THE SCIENCE OF NUTRITION SERIES
28
Lecture 8 – Dietary Approaches Part 2 1 THE SCIENCE OF NUTRITION SERIES LECTURE 8 – SON DIETARY APPROACHES – PART 2
Transcript of THE SCIENCE OF NUTRITION SERIES
Lecture 8 – Dietary Approaches Part 2 1
THE SCIENCE OF NUTRITION SERIES
LECTURE 8 – SON
DIETARY APPROACHES – PART 2

Lecture 8 – Dietary Approaches Part 2 2
Lecture 8 – Dietary Approaches Part 2 3
CONTENTS
INTRODUCTION - THERAPEUTIC DIETS
DETOXIFICATION DIETS
FASTING
ALLERGY EXCLUSION DIETS
LOW-CARBOHYDRATE DIETS
PRITIKIN DIET
HIGH-FIBRE DIET
THE GERSON DIET
LOW-SODIUM DIET
LOW-POTASSIUM DIET
REFERENCES

Lecture 8 – Dietary Approaches Part 2 4
Lecture 8 – Dietary Approaches Part 2 5
INTRODUCTION - THERAPEUTIC DIETS For the most part, the dietary approaches discussed in booklet 1 of this module are
used as every-day, long-term diets to maintain good health. The diets we will discuss
next are termed ‘therapeutic’ because they are typically done for a short period to bring the body back to balance, or to reverse adverse physical symptoms.
The therapeutic diets we will be discussing include: Detoxificaion Diets
Fasting
Allergy Exclusion Diets
Low-Carbohydrate weight loss diet
Pritikin Diet
High fibre diets
The Gerson Diet
Low-sodium and Low-potassium diets
DETOXIFICATION DIETS In your Nutrition Physiology I module, we discussed the process of detoxification. By
now, you should have a general understanding of the relationship between toxic
burden and disease in our bodies (I f you would like a review of this, refer to: Nutr.
Phys. Part 1, booklet 2). We remember that the liver is the key organ of
detoxification, and that other organs contribute as well. The liver’s role is to chemically alter toxins to make them more water-soluble. These toxins are then
excreted through the urine or faeces. Other avenues of elimination include the lungs
and skin
The detoxification system works by eliminating toxins through:
1. Neutralizing them (by chemical modification)
2. Excreting them v ia urine, faeces, lungs and skin.
The primary organs involved are the liver, intestine and kidneys. Other
tissues include the skin, lungs, lymphatic system and gall bladder.
Good health is maintained by consuming a diet that balances building foods (like
protein foods) and cleansing foods (like high-fibre vegetables). Each day we can
consume a balanced variety of these food types. There are also larger cycles
where we might do more building (say in the winter time) or more cleansing (in
the summertime). By honouring these natural cycles, the body can stay both
well-nourished and free of excess toxins.
At certain times, it is helpful to focus on the detoxification process. This is most
commonly done at the change of each season, particular the spring and autumn
equinox. There are a variety of books and methods of detoxification. Generally,
a detox diet can be as simple as cutting out the junk and increasing fluids,
nutrient-dense and high-fibre foods. It is safe for all people to follow, if one
modifies it to their needs.
Lecture 8 – Dietary Approaches Part 2 6
Why do a detox? One may choose to do a detox diet after a
period of poor eating habits, excessive
drinking or during a transition point in their
lives. There are times when all of us feel the
effects of not-so-healthy liv ing and feel we
need a good clean out.
When a detox diet may not be a good idea
As an individual or a health professional, it is important to know when NOT to advise
a detox diet.
Eating disorders: Some individuals have eating disorders where they are very
restrictive with their foods (such as anorexia nervosa). Imposing a detox diet
may simply re-enforce their restrictive behaviour and may not be appropriate
at the time. Others who suffer from compulsive/binge eating may find a
detox very calming and focusing.
Pregnant and lactating women need to be cautious about taking on a detox
diet. Not only do they have increased nutritional needs, but when toxins are
released, they can harm their child. It is highly advised for a woman to follow
a detoxification programme some months BEFORE conception. However, she
will still benefit from a moderate detox programme which simply excludes
harmful chemicals, sugar and junk foods and includes more water, fibre, fruits and vegetables in her diet.
Examples of how detox diets can vary
For a robust person: Follow the detox guidelines and rely solely on plant
protein sources to minimise build-up from excess protein. Also avoid saturated
fat and include lighter fats such as olive oil, avocados, nuts and seeds.
Consider a fast.
For a more deficient person: Follow the guidelines, but don’t restrict your intake. Include a moderate amount of building foods such as fish or organic
chicken each day. Also, include more cooked foods than raw foods.
There are common threads of a good ‘detox’ based on what we know about how our body eliminates wastes.
Indications that it might be time to
detox Skin eruptions
Constipation
Poor digestion
Excess gas
Bad breath
Achy joints
Low energy
Headaches
Insomnia
Fuzzy head
Lack of concentration
Lecture 8 – Dietary Approaches Part 2 7
A good detoxification regime
Restricts toxic chemicals such as alcohol, caffeine, drugs, additives and
preservatives.
Minimises or restricts heavy building foods such as red meat, other animal
proteins, dairy foods and eggs.
Minimises or restricts hard-to-digest foods such as wheat and refined grains
Restricts sodium, sugar and other sweeteners.
Includes adequate fluids to help flush toxins from the body
Includes adequate fibre to promote bile excretion and support colon
microflora
Emphasises moderate exercise to promote lymph circulation, oxygenation of
the lungs and sweating.
Emphasises other detoxification support methods such as colonics, fasting,
massage, nutritional and herbal support.
In order for the to rid itself of toxins, one must
Get the toxins from cells to the liver/kidney which requires physical movement
to move lymph (exercise, massage)
Provide the liver with adequate nutrients in order to process all the toxins (see
Detoxification section in Nut Phys I )
Have good bile secretion and bowel function (fibre, fluids, exercise, moderate
fat intake, herbal support)
Drink enough water to provide the medium through which the kidney can
release toxins.
Common side effects of ‘detoxing’
Headaches
Insomnia
Sensitivity to cold
Diarrhoea
Skin rashes
Feeling ‘flu-ish’ or tired
These can all be the side effects of your body eliminating toxins. Rest, warm baths, and extra attention to the process can help support you until they subside. They
shouldn’t last more than 3 days.
A detox is best done for 5-30 days. Often it is desirable to fast at some point during
your detox. While the detoxification process is slow and steady, providing
nourishment for your liver while supporting the elimination process, a fast will speed
things up a bit. After at least 3 days on a ‘detox diet’, a 1-3 day fast will expedite the
mobilization of toxins from your cells and their elimination.

Lecture 8 – Dietary Approaches Part 2 8
FASTING
Fasting is often associated with restriction and weight-loss. In a fast we deprive
ourselves, giv ing it a negative feeling. People often comment that when
undergoing a fast with a positive attitude, say when on a meditation retreat, they
feel nourished in deep way, rather than deprived. Religions such as Christianity,
Judaism and Eastern religions have encouraged fasting for a variety of reasons,
such as penitence, preparation for ceremony, purification, mourning, sacrifice and
union with god and the enhancement of knowledge and powers. The Essenes
believe that our body – our temple – must be purified for God to reside there.
But from a physiological perspective, Elson Haas, in his book Staying Healthy
with Nutrition, writes that ‘Fasting is the single greatest natural healing therapy.’ Indeed, fasting is used by all the ancient
healing traditions. Today, fasting can be
a marvellous tool with diseases of excess,
characteristic of our overconsuming
society. Physically it can reduce the toxic
load in our bodies. Equally as important,
it helps make us aware of our relationship
with hunger and food. Drs Murray and
Pizzorno state that fasting is one of the
quickest ways to increase elimination of
wastes and enhance the healing
processes of the body. Although
therapeutic fasting is one of the oldest
known therapies, it has largely been ignored by the medical community.
