The pathophysiology of heart failure with preserved ...
9
NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 507 The Division of Cardiovascular Diseases, Department of Medicine, Mayo Clinic College of Medicine, 200 First Street SW, Rochester, MN 55905, USA. [email protected] The pathophysiology of heart failure with preserved ejection fraction Barry A. Borlaug Abstract | Approximately half of all patients with heart failure have preserved ejection fraction (HFpEF) and, as life expectancies continue to increase in western societies, the prevalence of HFpEF will continue to grow. In contrast to heart failure with reduced ejection fraction (HFrEF), no treatment has been proven in pivotal clinical trials to be effective for HFpEF, largely because of the pathophysiological heterogeneity that exists within the broad spectrum of HFpEF. This syndrome was historically considered to be caused exclusively by left ventricular diastolic dysfunction, but research has identified several other contributory factors, including limitations in left ventricular systolic reserve, systemic and pulmonary vascular function, nitric oxide bioavailability, chronotropic reserve, right heart function, autonomic tone, left atrial function, and peripheral impairments. Multiple individual mechanisms frequently coexist within the same patient to cause symptomatic heart failure, but between patients with HFpEF the extent to which each component is operative can differ widely, confounding treatment approaches. This Review focuses on our current understanding of the pathophysiological mechanisms underlying HFpEF, and how they might be mechanistically related to typical risk factors for HFpEF, including ageing, obesity, and hypertension. Borlaug, B. A. Nat. Rev. Cardiol. 11, 507–515 (2014); published online 24 June 2014; doi:10.1038/nrcardio.2014.83 Introduction Cardiovascular disease is the leading cause of death worldwide. 1 In the USA, only two cardiovascular dis- orders are still increasing in prevalence—heart failure (HF) and atrial fibrillation. 2 The most-comprehensive epidemiological data on HF are derived from US pop- ulation studies; if current trends continue, 8.5 million Americans will have HF by 2030, 6 million of whom will be aged >65 years. 3 Although estimates vary, nearly half of patients with HF have preserved ejection fraction (≥45–50%; HFpEF), and the prevalence of HFpEF relative to HF with reduced ejection fraction (HFrEF) is growing by 10% per decade. 4–7 Over 90% of patients with HFpEF are aged ≥60 years at the time of diagnosis 8 meaning that, as increased longevity is achieved in western societies, the enormous public-health problem of HFpEF will continue to grow. In striking contrast to HFrEF, an effective treatment for HFpEF has not been identified in clinical trials. 5 HFpEF was historically referred to as ‘diastolic heart failure’. However, over the past decade our group and others have shown repeatedly that, rather than being solely caused by diastolic dysfunction, HFpEF is caused by the complex interplay of multiple impairments in ventricular diastolic and systolic reserve function, heart rate reserve and rhythm, atrial dysfunction, stiffening of the ventri- cles and vasculature, impaired vasodilatation, pulmonary hypertension, endothelial dysfunction, and abnormalities in the periphery, including skeletal muscle. 9–46 Many of these abnormalities are not apparent at rest, but are noted only when the cardiovascular system is stressed (that is, reserve limitation). 27 In many ways, this situation is an exaggerated version of phenomena seen with normal cardiovascular ageing. 47–57 Therefore, HFpEF could be considered to be the ultimate form of pre- mature cardiac ageing or ‘presbycardia’. These limitations in cardiovascular reserve then interact with systemic pro- cesses to cause symptoms of dyspnoea and fatigue, which ultimately culminate in systemic and pulmonary venous congestion, muscle wasting, and loss of functionality and independence, escalating the need for HF care. In this Review, I will summarize the current under- standing of the pathophysiology of HFpEF and how it relates to commonly observed HFpEF risk factors. Diagnosis and treatment of HFpEF are beyond the scope of the present article and will not be described in detail. Pathophysiological components of HFpEF LV structure and remodelling Early descriptive studies in HFpEF suggested that con- centric left ventricular (LV) hypertrophy with normal chamber size was typical. 58,59 However, population-based studies published since 2007 have shown that many patients with HFpEF have either concentric remodel- ling in the absence of hypertrophy, or even normal LV geometry. 19,23,60 At the structural level, cardiomyocytes in HFpEF are thicker and less elongated than in HFrEF, 61 and collagen content is increased compared with control Competing interests The author has acted as a consultant for Amgen, Cardiokinetix, DC Devices (unpaid), GlaxoSmithKline, and Merck. He has received research support from AtCor Medical. REVIEWS © 2014 Macmillan Publishers Limited. All rights reserved
Transcript of The pathophysiology of heart failure with preserved ...

NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 507
The Division of Cardiovascular Diseases, Department of Medicine, Mayo Clinic College of Medicine, 200 First Street SW, Rochester, MN 55905, USA. [email protected]
The pathophysiology of heart failure with preserved ejection fractionBarry A. Borlaug
Abstract | Approximately half of all patients with heart failure have preserved ejection fraction (HFpEF) and, as life expectancies continue to increase in western societies, the prevalence of HFpEF will continue to grow. In contrast to heart failure with reduced ejection fraction (HFrEF), no treatment has been proven in pivotal clinical trials to be effective for HFpEF, largely because of the pathophysiological heterogeneity that exists within the broad spectrum of HFpEF. This syndrome was historically considered to be caused exclusively by left ventricular diastolic dysfunction, but research has identified several other contributory factors, including limitations in left ventricular systolic reserve, systemic and pulmonary vascular function, nitric oxide bioavailability, chronotropic reserve, right heart function, autonomic tone, left atrial function, and peripheral impairments. Multiple individual mechanisms frequently coexist within the same patient to cause symptomatic heart failure, but between patients with HFpEF the extent to which each component is operative can differ widely, confounding treatment approaches. This Review focuses on our current understanding of the pathophysiological mechanisms underlying HFpEF, and how they might be mechanistically related to typical risk factors for HFpEF, including ageing, obesity, and hypertension.
Borlaug, B. A. Nat. Rev. Cardiol. 11, 507–515 (2014); published online 24 June 2014; doi:10.1038/nrcardio.2014.83
IntroductionCardiovascular disease is the leading cause of death worldwide.1 In the USA, only two cardiovascular dis-orders are still increasing in prevalence—heart failure (HF) and atrial fibrillation.2 The most-comprehensive epidemiological data on HF are derived from US pop-ulation studies; if current trends continue, 8.5 million Americans will have HF by 2030, 6 million of whom will be aged >65 years.3 Although estimates vary, nearly half of patients with HF have preserved ejection fraction (≥45–50%; HFpEF), and the prevalence of HFpEF relative to HF with reduced ejection fraction (HFrEF) is growing by 10% per decade.4–7 Over 90% of patients with HFpEF are aged ≥60 years at the time of diagnosis8 meaning that, as increased longevity is achieved in western societies, the enormous public-health problem of HFpEF will continue to grow.
In striking contrast to HFrEF, an effective treatment for HFpEF has not been identified in clinical trials.5 HFpEF was historically referred to as ‘diastolic heart failure’. However, over the past decade our group and others have shown repeatedly that, rather than being solely caused by diastolic dysfunction, HFpEF is caused by the complex interplay of multiple impairments in ventricular dia stolic and systolic reserve function, heart rate reserve and rhythm, atrial dysfunction, stiffening of the ventri-cles and vasculature, impaired vasodilatation, pulmonary
hypertension, endothelial dysfunction, and a bnormalities in the periphery, including skeletal muscle.9–46
Many of these abnormalities are not apparent at rest, but are noted only when the cardiovascular system is stressed (that is, reserve limitation).27 In many ways, this situation is an exaggerated version of phenomena seen with normal cardiovascular ageing.47–57 Therefore, HFpEF could be considered to be the ultimate form of pre-mature cardiac ageing or ‘presbycardia’. These limitations in cardio vascular reserve then interact with systemic pro-cesses to cause symptoms of dyspnoea and fatigue, which ultimately culminate in systemic and pulmonary venous congestion, muscle wasting, and loss of functionality and independence, escalating the need for HF care.
