Bile salt-induced cholesterol crystal formation from model bile

Gut 1997; 40: 182-187
The relationship between acid and bile reflux andsymptoms in gastro-oesophageal reflux disease
R E K Marshall, A Anggiansah, W A Owen, W J Owen
AbstractBackground-The role of bile in thegenesis of oesophageal symptoms anddisease is incompletely understood. A newmethod of ambulatory bile monitoringmay help to define this role.Ai>ns-To establish the relationshipbetween symptom events and acid and bilereflux episodes.Patients-59 consecutive patients pre-senting for further investigation of gastro-oesophageal reflux disease.Methods-All patients underwent com-bined ambulatory pH and bile monitoring.For each patient, a symptom index (SI)was calculated in relation to both acidreflux and bile reflux episodes.Results-Patients were divided into thosewithout (group 1, n=21) and those with(group 2, n=38) acid reflux. A total of 394symptoms were identified in 59 patients.In group 1, there were fewer symptomevents per patient (mean 4-1) than group2 (mean 8- 1). Twenty three per cent ofsymptom events were associated with acidreflux in group 1 and 41% in group 2. Only6% ofsymptom events in both groups wererelated to bile reflux. In group 1 both theacid and bile related SI score were low. Ingroup 2 the bile related SI score was low,but the acid related SI score was high.Conclusions-Symptoms are much moreoften related to acid reflux than bilereflux. Bile reflux does not seem to be amajor factor in producing oesophagealsymtoms.(Gut 1997; 40: 182-187)
Keywords: gastro-oesophageal reflux, symptom index,bile monitoring.
Department ofSurgery, Guy'sHospital, LondonRE K MarshallA AnggiansahW A OwenW J OwenCorrespondence to:Mr R E K Marshall,Department of Surgery,Guy's Hospital,London SE1 9RT.
Accepted for publication28 August 1996
While there is no doubt that gastro-oesophageal reflux of acid is responsible for theproduction of oesophagitis and its compli-cations, the role of duodenal contents (specifi-cally trypsin and bile acids) in oesophagealmucosal disease remains less certain. Bothanimal and human studies have suggested a
role for bile in the pathogenesis of oeso-
phagitis,' 2 Barrett's oesophagus,3 4 and oeso-
phageal adenocarcinoma,5 but the difficulty so
far has been in trying to quantify bile reflux invivo. In the past various methods have beenused but they all have their drawbacks. HIDAscintigraphy has been used, but this is a
comparatively insensitive and unphysiologicalmethod for the measurement of gastro-oesophageal reflux.6 Aspiration studies havealso been performed to determine the quantity
of bile acids in oesphageal refluxate, but this iscumbersome, invasive, and as with scinti-graphy it is unphysiological, measuring shorttime periods in static conditions. Ambulatory24 hour pH monitoring has been used, theassumption being that an alkaline shift in pH>7 equates with the presence of duodenalcontents. However, combined aspiration andpH monitoring studies have shown this not tobe the case.7
Bilitec 2000, a fibreoptic spectrophoto-metric probe, was developed to overcome theseproblems.8 Bilirubin has a characteristic ab-sorbance spectrum at 453 nm, and by con-tinuous monitoring of the oesophageal re-fluxate, the presence of bilirubin in therefluxate can be determined on an ambulatorybasis. In this way Bilitec 2000 uses bilirubin asa marker for the presence of duodenalcontents. Extensively validated both in vitroand in vivo,'9-" it has been shown that gastro-oesophageal bile reflux can be monitored in arelatively patient friendly manner, and that inpatients with normal gastro-intestinal anat-omy, acid and bile reflux times correlateextremely well, and that there is no relationshipbetween bile and alkaline reflux.'21-4The aim of the study was to analyse the
symptom events in a group of patients withgastro-oesophageal reflux disease (GORD),with regards to whether they were associatedwith episodes of acid or bile reflux. Thesimplest form of symptom analysis, the symp-tom index (SI), was used, to identify whetherbile reflux is as potent a cause of symptoms asacid reflux.