Paul Pitchford discusses fasting and purification methods at length in ‘Healing with
Whole Foods’. He reminds us that the word ‘fast’ itself indicates an important feature of a fast. It signifies a speeding up of the cleansing and renewal process
by slowing down the normal digestive routine.’ In this section, he rates some more gradual fasts which include some solid foods. Take a look at this section, in
particular note indications for recommending one type of fast over another.
Supportive reading: Review Fasting in Healing with Whole Foods
Fasting is a tool in detoxification. A true fast
restricts solid foods and takes water only. But
many feel that juice fasts are safer, and
possibly more conducive to detoxification, as
they can provide nutrients essential for the liver.
Animals instinctively fast when they are sick.
Often young children will refuse food (much to
the confusion of their parents) as they sense the
onset of illness.
Fasting as a Spiritual Tool Fasting is commonly used in spiritual
traditions. In yogic traditions, fasting is
used as a method of ‘tapas’. Tapas (a
sanskrit word) is thought of as creating
heat, burning up impurities, purification,
single-minded focus. In the Yoga-Sutras
of Patanjali, fasting is thought to teach us
why we eat. It teaches us that it is not
food we crave, but comfort. By fasting,
they say we are encouraged to look not
outwards towards food for this comfort,
but inwards to our deeper Self, or towards
‘God’. Buddhist traditions such as Vipassina use it to enhance our
awareness/mindfulness during some of
our most commonplace activities.
PCB Detoxification American Journal of Industrial
Medicine in 1984 reported a study in
which patients who had ingested rice
oil contaminated with
polychlorinated-biphenyls (PCBs)
found ‘dramatic’ relief after undergoing seven-to-10 day fasts.
Thus indicating its power in promoting
detoxification.
Lecture 8 – Dietary Approaches Part 2 9
Benefits of fasting
Acts as a catalyst for change
Supports a greater awareness and mindfulness (spiritual and otherwise)
Blood and lymph can clear toxins from tissues
Liver can spend more time detoxifying stored toxins when it’s not dealing with the process of digestion and absorption of food.
Increases release of toxins from the colon, kidneys, lungs and skin.
Fasting can be done unsupervised for up to 3-5 days. Many do longer fasts, but
these must be monitored for safety. Many people experience a ‘healing crisis’ during which old symptoms may reoccur, or new detoxification symptoms may
appear. They usually last 2-4 days and as long as they do not worsen, are not
problems other than the discomfort they cause. Watch for severe symptoms such as
fainting, heart arrhythmias or bleeding.
Fasting may be beneficial for the following conditions Colds
Flu
Bronchitis
Headaches
Constipation
Indigestion
Diarrhea
Food allergies
Environmental allergies
Asthma
Insomnia
Skin conditions
Arteriosclerosis
Coronary artery disease
Hypertension
Diabetes
Fever
Fatigue
Back pains
Mental illness
Obesity
Cancer Source: Staying Healthy with Nutrition by E. Haas
When to fast The natural times of fasting are spring and autumn. In Traditional Chinese
Medicine, fasting is recommended the ten days before and after the equinox.
Fasting can be difficult for the body in cold weather, so in colder climates, one
may want to shift the times slightly towards the warmer season. Alternately, some
do short (one day) fasts on a regular basis (fortnightly or monthly) or when on
retreat to support a meditation practice.

Lecture 8 – Dietary Approaches Part 2 10
How to fast
1. Phase one: Preparation and simplification. To keep the actual fast from being
so intense, and to minimize the healing crisis, one would do well to eat a pure,
healthy diet for a few days (like a ‘detox diet’). Avoid chemicals such as alcohol, caffeine, preservatives and heavier foods such as red meats, milk
products and eggs and increasing the amount of fluids, fruits and vegetables.
This begins a slow, nourishing detoxification process. Do this for at least 3 days
prior to fasting (longer if regular diet is particularly unhealthy).
2. Phase two: Fasting. This can be just water or a juice/broth of some type. Most
people do well to start with a one-day fast. Then subsequently (the next
season) do 2-3 days, working up to 5 days if they wish. This period is best done
when not involved in normal activ ities like working. I t is an ideal time for
reflection, meditation, exercise, massages and house cleaning projects.
3. Phase three: Breaking a fast. I t is important to make a gradual transition to a
regular diet, rather than planning a great feast on pizza and ice cream on
your first day off your fast. One can become very sick by overeating after a
week-long fast. Take a day or two to eat simply and minimally, going slowly
to allow your digestive system to readjust to food again. After a water fast,
start with juices and broths. With juice fasts, start with simple vegetable dishes
or fruits. The next day, move to well-cooked grains such as brown rice or
millet with vegetables.
Support during a fast
It is important to support the body and soul
during a fast. The liver detoxification process
needs support, which may require a
supplement. Some feel it helps to promote
bowel function, and recommend a fibre
supplement. To encourage the movement of
toxins around the body and out, one can
engage in activ ities like light exercise, massage,
dry skin brushing, colon irrigation. For the soul,
keep focused. I t’s best not to plan a hectic schedule during a fast, but stick to single
minded projects, and mindfulness/meditative
practices.
Fasting in Ayurvedic Medicine Vasant Lad, a well regarded
Ayurvedic physician and author of
books like Ayurveda, the Science
of Self-Healing, notes that people
should take their individual
constitutions into account when
planning a fast. In Ayurveda,
people will exhibit one or more
predominant ‘doshas’ which determine their constitution. Some
will flourish on long fasts, and
others must stick with shorter fasts.
Ayurveda also recommends herbs
and spices which have hot and
spicy attributes (like ginger, black
pepper and cayenne pepper)
help to kindle the agni, or
digestive fire and burn impurities.
Lecture 8 – Dietary Approaches Part 2 11
Ideas for support during a fast
Hazards of fasting
If overused, can create depletion and weakness, lower resistance.
Can temporarily lower thyroid levels
Female sex hormones may drop (with prolonged fasting), resulting in
delayed menses or amenorrhoea.
Cardiac arrhythmias can occur with prolonged fasting
When not to fast
Malnourished people should not fast. This includes overweight people who
are undernourished.
Those with fatigue resulting from nutrient deficiency (iron, B12, folic acid
related anaemia)
Those who are underweight
Pregnant or lactating women
Weak hearts (those with CHF)
Weakened immunity
Before or after surgery
Cancer patients who are experiencing wasting
Low blood pressure (may cause dizziness)
Cold weather (may not be a good time to fast)
Take multi v itamin/mineral
Vitamin C 1g 3x/day
1-2 Tbls fibre supplement at night before bed
Silymarin (milk thistle) at 70-210 mg 3x/day
Light exercise like walks or stretching
Massage, colon irrigation, dry skin brushing
Fresh juices
Extra rest
Lots of fluids
Meditation/mindfulness practice
Lecture 8 – Dietary Approaches Part 2 12
ALLERGY EXCLUSION DIETS
If you remember back a few modules to our study of food intolerances, we discussed
the use of an elimination diet as a method for determining which food(s) an
indiv idual was intolerant to. If you want a bit of background information, please
review that section, as well as the section on the General Adaptation Syndrome.
Background reading:
Nutritional Physiology Part 1 (book 2): Food Intolerances and elimination diets (p. 20)
Nutrition Physiology Part 2 (book 1): General Adaptation Syndrome (p. 14)
It can be very tricky to discern which foods (if any) are causing us to have
migraine headaches or other complaints. Often, people will attempt to figure it
out by avoiding the food for a few days or weeks to see if they have any
symptoms. However, we are usually not so strict, or do not know what categories
of foods to suspect in these cases. So our experiments, lacking in rigor, fail to give
us satisfactory answers. Often we just go back to the same old foods, or worse,
avoid all foods we suspect and live our lives in fear of wheat, dairy, citrus, peanuts
and other perfectly healthy foods.
Like it says in the tin, an exclusion diet is a diet which excludes one or more types
of food. These are done for one of two reasons, generally. Either to identify a
food which is causing an individual some problems, or to avoid a food which
someone has already identified as harmful. A ‘hypoallergenic’ diet refers to a diet which excludes the major food ‘allergens’. That is, the foods which most commonly cause people health problems.
