The Medical Journal of Australia · randomised controlled trial) in favour of therapeutic...
4
MJA 195 (7) · 3 October 2011 388 Clare’s story Clare is a 54-year-old, right-handed pastry chef who presented with discomfort, numbness and tingling in both hands. Her symptoms had begun insidiously 9 months earlier, initially in the right hand, and had since become bilateral and severe, such that she was having difficulty performing her usual tasks at work. She described intermittent dull aching pain extending from the hands up to the elbows bilaterally, and pins and needles in all of the fingers. The symptoms occurred most commonly at work or while she was driving or holding a phone to talk. They were also waking her from sleep most nights. Shaking her hands provided some relief. Clare’s past medical history was otherwise unremarkable. Her weight was 85 kg (body mass index, 33 kg/m 2 ); she had gained 20 kg over the past 2 years after giving up ballroom dancing. She had recently been tested for diabetes as part of a routine check-up and was found to have normal glucose tolerance. She remembered her mother having similar symptoms in her hands, but did not recall any diagnosis being made. On examination, Clare’s hands appeared normal, with no evidence of muscle wasting and no weakness or incoordination. Sensory examination showed a subjective reduction of sensation in the index and middle fingers and thumb of the right hand. Reflexes were present and symmetrical. Prolonged wrist flexion (Phalen test; Box 1) reproduced symptoms of bilateral hand pain and paraesthesiae, but percussion of the median nerves at the wrist (Tinel test; Box 1) did not. The remainder of the neurological examination was normal. APPROACH TO THE PROBLEM The clinical history and examination in this case are highly suggestive of a peripheral nerve disorder. The intermittent paraesthesiae and discomfort in the digits supplied by the median nerve, together with nocturnal symptoms and relief provided by shaking, are classical for carpal tunnel syndrome. Carpal tunnel syndrome is commonly bilateral, although it may be asymmetrical and is usually worst in the dominant hand. Many patients present with atypical symptoms. They may describe sensory symptoms and pain throughout the whole hand and forearm (as did Clare), finger swelling or loss of manual dexterity, or they may present with painless atrophy of the thenar eminence. They may simply com- plain of dropping objects. Clare had several risk factors for carpal tunnel syn- drome: an occupation involving repetitive use of the hands, female sex, positive family history, and obesity. At- risk occupations are those that involve repetitive wrist exertion, including factory work and trades such as carpen- try or those involving use of vibrating tools. DIFFERENTIAL DIAGNOSES Differential diagnoses of hand numbness and paraesthe- siae that should be considered in addition to carpal tunnel syndrome are summarised below. Cervical radiculopathy is usually unilateral, accompanied by neck pain, and with symptoms provoked by neck movement, coughing, sneezing and the Valsalva man- oeuvre. Normal results of a clinical neurological examina- tion, with normal power and reflexes, would argue against this diagnosis. Other neuropathies such as a more generalised neuro- pathic process, a peripheral neuropathy or mononeuritis multiplex would usually also include signs or symptoms in the legs. Proximal median nerve compression can occur at the level of either the pronator teres, most often due to nerve entrapment between the two heads of the muscle, or the brachial plexus, due to an inflammatory process, trauma or mass lesions. It is important to identify these patients so that unnecessary surgery can be avoided. Painful numb hands Clinical focus Marion A Simpson MB ChB(Hons), MRCP(UK), Neurology Registrar 1 Bruce Day MB BS, FRACP, Neurologist and Neurophysiologist, 1 and Senior Lecturer 2 1 The Alfred Hospital, Melbourne, VIC. 2 Monash University, Melbourne, VIC. [email protected] MJA 2011; 195: 388–391 doi: 10.5694/mja11.10900 Practical neurology – 2 • Carpal tunnel syndrome, resulting from median nerve compression at the wrist, is a common and often disabling mononeuropathy. • Risk factors include female sex, family history, repetitive hand use, obesity, pregnancy and a variety of medical comorbidities including diabetes mellitus, rheumatoid arthritis, and other connective tissue diseases. • In many cases, an accurate diagnosis can be reached on the basis of clinical history and supportive examination findings alone. • Neurophysiological investigations are essential for confirming the diagnosis, assessing severity and excluding more generalised neuropathies, as well as providing a baseline preoperative index of median nerve function. • Wrist splinting and local corticosteroid injection are effective treatments in the short term, but long-term data are lacking. • Surgical (endoscopic or open) carpal tunnel release is effective and nearly always required to enable a return to work for patients with occupationally induced carpal tunnel syndrome. Summary Series Editors Craig S Anderson MB BS, PhD, FRACP Leo Davies MB BS, MD, FRACP The grading system for recommendations in this article is described in MJA 2011; 195: 328 Previous article in this series “Blurred vision and pain in the eye” in MJA 2011; 195: 329–332
Transcript of The Medical Journal of Australia · randomised controlled trial) in favour of therapeutic...

