The Model For Improvement Part 1 Chapter Quality Network Asthma Pilot Project Asthma Learning...
61
The Model For Improvement Part 1 Chapter Quality Network Asthma Pilot Project Asthma Learning Collaborative Peter Margolis, MD PhD
-
Upload
pamela-peters -
Category
Documents
-
view
217 -
download
0
Transcript of The Model For Improvement Part 1 Chapter Quality Network Asthma Pilot Project Asthma Learning...

The Model For Improvement
Part 1Chapter Quality Network Asthma Pilot
ProjectAsthma Learning Collaborative
Peter Margolis, MD PhD

I have no relevant financial relationships with the manufacturers(s) of any commercial
products(s) and/or provider of commercial services discussed in this CME activity.

Session Objectives
• To describe the components of the Model for Improvement
• To write a clear aim statement for your team.– To identify goals that you will measure
to support your aim

Headlines: Previous Initiatives
• Sandhills Pediatrics reduces asthma admissions in Moore County to lowest among NC counties
• PHO cuts asthma admissions by 36%

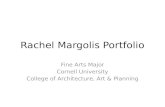
Aggregate Total Pop Asthma(8 SE-PA practices, average of 600 patients per practice)
(5,000 patients in total asthma population)-
7
-8
-8
-8
-8
-8
-8
-8
-8
-80
20
40
60
80
100
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Se
…
Oc
…
No
…
De
…
Ja…
Fe…
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Pct of asthma patients with control assessed
-7
-8
-8
-8
-8
-8
-8
-8
-8
-80
20
40
60
80
100
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Se
…
Oc
…
No
…
De
…
Ja…
Fe…
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Pct of asthma patients with action plan
-6
-8
-8
-8
-8
-8
-8
-8
-8
-80
20
40
60
80
100
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Se
…
Oc
…
No
…
De
…
Ja…
Fe…
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…Pct of asthma patients with controller med
-7
-8
-8
-8
-8
-8
-8
-8
-8
-80
20
40
60
80
100
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Se
…
Oc
…
No
…
De
…
Ja…
Fe…
Ma…
Ap
…
Ma…
Ju…
Jul…
Au
…
Pct asthma pts with current flu vaccine
29 percentage point improvement

Multiple Barriers and Opportunities for Promoting
Optimal Development• What are some challenges you are facing
in:– Eliciting parents’ concerns and addressing
information needs– Helping parents enhance their child’s
development – Identifying children at risk for developmental
and behavioral problems– Linking families with needed community
services

Barriers and Opportunities for Promoting Optimal
Development• Parent
– Knowledge about development– Skills at managing behavior– Willingness/ability to as clinicians about concerns
• Provider– Time – Counseling resources and skills
• Practice– Routine process for eliciting concerns– Organized materials and resources to meet families’
needs– Ability to link families with community resources

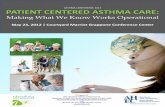
GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do

Three Fundamental Questions for Improvement
• What are we trying to accomplish?
• How will we know that a change is an improvement?
• What changes can we make that will result in an improvement?

Model for Improvement
• Aim
• Measures
• Ideas
What are we trying to accomplish?
How will we know that changes are an improvement?
What changes can we make that will result in
an improvement?

Teams with clear aim and goals are more successful!
Why Spend Time Refining Aim and Goals?

What Are We Trying to
Accomplish? Aim: A written statement of the accomplishments
expected from team’s improvement effort
Key component:– A general description of aim (e.g., provide optimal asthma
care)
You may want to add:– Identification of specific patient population (e.g., all children
under 5 years of age)– Some guidance for carrying out the work (e.g., can start with
one physician/nurse team and spread to others)

• I will give a talk about how to use QI to improve asthma care during LS 1.
• I will explain how to use the model for improvement
• By 3 pm on 9/17/09, 10 out of the 10 teams will have completed Aim statements for their work to improve asthma care.
My Aim

The Best Aim Statements:
• Provide a rationale and point of shared vision for team’s efforts
• S.M.A.R.T
S: SPECIFIC
M: MEASUREABLE
A: ACTION-ORIENTED
R: RELEVANT
T: TIMELY

We will increase the proportion of parents who whose asthma control is assessed.
We will implement a planned care approach to provide reliable asthma care.

We will increase the proportion of parents who receive optimal asthma care from 10% to 90% by Sept, 2010.
We will increase the proportion of patients with at least an annual assessment of asthma from 60% to 90% by Sept, 2010.