The top 7 ‘food intolerance’ culprits include: Wheat
Other gluten grains
Dairy (cow’s milk products) Soya
Citrus
Corn
Eggs
The most common exclusion diet used by nutritionists is an elimination diet. I t is
done when a person is exhibiting symptoms related to food intolerance and wants
to identify the precise foods causing them trouble. Quite often, the symptoms
associated with food intolerance do not appear immediately after consumption,
but appear hours or even days later. Sometimes symptoms only appear after
enough of the offending food is eaten, so one egg may be fine, but 2 would bring
on symptoms. This makes it hard for the individual to assess the situation on their
own.
Lecture 8 – Dietary Approaches Part 2 13
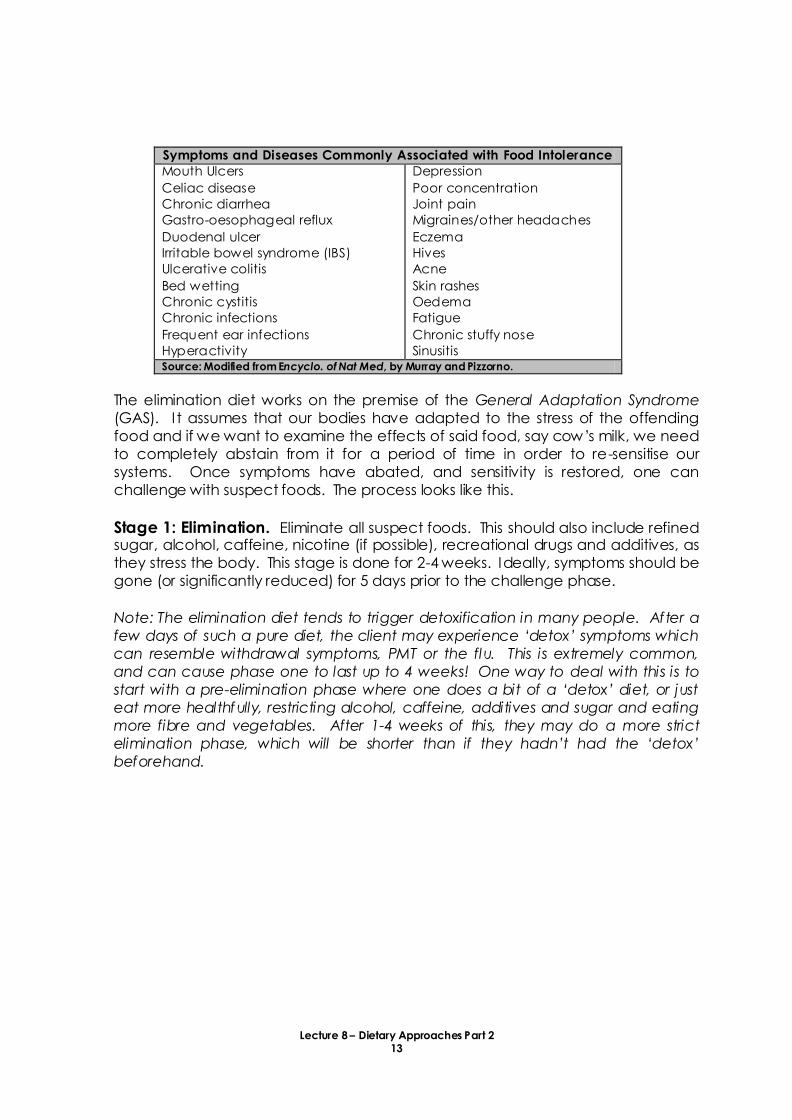
Symptoms and Diseases Commonly Associated with Food Intolerance
Mouth Ulcers
Celiac disease
Chronic diarrhea
Gastro-oesophageal reflux
Duodenal ulcer
Irritable bowel syndrome (IBS)
Ulcerative colitis
Bed wetting
Chronic cystitis
Chronic infections
Frequent ear infections
Hyperactivity
Depression
Poor concentration
Joint pain
Migraines/other headaches
Eczema
Hives
Acne
Skin rashes
Oedema
Fatigue
Chronic stuffy nose
Sinusitis Source: Modified from Encyclo. of Nat Med, by Murray and Pizzorno.
The elimination diet works on the premise of the General Adaptation Syndrome
(GAS). I t assumes that our bodies have adapted to the stress of the offending
food and if we want to examine the effects of said food, say cow’s milk, we need to completely abstain from it for a period of time in order to re-sensitise our
systems. Once symptoms have abated, and sensitivity is restored, one can
challenge with suspect foods. The process looks like this.
Stage 1: Elimination. Eliminate all suspect foods. This should also include refined sugar, alcohol, caffeine, nicotine (if possible), recreational drugs and additives, as
they stress the body. This stage is done for 2-4 weeks. Ideally, symptoms should be
gone (or significantly reduced) for 5 days prior to the challenge phase.
Note: The elimination diet tends to trigger detoxification in many people. After a
few days of such a pure diet, the client may experience ‘detox’ symptoms which can resemble withdrawal symptoms, PMT or the flu. This is extremely common,
and can cause phase one to last up to 4 weeks! One way to deal with this is to
start with a pre-elimination phase where one does a bit of a ‘detox’ diet, or just eat more healthfully, restricting alcohol, caffeine, additives and sugar and eating
more fibre and vegetables. After 1-4 weeks of this, they may do a more strict
elimination phase, which will be shorter than if they hadn’t had the ‘detox’ beforehand.

Lecture 8 – Dietary Approaches Part 2 14
Stage 2: Challenge. In this stage, the person challenges with one pure
food substance for 3 days, or until
there is a reaction. Pure food means
only one ingredient. For example, to
challenge wheat, you would use
bulgur wheat or 100% whole-wheat
noodles, rather than bread, as bread
may contain a variety of other
ingredients. Individual foods are
challenged one-at-a-time, and a
thorough diary is kept of what is
eaten, challenged and all possible
symptoms (including energy, moods,
bowel activity, digestion, skin
reactions, headaches, muscle pain).
The reaction is often not the original
complaint (i.e. a person who gets
migraine, may react with an unusual
skin rash instead).
Stage 3: Revise diet to avoid offending foods. This is a critical step. Often, when a person simply goes
in for blood tests or ‘food allergy testing’ they are told what to avoid, but not how to rebalance their diet. Here, the professional educates them on how to best
avoid the offending food and how they might plan their meals in order to achieve
balanced nutrition without. This is because the offending food is often frequently
consumed and a major macronutrient source.
Stage 4: Try the food again. Quite often, the food which once caused us so much trouble can be
reintroduced back into the diet. Usually, it has to be in small amounts. But once
the gut has healed and the body has found a better place of balance, the
offending food can come back in, allowing the individual to be more flexible in
situations such as holidays, eating our or travelling. Some recommend a ‘rotation diet’ to desensitise the individual to the food. This is beneficial to many. (Examples
of 4-day rotation diets can be found in Encyclopedia of Natural Medicine, by
Murray and PIzzorno)
All four stages are very important, so it is advisable to make a series of appointments
at each transition for the client to receive feedback and guidance.
The importance of keeping a DIARY This is critical for the whole process. Best
begun in stage 1 to assess the level of
original complaint. We tend to have a very
poor memory. It is fictional on a good day,
ESPECIALLY when it comes to what we ate or
how we felt a few days ago. By keeping a
diary, the individual (and nutrition
professional) can more objectively look
back and make connections between food
and symptom. Without it, the nutrition
professional only has the memory of the
client to base their recommendations on. In
stage 1, a general diet diary is kept with
more emphasis on undesirable symptoms,
bowel activity and activities. In stage 2,
challenge food is included, and a general
list of other foods eaten. Sometimes
symptoms could be complicated by skipped
meals, excessively heavy meals or stressful
life situations.
Lecture 8 – Dietary Approaches Part 2 15
Benefits When done under supervision and followed to the end, this can provide people
with a clear method to evaluate the effect of foods on their health. It can avoid
the common problem of people self-diagnosing food sensitivities and coming to
fear all foods unnecessarily.