Clinical focus
MJA 195 (388
Clinical focus
Marion A SimpsonMB ChB(Hons), MRCP(UK),
Neurology Registrar1
Bruce Day MB BS, FRACP, Neurologistand Neurophysiologist,1 and
Senior Lecturer2
1 The Alfred Hospital,Melbourne, VIC.
2 Monash University,Melbourne, VIC.
MJA 2011; 195: 388–391doi: 10.5694/mja11.10900
Series Editors
Craig S Anderson MB BS, PhD, FRACP
Leo Davies MB BS, MD, FRACP
The grading system forrecommendations in
this article is describedin MJA 2011; 195: 328
Previous article in thisseries “Blurred vision
and pain in the eye” inMJA 2011; 195: 329–332
Painful numb handsPractical neurology – 2
7) · 3 October 2011
• Carpal tunnel syndrome, resulting from median nerve compression at the wrist, is a common and often disabling mononeuropathy.
• Risk factors include female sex, family history, repetitive hand use, obesity, pregnancy and a variety of medical comorbidities including diabetes mellitus, rheumatoid arthritis, and other connective tissue diseases.
• In many cases, an accurate diagnosis can be reached on the basis of clinical history and supportive examination findings alone.
• Neurophysiological investigations are essential for confirming the diagnosis, assessing severity and excluding more generalised neuropathies, as well as providing a baseline preoperative index of median nerve function.
• Wrist splinting and local corticosteroid injection are effective treatments in the short term, but long-term data are lacking.
• Surgical (endoscopic or open) carpal tunnel release is effective and nearly always required to enable a return to work for patients with occupationally induced carpal tunnel syndrome.
Summary
Clare’s storyClare is a 54-year-old, right-handed pastry chef who presented with discomfort, numbness and tingling in both hands. Her symptoms had begun insidiously 9 months earlier, initially in the right hand, and had since become bilateral and severe, such that she was having difficulty performing her usual tasks at work. She described intermittent dull aching pain extending from the hands up to the elbows bilaterally, and pins and needles in all of the fingers. The symptoms occurred most commonly at work or while she was driving or holding a phone to talk. They were also waking her from sleep most nights. Shaking her hands provided some relief.
Clare’s past medical history was otherwise unremarkable. Her weight was 85 kg (body mass index, 33 kg/m2); she had gained 20 kg over the past 2 years after giving up ballroom dancing. She had recently been tested for diabetes as part of a routine check-up and was found to have normal glucose tolerance. She remembered her mother having similar symptoms in her hands, but did not recall any diagnosis being made.
On examination, Clare’s hands appeared normal, with no evidence of muscle wasting and no weakness or incoordination. Sensory examination showed a subjective reduction of sensation in the index and middle fingers and thumb of the right hand. Reflexes were present and symmetrical. Prolonged wrist flexion (Phalen test; Box 1) reproduced symptoms of bilateral hand pain and paraesthesiae, but percussion of the median nerves at the wrist (Tinel test; Box 1) did not. The remainder of the neurological examination was normal.
