MEDTRONIC GASTROENTEROLOGY Bile Reflux and Bilitec System.
24
MEDTRONIC GASTROENTEROLOGY Bile Reflux and Bilitec System
-
Upload
maya-mapstone -
Category
Documents
-
view
224 -
download
0
Transcript of MEDTRONIC GASTROENTEROLOGY Bile Reflux and Bilitec System.

MEDTRONICGASTROENTEROLOGY
Bile Reflux and Bilitec System

MEDTRONICGASTROENTEROLOGY
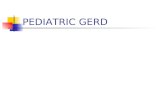
What is DG- or DGE- Reflux?
Retrograde movement of duodenal content such as bile, pancreatic and enteric juices to the stomach and esophagus:
Duodeno-Gastric Reflux (DGR)
Duodeno-Gastro-Esophageal Reflux (DGER)Stomach
Sphincter of Oddi
Gallblader
Pancreas
Duodenum
Bile reflux
Acid reflux
Esophagus
LES

MEDTRONICGASTROENTEROLOGY
Indications
Patients with symptoms of gastroesophageal reflux (GER) Evaluation in patients with complications of GER such as:
Barrett’s esophagus Strictures Ulceration of the esophagus
Patients that have failed medical therapy for acid reflux Patients with poor response to medical treatment of reflux
esophagitis Postgastrectomized patients with reflux symptoms Pre- and postoperative evaluation of anti-reflux surgery

MEDTRONICGASTROENTEROLOGY
How to Measure DG- and DGE- Reflux
The Bilitec System has been recognized as being the best method for detecting duodenogastric/bile reflux
4 studies has validated that:
Bilirubin is a suitable marker to measure the presence of bile acids – i.e. demonstrate that there is a correlation between Bilitec readout (presence of bilirubin) and presence of biliary salts
In-vivo spectrophotometric reading of Bilitec is reliable - i.e. compare Bilitec reading with spectrophotometric measurements carried out on samples drawn from the stomach and/or esophagus; this could be defined as optical validation

MEDTRONICGASTROENTEROLOGY
Why is Bile Reflux Important?
The main reason to measure bile-reflux is based on the indications that in GERD, duodenal juice is an important component in the refluxed gastric juice that causes damage to the esophageal mucosa.

MEDTRONICGASTROENTEROLOGY
Composition of Refluxed Juice in GERD*
*From DeMeester et al: Biology of Gastroesophageal Reflux Disease, 1999

MEDTRONICGASTROENTEROLOGY
Is measurement of DGR/DGER relevant?
Bile Reflux
Increased Risk for Mucosal Damage
The clinical benefit of the Bilitec system is to identify patients at risk for: Mucosal injuryBarret’s esophagusHigh grade dysplasia.
Select patients for further examination of esophageal damage (e.g. biopsy) and for whom anti-reflux surgery should be considered

MEDTRONICGASTROENTEROLOGY
Examples of Bile reflux studies
“Patients with erosive esophagitis and Barrett’s metaplasia have increased esophageal exposure to duodenal juice compared to normal subjects”, Kauer et al, 1995
“The combined reflux of gastric and duodenal juices causes severe esophageal mucosal damage. The vast majority of duodenal reflux occurs at a pH range of 4 to 7, at which bile acids, the major component of duodenal juice, are capable of damaging the esophageal mucos”, Kauer et al, 1995
“Duodenal juice adds a noxious component to the refluxed gastric juice and potentiates the injurious effects of gastric juice on the esophageal mucosa” Fein et al, 1997
“The prolonged simultaneous attack of bile and acid may play a key role in the development of Barrett's metaplasia”, Menges et al, 2001
...

MEDTRONICGASTROENTEROLOGY
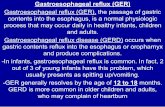
Detection of Bile/Bilirubin
Bilitec uses two wavelengths for detection of bilirubin: 470 nm and 565 nm
The absorbance is calculated from Beer’s law based on light intensities transmitted in absence and presence of absorbing substance (bilirubin)
The absorbance is proportional to the concentration of bilirubin however, Bilirubin is only a marker and the knowledge of its concentration is not important from a clinical point of view
Bilitec measures the exposure time of bile-containing reflux to the gastric-/esophageal mucosa
nm400 500 600 700 800
A
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Absorption spectrum of a gastric sample containing bile

