
The Pelleve Procedureeee.pelleve.com/pdf/The-Pelleve-Procedure-CC11067.pdf · Private Practice, 115...
12
Transcript of The Pelleve Procedureeee.pelleve.com/pdf/The-Pelleve-Procedure-CC11067.pdf · Private Practice, 115...


Author's personal copy
The Pelleve Procedure:an Effective Method forFacial Wrinkle Reductionand Skin TighteningMichael Stampar, DO
The use of thermal injury to rejuvenate and repairaging facial skin has been part of the nonsurgicalskin treatment for decades.1 Ablative light-basedenergies, the gold standard being full carbondioxide laser resurfacing, offered the potential forremarkable smoothing and moderate tighteningat a superficial level but came with significantpain, downtime, healing complications, and un-wanted pigment-related changes.2 To reduce thedowntime and complications, lesser-ablative andnonablative wavelengths were devised, but con-sistent results were still dependent on having theproper skin type, dosing, and healing response.The advent of the use of radiofrequency (RF)energy represented a change away from light-based energy, dependant on generating heat byabsorption of energy by a target chromophore.
High-frequency electron flow, RF, generatesheat because of the differences in impedancebetween tissue types (Fig. 1).
Streaming electrons flow through the low resis-tance of the epidermis and dermis and meet thehighly resistant fat at the dermal-subdermal junc-tion. The suddenchange in impedance turns kineticenergy into thermal energy, and the surroundingtissues are heated. Thismethod not only eliminatesthe problem of heating unwanted target chromo-phores in the skin, such as melanin, as seen withlight-based lasers, but also allows the heat to be
generated in the deep dermis where existingresidual collagen bundles are most plentiful. Alsopresent at the dermal-subdermal junction are theconnections of subdermal connective tissue bandsthat run through the subdermal fat to the underlyingfascia. A controlled thermal injury reaching thethreshold temperature for denaturing collagen of60!C to 65!C can cause contraction of the thinnedcollagen in the deep dermis immediately and triggeran inflammatory response that generates newcollagen bundle reorganization and thickeningevident at 12 weeks as seen on electron micro-scopy.3,4 Controlled thermal contraction down thedeep connective tissue bands causes a vertical and3-dimensional tissue contraction, compacting thefatty globules without injuring the fat itself (Fig. 2).
This mechanism is in contrast to that of uncon-trolled thermal injury in which temperatures ob-tained in deep tissue can reach or exceed 70!C,causing a necrotic injury, irregular wound con-traction, fat loss, and atrophy, which has been re-ported with pulsed devices.5 Despite the potentialbenefits of deep RF dermal heating, the pain asso-ciated with the treatments and the inability togenerate consistently predictable results continueto plague this technology.6
The shortcomings of pulsed RF-based devicesinclude the need to deliver a safe dose withoutcrossing the heat threshold that results in tissue
Disclosures: The author is a paid trainer of new users of the Ellman device. Training travel expenses are paid byEllman. The author neither holds equity in Ellman nor profit sharing in company sales.Private Practice, 115 Taylor Street, Punta Gorda, FL 33950, USAE-mail address: [email protected]
KEYWORDS
" Pelleve procedure " Monopolar radiofrequency" Dermal heating " Facial wrinkle reduction " Skin tightening" Cosmetic procedures
Facial Plast Surg Clin N Am 19 (2011) 335–345doi:10.1016/j.fsc.2011.05.0121064-7406/11/$ – see front matter ! 2011 Elsevier Inc. All rights reserved. fa
cialplastic
.theclin
ics.com

Author's personal copy
necrosis.7 To assure this safety, the treatmentprotocols are typically the same for all patients,not allowing customization of thedosing to improvetreatment outcomes. However, it is obvious thatnot all skins respond equally to the same amountof energy, thus, the reputation for unpredictableresults. Pulsed devices also raise the temperaturesrapidly, which can cause pain and necessitatessurface cooling to prevent superficial burns.However, without the control of the actual depthof cooling, favorable thermal effects on the dermis,such as wrinkle reduction, horizontal contraction,and shrinkage of pores, can be limited in thinned-skin individuals because of the excessive coolingof themiddle to upper dermis. The need to optimize
these treatment parameters of the myriad ofdevices available has been emphasized by manyinvestigators who have evaluated the devices thathave come into the market.8,9
MECHANISM OF CONTROLLED THERMALINJURY
The Pelleve procedure, performed using the 4.0 S5Surgitron (Ellman International, Oceanside, NY,USA), differs from other methods of delivering RFenergy because it delivers a progressive but con-trolled thermal injury to the dermis and subdermisand overcomes many of the shortcomings associ-ated with pulsed and fixed dosed methods.
