THE LONG-TERM OUTCOME OF FROZEN SHOULDER
78
THE LONG-TERM OUTCOME OF FROZEN SHOULDER HEIDI VASTAMÄKI Faculty of Medicine, University of Helsinki, Finland ORTON Orthopaedic Hospital and ORTON Research Institute, ORTON Foundation, Helsinki, Finland ACADEMIC DISSERTATION Esitetään Helsingin yliopiston lääketieteellisen tiedekunnan suostumuksella julkisesti tarkastettavaksi Invalidisäätiö ORTONin auditoriumissa toukokuun 29. päivänä 2015 kello 12. Academic dissertation to be publicly discussed, with the permission of the Medical Faculty of the University of Helsinki, in the auditorium of the ORTON Foundation, Tenholantie 10, Helsinki, on Friday 29 th May, 2015, at 12 noon. Helsinki 2015
Transcript of THE LONG-TERM OUTCOME OF FROZEN SHOULDER
THE LONG-TERM OUTCOME
OF FROZEN SHOULDER
HEIDI VASTAMÄKI
Faculty of Medicine, University of Helsinki, Finland
ORTON Orthopaedic Hospital and ORTON Research Institute,
ORTON Foundation, Helsinki, Finland
ACADEMIC DISSERTATION
Esitetään Helsingin yliopiston lääketieteellisen tiedekunnan suostumuksella julkisesti tarkastettavaksi Invalidisäätiö ORTONin auditoriumissa toukokuun 29. päivänä 2015 kello 12.
Academic dissertation to be publicly discussed, with the permission of the Medical Faculty of the University of Helsinki, in the auditorium of the ORTON Foundation, Tenholantie 10,
Helsinki, on Friday 29th May, 2015, at 12 noon.
Helsinki 2015
Author`s address: Heidi Vastamäki, M.D.
Research Institute ORTON, ORTON Foundation,
Tenholantie 10, 00280 Helsinki, Finland
and Turku University Hospital, Turku, Finland
Supervised by: Docent Martti Vastamäki, M.D., Ph.D.
Research Institute ORTON, ORTON Foundation
and University of Helsinki, Helsinki, Finland
Reviewed by: Docent Janne Lehtinen, M.D., Ph.D.
Department of Orthopaedics, Hatanpää Hospital,
and University of Tampere, Tampere, Finland
and
Docent Ville Äärimaa, M.D., Ph.D.
Department of Orthopaedics and Traumatology,
Turku University Hospital and University of Turku,
Turku, Finland
Opponent: Professor Lars Adolfsson
University of Linköping, Linköping, Sweden
ISBN: 978-952-9657-79-7 (paperback)
ISBN: 978-952-9657-80-3 (pdf)
ISSN: 1455-1330
Yliopistopaino Unigrafia, Helsinki 2015
http://ethesis.helsinki.fi

”It’s always about the patient. Always.”
Sumant Krishnan, MD, orthopedic surgeon,
in Dallas 2008
With love,
to my parents and Victoria
5
ABSTRACT
Vastamäki, Heidi Anita
The long-term outcome of frozen shoulder
Helsinki: University of Helsinki, 2015, 77 p.
Publications of the ORTON Research Institute, A:39
ISSN 1455-1330
ISBN 978-952-9657-79-7 (paperback)
Dissertation
The purpose of the current study was to assess and report the long-term outcome of frozen shoulder.
The 234 patients with 257 frozen shoulders were clinically followed up for a mean 9.7 years (range,
2-30). The study includes five peer-reviewed articles. The specific aims of this project were to
study: 1) the long-term outcome of the natural course of idiopathic frozen shoulder, 2) the very
long-term outcome of manipulation under anesthesia (MUA), 3) the incidence and long-term
outcome of postoperative frozen shoulder, 4) any influence of timing on the outcome of MUA, and
5) the long-term outcome of diabetic frozen shoulder.
In general, patients with frozen shoulder recovered spontaneously over a mean duration of 15
months. After 9 year follow-up, 94% of shoulders showed a range of motion (ROM) similar to that
of the contralateral, non-affected shoulder; 51% were totally pain-free, and 43% had pain 3/10 on
the Visual Analogue Scale (VAS). In the long-term follow-up, diabetic patients’ shoulder ROM
remained inferior to that of non-diabetic individuals. However, diabetic individuals’ frozen
shoulders recovered to the patients’ own contralateral level. The very long-term outcome of
manipulation under anesthesia was slightly inferior to the outcome of spontaneous recovery i.e. the
natural course. After a mean 23 years follow-up of MUA, 47% of the shoulders had no pain at all.
Even though ROM deteriorated between the last two follow-ups (7 vs. 23 years after MUA) the
once-manipulated shoulder did reach the ROM level of the contralateral shoulder. Timing of MUA
was statistically significantly associated with the outcome after manipulation of the idiopathic
frozen shoulder. Optimal timing for MUA may be between 6 and 9 months from the beginning of
symptoms. However, this finding may not be clinically significant. Concerning postoperative frozen

6
shoulder after an open rotator cuff repair (RCR), the incidence was 20%. Compared to patients with
no postoperative stiffness in their shoulders, the delay to postoperative healing was 3-6 months. The
external rotation resolved first. One year after the surgery, the abduction and the flexion
corresponded to that of the control patients’ shoulders. Patient age during RCR and the condition of
the biceps tendon were related to the postoperative stiffness.
In conclusion, the long-term outcome of frozen shoulder is good.
Keywords: frozen shoulder, adhesive capsulitis, outcome, long-term, follow-up, diabetic frozen
shoulder, postoperative stiff shoulder, postoperative frozen shoulder, timing, manipulation under
anesthesia

7
TIIVISTELMÄ
Vastamäki, Heidi Anita
The long-term outcome of frozen shoulder
Helsinki: University of Helsinki.
Publications of the ORTON Research Institute, A:39
ISSN 1455-1330
ISBN 978-952-9657-79-7 (paperback)
Summary in Finnish
Dissertation
Jäätynyt olkanivel on työikäisten yleisin ei-traumaattisen, pitkäaikaisen olkakivun ja olkanivelen
liikerajoituksen aiheuttaja. Ihmisen normaalisti liikkuvin nivel jäykistyy niin, että liikkeet etu- ja
sivusuuntiin sekä ulko- ja sisäkiertoon alenevat huomattavasti, jopa lähes kokonaan. Tämä aiheuttaa
suurta haittaa käden ja yläraajan käytölle, kun kättä ei juuri saa nostettua vaakatasoa ylemmäs.
Päivittäinen liikelaajuuden vähenemisen ja kivun aiheuttama haitta potilaalle on suuri, sillä
pienetkin jokapäiväiset toimet käyvät joko vaikeiksi tai mahdottomiksi alkaen syömisestä,
pukeutumisesta ja hygienian hoitamisesta. Taudinkuvalle on ominaista vaikea-asteinen yökipu, joka
saattaa kestää kuukausia. Jäätynyt olkanivel aiheuttaa usein myös työkyvyttömyyttä. Jäätyneen
olkanivelen pitkäaikaisseurannan raportoidut lopputulokset ovat ristiriitaisia. Tämän
väitöskirjatutkimuksen tarkoituksena oli tutkia jäätyneen olkanivelen luonnollisen kulun sekä sen
yleisen hoitomuodon, manipulaatiohoidon, pitkäaikaistuloksia. Lisäksi tutkimuksen tarkoituksena
oli selvittää kiertäjäkalvosimen korjausleikkauksen jälkeisen jäätyneen olkanivelen esiintyvyys ja
pitkäaikaistuloksia. Tämän takautuvan tutkimuksen tulosmuuttujina olivat ensisijaisesti olkanivelen
liikelaajuus ja liikeratojen sekä toiminnan palautuminen ja säilyminen sekä olassa koetun kivun
määrä. Tutkimuksessa käytettiin sekä potilaslähtöisiä, kyselylomakkeisiin perustuvia että
tutkijalähtöisiä, eri testeihin perustuvia sekä radiologisia menetelmiä. Potilastiedostoista kerättiin
tietoja sairauden alkuvaiheista, hoitotoimenpiteistä sekä hoitojen jälkeisistä tapahtumista. Kaikki
väitöskirjaan kuuluvat potilaat on jälkitutkittu kliinisesti.
8
Väitöskirjatyössä jälkitutkittiin yhteensä 234 jäätyneen olkanivelen sairastanutta potilasta.
Jäätyneitä olkapäitä oli yhteensä 257. Keskimääräinen seuranta-aika oli 9.7 vuotta (2-30 vuotta).
Väitöskirjatutkimus sisältää viisi osajulkaisua. Tulokset:
I. Jäätyneen olkanivelen luonnollinen kulku
Tutkimuksessa I tutkittiin kliinisesti 51 potilaan 52 jäätynyttä olkaa keskimäärin 9 vuoden seuranta-
ajan jälkeen. Potilaat eivät olleet saaneet vaivaansa muuta hoitoa, kuin särkylääkkeitä, eli kyseessä
on sairauden luonnollinen kulku ilman toimenpiteitä. Vaivan keskimääräinen kesto oli 15 kuukautta,
mutta 14 %:lla potilaista vaiva kesti yli kaksi vuotta. Olkanivelen liikerata parani 94 prosentilla
toisen, eli terveen olan tasolle. Myös potilaat, jotka olivat sairastaneet erityisen hankalan jäätyneen
olkanivelen, paranivat yhtä hyvin. Kontrollipotilaina tutkimuksessa toimivat konservatiivista hoitoa
tai manipulaatiohoitoa saaneet potilaat. Parhaan lopputuloksen saavuttivat luonnollisen kulun
ryhmään kuuluneet potilaat.
II. Jäätyneen olkanivelen anestesiamanipulaation pitkäaikaistulokset
Tutkimuksessa II seurattiin 15 potilaan 16 jäätynyttä olkaa keskimäärin 23 vuotta
anestesiamanipulaation jälkeen seuraavina ajankohtina: 1 kuukausi ennen hoitoa, 0-1 päivää ennen
hoitoa sekä keskimäärin 6 päivää, 3 kuukautta, 7 vuotta ja 23 vuotta hoidon jälkeen. Todettiin, että
liike parani useimmilla toista olkaa vastaavalle tasolle ja kipu hävisi. Pitkän seuranta-ajan aikana
olkanivelen liikerata ehti huonontua mahdollisesti iän vaikutuksesta molemmissa olkapäissä, myös
jäätymättömällä puolella. Voitiin todeta, että jäätyneen olkanivelen anestesiamanipulaation
jälkeinen tulos säilyy vuosikymmeniä.
III. Olkanivelen kiertäjäkalvosimen avoimen korjausleikkauksen jälkeinen jäykistynyt
olkanivel.
Tutkimuksessa III selvitettiin 56 potilaan olkanivelen kiertäjäkalvosimen repeämän avoimen
korjausleikkauksen jälkeen jäätyneen olkanivelen toipuminen keskimäärin 8.7 vuoden kuluttua
leikkauksesta. Avoimen kiertäjäkalvosimen korjausleikkauksen jälkeinen jäykkä olka oli varsin
yleinen esiintyen joka viidennellä potilaalla yhteensä 416 leikatusta olasta. Vaiva hidasti
leikkauksen jälkeistä olan liikkeiden palautumista 3-6 kuukaudella. Liikkeet kuitenkin paranivat 6-
12 kuukauden aikana valtaosalla potilaista vastaamaan ei-jäätyneiden leikkauspotilaiden
9
liikelaajuuksia. Korkeampi leikkauksenaikainen ikä sekä hauislihaksen jänteen eheys liittyivät
lisääntyneeseen leikkauksenjälkeiseen jäätymiseen. Tutkimuspotilaiden tuloksia 6 viikkoa, 3 ja 6
kuukautta sekä 1 vuosi leikkauksen jälkeen verrattiin kontrolliryhmän potilaisiin, joilla ei ollut
kiertäjäkalvosimen leikkauksen jälkeistä jäykistynyttä olkaniveltä. Olkanivelen keskimääräiset
liikeradat potilasryhmissä eivät eronneet enää vuoden kohdalla toisistaan.
IV. Onko anestesiamanipulaation ajankohta yhteydessä hoidon lopputulokseen?
Tutkimuksessa IV seurattiin 57 potilaan 65 manipuloidun jäätyneen olkanivelen tuloksia
keskimäärin 6 vuotta ja pyrittiin selvittämään, onko manipulaation suoritusajankohdalla yhteyttä
hoidon lopputulokseen. Tilastollisessa analyysissä 6-9 kuukauden kuluessa oireiden alusta
suoritettu anestesiamanipulaatio oli yhteydessä parempaan hoidon lopputulokseen kuin muina
ajankohtina suoritettu manipulaatio. Kyseisen ryhmän potilailla oli jälkiseurannassa muita
paremmat flexio-, ulkokierto-, lepokipu- ja Simple Shoulder Test- arvot.
V. Diabeteksen vaikutus jäätyneen olan paranemiseen
Tutkimuksessa V seurattiin 27 diabetespotilaan 29 jäätyneen olkanivelen paranemista keksimäärin
9.7 vuotta. Diabetespotilaiden tuloksia verrattiin 151 diabetesta sairastamattoman potilaan jäätyneen
olkanivelen paranemistuloksiin. Todettiin, että diabetespotilaiden jäätynyt olka paranee muuten
samalla tavoin kuin diabetesta sairastamattomien, mutta olkanivelen liikerata jää huonommaksi.