In this Review, I will summarize the current under-standing of the pathophysiology of HFpEF and how it relates to commonly observed HFpEF risk factors. Diagnosis and treatment of HFpEF are beyond the scope of the present article and will not be described in detail.
Pathophysiological components of HFpEFLV structure and remodellingEarly descriptive studies in HFpEF suggested that con-centric left ventricular (LV) hypertrophy with normal chamber size was typical.58,59 However, population-based studies published since 2007 have shown that many patients with HFpEF have either concentric remodel-ling in the absence of hypertrophy, or even normal LV geometry.19,23,60 At the structural level, cardiomyocytes in HFpEF are thicker and less elongated than in HFrEF,61 and collagen content is increased compared with control
Competing interestsThe author has acted as a consultant for Amgen, Cardiokinetix, DC Devices (unpaid), GlaxoSmithKline, and Merck. He has received research support from AtCor Medical.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

508 | SEPTEMBER 2014 | VOLUME 11 www.nature.com/nrcardio
populations.62 Notably, currently available biopsy data are from patients with HFpEF who were younger than those typically seen in the community, for whom detailed histomorphometric characterization is not yet available.
LV diastolic limitationsDiastolic dysfunction is defined as the inability to fill the ventricle to an adequate preload volume (end-diastolic volume; EDV) at acceptably low pressures.63 Diastolic function is often conceptualized as the totality of an active process of pressure decay (relaxation) during early
Key points
■ Heart failure with preserved ejection fraction (HFpEF) is an increasingly common form of cardiac disease associated with ageing, obesity, and hypertension, for which no treatment has proven effective
■ HFpEF is characterized by increased left ventricular (LV) filling pressure secondary to diastolic dysfunction; this pressure elevation can be observed at rest or during exercise and causes secondary pulmonary hypertension
■ Despite normal ejection fraction, HFpEF is characterized by mild systolic dysfunction and dramatic limitations in systolic reserve capacity during stress, with blunted increases in ejection fraction
■ Chronotropic incompetence, left atrial dysfunction, atrial fibrillation, arterial stiffening, autonomic imbalance, and endothelial dysfunction contribute to diastolic and systolic dysfunction to limit cardiac output reserve and increase LV filling pressures
■ Peripheral impairments, including abnormalities in endothelial function, body composition, and skeletal muscle function, also have an important role in HFpEF
■ These impairments in cardiac, vascular, and peripheral reserve can be caused by common risk factors for HFpEF, such as ageing, adiposity, hypertension, and metabolic stress
diastole related to myofilament dissociation and calcium reuptake, and ‘passive’ stiffness related to the visco elastic properties that are governed by mechanical changes from the sarcomere to extracellular matrix, chamber, and pericardium.5,64 Most, although not all, studies have demonstrated that the rate of LV pressure decay during isovolumic relaxation (time constant τ) is prolonged in HFpEF (Figure 1).13,14,22,25,33 In the healthy heart at rest, relaxation is complete by 3.5τ, which is much less time that the normal diastolic period. However, when heart rate increases, the left ventricle must enhance relaxation to allow for more-rapid pressure decay. In HFpEF, this enhancement is lost, contributing to LV and left atrial (LA) pressure elevation.25,33,65
Delayed relaxation is, however, only part of the problem in early diastole in HFpEF. The healthy left ventricle functions as a ‘vacuum cleaner’ that prevents LA hypertension by enhancing suction in response to increases in venous return, as with exercise.51,66–71 This role is achieved through the generation of intraventricu-lar pressure gradients that are determined by the speed of relaxation, the extent and velocity of mitral annular longitudinal motion, the LV ‘untwisting’ that occurs during early diastole, and the end-systolic volume (ESV) achieved in the preceding contraction cycle (reduced ESV below the equilibrium volume increases recoil to enhance filling, like a compressed spring).51,72,73 Studies have shown that each of these components is impaired in patients with HFpEF, particularly during the stress of exercise, such that the left ventricle can fill only at the expense of left atrial hypertension.17,24,33,70,71 In other words, although the healthy left ventricle effectively pulls in blood during early diastole,66–68 in patients with HFpEF, filling is reliant on high LA pressure to push blood into the chamber (Figure 1).28,29,33,68,69
Ventricular passive diastolic stiffness is also an impor-tant determinant of the increase in LV filling pressures in HFpEF.14,22 LV end-diastolic stiffness (Eed) is quanti-fied by the slope and position of the diastolic pressure–volume relationship (Figure 1).63 Eed increases with ageing, even when blood pressure is well controlled and in the absence of concentric LV remodelling.55 Most, but not all, studies have shown that, on average, Eed is increased in patients with HFpEF.13,14,19,22,25 Increased diastolic ventricular passive stiffness was originally thought to be determined predominantly by collagen quantity and the qualities of the extracellular matrix. However, studies conducted in the past decade have pointed to the importance of determinants within the cardiac myocytes, particularly the sarcomeric macro-molecule titin,5,61,62,74,75 in diastolic ventricular passive stiffness. Titin fu nctions as a bidirectional spring, the stiffness constant of which can be modified by isotype expression and by post-translational modification via phosphorylation by cyclic GMP-dependent kinase.76,77 Increases in cardiac myocyte stiffness in HFpEF are mediated in large part by relative hypophosphorylation of titin, which is related to cyclic GMP deficiency owing to increased nitroso-oxidative stress.74 This finding provides a novel therapeutic target to improve diastolic
a b
Time
LV p
ress
ure
LV volume
Normal (rest)Normal (exercise)HFpEF (rest)HFpEF (exercise)
Figure 1 | LV diastolic function in health and in HFpEF. a | LV pressure plotted against time. Normal LV pressure decay is shown in blue, with prolonged relaxation in HFpEF indicated in red. b | LV diastolic pressure–volume relationships. In the normal left ventricle at rest (solid blue line), the increase in pressure during diastole is minimal despite large increases in LV chamber volume, with normal LV end-diastolic pressure (blue circles). With exercise (dashed blue line), dynamic reduction in LV minimal diastolic pressure occurs (blue triangles) related to enhanced LV early-diastolic suction. In HFpEF, the resting diastolic pressure–volume relationship (solid red line) is generally shifted up and to the left, indicating increased chamber stiffness. With exercise (dashed red line), a further shift upward occurs, with both a steeper slope and a higher LV minimal pressure (red triangles) reflecting inadequate LV early diastolic suction, and contributing to dramatic increase in LV end-diastolic pressure (red circles). Abbreviations: HFpEF, heart failure with preserved ejection fraction; LV, left ventricular. Panel a adapted from Cardiol. Clinics, 29 (2), Borlaug, B. A. & Kass, D. A. Invasive hemodynamic assessment in heart failure, 269–280, © (2011), with permission from Elsevier.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 509
stiffness, and is speculated to mechanistically tie together the loss of nitric oxide (NO) bioavailability in HFpEF with common risk factors including obesity, ageing, and metabolic syndrome.75
Diastolic dysfunction is not universal in HFpEF, being observed by echocardiography in only two-thirds of patients at rest.43,60,78 However, many patients with HFpEF display elevated LV filling pressures only during the stress of exercise, indicating an earlier stage of disease.28,29 These patients commonly have a normal plasma level of B-type natriuretic peptide (BNP), leading clinicians to the false conclusion that they do not have HF.29,79 Obesity is associated with a lower than normal BNP level, and this observation, along with the intermittent nature of filling pressure elevation, is likely to explain the reduced BNP level observed in patients with HFpEF.29,79–81
Despite the high LV filling pressures in patients with HFpEF, at rest or with exercise, LV preload (EDV) is generally not compromised. LV volumes were slightly enlarged in HFpEF compared with controls in one study,82 but the majority of studies have shown normal chamber size19,40 and normal increases in EDV with exercise15,27,35,40 in patients with HFpEF. Therefore, diastolic dysfunction in HFpEF does not seem to compromise net chamber filling, but rather to require an abnormal elevation in pressure to achieve that degree of filling. Aggressive treat-ment to reduce LV filling pressures in HFpEF was associ-ated with reduced hospitalizations for HF in a prospective trial,83 supporting the importance of diastolic dysfunction in HFpEF. As well as leading to symptoms of dyspnoea, elevation in LA pressures produces secondary pulmonary hypertension and atrial remodelling that can predispose a patient to the development of right ventricular (RV) dy sfunction and atrial fibrillation, respectively.