Fig. 1. Principles of RF energy.
Fig. 2. Progressive heating of connective tissue bands, and contraction of fat compartment.
Stampar336
Author's personal copy
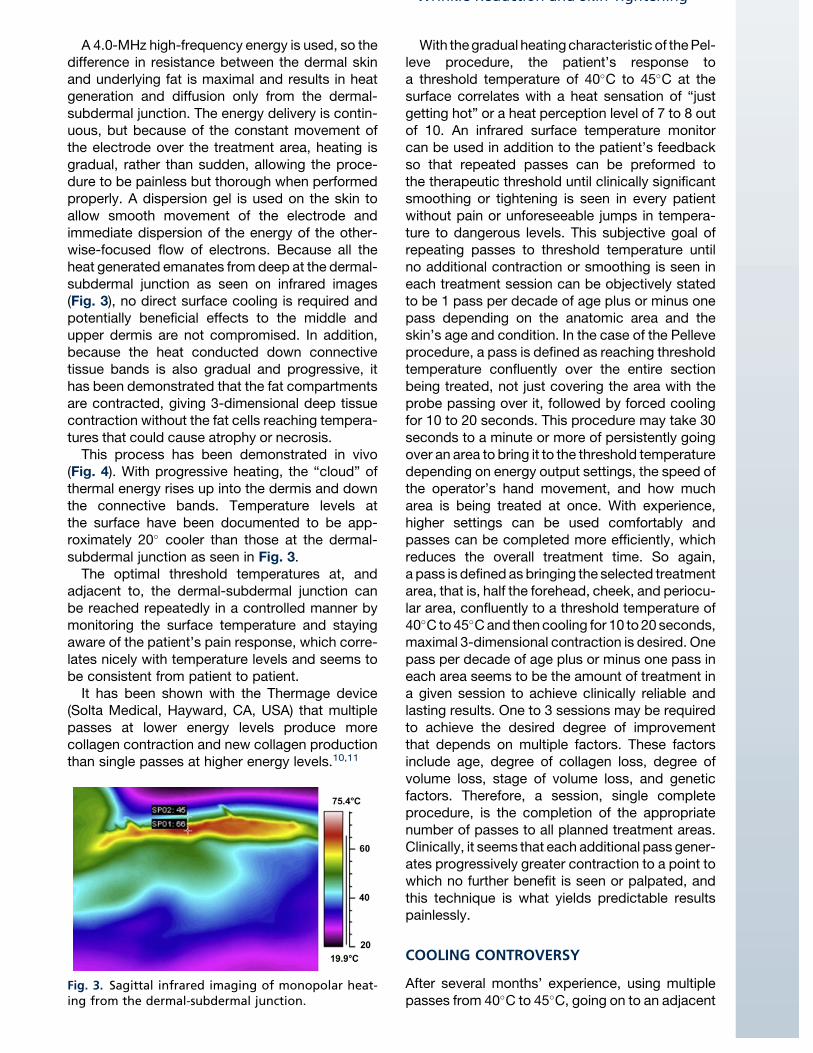
A 4.0-MHz high-frequency energy is used, so thedifference in resistance between the dermal skinand underlying fat is maximal and results in heatgeneration and diffusion only from the dermal-subdermal junction. The energy delivery is contin-uous, but because of the constant movement ofthe electrode over the treatment area, heating isgradual, rather than sudden, allowing the proce-dure to be painless but thorough when performedproperly. A dispersion gel is used on the skin toallow smooth movement of the electrode andimmediate dispersion of the energy of the other-wise-focused flow of electrons. Because all theheat generated emanates fromdeep at the dermal-subdermal junction as seen on infrared images(Fig. 3), no direct surface cooling is required andpotentially beneficial effects to the middle andupper dermis are not compromised. In addition,because the heat conducted down connectivetissue bands is also gradual and progressive, ithas been demonstrated that the fat compartmentsare contracted, giving 3-dimensional deep tissuecontraction without the fat cells reaching tempera-tures that could cause atrophy or necrosis.
This process has been demonstrated in vivo(Fig. 4). With progressive heating, the “cloud” ofthermal energy rises up into the dermis and downthe connective bands. Temperature levels atthe surface have been documented to be app-roximately 20! cooler than those at the dermal-subdermal junction as seen in Fig. 3.
The optimal threshold temperatures at, andadjacent to, the dermal-subdermal junction canbe reached repeatedly in a controlled manner bymonitoring the surface temperature and stayingaware of the patient’s pain response, which corre-lates nicely with temperature levels and seems tobe consistent from patient to patient.