APPROACH TO THE PROBLEM
The clinical history and examination in this case are highlysuggestive of a peripheral nerve disorder. The intermittentparaesthesiae and discomfort in the digits supplied by themedian nerve, together with nocturnal symptoms andrelief provided by shaking, are classical for carpal tunnelsyndrome. Carpal tunnel syndrome is commonly bilateral,although it may be asymmetrical and is usually worst inthe dominant hand.
Many patients present with atypical symptoms. Theymay describe sensory symptoms and pain throughout thewhole hand and forearm (as did Clare), finger swelling orloss of manual dexterity, or they may present with painlessatrophy of the thenar eminence. They may simply com-plain of dropping objects.
Clare had several risk factors for carpal tunnel syn-drome: an occupation involving repetitive use of thehands, female sex, positive family history, and obesity. At-risk occupations are those that involve repetitive wrist
exertion, including factory work and trades such as carpen-try or those involving use of vibrating tools.
DIFFERENTIAL DIAGNOSES
Differential diagnoses of hand numbness and paraesthe-siae that should be considered in addition to carpal tunnelsyndrome are summarised below.
Cervical radiculopathy is usually unilateral, accompaniedby neck pain, and with symptoms provoked by neckmovement, coughing, sneezing and the Valsalva man-oeuvre. Normal results of a clinical neurological examina-tion, with normal power and reflexes, would argue againstthis diagnosis.
Other neuropathies such as a more generalised neuro-pathic process, a peripheral neuropathy or mononeuritismultiplex would usually also include signs or symptoms inthe legs.
Proximal median nerve compression can occur at thelevel of either the pronator teres, most often due to nerveentrapment between the two heads of the muscle, or thebrachial plexus, due to an inflammatory process, trauma ormass lesions. It is important to identify these patients sothat unnecessary surgery can be avoided.

Clinical focus
APPROPRIATE USE OF INVESTIGATIONS
Clinical tests: Several clinical tests, which vary in theirdiagnostic utility,1 can be used in the diagnosis of carpaltunnel syndrome (Box 1). There is wide variation in thereported sensitivity and specificity of these tests: thePhalen test, for example, one of the most commonlyused, has a reported sensitivity of 10%–91% and specifi-city of 33%–86%.1 In general, the Phalen and Tinel testsare the most widely used and are both more specific thansensitive.Neurophysiological investigations: Although an accu-rate diagnosis of carpal tunnel syndrome can be madeclinically in many cases, nerve conduction studies areessential for confirming the diagnosis and assessingseverity.2 A baseline study before operative interventioncan also assist with documenting a successful carpaltunnel release.
Electrodiagnostic tests are also useful for confirming orexcluding an associated generalised neuropathy ormononeuritis multiplex, and for examining potential dif-ferential diagnoses such as cervical radiculopathy.
Results of Clare’s nerve conduction studies are given in Box 2, with important positive findings highlighted. Her median motor nerve conduction study demonstrated a prolonged right median distal motor latency recording at the wrist.
Many neurophysiology laboratories grade severity ofcarpal tunnel syndrome according to a series of definedparameters, which can include the amplitude of the sen-
sory action potential and the distal motor latency. How-ever, criteria vary between laboratories, and there is oftenpoor correlation of symptom severity with neurophysio-logical severity. Thus, severity grading may not be clinicallyuseful and should be interpreted with caution.
Although useful, nerve conduction studies can producefalse negative results in mild cases, or where intermittentischaemia of the median nerve occurs without more pro-longed demyelination.3 A repeat study after an interval ofseveral months can help to identify such cases.Radiological investigations: Ultrasonography and mag-netic resonance imaging (MRI) can be used in the evalua-tion of carpal tunnel syndrome, to examine the dimensionsof the median nerve at various points along its course andto detect macroscopic compression. However, commonlydue to resource constraints with MRI and operatordependence with ultrasound, neither test is used in routineclinical practice at present.3
Clare’s likely diagnosis was bilateral (right worse than left) carpal tunnel syndrome, based on her typical symptoms and neurophysiological evidence of bilateral median neuropathy at the wrist. She had no evidence of an underlying systemic disorder such as rheumatoid arthritis or endocrinopathy. Her manual occupation and recent weight gain were predisposing or exacerbating factors (Box 3).