Havaittiin, että diabetespotilaiden jäätyneen olan liikerata palasi kuitenkin samalle tasolle, kuin
heidän toisen, eli terveen olkansa liikerata.
Tämän väitöskirjatutkimuksen vahvuuksina voidaan pitää erittäin pitkiä seuranta-aikoja sekä sitä,
että kaikki jäätynyt olkanivel -potilaat on jälkitutkittu kliinisesti. Väitöskirja sisältää suurimman
tähän mennessä kliinisesti tutkitun ja julkaistun aineiston jäätyneen olkanivelen luonnollisesta
kulusta ja pisimpään kliinisesti tutkitun ja julkaistun jäätyneen olkanivelen anestesiamanipulaation
tulosseurannan.
Loppupäätelmänä voidaan todeta, että jäätynyt olkanivel paranee spontaanisti ilman hoitoa lähes
kaikilla potilailla. Diabetespotilailla olkanivelen liikerajoitukset jäävät suuremmiksi kuin ei-

10
diabeetikoilla, mutta näin käy myös diabetespotilaiden terveen olan liikeratojen suhteen.
Olkanivelen kiertäjäkalvosimen repeämän avoimen korjausleikkauksen jälkeinen jäätynyt, jäykkä
olkapää on yleinen ilmiö ja viivästyttää olan paranemista usealla kuukaudella, mutta paranee
yleensä runsaan puolen vuoden sisällä.
Avainsanat: jäätynyt olkanivel, pitkäaikaistulokset, seurantatutkimus, lopputulos, luonnollinen
kulku, anestesiamanipulaatio, leikkauksenjälkeinen jäätynyt olkanivel.
11
ABBREVIATIONS
CS Constant-Murley Score
MRI Magnetic resonance imaging
MUA Manipulation under anesthesia
NSAID Non-steroidal anti-inflammatory drug
p-value Statistical significance
RC Rotator cuff
RCR Rotator cuff repair
SST Simple shoulder test
VAS Visual analogue scale
12
FIGURES
FIGURE 1 Anatomy of the shoulder joint 1 19
FIGURE 2 Anatomy of the shoulder joint 2 20
TABLES
TABLE 1. The randomized controlled trials concerning the treatment of frozen shoulder published during the last 10 years. 29-31
TABLE 2. Summary of numbers of patients and shoulders and follow-up times in
Studies I to V 37
TABLE 3. Outcome in range of motion (ROM) in 178 patients
with 198 shoulders, a mean 10 years after idiopathic frozen shoulder. 42
TABLE 4. Function, Constant Score and Simple Shoulder Test and pain on the Visual Analogue Scale in 178 patients with 198 once frozen shoulders mean 10 years after idiopathic frozen shoulder. 42
TABLE 5. Short-, long-, and very long-term range of motion in patients who had undergone manipulation under anesthesia (MUA) for frozen shoulder. Mean values. 45
TABLE 6. Range of motion of affected (once frozen) and unaffected shoulders in diabetic and non-diabetic patients at final follow-up, a mean 10 years after frozen shoulder. 47
TABLE 7. Literature on outcome of the natural course of frozen shoulder. 49
13
LIST OF ORIGINAL PUBLICATIONS
The thesis is based on the following original publications, which are referred to in the text by the
Roman numerals I-V:
I. Vastamäki H, Kettunen J, Vastamäki M. The natural history of idiopathic frozen
shoulder: A 2- to 27-year followup study. Clin Orthop Relat Res 2012;470:1133-1143,
DOI 10.1007/s11999-011-2176-4.
II. Vastamäki H, Vastamäki M. Motion and pain relief remain 23 years after manipulation
under anesthesia for frozen shoulder. Clin Orthop Relat Res (2013) 471:1245-1250 DOI
10.1007/s11999-012-2542-x
III. Vastamäki H, Vastamäki M. Postoperative stiff shoulder after open rotator cuff repair.
A 3- to 20-year follow-up study. Scand J Surg. 2014 Dec;103(4):263-70. doi:
10.1177/1457496913514383. Epub 2014 Apr 2
IV. Vastamäki H, Varjonen L, Vastamäki M. Optimal time for manipulation for frozen
shoulder may be between 6 and 9 months. Scand J Surg. 2015 Jan 26. pii:
1457496914566637. [Epub ahead of print]
V. Vastamäki H, Ristolainen L, Vastamäki M. Range of motion of diabetic frozen
shoulder recovers to the contralateral level. Submitted.
The articles are reprinted with the kind permission of the copyright holders.
14
TABLE OF CONTENTS
ABSTRACT
TIIVISTELMÄ in Finnish
ABBREVIATIONS
LIST OF ORIGINAL PUBLICATIONS
1. INTRODUCTION 16 2. REVIEW OF THE LITERATURE 17 2.1. History 17 2.2. Nomenclature and etymology 17 2.3. Normal shoulder anatomy and function 18 2.4. Etiology, pathogenesis and pathoanatomy in frozen shoulder 20 2.5. Epidemiology 23 2.6. Diagnosis and diagnostic criteria 24 2.7. Differential diagnostics 25 2.8. Scoring and evaluation of shoulder pain and function 26 2.9. Stages of frozen shoulder 27 2.10. Natural course 28 2.11. Treatment modalities 28 2.11.1 Conservative treatment 32
2.11.2 Operative treatment 33 2.12. Cost effectiveness 35 2.13. Postoperative frozen shoulder 35 3 AIMS OF THE PRESENT STUDY 36 4 PATIENTS AND METHODS 37 4.1. The natural course of frozen shoulder 38 4.2. Very long-term outcome after manipulation under anesthesia
for idiopathic frozen shoulder 38 4.3. The outcome of postoperative frozen shoulder
after open rotator cuff repair 39 4.4. Does timing of MUA for frozen shoulder associate with results? 40 4.5. The outcome of diabetic frozen shoulder 41 5. RESULTS 42 5.1. The natural course of frozen shoulder 43 5.2. Very long-term outcome after manipulation under anesthesia
15
for idiopathic frozen shoulder 44 5.3. The outcome of postoperative frozen shoulder
after open rotator cuff repair 45 5.4. Does timing of MUA for frozen shoulder associate with results? 46 5.5. The outcome of diabetic frozen shoulder 47 6. DISCUSSION 49 6.1. The duration of frozen shoulder in natural course 49
6.2. Long-term range of motion and function after frozen shoulder 50
6.3. Pain after frozen shoulder 52
6.4. Outcome of postoperative stiff shoulder after open rotator cuff repair 53 6.5. Does timing of MUA for frozen shoulder associate with outcome? 55
6.6. Limitations of the study 57
6.7. Strengths of the study 58 6.8. Recommendations for future research 59 7. MAIN FINDINGS 60 8. CONCLUSIONS 60
ACKNOWLEDGEMENTS 61
REFERENCES 63
ORIGINAL PUBLICATIONS
16
1. INTRODUCTION
A healthy shoulder is the most mobile joint in the human body. One of the most common causes of
pain and disability of the shoulder is frozen shoulder. It significantly reduces the range of motion in
every direction, thus severely disabling the use of the upper extremity. Frozen shoulder causes
aching pain both at rest and during activity, and especially during nighttime. It often causes inability
to work and features longstanding pain and deteriorated function.
This thesis deals with the long-term outcome of frozen shoulder. The theme for this retrospective
study arose from the possibility to explore a large population of frozen-shoulder patients diagnosed
and treated mainly by a single surgeon with a similar protocol, giving the possibility to evaluate its
long-term outcome. Although over a thousand articles already exist on frozen shoulder, the outcome
still remains controversial (33,34,44,47,51,59,60,63,69,80,82,87,103,147-150,154,159). Only a few
studies concentrate on the natural course (20,63,148,159), outcome in diabetic patients’ frozen
shoulder (30,80,81), effect of timing for one of the most commonly used treatment methods,
manipulation under anesthesia (50,52,136,175), and long-term outcome after manipulation
(49,53,75). These, along with the outcome of postoperative frozen shoulder (118,177,199), were the
main themes for the thesis.
An American surgeon, Ernest Amory Codman, also referred to as the father of shoulder surgery,
claimed that even the most recalcitrant cases of frozen shoulder recover (34). Already in that era, he
believed in monitoring the outcome of his patients and used his so-called “end-result cards” with a
follow-up time of one year. Now, almost one hundred years later, we sought the end results and the
long-term outcome of our unique population of frozen-shoulder patients.
17
2. REVIEW OF THE LITERATURE
2.1. HISTORY
Nearly one and a half centuries have passed since French pathologist and surgeon Simon-
Emmanuel Duplay in 1872 described “pèri-arthrite scapula-humérale” (48). He differentiated this
mobility-restricting condition of the shoulder from osteoarthritis, and suggested manipulation under
anesthesia as a treatment method. Six years later, another French author, Desplats, also wrote on
“peri-arthrite scapulo humerale” (42). James J. Putnam was the first to write about it in English. He
published his article on “The treatment of a form of painful periarthritis of the shoulder” in The
Boston Medical and Surgical Journal in 1882 (142). Among principal symptoms, he listed the
inability to raise the arm above the horizontal level, and spontaneous pain, generally worst at night.
Putnam also found that “any attempt to move the arm at the scapula-humeral articulation, either by
abduction or rotation, causes sharp and severe pain, and is, indeed, nearly or quite impossible.” In
1906, Codman spoke on “subdeltoid bursitis” (32) as did Painter a year later (133), and Klapp in
Europe (88). Codman gave the condition its widely used name “frozen shoulder” (32-34). Robert
Lippman, in 1943, used the same term (97). Julius Neviaser, in 1945, introduced the term “adhesive
capsulitis” and summed up the opinions of previous writers by defining frozen shoulder or adhesive
capsulitis as a separate clinical entity (119). Ever since, researchers have tried to explore this entity,
first in the fifties (41,98,111,114,165), then later were joined by numerous authors
(6,9,10,20,24,30,36,40,44,60,61,63,64,69,78,101,104,112,113,115,121,122,123,125,130,145,146,
148,154,178,186-188,208). Frozen shoulder has often been referred to as a mystery or enigma
(20,22).
2.2. NOMENCLATURE AND ETYMOLOGY
The multiple names and terms introduced to describe this condition have included “frozen shoulder,
adhesive capsulitis, checkrein shoulder, painful stiff shoulder, retractile capsulitis, periarthritis,
adherent subacromial bursitis, and Duplay’s disease” (16,109). In Japan, the term “goju-kata” has
meant “a 50-year-old-shoulder” (170) referring to the age when it usually strikes.
The first term written down was “periarthritis humeroscapularis”. “Peri”- is a prefix meaning
“about”/ “around”; “arthritis” refers to inflammation of a joint. The most used names are frozen
18
shoulder and adhesive capsulitis. The word adhesive is derived from the Latin word
adhaesivus/adhasus meaning, “clinging, tenacious, sticking fast”. Capsulitis is derived from the
Latin word capsula, or the English word “capsule,” which means a “membranous sac or
integument” surrounding the shoulder joint (204), and –“itis” refers to an inflammation.
“Retractile” means withdrawn, being drawn back or in, as with the upper extremity held close to the
body.
Criticism has arisen towards many of the names. It is obvious that no arthritis is involved and that
the primary cause is not in the subacromial bursae (23,24). Even the widely used name “frozen
shoulder” has its opponents (21), for the shoulder during the disease is neither cold nor icy. The
term “frozen” refers more to the rigidity and stiffness.