LV systolic limitationsAlthough ejection fraction is the measure that is used most often clinically to assess systolic function, it is more-appropriately viewed as a reflection of ventricular–arterial coupling.23,63 Ejection fraction can be low owing to very high afterload despite normal contractility, or it can be normal even when contractile function is impaired when afterload is low. Multiple studies have shown that, despite relative preservation in LV ejection fraction, patients with HFpEF display subtle abnormalities in systolic function. This finding is evident with tissue Doppler and strain-based imaging techniques, particularly longitudinal tissue shortening, or when chamber and myocardial level con-tractile function is examined using load-independent parameters.11,12,17,23,37,44,84 Intriguingly, the severity of LV myocardial contractile dysfunction predicts risk of death in HFpEF.23 Studies have shown that some patients with HFpEF, primarily those with concomitant coronary artery disease, go on to develop HFrEF.85,86
The subtle deficits in resting systolic performance become dramatic during physiological stress.15,17,24,27,32,34,40,87 In other words, although ejection fraction is preserved at rest, enhancement in ejection fraction with stress is mark-edly limited in HFpEF,21,27 primarily owing to the inability to reduce chamber volume to a sufficiently low ESV rather than to a limitation in the increase in EDV (Figure 2).27,35,40 Diminished reductions in ESV impair early diastolic suction, promoting left atrial hypertension,67,87 while also blunting the normal increase in forward stroke volume that is required with exercise.27,28,40 Limited stroke volume reserve in HFpEF, coupled with the common presence of chronotropic incompetence significantly limits cardiac output in response to exercise in HFpEF, which is inade-quate to meet the increased metabolic demands associated with locomotion.40
Ventricular dyssynchronyAlthough electrical dyssynchrony (bundle branch block) is uncommon in patients with HFpEF, studies have shown that systolic and diastolic mechanical dyssynchrony is fairly prevalent.32,45,88 The magnitude of dyssynchrony is related to the extent of diastolic dysfunction45 and the magnitude of aerobic limitation.41 In contrast to HFrEF, however, whether mechanical dyssynchrony can be ef fectively resynchronized in HFpEF remains unclear.
Atrial dysfunction and atrial fibrillationThe left atrium functions as an important barrier between the left ventricle and the pulmonary circulation, by facili-tating LV filling through its conduit and booster functions and by shielding the pulmonary vasculature from wide LV pressure oscillations in concert with the mitral valve appa-ratus. In healthy hearts, ~80% of LV filling occurs during early diastole and the remaining 20% occurs with atrial contraction. Research indicates that patients with early-stage HFpEF might be more reliant on LA contraction to achieve LV filling than are healthy controls.89 In more-advanced stages of HFpEF, progressive atrial dilatation and loss of atrial contractile reserve occurs, p articularly with stress.18,30
a bHealthy adult Patient with HFpEF
Exercise Exercise
End diastole End systole End diastole End systole
Figure 2 | Depiction of short-axis views of the left ventricle at end diastole and end systole. a | In a healthy adult at rest (top) and with exercise (bottom). b | In a typical patient with HFpEF at rest (top) and with exercise (bottom). At rest, both healthy individuals and those with HFpEF have similar and normal left ventricular ejection fraction. However, with exercise stress, the increase in ejection fraction is blunted in the patient with HFpEF owing to the inability to contract to as low an end-systolic volume, despite similar increases in cavity size at end diastole. This systolic impairment limits stroke volume reserve, which in tandem with chronotropic incompetence blunts the cardiac output response to exercise. Abbreviation: HFpEF, heart failure with preserved ejection fraction.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

510 | SEPTEMBER 2014 | VOLUME 11 www.nature.com/nrcardio
The importance of LA function in HFpEF is under-scored by observations that atrial fibrillation is very poorly tolerated in patients with HFpEF.20 Compared with patients with HFpEF who are in sinus rhythm, those in atrial fibrillation have lower exercise capacity despite similar chronotropic reserve,90 more-severe right ven-tricular dysfunction,91 and an increased risk of death.92 Atrial dilatation precedes atrial fibrillation and is asso-ciated with chronic LV diastolic dysfunction as well as comorbidities commonly associated with HFpEF, such as obesity and disordered breathing during sleep.93
RV dysfunction and pulmonary vascular diseasePulmonary hypertension is common in patients with HFpEF,26,94 particularly during exercise, because down-stream elevations in LA pressure add to components of pulmonary vascular load related to arteriolar resist-ance and cardiac output.29 In patients with HFpEF, each 10 mmHg increment in pulmonary artery pressure is asso-ciated with a 28% increase in 3-year mortality.26 Increases in LA pressure preferentially increase pulsatile RV loading, even acutely during exercise,95 but the increase in pulmonary artery pressures in HFpEF is not simply the result of passive LA hypertension.94 Pulmonary vascular disease in HFpEF can be as severe as in HFrEF, with eleva-tion in pulmonary vascular resistance being observed in roughly 50% of patients referred to the catheter ization laboratory.94,96 Chronic obstructive pulmonary disease commonly coexists with HFpEF, can worsen pulmo-nary hypertension, and also makes determining whether symptoms of dyspnoea are primarily related to the heart or lungs difficult.97
Studies have shown that RV function is impaired in HFpEF, even when accounting for the degree of pulmo-nary hypertension, and that the right ventricle seems to demonstrate enhanced afterload sensitivity.91 Pulmonary artery systolic pressures drop more pre cipitously with acute vasodilator therapy in HFpEF than in HFrEF, suggesting increased RV end-systolic elastance96 and, like the left ventricle, the right ventricle in HFpEF also displays increased diastolic stiffness.91 RV dysfunc-tion in HFpEF is independently related to the presence of coronary disease, is worse in men and patients with atrial fibrillation, and is related to the degree of LV dys-function through systolic ventricular interaction.91 This term refers to LV contributions to RV function, which are mediated through helical fibres in the intraventricular septum that contribute to RV ejection in the setting of RV failure.94,98 Therefore, subtle deficits in septal LV systolic longitudinal deformation might contribute to RV dys-function in HFpEF, in addition to systolic and diastolic LV reserve limitations.