Drawbacks Even when done to the letter, the results are sometimes not crystal-clear. Often, a
food must be challenged twice to be sure the reaction wasn’t due to someth ing
else. This is why the diary is so important. It allows the individual AND the
practitioner to look back with better objectivity to see how the body responded to
foods. Also, this process can take from 4-8 weeks. This is a significant amount of
time to have a restricted diet, particularly if one is avoiding and challenging a
number of different foods. A sincere commitment must be made and support
given by the practitioner and family members or the efforts will be in vain.
Different types of exclusion diets may avoid the following food groups:
Resources for these diets include books by Elson Haas, ‘The False Fat Diet’ Dr. Alan Gaby
Suzanne Meyer
Brostoff and Gamlin, Food Allergy and Intolerance
Murray and Pizzorno, Encyclopedia of Natural Medicine.
Main food allergens: wheat, other gluten grains, dairy, eggs, soya, corn, and
citrus.
Additional foods:
Vasoactive amines/tyramines: These compounds are culprits in triggering
migraine headaches and rosacea. Food sources include: Red wine, aged
cheeses, aged meats, chocolate, dried sausages, and smoked fish.
Salicylates: Salicylates are a very common component of many plant foods.
Salicylic acid is the active component in aspirin, and is considered generally
beneficial in foods, connected with lower cancer rates and anti-inflammatory
actions. However, some feel excessive amounts of this compound can lead
to headaches and joint pains. Foods high in salicylates include: Peppermint,
black tea, most spices, licorice, honey, port, rum and wine. Most people find
that if they ARE sensitive to salicylates, they can still eat foods which contain
them, they just have to find their threshold and avoid over consumption. The
challenge for this substance is usually pure aspirin.
Yeast-containing foods: Breads and bread products, mushrooms, cheeses,
vinegars (most pickles and condiments), beer, wine, Quorn and tempeh.
Peanuts, or other nuts eating regularly.
Beef, chicken, shellfish. Any food you eat every day or have cravings for.
Caffeine, alcohol, sugar, food colourings and artificial preservatives.
Lecture 8 – Dietary Approaches Part 2 16
LOW-CARBOHYDRATE DIETS
The low-carb diets have seen massive popularity between 2000-2004. The man who
made this method so popular was Dr. Robert Atkins, who first published these ideas to
the mainstream in 1992. His method, called ‘The Atkins Diet’, is based on the basics of carbohydrate metabolism and the actions of insulin.
Principles of the Atkins diet
When we eat a carbohydrate containing food, our bodies produce insulin in
response.
Insulin is an anabolic hormone which facilitates the storage of fat/energy.
Only in the absence of insulin, can we release stored fat and oxidize it.
Therefore, if we avoid (or minimise) carbohydrate foods, we reduce our
insulin secretion and promote ‘fat burning’.
The Atkins diet Stage one is characterised by strict avoidance of carbohydrates, and the
induction of ketosis. This creates an acidic environment for the body, but forces
the body to utilize stored fat for energy. Stage two allows for small increases in
carbohydrates which control how much insulin is produced. Generally, the Atkins
Diet does not place much emphasis on food quality. I t is mainly concerned with
how many grams of carbohydrate are in a food.
Other low-carb diets
Other popular low-carb diets have been ‘The Zone’ by Barry Sears, ‘The
Schwarzbein Principle’ by Diana Schwarzbein, and ‘The South Beach Diet’. They all use similar principles, with variations in their approaches. Diana Schwarzbein is
a practicing endocrinologist who promotes the use of whole, natural foods and tailors the diet to suit a few different types
of people.
The basic ‘low-carb’ approach is not as
extreme as one might think. Aside from the
phase 1 (induction phase) of the Atkins
diet, ‘low-carb’ is just a sexy way of advising we eat carbohydrates in
moderation, balanced with lots of non-
starchy vegetables, healthy fats and
protein sources. When you look at the
average diet these days, one sees a heavy
reliance of carbohydrates, particularly
simple carbohydrates. See box to the right.
The following 2 pages demonstrate the quantity of carbohydrates in certain foods
and how one might plan their diet while staying within fairly strict carbohydrate
restrictions.
A typical day demonstrates our
reliance on carbohydrates Breakfast: Cereal, milk, fruit/juice,
tea
Snack: Biscuits and tea
Lunch: Sandwich and fruit
Snack: Crisps or crackers
Dinner: pasta, rice or potatoes with
vegetables
Snack: Sweets
Carbohydrate foods are cheapest
and most convenient foods to
obtain or prepare. We tend to rely
on them to the exclusion of other
nutritious foods.
Lecture 8 – Dietary Approaches Part 2 17
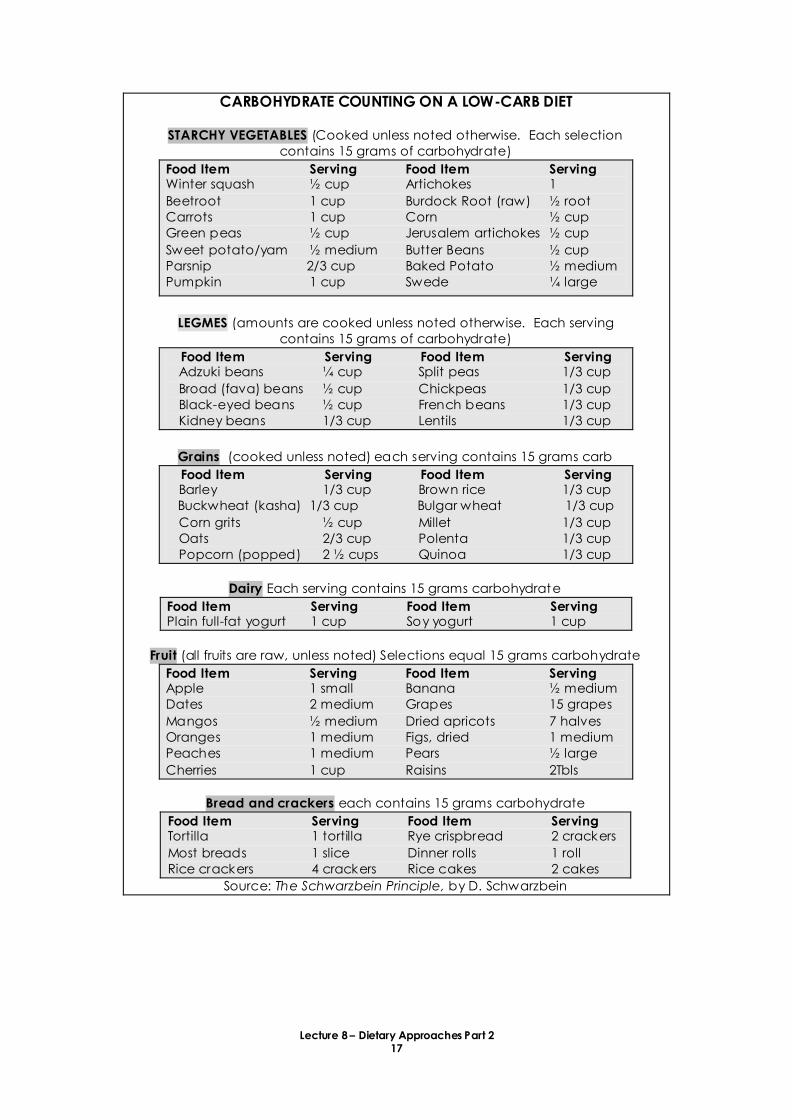
CARBOHYDRATE COUNTING ON A LOW-CARB DIET
STARCHY VEGETABLES (Cooked unless noted otherwise. Each selection