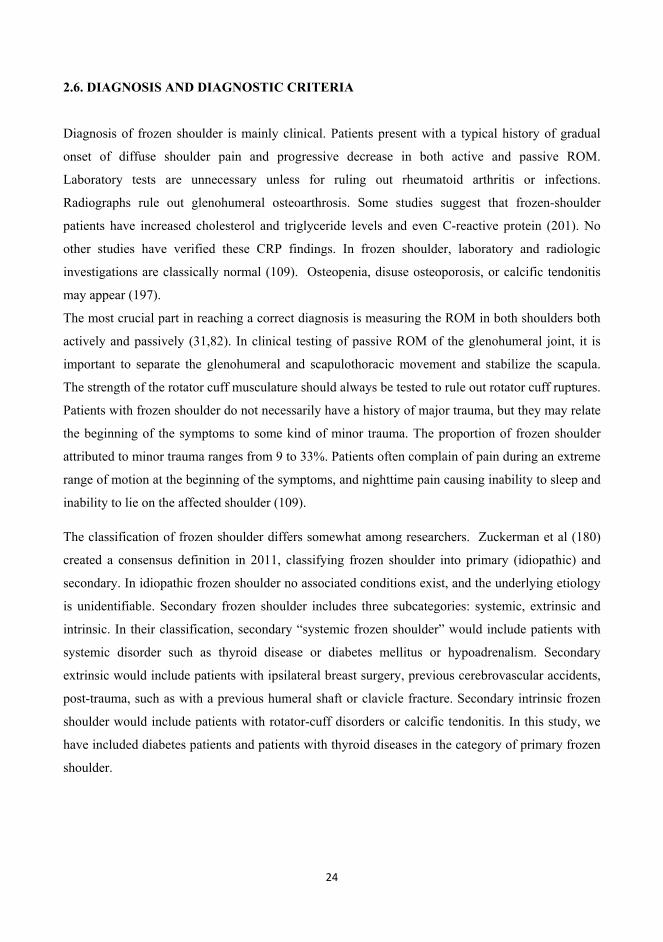
2.3. NORMAL SHOULDER ANATOMY AND FUNCTION
The shoulder is a synovial joint, meaning that the articulating bones, the head of the humerus and
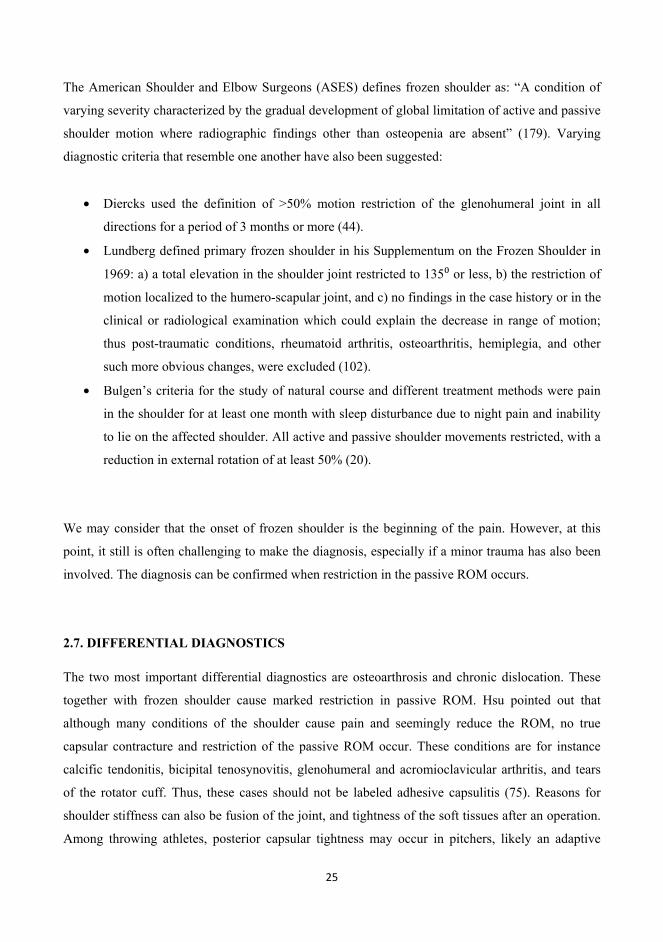
the glenoid (Figure 1), are separated by a fluid-containing joint cavity. The joint capsule (capsula
articularis) (Figure 2) is a sack-type formation around the joint, reaching from the glenoid to the
head of the humerus. The inner surface of the joint capsule is the collagenous synovium, the
synovial membrane that produces and secretes the synovia, a viscous liquid that lubricates the
movements of the joint, the articular surfaces (26). The outer surface of the joint capsule is
membrane fibrosa/stratum fibrosum, a collagenous membrane. The capsule completely covers the
joint, but is loose. Normally, the surface area of the capsule is nearly double that of the humeral
head (201). The sleeve-type stabilizers of the glenohumeral joint are the rotator cuff musculature,
the capsuloligamentous complex, and the long head of the biceps tendon. The rotator cuff
surrounding the glenohumeral joint is composed of four muscle tendons, the supraspinatus,
infraspinatus, subscapularis and teres minor that surround the glenohumeral joint anteriorly,
superiorly, and posteriorly. The capsule, the coracohumeral ligament, and the superior, middle, and
inferior glenohumeral ligaments comprise the capsuloligamentous complex that also surrounds the
glenohumeral joint. The inferior glenohumeral ligament forms a lax double-fold of the capsule
forming the inferior or axillary recess (201). The long head of the biceps tendon lies under the
coracohumeral ligament (82). The rotator interval is a tissue bridge between the anterior
supraspinatus edge and the upper subscapularis border, with the apex located on the biceps sulcus
lateral ridge at the margin of the transverse humeral ligament. It is mostly formed by the superior
glenohumeral ligament and the coracohumeral ligament (84, 134).
19
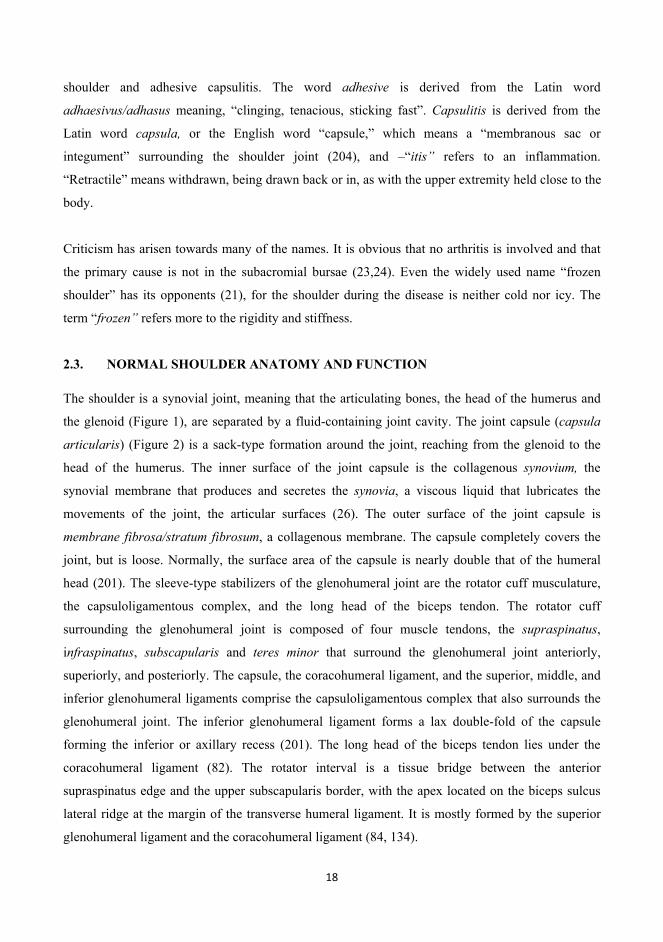
FIGURE 1. Anatomy of the shoulder joint 1.
The whole shoulder girdle complex takes part in the motion of the shoulder (2); glenohumeral joint,
acromioclavicular, sternoclavicular, and scapulothoracic articulations. Scapulothoracic and
glenohumeral movements occur simultaneously at a ratio of 1:2, with most of the elevation
attributed to the glenohumeral joint (201). The abductors include the deltoid, supraspinatus, the long
head of the biceps tendon, but also to some extent the infraspinatus. The serratus anterior and
trapezius may aid this movement by producing some scapular rotation. The infraspinatus is the
strongest external rotator, but also the teres minor and the spinal part of the deltoid perform some
rotation. Internal rotation is mainly carried out by the subscapularis, but also to some extent by
pectoralis major, the long head of the biceps, the clavicular part of the deltoid, the teres major and
also to some degree by the latissimus dorsi (2).
20
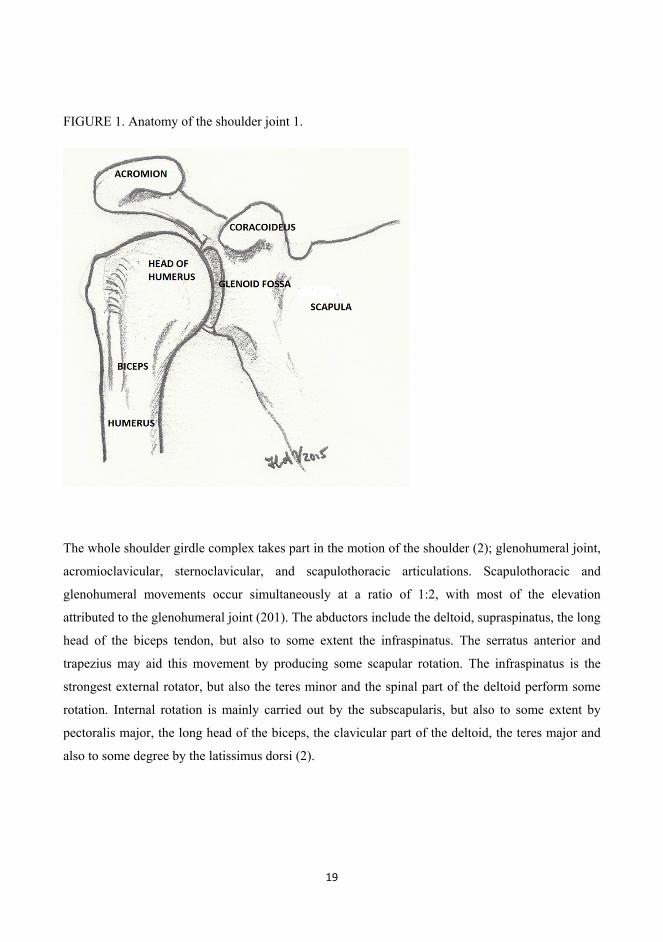
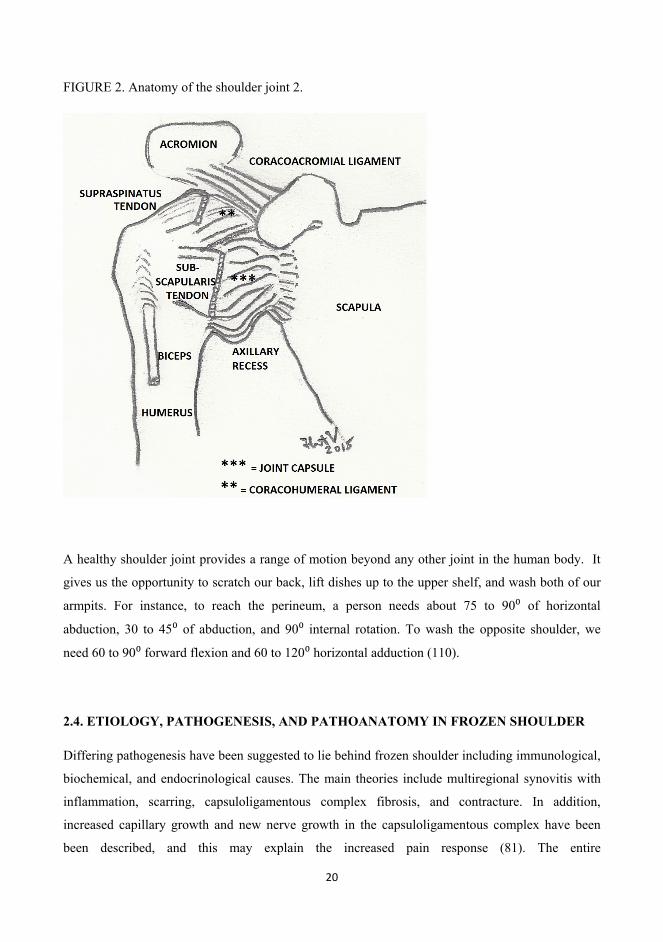
FIGURE 2. Anatomy of the shoulder joint 2.
A healthy shoulder joint provides a range of motion beyond any other joint in the human body. It
gives us the opportunity to scratch our back, lift dishes up to the upper shelf, and wash both of our
armpits. For instance, to reach the perineum, a person needs about 75 to 90 of horizontal
abduction, 30 to 45 of abduction, and 90 internal rotation. To wash the opposite shoulder, we
need 60 to 90 forward flexion and 60 to 120 horizontal adduction (110).
2.4. ETIOLOGY, PATHOGENESIS, AND PATHOANATOMY IN FROZEN SHOULDER
Differing pathogenesis have been suggested to lie behind frozen shoulder including immunological,
biochemical, and endocrinological causes. The main theories include multiregional synovitis with
inflammation, scarring, capsuloligamentous complex fibrosis, and contracture. In addition,
increased capillary growth and new nerve growth in the capsuloligamentous complex have been
been described, and this may explain the increased pain response (81). The entire
21
capsuloligamentous complex may become fibrotic, but specifically the rotator cuff interval and
biceps tendon are involved (206). Hand et al took biopsies from resistant frozen-shoulder patients
from the rotator interval and the coracohumeral ligament (68). They found fibroblasts, proliferating
fibroblasts, and chronic inflammatory cells; mast cells, T cells, B cells and macrophages. They
concluded that “the pathology of frozen shoulder includes a chronic inflammatory response with
fibroblastic proliferation which may be immunomodulated.” Bulgen et al reported frozen shoulder
patients as being significantly more often HLA-B27-positive than were the controls (42% vs. 10%).
Their result may support the theory of immunological pathogenesis (19).
According to Bunker, (24) pathology lies behind the fibrous contracture of the rotator interval and
coracohumeral ligament of the shoulder. First, new blood vessels emerge in the synovial membrane,
especially in the area of the rotator interval. Then, during the stiff stage, the blood-vessel formation
decreases, and a thick white scar evolves within the capsule. This results in capsular contracture.
Frozen shoulder has been associated with many systemic conditions, including diabetes mellitus,
thyroid diseases, and, Dupuytren’s disease (24,160). Bunker also stated that frozen shoulder should
perhaps be classified within the group of diseases termed fibromatoses, which includes Dupuytren’s
disease. Dupuytren is 8.27 times as common in frozen shoulder patients as in the general population
(p<0.001) (24, 168) and occurred in 58% of Bunker’s and 25% of Schaer’s frozen-shoulder
patients. Histologically, the predominant cells are fibroblasts and myofibroblasts which lay down a
dense collagen matrix, mostly of mature type III and type I within the capsule. The tissue is higly
cellular with fibroblasts and contractile myofibroblasts resembling the findings in Dupuytren’s
contracture (23,24). Raykha’s findings (147) support Bunker’s theory of a fibrotic disease
resembling Dupuytren’s contracture. They found that expression of IGF2 and level of -catenin
were significantly higher in frozen-shoulder patients than in patients with rotator cuff tears. In
patients with Dupuytren’s disease, IGF2 and -catenin are also increased (147). Bunker also found
this phenomenon to be related to expression of growth factors, cytokines, and matrix
metalloproteinases in frozen shoulder (25).
