawnc, Shellystander, Stamboltsyan, Str13, Visium, Woohookitty, 23 anonymous edits
Rotator cuff Source: http://en.wikipedia.org/w/index.php?oldid=568890260 Contributors: Abbaroodle, Alansohn, AlbertBickford, Allens, Alwebuser, Amerikenny, Angela26, AnthonyAppleyard, Arcadian, BD2412, Badgettrg, Basicsharingwatuknow!, Beigemush, Boothy443, Bubba73, Calabe1992, Catpochi, Chris Capoccia, Cloudedcrimson, Colin Kimbrell, Collinpark,CommonsDelinker, Cshay, DanB, Danandlollie, Dangling Conversation, Davidhaha, Dbizz, Deathawk, Dictabeard, Download, Editor randy, Esrever, FXShannon, Fama Clamosa, Fraggle81,FutureNJGov, GamingFreek101, Gareth Griffith-Jones, Glacian79, Grafen, Grayshi, GregorB, Grey Knight 1ce, Hraefen, Imesj, Infinity95695, J.delanoy, Jack Greenmaven, Jack Schlederer,JakobSteenberg, Jehochman, Jfdwolff, Jmh649, Jncraton, Julesd, KC Panchal, KGV, Kevin.cohen, Kghusker, KnightRider, LedgendGamer, Lenny Kaufman, Leonard glas, Libbydelux, Loco7,Magioladitis, Matsen, MatthewS1973, Mawa, Mme Mim, MrOllie, Mzkitteh, Naniwako, Nick123, Nishanthb, Opelio, Osm agha, Outside Media, PaganPliskin, Philippe, Piano non troppo,Pinethicket, Porco-esphino, Protenpinner, Quintote, RSatUSZ, RaseaC, Raven in Orbit, Rgoodwin13, Rich Farmbrough, Rjwilmsi, Roger Roger, Ryuko2001, SMC, SaintedLegion, SasukeSarutobi, Sballdaway, Scarian, SchreiberBike, ScottDT1, Steve p, StevenLewis, Stismail, Sue Douglasss, Swim360, TaalVerbeteraar, Tamfang, Tanabesan, Tarek, Tbhotch, Tentinator, Texx064,Thestraycat57, Tristanb, User At Work, Vasi, Versus22, WLU, Wegesrand, Wiz9999, Woohookitty, Wouterstomp, WriterHound, Y12J, Yunshui, Zappernapper, Ziphon, 245 ,יוסי anonymousedits

Image Sources, Licenses and Contributors 22
Image Sources, Licenses and ContributorsFile:Shoulderjoint.PNG Source: http://en.wikipedia.org/w/index.php?title=File:Shoulderjoint.PNG License: Public Domain Contributors: National Institute Of Arthritis And MusculoskeletalAnd Skin Diseases (NIAMS)File:Gray327.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray327.png License: Public Domain Contributors: Fama Clamosa, Grook Da Oger, Mats Halldin, Phyzome, Was abee, 1 anonymous editsFile:Leonardo da Vinci - Anatomical studies of the shoulder - WGA12824.jpg Source:http://en.wikipedia.org/w/index.php?title=File:Leonardo_da_Vinci_-_Anatomical_studies_of_the_shoulder_-_WGA12824.jpg License: Public Domain Contributors: Beria, Jacklee, Pe-Jo,Shakko, Was a beeFile:Gray326.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray326.png License: Public Domain Contributors: Hellerhoff, Mats Halldin, Phyzome, Was a bee, 2 anonymouseditsFile:shoulder_2.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Shoulder_2.jpg License: Public Domain Contributors: GraichenFile:Blausen 0797 ShoulderJoint.png Source: http://en.wikipedia.org/w/index.php?title=File:Blausen_0797_ShoulderJoint.png License: Creative Commons Attribution 3.0 Contributors:User:BruceBlausImage:Shoulderjoint.PNG Source: http://en.wikipedia.org/w/index.php?title=File:Shoulderjoint.PNG License: Public Domain Contributors: National Institute Of Arthritis AndMusculoskeletal And Skin Diseases (NIAMS)Image:Gray326.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray326.png License: Public Domain Contributors: Hellerhoff, Mats Halldin, Phyzome, Was a bee, 2 anonymouseditsFile:Slide1KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide1KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide2KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide2KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide5KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide5KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide7KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide7KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide8KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide8KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide9KKKK.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide9KKKK.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Gray412.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray412.png License: Public Domain Contributors: Arcadian, Was a beeFile:Gray521.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray521.png License: Public Domain Contributors: Arcadian, Hellerhoff, Mats Halldin, Was a beeImage:side-lying abduction begin.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Side-lying_abduction_begin.jpg License: Public Domain Contributors: User:Porco-esphinoImage:side-lying abduction end.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Side-lying_abduction_end.jpg License: Public Domain Contributors: User:Porco-esphinoImage:Propped external rotator begin.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Propped_external_rotator_begin.jpg License: Public Domain Contributors:User:Porco-esphinoImage:Propped external rotator end1.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Propped_external_rotator_end1.jpg License: Public Domain Contributors:User:Porco-esphinoImage:LRIR begin.jpg Source: http://en.wikipedia.org/w/index.php?title=File:LRIR_begin.jpg License: Public Domain Contributors: User:Porco-esphinoImage:LRIR end.jpg Source: http://en.wikipedia.org/w/index.php?title=File:LRIR_end.jpg License: Public Domain Contributors: User:Porco-esphinoFile:CR. shoulder x-ray, a.p..jpg Source: http://en.wikipedia.org/w/index.php?title=File:CR._shoulder_x-ray,_a.p..jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors:User:RSatUSZImage:Transaxillary CR shoulder.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Transaxillary_CR_shoulder.jpg License: Creative Commons Attribution-Share Alike Contributors: RSatUSZFile:Transaxillary projection. Schematic drawing..jpg Source: http://en.wikipedia.org/w/index.php?title=File:Transaxillary_projection._Schematic_drawing..jpg License: Creative CommonsAttribution-Sharealike 3.0 Contributors: User:RSatUSZImage:Y CR shoulder.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Y_CR_shoulder.jpg License: Creative Commons Attribution-Share Alike Contributors: RSatUSZImage:Longitudinal US supraspinatus.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Longitudinal_US_supraspinatus.jpg License: Creative Commons Attribution-Share Alike Contributors: RSatUSZImage:Transversal US supraspinatus.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Transversal_US_supraspinatus.jpg License: Creative Commons Attribution-Share Alike Contributors: RSatUSZFile:Magic angle artifact.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Magic_angle_artifact.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors:User:RSatUSZImage:Gray810.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray810.png License: Public Domain Contributors: Arcadian, Cookie, Hellerhoff, Jacklee, Mats Halldin, Was a beeImage:Gray818.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray818.png License: Public Domain Contributors: Arcadian, Magnus Manske, Was a bee, Wknight94, 1anonymous edits

License 23
LicenseCreative Commons Attribution-Share Alike 3.0 Unported//creativecommons.org/licenses/by-sa/3.0/