Given the persistent and disabling nature of her symptoms and the significant abnormalities demonstrated on her nerve conduction studies, Clare was counselled to pursue treatment.
1 Abnormal findings of clinical tests supporting a diagnosis of carpal tunnel syndrome
389MJA 195 (7) · 3 October 2011

Clinical focus
MJA 195 (7) · 3 October 2011390
2 How to interpret Clare’s nerve conduction studies
These tests confirm bilateral median neuropathies at the wrist, as evidenced by the following abnormalities (shown in blue):A. Prolonged right median distal motor latency (DML) recording at the wrist, with normal conduction velocity in the forearm (recorded at elbow), suggesting focal abnormality at or distal to the wrist, rather than a diffuse process affecting the whole median nerve (see graph below). The left median DML at the wrist is just within normal limits.B. Significant latency difference (� 1.0 ms) on the left lumbrical median versus ulnar study, performed over the same distance for each nerve, suggesting abnormality affecting only the distal median nerve rather than a diffuse neuropathy.C. Absent right median palmar potential — this has no localising value but does suggest median nerve abnormality.D. Significant latency difference (� 0.4 ms) on the left median versus ulnar palmar mixed nerve study, and bilateral median versus radial digit sensory studies, suggesting abnormality affecting only the median nerve.E. Reduction in right median digit sensory action potential amplitude, suggesting more severe abnormality on this side, consistent with the patient’s right hand dominance and initially right-sided symptoms.
Median motor nerve conduction study
Nerve and site Latency (ms) Amplitude (mV)Velocity (m/s)
(RR, > 48)
Right median — abductor pollicis brevis
Wrist (A) 7.1 (RR, < 4.5) 6.8 (RR, > 5)
Elbow 9.1 6.6 51.4
Left median — abductor pollicis brevis
Wrist 4.5 10.2
Elbow 8.1 9.8 59.3
Left carpal tunnel — lumbrical (B)
Median wrist 5.2 2.0
Ulnar wrist 3.5 5.9
Median sensory nerve conduction study (recording site: wrist)
Nerve and site Latency (ms) Amplitude (μV)Velocity (m/s)
(RR, > 48)
Right median palmar
Median palm (C) nr nr
Left median palmar
Median palm (D) 2.1 3.9 35.7
Ulnar palm 1.7 2.0 54.9
Right carpal tunnel — digits
Ulnar digit V 2.0 4.5 50.0
Median digit II (D, E) 4.4 1.7 (RR, � 6) 29.5
Median digit I (D, E) 3.6 2.5 (RR, � 6) 27.8
Radial digit I 1.8 5.5 55.6
Left carpal tunnel — digits
Ulnar digit V 1.8 4.7 61.1
Median digit II (D) 3.1 12.3 39.3
Median digit I (D) 3.0 6.8 30.5
Radial digit I 1.5 6.0 60.0
RR = reference range. nr =not recorded.
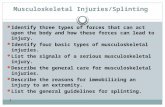
Nerve conduction studies for median motor nerve: normal and abnormal (Clare’s)
These studies were recorded at the abductor pollicis brevis, from stimulation at the wrist (top row) and elbow (bottom row). The number "1" indicates distal motor latency, which is 3.7 ms at the wrist in the normal study and 7.1 ms in Clare's study (RR, < 4.5 ms). ◆
MANAGEMENT
Conservative management
Several non-surgical treatments for carpal tunnel syn-drome have been advocated, including rest, wrist splintingand medications (non-steroidal anti-inflammatory agents,diuretics, pyridoxine, and oral or intracarpal corticoster-oids). Wrist splinting is the mainstay of conservative man-agement. Splints worn at night, which keep the wrist in aneutral position and reduce nerve trauma due to flexion orextension during sleep, are often very effective for reducingwaking caused by nocturnal symptoms in someone whohas had a transient exacerbation after unusual activity (eg,performing home repairs) or during pregnancy.