Research has shown that RV dysfunction and hyper-trophy in patients with HFpEF predicts adverse outcome, even after accounting for the degree of pulmonary hyper-tension present.91,99 The right ventricle functions as the ultimate mediator of the deleterious effects of pulmonary hypertension on the body.91 With RV failure, progres-sive systemic venous congestion leads to gut oedema, malabsorption, congestive hepatopathy, cardiorenal
syndrome, systemic inflammation and, ultimately, to the development of cardiac cachexia.100,101 In a multi-centre, randomized trial, the pulmonary vasodilator sildenafil did not improve exercise capacity or quality of life, or reduce levels of biomarkers in patients with HFpEF. However, estimated pulmonary artery systolic pressures were not much elevated (median 41 mmHg) above normal (<35 mmHg) in this population, and alter-native approaches to reducing pulmonary artery resist-ance might still be effective in patients with both HFpEF and pulmonary hypertension.102
Pericardial restraintRight-sided chamber and LA enlargement in HFpEF can lead to a marked increases in total cardiac volume, even though LV cavity volume is normal.18 This increase in heart size creates the substrate for increased pericardial restraint and diastolic ventricular interaction (DVI), in which changes in right heart pressure and volume influ-ence the left heart in parallel.94,98 When DVI is enhanced, left heart filling pressures can be elevated even when LV diastolic compliance is normal and LVEDV is normal or reduced. Many patients with HFrEF display enhanced DVI during exercise, whereby LV filling pressures and right atrial pressure increase in a 1:1 ratio, with no further enhancement in stroke volume, owing to the restraining effects of the pericardium that prevent additional preload recruitment.103 In patients with HFpEF, the slope of the increase in right atrial pressure to LV filling pressure with exercise has been reported to be 0.4,29 in keeping with the previously described 40% contribution of pericardial restraint to LV end-diastolic pressures in patients with healthy hearts and in those with HFrEF.104 Further study is required to determine whether pericardial restraint or enhanced DVI contributes to the pathophysiology of HFpEF, which would then beg the question as to whether surgical approaches to remove pericardial restraint might improve symptoms related to venous congestion.105
Vascular stiffening and dysfunctionIn addition to impaired contractile reserve, inadequate vasodilation seems to contribute to the inability to reduce ESV and increase stroke volume in patients with HFpEF. Attenuated reductions in mean systemic vascu-lar resistance and effective arterial elastance, increases in pulse wave velocity and arterial elastic moduli, and impairments in aortic distensibility with exercise, which are all associated with the severity of exercise disability, have been observed in patients with HFpEF.10,15,21,27,38 The inability to vasodilate, together with previously described limitations in systolic reserve, leads to dynamic limitations in ventricular–arterial coupling with exer-cise in patients with HFpEF.24,27 In addition, increased arterial stiffness combined with increases in LV end-systolic stiffness or elastance, lead to dramatic fluctua-tions in blood pressure for any given change in preload, afterload, or stroke volume.13,96 These changes explain the common presence of marked blood pressure lability in patients with HFpEF, and can be very challenging to manage with pharmacotherapies.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 511
Patients with HFpEF display endothelial dysfunction compared with age-matched controls.27 Intriguingly, the severity of dyspnoea and fatigue with submaximal exercise is correlated with the degree of flow-mediated vasodilatation impairment (a measure of NO bio-availability).27 The presence of endothelial dysfunction has subsequently been related to adverse outcomes in a large series of patients with HFpEF (n = 321),106 and this loss of NO availability has been suggested to have a central role in the global pathophysiology of the disease.75 However, endothelial dysfunction has not been observed in all studies of patients with HFpEF.107
Just as systolic dysfunction contributes to impairment in LV diastolic suction, cross-talk occurs between vas-cular stiffening and diastolic reserve. Acute increases in arterial pressure prolong relaxation, particularly in failing hearts.108 Loading sequence seems also to be important, with increases in late-systolic afterload having more deleterious effects on LV relaxation than increases in early-systolic load.109,110
Chronotropic reserve and autonomic toneMost, although not all, studies of patients with HFpEF have shown that the increase in heart rate in response to exer-cise is blunted.15,16,27,28,35,40,111 By contrast, an improvement in exercise capacity with ivabradine, which selectively reduces heart rate, was reported in a small, 1-week study of patients with HFpEF, although the participants did not have chronotropic incompetence.112 Evidence exists for abnormalities in autonomic balance in HFpEF. In an early study, cardioacceleration during the early phase of exer-cise, which is driven predominantly by with drawal of para-sympathetic tone, was blunted in patients with HFpEF,15 although heart rate deficits have been reported only at peak exercise in most subsequent studies.27 Heart rate recov-ery, defined as the reduction in heart rate after cessation of exercise, is also frequently abnormal in patients with HFpEF.15,111 This marker is related to autonomic tone— patients with excessive sympathoexcitation and impaired parasympathetic tone have a slower reduction in heart rate after exercise compared with healthy controls. This abnor-mality in heart rate recovery is i ndependently associated with adverse outcome.113
Patients with HFpEF have been observed to display attenuated arterial baroreflex sensitivity compared with age-matched control individuals with hypertension,15 who themselves are known to exhibit abnormal cardiac sym-pathoexcitation.114 In a rat model, abrogation of normal arterial baroreflex function lead to dramatic intolerance to volume loading, with greater increases in left atrial and sys-temic arterial pressure with saline loading than in animals with intact baroreflex function.115 Whether such impair-ments occur in human HFpEF is unknown, but they might be contributory factors given that many patients do not seem to be markedly hypervolaemic at the time of pres-entation. Exercise-induced increases in plasma norepine-phrine and epinephrine do not differ between patients with HFpEF and age-matched and sex-matched control individuals with hypertension.15 However, this finding does not necessarily reflect cardiac-specific sympathetic
nerve activity, which has not yet been studied in HFpEF, but is known to be severely deranged in HFrEF.116
Peripheral factorsAerobic capacity, measured as the peak oxygen con-sumption (peak VO2) achieved during exercise, is char-acteristically depressed in HFpEF.117 According to the Fick equation, VO2 is equal to the product of cardiac output and arterial–venous oxygen content difference (AVO2diff). When objective evidence exists of maximal volitional effort, a low peak VO2 in patients with HF is generally thought to indicate low cardiac output reserve, on the basis of the assumption that AVO2diff becomes maximized to a similar extent in all patients.35,36 However, studies have suggested that this situation might not be the case in patients with HFpEF.35,36 Although peak VO2 has been observed to correlate with both changes in cardiac output and AVO2diff with exercise in patients with HFpEF, the change in AVO2diff was the strong-est independent predictor of peak VO2.
35 Indeed, the beneficial effects of exercise training seem to be medi-ated predominantly through effects in the periphery in HFpEF118 as well as in other chronic cardiorespiratory diseases.119 In another study, although both exercise cardiac output and peak VO2 were depressed in patients with HFpEF, the increase in output relative to VO2 was enhanced—a finding previously reported in patients with mitochondrial myopathies.36
By contrast, in an invasive study in which arterial and mixed venous oxygen contents were directly measured, no difference was seen in AVO2diff at peak exercise between patients with HFpEF and control individu-als.40 In fact, when scaled to VO2, AVO2diff was some-what enhanced in HFpEF, which is likely to be a chronic adaptation to inadequate perfusion from cardiac output reserve dysfunction. How to reconcile these conflicting results is not clear at this time; however, they are likely to further underscore the substantial pathophysio-logical heterogeneity within the spectrum of HFpEF, and point to the important need for improved methods to i ndividualize therapies to specific phenotypes.40,120
Other peripheral limitations have been described in HFpEF. Studies examining body composition in patients with HFpEF have shown proportionate reductions in lean total body and leg mass in HFpEF compared with age-matched control individuals.39 Lower extremity skel-etal muscle has been found to display increased intra-muscular fat content in patients with HFpEF compared with age-matched control individuals, the extent of which was inversely correlated with exercise capacity.121 In this population, muscle biopsies showed reductions in type 1 fibres (slow-twitch, high oxidative potential) and reduced capillary density in patients with HFpEF c ompared with controls.122
Anaemia is common in patients with HFpEF and impairs oxygen-carrying capacity. The severity of anaemia predicts mortality, but the role of treatment is uncertain.42 As described above, peripheral endothelial dysfunction has been reported in HFpEF,27 and might impair dynamic flow-mediated dilatation responses during exercise while