Julius Neviaser describes adhesions (119). Within a normal capsule there is a loose axillary fold.
During frozen shoulder, the capsule thickens with inflammatory infiltrate and subsynovial fibrosis.
This obliterates the normal, patulous axillary fold as a result of adhesions and fibrosis of the capsule
itself (141). Others findings are that a contracted glenohumeral joint capsule is not associated with
22
capsular adhesions; some refuse to use the term “adhesions”, however, because these cannot really
be seen (43,140). Thus, the basic pathological changes are said to be thickening of the joint capsule
and its adherence to the head of the humerus (4,155).
The main abnormalities seen in frozen shoulder patients are synovitis in the anterior superior
glenohumeral joint, thickening of the coracohumeral ligament, and periarticular soft-tissue
inflammation in the rotator cuff interval. MRI shows a thicker coracohumeral ligament, obliteration
of the subcoracoid fat triangle and the axillary recess, variable filling of the biceps tendon sheath,
and, surprisingly, no significant thickening of the joint capsule (141). Typical for frozen shoulder
are dense collagen fibers, fibroplasia resembling Dupuytren’s, and also thickening and contracture
of the capsule, especially anteroinferiorly (102,140,152,207).
Some studies comment on the appearance of frozen shoulder inside the shoulder. “Hot spots”
gleaming in a radioisotope scan have been noted (9), or the rotator cuff as being “tender and friable,
rather cooked than frozen”. In the early phase of the disease, there is highly vascular, abnormal
content arising from the subscapularis bursa and spreading to a variable extent across the rotator
interval area. Later on, dense scarring is found in the same area (22). Synovitis is usually found and
then thickening and scarring but no adhesions (157). Andersen et al found, during arthroscopy,
reduced intra-articular volume, an agglutinated inferior recess and diffuse synovitis in all their
frozen-shoulder patients (3). Intra-articularly, first at stage 1, vascular inflammatory synovitis is
evident (202); at stage 2, a predominance of red synovium and early adhesion formation; at stage 3,
pink synovium and more pronounced adhesion formation; but, at stage 4, synovitis is no longer a
predominant feature, and the joint appears white because of the marked capsular adhesions.
In cases of frozen shoulder, the range of motion in the shoulder joint declines both actively and
passively. The scapulohumeral rhythm changes, and the scapula moves excessively in upward
rotation to compensate for the loss of glenohumeral motion (124). Acromion morphology and
frozen shoulder have no reported relationship (150). A frozen shoulder has reduced joint volume.
The normal volume of a shoulder joint is about 10 to15 ml, but with frozen shoulder only some 3 to
4 ml (9, 22).
The term “postoperative frozen shoulder” has been introduced referring to the postsurgical stiffness
after a rotator-cuff repair (106). Stiffness after a fracture has also been called secondary frozen
shoulder (68). Secondary frozen shoulder has been defined as that associated with major trauma,
23
shoulder surgery, cardiovascular disease, and hemiparesis. A discrepancy exists between the extent
of trauma and severity of subsequent frozen shoulder (40). The true etiology of frozen shoulder still
remains unknown and presumably is multifactorial.
2.5. EPIDEMIOLOGY
Incidence of frozen shoulder in the general population is 2% (4,13,24,81,96,176,182). The
cumulative incidence of frozen shoulder is estimated at 2.4 / 1000 population per year, based on a
Dutch general-practice sample (190). A large UK-based primary care study found that frozen
shoulder affected 8.2% of men and 10.1% of women of working age (192). In contrast, based on
one specialist shoulder surgeon’s hospital care experience, frozen shoulder was estimated to affect
only 0.75% of the UK population (23). This inconsistency in estimated prevalence could be
explained by the fact that only the most resistant cases are referred to hospitals (67). Difficulty in
indicating the true incidence of frozen shoulder can be explained by the vague and insidious nature
of the condition; many patients do not seek medical care (75). Frozen-shoulder patients usually are
women in their mid-50s (75, 109). Frozen shoulder does not affect the same shoulder twice (75),
although, at least one recurrence has been reported (28). Bilateral cases constitute 6% to 50%,
some 14% are simultaneously bilateral (201). It has been estimated that the opposite shoulder
becomes affected in 6% to 17% of patients within 5 years (109). Incidence of frozen shoulder
among diabetes patients has been reported to be as high as 10% to 36%, with prevalence being
10.3% to 22.4%. (4,13). The prevalence of diabetes or prediabetes in patients with frozen shoulder
has been estimated to be as high as 71.5% (176). Race does not affect the incidence level (75).
Finland has a population of 5 470 820 (figure of January 10 2014, from Väestörekisterikeskus, the
Finnish population register). Those in their thirties hardly ever have frozen shoulder, unless they
have diabetes. Elderly patients in their seventies and eighties more frequently suffer from rotator-
cuff problems or osteoarthrosis. At the end of 2013, there were 1 486 575 persons in Finland of the
age 50-69 years. An incidence of only 2% would mean 29 731 frozen-shoulder patients. When it
comes to patients with diabetes, Finland has approximately 500 000 (Diabetesbarometria 2010,
Diabetesliitto). Incidence among them by a moderate estimate would be some 10%, amounting to
50 000 frozen-shoulder patients. However, exact numbers are unknown.
24
2.6. DIAGNOSIS AND DIAGNOSTIC CRITERIA
Diagnosis of frozen shoulder is mainly clinical. Patients present with a typical history of gradual
onset of diffuse shoulder pain and progressive decrease in both active and passive ROM.
Laboratory tests are unnecessary unless for ruling out rheumatoid arthritis or infections.
Radiographs rule out glenohumeral osteoarthrosis. Some studies suggest that frozen-shoulder
patients have increased cholesterol and triglyceride levels and even C-reactive protein (201). No
other studies have verified these CRP findings. In frozen shoulder, laboratory and radiologic
investigations are classically normal (109). Osteopenia, disuse osteoporosis, or calcific tendonitis
may appear (197).
The most crucial part in reaching a correct diagnosis is measuring the ROM in both shoulders both
actively and passively (31,82). In clinical testing of passive ROM of the glenohumeral joint, it is
important to separate the glenohumeral and scapulothoracic movement and stabilize the scapula.
The strength of the rotator cuff musculature should always be tested to rule out rotator cuff ruptures.
Patients with frozen shoulder do not necessarily have a history of major trauma, but they may relate
the beginning of the symptoms to some kind of minor trauma. The proportion of frozen shoulder
attributed to minor trauma ranges from 9 to 33%. Patients often complain of pain during an extreme
range of motion at the beginning of the symptoms, and nighttime pain causing inability to sleep and
inability to lie on the affected shoulder (109).
The classification of frozen shoulder differs somewhat among researchers. Zuckerman et al (180)
created a consensus definition in 2011, classifying frozen shoulder into primary (idiopathic) and
secondary. In idiopathic frozen shoulder no associated conditions exist, and the underlying etiology
is unidentifiable. Secondary frozen shoulder includes three subcategories: systemic, extrinsic and
intrinsic. In their classification, secondary “systemic frozen shoulder” would include patients with
systemic disorder such as thyroid disease or diabetes mellitus or hypoadrenalism. Secondary
extrinsic would include patients with ipsilateral breast surgery, previous cerebrovascular accidents,
post-trauma, such as with a previous humeral shaft or clavicle fracture. Secondary intrinsic frozen
shoulder would include patients with rotator-cuff disorders or calcific tendonitis. In this study, we
have included diabetes patients and patients with thyroid diseases in the category of primary frozen
shoulder.
25
The American Shoulder and Elbow Surgeons (ASES) defines frozen shoulder as: “A condition of
varying severity characterized by the gradual development of global limitation of active and passive
shoulder motion where radiographic findings other than osteopenia are absent” (179). Varying
diagnostic criteria that resemble one another have also been suggested:
• Diercks used the definition of >50% motion restriction of the glenohumeral joint in all
directions for a period of 3 months or more (44).
• Lundberg defined primary frozen shoulder in his Supplementum on the Frozen Shoulder in
1969: a) a total elevation in the shoulder joint restricted to 135 or less, b) the restriction of
motion localized to the humero-scapular joint, and c) no findings in the case history or in the
clinical or radiological examination which could explain the decrease in range of motion;
thus post-traumatic conditions, rheumatoid arthritis, osteoarthritis, hemiplegia, and other
such more obvious changes, were excluded (102).
• Bulgen’s criteria for the study of natural course and different treatment methods were pain
in the shoulder for at least one month with sleep disturbance due to night pain and inability
to lie on the affected shoulder. All active and passive shoulder movements restricted, with a
reduction in external rotation of at least 50% (20).
We may consider that the onset of frozen shoulder is the beginning of the pain. However, at this
point, it still is often challenging to make the diagnosis, especially if a minor trauma has also been
involved. The diagnosis can be confirmed when restriction in the passive ROM occurs.
2.7. DIFFERENTIAL DIAGNOSTICS
The two most important differential diagnostics are osteoarthrosis and chronic dislocation. These
together with frozen shoulder cause marked restriction in passive ROM. Hsu pointed out that
although many conditions of the shoulder cause pain and seemingly reduce the ROM, no true
capsular contracture and restriction of the passive ROM occur. These conditions are for instance
calcific tendonitis, bicipital tenosynovitis, glenohumeral and acromioclavicular arthritis, and tears
of the rotator cuff. Thus, these cases should not be labeled adhesive capsulitis (75). Reasons for
shoulder stiffness can also be fusion of the joint, and tightness of the soft tissues after an operation.
Among throwing athletes, posterior capsular tightness may occur in pitchers, likely an adaptive
26
change from the powerful forces created in repetitive pitching. One reason for selective stiffness in
limited external rotation may be that patients have undergone an anterior stabilization operation. In
these cases, the reason for stiffness may be over-tightening (87).
In the very beginning of frozen shoulder, during the first stage, it is often difficult to differentiate it
from other painful conditions such as impingement, because there is as yet no restriction in passive
range of motion. A stiff shoulder may often simulate supraspinatus-tendinitis/rotator cuff tendinitis
(110). Diagnosis is clinical examination with a careful medical history. The key feature in diagnosis
is the restriction of shoulder movement in all directions both actively and passively (125).
Sometimes associated with stiffening of the shoulder, especially after a minor trauma, a partial
rotator cuff tear may be detected in imaging studies. Physicians should be aware not to treat an
insignificant tear surgically when the true cause of the pain is frozen shoulder.
2.8. SCORING AND EVALUATION OF SHOULDER PAIN AND FUNCTION
Several scoring systems exist to evaluate shoulder function. In Europe, a widely used scoring
system has been the Constant-Murley Score (CS) (35). It includes both subjective patient-reported
and an observer-reported evaluation of the shoulder. The CS is a 100-points scale with four
subscales: pain (15 points), activities of daily living (20 points), strength (25 points) and range of
motion: flexion, abduction, external and internal rotation (40 points). The higher the score is, the
higher the quality of the function is. In frozen shoulder, specifically ROM and activities of daily
living are affected along with the pain.
The Simple Shoulder Test (SST) is a purely patient-reported evaluation of the shoulder. It is a
questionnaire with 12 questions with yes or no responses and was devised to assess improvement in
shoulder function after treatment interventions for all shoulder conditions. The minimal clinically
important difference in SST has reported to be 2 points (172). Visual Analogue Scale (VAS) is a
questionnaire and purely subjective patient-reported scale. It is continuous and measures pain on a
scale from 0 (no pain) to 10 (maximal imaginable pain).
Other scales in evaluating shoulder ROM, function or pain would be for instance The Shoulder Pain
and Disability Index (SPADI), Oxford Shoulder Score (OSS), the American Shoulder and Elbow
Surgeons (ASES) score (95), The University of California at Los Angeles Shoulder Rating scale
27
(UCLA), the Disabilities of the Arm, Shoulder and Hand (DASH) score, and the Shoulder
Disability Questionnaire (SDQ) (95, 138, 210).
2.9. STAGES OF FROZEN SHOULDER
The course of frozen shoulder has typically been divided into three stages. More recent
classification separates stage 1 into two phases, thus giving four overlapping stages of frozen
shoulder (163).
STAGE 1. The first stage of frozen shoulder is characterized by increasing pain on movement. The
pain is described as achy at rest and sharp with end range of motion. The night pain usually makes
sleeping and lying on the affected side difficult or impossible. There is as yet no restriction of
passive motion under anesthesia (months 0-2), making it challenging to differentiate for instance
from supraspinatus tendonitis. The first stage might also be called the pre-adhesive stage.
STAGE 2. The second stage resembles stage 1 but with progressive stiffening and loss of motion in
the shoulder, often with severe pain. Passive restriction of glenohumeral joint becomes clear. Stages
1 and 2 together are usually referred to as the painful phase (months 1-6). Significant sleep
disturbance may exist. According to Nagy, stage 2 lasts for 3 months (117). In Reeves’ prospective
study of natural history, the painful phase lasted for 2.5-9 months (148).
