The Non-surgical Treatment of Peyronie's Disease
4
British Journal of Uro/ogy (1980). 52. 392-395 0 1980 British Association of Urological Surgeons 0007- I33 I /80/02840392$02.00 The Non-surgical Treatment of Peyronie‘s Disease GORDON WILLIAMS and N. A. GREEN Department of Urology, Norfolk and Norwich Hospital, Norwich Summary - Forty-five patients with Peyronie’s disease are described. No patient received treatment for one year from the time of presentation. Three had a complete resolution of their symptoms and signs during this period. The remaining patients received injections of triamcinolone hexacetonide (Lederle) into the plaques at 6-weekly intervals for 36 weeks. Thirty-three per cent had complete or marked improvement in their symptoms; those responding were younger patients with small, firm, discrete plaques in the distal penis. We recommend a non-operative approach in this group. Surgery or chemotherapy should be reserved for those older patients with harder, larger or confluent plaques. This condition was first described by Francois de la Peyronie in 1743. Since then many series have been reported and a variety of methods used for treatment. The clinical features of Peyronie’s disease are well established, but the aetiology and the natural history of the disease, if left alone, are still unknown. Treatment of the condition remains an enigma to urologists. Williams and Thomas (1970), who reported 21 cases, felt that “Peyronie’s disease is fully manifest when the patient is first seen”. No patient in their series became worse and the natural history was one of resolution, albeit over many months. We report a series of 45 patients seen by one of us (N.A.G.) over a 10-year period from 1964 to 1974 with a minimum follow-up of 4 years. We have tried to determine those features of the condition which may lead to spontaneous improve- ment and those which may indicate that some form of treatment will be required. Patients and Methods There were 45 patients whose age at presentation ranged from 32 to 78 years with a mean of 57 years (Fig.). A detailed family history was taken from each patient to determine whether there was any association between Peyronie’s disease and collagen disorders, gout and Dupuytren’s dia- thesis. The latter may present as a spectrum of manifestations ranging from nodule formation in the palmar fascia alone to the complete syndrome of palmar contracture, fibrous plantar nodules and Garrod’s pads-the knuckle pads over the dorsum of the interphalangeal joints (Garrod, 1904; Lettin, 1964). The history where deformity of the penis occurred was directed towards the type of devia- tion of the penis during erection. Direct question- ing as to whether sexual intercourse was possible or not was recorded in an attempt to evaluate whether this improved with or without treatment. Presenting symptoms, whether of pain, plaque or deformity, were noted. The site, size and con- sistency of the main plaque or plaques were also recorded. The plaques were classified as being either hard or firm in consistency, confluent or diffuse, multiple or discrete. Blood was taken for haemoglobin, white count, ESR, tests of liver and renal function, uric acid and rheumatoid factors. X-rays of the chest and penis were carried out on all patients. Received 8 December 1978. Accepted for publication 27 March 1979. Fig. The age incidence at the time of presentation of 45 patients with Peyronie’s disease. 392
-
Upload
gordon-williams -
Category
Documents
-
view
212 -
download
0
Transcript of The Non-surgical Treatment of Peyronie's Disease
British Journal of Uro/ogy (1980). 52. 392-395 0 1980 British Association of Urological Surgeons
0007- I33 I /80/02840392$02.00
The Non-surgical Treatment of Peyronie‘s Disease
GORDON WILLIAMS and N. A. GREEN Department of Urology, Norfolk and Norwich Hospital, Norwich
Summary - Forty-five patients with Peyronie’s disease are described. No patient received treatment for one year from the time of presentation. Three had a complete resolution of their symptoms and signs during this period. The remaining patients received injections of triamcinolone hexacetonide (Lederle) into the plaques at 6-weekly intervals for 36 weeks. Thirty-three per cent had complete or marked improvement in their symptoms; those responding were younger patients with small, firm, discrete plaques in the distal penis. We recommend a non-operative approach in this group. Surgery or chemotherapy should be reserved for those older patients with harder, larger or confluent plaques.
This condition was first described by Francois de la Peyronie in 1743. Since then many series have been reported and a variety of methods used for treatment. The clinical features of Peyronie’s disease are well established, but the aetiology and the natural history of the disease, if left alone, are still unknown. Treatment of the condition remains an enigma to urologists. Williams and Thomas (1970), who reported 21 cases, felt that “Peyronie’s disease is fully manifest when the patient is first seen”. No patient in their series became worse and the natural history was one of resolution, albeit over many months.
We report a series of 45 patients seen by one of us (N.A.G.) over a 10-year period from 1964 to 1974 with a minimum follow-up of 4 years. We have tried to determine those features of the condition which may lead to spontaneous improve- ment and those which may indicate that some form of treatment will be required.
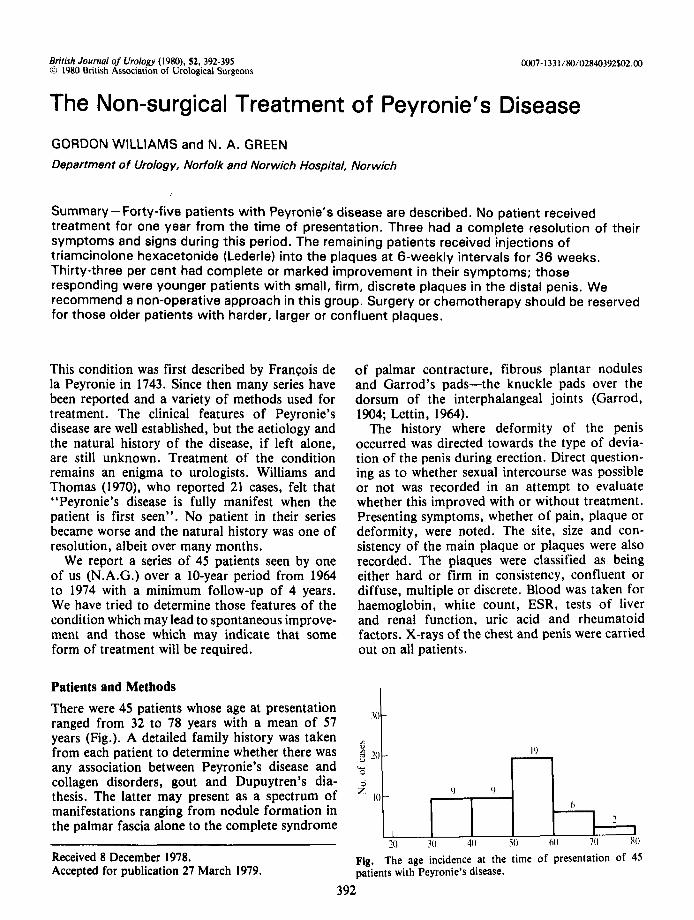
Patients and Methods There were 45 patients whose age at presentation ranged from 32 to 78 years with a mean of 57 years (Fig.). A detailed family history was taken from each patient to determine whether there was any association between Peyronie’s disease and collagen disorders, gout and Dupuytren’s dia- thesis. The latter may present as a spectrum of manifestations ranging from nodule formation in the palmar fascia alone to the complete syndrome
of palmar contracture, fibrous plantar nodules and Garrod’s pads-the knuckle pads over the dorsum of the interphalangeal joints (Garrod, 1904; Lettin, 1964).
The history where deformity of the penis occurred was directed towards the type of devia- tion of the penis during erection. Direct question- ing as to whether sexual intercourse was possible or not was recorded in an attempt to evaluate whether this improved with or without treatment. Presenting symptoms, whether of pain, plaque or deformity, were noted. The site, size and con- sistency of the main plaque or plaques were also recorded. The plaques were classified as being either hard or firm in consistency, confluent or diffuse, multiple or discrete. Blood was taken for haemoglobin, white count, ESR, tests of liver and renal function, uric acid and rheumatoid factors. X-rays of the chest and penis were carried out on all patients.
Received 8 December 1978. Accepted for publication 27 March 1979.
Fig. The age incidence at the time of presentation of 45 patients with Peyronie’s disease.
392
THE NON-SURGICAL TREATMENT OF PEYRONIE’S DISEASE 393
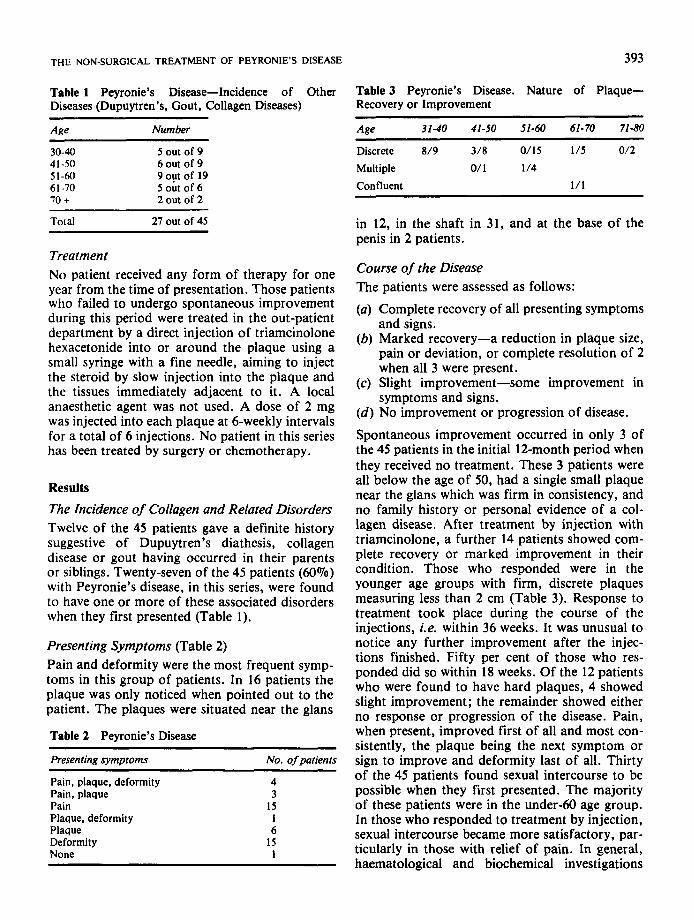
Table 1 Peyronie’s Disease-Incidence of Other Diseases (Dupuytren’s, Gout, Collagen Diseases)
~
Ane Number
30-40 5 out of 9 41-50 6 out of 9 51-60 9 out of 19 61-70 5 out of 6 70 + 2 out of 2
Total 21 out of 45
Treatment No patient received any form of therapy for one year from the time of presentation. Those patients who failed to undergo spontaneous improvement during this period were treated in the out-patient department by a direct injection of triamcinolone hexacetonide into or around the plaque using a small syringe with a fine needle, aiming to inject the steroid by slow injection into the plaque and the tissues immediately adjacent to it. A local anaesthetic agent was not used. A dose of 2 mg was injected into each plaque at 6-weekly intervals for a total of 6 injections. No patient in this series has been treated by surgery or chemotherapy.
Results The Incidence of Collagen and Related Disorders Twelve of the 45 patients gave a definite history suggestive of Dupuytren’s diathesis, collagen disease or gout having occurred in their parents or siblings. Twenty-seven of the 45 patients (6OVo) with Peyronie’s disease, in this series, were found to have one or more of these associated disorders when they first presented (Table 1).
Presenting Symptoms (Table 2) Pain and deformity were the most frequent symp- toms in this group of patients. In 16 patients the plaque was only noticed when pointed out to the patient. The plaques were situated near the glans
Table 2 Peyronie’s Disease
Presenting symptoms No. of patients
Pain, plaque, deformity 4 Pain, plaque 3 Pain I5 Plaque, deformity 1 Plaque 6 Deformity 15 None 1
Table 3 Peyronie’s Disease. Nature of Plaque- Recovery or Improvement
Age 31-40 41-50 51-40 61-70 71-80
Discrete 819 318 0/15 115 012
Multiple O/ 1 114
Confluent 111
in 12, in the shaft in 31, and at the base of the penis in 2 patients.
Course of the Disease The patients were assessed as follows:
(a) Complete recovery of all presenting symptoms and signs.
(b) Marked recovery-a reduction in plaque size, pain or deviation, or complete resolution of 2 when all 3 were present.
(c) Slight improvement-some improvement in symptoms and signs.
( d ) No improvement or progression of disease.
Spontaneous improvement occurred in only 3 of the 45 patients in the initial 12-month period when they received no treatment. These 3 patients were all below the age of 50, had a single small plaque near the glans which was firm in consistency, and no family history or personal evidence of a col- lagen disease. After treatment by injection with triamcinolone, a further 14 patients showed com- plete recovery or marked improvement in their condition. Those who responded were in the younger age groups with firm, discrete plaques measuring less than 2 cm (Table 3). Response to treatment took place during the course of the injections, i.e. within 36 weeks. It was unusual to notice any further improvement after the injec- tions finished. Fifty per cent of those who res- ponded did so within 18 weeks. Of the 12 patients who were found to have hard plaques, 4 showed slight improvement; the remainder showed either no response or progression of the disease. Pain, when present, improved first of all and most con- sistently, the plaque being the next symptom or sign to improve and deformity last of all. Thirty of the 45 patients found sexual intercourse to be possible when they first presented. The majority of these patients were in the under-60 age group. In those who responded to treatment by injection, sexual intercourse became more satisfactory, par- ticularly in those with relief of pain. In general, haematological and biochemical investigations
394 BRITISH JOURNAL OF UROLOGY
were of little value. Three patients had a raised serum uric acid and 3 positive rheumatoid factor. Radiography of the penis showed calcification to be present in a plaque in only one case.
Discussion Since Peyronie’s initial description of this disease, a considerable volume of literature has accumu- lated. The aetiology of the disease is still unknown. It has been suggested that it is an expression of premature ageing of connective tissue which has received repeated small vascular insults (Desanctis and Furey, 1967). There seems to be a connection with the fibrous involvement observed in Dupuy- tren’s diathesis. Gallizia (1964) reported that 10% of patients with Peyronie’s disease have a co- existent Dupuytren’s contracture. In our series, the coexistence of Dupuytren’s diathesis with Peyronie’s disease was much higher at 47%.
The maximum incidence of the disease occurred between the fortieth and sixtieth year and is simi- lar to that reported by Ashworth (1960) and Pugh (1960). There is no difference in this series in the clinical findings which were reviewed by McRoberts (1969). A higher proportion of plaques occurred in the distal penis in our patients. In other larger series, an equal incidence has been reported, plaques occurring throughout the length of the penis but not in the glans (Pugh, 1960).
An objective evaluation of a particular type of treatment is hampered by the lack of untreated controls. Ashworth (1960) published a series of 32 patients, 11 of whom were untreated and 8 of these were observed for periods of up to 5 years. On the basis of these 8 patients and the remaining treated patients, he believed that “the onset of Peyronie’s disease heralds the end of effective sexual life”. However, Williams and Thomas (1970), in their series of 21 patients, concluded that Peyronie’s disease is fully manifest when the patients are first seen. Six of their patients’ symp- toms resolved completely without treatment, 10 improved so that sexual intercourse was possible and 5 remained unchanged. The average period for resolution in their series, however, was 4 years.
We have tried to determine those features of the condition which might indicate spontaneous improvement or an accelerated rate of improve- ment of symptoms.
It might be argued that a period of observation of one year is too short to assess the incidence of
spontaneous improvement. However, we feel that a patient with pain and deformity of the penis should not be left for up to 4 years in the hope that spontaneous improvement may occur. Three patients, all below the age of 50, under- went spontaneous improvement within the first 12 months of observation, although all had small plaques (<2 cm) in the distal penis.
The use of steroid injections into the plaques has been extensively reported. Desanctis and Furey (1967) noted that 81% of their patients treated by steroid injections benefited to a moderate or marked degree. Triamcinolone hexacetonide is a long-acting glucocorticoid with low solubility, producing, in theory, maximal local action with minimal side effects. It has been shown to be effective in the treatment of Dupuytren’s contrac- ture and hypertrophic scars. Of the 42 patients who received injections of this drug, 33% had complete recovery or marked improvement in their symptoms and signs during the course of treatment. Twelve of these patients were below the age of 50 with firm, discrete plaques measuring less than 2 cm in the shaft or distal penis. Patients with hard or larger plaques and those with associ- ated collagen disorders were unlikely to respond to this form of treatment. Whether those patients who responded to steroid injections would have improved spontaneously if left untreated for longer periods will remain unknown. However, there were no complications or side effects in this method of treatment and the speed of response was encouraging.
Chemotherapy or surgery should be considered only for older patients with hard, multiple or con- fluent plaques. Procarbazine, a cytostatic drug, has been used to treat 24 patients with Peyronie’s disease (Chesney, 1975). Good results were reported in 11. The drug is also a monoamine oxidase inhibitor and should be administered with caution. Severe bone marrow depression may occur and there is experimental evidence that the drug can cause damage to the germinal epi- thelium of the testes. In his series, 3 patients still had complete azoospermia at the end of their treatment 3 months later. Potassium para-amino benzoate (Potaba) has also been used (Hasche- Klunder, 1970). This involves taking 12 g of the drug each day for at least 6 to 12 months for maximum response. The action of the drug is antagonised by sulphonamides, and anorexia and nausea may occur during the course of therapy. Treatment by local injectiop involved a shorter
THE NON-SURGICAL TREATMENT OF PEYRONIE’S DISEASE 395
course of treatment and was free of side effects. We feel that in younger patients with small,
firm plaques, the conservative approach to management should be adopted.
References Ashworth, A. (1960). Peyronie’s disease. Proceedings of the
Royal Sociefy of Medicine, 53, 692-694. Chesney, J. (1975). Peyronie’s disease. British Journal of
Urology, 41, 209-2 1 8. Desanctis, P. N. and Furey, C. A., Jun. (1967). Steroid injec-
tion therapy for Peyronie’s disease: a 10 year summary and review of 38 cases. Journal of Urology, 91, 114-1 16.
Callizia, F. A. (1964). Triade collaghe: maladie de La Peyronie, maiadie de Dupuytren et fibrose du cartilage auriculaire. Journal d’Urologie et de Nkphrologie, 70, 424-427.
Carrod, A. E. (1904). Concerning pads upon the finger joints and their clinical relationships. British Medical Journal, 2, 8 .
Hasche-Klunder, R. (1970). Behandlung der Induration penis plastic. Urologe, 9, 335-336.
Lettin, A. W. F. (1964). Dupuytren’s diathesis-a case report. Journal of Bone and Joint Surgery, 46B, 220-225.
McRoberts, J. W. (1969). Peyronie’s disease. Surgery, Gyne- cology and Obstetrics, 129, 1291-1294.
Peyronle, F. de La (1743). Sur quelques obstacles qui s’opposent a I’kjaculation naturelle de la semence. Mkmoires de I’Acadkmie Royale de Chirurgie, 425-434.
Pugh, R. C. B. (1960). The pathology of fibrotic lesions. Proceedings of the Royal Society of Medicine, 53, 685-689.
Williams, J. L. and Thomas, G. C. (1970). The natural history of Peyronie’s disease. Journal of Urology, 103, 75-16.
The Authors Gordon Williams, MB, FRCS, formerly Senior Registrar. Now Consultant Urologist, Hammersmith Hospital, London.
N. A. Green, MS, FRCS, Consultant Urologist.
Requests for reprints to: Gordon Williams, Department of Urology, Hammersmith Hospital, Ducane Road, London W12 OHS.