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

512 | SEPTEMBER 2014 | VOLUME 11 www.nature.com/nrcardio
also impairing matching of perfusion to regional demand in skeletal muscle microcirculation.35,123
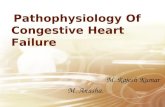
Combined cardiovascular reserve limitationClearly, HFpEF is not simply caused by one pathophysio-logical factor, but in fact is a complex, highly-integrated, multisystem loss of cardiac and vascular reserve capacity —affecting the left and right ventricles, diastolic and sys-tolic function, atrial reserve, heart rate and rhythm, auto-nomic control, the vasculature and microcirculation, and the periphery (Figure 3). Patients with HFpEF typically display a conglomeration of several reserve impairments that combine to cause symptomatic HF, but the dominant contributors can differ from patient to patient.27,120
The most-important next steps, if we are to improve outcomes, will be to devise ways to subcategorize patients with HFpEF into discrete phenotypes to reduce hetero-geneity124 and to identify overarching systemic processes
that might underlie limitations in global cardio vascular reserve. Risk factors for HFpEF include obesity, hyperten-sion, metabolic syndrome, and sedentary lifestyle, which seem to interact with cardio vascular ageing to promote transition to symptomatic HFpEF (Figure 4). Improved understanding of how these risk factors affect the heart and vasculature might better inform our understanding of combined reserve l imitation in HFpEF.5,75
Cardiac ageingCardiac ageing is known to affect many, if not all, of the pathophysiological components present in HFpEF. LV diastolic stiffness increases with normal ageing, even when blood pressure is well-controlled and LV mass does not increase.50,54–56 In addition to passive chamber stiffness, diastolic relaxation also becomes compromised with ageing, impairing the effects of diastolic suction.51–53 Age has no effect on resting heart rate, contractility, or cardiac output but, even in healthy adults, ageing blunts the capacity to enhance heart rate, systolic function, and cardiac output in response to exercise.47,48 Ageing is also associated with impaired endothelium-dependent vasodilatation.49,57 In HFpEF, these combined limit-ations are exaggerated above and beyond what is seen in normal ageing.27
Exciting new research is shedding light on the mecha-nisms of cardiac ageing, with the hope that some of these processes might be at least partially reversible. Mito-chondria seem to have a major role in cardiac ageing through DNA damage acquired with senescence and sec-ondary impairments in biogenesis that promote oxidative stress, fibrosis, and energy availability.125 Ageing is associ-ated with reductions in cardiac myocyte renewal that can impair overall reserve capacity,126 and increases in sys-temic inflammation that impair NO bioavailabi lity75 and promote fibrotic remodelling of the ex tracellular matrix owing to reduced collagen degradation.75,127
Nutrient-sensing molecules, known as sirtuins, have emerged as important regulators of cardiac function and longevity, which might contribute to premature cardiac ageing in humans.128 Small, noncoding RNAs (micro-RNAs [miRNA]), such as miRNA-34, might have an important role in cardiac ageing via effects on apoptosis, DNA damage, and telomere shortening.129 Autophagy, the process by which byproducts of cellular damage are cleared, might also be involved, although our under-standing of these processes in the human heart is in its infancy.130 Using a novel method, known as hetero-chronic para biosis, administration of growth/differ-entiation factor 11 has been shown to partially reverse age-associated changes in cardiac structure and function in mice.131 Although these basic studies are years from translation to humans, they have engendered new hope that we might be able to mitigate or reverse some of the components that constitute the ‘presbycardia’ known as HFpEF.
Obesity and related comorbiditiesAge seems to be the dominant risk factor for HFpEF. However, obesity and obesity-related comorbidities,
Peripheral limitations
LV diastolicreserve
LV systolicreserve
HRreserve
Cardiac output reserve
Pulmonaryhypertension
Atrial�brillation
RV dysfunction
Activityavoidance
Arterial stiffeningEndothelial dysfunction
LV �llingpressures
Oedema, ascites,and cachexia
Exertional dyspnoeaand fatigue
Figure 3 | The pathophysiology of heart failure with preserved ejection fraction. Arrows show causal inter-relationships between components. Abbreviations: HR, heart rate; LV, left ventricular; RV, right ventricular.
Hypertensiveremodelling
Sedentary lifestylePoor �tness
Obesity andmetabolic stress
Ventricular andvascular stiffening
Global loss of cardiac, vascular,and peripheral reserve
HFpEF
Ageing
Figure 4 | The interaction between risk factors, cardiac ageing, and loss of cardiovascular reserve, which results in the development of symptomatic HFpEF. Abbreviation: HFpEF, heart failure with preserved ejection fraction.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 513
such as metabolic syndrome, sedentary lifestyle, and hypertension, are also commonly observed and interact with ageing to confer increased risk of HFpEF (Figure 4). Indeed, the role of obesity in HFpEF could have thera-peutic implications. Studies suggest that weight gain, increased adiposity, and central obesity might acceler-ate age-associated ventricular stiffening, especially in women.55,56 Weight loss secondary to bariatric surgery improves diastolic function.132 Moreover, chronically active athletes do not display the typical age-associated loss of LV compliance that is observed in sedentary indi-viduals,50 suggesting that fitness might modulate the deleterious effects of adiposity on the heart, although teasing these two components apart is difficult.133 Both obesity and hypertension are associated with impair-ments in myocardial stress reserve with adrenergic stimulation,134,135 which is also observed in HFpEF136 in association with impairments in energetic availability.24 Obesity and its metabolic sequelae can increase nitroso-oxidative stress and, therefore, limit NO bioavailability in both the heart and the vasculature, potentially account-ing for many of the abnormalities observed in HFpEF, as has been suggested.75 Myocardial ischaemia might also affect systolic and diastolic reserve and, intriguingly, symptoms of angina are similarly prevalent and severe in patients with HFpEF with or without coronary artery disease. This finding suggests that ischaemia caused by small-vessel disease or coronary endothelial dysfunction
might contribute to diastolic and systolic ventricular reserve limitations.86,137
ConclusionsThe prevalence of HFpEF is growing to epidemic pro-portions owing to the changing age demographics and increase in obesity in western societies. No effective treatment for HFpEF has yet been identified. This lack of therapeutic options is largely related to the complexities in the pathophysiology of HFpEF, where limitations in ventricular diastolic, systolic, and chronotropic reserve interact with abnormalities in the periphery including the vasculature, endothelium, autonomic nervous system, and skeletal muscle. Only through rigorous phenotyping of patient-specific limitations and further research into the mechanisms underlying combined cardiac and vascular reserve dysfunction will we see improvements in outcome for this common and growing form of cardiac disease.
Review criteria
A search of the PubMed database was performed using the following terms: “heart failure with preserved ejection fraction”, “diastolic heart failure”, “heart failure”, and “hemodynamics”. Only full-text, peer-reviewed articles published in English were included, predominantly from 2000 to 2014. Bibliographies of the studies identified in the search were also reviewed for additional papers relevant to this topic.
1. WHO. Cardiovascular diseases. Fact sheet number 317 [online], http://www.who.int/mediacentre/factsheets/fs317/en/ (2013).
2. Braunwald, E. Shattuck lecture—cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N. Engl. J. Med. 337, 1360–1369 (1997).
3. Heidenreich, P. A. et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ. Heart Fail. 6, 606–619 (2013).
4. Owan, T. E. et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med. 355, 251–259 (2006).
5. Borlaug, B. A. & Paulus, W. J. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur. Heart J. 32, 670–679 (2011).
6. Lee, D. S. et al. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation 119, 3070–3077 (2009).
7. Bhatia, R. S. et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N. Engl. J. Med. 355, 260–269 (2006).
8. Bursi, F. et al. Systolic and diastolic heart failure in the community. JAMA 296, 2209–2216 (2006).
9. Kitzman, D. W., Higginbotham, M. B., Cobb, F. R., Sheikh, K. H. & Sullivan, M. J. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank–Starling mechanism. J. Am. Coll. Cardiol. 17, 1065–1072 (1991).
10. Hundley, W. G. et al. Cardiac cycle-dependent changes in aortic area and distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise
intolerance. J. Am. Coll. Cardiol. 38, 796–802 (2001).
11. Yip, G. et al. Left ventricular long axis function in diastolic heart failure is reduced in both diastole and systole: time for a redefinition? Heart 87, 121–125 (2002).
12. Yu, C. M. et al. Progression of systolic abnormalities in patients with “isolated” diastolic heart failure and diastolic dysfunction. Circulation 105, 1195–1201 (2002).
13. Kawaguchi, M., Hay, I., Fetics, B. & Kass, D. A. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation 107, 714–720 (2003).