MEDTRONICGASTROENTEROLOGY
Normal values
Normal values proposed by P.Bechi for gastric studies:Pct. Time of bilirubin exposure>0.14 in proximal stomach*
Stomach
Total: 12.9 %Supine: 24.2 %Upright: 4.0 %*Bilitec probe placed 10 cm below LES lower boarder
Normal values from Kauer, DeMeester et al for esophageal studies:Pct. Time of esophageal* bilirubinexposure >0.2
Esophagus
Total: 2.9 %Supine: 0.4 %Upright: 4.0 %*Bilitec probe placed 5 cm above LES upper boarder

MEDTRONICGASTROENTEROLOGY
Selection of Absorbance Threshold
A default threshold of 0.14 in absorbance values is considered in all the validations. This is the threshold introduced by P. Bechi: “it is the lowest value where the absorbance can be considered as an actual measurement of bilirubin and not as noise due to mucus in the stomach”
There are different opinions on the threshold level, and in other studies higher absorbance values are used as threshold (e.g. 0.2 and 2.5).
From presentation by T.DeMeester, DDW, 2001

MEDTRONICGASTROENTEROLOGY
Correction of absorbance values rel. pH
Is Bile reflux underestimated in an acidic environment?
This is a controversial subject discussed in a few papers: J.Richter: 30% underestimation of Bilitec reading for pH<3.5 P.Bechi: 18% underestimation of Bilitec reading for pH<3.5 J.Janssens: such underestimation has only minor effect on the
results of Bile reflux testing and thereby, have no clinical impact.
Only few centers consider this in their analysis of Bile reflux

MEDTRONICGASTROENTEROLOGY
Bilitec System Components
Fiber Optic Catheter
Bilitec 2000 Carrying case Cable for serial interface Optical calibration chambers Manuals
Fiber Optic Bile Catheter Single-use catheter, length 175 cm, diam. 3.0 mm
Bile Upload and analysis option for P98 pH
Note: Available in US when 510(k) cleared

MEDTRONICGASTROENTEROLOGY
The Bilitec Procedure
Set-up Bilitec 2000 device Set average time and 1 or 2 channels Calibrate Bilitec system in water
Intubate patient with single-use fiber optic probe w/wo pH recording
Start the measurement Standard Diet: abs. < 0.05 at 470 nm Patient Keeps Diary: symptoms & events
Extubate patient, upload and analyze data

MEDTRONICGASTROENTEROLOGY
Features and Benefits
Features BenefitsUp to 2 channels can be recordersimultaneously over 24 hours
Perform simultaneous gastric- and esophagealbile studies.
Compatible with both Polygram 98 pH TestingApplication, PW EsopHogram Reflux AnalysisModule and DOS EsopHogram
Current users can analyze data using theirexisting Medtronic software.
Single-Use optic probe and Calibration is easilydone in water before each study
Limited resources and no special componentsneeded for preparation of the system
Absorbance threshold can be defined by user Ability to set reflux threshold to match everystudy design
Correction algorithm of bile values can beenabled in protocol settings
Ability to adjust for underestimation of bile refluxin acid environment (if required)
Record and analyses data for 24 hours Evaluate the circadian pattern of bile reflux, i.e.total, upright, supine periods and correlatesymptoms to reflux episodes.

MEDTRONICGASTROENTEROLOGY
Polygram Bile Analysis Software
Technical Review of the Software

MEDTRONICGASTROENTEROLOGY
Protocol Settings
0-4 channels pH and1-2 channels Bile
Adjustment of Bile values

MEDTRONICGASTROENTEROLOGY
Protocol Settings
Analysis of Bile Reflux:

MEDTRONICGASTROENTEROLOGY
Bile Analysis

MEDTRONICGASTROENTEROLOGY
Upload Procedure for Combined Studies
Upload pH data first
…awaiting data from the Bilitec2000 device connect Bilitec to the serial port go to data transfer mode and press “Enter”
NB: Uses Digitrapper time for Combined Studies- the Bilitec 2000 has no Clock

MEDTRONICGASTROENTEROLOGY
Capture View

MEDTRONICGASTROENTEROLOGY
Review view

MEDTRONICGASTROENTEROLOGY
Combined pH and Bile Report

MEDTRONICGASTROENTEROLOGY
Pitfalls
Variety of substances in food may result in false-positive readings.- Therefore, it is important to use a modified diet.
If long periods of bile reflux are recorded, this may be simply a “contaminated” detector or other artifact.
Presence of blood may distort the readings obtained from the device
Underestimation of bile reflux in an acid environment (pH < 3.5)