contains 15 grams of carbohydrate)
Food Item Serving Food Item Serving Winter squash ½ cup Artichokes 1
Beetroot 1 cup Burdock Root (raw) ½ root
Carrots 1 cup Corn ½ cup
Green peas ½ cup Jerusalem artichokes ½ cup
Sweet potato/yam ½ medium Butter Beans ½ cup
Parsnip 2/3 cup Baked Potato ½ medium
Pumpkin 1 cup Swede ¼ large
LEGMES (amounts are cooked unless noted otherwise. Each serving
contains 15 grams of carbohydrate)
Food Item Serving Food Item Serving Adzuki beans ¼ cup Split peas 1/3 cup
Broad (fava) beans ½ cup Chickpeas 1/3 cup
Black-eyed beans ½ cup French beans 1/3 cup
Kidney beans 1/3 cup Lentils 1/3 cup
Grains (cooked unless noted) each serving contains 15 grams carb
Food Item Serving Food Item Serving Barley 1/3 cup Brown rice 1/3 cup
Buckwheat (kasha) 1/3 cup Bulgar wheat 1/3 cup
Corn grits ½ cup Millet 1/3 cup
Oats 2/3 cup Polenta 1/3 cup
Popcorn (popped) 2 ½ cups Quinoa 1/3 cup
Dairy Each serving contains 15 grams carbohydrate
Food Item Serving Food Item Serving Plain full-fat yogurt 1 cup Soy yogurt 1 cup
Fruit (all fruits are raw, unless noted) Selections equal 15 grams carbohydrate
Food Item Serving Food Item Serving Apple 1 small Banana ½ medium
Dates 2 medium Grapes 15 grapes
Mangos ½ medium Dried apricots 7 halves
Oranges 1 medium Figs, dried 1 medium
Peaches 1 medium Pears ½ large
Cherries 1 cup Raisins 2Tbls
Bread and crackers each contains 15 grams carbohydrate
Food Item Serving Food Item Serving Tortilla 1 tortilla Rye crispbread 2 crackers
Most breads 1 slice Dinner rolls 1 roll
Rice crackers 4 crackers Rice cakes 2 cakes
Source: The Schwarzbein Principle, by D. Schwarzbein
Lecture 8 – Dietary Approaches Part 2 18
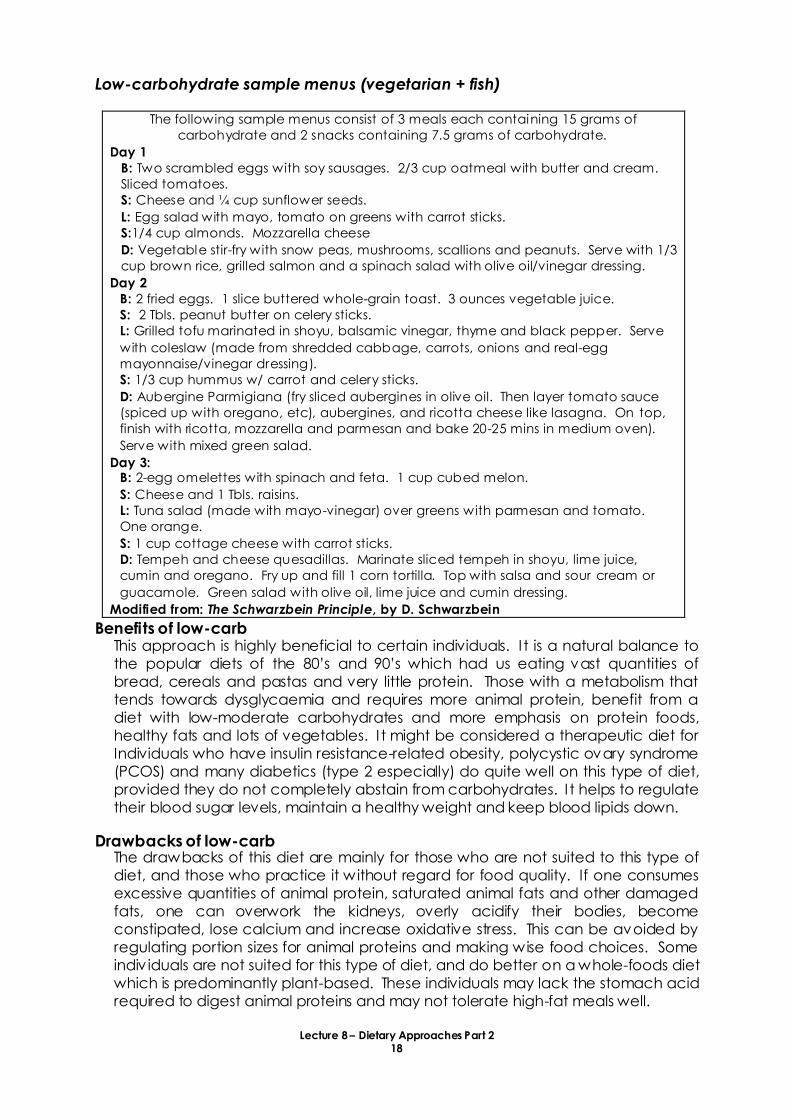
Low-carbohydrate sample menus (vegetarian + fish)
Benefits of low-carb This approach is highly beneficial to certain individuals. I t is a natural balance to
the popular diets of the 80’s and 90’s which had us eating vast quantities of bread, cereals and pastas and very little protein. Those with a metabolism that
tends towards dysglycaemia and requires more animal protein, benefit from a
diet with low-moderate carbohydrates and more emphasis on protein foods,
healthy fats and lots of vegetables. I t might be considered a therapeutic diet for
Individuals who have insulin resistance-related obesity, polycystic ovary syndrome
(PCOS) and many diabetics (type 2 especially) do quite well on this type of diet,
provided they do not completely abstain from carbohydrates. I t helps to regulate
their blood sugar levels, maintain a healthy weight and keep blood lipids down.
Drawbacks of low-carb The drawbacks of this diet are mainly for those who are not suited to this type of
diet, and those who practice it without regard for food quality. If one consumes
excessive quantities of animal protein, saturated animal fats and other damaged
fats, one can overwork the kidneys, overly acidify their bodies, become
constipated, lose calcium and increase oxidative stress. This can be avoided by
regulating portion sizes for animal proteins and making wise food choices. Some
indiv iduals are not suited for this type of diet, and do better on a whole-foods diet
which is predominantly plant-based. These individuals may lack the stomach acid
required to digest animal proteins and may not tolerate high-fat meals well.
The following sample menus consist of 3 meals each containing 15 grams of
carbohydrate and 2 snacks containing 7.5 grams of carbohydrate.
Day 1
B: Two scrambled eggs with soy sausages. 2/3 cup oatmeal with butter and cream.
Sliced tomatoes.
S: Cheese and ¼ cup sunflower seeds.
L: Egg salad with mayo, tomato on greens with carrot sticks.
S:1/4 cup almonds. Mozzarella cheese
D: Vegetable stir-fry with snow peas, mushrooms, scallions and peanuts. Serve with 1/3
cup brown rice, grilled salmon and a spinach salad with olive oil/vinegar dressing.
Day 2
B: 2 fried eggs. 1 slice buttered whole-grain toast. 3 ounces vegetable juice.
S: 2 Tbls. peanut butter on celery sticks.
L: Grilled tofu marinated in shoyu, balsamic vinegar, thyme and black pepper. Serve
with coleslaw (made from shredded cabbage, carrots, onions and real-egg
mayonnaise/vinegar dressing).
S: 1/3 cup hummus w/ carrot and celery sticks.
D: Aubergine Parmigiana (fry sliced aubergines in olive oil. Then layer tomato sauce
(spiced up with oregano, etc), aubergines, and ricotta cheese like lasagna. On top,
finish with ricotta, mozzarella and parmesan and bake 20-25 mins in medium oven).
Serve with mixed green salad.
Day 3: B: 2-egg omelettes with spinach and feta. 1 cup cubed melon.
S: Cheese and 1 Tbls. raisins.
L: Tuna salad (made with mayo-vinegar) over greens with parmesan and tomato.
One orange.
S: 1 cup cottage cheese with carrot sticks.
D: Tempeh and cheese quesadillas. Marinate sliced tempeh in shoyu, lime juice,
cumin and oregano. Fry up and fill 1 corn tortilla. Top with salsa and sour cream or
guacamole. Green salad with olive oil, lime juice and cumin dressing.