It has been shown with the Thermage device(Solta Medical, Hayward, CA, USA) that multiplepasses at lower energy levels produce morecollagen contraction and new collagen productionthan single passes at higher energy levels.10,11
With thegradual heatingcharacteristic of thePel-leve procedure, the patient’s response toa threshold temperature of 40!C to 45!C at thesurface correlates with a heat sensation of “justgetting hot” or a heat perception level of 7 to 8 outof 10. An infrared surface temperature monitorcan be used in addition to the patient’s feedbackso that repeated passes can be preformed tothe therapeutic threshold until clinically significantsmoothing or tightening is seen in every patientwithout pain or unforeseeable jumps in tempera-ture to dangerous levels. This subjective goal ofrepeating passes to threshold temperature untilno additional contraction or smoothing is seen ineach treatment session can be objectively statedto be 1 pass per decade of age plus or minus onepass depending on the anatomic area and theskin’s age and condition. In the case of the Pelleveprocedure, a pass is defined as reaching thresholdtemperature confluently over the entire sectionbeing treated, not just covering the area with theprobe passing over it, followed by forced coolingfor 10 to 20 seconds. This procedure may take 30seconds to a minute or more of persistently goingover an area to bring it to the threshold temperaturedepending on energy output settings, the speed ofthe operator’s hand movement, and how mucharea is being treated at once. With experience,higher settings can be used comfortably andpasses can be completed more efficiently, whichreduces the overall treatment time. So again,a pass is defined as bringing the selected treatmentarea, that is, half the forehead, cheek, and periocu-lar area, confluently to a threshold temperature of40!C to45!Cand thencooling for 10 to 20 seconds,maximal 3-dimensional contraction is desired. Onepass per decade of age plus or minus one pass ineach area seems to be the amount of treatment ina given session to achieve clinically reliable andlasting results. One to 3 sessions may be requiredto achieve the desired degree of improvementthat depends on multiple factors. These factorsinclude age, degree of collagen loss, degree ofvolume loss, stage of volume loss, and geneticfactors. Therefore, a session, single completeprocedure, is the completion of the appropriatenumber of passes to all planned treatment areas.Clinically, it seems that each additional pass gener-ates progressively greater contraction to a point towhich no further benefit is seen or palpated, andthis technique is what yields predictable resultspainlessly.
COOLING CONTROVERSY
After several months’ experience, using multiplepasses from 40!C to 45!C, going on to an adjacent
Fig. 3. Sagittal infrared imaging of monopolar heat-ing from the dermal-subdermal junction.
Wrinkle Reduction and Skin Tightening 337

Author's personal copy
area to allow spontaneous cooling of the treatedarea, and then returning to the treatment area,the possibility that the progressive swelling occur-ring with each pass might overcome the ability foracute tissue contraction became apparent. At thattime, I began cooling the treated area directly withfrozen reusable cold packs to force contraction ofthe solid proteins that were being heated and, atthe same time, minimized the acute swellingassociated with repeated heating. The immediatecontraction and firming of the treated area wasapparent, and it allowed repeated passes of con-tinuing RF energy on the same areas until maximalcontraction was seen without having to go to adja-cent areas to allow passive cooling to occur. Afteronly 20 to 30 seconds of cooling, the subsequentpasses seemed to trigger an even more significantcontraction without the swelling seen when lettingthe tissue cool passively. The distance betweena point on the nasolabial fold and the tragus, forinstance, increases after a pass of heat solelybut decreases after a pass followed by cooling.The principle of physics governing cooling solidsis that all solids, except water, contract with cool-ing. If application of cold causes even a fraction ofa millimeter of additional contraction of the dena-tured collagen, then each subsequent pass wouldreach that much deeper and cause greater con-traction and increase the density of the layers ofdeep dermal collagen. This occurrence is apparenton pinching the skin after each pass of hot andcold application.Some investigators have suggested that heat
shock proteins triggered by the injury could beadversely affected.12 It was shown that only cool-ing at or less than 5!C adversely affected thetissue’s response to injury, and cooling to thatlevel is not advocated here.To document what I have observed over the
past several years, 10 consecutive patients were
treated with one side heated to threshold temper-ature and then cooled for 30 seconds using aniced stainless steel roller and the other side of theface heated to threshold but left to cool passivelywhile an adjacent area was treated. The midfacewas treated at a setting of 80 for 5 passes; theforced cooling for 30 seconds reduced thetemperature to 20!C to 24!C. The opposite mid-face was treated at the same level for 5 passesbut allowed to come to baseline temperature ofapproximately 33!C passively while an adjacentarea was treated. The acute evaluation at theend of the treatment session and an evaluation 1month later revealed significantly more contractionand lift on the side with cold applied for forcedcontraction at both end points. All 10 patients feltthat the side with cold applied for forced contrac-tion felt tighter at rest and felt denser whenpinched relative to the passively cooled side. Allpatients were then treated the opposite way,and, at the end of the second month, all felt equallytight. The acute response at the end session wasthe same, the cooled side felt tighter and denser.All 10 patients also felt that the 2 treatmentsgave significant firmness and tightening to theirskin, greater with the second treatment, andeach could see an obvious contraction throughthe midface relative to their pretreatment photos.