Global Aim
What will we accomplish over 1 year, 2 years, 3 years?
Allows the entire practice to understand and eventually buy-in to goal
Keeps team focused and goal-oriented

Specific Aim Statement
What is the work we are doing right now?
What will we accomplish in the next 90 days?
How do you run a marathon?
ONE MILE AT A TIME

Goals Tell You When You’ve Reached Your
Aim• They define the way you expect your
improved system to work • They establish specific numeric targets
for your work• They describe the magnitude of change
expected• They should be challenging, but
attainable– Stretch goals encourage creativity and
innovation

Model Aim StatementABC Pediatrics intends to improve preventive and developmental care for children by developing efficient practice-based systems to organize preventive and developmental care.
We will integrate standardized screening tools and anticipatory guidance into the practice workflow, increase family involvement through the use of brief parent questionnaires to assist us in discussing their concerns. We will also increase our knowledge of community services by documenting each child’s early care providers and developing a community resource list. We will implement a standard letter for parents to share with ECE providers from ABC Pediatrics indicating our involvement with a specific child that includes contact information to reach our practice.
By (date): Sept 1, 2009 for children up to 5 years of age and their families in our practice.
Our goals are: 1.>90% of parents report needs met: AGPE and child’s development2.>95% of appropriate encounters include screening for depression, pyschosocial issues and structured developmental screening3.>90% of parents report receiving information to address their concerns 4.>75% of parents read with child daily5.> 90% of parents report screening about substance abuse and domestic violence6.>12 Office System Inventory items in place

Model Aim StatementABC Pediatrics intends to improve preventive and developmental care for children by developing efficient practice-based systems to organize preventive and developmental care.
We will integrate standardized screening tools and anticipatory guidance into the practice workflow, increase family involvement through the use of brief parent questionnaires to assist us in discussing their concerns. We will also increase our knowledge of community services by documenting each child’s early care providers and developing a community resource list. We will implement a standard letter for parents to share with ECE providers from ABC Pediatrics indicating our involvement with a specific child that includes contact information to reach our practice.
By (date): Sept 1, 2009 for children up to 5 years of age and their families in our practice.
Our goals are: 1.>90% of parents report needs met: AGPE and child’s development2.>95% of appropriate encounters include screening for depression, pyschosocial issues and structured developmental screening3.>90% of parents report receiving information to address their concerns 4.>75% of parents read with child daily5.> 90% of parents report screening about substance abuse and domestic violence6.>12 Office System Inventory items in place
Gap this work is addressing

Model Aim StatementABC Pediatrics intends to improve preventive and developmental care for children by developing efficient practice-based systems to organize preventive and developmental care.
We will integrate standardized screening tools and anticipatory guidance into the practice workflow, increase family involvement through the use of brief parent questionnaires to assist us in discussing their concerns. We will also increase our knowledge of community services by documenting each child’s early care providers and developing a community resource list. We will implement a standard letter for parents to share with ECE providers from ABC Pediatrics indicating our involvement with a specific child that includes contact information to reach our practice.
By (date): Sept 1, 2009 for children up to 5 years of age and their families in our practice.
Our goals are: 1.>90% of parents report needs met: AGPE and child’s development2.>95% of appropriate encounters include screening for depression, pyschosocial issues and structured developmental screening3.>90% of parents report receiving information to address their concerns 4.>75% of parents read with child daily5.> 90% of parents report screening about substance abuse and domestic violence6.>12 Office System Inventory items in place
Goals
Ambitious numeric targets

Model Aim StatementABC Pediatrics intends to improve preventive and developmental care for children by developing efficient practice-based systems to organize preventive and developmental care.
We will integrate standardized screening tools and anticipatory guidance into the practice workflow, increase family involvement through the use of brief parent questionnaires to assist us in discussing their concerns. We will also increase our knowledge of community services by documenting each child’s early care providers and developing a community resource list. We will implement a standard letter for parents to share with ECE providers from ABC Pediatrics indicating our involvement with a specific child that includes contact information to reach our practice.
By (date): Sept 1, 2009 for children up to 5 years of age and their families in our practice.
Our goals are: 1.>90% of parents report needs met: AGPE and child’s development2.>95% of appropriate encounters include screening for depression, pyschosocial issues and structured developmental screening3.>90% of parents report receiving information to address their concerns 4.>75% of parents read with child daily5.> 90% of parents report screening about substance abuse and domestic violence6.>12 Office System Inventory items in place
Guidance about how the work will be done

Team Exercise: Aim Statement Worksheet
Name of Organization:Intends to: General Aim By: Timely (Global and Specific for next 90 days) For: Specific populationBecause: Rationale/Framework (clear for others)
Goals: Measurable, Relevant Goals

GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0

The Model For Improvement Part 2
and Accelerating ImprovementChapter Quality Network Asthma Pilot
ProjectAsthma Learning Collaborative
Peter Margolis, MD, PhD

I have no relevant financial relationships with the manufacturers(s) of any commercial
products(s) and/or provider of commercial services discussed in this CME activity.

What are we trying toaccomplish?
How will we know that achange is an improvement?
What changes can we make thatwill result in improvement?
Act Plan
Study Do
Model for Improvement

How will we knowthat a change is
an improvement?