Modified from: The Schwarzbein Principle, by D. Schwarzbein
Lecture 8 – Dietary Approaches Part 2 19
PRITIKIN DIET On the other end of the weight-loss spectrum, we have the Pritikin Diet. Nathan
Pritikin, the late scientist, inventor and founder of the Pritikin Center in Santa Monica,
California, developed the ‘Pritikin Diet’ after he discovered a way to cure his own cardiovascular ailments through diet.
This diet is designed to counterbalance the standard American diet (SAD), which
leads to obesity, diabetes and heart disease. The SAD is high in fat, high in protein,
high in salt, high in sugar and low in fibre. The Pritikin Diet balances it by eliminating
all of the excesses of the former diet, forcing the body to use up its own stores and
come back to balance. Those adhering to it following a heart attack have reported
excellent results in the months after, reducing lipid levels and insulin requirements and
blood pressure.
The Pritikin Diet consists of (daily recommendations)
Whole grains, beans (except soya beans), vegetables (except avocados and
olives), fruits (except coconut), limited dried fruit
3 oz lean meat, skinless chicken or fish
One glass skim milk and 2 oz cottage cheese daily
Linden tea
Egg whites
Exercise
It Forbids
All fats, oils, avocados, olives, salty meats, full-fat dairy, soybeans, table salt and
prepared foods containing it, refined carbohydrates, caffeinated drinks, whole
eggs, egg yolks, alcohol and soft drinks.
Nutritional Breakdown
10% of calories from fats
10-12% of calories from proteins
80% of calories from complex carbohydrates
Benefits
Many people who have followed this diet have found their health improve
drastically. In people who formerly followed SAD, it increased their intake of fibre,
increased potassium/sodium ratio, increase vegetable intake and balanced their
tendency for a diet excessively high in fat and protein.
Drawbacks
Complete lack of added fats can lead to deficiencies in fat-soluble vitamins,
digestive disorders, lack of satiety and overeating carbohydrates and essential
fatty acid deficiencies. While in the short-term, it may quickly bring a person back
into health, in the long-term it may cause the opposite imbalances. Deficiencies,
coldness, lack of grounding and cravings for salt and fat may result in the long
term.
Lecture 8 – Dietary Approaches Part 2 20
HIGH FIBRE DIET
Dietary fibre was discussed at length in the macronutrient section as a
heterogeneous group of non-nutritive components of plants. That is, we can’t absorb them.
Some general properties of dietary fibre include: Some are soluble in water and some insoluble
Some are fermentable by colon microflora
Some speed up GI transit time and some slow it down
Some dietary fibre can bind bile acids, promoting their excretion
Fibre generally increases faecal bulk
Can bind up nutrients preventing their absorption (this can be beneficial or not)
Health issues A low-fibre diet is generally associated with a variety of adverse health situations (see table below). Numerous studies have demonstrated links between higher
fibre diets and better health. Of course, a high-fibre diet will naturally include lots
of whole grains, legumes, fruits and vegetables. These also contain multiple
vitamins, minerals and other phytonutrients prev iously discussed. It is difficult to
separate the effects of individual nutrients. However, some studies simply add
dietary fibre of various types and have demonstrated that it improves blood sugar
regulation in diabetics and non-diabetics.
Diseases highly associated with a low-fibre diet Metabolic Obesity, gout, diabetes, kidney stones, gallstones
Cardiovascular Hypertension, cerebrovascular disease, ischemic heart
disease, varicose veins, deep vein thrombosis, pulmonary
embolism
Colonic Constipation, appendicitis, diverticulosis, diverticulosis,
haemorrhoids, colon cancer, irritable bowel syndrome,
ulcerative colitis, Crohn’s disease
Other Dental caries, autoimmune disorders, pernicious anaemia,
multiple sclerosis, thyrotoxicosis, dermatological conditions. Source: Encyclo. of Nat. Med. by Murray and Pizzorno
Recommendations for fibre in the diet
Most people consume only 10-15grams of fibre each day. Most health professions
now recommend a diet which includes 25-35 grams of dietary fibre each day. This is easy to achieve when consuming a whole-foods diet rich in unprocessed
plant foods. In studies with constipation, greater than 50g of fibre per day did not
appear to improve bowel function any further, and may actually create problems
with abdominal distention and excessive flatulence.
Extra water is required with a high-fibre diet. Again, this is easily achieved by eating whole foods including cooked whole grains. The fruits and vegetable
contain a lot of water and cooking grains and legumes causes them to absorb
quite a bit of water proportional to their fibre content. The trouble comes when
people get their fibre from whole-grain breads, dry muslei, dry cereals or fibre
supplements which are lacking in water. This excess fibre without water can
cause gastric obstruction and faecal impaction. Therefore, if an individual with a
low-fibre diet and constipation wants to improve their lot, it is best to increase fibre
intake slowly and do so with attention to their hydration status.
Lecture 8 – Dietary Approaches Part 2 21
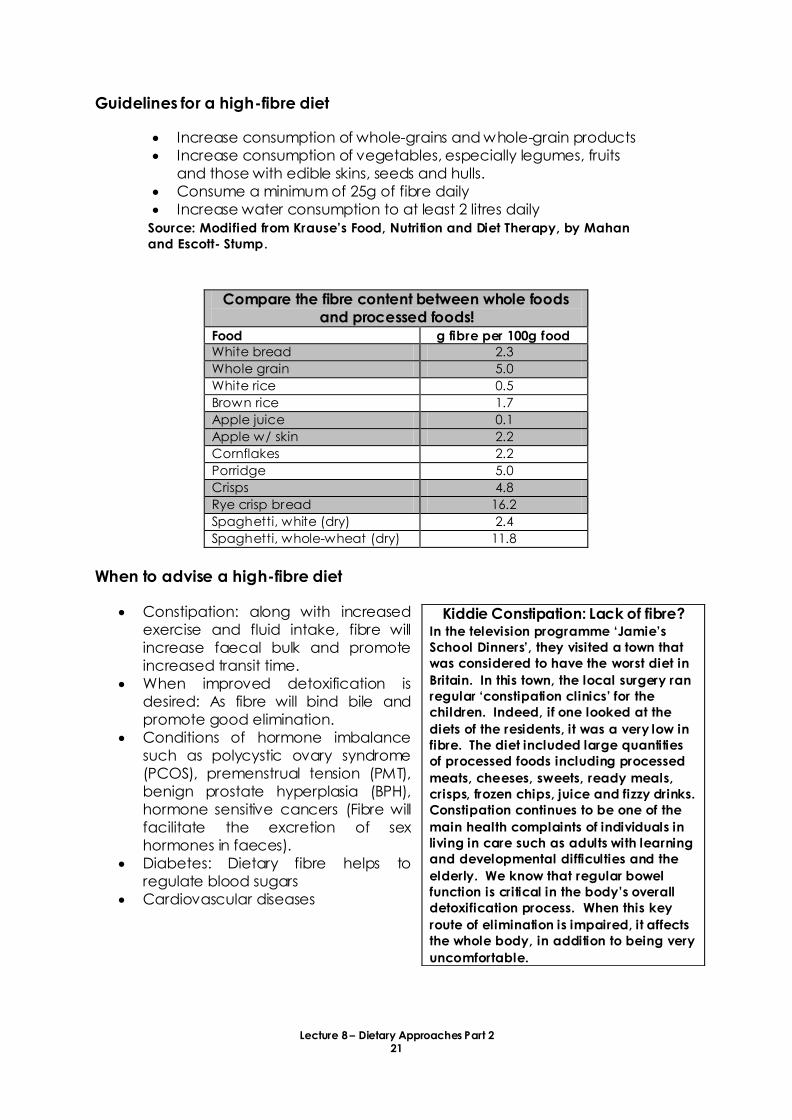
Guidelines for a high-fibre diet
Increase consumption of whole-grains and whole-grain products
Increase consumption of vegetables, especially legumes, fruits
and those with edible skins, seeds and hulls.
Consume a minimum of 25g of fibre daily
Increase water consumption to at least 2 litres daily
Source: Modified from Krause’s Food, Nutrition and Diet Therapy, by Mahan and Escott- Stump.
Compare the fibre content between whole foods
and processed foods!