INDICATIONS
The ideal candidates for the Pelleve procedure arefrom their late 30s to mid-40s showing somevisible lines at rest, some midface laxity and upperface volume loss, and early neck softening. At thisstage, with firm dermal support, all these signs ofaging can be significantly reduced or erased witha single treatment or with a second treatment ifcomplete improvement is not seen 4 to 6 monthslater. The typical Pelleve patients in Southwest
Fig. 4. Infrared images: in vivo abdominal flap.
Stampar338

Author's personal copy
Florida are in their early 50s to mid-60s and havesignificant wrinkles at rest, nasolabial and melola-bial folds, neck laxity, and midface ptosis. Thedegree of severity of these findings relative tothe patient’s chronologic age helps predict thesuccess of the procedure outcome and howmany sessions will be required to achieve a clini-cally obvious and satisfactory result. Most patientsrespond to 2 sessions delivering a pass perdecade to each treated area, but fuller faces,extremely thick dermis, and male faces require 3sessions. Regardless of the chronologic age, theskin responds more promptly with generousdermal density; those with a greater overall volumeloss and loss of dermal collagen integrity respondless favorably. However, all skins become moresmooth and firm when enough passes to thresholdtemperature are delivered in a single session.Long-term observations allow patients to be toldin the middle of their aging process that the proce-dure typically needs to be repeated every 12 to 18months. The youngest and oldest patients are toldthat it may last for 2 years or more, always relativeto how fast they are losing volume. Treatmentsessions 4 to 6 weeks apart allow the acuteresponse to the thermal injury to subside. Severalexperienced physicians from Japan and Russiatreat every 2 weeks for a total of 3 sessions andfeel no detriment to this schedule. Some patientshave been treated as soon as 3 weeks and haveseen significant additional smoothing and tight-ening at that time. In fuller faces, less dramaticchanges should be expected with the first proce-dure because much of the initial contraction is inthe anteroposterior dimension, which is more diffi-cult for the patient to appreciate. Once this slack is
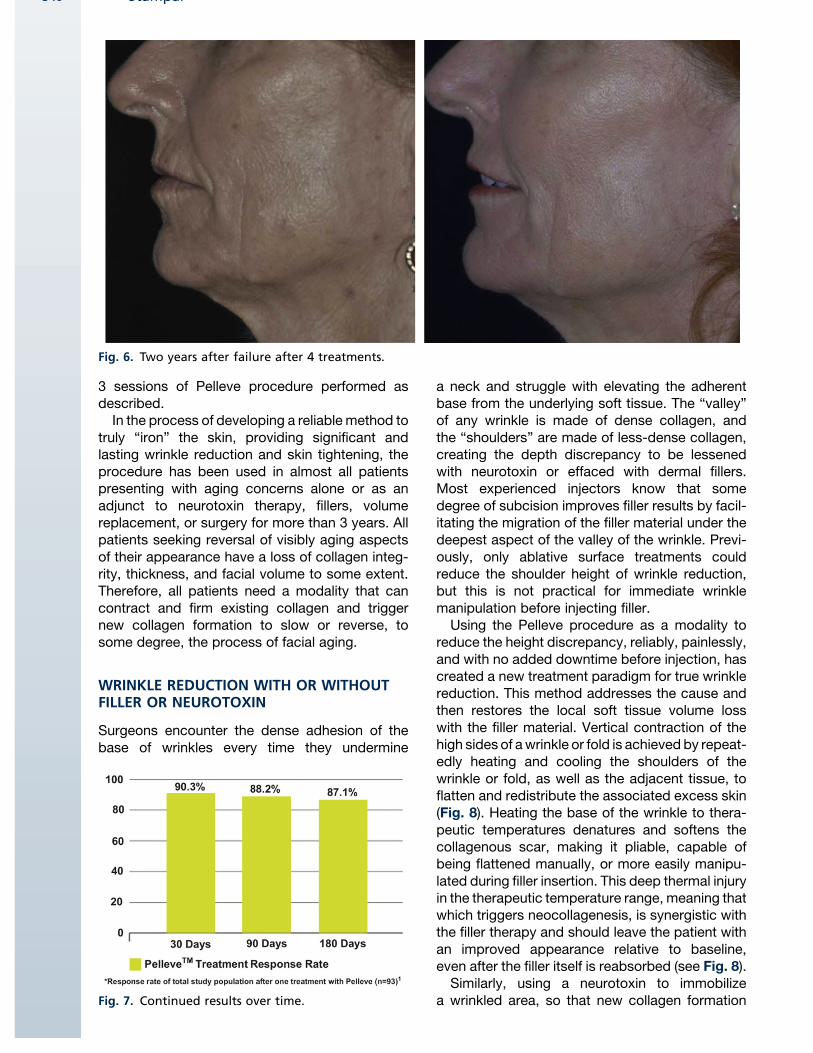
taken up, further contraction results in moreobvious horizontal contraction. One patientconsidered a failure after 4 sessions returned after2 years and showed a remarkable and persistentimprovement in skin laxity and the depth of severalfacial folds (Figs. 5 and 6).