Two Cochrane reviews have evaluated non-surgicaltreatments for carpal tunnel syndrome (Grade A evi-dence).5,6 One review (12 trials, 671 patients) found localcorticosteroid injections in the region of the carpal tunnelto be more effective than placebo at 1 month (relative risk,2.58; 95% CI, 1.72–3.87), and relative to oral steroids at 3months, with no benefit shown for multiple injectionsover single injections.5 The other review (24 trials, 884patients) found moderate evidence (from more than onerandomised controlled trial) of short-term benefits (up to3 months) from oral steroids, typically doses of 10–20 mgof prednisolone per day, and limited evidence (from onerandomised controlled trial) in favour of therapeutic ultra-sound, splinting and carpal bone mobilisation, whichinvolves physiotherapy-based techniques and stretchingto “move” the bones and ligaments of the wrist.6 Fewtrials have examined long-term outcomes of non-surgicaltreatments.
Surgical management
Surgery for carpal tunnel syndrome may be performed byhand surgeons, orthopaedic surgeons, plastic surgeons orneurosurgeons. Two Cochrane reviews have evaluated sur-gical treatments of carpal tunnel syndrome (Grade Aevidence). One review (four trials, 317 patients) demon-strated a clear benefit of surgery over splinting overall,although there was insufficient evidence regarding theeffect of surgical treatment in the subgroup of milder casesor its relative efficacy over local steroid injection.7 Thesecond review (33 trials, total number of patients notreported) compared endoscopic with open carpal tunnelrelease, and demonstrated equivalence in short-term andlong-term outcomes between these techniques.8
Endoscopic decompression probably shortens the recov-ery period in uncomplicated carpal tunnel syndrome byabout 6 days from an average of around 4 weeks,8 but it isnot recommended in complicated cases where there iswrist deformity from arthritis or old fractures.
Prognosis after surgery can be difficult to predict, but aworse outcome is associated with longer duration of symp-toms (> 6 months), older age, preoperative thenar wastingand poor response to local corticosteroid injection.9 Surgi-cal failure has been associated with incomplete decom-pression of the carpal tunnel (when the incision has notbeen extended far enough into the palm). Horizontalincisions along the line of the wrist crease have been

Clinical focus
abandoned because of a high failure rate and postoperativedysaesthesiae from severing the small palmar cutaneousbranch of the median nerve.
Occupationally induced carpal tunnel syndrome nearlyalways requires surgical decompression to enable a returnto work. We usually advise those requiring surgery toanticipate being off work for 1 month. Usually, the symp-toms are considerably if not completely better almostimmediately after surgery, and patients can use their handsto perform their usual domestic tasks by the end of the firstweek. A return to heavy manual labour generally takesanother 2–3 weeks. We also advise operating on one handat a time, starting with the most symptomatic. Somesurgeons recommend having surgery on both hands at thesame time, but this approach requires the help of anunderstanding partner for toileting and other activities ofdaily living in the postoperative period.
Clare trialled wrist splinting for 1 month, but derived no benefit and was referred to a hand surgeon for carpal tunnel release. She underwent endoscopic release of her right carpal tunnel, with a good immediate result. She returned 3 months later to have the left hand treated, again with good relief of her symptoms. Clare successfully returned to work between the two procedures, performing light duties that involved minimal repetitive wrist movement, such as taking orders and answering phones rather than working on the production line, and returned to her full occupational duties 4 weeks after the second procedure. She did not require any further follow-up.
Competing interests: No relevant disclosures.
Provenance: Commissioned; externally peer reviewed.