STAGE 3. During the third stage, pain gradually decreases, but stiffness remains. Considerable
restriction occurs in range of movement (months 4–15). In Reeves’ prospective study on natural
history, the period of stiffness lasted for 4 to 12 months (148).
STAGE 4. During the last stage, range of motion improves. At this point, patients usually report
minimal pain. There is capsular remodeling (months 9-24) (109,163).
We may simplify the course of frozen shoulder as follows:
• Stage 1 = PAIN.
• Stage 2 = PAIN + FREEZING.
• Stage 3 = FROZEN/STIFF.
• Stage 4 = RESOLUTION/THAWING.

28
2.10. NATURAL COURSE
The natural course of idiopathic frozen shoulder is usually self-limiting, but may be prolonged. The
reported average duration is from 1 to 2.5 years, but in a proportion of individuals, symptoms may
also persist indefinitely (44,148,159). Frozen shoulder can be highly painful and debilitating,
affecting daily and social activities and the ability to work. According to Maund (109), “there is
variation across case series in the proportion of patients who do not regain full shoulder motion,
possibly a reflection of variation in how outcome was assessed”.
The largest series including 223 frozen-shoulder patients followed up for 3 years via questionnaire,
showed 59% with normal or near-normal shoulders, 35% with mild to moderate symptoms with
pain being the most common complaint, and 6% with severe symptoms (69). In another series, after
3 years, 43% continued to suffer pain and stiffness (165). At 7 years, 50% had mild pain, stiffness
or both; a high 60% had measurable restriction of passive mobility, and 11% reported mild
functional limitation (159). Even among the satisfied patients, a substantial number are not pain-
free (62). Recurrence is extremely unusual.
2.11. TREATMENT MODALITIES
For frozen shoulder, numerous treatment methods exist, both operative and conservative. These
include 1) supervised neglect or so-called watchful waiting, meaning, the natural course, 2) oral
medications, such as non-steroidal anti-inflammatory drugs (NSAID) and oral steroids, 3) gentle
exercise supervised by a physiotherapist or as part of a home-exercise program and different kinds
of physical therapies, 4) intra-articular conrticosteroid injections, 5) arthrographic distension or
hydrodilatation 6) manipulation under anesthesia (MUA), and 7) arthroscopic capsular and open
surgical release. Acupuncture, sodium hyaluronate, stellate ganglion block and low-power laser
treatment are other techniques mentioned (109,169,207). “Advocates of each approach have
published supporting results in the general population” (63,80,116,151). In the past ten years, some
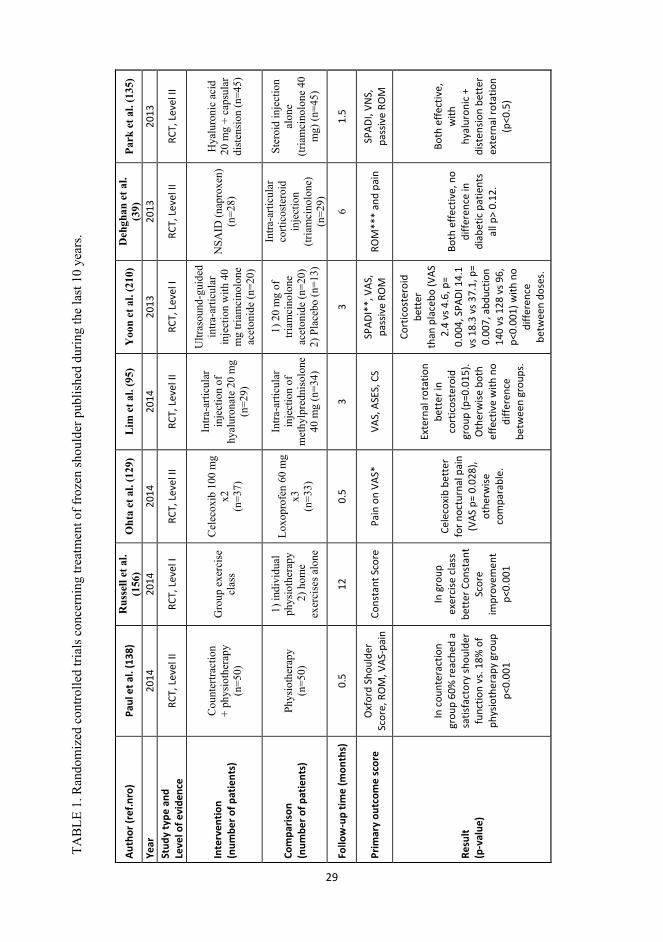
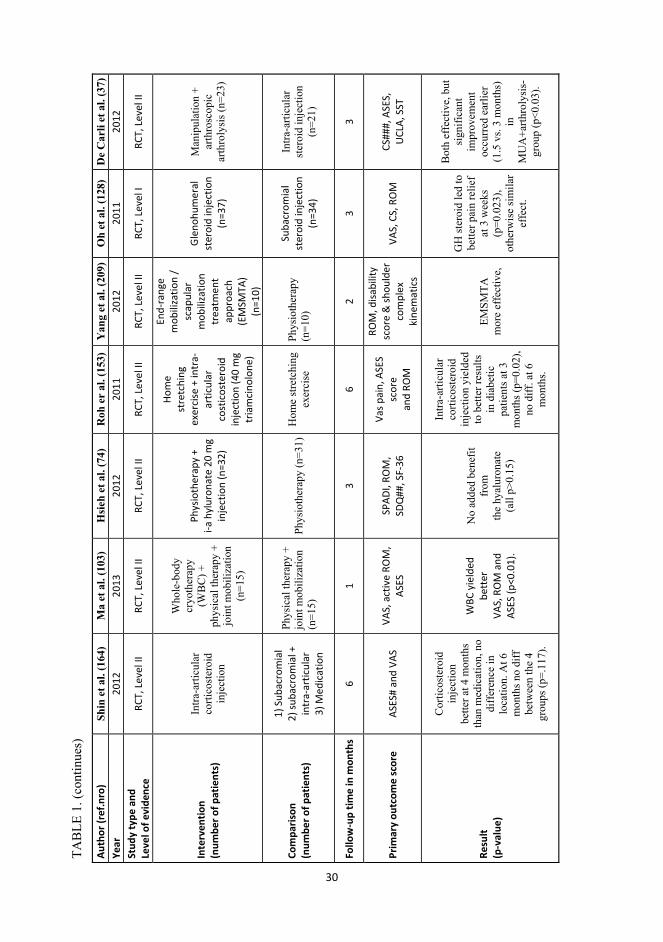
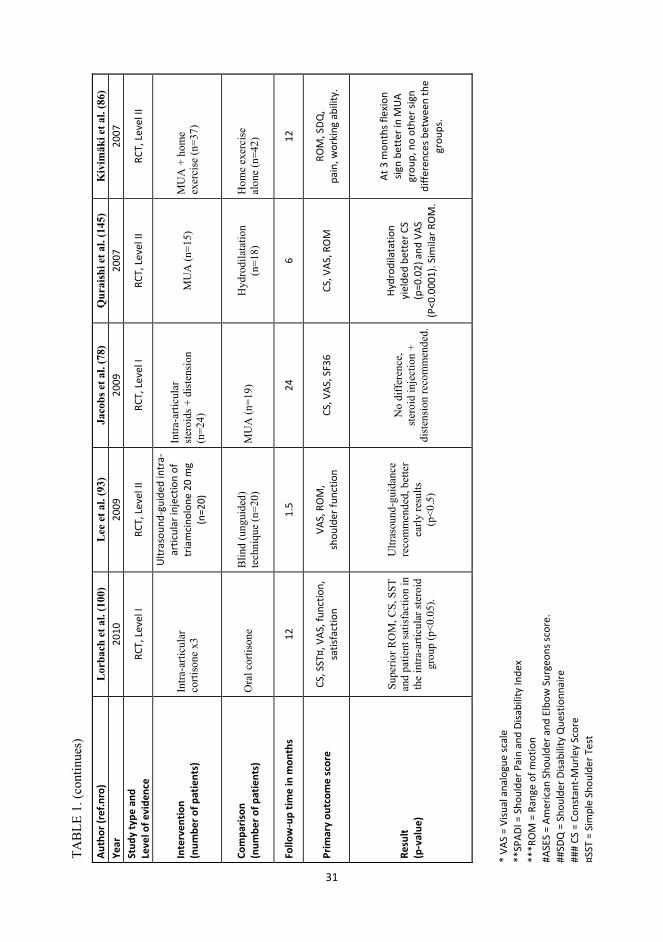
19 RCT:s have appeared in the literature (TABLE 1).
29
TAB
LE 1
. Ran
dom
ized
con
trolle
d tri
als c
once
rnin
g tre
atm
ent o
f fro
zen
shou
lder
pub
lishe
d du
ring
the
last
10
year
s.
Auth
or (r
ef.n
ro)
Paul
et a
l. (1
38)
Rus
sell
et a
l. (1
56)
Oht
a et
al.
(129
) L
im e
t al.
(95)
Y
oon
et a
l. (2
10)
Deh
ghan
et a
l. (3
9)
Park
et a
l. (1
35)
Year
20
14
2014
20
14
2014
20
13
2013
20
13
Stud
y ty
pe a
nd
Leve
l of e
vide
nce
RCT,
Lev
el II
RC
T, L
evel
I RC
T, L
evel
II
RCT,
Lev
el II
RC
T, L
evel
I RC
T, L
evel
II
RCT,
Lev
el II
Inte
rven
tion
(n
umbe
r of p
atie
nts)
Cou
nter
tract
ion
+
phys
ioth
erap
y
(n=5
0)
Gro
up e
xerc
ise
clas
s
Cel
ecox
ib 1
00 m
g x2
(n
=37)
Intra
-arti
cula
r in
ject
ion
of
hyal
uron
ate
20 m
g (n
=29)
Ultr
asou
nd-g
uide
d in
tra-a
rticu
lar
inje
ctio
n w
ith 4
0 m
g tri
amci
nolo
ne
acet
onid
e (n
=20)
NSA
ID (n
apro
xen)
(n=2
8)
Hya
luro
nic
acid
20
mg
+ ca
psul
ar
dist
ensi
on (n
=45)
Com
paris
on
(num
ber o
f pat
ient
s)
Phys
ioth
erap
y (n
=50)
1) in
divi
dual
ph
ysio
ther
apy
2) h
ome
exer
cise
s alo
ne
Loxo
prof
en 6
0 m
g x3
(n
=33)
Intra
-arti
cula
r in
ject
ion
of
met
hylp
redn
isol
one
40 m
g (n
=34)
1) 2
0 m
g of
tri
amci
nolo
ne
acet
onid
e (n
=20)
2)
Pla
cebo
(n=1
3)
Intra
-arti
cula
r co
rtico
ster
oid
inje
ctio
n (tr
iam
cino
lone
) (n
=29)
Ster
oid
inje
ctio
n al
one
(tr
iam
cino
lone
40
mg)
(n=4
5)
Follo
w-u
p tim
e (m
onth
s)
0.5
12
0.5
3 3
6 1.
5
Prim
ary
outc
ome
scor
e
Oxf
ord
Shou
lder
Sc
ore,
RO
M, V
AS-p
ain
Cons
tant
Sco
re
Pain
on
VAS*
VA
S, A
SES,
CS
SPAD
I**,
VAS
, pa
ssiv
e RO
M
ROM
***
and
pain
SP
ADI,
VNS,
pa
ssiv
e RO
M
Resu
lt
(p-v
alue
)
In c
ount
erac
tion
grou
p 60
% re
ache
d a
satis
fact
ory
shou
lder
fu
nctio
n vs
. 18%
of
phys
ioth
erap
y gr
oup
p<0.
001
In g
roup
ex
erci
se c
lass
be
tter
Con
stan
t Sc
ore
im
prov
emen
t p<
0.00
1
Cele
coxi
b be
tter
fo
r noc
turn
al p
ain
(VAS
p=
0.02
8),
othe
rwise
co
mpa
rabl
e.
Exte
rnal
rota
tion
bett
er in
co
rtic
oste
roid
gr
oup
(p=0
.015
). O
ther
wise
bot
h ef
fect
ive
with
no
diffe
renc
e be
twee
n gr
oups
.
Cort
icos
tero
id
bett
er
than
pla
cebo
(VAS
2.
4 vs
4.6
, p=
0.00
4, S
PADI
14.
1 vs
18.
3 vs
37.
1, p
= 0.
007,
abd
uctio
n 14
0 vs
128
vs 9
6,
p<0.
001)
with
no
diffe
renc
e be
twee
n do
ses.
Both
effe
ctiv
e, n
o di
ffere
nce
in
diab
etic
pat
ient
s al
l p>
0.12
.
Both
effe
ctiv
e,
with
hy
alur
onic
+
dist
ensio
n be
tter
ex
tern
al ro
tatio
n (p
<0.5
)
30
TAB
LE 1
. (co
ntin
ues)
Auth
or (r
ef.n
ro)
Shin
et a
l. (1
64)
Ma
et a
l. (1
03)
Hsi
eh e
t al.
(74)
R
oh e
r al
. (15
3)
Yan
g et
al.
(209
)O
h et
al.