14. Zile, M. R., Baicu, C. F. & Gaasch, W. H. Diastolic heart failure—abnormalities in active relaxation and passive stiffness of the left ventricle. N. Engl. J. Med. 350, 1953–1959 (2004).
15. Borlaug, B. A. et al. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 114, 2138–2147 (2006).
16. Brubaker, P. H. et al. Chronotropic incompetence and its contribution to exercise intolerance in older heart failure patients. J. Cardiopulm. Rehabil. 26, 86–89 (2006).
17. Tan, Y. T. et al. The pathophysiology of heart failure with normal ejection fraction: exercise echocardiography reveals complex abnormalities of both systolic and diastolic ventricular function involving torsion, untwist, and longitudinal motion. J. Am. Coll. Cardiol. 54, 36–46 (2009).
18. Melenovsky, V. et al. Cardiovascular features of heart failure with preserved ejection fraction versus nonfailing hypertensive left ventricular hypertrophy in the urban Baltimore community:
the role of atrial remodeling/dysfunction. J. Am. Coll. Cardiol. 49, 198–207 (2007).
19. Lam, C. S. et al. Cardiac structure and ventricular–vascular function in persons with heart failure and preserved ejection fraction from Olmsted County, Minnesota. Circulation 115, 1982–1990 (2007).
20. Fung, J. W., Sanderson, J. E., Yip, G. W., Zhang, Q. & Yu, C. M. Impact of atrial fibrillation in heart failure with normal ejection fraction: a clinical and echocardiographic study. J. Card. Fail. 13, 649–655 (2007).
21. Ennezat, P. V. et al. Left ventricular abnormal response during dynamic exercise in patients with heart failure and preserved left ventricular ejection fraction at rest. J. Card. Fail. 14, 475–480 (2008).
22. Westermann, D. et al. Role of left ventricular stiffness in heart failure with normal ejection fraction. Circulation 117, 2051–2060 (2008).
23. Borlaug, B. A., Lam, C. S., Roger, V. L., Rodeheffer, R. J. & Redfield, M. M. Contractility and ventricular systolic stiffening in hypertensive heart disease insights into the pathogenesis of heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 54, 410–418 (2009).
24. Phan, T. T. et al. Heart failure with preserved ejection fraction is characterized by dynamic impairment of active relaxation and contraction of the left ventricle on exercise and associated with myocardial energy deficiency. J. Am. Coll. Cardiol. 54, 402–409 (2009).
25. Wachter, R. et al. Blunted frequency-dependent upregulation of cardiac output is related to impaired relaxation in diastolic heart failure. Eur. Heart J. 30, 3027–3036 (2009).
26. Lam, C. S. et al. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J. Am. Coll. Cardiol. 53, 1119–1126 (2009).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

514 | SEPTEMBER 2014 | VOLUME 11 www.nature.com/nrcardio
27. Borlaug, B. A. et al. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 56, 845–854 (2010).
28. Maeder, M. T., Thompson, B. R., Brunner-La Rocca, H. P. & Kaye, D. M. Hemodynamic basis of exercise limitation in patients with heart failure and normal ejection fraction. J. Am. Coll. Cardiol. 56, 855–863 (2010).
29. Borlaug, B. A., Nishimura, R. A., Sorajja, P., Lam, C. S. & Redfield, M. M. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ. Heart Fail. 3, 588–595 (2010).
30. Tan, Y. T. et al. Reduced left atrial function on exercise in patients with heart failure and normal ejection fraction. Heart 96, 1017–1023 (2010).
31. Prasad, A. et al. Characterization of static and dynamic left ventricular diastolic function in patients with heart failure with a preserved ejection fraction. Circ. Heart Fail. 3, 617–626 (2010).
32. Lee, A. P. et al. Importance of dynamic dyssynchrony in the occurrence of hypertensive heart failure with normal ejection fraction. Eur. Heart J. 31, 2642–2649 (2010).
33. Borlaug, B. A. et al. Diastolic relaxation and compliance reserve during dynamic exercise in heart failure with preserved ejection fraction. Heart 97, 964–969 (2011).
34. Shibata, S. et al. Congestive heart failure with preserved ejection fraction is associated with severely impaired dynamic Starling mechanism. J. Appl. Physiol. 110, 964–971 (2011).
35. Haykowsky, M. J. et al. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. J. Am. Coll. Cardiol. 58, 265–274 (2011).
36. Bhella, P. S. et al. Abnormal haemodynamic response to exercise in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 13, 1296–1304 (2011).
37. Yip, G. W. et al. Resting global and regional left ventricular contractility in patients with heart failure and normal ejection fraction: insights from speckle-tracking echocardiography. Heart 97, 287–294 (2011).
38. Tartière-Kesri, L., Tartière, J. M., Logeart, D., Beauvais, F. & Cohen Solal, A. Increased proximal arterial stiffness and cardiac response with moderate exercise in patients with heart failure and preserved ejection fraction. J. Am. Coll. Cardiol. 59, 455–461 (2012).
39. Haykowsky, M. J. et al. Impaired aerobic capacity and physical functional performance in older heart failure patients with preserved ejection fraction: role of lean body mass. J. Gerontol. A Biol. Sci. Med. Sci. 68, 968–975 (2013).
40. Abudiab, M. M. et al. Cardiac output response to exercise in relation to metabolic demand in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 15, 776–785 (2013).
41. Tan, Y. T., Wenzelburger, F. W., Sanderson, J. E. & Leyva, F. Exercise-induced torsional dyssynchrony relates to impaired functional capacity in patients with heart failure and normal ejection fraction. Heart 99, 259–266 (2013).
42. Maurer, M. S., Teruya, S., Chakraborty, B., Helmke, S. & Mancini, D. Treating anemia in older adults with heart failure with a preserved ejection fraction with epoetin alfa: single-blind randomized clinical trial of safety and efficacy. Circ. Heart Fail. 6, 254–263 (2013).
43. Shah, A. M. et al. Cardiac structure and function in heart failure with preserved ejection fraction: baseline findings from the echocardiographic study of the treatment of preserved cardiac function heart failure with an aldosterone antagonist trial. Circ. Heart Fail. 7, 104–115 (2014).
44. Kraigher-Krainer, E. et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 63, 447–456 (2014).
45. Santos, A. B. et al. Left ventricular dyssynchrony in patients with heart failure and preserved ejection fraction. Eur. Heart J. 35, 42–47 (2014).
46. Borlaug, B. A. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction. Circ. J. 78, 20–32 (2013).
47. Stratton, J. R., Levy, W. C., Cerqueira, M. D., Schwartz, R. S. & Abrass, I. B. Cardiovascular responses to exercise. Effects of aging and exercise training in healthy men. Circulation 89, 1648–1655 (1994).
48. Fleg, J. L. et al. Impact of age on the cardiovascular response to dynamic upright exercise in healthy men and women. J. Appl. Physiol. 78, 890–900 (1995).
49. DeSouza, C. A. et al. Regular aerobic exercise prevents and restores age-related declines in endothelium-dependent vasodilation in healthy men. Circulation 102, 1351–1357 (2000).
50. Arbab-Zadeh, A. et al. Effect of aging and physical activity on left ventricular compliance. Circulation 110, 1799–1805 (2004).
51. Popovic, Z. B. et al. Relationship among diastolic intraventricular pressure gradients, relaxation, and preload: impact of age and fitness. Am. J. Physiol. Heart Circ. Physiol. 290, H1454–H1459 (2006).
52. Prasad, A. et al. The effects of aging and physical activity on Doppler measures of diastolic function. Am. J. Cardiol. 99, 1629–1636 (2007).
53. Carrick-Ranson, G. et al. Effect of healthy aging on left ventricular relaxation and diastolic suction. Am. J. Physiol. Heart Circ. Physiol. 303, H315–H322 (2012).
54. Fujimoto, N. et al. Effect of ageing on left ventricular compliance and distensibility in healthy sedentary humans. J. Physiol. 590, 1871–1880 (2012).
