
The Relationship Between Perceived Exertion and Heart Rate ... · PDF filePediatric Exercise...
9
Pediatric Exercise Science, 1989, 1, 360368 The Relationship Between Perceived Exertion and Heart Rate in Children and Adults Mary C. Gillach, James F. Sallis, Michael J. Buono, Patricia Patterson, and Philip R. Nader This study examined the relationship between heart rate (HR) as a measure of physiological strain and ratings of perceived exertion (RPE) in 193 children (mean age= 11 yrs) and 188 adults (mean age =36 yrs) during submaximal cycle ergometry. Two methods of correlating HR and RPE were compared. Computing correlations (r) for each individual's data and then taking the group mean produced very high rs, ranging from 0.92 to 0.95. Correlating HR and RPE for the entire group at all powers simultaneously produced much lower rs, ranging from 0.63 to 0.65. Correlations were essentially the same for children and adults, and there was no evidence of a practice effect. The results indicated that (a) children in this age group were as capable of ex- pressing RPE as adults, and @) absolute levels of perceived exertion were not predictive of physiological strain (as indicated by heart rate). Exercise intensity is reflected in the response of many physiological pro- cesses including oxygen consumption, blood pressure, blood lactate levels, and heart rate (HR). Because HR is linearly related to power and oxygen consump- tion (VOz) in adults (1, 18, 27), it is accepted as an accurate index of physio- logical strain. An alternative method of monitoring exercise intensity is ratings of per- ceived exertion (WE). These ratings, obtained from subjects during testing, are subjective estimates of strain that simultaneously reflect both physiological and psychological variables. The most commonly used RPE scale is the 15-point scale by Borg (6). This scale, which ranges from 6 to 20, was constructed to correspond with the normal HR range for most healthy middle-aged subjects. Thus, a given RPE value multiplied by 10 should approximate exercising HR (7, 8). Several studies by Borg and others have confirmed this 1:10 ratio of RPE to exercise HR in adults (6, 9, 13, 14, 17, 27) while others have not (12, 28). One study found this ratio to be accurate in adults but not in children (2). Whether HR can be reliably estimated by RPE remains unclear. Mary C. Gillach, Michael J. Buono, and Patricia Patterson are with the Depart- ments of Biology and Physical Education at San Diego State University, San Diego, CA 92182. James F. Sallis and Philip R. Nader, M.D., are with the Department of Pediatrics at the University of California at San Diego, La Jolla, CA 92093. Supported in part by NM grant HL 30872.
Transcript of The Relationship Between Perceived Exertion and Heart Rate ... · PDF filePediatric Exercise...

Pediatric Exercise Science, 1989, 1 , 360368
The Relationship Between Perceived Exertion and Heart Rate in Children and Adults
Mary C. Gillach, James F. Sallis, Michael J. Buono, Patricia Patterson, and Philip R. Nader
This study examined the relationship between heart rate (HR) as a measure of physiological strain and ratings of perceived exertion (RPE) in 193 children (mean age= 1 1 yrs) and 188 adults (mean age =36 yrs) during submaximal cycle ergometry. Two methods of correlating HR and RPE were compared. Computing correlations (r) for each individual's data and then taking the group mean produced very high rs, ranging from 0.92 to 0.95. Correlating HR and RPE for the entire group at all powers simultaneously produced much lower rs, ranging from 0.63 to 0.65. Correlations were essentially the same for children and adults, and there was no evidence of a practice effect. The results indicated that (a) children in this age group were as capable of ex- pressing RPE as adults, and @) absolute levels of perceived exertion were not predictive of physiological strain (as indicated by heart rate).
Exercise intensity is reflected in the response of many physiological pro- cesses including oxygen consumption, blood pressure, blood lactate levels, and heart rate (HR). Because HR is linearly related to power and oxygen consump- tion (VOz) in adults (1, 18, 27), it is accepted as an accurate index of physio- logical strain.
