
Splinting in Neurology - Tuckey
37
Wessex ACPIN Wessex ACPIN Spasticity Spasticity Presentation 2009. Presentation 2009. © © Jo Jo Tuckey Tuckey Splinting in Neurology Splinting in Neurology Jo Jo Tuckey Tuckey MSc MCSP MSc MCSP
-
Upload
raluca-andreea -
Category
Documents
-
view
29 -
download
0
description
splinting
Transcript of Splinting in Neurology - Tuckey

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting in NeurologySplinting in Neurology
Jo Jo TuckeyTuckey MSc MCSPMSc MCSP

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting in NeurologySplinting in Neurology
When should splinting be considered?When should splinting be considered?How to choose the most appropriate splint How to choose the most appropriate splint or position for splinting.or position for splinting.Practicalities of providing a splinting Practicalities of providing a splinting regime.regime.Outcome measures for determining effect.Outcome measures for determining effect.What is the evidence.What is the evidence.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
DefinitionDefinition
““Splints and casts are external devices Splints and casts are external devices designed to apply, distribute or remove designed to apply, distribute or remove forces to or from the body in a controlled forces to or from the body in a controlled manner to perform one or both basic manner to perform one or both basic functions of control of body motion and functions of control of body motion and alteration or prevention in the shape of alteration or prevention in the shape of body tissue.body tissue.””
Rose 1986Rose 1986
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
1. When should splinting be 1. When should splinting be considered?considered?
Splints can be considered for any of the Splints can be considered for any of the following reasons:following reasons:
To maintain range of movement.To maintain range of movement.To regain range of movement.To regain range of movement.For functionFor function

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
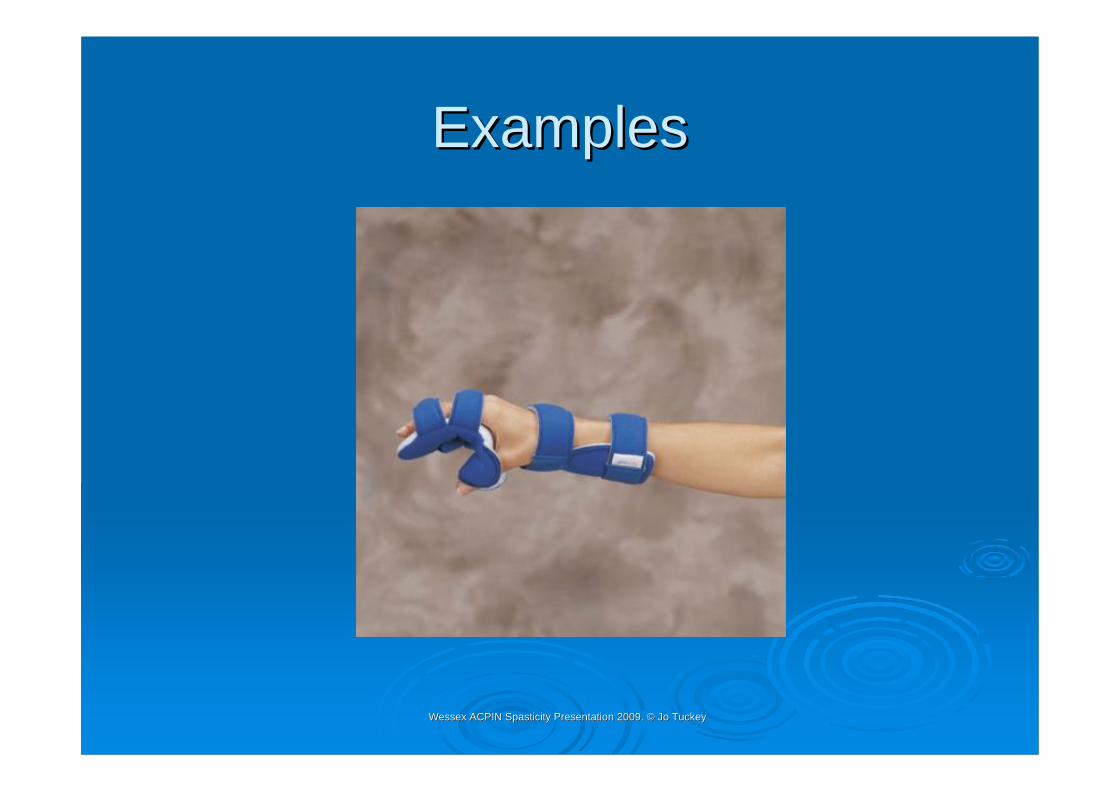
ExamplesExamples
Edwards (2002)
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
ExamplesExamples

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
ExamplesExamples
Edwards (2002)