Food g fibre per 100g food
White bread 2.3
Whole grain 5.0
White rice 0.5
Brown rice 1.7
Apple juice 0.1
Apple w/ skin 2.2
Cornflakes 2.2
Porridge 5.0
Crisps 4.8
Rye crisp bread 16.2
Spaghetti, white (dry) 2.4
Spaghetti, whole-wheat (dry) 11.8
When to advise a high-fibre diet
Constipation: along with increased
exercise and fluid intake, fibre will
increase faecal bulk and promote
increased transit time.
When improved detoxification is
desired: As fibre will bind bile and
promote good elimination.
Conditions of hormone imbalance
such as polycystic ovary syndrome
(PCOS), premenstrual tension (PMT),
benign prostate hyperplasia (BPH),
hormone sensitive cancers (Fibre will
facilitate the excretion of sex
hormones in faeces).
Diabetes: Dietary fibre helps to
regulate blood sugars
Cardiovascular diseases
Kiddie Constipation: Lack of fibre? In the television programme ‘Jamie’s School Dinners’, they visited a town that was considered to have the worst diet in
Britain. In this town, the local surgery ran
regular ‘constipation clinics’ for the children. Indeed, if one looked at the
diets of the residents, it was a very low in
fibre. The diet included large quantities
of processed foods including processed
meats, cheeses, sweets, ready meals,
crisps, frozen chips, juice and fizzy drinks.
Constipation continues to be one of the
main health complaints of individuals in
living in care such as adults with learning
and developmental difficulties and the
elderly. We know that regular bowel
function is critical in the body’s overall detoxification process. When this key
route of elimination is impaired, it affects
the whole body, in addition to being very
uncomfortable.

Lecture 8 – Dietary Approaches Part 2 22
When high-fibre is not appropriate
While the vast majority of us greatly benefit from a high-fibre diet, sometimes a
low-residue diet is called for. Residue refers to the amount of net faecal mass
remaining after the processes of food ingestion, absorption and fermentation. The
primary components of faecal residue are bacteria and water. The remaining
content includes dietary fibre, sloughed mucosal cells, mucous and varying
amounts of unabsorbed starches, sugars, protein and minerals.
Reduced faecal output is desired when the GI tract is restricted or obstructed. This
can include inflammatory bowel disease (sometimes), severe peptic ulcers or GI
surgeries. Small amounts of fibre with small particle sizes may be beneficial (i.e.
pureed vegetable soups). Individuals who have had a portion of their large
intestine removed and diverted to an external bag (ileostomy or colostomy) may
need to monitor their fibre intake. Increase fibre can lead to excess gas, and
poorly chewed fibrous foods can cause blockages in the stoma (the hole).
Historically, people advised those with colitis and other inflammatory bowel
diseases to follow a low-residue and low-fibre diet. While this may suit some, it is
recognized that optimal GI health can be achieved by including high fibre foods
which are more easily digestible (minimize gluten, soak/ferment grains, well-
cooked grains only) and identifying the specific foods which aggravate their
condition (through an elimination diet).

Lecture 8 – Dietary Approaches Part 2 23
THE GERSON DIET
The Gerson Institute is a non-profit organization founded in 1977 by Charlotte Gerson.
The aim is to heal and prevent chronic and degenerative diseases based on the
philosophy of Max Gerson, MD. He believed that degenerative diseases were
brought on by toxic and degraded food, water and air.
Proponents of the diet say it is designed to ‘boost your body’s own immune system to heal cancer, arthritis, heart disease, allergies and many other degenerative
diseases.’ I t works to cleanse and reactivate the body.
Emphasis of the Gerson Diet Most of the work focuses on cancer.
The diet works to restore cellular health in the entire body.
Its focus is to eliminate built-up waste and increase ‘oxygenation’ and strengthening the immune system so the body can better heal itself.
They believe too much sodium and too little potassium connects with disease
and water retention and restoring the Na/K balance is crucial to healing.
Extensive detoxification is employed to eliminate wastes. Enemas aid in
elimination of toxins.
What does the Gerson Diet look like? The Gerson Diet Advises a Daily intake of:
13 juices, raw carrot/apple and green-leaf juices each hour (using nearly 20
pounds of organic produce)
Three full vegetarian meals, using organic fruit, veg and whole grains. (Examples:
salad, cooked vegetables, baked potato, vegetable soup and juice)
Fresh fruit and fresh fruit desserts for snacking.
Medications used on the Gerson Diet Potassium compound
Lugol’s solution
Vitamin B12
Thyroid hormone
Injectable crude liver extract
Pancreatic enzymes
Enemas of coffee and/or chamomile
Caster oil
The Gerson Diet avoids heavy animal fats, excess protein, sodium and other toxins
Dr. Max Gerson has published extensively on diet therapy and cancer, and there are
many other published works evaluating the effectiveness of Gerson Therapy in other
degenerative diseases.
See http://gerson-research.org/overview.html for more details
Lecture 8 – Dietary Approaches Part 2 24
LOW-SODIUM DIET
One can look at low-sodium diets much the way we have looked at low-carb diets.
Our modern diets are so high in sodium, that for some, coming back to a sensible
diet has to be termed ‘low-sodium’. In fact, the 2 grams of sodium (per day) recommended by a moderately low-sodium diet is easily achieved on a whole-foods
diet which avoids processed foods and most commercial condiments. There are a
few disease states where low-sodium diets are advised that you may want to know
about.
Congestive heart failure (CHF)
CHF is a disease characterized by a mix of symptoms such as fatigue, shortness of
breath and congestion that occurs because the heart cannot pump blood
through the body adequately. This tends to occur as a result of cardiovascular
diseases which weaken the left ventricle of the heart. 5-year survival rates from
CHF are quite low, and involve significant nutritional management. For example,
because of inadequate blood flow, fluid balance is severely compromised.
Oedema develops, where the patient retains excessive amounts of sodium and
fluid in their tissues. Sodium restriction is advised in this case, maintaining a diet of
less than 2 grams sodium per day. Less sodium may be needed, but the
recommendation is to follow the least restrictive diet necessary to achieve the
desired results.
In CHF, people are often given diuretics to minimise oedema. It is important to
evaluate the type of diuretic to know if it is potassium sparing or not. Diuretics (like
hydrochlorothiazide) increase potassium excretion, which can lead to digitalis
toxicity, and may require an increase of high-potassium foods or supplements
Hypertension is another case when a low-sodium diet is often recommended.
However, we know that there is only a fraction of people with hypertension who
are ‘salt-sensitive’. (See micronutrient section for a discussion of other nutrient factors in hypertension.)
In order to determine if someone IS salt-sensitive, follow this protocol:
Step 1: Eat normally for a week, keep a diet diary and calculate sodium
intake. Take blood pressure, and if possible, determine urinary sodium
excretion.
Step 2: Consume a diet under 2g sodium per day for 2 weeks. Then measure
blood pressure.
If diastolic blood pressure is <90mg/Hg, the patient is salt-sensitive
If after one month on this diet, the diastolic blood pressure is >90 mmHg, with
a urinary NaCl of <34 mmol/24 hours, then patient is salt-resistant
Step 3: If salt-sensitive, stay on 2g/day diet, but add 300mg sodium per day,
taking blood pressure each day to determine when pressure goes up. This will
help determine sodium threshold.

Lecture 8 – Dietary Approaches Part 2 25
Acute or chronic renal failure
Is another incidence where sodium restriction is prudent. When in renal failure,
whether acute or chronic, most patients are monitored by their doctors for their
blood electrolytes (and cared for by a registered dietician in hospital). Both
sodium and potassium levels must be watched and these will vary depending on
dialysis and use of diuretics. It is recommended that those in renal failure observe
a diet that contains 2 grams sodium per day, balanced with fluid intake.
Congestive heart failure (CHF) is a disease characterized by a mix of symptoms
such as fatigue, shortness of breath and congestion that occurs because the
heart cannot pump blood through the body adequately. This tends to occur as a
result of cardiovascular diseases which weaken the left ventricle of the heart. 5-
year survival rates from CHF are quite low, and involve significant nutritional
management. For example, because of inadequate blood flow, fluid balance is
severely compromised. Oedema develops, where the patient retains excessive
amounts of sodium and fluid in their tissues. Sodium restriction is advised in this
case, maintaining a diet of less than 2 grams sodium per day. Less sodium may be
needed, but the recommendation is to follow the least restrictive diet necessary to
achieve the desired results.