Do a statistical test to rule out the null hypothesis

Measurement for Improvement
Conduct repeated tests (PDSA cycles or planned experiments) to increase our
degree of belief (provide evidence) that a change
led to an improvement

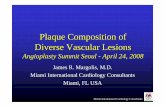
Percentage of Parents Who Report Concerns Are Addressed
%
%
%
%
%
%
Weeks

%
%
%
%
%
%
Weeks
Change #1
Percentage of Parents Who Report Concerns Are Addressed

Percentage of Parents Who Report Concerns Are Addressed
%
%
%
%
%
%
Weeks
Change #1

Measures: Quantitative Data
• Monthly report of % parents report needs met: AGPE and child’s development
• Monthly report of % of appropriate encounters that include screening for depression, other pyschosocial issues and structured developmental screening
• Monthly report of % of parents who report receiving information to address their concerns
• Monthly report of % of parents who read with child daily

North Willow Grove Pediatrics, PC
2701 Blair Mill Road, Suite 10Willow Grove, PA 19090
1010 Horsham Road, Suite 210 North Wales, PA 19454
Marie Smolenski, RN, MSN, CRNPNancy Dockstader

Pct asthma pts w ith current f lu vaccine
020406080
100
Pct of asthma patients w ith 3 care components
020406080
100
Pct of asthma patients w ith action plan
020406080
100

Accelerating Improvement
PDSA CYCLES

GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0

What are we trying toaccomplish?
How will we know that achange is an improvement?
What changes can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do

Why Test?
Act Plan
Study Do
The PDSA Cycle
Why Test?

Cycles for Testing
• Learn how to adapt change to local environment
• Increase belief that change will result in improvement
• Opportunity for “failures” without impacting performance
• Document how much improvement can be expected from change
• Evaluate costs and side-effects of change• Minimize resistance upon implementation

The PDSA Cycle
Act
• What changes are to be made?• Next cycle?
Plan• Objective• Questions and predictions (why)• Plan to carry out the cycle (who, what, where, when)
Study• Complete analysis • of the data
•Compare data to predictions
• Summarize what was learned
Do• Carry out the plan• Document problems & unexpected observations• Begin analysis of the data

Act Plan
Study Do
Use PDSA Cycles to Test and Implement Changes

Act Plan
Study Do
Use PDSA Cycles to Test and Implement Changes
PLAN: Objective/Question
Predict outcome of test
Plan details of test (who, what, when?)

Act Plan
Study Do
Use PDSA Cycles to Test and Implement Changes
Do: Conduct the test and collect data
Document observations – successes/failures
Begin analysis
Plan: Objective/Question
Predict outcome of test
Plan details of test (who, what, when?)

Act Plan
Study Do
Use PDSA Cycles to Test and Implement Changes
Do: Conduct the test and collect data
Document observations – successes/failures
Begin analysis
Plan: Objective/Question
Predict outcome of test
Plan details of test (who, what, when?)
Study: Complete analysis
Compare predictions to test results
Summarize what was learned

Act Plan
Study Do
Use PDSA Cycles to Test and Implement Changes
Do: Conduct the test and collect data
Document observations – successes/failures
Begin analysis
Plan: Objective/Question
Predict outcome of test
Plan details of test (who, what, when?)
Study: Complete analysis
Compare predictions to test results
Summarize what was learned
Act: Take action based on new knowledge
What changes will be made?
Next test?

The Model Provides Structure
for Repeated Tests
Hunches Theories
Ideas
Changes That Result
in Improvement
A P
S D
APS
D
A P
S DD S
P ADATA

Measurement for PDSA
• “Study” is specific to the PDSA– See implementation checklists– Usually not one of core measures – Usually begins and ends with PDSA cycle– Often qualitative (e.g., partner’s views)
• For PDSA Cycle measures, collect data only while you are testing or adapting a change to your system
• Identify/create tools to be used for data collection – make it simple and easy

The PDSA Cycle for Learning and Improvement
Act
• What changes are to be made?• Next cycle?
Plan• Objective• Questions and predictions (why)• Plan to carry out the cycle (who, what, where, when)
Study• Complete analysis • of the data
•Compare data to predictions
• Summarize what was learned
Do• Carry out the plan• Document problems & unexpected observations• Begin analysis of the data

Decrease the Time Frame for a PDSA Test Cycle
• Years• Quarters• Months• Weeks• Days• Hours• Minutes
Drop down two levels to plan Test Cycle!

Do Study
• Reasons for failed tests 1. Change not executed well 2. Support processes inadequate 3. Hypothesis/hunch wrong:
• Change executed but did not result in improvement
• Collect data during the Do phase of the Cycle to help differentiate these situations

GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0


Next Steps: Plan a Ramp of PDSA’s to Reach 90 Day Aim
• Very Small Scale Test
• Follow-up Tests
• Wide-Scale Tests of Change
• Implementation of Change

What Can We Do Now!
By Next Week,By Tuesday,
By Tomorrow

Learning from Each Other
• Transparent Sharing of Data• Sharing Results of PDSA’s• Learning from Successes and Failures

Report Your First PDSA on the Listserv by
Friday, September 18th

Model for ImprovementMeasurement
& PDSA
QUESTIONS?