In the United States, the Pelleve procedure hasreceived the Food and Drug Administration (FDA)clearance for the treatment of mild to moderatefacial wrinkles for skin types I to IV with a durationclaim of 6 months. In their submission to the FDA,87% of the patients receiving a single treatmentshowed persistent results at 6 months (Fig. 7).
In my experience since April 2007, I have seenresults last 18 months or more and as long as 4years in a case of sculpting the midface. Mostpatients older than 50 years, having no othercosmetic treatment other than 1 to 2 treatmentsessions with the Pelleve procedure, return 18 to24 months later with complaints of progressiveaging. Examination of the treated areas usuallyreveals volume loss resulting in recurring skin laxity.No patient failed to respond to a single additionalPelleve procedure at the time of retreatment, withimproved skin tightness, density, and smoothing.
Given that the process of denaturing and con-tracting the collagen proteins is irreversible,persistence of the result depends on the degreeof improvement achieved, the degree of volumeloss, and the rate of aging, which includes furtherloss of collagen, native or newly developed withthe procedure. Obviously, the younger the patientand thicker the dermal collagen at the time of theprocedure, the longer the result remains visiblyapparent. From the perspective of an acuteresponse, no patient has failed to respond to 1 to
Fig. 5. Two years after failure after 4 treatments.
Wrinkle Reduction and Skin Tightening 339
Author's personal copy
3 sessions of Pelleve procedure performed asdescribed.In the process of developing a reliable method to
truly “iron” the skin, providing significant andlasting wrinkle reduction and skin tightening, theprocedure has been used in almost all patientspresenting with aging concerns alone or as anadjunct to neurotoxin therapy, fillers, volumereplacement, or surgery for more than 3 years. Allpatients seeking reversal of visibly aging aspectsof their appearance have a loss of collagen integ-rity, thickness, and facial volume to some extent.Therefore, all patients need a modality that cancontract and firm existing collagen and triggernew collagen formation to slow or reverse, tosome degree, the process of facial aging.
WRINKLE REDUCTION WITH OR WITHOUTFILLER OR NEUROTOXIN
Surgeons encounter the dense adhesion of thebase of wrinkles every time they undermine
a neck and struggle with elevating the adherentbase from the underlying soft tissue. The “valley”of any wrinkle is made of dense collagen, andthe “shoulders” are made of less-dense collagen,creating the depth discrepancy to be lessenedwith neurotoxin or effaced with dermal fillers.Most experienced injectors know that somedegree of subcision improves filler results by facil-itating the migration of the filler material under thedeepest aspect of the valley of the wrinkle. Previ-ously, only ablative surface treatments couldreduce the shoulder height of wrinkle reduction,but this is not practical for immediate wrinklemanipulation before injecting filler.Using the Pelleve procedure as a modality to
reduce the height discrepancy, reliably, painlessly,and with no added downtime before injection, hascreated a new treatment paradigm for true wrinklereduction. This method addresses the cause andthen restores the local soft tissue volume losswith the filler material. Vertical contraction of thehigh sides of awrinkle or fold is achieved by repeat-edly heating and cooling the shoulders of thewrinkle or fold, as well as the adjacent tissue, toflatten and redistribute the associated excess skin(Fig. 8). Heating the base of the wrinkle to thera-peutic temperatures denatures and softens thecollagenous scar, making it pliable, capable ofbeing flattened manually, or more easily manipu-lated during filler insertion. This deep thermal injuryin the therapeutic temperature range, meaning thatwhich triggers neocollagenesis, is synergistic withthe filler therapy and should leave the patient withan improved appearance relative to baseline,even after the filler itself is reabsorbed (see Fig. 8).Similarly, using a neurotoxin to immobilize
a wrinkled area, so that new collagen formation
Fig. 6. Two years after failure after 4 treatments.
Fig. 7. Continued results over time.