(128
) D
e C
arli
et a
l. (3
7)
Year
20
12
2013
20
12
2011
20
12
2011
20
12
Stud
y ty
pe a
nd
Leve
l of e
vide
nce
RCT,
Lev
el II
RC
T, L
evel
II
RCT,
Lev
el II
RC
T, L
evel
II
RCT,
Lev
el II
RC
T, L
evel
I RC
T, L
evel
II
Inte
rven
tion
(n
umbe
r of p
atie
nts)
Intra
-arti
cula
r co
rtico
ster
oid
inje
ctio
n
Who
le-b
ody
cryo
ther
apy
(WB
C) +
ph
ysic
al th
erap
y +
join
t mob
iliza
tion
(n=1
5)
Phys
ioth
erap
y +
i-a
hyl
uron
ate
20 m
g in
ject
ion
(n=3
2)
Hom
e
stre
tchi
ng
exer
cise
+ in
tra-
artic
ular
co
stic
oste
roid
in
ject
ion
(40
mg
tria
mci
nolo
ne)
End-
rang
e m
obili
zatio
n /
scap
ular
m
obili
zatio
n tr
eatm
ent
appr
oach
(E
MSM
TA)
(n=1
0)
Gle
nohu
mer
al
ster
oid
inje
ctio
n (n
=37)
Man
ipul
atio
n +
ar
thro
scop
ic
arth
roly
sis (
n=23
)
Com
paris
on
(num
ber o
f pat
ient
s)
1) S
ubac
rom
ial
2) su
bacr
omia
l +
intr
a-ar
ticul
ar
3)
Med
icat
ion
Phys
ical
ther
apy
+ jo
int m
obili
zatio
n (n
=15)
Ph
ysio
ther
apy
(n=3
1)H
ome
stre
tchi
ng
exer
cise
Ph
ysio
ther
apy
(n
=10)
Suba
crom
ial
ster
oid
inje
ctio
n (n
=34)
Intra
-arti
cula
r st
eroi
d in
ject
ion
(n=2
1)
Follo
w-u
p tim
e in
mon
ths
6 1
3 6
2 3
3
Prim
ary
outc
ome
scor
e
ASES
# an
d VA
S VA
S, a
ctiv
e RO
M,
ASES
SP
ADI,
ROM
, SD
Q##
, SF-
36
Vas p
ain,
ASE
S sc
ore
and
ROM
ROM
, disa
bilit
y sc
ore
& sh
ould
er
com
plex
ki
nem
atic
s
VAS,
CS,
RO
M
CS##
#, A
SES,
U
CLA,
SST
Resu
lt
(p-v
alue
)
Cor
ticos
tero
id
inje
ctio
n
bette
r at 4
mon
ths
than
med
icat
ion,
no
diff
eren
ce in
lo
catio
n. A
t 6
mon
ths n
o di
ff
betw
een
the
4 gr
oups
(p=.
117)
.
WBC
yie
lded
be
tter
VA
S, R
OM
and
AS
ES (p
<0.0
1).
No
adde
d be
nefit
fr
om
the
hyal
uron
ate
(a
ll p>
0.15
)
Intra
-arti
cula
r co
rtico
ster
oid
inje
ctio
n yi
elde
d to
bet
ter r
esul
ts
in d
iabe
tic
patie
nts a
t 3
mon
ths (
p=0.
02),
no d
iff. a
t 6
mon
ths.
EMSM
TA
mor
e ef
fect
ive,
GH
ster
oid
led
to
bette
r pai
n re
lief
at 3
wee
ks
(p=0
.023
), ot
herw
ise
sim
ilar
effe
ct.
Bot
h ef
fect
ive,
but
si
gnifi
cant
im
prov
emen
t oc
curr
ed e
arlie
r (1
.5 v
s. 3
mon
ths)
in
M
UA
+arth
roly
sis-
grou
p (p
<0.0
3).
31
TAB
LE 1
. (co
ntin
ues)
Auth
or (r
ef.n
ro)
Lor
bach
et a
l. (1
00)
Lee
et a
l. (9
3)
Jaco
bs e
t al.
(78)
Q
urai
shi e
t al.
(145
) K
ivim
äki e
t al.
(86)
Ye
ar
2010
20
09
2009
20
07
2007
St
udy
type
and
Le
vel o
f evi
denc
e RC
T, L
evel
I RC
T, L
evel
II
RCT,
Lev
el I
RCT,
Lev
el II
RC
T, L
evel
II
Inte
rven
tion
(n
umbe
r of p
atie
nts)
In
tra-a
rticu
lar
corti
sone
x3
Ultr
asou
nd-g
uide
d in
tra-
artic
ular
inje
ctio
n of
tr
iam
cino
lone
20
mg
(n=2
0)
Intra
-arti
cula
r st
eroi
ds +
dis
tens
ion
(n=2
4)
MU
A (n
=15)
M
UA
+ h
ome
ex
erci
se (n
=37)
Com
paris
on
(num
ber o
f pat
ient
s)
Ora
l cor
tison
e
Blin
d (u
ngui
ded)
te
chni
que
(n=2
0)
MU
A (n
=19)
H
ydro
dila
tatio
n
(n=1
8)
Hom
e ex
erci
se
alon
e (n
=42)
Follo
w-u
p tim
e in
mon
ths
12
1.5
24
6 12
Prim
ary
outc
ome
scor
e
CS, S
ST¤,
VAS
, fun
ctio
n,
satis
fact
ion
VAS,
RO
M,
shou
lder
func
tion
CS, V
AS, S
F36
CS, V
AS, R
OM
RO
M, S
DQ,
pain
, wor
king
abi
lity.
Resu
lt
(p-v
alue
)
Supe
rior R
OM
, CS,
SST
an
d pa
tient
satis
fact
ion
in
the
intra
-arti
cula
r ste
roid
gr
oup
(p<0
.05)
.
Ultr
asou
nd-g
uida
nce
reco
mm
ende
d, b
ette
r ea
rly re
sults
(p
<0.5
)
No
diff
eren
ce,
ster
oid
inje
ctio
n +
dist
ensi
on re
com
men
ded.
Hydr
odila
tatio
n
yiel
ded
bett
er C
S (p
=0.0
2) a
nd V
AS
(P<0
.000
1). S
imila
r RO
M.
At 3
mon
ths f
lexi
on
sign
bett
er in
MU
A gr
oup,
no
othe
r sig
n di
ffere
nces
bet
wee
n th
e gr
oups
.
* VA
S =
Visu
al a
nalo
gue
scal
e **
SPAD
I = S
houl
der P
ain
and
Disa
bilit
y In
dex
***R
OM
= R
ange
of m
otio
n #A
SES
= Am
eric
an S
houl
der a
nd E
lbow
Sur
geon
s sco
re.
##SD
Q =
Sho
ulde
r Disa
bilit
y Q
uest
ionn
aire
##
# CS
= C
onst
ant-
Mur
ley
Scor
e ¤S
ST =
Sim
ple
Shou
lder
Tes
t
32
2.11.1. CONSERVATIVE TREATMENT
1) Watchful waiting or supervised neglect means letting the condition run its natural course.
It involves explaining the condition to the patient, and providing education and advice about
mobilization within pain limits, plus use of pain relief (44).
2) Oral medications including non-steroidal anti-inflammatory drugs (NSAIDs) and oral
steroids.
Oral steroids such as prednisolone or cortisone (144) are one treatment for frozen shoulder. The
Buchbinder group’s review on oral steroids for adhesive capsulitis (18) included five trials: two
trials with oral steroids and placebo, one with oral steroid and no treatment, one with oral and intra-
articular steroid, and one with MUA + intra-articular steroid combined with or without oral steroids.
They concluded that there was no certain long-term benefit, but in the short-term, oral steroids may
be beneficial in reducing pain and disability and increasing motion (18). They also concluded that
use of oral steroids for a short time does not lead to serious side effects. Oral steroids were mostly
given for 3 to 4 weeks and sometimes, if stiffness and pain persisted, for another 3 to 4 weeks. The
equivalent amount of prednisolone ranged from 8 to 30 mg daily, often in gradually decreasing
doses. In a randomized control trial, a 3-week course of prednisolone daily had a significant short-
term benefit not maintained beyond 6 weeks (17). Oral steroids are no longer a commonly used
intervention for frozen shoulder in Finland. Concerning other pain relief, non-steroidal anti-
inflammatory drugs can be effective, but no randomized controlled trial documents their efficacy
compared to that of placebo (201). NSAIDs have been effective in comparison to intra-articular
corticosteroid injections in diabetes patients (39). The selective cyclo-oxygenase-2 inhibitor
celecoxib (100 mg x2) for 1 to 2 weeks was comparable to loxoprofen (60 mg x3) in terms of
analgesic efficacy (129).
3) Physiotherapy.
Various kinds of physiotherapies and techniques have been introduced, including supervised
exercise, mobilization, acupuncture, osteopathic and chiropractic techniques (95,126), and
electrotherapeutic interventions such as laser therapy and ultrasound (46). It is believed that,
intensive physiotherapy in the early stages of the disease, inflammation, proliferation, and perhaps
even the early phase of the fibrotic stage would only activate the inflammatory process and result in
inferior outcome comparedo that with the natural course of frozen shoulder (44).
33
According to one recent review, based on the qualities of studies concerning physiotherapies or
other therapeutic techniques, the following conclusions could be reached: short-wave diathermy
(SWD) (190) with stretching may be more effective than home exercise; a high-grade mobilization
technique (HGMT) may be more effective than a low-grade mobilization technique (LGMT); it
may be beneficial to add physiotherapy to steroid injection; and steroids and physiotherapy are
better than placebo (109).
4) Intra-articular corticosteroid injections have reduced inflammation and provided pain relief,
and a range of doses and of number of injections introduced (15,39,40,100,128,143,205). This
intervention is usually delivered early in the disease, in the synovitis phase, stage 1. According to
the Clinical Practice Guidelines, there is strong evidence that “intra-articular corticosteroid
injections combined with shoulder mobility and stretching exercises are more effective in providing
short-term (4-6 weeks) pain relief and improved function than is shoulder mobility and stretching
exercise alone (84). On the other hand, Arslan found no short-term difference between intra-
articular corticosteroid and physiotherapy in their 20 patients (6). In one meta-analysis, higher doses
of corticosteroids provided greater improvement of shoulder pain (5).
5) Arthrographic distension, hydrodilatation.
In dilatation treatment, the joint capsule is dilated with sterile saline or other solution such as a local
anesthetic or steroid, guided by radiological imaging (ultrasound or arthrography) (16,162). The
injection is continued with high enough pressure until the contracted capsule expands and ruptures;
this usually requires 30 to 40 ml. The rupture usually occurs through the subscapular bursae, but
occasionally down the biceps sheath (145). By the hydrodilatation method, fluid is injected into the
glenohumeral joint.
2.11.2. OPERATIVE TREATMENT
6) Manipulation under anesthesia (MUA) forces the adhesive and contracted capsule of the
glenohumeral joint to break free under brief general anesthesia. (71,77,161,189,201,203). This can
be undertaken as a one-day procedure, but it is important to secure adequate postoperative
physiotherapy. In retrospective series, after MUA, 75% have had satisfactory results and 8% had
recurrences (3), diabetes did not lead to deterioration in results. However, RCT studies have shown
no long-term benefit from MUA. For instance, MUA added no more benefit to home exercise (86),
34
the MUA result did not exceed the results of hydrodilatation (145), and no difference emerged
between MUA and intra-articular steroid injection + distension (78). However, one RCT has shown
some short-term benefit from MUA, for instance MUA + arthrolysis showed earlier significant
improvement than did steroid injection (37). Complications related to MUA are unusual, but they
do exist (121,131): ones like articular lesions (99) or glenoid fracture (105).
7) Arthroscopic capsular release is a surgical procedure conducted under general or regional
anesthesia, during which the contracted capsule is released under visual control (167,197,198).
Open capsular release is another surgical option, usually recommended in those resistant to
arthroscopic intervention (130). Each can be undertaken as a one-day procedure. The key step in
arthroscopic capsular release is to release the rotator interval region from the biceps to the upper
level of the subscapularis. In open surgical release, excision of the coracohumeral ligament is said
to produce immediate release (130). In pan-capsular arthroscopic release, all the following steps
may be done: dissection of the rotator interval, resection of the coracoacromial and part of the
coracohumeral ligaments from the coracoid process, and dissection of the superior, middle, and
inferior glenohumeral ligaments, as well as of the posterior capsule (127).
Walther et al found no significant differences in outcome ROM between the three surgical
procedures for persistent frozen shoulder: Arthroscopic capsular release + subacromial
decompression, subacromial decompression with MUA, or arthroscopic capsular release (193).
No general agreement exists on which treatment is the best. Often, several treatment methods are
combined. Criticism has arisen towards any interventional approach for frozen shoulder due to the
absence of true evidence as to whether the interventions actually change the outcome from the
natural course (81). Many specialist do, however, agree that treatments chosen should depend on
the stage of frozen shoulder and that conservative treatments should be chosen before surgical ones
(36,43,107). Aggressive mobilization should be avoided in the early stages with its intense pain.
Surgery is nowadays usually adopted only in rare, resistant cases (107). No consensus exists on
when exactly a surgical intervention would be indicated.