55. Borlaug, B. A. et al. Longitudinal changes in left ventricular stiffness: a community-based study. Circ. Heart Fail. 6, 944–952 (2013).
56. Wohlfahrt, P. et al. Impact of general and central adiposity of ventricular-arterial aging in women and men. JACC Heart Fail. (in press).
57. Gerhard, M., Roddy, M. A., Creager, S. J. & Creager, M. A. Aging progressively impairs endothelium-dependent vasodilation in forearm resistance vessels of humans. Hypertension 27, 849–853 (1996).
58. Topol, E. J., Traill, T. A. & Fortuin, N. J. Hypertensive hypertrophic cardiomyopathy of the elderly. N. Engl. J. Med. 312, 277–283 (1985).
59. Zile, M. R. et al. Heart failure with a normal ejection fraction: is measurement of diastolic function necessary to make the diagnosis of diastolic heart failure? Circulation 104, 779–782 (2001).
60. Zile, M. R. et al. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation 124, 2491–2501 (2011).
61. van Heerebeek, L. et al. Myocardial structure and function differ in systolic and diastolic heart failure. Circulation 113, 1966–1973 (2006).
62. Borbély, A. et al. Cardiomyocyte stiffness in diastolic heart failure. Circulation 111, 774–781 (2005).
63. Borlaug, B. A. & Kass, D. A. Invasive hemodynamic assessment in heart failure. Cardiol. Clin. 29, 269–280 (2011).
64. Borlaug, B. A. & Kass, D. A. Mechanisms of diastolic dysfunction in heart failure. Trends Cardiovasc. Med. 16, 273–279 (2006).
65. Hay, I., Rich, J., Ferber, P., Burkhoff, D. & Maurer, M. S. Role of impaired myocardial relaxation in the production of elevated left
ventricular filling pressure. Am. J. Physiol. Heart Circ. Physiol. 288, H1203–H1208 (2005).
66. Nonogi, H., Hess, O. M., Ritter, M. & Krayenbuehl, H. P. Diastolic properties of the normal left ventricle during supine exercise. Br. Heart J. 60, 30–38 (1988).
67. Udelson, J. E., Bacharach, S. L., Cannon, R. O. 3rd & Bonow, R. O. Minimum left ventricular pressure during beta-adrenergic stimulation in human subjects. Evidence for elastic recoil and diastolic “suction” in the normal heart. Circulation 82, 1174–1182 (1990).
68. Cheng, C. P., Igarashi, Y. & Little, W. C. Mechanism of augmented rate of left ventricular filling during exercise. Circ. Res. 70, 9–19 (1992).
69. Cheng, C. P., Noda, T., Nozawa, T. & Little, W. C. Effect of heart failure on the mechanism of exercise-induced augmentation of mitral valve flow. Circ. Res. 72, 795–806 (1993).
70. Tan, Y. T. et al. Abnormal left ventricular function occurs on exercise in well-treated hypertensive subjects with normal resting echocardiography. Heart 96, 948–955 (2010).
71. Ohara, T. et al. Loss of adrenergic augmentation of diastolic intra-LV pressure difference in patients with diastolic dysfunction: evaluation by color M-mode echocardiography. JACC Cardiovasc. Imaging 5, 861–870 (2012).
72. Opdahl, A. et al. Determinants of left ventricular early-diastolic lengthening velocity: independent contributions from left ventricular relaxation, restoring forces, and lengthening load. Circulation 119, 2578–2586 (2009).
73. Opdahl, A., Remme, E. W., Helle-Valle, T., Edvardsen, T. & Smiseth, O. A. Myocardial relaxation, restoring forces, and early-diastolic load are independent determinants of left ventricular untwisting rate. Circulation 126, 1441–1451 (2012).
74. van Heerebeek, L. et al. Low myocardial protein kinase G activity in heart failure with preserved ejection fraction. Circulation 126, 830–839 (2012).
75. Paulus, W. J. & Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 62, 263–271 (2013).
76. LeWinter, M. M. & Granzier, H. Cardiac titin: a multifunctional giant. Circulation 121, 2137–2145 (2010).
77. Hidalgo, C. & Granzier, H. Tuning the molecular giant titin through phosphorylation: role in health and disease. Trends Cardiovasc. Med. 23, 165–171 (2013).
78. Persson, H. et al. Diastolic dysfunction in heart failure with preserved systolic function: need for objective evidence: results from the CHARM Echocardiographic Substudy-CHARMES. J. Am. Coll. Cardiol. 49, 687–694 (2007).
79. Anjan, V. Y. et al. Prevalence, clinical phenotype, and outcomes associated with normal B-type natriuretic peptide levels in heart failure with preserved ejection fraction. Am. J. Cardiol. 110, 870–876 (2012).
80. Wang, T. J. et al. Impact of obesity on plasma natriuretic peptide levels. Circulation 109, 594–600 (2004).
81. Bertoni, A. G. et al. Impact of the look AHEAD intervention on NT-pro brain natriuretic peptide in overweight and obese adults with diabetes. Obesity (Silver Spring) 20, 1511–1518 (2012).
82. Maurer, M. S. et al. Ventricular structure and function in hypertensive participants with heart failure and a normal ejection fraction: the Cardiovascular Health Study. J. Am. Coll. Cardiol. 49, 972–981 (2007).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CARDIOLOGY VOLUME 11 | SEPTEMBER 2014 | 515
83. Abraham, W. T. et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 377, 658–666 (2011).
84. Petrie, M. C., Caruana, L., Berry, C. & McMurray, J. J. “Diastolic heart failure” or heart failure caused by subtle left ventricular systolic dysfunction? Heart 87, 29–31 (2002).
85. Dunlay, S. M., Roger, V. L., Weston, S. A., Jiang, R. & Redfield, M. M. Longitudinal changes in ejection fraction in heart failure patients with preserved and reduced ejection fraction. Circ. Heart Fail. 5, 720–726 (2012).
86. Hwang, S. J., Melenovsky, V. & Borlaug, B. A. Implications of coronary artery disease in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. http://dx.doi.org/10.1016/ j.jacc.2014.03.034.
87. Tan, Y. T. et al. Abnormal left ventricular function occurs on exercise in well-treated hypertensive subjects with normal resting echocardiography. Heart 96, 948–955 (2010).
88. Yu, C. M. et al. Diastolic and systolic asynchrony in patients with diastolic heart failure: a common but ignored condition. J. Am. Coll. Cardiol. 49, 97–105 (2007).
89. Phan, T. T. et al. Increased atrial contribution to left ventricular filling compensates for impaired early filling during exercise in heart failure with preserved ejection fraction. J. Card. Fail. 15, 890–897 (2009).
90. Zakeri, R. et al. Impact of atrial fibrillation on exercise capacity in heart failure with preserved ejection fraction: a RELAX trial ancillary study. Circ. Heart Fail. 7, 123–130 (2014).
91. Melenovsky, V., Hwang, S.-J., Lin, G., Redfield, M. M. & Borlaug, B. A. Right heart dysfunction in heart failure with preserved ejection fraction. Eur. Heart J. http://dx.doi.org/ 10.1093/eurheartj/ehu193.
92. Zakeri, R., Chamberlain, A. M., Roger, V. L. & Redfield, M. M. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: a community-based study. Circulation 128, 1085–1093 (2013).
93. Tsang, T. S., Barnes, M. E., Gersh, B. J., Bailey, K. R. & Seward, J. B. Left atrial volume as a morphophysiologic expression of left ventricular diastolic dysfunction and relation to cardiovascular risk burden. Am. J. Cardiol. 90, 1284–1289 (2002).
94. Guazzi, M. & Borlaug, B. A. Pulmonary hypertension due to left heart disease. Circulation 126, 975–990 (2012).
95. Tedford, R. J. et al. Pulmonary capillary wedge pressure augments right ventricular pulsatile loading. Circulation 125, 289–297 (2012).