Methods
PatientsFifty nine consecutive patients (36 female;mean age 46&6 years; range 23 to 76) referredto the Oesophageal Laboratory at Guy's Hos-pital for further investigation of GORD wereincluded in this study. All patients were com-plaining of heartburn or acid regurgitation, orboth. None had previously undergone gastricor oesophageal surgery. Seven patients hadundergone previous open cholecystectomy. Allpatients had stopped acid suppression therapy(either 48 hours beforehand for those taking H2receptor antagonists, or seven days beforehandfor those using proton pump inhibitors).
Study designStatic manometry was carried out beforehandin all cases. The nasal mucosa was sprayedwith lignocaine, and a solid state pressure
182
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from

Relationship between acid and bile reflux in GORD
manometer (Gaeltec Ltd, Isle of Skye, UK)with six transducers, at 5 cm intervals andradially oriented at 900, was introduced. Oeso-phageal manometry was then carried out usingthe station pull through technique todetermine lower oesophageal sphincter (LOS)position and pressure, and to exclude patientswith primary oesophageal motility disorders. ABerstein acid perfusion test was carried out.
After manometry, a dual channel antimonypH electrode (2 1 mm diameter) and a fibre-optic bile probe (3 mm diameter) (bothSynectics Medical, Stockholm, Sweden) werestrapped together using 12-5 mm Microporetape (3M Medical-Surgical Division, St Paul,MN), taking care not to obstruct the gap in thebile probe tip or the pH sensors. Before andafter each study, the pH probes were calibratedin buffer solutions of pH 7 and pH 1, and thebile probe calibrated in water. The proximalpH sensor was strapped next to the bile probeand these placed 5 cm above the upper borderof the manometrically determined LOS, withthe distal pH sensor 15 cm distal to this, in thegastric body. We have found a dual channel pHprobe with the bile probe next to the proximalpH sensor much easier to insert than a singlechannel pH probe, which presents quite a largeend when combined with a bile probe.Both probes were attached to data collecting
devices worn on a belt on the patients' waist.Patients were given a diary sheet to record thetime and content of their meals, time of goingto bed and getting up, and their symptoms.They were also asked to press a marker buttonto record their symptom events. Patients wereasked to avoid acidic foods that may interferewith pH monitoring and dark coloured foodsthat interfere with bilirubin absorbance (a listwas provided), and were consequently told thefoodstuffs they could eat. They were en-couraged to carry out their normal dailyactivities, and to return the following day forthe probes to be removed. Both bile and acidreflux data were then downloaded onto acomputer for analysis.The 59 patients were divided into two
groups: group 1, those without significant acidreflux (n=21 (36%), 17 female), and group 2,those with significant acid reflux (n=38 (64%),19 male (Table I)).
Data analyisData were analysed on commercially availablesoftware (EsopHogram, Gastrosoft Inc, USA).Analysis of the 24 hour tracing was dividedinto total, upright interprandial, meal, post-prandial, and supine periods. Acid reflux was
TABLE I Acid and bile reflux data for group 1 (nosignificant acid reflux) and group 2 (significant acid reflux)
Acid reflux Bile reflux(%lo of total time (% of total timepH <4) absorbance >0-14)
Group 1 (n=21) 0-8 (0-2-1-4) 0-1 (0-1 7)(No significant acid reflux)Group 2 (n=38) 7-7 (4-7-15-4) 13-25 (53-26-5)(Significant acid reflux)
Values expressed as median (interquartile range).
defined as a drop in intraoesophageal pH <4,and bile reflux as bilirubin absorbance >0 14.Significant gastro-oesophageal reflux was saidto have occurred if the DeMeester score wasgreater than 14-7. Each symptom event wasanalysed: acid reflux was said to be associatedwith the symptom event if the pH droppedbelow 4 for more than 10 seconds in the twominutes either side of the symptom event, andbile reflux was said to have occurred if thebilirubin absorbance was greater than 0-14 formore than 10 seconds in the two minutes eitherside of the symptom event.For each patient the SI was calculated for
bile reflux:number of symptoms with bilirubin absorbance >0-14
SI= x 100total number of symptoms
and the SI for acid reflux was calculated:
SInumber of symptoms with pH <4
x 10total number of symptoms
This percentage was then converted to a SIscore in the following manner: 0%=O,1-24%=1, 25-49%=2, 50-74%=3, 75-99%=4,100%=5.
Statistical analysisValues are expressed as mean (SD) for para-metric data and median (interquartile range)for non-parametric data. The Mann-WhitneyU test was used to establish differences be-tween two sets of non-parametric data,Student's t test for parametric data, and corre-lations were established using the Spearmanrank test. A p value <0 05 was consideredsignificant.
Results
pH and bile reflux dataFor the group 1 patients, the median (inter-quartile range) total time pH <4 was 0-8%(0.2-1 4%) and bilirubin absorbance >0-14was 0-1% (00/o-1 7%). The median (inter-quartile range) DeMeester score was 3-8(1-5-3). For the group 2 patients, the median(interquartile range) total time pH <4 was7.7% (4.70/o-15.4%) and bilirubin absorbance>0 14 was 13-25% (5.30/626.5%). Themedian (interquartile range) DeMeester scorewas 33-5 (18-7-61-2). The correlation betweentotal time pH <4 and total time bilirubinabsorbance >0 14 for all patients wasextremely good: r=0*55, p<0*001.
Symptom and manometry dataThe various symptoms the patients com-plained of are listed in Table II. It can be seenthat all patients complained of heartburn, andthat belching and regurgitation were the nextmost frequent symptoms. Epigastric pain, dys-phagia, and chest pain were less frequentlycomplained of. However, the distribution ofthe symptoms between the two groups wascomparable, the only difference being thegreater frequency of chest pain in group 2(those with significant acid reflux).
183
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from

Marshall, Anggiansah, Owen, Owven
TABLE II Occurrence of differenit symnptoms among patientsi.n group I and group 2
S,VnIptoni Grouip I Group 2
Heartburn 21 (100) 38 (100)Belching 15 (71) 27 (71)Rergurgitation 11 (52) 23 (60)Dvsphagia 7 (33) 15 (39)Epigastric pain 7 (33) 11(29)Chest pain 1 (5) 9 (24)
Figures in parentheses are percentages.
There was no difference in the frequency ofa positive Bernstein test between the twogroups, with 14 patients (66%) in group 1 and26 patients (68%) in group 2 complaining ofheartburn during intraoesophageal acid per-fusion. There was a significant difference in thelower oesophageal sphincter pressure (LOSP)between the groups, the mean (SD) LOSPbeing 919 (47) mm Hg in group 1 and 554(3 35) mm Hg in group 2 (p<0O001, Student'st test).
Synmptom analysisA total of 394 symptom events were identifiedin 59 patients (range 1-24 per patient) (TableIII) Each event was defined by the time periodin which it occurred (meal, postprandial, inter-prandial upright or supine) and by whether itwas related to an episode of acid reflux, bilereflux, both acid and bile reflux, or neither.The majority of symptom events occurred inthe upright interprandial (173 events, 44%)and the postprandial (165 events, 42%)periods, with 42 events (11 1%) occurring in thesupine period and only 14 events (3%)occurring in the meal period.With regards to the type of reflux associated
with the symptom event, the greatest numberof events was associated with neither acid norbile reflux (178 events, 45%). A total of 147events (37%) were associated with acid refluxalone, 45 events (11%) were associated withboth acid and bile reflux, and only 24 events(7%) were associated with bile reflux alone.
In group 1, 86 symptom events (22%)occurred in 21 patients (36%), an average of4-1 symptom events per patient. In group 2,308 symptom events (78%) occurred in 38patients (64%), an average of 8 1 symptomevents per patient. Hence, symptoms weretwice as frequent in those with significant acidreflux. When considering group 1 and group 2separately, in each case the symptom eventswere distributed in a similar fashion betweenthe time periods (the majority occurring inthe postprandial and upright interprandialperiods). However, there was a difference in
TABL E III Relationi between the type of refluxate anid symptom evenits, and the tinie penrodi7n which symwptom events occurred
Acid Bile Both acidreflux reflux atnd bile Neither
Postprandial 67 11 15 72 165 (42)Meal 0 3 2 9 14 (4)Upright interprandial 65 8 17 83 173 (44)Supine 15 2 11 14 42 (10)
147 (37) 24 (60) 45 (11) 178 (45) 394
Figures in parentheses are percentages.
Both0%
Figure 1: Nature of the refluxate associated zwith syniptonevents in patients wzithout significanit gastro-oesophagealacid reflu'x (group 1).
the type of refluxate associated with the symp-tom event: in group 1 (those without signifi-cant acid reflux), the majority of symptomevents were associated with neither acid norbile reflux (61 events, 71%), with 20 events(23%) associated with acid reflux and only fiveevents (6%) associated with bile reflux (Fig 1).In group 2 however (those with significant acidreflux), 127 symptom events (41%) were asso-
ciated with acid reflux, 45 symptom events(1 5%) with both acid and bile reflux, only 19symptom events (6%) were associated with bilereflux alone and 117 symptom events (38%)with neither acid nor bile reflux (Fig 2). Hencein group 2 there was a much higher proportionof symptoms associated with acid reflux thangroup 1, and in group 1 a much larger pro-portion were associated with neither acid norbile reflux than in group 2, although in bothgroups there was a similarly small proportionof symptoms associated with bile reflux alone.
Symptom in'dexThe symptom index was calculated for eachpatient, for both bile reflux and acid reflux. Ingroup 1 (Fig 3), with regards to acid reflux, theSI score was 0 for 13 patients, 2 for five patients,3 for two patients, and only one patient had anSI of 5. A similar picture is seen for bile reflux,
Acidreflux41%
Neither38% /
Both Bile15% reflux
6%Figure 2: Nature of the refluxate associated with symiptonievents i7n patienits wi'th significant gastro-oesophageal acidreflux (group 2).
Acidreflux23%
Neither71%
Bilereflux6%
184
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from

185Relationship between acid and bile reflux in GORD
20 n
15[
10 F-
5
o
M Acid related= Bile related
0 1 2 3 4 5
Symptom index
Figure 3: Symptom index scores for patients withoutsignificant gastro-oesophageal acid reflux (group 1). Notethatfor the majority ofpatients the score is very low whetherrelated to acid or bile, indicating a poor correlation betweensymptom events and reflux episodes.
with 18 patients having an SI score of 0. Inother words, there was generally a very poorcorrelation between symptoms and refluxepisodes of either acid or bile in group 1.
In group 2 on the other hand (Fig 4), 27patients (71%) had an acid related SI of 50%or greater (that is, a SI score of 3, 4 or 5),whereas 32 patients (84%) had a bile relatedSI of less than 50% (that is, a SI score of 0,1 or 2). In other words, it seems that in patientswith significant acid reflux, symptoms arestrongly related to acid reflux in most patients,but are poorly related to bile reflux in a greatermajority.
DiscussionThe relationship between acid reflux episodesand symptoms has long been established.Several methods of symptom analysis havebeen described in an effort to relate symptomsto episodes of acid reflux. The SI, defined asthe percentage of reflux related symptom epi-sodes,'5 is the simplest form of symptomanalysis. The drawback of this method is thatit fails to take into account the total number ofreflux episodes, with the possibility that a highSI may be the result of a random associationbetween reflux and symptoms. The symptomsensitivity index, defined as the percentage ofsymptom associated reflux episodes,'6 wasintroduced to try to overcome this drawback,but it fails to take into account the number of
20m Acid relatedWBile related
15-
CL
5-
0 o 1 2 3 4 5Symptom index
Figure 4: SI scores for patients with significant gastro-oesophageal acid reflux (group 2). Note the generally lowscores with regards to bile reflux, but the relatively highscores achieved by the majority ofpatients with regards toacid reflux.
symptom episodes, thus limiting its value.Other techniques of symptom analysis havealso been developed with the aim of improvingthe way in which symptoms and reflux can berelated, but these have become increasinglycomplicated.'7 18 It was therefore felt that, forthe purpose of merely comparing the relativecontributions of acid and bile in the genesis ofsymptoms, the SI was an appropriate methodof symptom analysis.One of the difficulties in trying to relate bile
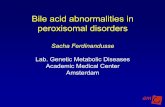
reflux episodes to symptom events can be seenby looking at the segment of a 24 hour com-bined acid and bile reflux tracing in Figure 5.Acid reflux episodes are easily recognised -definite, relatively fast, sharp downward deflec-tions in pH from around pH 6 or 7 to pH 4and below, often closely coinciding with asymptom event. Bile reflux episodes, however,are less well demarcated, and usually there isa smooth, gradual increase in bilirubin ab-sorbance to above the threshold value of 0 14,which often lasts many minutes, rather than asharp upward deflection. The other difficultylies in the fact that an acid reflux episode frompH 7 to pH 1 represents, on a pH scale of 0-9,a change of 66%, whereas a bile reflux episodefrom, for instance, 0-12 to 0-2, on a scale of0-1-0, represents a change of only 8%. In otherwords bile reflux is said to occur in thepresence of only a small increase in bilirubinabsorbance. One of the reasons why bile refluxis not represented by a sharp deflection prob-ably lies in the method of refluxate sampling.When measuring pH, an antimony pH probedetects changes in the hydrogen ion con-centration of the fluid directly surroundingthe outer surface of the probe. Oesophagealclearance ofthe refluxate should therefore clearthe outer surface of the pH probe with relativespeed. This is compared with the bile probe,which relies on the oesophageal refluxatemoving into the 2 mm gap within the bile probetip, between the end of the optical fibres andthe white Teflon probe head (Fig 6). Bearingin mind that, with associated mucus andparticulate matter, oesophageal refluxate maybe more viscous than pure water, it is probablethat meniscal forces play a part in themovement of fluid into and out of the probegap. Hence it is probable not only that a bilereflux episode may take longer to register thanacid reflux episode, but also that oesophagealclearance of bile from the probe tip gap willtake longer. All this would presumably result ina slower increase in bilirubin absorbanceduring an espisode of bile reflux in comparisonwith the sharp changes in pH observed duringan acid reflux episode. This is the reason why,although the optimum time window for symp-tom analysis of 24 hour pH monitoring isconsidered to be the two minutes preceedingthe symptom event,'9 in this study we used atime window of two minutes either side of thesymptom event. It should be noted, however,that despite this larger time window, symptomepisodes were still much more frequently asso-ciated with acid reflux than with bile reflux.
Despite the fact that in group 1 29% and ingroup 2 62% of symptoms are related to a bile
a)
co0-
JEEL---Jlivi
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from

186Marshall, Anggiansah, Owen, Owen
M pS _
13:00 15:00 17:00 19:00 21:00
3
23:00
Figure 5: A 12 hour segment ofa 24 hour combinedpH and bile monitoring (oesophagealpH above, bilirubin absorbancebelow) in a patient with gastro-oesophageal reflux. Note how acid reflux episodes are represented by sharp, easily identifiedfalls inpH whereas bile reflux, defined as a bilirubin absorbance >0-14, occurs as slower, less discrete rises in absorbance.
or an acid reflux episode, or both, it should berecognised that the remainder are not, and anexplanation for this should be sought. Onmany occasions, a reflux episode can be ident-ified just outside the four minute time window,and it is possible that this is due to poorsymptom recognition or inadequate regis-tration of the event by the patient. Gastric,biliary or even cardiac disorders may well beresponsible for some of the symptoms. It isinteresting to see that similar proportions of
Figure 6: Photograph ofan antimonypHprobe next to the larger Bilitec bile probe. Note the2 mm gap between the white Teflon head and the end of the opticalfibres in which therefluxate is sampled.
each group had a positive Bernstein test. Thismay well reflect the comparatively poor sensi-tivity and specificity of this test in the detectionof gastro-oesophageal reflux.20 In a study ofpatients with non-cardiac chest pain, Rokkaset alP found that only 67% of patients with a
positive Bernstein test had abnormal gastro-oesophageal reflux, so it is possible that someof our patients in group 1 had a motilitydisorder that would have required ambulatorymotility studies to detect.There is a difference ofopinion in the medical
literature over the most appropriate protocol forthe use of Bilitec 2000 in the measurement ofoesophageal bile reflux. In particular, it has beendisputed whether it is better to allow the patientto have an unrestricted diet, and then to excludethe meal and postprandial periods from theanalysis, or whether to specify a diet that avoidsinterference with bilirubin absorbance and toinclude the whole 24 hour time period in theanalysis.22 When 24 hour pH data are normallyanalysed, the whole 24 hours is included, andthe results of this study of symptom analysislend weight to the argument that this should bethe case when analysing bile reflux data as well:46% of all symptoms occurred in the meal andpostprandial periods, and it is often these periodswhen the patients complain most bitterly of theirsymptoms. We believe, therefore, that patientsshould be instructed to have a diet that avoidsinterference with bilirubin absorbance so that thewhole 24 hour period can be included in theanalysis. As long as patients keep a good recordof the foodstuffs they eat, any artefactual rise inbilirubin absorbance can be identified andexcluded from the analysis.
8
7
6-
5-
4
3
2
0.90.8
0.70.6
0.5
0.4
0.3
0.20.1 _
11:00
1
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from

Relationship between acid and bile reflux in GORD
The good correlation between acid refluxand bile reflux reflects the results that havebeen published elsewhere using Bilitec 2000. Itis interesting to observe that despite this goodcorrelation, the number of symptoms related toacid reflux is much greater than the numberrelated to bile reflux. This is so not only ingroup 1 but also in group 2. One of the areasin which it was felt that bile reflux may play apart was in those patients who were sympto-matic and yet had normal pH studies. In thisseries of patients with normal pH studies(group 1), only two of 21 patients had bilereflux, and yet in neither of these was there astrong SI with respect to bile reflux. It seemsthat not only is bile reflux in the absence of acidreflux a rare event in patients with an intactstomach, but that the bile itself is not oftendirectly related to symptom events in thesepatients. A parallel can be drawn here with astudy by Sears et al23 who looked at acid andbile reflux in patients who had undergoneprevious partial gastrectomy. They observedthat 10 of 13 patients had abnormal amountsof duodenogastro-oesophageal reflux and threeof these 10 patients also had excessive gastro-oesophageal acid reflux. It was only these threepatients who had oesophagitis on endoscopy,and in these patients 97% of the symptomswere acid related. They concluded thatalthough excessive amounts of duodenogastricreflux are common in partial gastrectomypatients, oesophagitis is found in those withconcomitant acid reflux, and that most of thesymptoms are acid rather than bile related.
In summary, although the physical character-istics of bile detection using the Bilitec 2000system do not result in discrete reflux episodessuch as are seen with acid reflux, bile itself doesnot seem to contribute to the symptomatologyof oesophageal disease in the same way that aciddoes. It may be, of course, that the nature ofoesophageal bile reflux is different from acidreflux, and the results of Bilitec are reflectingthis. It should be emphasised that this study isconcerned with symptoms, and does not attemptto draw any conclusions with regards to the roleof bile in the pathogenesis of oesophagealmucosal damage. What seems to be certain,however, is that although there is a good corre-lation between the percentage times for oeso-phageal bile and acid reflux within people, bileand acid reflux does not always occur simul-taneously, and the vast majority of symptomevents are asociated with acid reflux episodes.
1 Mittal RK, Reuben A, Whitney JO, McCallum RW. Do bileacids reflux into the oesophagus? A study in normalsubjects and patients with gastroesophageal reflux disease.Gastroenterology 1987; 92: 371-5.
2 Johnsson F, Joelsson B, Floren CH, Nilsson A. Bile salts inthe oesophagus of patients with oesophagitis. Scand JfGastroenterol 1988; 23: 712-6.
3 Hamilton SR, Yardley JH. Regeneration of cardiac typemucosa and acquisition of Barrett's mucosa afteroesophagogastrostomy. Gastroenterology 1977; 72:669-75.
4 Iftikhar SY, Ledingham S, Steele RJ, Evans DF, Lendrum K,Atkinson M, et aL Bile reflux in columnar-lined Barrett'soesophagus. Ann R Coll Surg Engl 1993; 75: 411-6.
5 Miwa K, Hattori T, Miyazaki I. Duodenogastric reflux andforegut carcinogenesis. Cancer 1995; 75: 1426-32.
6 Houghton PW, Mortensen NJ, Thomas WE, Cooper MJ,Morgan AP, Davies P, et al. Intragastric bile acids andscintigraphy in the assessment of duodenograstric reflux.BrjSurg 1986; 73: 292-4.
7 Iftikhar SY, Ledingham S, Evans D, Yusuf SW, Steele RJC,Atkinson M, et al. Alkaline gastro-oesophageal reflux:dual pH probe monitoring. Gut 1995; 37: 465-70.
8 Baldini F, Falciai R, Scheggi AM, Bechi P. A new fibre-opticsensor for bile reflux. In: Proceedings optical fiber sensors(OFS '88) (New Orleans, Louisiana). Norwood,Massachusetts: Artech House, 1988: 353-6.
9 Bechi P, Pucciani F, Baldini F, Cosi F, Falciai R, Mazzanti R,et al. Long-term ambulatory enterogastric reflux moni-toring. Validation of a new fibreoptic technique. Dig DisSci 1993; 38: 1297-306.
10 Vaezi MF, Lacamera RG, Richter JE. Validation studies ofBilitec 2000: an ambulatory duodenogastric reflux moni-toring system. Amj Physiol 1994; 267: G1050-7.
11 Caldwell MT, Byrne PJ, Brazil N, Crowley V, Attwood SE,Walsh TN, et al. An ambulatory bile reflux monitoringsystem: an in vitro appraisal. Physiol Meas 1994; 15:57-65.
12 Vaezi MF, Richter JE. Synergism of acid and duodeno-gastroesophageal reflux in complicated Barrett'sesophagus. Surgery 1995; 117: 699-704.
13 Champion G, Richter JE, Vaezi MF, Singh S, Alexander R.Duodenogastroesophageal reflux: relationship to pH andimportance in Barrett's oesophagus. Gastroenterology1994; 107: 747-54.
14 Marshall REK, Anggiansah A, Owen WA, Owen WJ.Oesophageal acid and bile reflux correlate well: norelationship to alkaline pH. Gut 1996; 38: A25.
15 Wiener GJ, Richter JE, Copper JB, Wu WC, Castell DO.The symptom index: a clinically important parameter ofambulatory 24-hour esophageal pH monitoring. Am JGastroenterol 1988; 83: 358-61.
16 Breumelhof R, Smout AJ. The symptom sensitivity index:a valuable additional parameter in 24 hour oesophagealpH recording. Am J Gastroenterol 1991; 86: 160-4.
17 Johnston BT, McFarland RJ, Collins JSA. The binomialsymptom index: correlating oesophageal symptoms withacid reflux. Gastroenterology 1992; 102: A92.
18 Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-associationprobability: an improved method for symptom analysis of24-hour esophageal pH data. Gastroenterology 1994; 107:1741-5.
19 Lam HG, Breumelhof R, Roelofs JM, Van BergeHenegouwen GP, Smout AJ. What is the optimal timewindow in symptom analysis of 24-hour oesophagealpressure and pH data. Dig Dis Sci 1994; 39: 402-9.
20 Richter JE, Hewson EG, Sinclair JW, Dalton CB. Acidperfusion test and 24-hour oesophageal pH monitoringwith symptom index: a comparison of tests for oeso-phageal acid sensitivity. Dig Dis Sci 1991; 36: 565-71.
21 Rokkas T, Anggiansah A, McCullagh M, Owen WJ. Acidperfusion and edrophonium provocation tests in patientswith chest pain of undetermined aetiology. Dig Dis Sci1992; 37: 1212-6.
22 Marshall REK, Anggiansah A. Ambulatory oesophageal bilereflux monitoring in Barrett's oesophagus. Br J Surg1996; 83: 425-6.
23 Sears RJ, Champion GL, Richter JE. Characteristics ofdistal partial gastrectomy patients with oesophageal symp-toms of duodenogastric reflux. Am J Gastroenterol 1995;90: 211-5.
187
on July 31, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.40.2.182 on 1 February 1997. D
ownloaded from