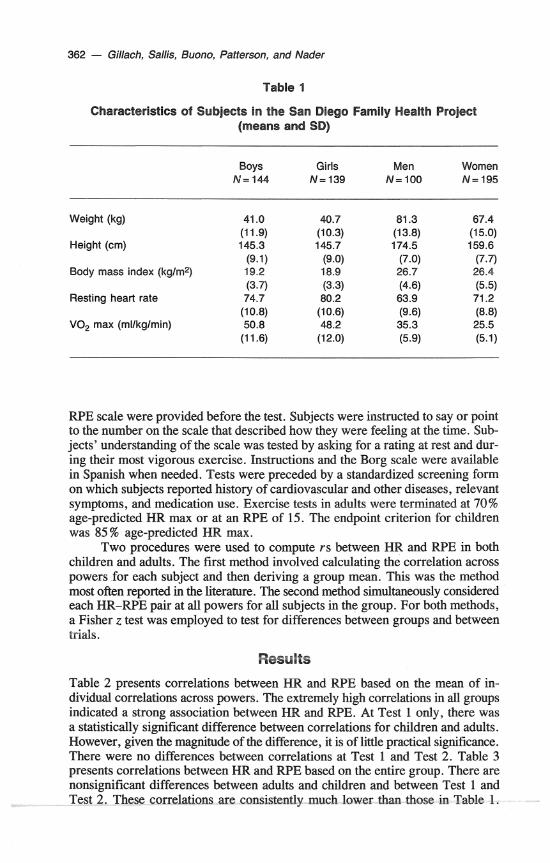
An alternative method of monitoring exercise intensity is ratings of per- ceived exertion (WE). These ratings, obtained from subjects during testing, are subjective estimates of strain that simultaneously reflect both physiological and psychological variables. The most commonly used RPE scale is the 15-point scale by Borg (6). This scale, which ranges from 6 to 20, was constructed to correspond with the normal HR range for most healthy middle-aged subjects. Thus, a given RPE value multiplied by 10 should approximate exercising HR (7, 8). Several studies by Borg and others have confirmed this 1: 10 ratio of RPE to exercise HR in adults (6, 9, 13, 14, 17, 27) while others have not (12, 28). One study found this ratio to be accurate in adults but not in children (2). Whether HR can be reliably estimated by RPE remains unclear.
Mary C. Gillach, Michael J. Buono, and Patricia Patterson are with the Depart- ments of Biology and Physical Education at San Diego State University, San Diego, CA 92182. James F. Sallis and Philip R. Nader, M.D., are with the Department of Pediatrics at the University of California at San Diego, La Jolla, CA 92093.
Supported in part by NM grant HL 30872.
Perceived Exertion and Heart Rate - 361
The positive linear relationship between HR and RPE over a range of powers is well documented in adults (6, 11, 24, 25, 28, 29). Numerous studies report correlations (r) ranging from 0.77 to 0.90 (4, 6, 10, 27). Based on these high correlations, subjective ratings are presumed to accurately reflect physiological strain in adults. However, the statistical methodology used to calculate rs in these studies is often inadequately described. Few authors specified whether rs for in- dividual subjects were used to calculate group mean rs or if rs were calculated from the simultaneous analysis of all subjects' HR and RPE data. Most studies that reported their methodology used the former method, which is likely to inflate the correlation. It appears that the latter correlation method, which considers all variables at each power, is more appropriate.
Few studies have examined how children perceive their physiological strain. It is difficult to compare existing studies of adults and children because of dif- ferences in methodology. Studies of adults usually correlate absolute HR with RPE while few studies in children did so (2, 3). Most studies of children cor- relate percent HR max with RPE, with resulting rs ranging from 0.69 to 0.94 in children over 9 years of age (22,30). Nevertheless, several investigators sug- gest that the reliability and validity of W E may be just as high in children as in adults (2, 22, 30). Test-retest reliabilities of the use of RPE by children have ranged from 0.37 to 0.89 (19, 22, 30) while reliabilities in adults have ranged from 0.78 to 0.98 (20, 21, 28). Although a few studies have indicated that chil- dren are able to use WE, no studies have compared the validity of RPE scales in children and adults from the same population using the same methods. The purpose of the present study was to assess age-related differences in the relation- ship of RPE to physiological strain (HR).
Methods Subjects
The subjects for this study were drawn from 95 Anglo and 11 1 Mexican Ameri- can families (N=623) who were participating in the San Diego Family Health Project (23). Families with fifth- or sixth-grade children were recruited from 12 elementary schools. For this analysis, 283 children ages 10 to 14 years (mean age = 1 1 yrs) and 295 adults ages 22 to 55 (mean age = 36 yrs), who completed two submaximal cycle ergometer testing sessions 1 year apart, were studied. Sub- ject characteristics for adults and children, by gender, are displayed in Table 1.
Procedure
Assessments were conducted by pairs of exercise physiology graduate students who were thoroughly trained and certified in the protocols. Testing was conducted on calibrated Monark cycle ergometers using a modified Astrand-Ryhming protocol of gradually increasing power (26). Subjects pedaled at 50 rpm at an initial power of 25 watts (W), and the power was increased 25 W every 2 minutes. Most subjects completed three to five workloads. HR was assessed at the end ofaach 2-min stage with a cardiotachometer and photoplethethysmograph attached to the earlobe (CIC Instruments, Hempstead, NY, Model 60200). Radial palpa- tion was used in rare instances when the cardiotachometer malfunctioned. W E was measured at rest and at the end of each 2-min stage with Borg's original 15-point scale (6) (see Figure 1). Brief standard instructions in the use of the
362 - Gillach, Sallis, Buono, Patterson, and Nader
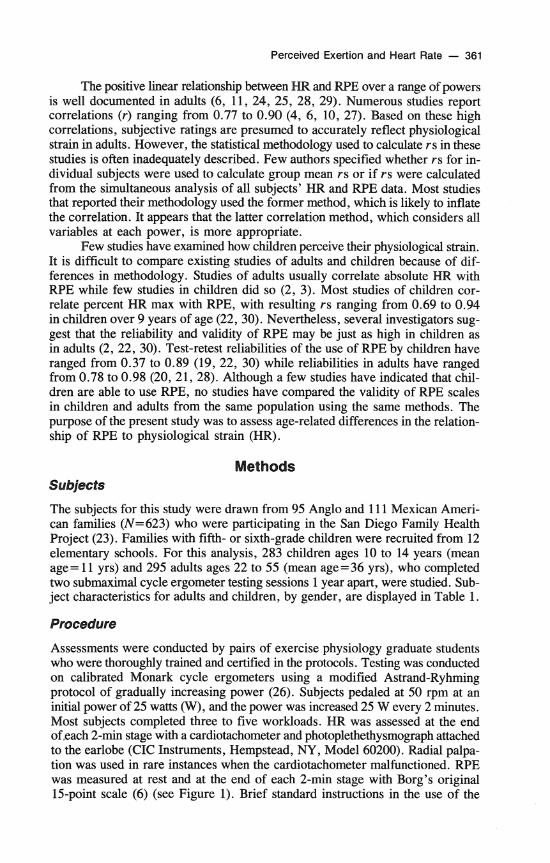
Table 1
Characteristics of Subjects in the San Diego Family Health Project (means and SD)
Boys Girls Men Women N=144 N = 139 N= 100 N=195
Weight (kg) 41 .O (1 1.9)
Height (cm) 145.3 (9.1)
Body mass index (kglmz) 19.2 (3.7)
Resting heart rate 74.7 (10.8)
VO, max (mllkglmin) 50.8 (1 1.6)
W E scale were provided before the test. Subjects were instructed to say or point to the number on the scale that described how they were feeling at the time. Sub- jects' understanding of the scale was tested by asking for a rating at rest and dur- ing their most vigorous exercise. Instructions and the Borg scale were available in Spanish when needed. Tests were preceded by a standardized screening form on which subjects reported history of cardiovascular and other diseases, relevant symptoms, and medication use. Exercise tests in adults were terminated at 70% age-predicted HR rnax or at an RPE of 15. The endpoint criterion for children was 85% age-predicted HR max.
Two procedures were used to compute rs between HR and RPE in both children and adults. The first method involved calculating the correlation across powers for each subject and then deriving a group mean. This was the method most often reported in the literature. The second method simultaneously considered each HR-RPE pair at all powers for all subjects in the group. For both methods, a Fisher z test was employed to test for differences between groups and between trials.