96. Schwartzenberg, S. et al. Effects of vasodilation in heart failure with preserved or reduced ejection fraction implications of distinct pathophysiologies on response to therapy. J. Am. Coll. Cardiol. 59, 442–451 (2012).
97. Hawkins, N. M. et al. Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology. Eur. J. Heart Fail. 11, 130–139 (2009).
98. Schwarz, K., Singh, S., Dawson, D. & Frenneaux, M. P. Right ventricular function in left ventricular disease: pathophysiology and implications. Heart Lung Circ. 22, 507–511 (2013).
99. Burke, M. A. et al. Prognostic importance of pathophysiologic markers in patients with heart failure and preserved ejection fraction. Circ. Heart Fail. 7, 288–299 (2014).
100. Liu, M. et al. Albumin levels predict survival in patients with heart failure and preserved ejection fraction. Eur. J. Heart Fail. 14, 39–44 (2012).
101. Melenovsky, V. et al. Relationships between right ventricular function, body composition, and prognosis in advanced heart failure. J. Am. Coll. Cardiol. 62, 1660–1670 (2013).
102. Redfield, M. M. et al. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA 309, 1268–1277 (2013).
103. Janicki, J. S. Influence of the pericardium and ventricular interdependence on left ventricular diastolic and systolic function in patients with heart failure. Circulation 81 (2 Suppl.), III15–III20 (1990).
104. Dauterman, K. et al. Contribution of external forces to left ventricular diastolic pressure. Implications for the clinical use of the Starling law. Ann. Intern. Med. 122, 737–742 (1995).
105. Stray-Gundersen, J. et al. The effect of pericardiectomy on maximal oxygen consumption and maximal cardiac output in untrained dogs. Circ. Res. 58, 523–530 (1986).
106. Akiyama, E. et al. Incremental prognostic significance of peripheral endothelial dysfunction in patients with heart failure with normal left ventricular ejection fraction. J. Am. Coll. Cardiol. 60, 1778–1786 (2012).
107. Haykowsky, M. J. et al. Relationship of flow-mediated arterial dilation and exercise capacity in older patients with heart failure and preserved ejection fraction. J. Gerontol. A Biol. Sci. Med. Sci. 68, 161–167 (2013).
108. Leite-Moreira, A. F. et al. Diastolic tolerance to systolic pressures closely reflects systolic performance in patients with coronary heart disease. Basic Res. Cardiol. 107, 251 (2012).
109. Chirinos, J. A. et al. Early and late systolic wall stress differentially relate to myocardial contraction and relaxation in middle-aged adults: the Asklepios study. Hypertension 61, 296–303 (2013).
110. Borlaug, B. A. et al. Impact of arterial load and loading sequence on left ventricular tissue velocities in humans. J. Am. Coll. Cardiol. 50, 1570–1577 (2007).
111. Phan, T. T. et al. Impaired heart rate recovery and chronotropic incompetence in patients with heart failure with preserved ejection fraction. Circ. Heart Fail. 3, 29–34 (2009).
112. Kosmala, W. et al. Effect of If -channel Inhibition on hemodynamics and exercise tolerance in heart failure with preserved ejection fraction: a randomized trial. J. Am. Coll. Cardiol. 62, 1330–1338 (2013).
113. Cole, C. R., Blackstone, E. H., Pashkow, F. J., Snader, C. E. & Lauer, M. S. Heart-rate recovery immediately after exercise as a predictor of mortality. N. Engl. J. Med. 341, 1351–1357 (1999).
114. Schlaich, M. P. et al. Relation between cardiac sympathetic activity and hypertensive left ventricular hypertrophy. Circulation 108, 560–565 (2003).
115. Funakoshi, K., Hosokawa, K., Kishi, T., Ide, T. & Sunagawa, K. Striking volume intolerance is induced by mimicking arterial baroreflex failure in normal left ventricular function. J. Card. Fail. 20, 53–59 (2014).
116. Floras, J. S. Sympathetic nervous system activation in human heart failure: clinical implications of an updated model. J. Am. Coll. Cardiol. 54, 375–385 (2009).
117. Kitzman, D. W. et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 288, 2144–2150 (2002).
118. Haykowsky, M. J. et al. Effect of endurance training on the determinants of peak exercise
oxygen consumption in elderly patients with stable compensated heart failure and preserved ejection fraction. J. Am. Coll. Cardiol. 60, 120–128 (2012).
119. Vogiatzis, I. & Zakynthinos, S. The physiological basis of rehabilitation in chronic heart and lung disease. J. Appl. Physiol. (1985) 115, 16–21 (2013).
120. Shah, S. J. Matchmaking for the optimization of heart failure with preserved ejection fraction clinical trials: no laughing matter. J. Am. Coll. Cardiol. 62, 1339–1342 (2013).
121. Haykowsky, M. J. et al. Skeletal muscle composition and its relation to exercise intolerance in older patients with heart failure and preserved ejection fraction. Am. J. Cardiol. 113, 1211–1216 (2014).
122. Kitzman, D. W. et al. Skeletal muscle abnormalities and exercise intolerance in older patients with heart failure and preserved ejection fraction. Am. J. Physiol. Heart Circ. Physiol. 306, H1364–H1370 (2014).
123. Poole, D. C., Hirai, D. M., Copp, S. W. & Musch, T. I. Muscle oxygen transport and utilization in heart failure: implications for exercise (in)tolerance. Am. J. Physiol. Heart Circ. Physiol. 302, H1050–H1063 (2012).
124. Borlaug, B. A. Heart failure with preserved and reduced ejection fraction: different risk profiles for different diseases. Eur. Heart J. 34, 1393–1395 (2013).
125. Dai, D. F., Rabinovitch, P. S. & Ungvari, Z. Mitochondria and cardiovascular aging. Circ. Res. 110, 1109–1124 (2012).
126. Bergmann, O. et al. Evidence for cardiomyocyte renewal in humans. Science 324, 98–102 (2009).
127. Biernacka, A. & Frangogiannis, N. G. Aging and cardiac fibrosis. Aging Dis. 2, 158–173 (2011).
128. Pillai, V. B., Sundaresan, N. R. & Gupta, M. P. Regulation of Akt signaling by sirtuins: its implication in cardiac hypertrophy and aging. Circ. Res. 114, 368–378 (2014).
129. Boon, R. A. et al. MicroRNA-34a regulates cardiac ageing and function. Nature 495, 107–110 (2013).
130. Madeo, F., Tavernarakis, N. & Kroemer, G. Can autophagy promote longevity? Nat. Cell Biol. 12, 842–846 (2010).
131. Loffredo, F. S. et al. Growth differentiation factor 11 is a circulating factor that reverses age-related cardiac hypertrophy. Cell 153, 828–839 (2013).
132. Rider, O. J. et al. Beneficial cardiovascular effects of bariatric surgical and dietary weight loss in obesity. J. Am. Coll. Cardiol. 54, 718–726 (2009).
133. Lavie, C. J., McAuley, P. A., Church, T. S., Milani, R. V. & Blair, S. N. Obesity and cardiovascular diseases—implications regarding fitness, fatness and severity in the obesity paradox. J. Am. Coll. Cardiol. 63, 1345–1354 (2014).
134. Rider, O. J. et al. Effects of catecholamine stress on diastolic function and myocardial energetics in obesity. Circulation 125, 1511–1519 (2012).
135. Kozakova, M. et al. Reduced left ventricular functional reserve in hypertensive patients with preserved function at rest. Hypertension 45, 619–624 (2005).
136. Norman, H. S. et al. Decreased cardiac functional reserve in heart failure with preserved systolic function. J. Card. Fail. 17, 301–308 (2011).
137. Nelson, M. D. et al. Diastolic dysfunction in women with signs and symptoms of ischemia in the absence of obstructive coronary artery disease: a hypothesis-generating study. Circ. Cardiovasc. Imaging 7, 510–516 (2014).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved