The New Surgical Ablation Guidelines The Heart Hospital ... · COR I, LOE C-EO • 2017 HRS...
41
The Heart Hospital James R. Edgerton, MD, FACS, FACC, FHRS • Surgical Director of Dysrhythmia Clinic, Center for Advanced Cardiac Care • Chair , Quality and Research Committee, Texas Quality Initiative The Heart Hospital Baylor Plano Plano, Texas The New Surgical Ablation Guidelines AATS STARS Meeting Miami Beach November 17, 2017
Transcript of The New Surgical Ablation Guidelines The Heart Hospital ... · COR I, LOE C-EO • 2017 HRS...

The Heart Hospital
James R. Edgerton, MD, FACS, FACC, FHRS• Surgical Director of Dysrhythmia Clinic, Center for Advanced Cardiac Care • Chair, Quality and Research Committee, Texas Quality Initiative
The Heart Hospital Baylor PlanoPlano, Texas
The New Surgical Ablation Guidelines AATS STARS Meeting
Miami BeachNovember 17, 2017

Disclosures 2017
Edgerton Disclosures• Paid consultant - AtriCure• Speakers Bureau - AtriCure
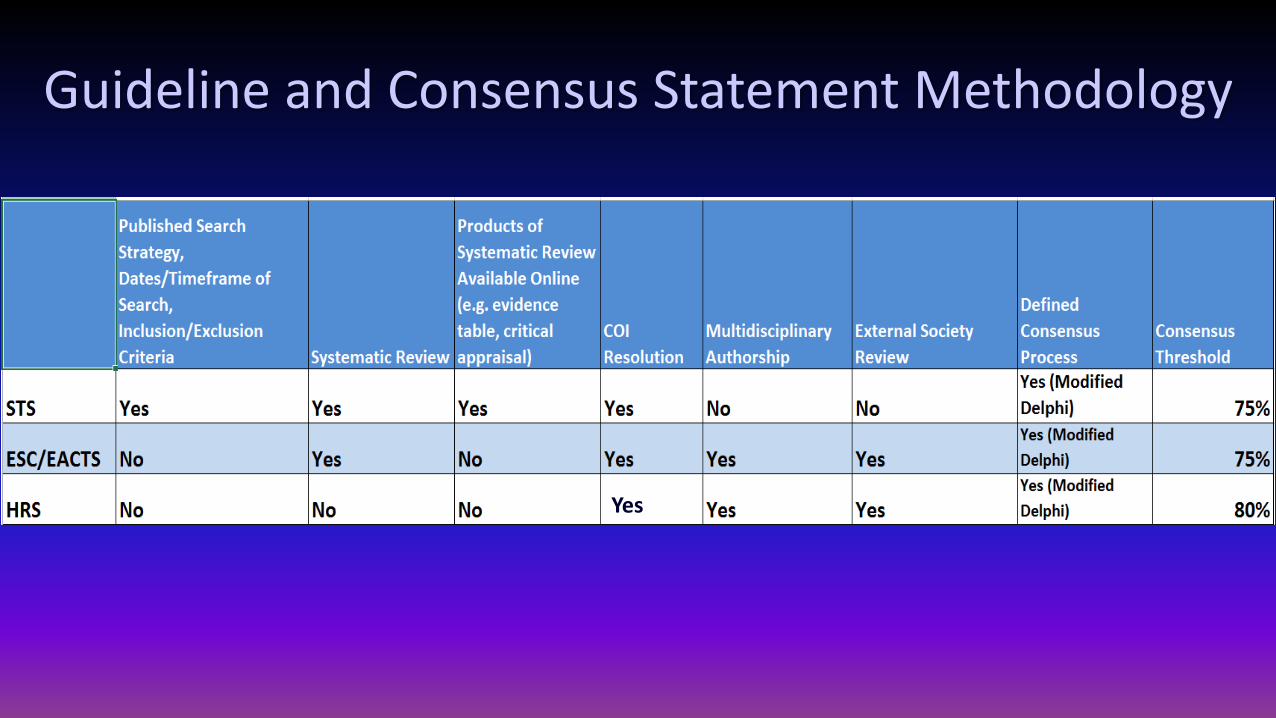
Guideline and Consensus Statement Methodology
Yes

Current...Class of Recommendation: CORLevel of Evidence: LOE
• Changes in:• COR III
• Moderate, No Benefit (C-NB)• Strong, Harm (C-Harm)
• LOE B• Randomized (B-R)• Nonrandomized (B-NR)
• LOE C• Limited Data (C-LD)• Expert Opinion (E-O)

LOE C-EOTwo guys with grey hair playing Ouija

2014 ACC AHA HRS Guideline for the Management ofPatients with Atrial Fibrillation
This becomes IIa in 2016 ESC Guidelines


2016 ESC AF Ablation Decision Tree


2016 ESC AF Ablation Decision Tree

2016 ESC AF Ablation Decision Tree
In ESC, Hybrid Therapy =• AAD + CA• AAD + PPM

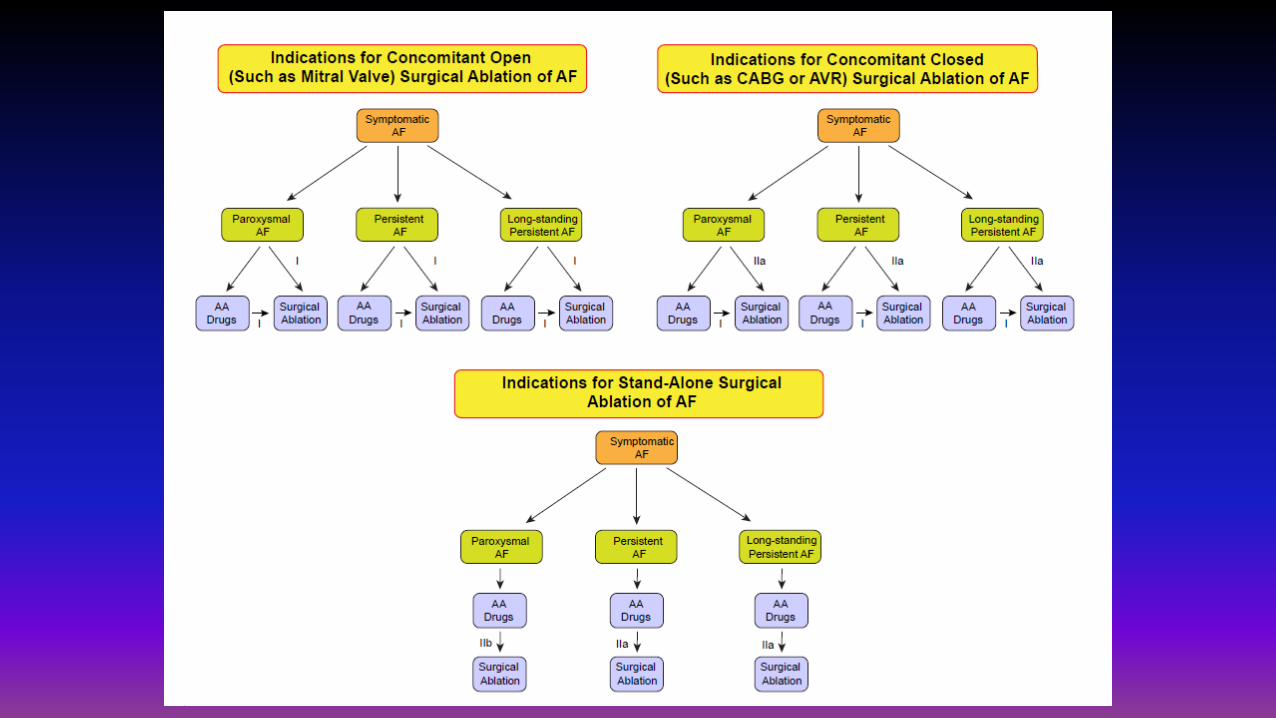
• Uses Updated COR & LOE• Separates Concomitant recommendations into:
– Open atrium procedures (e.g.: Mitral valve)– Closed atrium procedures (e.g.: Aortic valve, CABG)

2017 Society of Thoracic Surgeons GuidelinesConcomitant Ablation
• Concomitant to Mitral Surgery: COR I LOE B-R• Concomitant to CABG, AVR, AVR/CABG: COR I LOE B-NR

2017 Society of Thoracic Surgeons GuidelinesSize of LAA
• Surgical Ablation for symptomatic AF, with LA > 4.5 cmor > moderate MR, by PVI alone: COR III-NB, LOE C-EO
2017 Society of Thoracic Surgeons GuidelinesStand Alone Ablation
• Primary Surgical Ablation, for symptomatic AF, in absence of structural Heart disease, and refractory to AAD and/or CA: COR 2A, LOE B-R
2017 Society of Thoracic Surgeons GuidelinesStand Alone Ablation for Persistent & LSP
• Surgical ablation for symptomatic persistent or longstanding persistent AF in the absence of structural heart disease is reasonable, using the Cox-Maze III/IV lesion set compared with pulmonary vein isolation alone. COR 2A, LOE B-NR

2017 Society of Thoracic Surgeons GuidelinesStand Alone Ablation for Persistent & LSP
• Surgical ablation for symptomatic persistent or longstanding persistent AF in the absence of structural heart disease is reasonable, using the Cox-Maze III/IV lesion set compared with pulmonary vein isolation alone. COR 2A, LOE B-NR
• So what are we saying here.....???• We are saying that PVI alone is totally inadequate therapy.

2017 HRS Consensus Statement on Catheter and Surgical Ablationof
Atrial Fibrillation
• Released May 12, 2017• Heart Rhythm e-pub Sept 15, 2017
(DOI: 10.1016/j.hrthm.2017.05.012),
• Executive Summary print publication October 2017(J Interv Card Electrophysiol (2017) 50:1–55, DOI 10.1007/s10840-017-0277-z)
• Scheduled for print publication in Heart Rhythm and Europace

endorsed by the Society of Thoracic Surgeons (STS), the American College of Cardiology (ACC) , the American Heart Association (AHA) the Canadian Heart Rhythm Society (CHRS) , the Japanese Heart Rhythm Society (JHRS), and the Brazilian Society of CardiacArrhythmias (Sociedade Brasileira de Arritmias Cardíacas [SOBRAC]).

• Is a CONSENSUS Statement not a Guideline Statement• Uses Updated COR & LOE• Separates Concomitant recommendations into:
– Open atrium procedures (e.g.: Mitral valve)– Closed atrium procedures (e.g.: Aortic valve, CABG)
• SEPARATES SYMPTOMATIC AND ASSYMPTOMATIC Recommendations

2017 HRS Consensus StatementConcomitant Ablation
• Concomitant to Mitral Surgery: COR I LOE B-R

2017 HRS Consensus StatementConcomitant Ablation
• Concomitant to Mitral Surgery: COR I LOE B-R

2017 HRS Consensus StatementConcomitant Ablation
• Concomitant to CABG, AVR, AVR/CABG: COR I LOE B-NR

2017 HRS Consensus StatementConcomitant Ablation
• Concomitant to CABG, AVR, AVR/CABG: COR I LOE B-NR

2017 HRS GuidelinesStand Alone Ablation
• Primary Surgical Ablation, for symptomatic AF, in absence of structural Heart disease, and refractory to AAD and/or CA: – Paroxysmal: COR 2B, LOE B-NR– Persistent: COR 2A, LOE B-NR– LSP: COR 2A, LOE B-NR

2017 HRS GuidelinesHYBRID Ablation
• It may be reasonable to apply the indications for stand-alone surgical ablation to patients being considered for hybrid ablation: 2B, C-EO
• So these stand alone recommendations hold for HYBRID– Paroxysmal: COR 2B, LOE B-NR– Persistent: COR 2A, LOE B-NR– LSP: COR 2A, LOE B-NR

Treatment of LAA• 2014 ACC, AHA, HRS Guideline:
– Surgical excision of the LAA may be considered in patients undergoing cardiac surgery. COR IIb LOE C
• 2016 ESC Guidelines– Consider adding surgical LAA exclusion in selected patients: COR IIb, LOE C
• 2017 STS Guidelines– During concomitant procedures, it is reasonable to surgically manage the LAA.
COR IIA, LOE C-EO • 2017 HRS Consensus Statement: Silent
– “... It is reasonable and probably helpful to eliminate the LAA with any technique at the time of AF surgery, ... We have elected not to make recommendations regarding LAA occlusion, resection, or ligation in this document...”

Heart Team Approach• 2014 ACC AHA HRS Guidelines: Silent• 2016 ESC Guidelines:
– “This Task Force proposes that decisions involving AF surgery or extensive AF ablation should be based on advice from an AF Heart Team....consisting of a cardiologist, electrophysiologist, cardiac surgeon”
• 2017 STS Guidelines:– multidisciplinary heart team assessment, treatment planning, and long-
term follow-up can be useful. COR I, LOE C-EO
• 2017 HRS Consensus Statement: Silent

Edgerton Guideline/Consensus Comparison TableConcomitant Open Atrium
Concomitant Closed Atrium
Asymptomatic Concomitant
Stand AloneSymptomaticRefractory by PVI
Stand Alone Symptomatic Persistent & LSPby Full Maze
LAA Closure Heart Team
COR LOE COR LOE COR LOE COR LOE COR LOE COR LOE COR LOE
2014 ACC AHA HRS
Ila C IIa C Same IIb B IIb B(must be refractory)
IIb C _
2016 ECS IIa A IIa A IIa A IIa B IIa C(must be refractory)
IIb C supports
2017 STS I A I B-NR Same as symptomatic
IIa B-R IIa B-NR IIa C-LD I C-EO
2017 HRS Consensus
I B-R I B-NRPrior to AADs:IIA B-NR
No Recommendation
Paroxysmal:IIb B-NR
IIa B-NR silent silent
Hybrid Catheter/Surgical Ablation
2017 HRS Consensus PAF: IIb, B-NR Persistent and LSP: IIa, B-NR

So what is current practice?Penetrance of Concomitant Ablation in Patients with Atrial Fibrillation
• STS Database• MVRR±CABG : 68.4% • AVR+MVR : 59.1% • AVR±CABG : 39.3%• isolated CABG : 32.8%

How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines:
Examining Surgical Ablation for Atrial Fibrillation
• To provide recommendations related to – general outcomes of surgical ablation,– state of hybrid procedures, – optimal ablation tools – education and training of surgeons.
AATS Statement uses a different approach of examining research questions

How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines:
Examining Surgical Ablation for Atrial Fibrillation
• Research Question 1: Does concomitant surgical ablation for atrial fibrillation increase the incidence of perioperative morbidity?– Recommendation #1. Addition of a concomitant surgical ablation procedure
for atrial fibrillation does not increase morbidity
• Research Question #2A: Does concomitant surgical ablation for AF reduce the incidence of early stroke/transient ischemic attack (TIA)?– Recommendation #2. Addition of a concomitant surgical ablation procedure
for atrial fibrillation does not change the incidence of early stroke• Class IIa: It is reasonable to perform ablation because the incidence of perioperative morbidity is not increased.• Level of Evidence: A
AATS Statement uses a different approach of examining research questions

How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines
• Research Question #2B. Does concomitant surgical ablation for atrial fibrillation reduce the incidence of late stroke/TIA?– Recommendation #3. Overall, addition of a concomitant surgical ablation procedure for
atrial fibrillation does not change the incidence of late stroke/TIA, but subgroup analysis of non-randomized controlled trials (RCTs) found a significant reduction in late stroke/TIA incidence.
• Research Question #3. Does concomitant surgical ablation for atrial fibrillation improve health-related quality of life and atrial fibrillation (AF)-related symptoms?– Recommendation #4. A surgical procedure that includes concomitant surgical ablation
for AF does improve health-related quality of life, but this improvement is similar to that observed in patients who undergo cardiac surgery without surgical ablation. Addition of concomitant surgical ablation for atrial fibrillation does improve AF-related symptoms and this improvement is greater than in patients without surgical ablation.
AATS Statement uses a different approach of examining research questions

How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines
• Research Question #4A: Does concomitant surgical ablation for atrial fibrillation improve short-term survival?– Recommendation #5. Addition of concomitant surgical ablation for atrial
fibrillation does improve 30-day operative mortality.
• Research Question #4B: Does concomitant surgical ablation for atrial fibrillation improve long-term survival (>30 days)?– Recommendation #6. Overall, addition of a concomitant surgical ablation
procedure for atrial fibrillation improves long-term survival, but subgroup analysis of RCTs found no significant improvement.
AATS Statement uses a different approach of examining research questions

How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines
• Research Question #5: What are the indications for a hybrid ablation or stand alone off pump epicardial ablation in patients with atrial fibrillation?– Recommendation #7. Overall, hybrid procedures have shown promising results
compared to percutaneous catheter ablation in a subgroup of symptomatic patients with AF in which medical treatment and/or percutaneous catheter ablation have failed.
• Research Question #6: Which surgical ablation devices are associated with reliable transmural lesions?– Recommendation #9. The best evidence exists for the use of bipolar
radiofrequency clamps and cryoablation devices, which have become integral parts of many procedures including pulmonary vein isolation and the Cox maze IV procedure. The use of epicardial unipolar radiofrequency ablation outside of clinical trials is not recommended, as its efficacy remains questionable
AATS Statement uses a different approach of examining research questions
How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines
• Research Question #7: What is the impact of surgeon experience with surgical ablation on return to sinus rhythm in patients with AF?– Recommendation #10. Training and education should be completed prior to
the performance of surgical ablation. We highly recommend surgeons that are new to surgical AF be proctored by an experienced surgeon for 3-5 cases prior to performing surgical ablation alone.
• All the above recommendations are accompanied by COR and LOE – I have somewhat simplified them here– You are encouraged to read the document
AATS Statement uses a different approach of examining research questions
How do we bridge the gap: Know the DataAATS Expert Consensus Guidelines:
Examining Surgical Ablation for Atrial Fibrillation
• Recommendation #8. minimally invasive approaches to isolate the pulmonary veins bilaterally have shown promising results compared to percutaneous catheter ablation in a subgroup of symptomatic patients with paroxysmal AF and a small left atrium in which medical treatment and/or percutaneous catheter ablation have failed– Class IIa: It is reasonable to perform stand alone surgical ablation for
pulmonary vein isolation in patients with symptomatic paroxysmal AF and small left atria..
– Level of Evidence: B-R
How are the Guidelines Different• Multidisciplinary Authorship – increases credibility
– AATS and STS Guidelines: NO– ECS and HRS: YES (EPs, Cardiologists, & Surgeons all agree)
• Stress SYMPTOMATIC AF– AATS and STS Guidelines: NO– ECS and HRS: YES,
• but HRS has cracked the door open for CA of select asymptomatic pts – COR 2B • Recommendations based on Efficacy
– STS– HRS– ECS
• AATS– “...AATS guidelines are focused less on the efficacy of surgical ablation and more on the surgical
outcomes, both short and long term.”– They address 5 “Research Questions”

Terlingua, Texas
Thank You