Results
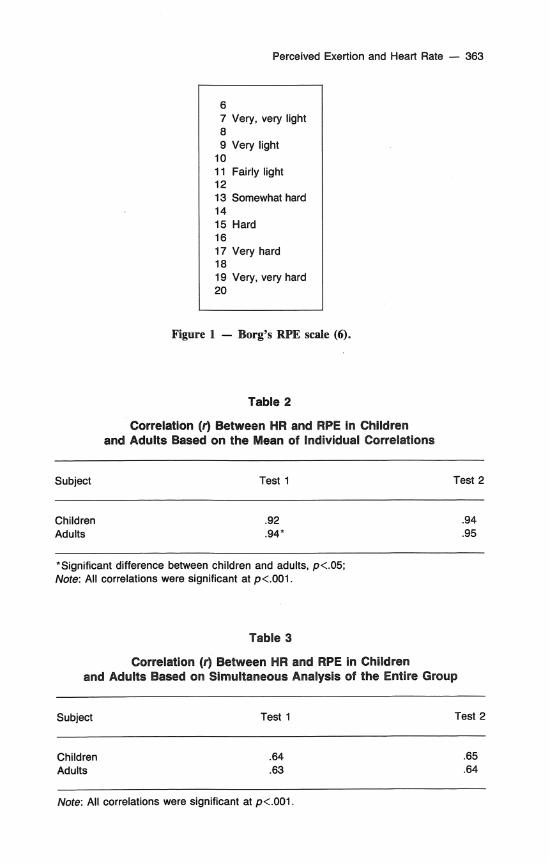
Table 2 presents correlations between HR and RPE based on the mean of in- dividual correlations across powers. The extremely high correlations in all groups indicated a strong association between HR and RPE. At Test 1 only, there was a statistically significant difference between correlations for children and adults. However, given the magnitude of the difference, it is of little practical significance. There were no differences between correlations at Test 1 and Test 2. Table 3 presents correlations between HR and W E based on the entire group. There are nonsignificant differences between adults and children and between Test 1 and Test 2. These correlations are consistently much lower than those in Table 1.
Perceived Exertion and Heart Rate - 363
6 7 Very, very light 8 9 Very light
10 11 Fairly light 12 13 Somewhat hard 14 15 Hard 16 17 Very hard 18 19 Very, very hard 20
Figure 1 - Borg's RPE scale (6).
Table 2
Correlation (0 Between HR and RPE in Children and Adults Based on the Mean of Individual Correlations
Subject Test 1 Test 2
Children Adults
*Significant difference between children and adults, p<.05; Note: All correlations were significant at p<.OOl.
Table 3
Correlation (r) Between HR and RPE in Children and Adults Based on Simultaneous Analysis of the Entire Group
Subject Test 1 Test 2
Children Adults
Note: All correlations were significant at p<.001.
364 - Gillach, Sallis, Buono, Patterson, and Nader
Correlations were conducted separately for boys, girls, men, and women. Within age groups, correlations were essentially identical for both gender groups.
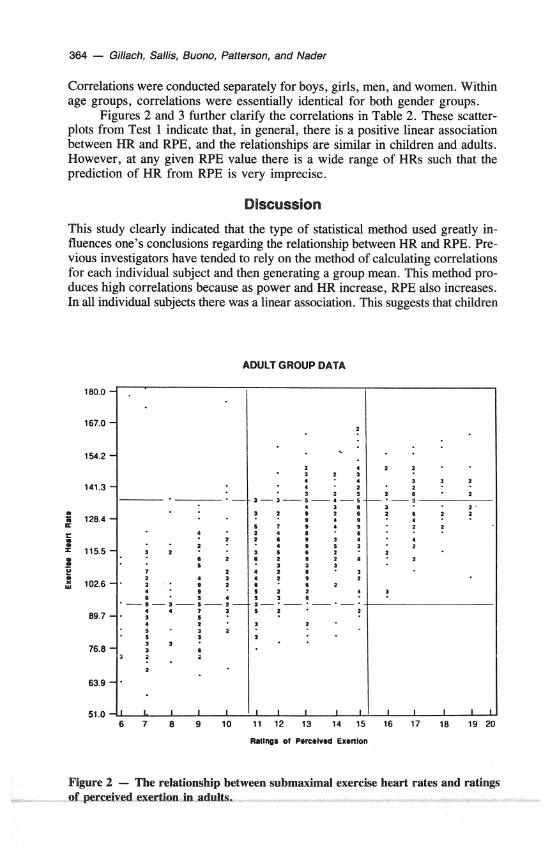
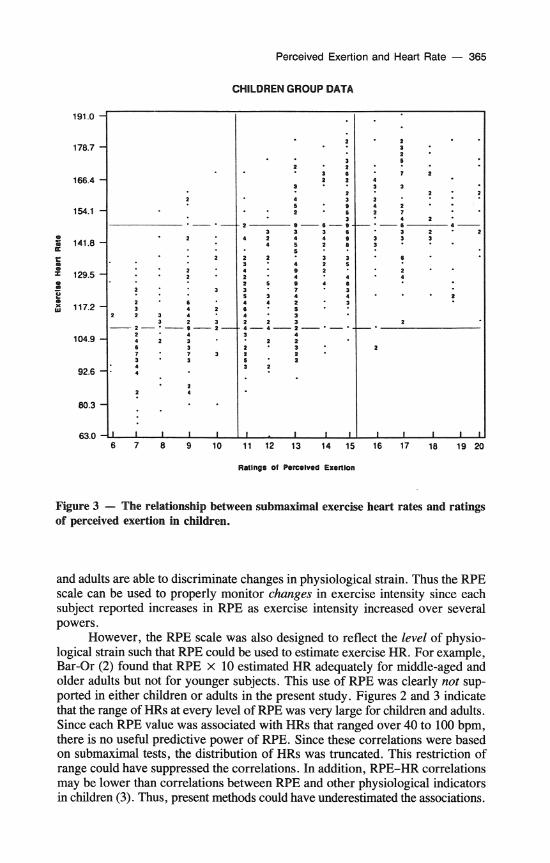
Figures 2 and 3 further clarify the correlations in Table 2. These scatter- plots from Test 1 indicate that, in general, there is a positive linear association between HR and RPE, and the relationships are similar in children and adults. However, at any given RPE value there is a wide range of HRs such that the prediction of HR from RPE is very imprecise.
Discussion
This study clearly indicated that the type of statistical method used greatly in- fluences one's conclusions regarding the relationship between HR and RPE. Pre- vious investigators have tended to rely on the method of calculating correlations for each individual subject and then generating a group mean. This method pro- duces high correlations because as power and HR increase, RPE also increases. In all individual subjects there was a linear association. This suggests that children
ADULT GROUP DATA
Figure 2 - The relationshi f perceived exertion in adu
Perceived Exertion and Heart Rate - 365
CHILDREN GROUP DATA
Figure 3 - The relationship between submaximal exercise heart rates and ratings of perceived exertion in children.
and adults are able to discriminate changes in physiological strain. Thus the RPE scale can be used to properly monitor changes in exercise intensity since each subject reported increases in RPE as exercise intensity increased over several powers.
However, the RPE scale was also designed to reflect the level of physio- logical strain such that RPE could be used to estimate exercise HR. For example, Bar-Or (2) found that RPE x 10 estimated HR adequately for middle-aged and older adults but not for younger subjects. This use of W E was clearly not sup- ported in either children or adults in the present study. Figures 2 and 3 indicate that the range of HRs at every level of RPE was very large for children and adults. Since each RPE value was associated with HRs that ranged over 40 to 100 bpm, there is no useful predictive power of WE. Since these correlations were based on submaximal tests, the distribution of HRs was truncated. This restriction of range could have suppressed the correlations. In addition, RPE-HR correlations may be lower than correlations between RPE and other physiological indicators in children (3). Thus, present methods could have underestimated the associations.
366 - Gillach, Sallis, Buono, Patterson, and Nader
The confidence in these results is increased since almost identical results were found for children and adults and for males and females. There were no indications that practice improved the HR-RPE association. It is reasonable to hypothesize that the ability of a 35-year-old subject to accurately report his or her level of exertion would be better than that of a 10-year-old, given differences in cognitive abilities. However, no such differences were found. Given that very few subjects had previous experience with exercise testing or rating their exer- tion level, improvement with practice could be expected. This was tested by eval- uating subjects' first exercise test and later their third test. A second test was conducted at the 3-month point but those data were not analyzed for this paper. Although the practice hypothesis was not supported by the present study, the measurement schedule was not optimal for testing the hypothesis. For maximal effect, a practice session should probably be held a few days prior to the testing session.
Ratings of perceived exertion are commonly used as indices of exercise intensity when prescribing exercise regimens (5, 15, 16). This practice is based on the assumption that RPE reflects physiological strain, but it appears that such an assumption is unwarranted because many previous studies may have over- estimated associations between RPE and physiological strain. The results of the present study suggest that, while RPE-HR associations may be reliable over testing sessions in adolescents (19). RPE does not accuratelv reflect HR in either chil- dren or adults. These fihdings are essentially in agriement with the conclusion of Bar-Or (2), who found high WE-HR associations only in middle-aged and older adults. Adults in the present study averaged 36 years of age. Using RPE to prescribe and monitor exercise intensity is therefore a questionable practice, since at any given RPE, HR may vary by 40 to 100 bpm. In healthy individuals this degree of error would render RPE useless. In clinical populations, basing - -
exercise intensity on RPE could be dangerous. The primary conclusion from this study is that RPE is useful for tracking
changes in exercise intensity within a session, but that absolute levels of perceived exertion are not related to indices of physiological strain. Therefore, using RPE X 10 as an estimate of heart rate may be dangerously misleading. ~ a t i n ~ s of perceived exertion should not be used as substitutes for heart rate or other physio- logical measures. The associations between RPE and HR were similar in chil- dren and adults.
References
1. Astrand, I. Aerobic work in men and women with special reference to age. Acta Physiol. Scand. 49 (Suppl. 169): 1-92, 1960.
2. Bar-Or, 0 . Age-related changes in exercise perception. In: Physical Work and Ef- fort, G . Borg (Ed.). Oxford: Pergamon Press, 1977, pp. 255-266.
3. Bar-Or, O., and S.L. Reed. Rating of perceived exertion in adolescents with neuro- muscular disease. In: The Perception of Exertion in Physical Work, G . Borg and D. Ottoson (Eds.). Southampton, U.K. : MacMillan, 1986, pp. 137-148.
4. Bar-Or, O., J.S. Skinner, E.R. Buskirk, and G. Borg. Physiological and perceptual indicators of physical stress in 40 to 60-year-old men who vary in conditioning level and in body fat. Med. Sci. Sports 4:96-100, 1972.
Perceived Exertion and Heart Rate - 367
5. Birk, T.J., and C.A. Birk. Use of ratings of perceived exertion for exercise prescrip- tion. Sports Med. 4:l-8, 1987.
6. Borg, G. Physical Performame and Perceived Exertion. Lund, Sweden: Gleerup, 1962. 7. Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehab. Med.
2-3:92-98, 1970. 8. Borg, G. Perceived exertion: A note on "history" and methods. Med. Sci. Sports,
5:90-93, 1973. 9. Borg, G., J-G. Karlsson, and L. Ekelund. A comparison between two work tests con-
trolled subjectively and by heart rate. In: Physical Work and Effort, G. Borg (Ed.). Oxford: Pergamon Press, 1977, pp. 239-254.
10. Borg, G., and H. Linderholm. Perceived exertion and pulse rate during graded exer- cise in various age groups. Acta Med. Scand. 172: 194-206, 1967.
1 1. Borg, G., and B. Noble. Perceived exertion. In: Exercise and Sport Science Reviews, J. Wilmore (Ed.). New York: Academy Press, 1974, pp. 131-153.
12. Burke, E.J., and M.L. Collins. Using perceived exertion for the prescription of exercise in healthy adults. In: Clinical Sports Medicine, R.C. Cantu (Ed.). Boston: Collarnore Press, 1983, pp. 93-105.
13. Burke, E.J., and T.J. Keenan. Energy cost, heart rate and perceived exertion during elementary backstroke. Phys. Sportsmed. 12:55-59, 1984.
14. Carton, R.L., and E.C. Rhodes. A critical review of the literature on rating scales for perceived exertion. Sports Med. 2:198-222, 1985.
15. Dishman, R.K., R.W. Patton, J. Smith, R. Weinberg, and A. Jackson. Using per- ceived exertion to prescribe and monitor exercise training heart rate. Inter. J. Sports Med. 8:208-213, 1987.
16. Eston, R.G., B.L. Davies, and J.G. Williams. Use of perceived effort ratings to con- trol exercise intensity in young healthy adults. Euro. J. Appl. Physiol. 56:222-224, 1987.
17. Grirnby, G., J. Bjure, A. Mattias, B. Ekstrom-Jodal, G. Tibbin, and L. Wilhelmser. Work capacity and physiological responses to work. Am. J. Cardiol. 30:37-42, 1972.
18. Hellerstein, H.K., and R. Ader. ~ela t ionshi~ between per cent maximal oxygen up- take (% max V02) and per cent maximal heart rate (% MHR) in normals and cardiacs. Circulation, 44 (Suppl. 2): 71-76, 1971.
19. Komi, P.U., and S-L. Karppi. Genetic and environmental variation in perceived exertion and heart rate during bicycle ergometer work. In: Physical Effort and Work, G . Borg (Ed.). Oxford: Pergamon, 1977, pp. 91-99.
20. Lollgen, H., H-V. Ulmer, R. Gross, G. Wilbert, and G.V. Nieding. Methodological aspects of perceived exertion rating and its relation to pedalling rate and rotating mass. Euro. J. Appl. Physiol. 34:205-215, 1975.
21. Lollgen, H., H-V. Ulmer, and G.V. Nieding. Heart rate and perceptual response to exercise with different pedalling speeds in normal subjects and patients. Euro. J. Appl. Physiol. 37:297-304, 1977.
22. Miyashita, M., K. Onodera, and I. Tabata. How Borg's RPE-scale has been applied to the Japanese. In: R e Perception of Exertion in Physical Work, G. Borg and D. Ottosen (Eds.). Southampton, UK: MacMillan, 1986, pp. 27-34.
23. Nader, P.R., J.F. Sallis, J. Rupp, C. Atkins, T. Patterson, and I. Abramson. San Diego Family Health Project: Reaching families through the schools. J. School Health, 56:227-231, 1986.
368 - Gillach, Sallis, Buono, Patterson, and Nader
24. Pandolf, K.B. Advances in the study and application of perceived exertion. Exer. Sport Sci. Rev. 11:118-158, 1983.
25. Sargeant, A.J., and C.T. Davies. Perceived exertion during rhythmic exercise in- volving different muscle masses. J. Hum. Ergonom. 2:3-11, 1973.
26. Siconolfi, S.F., E.M. Cullinane, R.A. Carleton, and P.D. Thompson. Assessing VOzmax in epidemiological studies: Modification of the Astrand Ryhming test. Med. Sci. Sports Exer. 14:335-338, 1982.
27. Skinner, J.S., G. Borg, and E.R. Buskirk. Physiological and perceptual reactions to exertion of young men differing in activity and body size. In: Exercise and Fitness, B.D. Franks (Ed.). Chicago: The Athletic Institute, 1969, pp. 53-66.
28. Skinner, J.S., R. Hustler, V. Bergsteinova, and E.R. Buskirk. The validity and reli- ability of a rating scale of perceived exertion. Med. Sci. Sports, 5:94-96, 1973.
29. Skimer, J.S., R. Hustler, V. Bergsteinova, and E.R. Buskirk. Perception of effort during different types of exercise and under different environmental conditions. Med. Sci. Sports, 5:llO-115, 1973.
30. Ward, D.S., and 0. Bar-Or. Usefulness of a RPE scale for exercise prescription with obese youth. Unpublished manuscript, University of South Carolina, 1987.


