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
ExamplesExamples
So what does the splint actually do to So what does the splint actually do to maintain or regain ROM?maintain or regain ROM?
Muscles and soft tissues constantly held in a Muscles and soft tissues constantly held in a lengthened or shortened position will adapt to lengthened or shortened position will adapt to that position and become longer or shorter.that position and become longer or shorter.The splint either prevents this occurring in The splint either prevents this occurring in ‘‘at at riskrisk’’ muscle groups or re alters the length by muscle groups or re alters the length by providing a prolonged low load stretch to the providing a prolonged low load stretch to the shortened muscles.shortened muscles.
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Moseley (1993)Moseley (1993) -- 19 HI subjects. 19 HI subjects. CastedCastedfor 7 days. Improvement seen of between for 7 days. Improvement seen of between 33--36 degrees of passive ankle 36 degrees of passive ankle dorsiflexiondorsiflexionin 28/32 limbs. Statistically significant.in 28/32 limbs. Statistically significant.
Moseley (1997)Moseley (1997) -- Similar study. 9 HI Similar study. 9 HI subjects. Methodology tighter. Same subjects. Methodology tighter. Same result.result.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Moseley et al 2008Moseley et al 2008
Serial casting versus positioning for the Serial casting versus positioning for the treatment of elbow contractures in adults treatment of elbow contractures in adults with traumatic brain injury: a randomised with traumatic brain injury: a randomised controlled trialcontrolled trial

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Moseley et al 2008Moseley et al 200826 Subjects26 SubjectsSustained TBISustained TBIElbow contracture of at least 15Elbow contracture of at least 15˚̊Treatment group casts applied for 2 weeks, Treatment group casts applied for 2 weeks, cast changed after 7 days cast changed after 7 days Positioning group had passive stretch applied Positioning group had passive stretch applied to the elbow flexors for 1 hour a dayto the elbow flexors for 1 hour a day
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Moseley et al 2008Moseley et al 2008Results greater reductions in elbow flexion Results greater reductions in elbow flexion contracture with serial casting by an average contracture with serial casting by an average of 22of 22˚̊..Results not maintained. Diminished by half Results not maintained. Diminished by half one day post intervention and completely one day post intervention and completely disappeared at 4 weeks follow up.disappeared at 4 weeks follow up.
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
ExamplesExamples
Edwards (2002)
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
ExamplesExamples
Edwards (2002)

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
2. Options 2. Options –– How to choose the most How to choose the most appropriate splint / position for splintingappropriate splint / position for splinting
It depends upon what you are wanting to It depends upon what you are wanting to achieve.achieve.
On deciding the most appropriate splint On deciding the most appropriate splint also depends upon:also depends upon:
Knowledge and skills of the treating therapistKnowledge and skills of the treating therapistResources availableResources available

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
How to choose the most appropriate splintHow to choose the most appropriate splint
You should only make a splint using the You should only make a splint using the material you are trained to use.material you are trained to use.A custom made splint may be equally as A custom made splint may be equally as effective and might be more cost effective. effective and might be more cost effective. NB politics / budgetsNB politics / budgetsPotential problems Potential problems Resources available for provision of Resources available for provision of splinting materialssplinting materials
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
How to choose the most appropriate splintHow to choose the most appropriate splint
Whether we like it or not, choosing the Whether we like it or not, choosing the most appropriate splint means:most appropriate splint means:
Looking at materials or products you have Looking at materials or products you have available and the skills you have within your available and the skills you have within your team.team.Asking, Asking, ‘‘Will it do the job?Will it do the job?’’
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
How to choose the most appropriate splintHow to choose the most appropriate splint
Removable versus non removableRemovable versus non removableNB Problems of pressureNB Problems of pressure
Advantages of removable splints:Advantages of removable splints:Cut them off from the startCut them off from the startDaily checking / washing of skinDaily checking / washing of skinCan monitor effectCan monitor effectCan still get Can still get ““24 hr24 hr”” effect if bandage back on.effect if bandage back on.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Timing of splintsTiming of splintsPohl et al (2002)Pohl et al (2002)105 brain injured patients.105 brain injured patients.Compared 5Compared 5--7 day casting interval with 17 day casting interval with 1--4 days. 4 days. ResultsResults Improvement seen in all patients Improvement seen in all patients still present after 1 month. 1still present after 1 month. 1--4 days 4 days considered superior as reduced considered superior as reduced complications & discontinuation rates.complications & discontinuation rates.
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
The most appropriate position for splintingThe most appropriate position for splinting
Need to consider this according to the type Need to consider this according to the type of splint being made:of splint being made:
BackslabBackslabIncreasing ROMIncreasing ROMMaintaining ROMMaintaining ROM
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
3. Practicalities of a splinting regime3. Practicalities of a splinting regime
Splints need to be put on properly and taken off.Splints need to be put on properly and taken off.Problems need to be identified and action taken Problems need to be identified and action taken if found if found egeg pressure areas.pressure areas.Decisions need to be made as to the Decisions need to be made as to the effectiveness of the splint and ongoing need.effectiveness of the splint and ongoing need.If you made or supplied it its your responsibility If you made or supplied it its your responsibility to put in place and document an appropriate to put in place and document an appropriate regime regime SO, BE REALISTIC!SO, BE REALISTIC!
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
3. Outcome measures3. Outcome measures
Changing ROM is not enough.Changing ROM is not enough.Ask, what is that changed ROM required Ask, what is that changed ROM required for?for?Clinical examplesClinical examplesegeg ROM at knees for standing or to be ROM at knees for standing or to be seated?seated?Hands that can function or for hygiene?Hands that can function or for hygiene?