Stampar340

Author's personal copy
after the Pelleve procedure can be generatedwithout the repetitive crush-inducing movementthat caused the wrinkle, should lead to moreeffective flattening of the wrinkle. The denaturedcollagen is softened and flattened, and newcollagen can be laid down to restore some of theloss that led to the wrinkle being visible at rest.These expected results have now been observedroutinely. Patients who underwent filler therapy re-turning 1 year after filler placement pretreated withPelleve procedure persist to have an improvementover baseline, despite the need to augment thesoft volume deficit. Although the Pelleve proce-dure can reduce the resting depth of wrinkleswhen used alone, patients who have undergonethe procedure in the forehead and perioculararea while the area is immobilized with neurotoxinreturn for repeat neurotoxin treatment and showreduced or, occasionally, imperceptible wrinklesat rest relative to their appearance before theprocedure.
SKIN TIGHTENING AND VOLUMECONTRACTION WITH OR WITHOUTVOLUME REPLACEMENT
The Pelleve procedure is also a valuable adjuncttherapy to facial volume restoration. The midfacialskin envelope becomes lax as panfacial volumeloss occurs. Contraction of the connective tissuebands that tether the skin to the deep fasciacontracts and firms the soft tissue compartment.With decreased compliance, the volume deliveredhas a greater volumizing effect. I have used thePelleve procedure as an adjunct to facial volumerestoration for more than 3 years and seen a syner-gistic effect of triggering new collagen formation.With poly-L-lactic acid (PLLA), “seeds of newcollagen growth” via a controlled foreign bodyreaction are laid down in the same anatomic planethat the Pelleve is triggering new collagen growthvia a response to thermal injury. The PLLA injection
procedure can be administered immediately afterthe Pelleve procedure to bolster the lift andcontraction achieved with a properly performedmidface tightening (Fig. 9). This routine exampleshows how the skin envelope can be contractedto the residual volume even with an acute weightloss in a woman in her late 50s.
METHOD
It should be noted that this method is consistentlyreferred to as a procedure, not a treatment,a semantic distinction important to obtainingconsistent results. Most light-based technologyand other RF energy devices have set dosingprotocols that define a treatment session, usuallydeveloped to be within established safe dosingparameters. The use of the continuous RF energydelivery, with the end point being an obvious clin-ically evident smoothing and tightening of the skin,has to be approached as a procedure, not unlikea surgery in which certain steps are taken andcustomized to the patient’s needs to reach anoptimal end point. As with surgery, that end pointshould satisfy the provider and the patient.
In evaluating each patient before starting theprocedure, standard 5 position photos, verticallyoriented hairline to clavicle in height and pinna-to-pinna in width, should be taken. The subject’sface should then be assessed for asymmetryside to side in cheek height and fullness and inthe flair of the jaw line. See Video 1 online [www.facialplastic.theclinics.com]. With few exceptions,all patients have 3 to 10 mm of asymmetry in thevertical height and length of one side of the facecompared with the other when measuring fromthe lateral canthus to a point on the jawline directlybelow it. The higher side is also most often fullerwith greater overall midface volume, whereas thelower side is shorter with greater volume loss. Itis important that this difference be demonstratedto the patient for 2 reasons. First, the patient
Fig. 8. Rf treatment of glabellar lines and the forehead prior to filler injection.
Wrinkle Reduction and Skin Tightening 341

Author's personal copy
should not notice this difference for the first time inthe postprocedure period and think that the proce-dure created the asymmetry. Second, it is vital totreat the high side first and exaggerate the asym-metry so that at the half-treated point, the patientwill be impressed with the degree of change achie-ved. If the low side is treated first, the patients whomay have never seen themselves as anything butsymmetric in the past will be unimpressed if thelow side is brought up even with the untreatedhigh side. The flair of the body of the jaw is lessoften an issue, but, in many patients, one sidetapers posteriorly at 45!, whereas the other sidetapers back at 60!. If the providers fail to noticethis asymmetry, they may grow frustrated tryingto get the midface to taper symmetrically whenthe bony skeletal support is the cause, and notsoft tissue fullness. Discussing these findingsbuilds patient confidence in the providers’ under-standing of the anatomy and also opens the doorto discuss volume replacement filler therapy toachieve more youthful height on the low side orbalance the face overall after the skin sleeve hasbeen tightened (Fig. 10).All makeup should be removed from treatment
areas; jewelry and hearing aids should beremoved. Men should be clean shaven. Beardedskin cannot be treated because of the spark gapcreated by the hair density and thickness, but no
effect on underlying hair follicle growth has beenobserved clinically. The Pelleve procedure is per-formed on the facial skin surface where wrinklesand underlying laxity predisposing to wrinklesare present. A 7.5, 10.0, 15.0, or 20.0 mm monop-olar electrode handpiece transfers the energy tothe patient from the ellman S5 Surgitron RF gener-ator and adhesive disposable return pad that isplaced on the upper back skin between theshoulder blades. Pelleve gel is used on all treatedskin and adjacent skin areas to avoid burn injuryfrom applying the RF energy to unprotected skin.Only a thin layer is needed to provide smoothgliding of the electrode on the skin. The treatmentelectrode must always be in contact with thepatient’s skin and gel before activation to avoidgenerating a spark gap that can cause pain anda superficial burn similar in size to a razor nick.The treatment electrode should be deactivatedbefore breaking contact with the skin. Any treat-ment of the periocular skin within the orbital rimrequires plastic eye shields inserted after a topicalanesthetic drop is applied to the cornea.Using settings comfortable for the patient which
can range from 15-80 depending on the areaundergoing treatment, and no anesthetic of anykind that might impair heat perception, the areaof skin is gradually heated to a surface tempera-ture of 40!C to 45!C monitored by a handheld
Fig. 9. The 6-month result after 2 treatments (despite 10-kg weight loss).