35
2.12. COST EFFECTIVENESS
Studies that include or present any cost-effectiveness data, or precise economic data for frozen
shoulder barely exist (109). Concerning physiotherapy, one suggestion is that a low-grade
mobilization technique (LGMT in the pain-free zone) may be more cost-effective than high-grade
mobilization (HGMT with intensive end-range motion) (181). However, from the clinical point of
view, HGMT has been reported to be statistically more effective for the patients (190). Another
study of patients with unilateral shoulder pain suggests that steroids alone may be more cost-
effective than steroids plus physiotherapy or physiotherapy alone (79). With current evidence it is
impossible to develop a full economic model of frozen shoulder.
2.13. POSTOPERATIVE FROZEN SHOULDER
Postoperative stiff shoulder after RCR is a common complication (54,55,72). It has also been called
“postoperative frozen shoulder” by some experienced shoulder surgeons (72). It has been postulated
that a larger amount of tissue in RCT meaning a smaller tear may be associated with postoperative
stiffness (106).
36
3. AIMS OF THE PRESENT STUDY
The purpose of this academic dissertation was to investigate the long-term outcome of frozen
shoulder. The specific aims of the study were to discover:
I. The long-term outcome of the natural course of idiopathic frozen shoulder.
II. The very long-term outcome after manipulation under anesthesia (MUA) for idiopathic
frozen shoulder.
III. The incidence and long-term outcome of postoperative frozen shoulder after an open
rotator cuff repair including factors predicting postoperative stiffness.
IV. Whether timing of MUA has any association on the outcome of MUA.
V. The long-term outcome of diabetic frozen shoulder, comparing it with the outcome of
frozen-shoulder patients without diabetes.
37
4. PATIENTS AND METHODS
Over 15 000 patient records were manually evaluated to identify 234 patients with frozen
shoulder. Of these patients, 177 were seen and diagnosed at ORTON Orthopaedic Hospital by a
shoulder surgeon and at his private-practice office. In addition, 57 frozen-shoulder patients with
manipulation under anesthesia were traced from Rauma Hospital, Rauma Finland, and also
diagnosed and treated by a shoulder surgeon. The total number of shoulders and patients
included in this project is 198 shoulders (178 patients) with idiopathic frozen shoulder, 56
patients (59 shoulders) with postoperative frozen shoulder, and 61 control patients with 69
shoulders with no stiffness after surgery. Altogether, 234 patients (257 shoulders) were
clinically followed up and evaluated for their long-term outcome. The mean follow-up time for
idiopathic frozen-shoulder patients was 9.7 years and, for postoperative frozen-shoulder
patients, 8.7 years. All the initial diagnoses of frozen shoulder were made by a specialized
shoulder surgeon. The final follow-up examinations, interview and clinical examinations, ROM
and Constant-Murley Scores, were made by an independent physician specializing in surgery.
All surgeries (open rotator cuff repairs) were performed in a similar fashion under general
anesthesia at the ORTON Orthopaedic Hospital, Helsinki (Study III). All planned manipulations
under anesthesia were performed either at the ORTON Orthopaedic Hospital, Helsinki (Study II
and V) or Rauma Hospital, Rauma (Study IV).
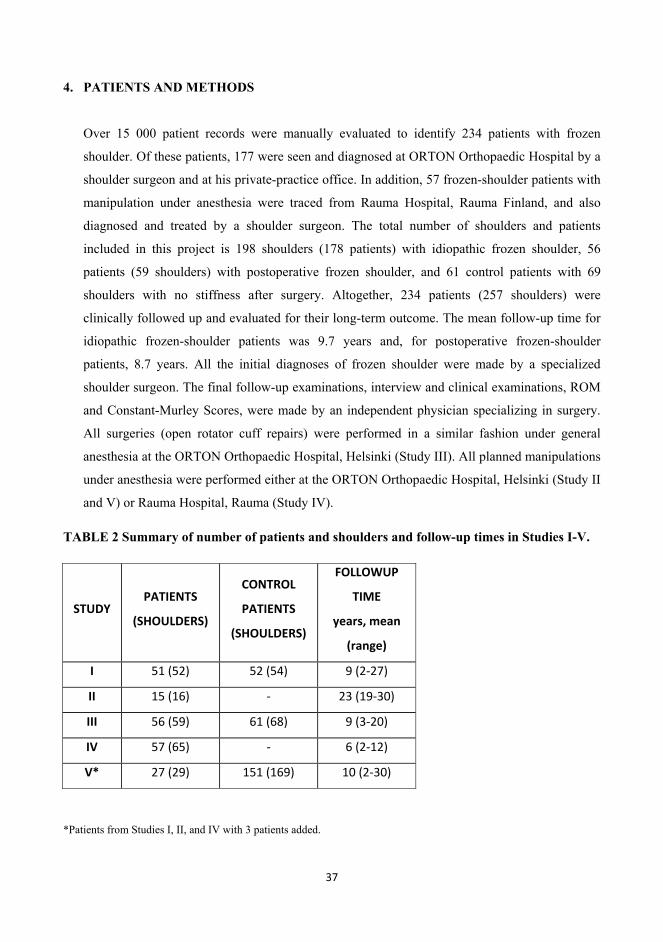
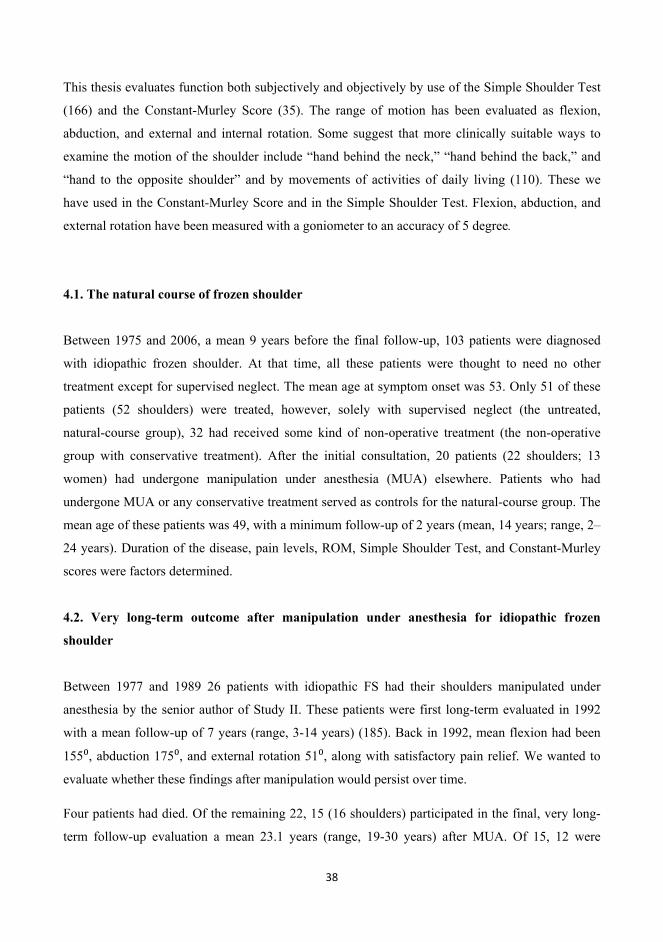
TABLE 2 Summary of number of patients and shoulders and follow-up times in Studies I-V.
STUDY PATIENTS
(SHOULDERS)
CONTROL
PATIENTS
(SHOULDERS)
FOLLOWUP
TIME
years, mean
(range)
I 51 (52) 52 (54) 9 (2-27)
II 15 (16) - 23 (19-30)
III 56 (59) 61 (68) 9 (3-20)
IV 57 (65) - 6 (2-12)
V* 27 (29) 151 (169) 10 (2-30)
*Patients from Studies I, II, and IV with 3 patients added.
38
This thesis evaluates function both subjectively and objectively by use of the Simple Shoulder Test
(166) and the Constant-Murley Score (35). The range of motion has been evaluated as flexion,
abduction, and external and internal rotation. Some suggest that more clinically suitable ways to
examine the motion of the shoulder include “hand behind the neck,” “hand behind the back,” and
“hand to the opposite shoulder” and by movements of activities of daily living (110). These we
have used in the Constant-Murley Score and in the Simple Shoulder Test. Flexion, abduction, and
external rotation have been measured with a goniometer to an accuracy of 5 degree.
4.1. The natural course of frozen shoulder
Between 1975 and 2006, a mean 9 years before the final follow-up, 103 patients were diagnosed
with idiopathic frozen shoulder. At that time, all these patients were thought to need no other
treatment except for supervised neglect. The mean age at symptom onset was 53. Only 51 of these
patients (52 shoulders) were treated, however, solely with supervised neglect (the untreated,
natural-course group), 32 had received some kind of non-operative treatment (the non-operative
group with conservative treatment). After the initial consultation, 20 patients (22 shoulders; 13
women) had undergone manipulation under anesthesia (MUA) elsewhere. Patients who had
undergone MUA or any conservative treatment served as controls for the natural-course group. The
mean age of these patients was 49, with a minimum follow-up of 2 years (mean, 14 years; range, 2–
24 years). Duration of the disease, pain levels, ROM, Simple Shoulder Test, and Constant-Murley
scores were factors determined.
4.2. Very long-term outcome after manipulation under anesthesia for idiopathic frozen
shoulder
Between 1977 and 1989 26 patients with idiopathic FS had their shoulders manipulated under
anesthesia by the senior author of Study II. These patients were first long-term evaluated in 1992
with a mean follow-up of 7 years (range, 3-14 years) (185). Back in 1992, mean flexion had been
155 , abduction 175 , and external rotation 51 , along with satisfactory pain relief. We wanted to
evaluate whether these findings after manipulation would persist over time.
Four patients had died. Of the remaining 22, 15 (16 shoulders) participated in the final, very long-
term follow-up evaluation a mean 23.1 years (range, 19-30 years) after MUA. Of 15, 12 were
39
women (80%). The mean age of these patients was 48.5 at MUA and 72 at final follow-up. Four
patients had diabetes. Between their onset of symptoms and the manipulation, the time averaged 7.6
months. Inclusion criteria were: 1) No, or only minor shoulder trauma, 2) Marked loss of active and
passive shoulder motion (forward flexion <120 and/or abduction <120 , external and internal
rotation almost absent, 3) Normal findings on a true AP radiograph of the glenohumeral joint, 4)
Diagnosis of FS by an experienced orthopedic surgeon, 5) Manipulation under anesthesia done.
Exclusion criteria were: 1) An intrinsic glenohumeral disorder such as arthritis or rotator-cuff tear,
2) Any history of substantial shoulder trauma, 3) Previous or subsequent shoulder surgery. Pain
levels, ROM, the Simple Shoulder Test, and Constant-Murley Scores were determined.
4.3. The outcome of postoperative frozen shoulder after open rotator cuff repair
Between 1988 and 2004, 416 consecutive open rotator-cuff repairs (RCR) were performed at
ORTON Orthopaedic Hospital, Helsinki, Finland. Among them we identified a total of 103 patients
with severe painful postoperative restriction of ROM. Of these, 15 were excluded for various
reasons: preoperative posttraumatic stiff shoulders manipulated before surgery, posttraumatic
adhesive capsulitis diagnosed and manipulated at surgery, shoulders treated only for partial repair
(poor tendon quality, severe retraction), and manipulation done 2 months after surgery. Of the 88
patients remaining, one had an evident re-tear with poor shoulder strength, and in four instances,
clinical follow-up data were insufficient, leaving 83. Of these, four had died. Of the 56 patients
(71%, 59 shoulders) who volunteered to participate, 39 were men (70%) and 17 women. Forty-five
(76%) tears were traumatic. Mean age during surgery was 56 (range, 40-83 years). Time from
beginning of symptoms to surgery averaged 8.4 months (range, 2 weeks to 84 months, median, 4.0
months). Operative delay was <6 months in 38 cases and less than one year in 78%. All operations
were performed in a similar manner. The mean size of the tear was 3x4 cm (12.6 cm2). The
supraspinatus tendon was involved in all cases, the subscapular in seven (12%). Mean follow-up
time was 8.7 years (3–20 years). In many studies, preoperative stiff patients have also been
included. We wanted to study purely postoperative stiffness and therefore carefully excluded all
those patients who already had preoperative or perioperative passive shoulder stiffness. We
included only patients who had free passive range of motion pre- and peri-operatively. We believe
this provides better information on pure postoperative stiffness. The incidence is greater, if one
40
includes preoperative stiff shoulders too. We determined range of motion, pain, shoulder strength,
Constant-Murley Score and Simple Shoulder Test.
4.4. Does timing of MUA for frozen shoulder associate with results?
Study IV is a retrospective evaluation of single-surgeon, single institution consecutive series of
frozen shoulder patients that were manipulated under anesthesia from April 1997 to October 2002
in Hospital of Rauma. Two independent investigators evaluated the long-term results. 57 (65
shoulders) participated in the study (71%). Mean follow-up time was 6 years (range, 2-12), and of
the participants, 30 were women (53%). Mean age at MUA was 54.0 (range, 37-59). Delay from the
beginning of symptoms to MUA averaged 8.8 months (range, 3-36 months). Ten patients (18%)
were diabetic. The right shoulder was involved in 30 (46%), and 16 patients (28%) had a history of
minor trauma prior their symptoms. Inclusion criteria for Study IV were 1) No, or only minor
shoulder trauma, 2) Marked loss of active and passive shoulder motion (forward flexion <120,
abduction <110, severe restriction in external rotation, 3) Normal findings on a true antero-posterior
radiograph of the glenohumeral joint, 4) Diagnosis of frozen shoulder made by an experienced
orthopedic surgeon and, 5) MUA performed. We excluded patients who had any intrinsic
glenohumeral disorder such as rotator cuff tear or glenohumeral arthritis, any history of substantial
shoulder trauma, such as traffic accidents, fracture of the ipsilateral extremity or insufficient patient
status recordings (no mention of preoperative ROM in degrees).