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
4. The evidence 4. The evidence –– what does the literature what does the literature say?say?
Review paper:Review paper:
MortensonMortenson et al (2003)et al (2003) The use of casts The use of casts in the management of joint mobility and in the management of joint mobility and hypertonia following brain injury in adults: hypertonia following brain injury in adults: A systematic reviewA systematic review

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
AimAim
To report on best practice for the use of To report on best practice for the use of casting in brain injury rehabilitation.casting in brain injury rehabilitation.
Only 13 articles fulfilled the criteria.Only 13 articles fulfilled the criteria.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
3 categories emerged re: effect of3 categories emerged re: effect ofcasting:casting:
1.Reduction of spasticity1.Reduction of spasticity –– only 5/12 only 5/12 measured properties of spasticitymeasured properties of spasticity
Awarded grade CAwarded grade C

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
2. Passive ROM2. Passive ROM10 studies measured this and in all 10 studies measured this and in all improvements were seen except 1 (but it improvements were seen except 1 (but it was not the first aim)was not the first aim)
Awarded grade BAwarded grade B

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
3. Function3. Function““Trends regarding the effect of casting on Trends regarding the effect of casting on ‘‘functionfunction’’ could not be identified from the could not be identified from the inconsistent results identifiedinconsistent results identified””
No grade level of recommendation givenNo grade level of recommendation given
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
Therefore only improvement / prevention Therefore only improvement / prevention of loss of ROM suggested as having of loss of ROM suggested as having
sufficient evidence to support use of casts sufficient evidence to support use of casts as best practice.as best practice.
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
The National Clinical Guidelines for Stroke The National Clinical Guidelines for Stroke 2008 state:2008 state:
If stretching alone does not control If stretching alone does not control contractures, serial casting around a joint contractures, serial casting around a joint should be considered as a treatment for should be considered as a treatment for reducing contractures.reducing contractures.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
The National Clinical Guidelines for Stroke The National Clinical Guidelines for Stroke 2008 state:2008 state:
Inflatable arm splints enveloping the hand, Inflatable arm splints enveloping the hand, forearm and elbow, and resting wrist and forearm and elbow, and resting wrist and hand splints should not be used routinely.hand splints should not be used routinely.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
LanninLannin et al 2003et al 200328 subjects28 subjectsInclusion criteria Inclusion criteria –– single stroke / BI leading to single stroke / BI leading to hemiparesishemiparesis no more than 6 months beforeno more than 6 months beforeUnable to actively extend wristUnable to actively extend wristRx group wore a functional resting hand splint Rx group wore a functional resting hand splint for up to 12 hours a nightfor up to 12 hours a nightBoth Rx and control group had x2 / day 30 Both Rx and control group had x2 / day 30 min stretches applied to handsmin stretches applied to hands

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
LanninLannin et al 2003et al 2003ResultResult
No difference between groupsNo difference between groups
BUTBUTUnable to conclude the effect of hand Unable to conclude the effect of hand splints alone as all subjects additionally splints alone as all subjects additionally received stretchesreceived stretches
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
LanninLannin 20032003Is hand splinting effective for adults following Is hand splinting effective for adults following stroke? A systematic review and stroke? A systematic review and methodological critique of published research.methodological critique of published research.
ConclusionConclusionThere is insufficient evidence to support or There is insufficient evidence to support or refute effectiveness of hand splinting following refute effectiveness of hand splinting following stroke.stroke.

Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiterature
LanninLannin et al 2007et al 200763 subjects63 subjectsAll within 8 weeks of having strokeAll within 8 weeks of having strokeNo active wrist extensionNo active wrist extension3 groups:3 groups:Routine therapy (no stretches) plus splint in neutralRoutine therapy (no stretches) plus splint in neutralRoutine therapy (no stretches) plus splint in extensionRoutine therapy (no stretches) plus splint in extensionRoutine therapy ( no stretches) Routine therapy ( no stretches) ieie control groupcontrol group
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting Splinting -- LiteratureLiteratureLanninLannin 20072007ResultResultThere was no significant difference betweenThere was no significant difference betweenthe groupsthe groups
ConclusionConclusionThese findings suggest that the practice of routineThese findings suggest that the practice of routinewrist splinting soon after stroke should bewrist splinting soon after stroke should bediscontinueddiscontinued
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting the wrist and handSplinting the wrist and hand
How should these results accurately How should these results accurately inform clinical practice?inform clinical practice?
How can these results be misinterpreted How can these results be misinterpreted and impact upon clinical practice?and impact upon clinical practice?
Wessex ACPIN Wessex ACPIN SpasticitySpasticity Presentation 2009. Presentation 2009. ©© Jo Jo TuckeyTuckey
Splinting in NeurologySplinting in Neurology
And finallyAnd finally……
ACPIN splinting guidelines.ACPIN splinting guidelines.


