Stampar342

Author's personal copy
infrared heat gun or the patient’s response to thelevel of heat as “that’s getting hot.” After hundredsof treatments, the patient’s level of pain percep-tion has been observed to reliably predict skinsurface temperature. The patient is advised thatthe sensation goes from warm to warmer butdoes not have to hurt to work and hotter doesnot mean a better result. The patients are encour-aged to signal if they feel that the heat is about toget too hot to avoid allowing the heat to get to thepoint of the patient reflexively pulling away.Although the handheld infrared temperature gunis helpful in monitoring treatment temperatures,experience allows the treating personnel to moveto adjacent areas or stop treating at the appro-priate temperature. Close observation of skincolor and texture as well as subtle body languageprojected by the patient prevents getting touncomfortable treatment levels.
The ability to rely on patient feedback to guidethe treatment comes from the fact that the toler-able target therapeutic temperature of 40!C to44!C at the surface reflects a 20! differential atthe dermal-subdermal junction, and the responseto the gradual heating is consistent within a fewdegrees from patient to patient. Within that temp-erature range, based on thousands of observa-tions by the author, patients report “that’s gettinghot” or a 7 to 8 out of 10 on a 10-point pain scale.There should be no pain if the provider remainsaware of the tissue and patient response. At45!C to 46!C, most patients spontaneously pullaway. Surface temperatures of 48!C to 50!C,which can cause a necrotic thermal injury, cannot
be reached in an awake subject with no anes-thesia. Temperatures less than 40!C does notdenature type I collagen and does not give effec-tive lasting results and can be tolerated indefi-nitely. The infrared temperature gun is useful inpreventing undertreatment in patient’s whoseskin turns red easily at subthreshold temperatures,such as those with rosacea.
Passes of the energy are repeated after coolingthe area with cold application to force solid tissueand collagen contractions. The cooling is tran-sient, 10 to 15 seconds per area, and typicallytakes the tissue down to temperatures in themid-20s. This heating and cooling is repeated untilno additional visible or palpable tightening andsmoothing is evident. Objectively this proceduretranslates to approximately 1 pass per decade ofage plus or minus 1 pass (ie, 4 passes for a 42-year-old individual and 6 passes for a 65-year-old individual). Foreheads take fewer passes thanthe lower face and heavier skin takes more passesthan thin skin. The cooling can be achieved withany reusable frozen cold pack or a stainless steelroller soaked in ice water. Typically, the face istreated half at a time, forehead to below thejawline, to allow comparison with the untreatedside. Again, as a rule of thumb, 1 pass per decadeof age is needed for optimum contraction, and 1 to3 treatment sessions are needed 4 to 6 weeksapart for maximal long-term results. Single treat-ment sessions can last for 1 year or more inpatients younger than 45 years, 2 treatments areneeded for most patients, and 3 or more treat-ments may be required in extremely heavy or
Fig. 10. Common congenital facial asymmetry.
Wrinkle Reduction and Skin Tightening 343

Author's personal copy
wrinkled skin. No special skin care before or afterthe treatment is needed, and patients can returnto normal activities immediately.
RESULTS
In 4 years of observing hundreds of treated areas,all patients treated had good to excellent results.Although the number of treatment sessionsneeded may vary with age and skin condition, allskins smoothen and tighten when heated repeat-edly in each session to a visible clinical end point.Additional sessions have always yielded greatersmoothing and contraction, and no adverse effecthas been seen with as many as 5 sessions in 6months. Performed properly, the procedureshould be painless and should present little riskof inadvertent superficial burn injury. Results canlast for more than 1.5 years in many patients de-pending on age and indications, with some wrinkleresults showing persistent improvement beyond1.5 years (Fig. 11).