1 D’Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal tunnel syndrome? JAMA 2000; 283: 3110-3117.
2 Jablecki CK, Andary MT, Floeter MK, et al. Practice parameter: electrodiagnostic studies in carpal tunnel syndrome. Report of the American Association of Electrodiagnostic Medicine, American Academy of Neurology, and the American Academy of Physical Medicine and Rehabilitation. Neurology 2002; 58: 1589-1592.
3 Hui ACF, Wong S, Griffith J. Carpal tunnel syndrome [review]. Pract Neurol 2005; 5: 210-217.
4 Bland JD, Rudolfer SM. Clinical surveillance of carpal tunnel syndrome in two areas of the United Kingdom, 1991–2001. J Neurol Neurosurg Psychiatry 2003; 74: 1674-1679.
5 Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database Syst Rev 2002; (4): CD001554.
6 O’Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome. Cochrane Database Syst Rev 2003; (1): CD003219.
7 Verdugo RJ, Salinas RA, Castillo JL, Cea JG. Surgical versus non-surgical treatment of carpal tunnel syndrome. Cochrane Database Syst Rev 2008; (4): CD001552.
8 Scholten RJPM, Mink van der Molen A, Uitdehaag BMJ, et al. Surgical treatment options for carpal tunnel syndrome. Cochrane Database Syst Rev 2007; (4): CD003905.
9 Katz JN, Losina E, Amick BC. Predictors of outcomes of carpal tunnel release. Arthritis Rheum 2001; 44: 1184-1193. ❏
FINAL DIAGNOSIS
Bilateral (right worse than left) carpal tunnel syndrome
3 Pathophysiology of carpal tunnel syndrome
Carpal tunnel syndrome is the most common of the entrapment neuropathies, with a study in the United Kingdom finding an estimated annual incidence of 120 per 100 000 in women and 60 per 100 000 in men.4 It is also a disabling condition; occupation-associated carpal tunnel syndrome reportedly accounts for more work days lost than any other work-related injury or illness, with a median duration off work of 32 days.3
The carpal tunnel is formed by the carpal bones on the dorsal side and the flexor retinaculum on the palmar aspect. It contains the median nerve, together with the flexor tendons to the flexor digitorum profundus, flexor digitorum superficialis and flexor pollicis longus muscles. The size of the carpal tunnel varies with movement: wrist flexion causes the flexor retinaculum to move closer to the radius, and decreases its size. Extreme extension can also reduce the size of the carpal tunnel by moving the lunate bone towards the interior of the tunnel.
The most likely pathophysiology of carpal tunnel syndrome is compression of the median nerve in the narrow carpal tunnel, either by surrounding tissue or raised interstitial fluid pressure. However, the absolute size of the carpal tunnel has little bearing on the risk of developing symptoms.
Systemic conditions associated with carpal tunnel syndrome include diabetes mellitus, pregnancy, obesity, rheumatoid arthritis, other connective tissue diseases, hypothyroidism, amyloidosis and acromegaly.
Symptoms of carpal tunnel syndrome may be transient (eg, during pregnancy) or mild and non-disabling. The mechanism of pregnancy-related carpal tunnel syndrome is believed to be related to increased fluid in tissues. It most often resolves after the infant's birth but can predict a higher risk of recurrent symptoms in later life. The mechanism by which obesity produces carpal tunnel syndrome is unknown. Weight loss has not been proven to relieve or resolve symptoms. ◆
FACT OR FICTION?
FACT: It is true that asymptomatic median neuropathy at the wrist, as an incidental finding during neurophysiological studies, is very common, particularly in patients with other neuropathies and arthritis of the hands. Such patients may also have wrist and joint pain.
FICTION: It is not true that all median neuropathy is carpal tunnel syndrome. Unless there is a clinical correlation showing that the neuropathy is due to median nerve compression (and carpal tunnel syndrome), patients are unlikely to respond to carpal tunnel release. Patients with severe median neuropathy, where the nerve is badly damaged and minimally functional, may no longer report symptoms and also may not benefit from surgery. ◆
391MJA 195 (7) · 3 October 2011