In CHF, people are often given diuretics to minimise oedema. It is important to
evaluate the type of diuretic to know if it is potassium sparing or not. Diuretics (like
hydrochlorothiazide) increase potassium excretion, which can lead to digitalis
toxicity, and may require an increase of high-potassium foods or supplements
Lecture 8 – Dietary Approaches Part 2 26
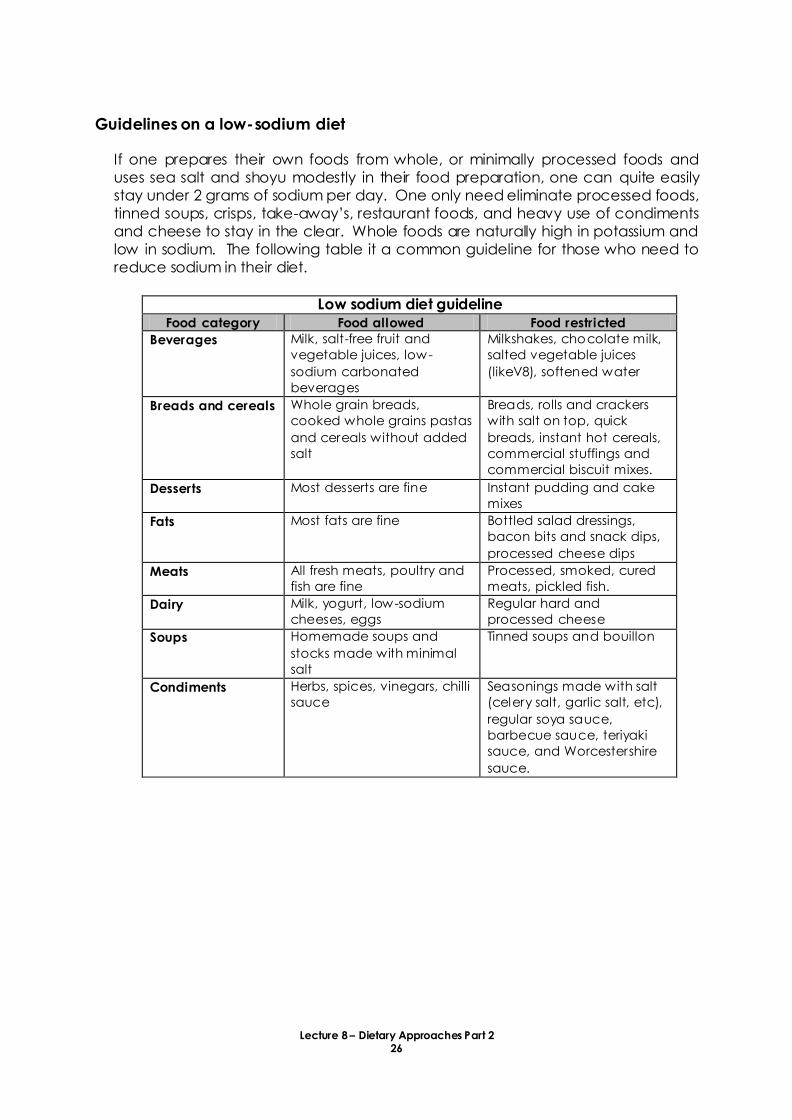
Guidelines on a low-sodium diet
If one prepares their own foods from whole, or minimally processed foods and
uses sea salt and shoyu modestly in their food preparation, one can quite easily
stay under 2 grams of sodium per day. One only need eliminate processed foods,
tinned soups, crisps, take-away’s, restaurant foods, and heavy use of condiments and cheese to stay in the clear. Whole foods are naturally high in potassium and
low in sodium. The following table it a common guideline for those who need to
reduce sodium in their diet.
Low sodium diet guideline
Food category Food allowed Food restricted
Beverages Milk, salt-free fruit and
vegetable juices, low-
sodium carbonated
beverages
Milkshakes, chocolate milk,
salted vegetable juices
(likeV8), softened water
Breads and cereals Whole grain breads,
cooked whole grains pastas
and cereals without added
salt
Breads, rolls and crackers
with salt on top, quick
breads, instant hot cereals,
commercial stuffings and
commercial biscuit mixes.
Desserts Most desserts are fine Instant pudding and cake
mixes
Fats Most fats are fine Bottled salad dressings,
bacon bits and snack dips,
processed cheese dips
Meats All fresh meats, poultry and
fish are fine
Processed, smoked, cured
meats, pickled fish.
Dairy Milk, yogurt, low-sodium
cheeses, eggs
Regular hard and
processed cheese
Soups Homemade soups and
stocks made with minimal
salt
Tinned soups and bouillon
Condiments Herbs, spices, vinegars, chilli
sauce
Seasonings made with salt
(celery salt, garlic salt, etc),
regular soya sauce,
barbecue sauce, teriyaki
sauce, and Worcestershire
sauce.
Lecture 8 – Dietary Approaches Part 2 27
LOW-POTASSIUM DIET
Given all the (positive) attention we’ve given potassium in our nutrition education,
you might be wondering why we would ever advise a low-potassium diet! The
situations you would advise this are rare and include when a person takes potassium
sparing diuretics and renal failure.
Renal failure This is one situation in particular where a low-potassium diet is advised. Normally,
our kidneys are quite efficient at getting rid of potassium, which is why it’s so important to eat lots of it every day. However, if the kidneys are not able to
excrete it, and/or the individual is taking potassium-sparing diuretics (as in the
case of CHF), there may be elevated potassium levels in the blood. In cases such
as these, diets containing a maximum of 2-3g of potassium per day are advised,
along with regular monitoring.
The low-potassium diet
This type of diet is VERY difficult to achieve, especially with whole foods. One
example of a tactic used by dieticians is to soak potatoes (cut up) in cold water
first, so they leach their potassium out into the soaking water before they are
cooked. By the same token, boiling vegetables and throwing away the cooking
water helps to minimise potassium. Patients are advised to avoid foods with over
250mg potassium per serv ing.
Generally, serum potassium levels can fluctuate markedly in patients with renal
disease and this needs to be monitored regularly. In this case, serum potassium is
regulated with dialysis, and between dialysis, intake must be based on serum
levels. These individuals should be under regular supervision by their doctor and
hospital dietician who is trained in critical care nutrition.
Lecture 8 – Dietary Approaches Part 2 28
REFERENCES
Billings TE. Notes for a talk held at the SF-LiFE Expo on June 1, 1997. Taken from the
website: www.living-foods.com.
Colbin A. Food and Healing. Ballentine Books, New York 1986.
D’Adamo PJ. Eat Right for your type. Century, London 2001.
Dries J and Dries I . The complete book of food combining. Element Books Limited,
Shaftesbury, Dorset 1998.
Fallon S. Nourishing Traditions. ProMotion Publishing, SanDiego, California. 1995.
Farquharson M. Natural Detox. Element Books Ltd, Shaftesbury, Dorset 1999.
Gates D. The Body Ecology Diet. B.E.D. Publications, Decatur, Georgia. 1996
Haas EM. Staying Healthy with Nutrition. Celestial Arts. Berkeley, California.1992.
Howell, Edward MD. Enzyme Nutrition 1985. Avery Publishing Group Inc. Wayne, New
Jersey.
Lad V. Ayurveda, the science of self-healing. Lotus Press. Wilmot, Wisconsin 1984.
Price, WA DDS. Nutritional Degeneration, 1945 Price Pottenger Nutrition Foundataion,
Inc., La Mesa, California.
Ray Peat, Health Freedom News, September 1993, 33-34. In Fallon
Schwarzbein, D. The Schwarzbein Principle, Health Communications Inc., 1999.
Turner K. The Self-Healing Cookbook, A macrobiotic Primer. Earthtones Press, 1987
Grass Valley, California.