SUMMARY
The Pelleve procedure, done properly and to a trulysignificant clinical end point with each treatment,can reliably smooth and contract facial and neckskin without pain or downtime. The Pelleve repre-sents a vital adjunct to filler procedures and any
antiaging treatment plan, be it surgical or nonsur-gical. The key to success in tightening andsmoothing skin seems to be the ability tocustomize the dose, number of passes withoutconcern for safety, discomfort, or cost. Additionalsafety in performing the Pelleve procedure comesin the form of GlideSafe treatment tips that will bepressure activated, greatly reducing the possibilityof a spark gap if patient contact is lost.
TREATMENT PEARLS
" Always start the procedure on the side ofthe face where the midface appears higherand more full, so at the half-treated point,the result is obvious.
" Always assure you are in contact with thegel and skin before activating the electrode,and deactivate the electrode beforebreaking contact.
" Use a gloved hand and 4 # 4 sponges tostretch the skin in the lateral brow and lowerlateral face while heating, and maintain thetension until cooling is complete.
" In areas, such as the midforehead, upperlip, lateral orbit, and neck, where wrinklereduction is the first priority, do not applycold for forced contraction after the last 1to 2 passes so that the denatured collagen
Fig. 11. Full face treated twice 6 weeks apart in January 2008 (January 23, 2008, to September 9, 2009).
Stampar344

Author's personal copy
can remain hot and amorphous. Physicallysmoothing over these areas firmly with4 # 4 sponges may give even better long-term results.
" Encourage these patients to be pretreatedwith neurotoxin 2 weeks before theirPelleve procedure to avoid “wrinkling yourwork,” and essentially allow the wrinklesto heal immobilized as if they were in a cast.
VIDEO ON PATIENT EVALUATION FORPELLEVE PROCEDURE
A video showing patient evaluation prior to theperforming the Pelleve Procedure is availableonline at www.facialplastic.theclinics.com. Thisvideo focuses on the assessment for asymmetryand other considerations to demonstrate for anddiscuss with the patient.
REFERENCES
1. Rusciani A, Curinga G, Menichini G, et al. Nonsur-
gical tightening of skin laxity: a new radiofrequency
approach. J Drugs Dermatol 2007;6:377.
2. FitzpatrickRE. Laser resurfacing. AdvDermatol 1998;
13:463–501, 1998.
3. Zelickson BD, Kist D, Bernstein E, et al. Histologic
and ultra structural evaluation of the effects of a radio-
frequency-based non-ablative dermal remodeling
device: a pilot study. Arch Dermatol 2004;140:204–9.
4. Javate R, Cruz R, Khan J, et al. Nonablative 4-MHz
dual radiofrequency wand rejuvenation treatment
for periorbital rhytides and midface laxity. Ophthal
Plast Reconstr Surg 2011;27(3):180–5.
5. Fitzpatrick RE, Geronemus R, Goldberg D, et al.
Multicenter study of noninvasive radiofrequency for
periorbital tissue tightening. Lasers Surg Med
2003;33:232–42.
6. Fritz M, Counters JT, Zelickson BD. Radiofrequency
treatment for middle and lower face laxity. Arch
Facial Plast Surg 2004;6:370–3.
7. Arnoczky SP, Aksan A. Thermal modification of
connective tissues: basic science considerations
and clinical implications. J Am Acad Orthop Surg
2000;8(5):305–13.
8. Alster TS, Lupton JR. Nonablative cutaneous remod-
eling using radiofrequency devices. Clin Dermatol
2007;25:487–91.
9. Biesman BS, Baker SS, Carruthers J, et al. Mono-
polar radiofrequency treatment of human eyelids: a
prospective, multicenter, efficacy trial. Lasers Surg
Med 2006;38:890–8.
10. Kist D, Burns AJ, Sanner R, et al. Ultrastructural
evaluation of multiple pass low energy versus single
pass high energy radiofrequency treatment. Lasers
Surg Med 2006;38(2):150–4.
11. Finzi E, Spangler A. Multipass vector (mpave)
technique with nonablative radiofrequency to treat
facial and neck laxity. Dermatol Surg 2005;31:
916–22.
12. Brown SA, Farkas JP, Arnold C, et al. Heat shock
proteins 47 and 70 expression in rodent skin model
as a function of contact cooling temperature: are we
overcooling our target? Lasers Surg Med 2007;
39(6):504–12.
Wrinkle Reduction and Skin Tightening 345


