The pre-operative flexion averaged 95º (10º-130º) and abduction 80º (10º-120º). Seven frozen
shoulders were bilateral and one simultaneous bilateral. Non-operative treatment prior to the MUA
included physiotherapy in 3 patients and subacromial corticoid injection (mean 1.9 injections per
shoulder) in 26. Only 8 (14%) smoked, and 35 (61%) drank some alcohol weekly.
Referring to the earlier literature concerning timing of manipulation of FS, two groups were
formed; Those mobilized between 6 and 9 months (Group A, 25 shoulders, MUA done at 6 - <9
months after symptom onset), and the others (Group B, 40 shoulders, MUA at <6 or 9 months
after symptom onset). The two groups did not differ when it came to patient age, gender, affected-
shoulder side, range of motion in flexion or abduction prior to MUA, smoking, or alcohol
consumption. We determined pain by a patient-generated VAS and recorded ROM, SST, and CS at
follow-up.
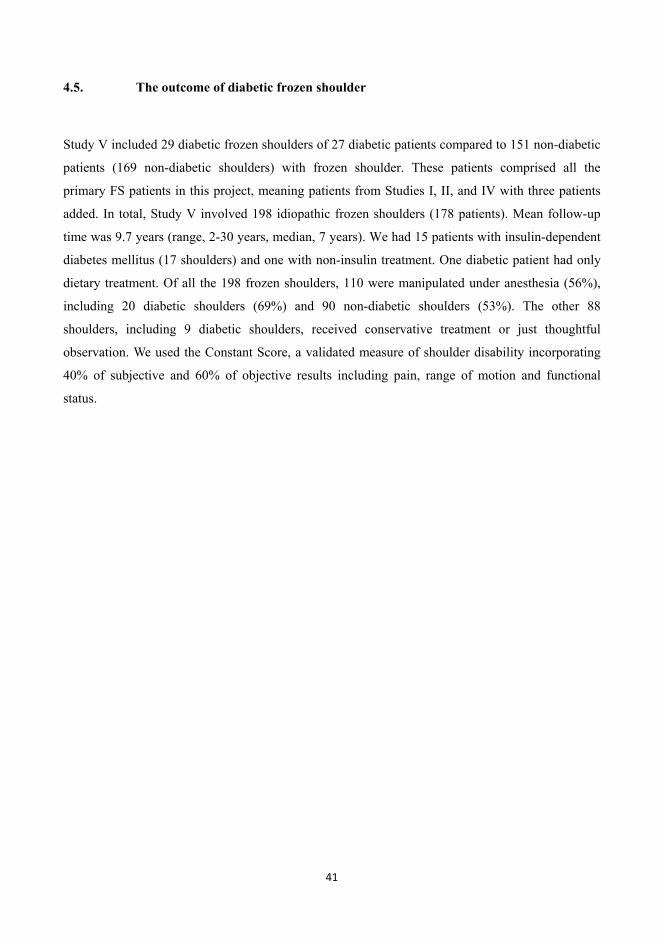
41
4.5. The outcome of diabetic frozen shoulder
Study V included 29 diabetic frozen shoulders of 27 diabetic patients compared to 151 non-diabetic
patients (169 non-diabetic shoulders) with frozen shoulder. These patients comprised all the
primary FS patients in this project, meaning patients from Studies I, II, and IV with three patients
added. In total, Study V involved 198 idiopathic frozen shoulders (178 patients). Mean follow-up
time was 9.7 years (range, 2-30 years, median, 7 years). We had 15 patients with insulin-dependent
diabetes mellitus (17 shoulders) and one with non-insulin treatment. One diabetic patient had only
dietary treatment. Of all the 198 frozen shoulders, 110 were manipulated under anesthesia (56%),
including 20 diabetic shoulders (69%) and 90 non-diabetic shoulders (53%). The other 88
shoulders, including 9 diabetic shoulders, received conservative treatment or just thoughtful
observation. We used the Constant Score, a validated measure of shoulder disability incorporating
40% of subjective and 60% of objective results including pain, range of motion and functional
status.
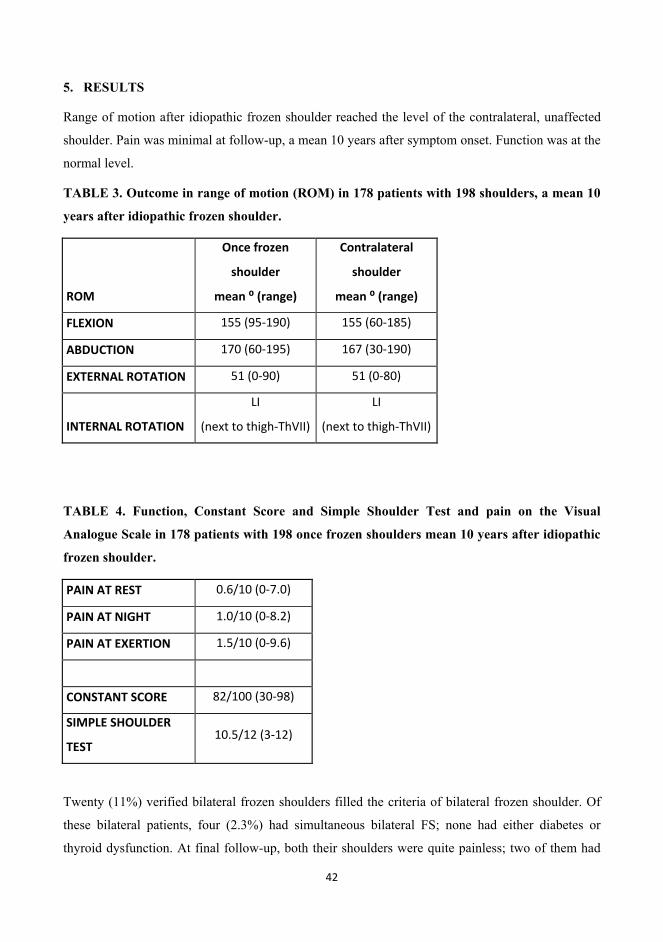
42
5. RESULTS
Range of motion after idiopathic frozen shoulder reached the level of the contralateral, unaffected
shoulder. Pain was minimal at follow-up, a mean 10 years after symptom onset. Function was at the
normal level.
TABLE 3. Outcome in range of motion (ROM) in 178 patients with 198 shoulders, a mean 10
years after idiopathic frozen shoulder.
ROM
Once frozen
shoulder
mean (range)
Contralateral
shoulder
mean (range)
FLEXION 155 (95-190) 155 (60-185)
ABDUCTION 170 (60-195) 167 (30-190)
EXTERNAL ROTATION 51 (0-90) 51 (0-80)
INTERNAL ROTATION
LI
(next to thigh-ThVII)
LI
(next to thigh-ThVII)
TABLE 4. Function, Constant Score and Simple Shoulder Test and pain on the Visual
Analogue Scale in 178 patients with 198 once frozen shoulders mean 10 years after idiopathic
frozen shoulder.
PAIN AT REST 0.6/10 (0-7.0)
PAIN AT NIGHT 1.0/10 (0-8.2)
PAIN AT EXERTION 1.5/10 (0-9.6)
CONSTANT SCORE 82/100 (30-98)
SIMPLE SHOULDER
TEST 10.5/12 (3-12)
Twenty (11%) verified bilateral frozen shoulders filled the criteria of bilateral frozen shoulder. Of
these bilateral patients, four (2.3%) had simultaneous bilateral FS; none had either diabetes or
thyroid dysfunction. At final follow-up, both their shoulders were quite painless; two of them had
43
all pain (rest, activity and night) rated as <1/10. One had rest and activity pain <1 but pain during
the night at 2.3/10. One patient with simultaneous bilateral frozen shoulder had no pain at all in her
shoulders.
The specific results of the study were:
5.1. Natural course of frozen shoulder
The duration of frozen shoulder averaged 15 months (range, 4–36 months) in the natural course
group, and 20 months (range, 6–60 months) in the non-operative group with no statistically
significant difference (p=0.080). At final follow-up, the range of motion had improved to the
contralateral level in 94% of the natural-course group, in 91% in the non-operative group, and in
91% in the MUA group. The percentage of patients that were totally pain-free at rest, during the
night, and with exertion was 51% with the natural-course patients, 44% in non-operative group, and
30% in the MUA group. Pain at rest was less than 3 on the Visual Analogue Scale in 94% of
patients in the natural-course group, 91% in the non-operative group, and 90% in the manipulation
group. The mean Constant-Murley score was 83 in the untreated group, 81 in the non-operative
group, and 82 in the manipulation group.
Four patients had long-term follow-up with Constant Score <70/100; One 61-year old male farmer
with Dupuytren’s disease who had 65 Constant Score points had a severe osteoarthrosis in his
glenohumeral joint and a high level of pain. One 78-year-old male patient had a Constant Score of
only 35 with no arthrosis, but with a high level of pain in his shoulder. He also had a high level of
pain and swelling in both his wrists, and in addition his prosthetic knee had been operated on three
times for pain. The recommendation was laboratory investigations for rheumatism. The passive
range of motion in his glenohumeral joint was not restricted. One 59-year-old retired female patient
had a Constant Score of 69 with no osteoarthrosis, a free passive ROM of her glenohumeral joint,
and abduction power of 6.5 kg. However, her Simple Shoulder Test score was a full 12 points. She
had diabetes and Maya Maya disease and a recent history of loss-of-consciousness attacks. The
fourth natural-course patient with a poor follow-up Constant Score of 54 points was a 61-year-old
female retired bank clerk with no osteoarthrosis and very little pain, but inferior active flexion of
135 and also passive flexion restricted to 145 degrees. Her abduction was 155, external rotation 45,
and internal rotation LIII. These patients with a poor final Constant Score did not experience
44
specifically poor ROM during frozen shoulder. We could find no specific frozen-shoulder related
conjunctive reason to explain their poor final Constant Score results.
5.2. Very long-term outcome after manipulation under anesthesia for idiopathic
frozen shoulder
At 7 years, improvement had occurred in forward flexion to 155°, in abduction to 175°, in external
rotation to 51°, and in internal rotation to the T7 level. During the next 16 years, ROM deteriorated
by 8° to 23°, but still equaled the contralateral shoulder’s ROM. On a VAS (range, 0–10; 0 = none,
10 = maximal), pain averaged 0.3 at rest, 0.8 at night, and 1.5 with exertion. The mean Constant-
Murley score was 70 (range, 34–88), with 12 patients reaching an age- and sex-adjusted normal
Constant-Murley score. Two small fractures of the inferior glenoid rim were visible in the 1992 x-
rays. They had no history of trauma, nor any arthrosis at final follow up.
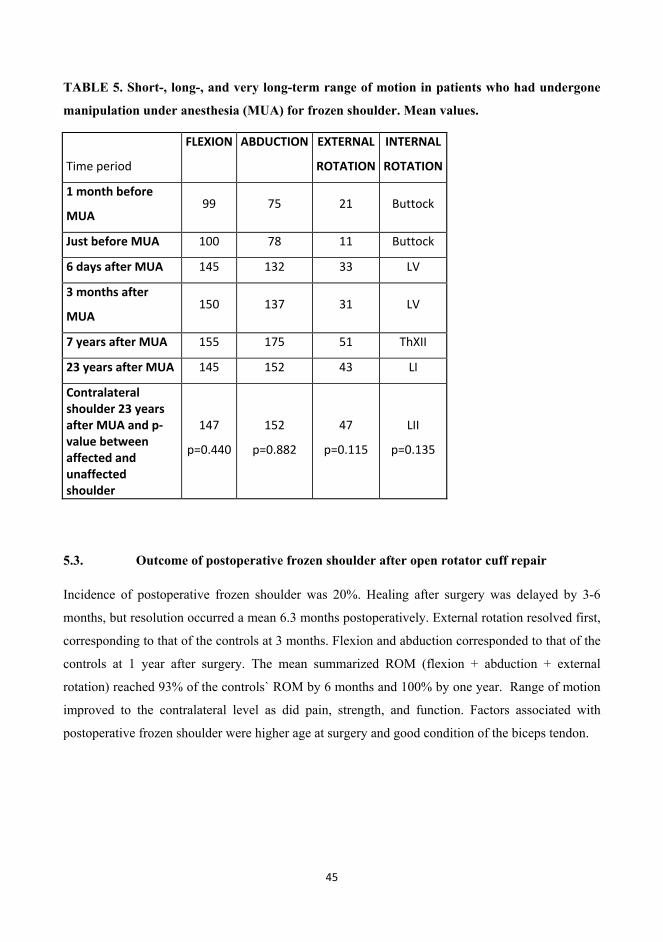
45
TABLE 5. Short-, long-, and very long-term range of motion in patients who had undergone
manipulation under anesthesia (MUA) for frozen shoulder. Mean values.
Time period
FLEXION
ABDUCTION
EXTERNAL
ROTATION
INTERNAL
ROTATION
1 month before
MUA 99 75 21 Buttock
Just before MUA 100 78 11 Buttock
6 days after MUA 145 132 33 LV
3 months after
MUA 150 137 31 LV
7 years after MUA 155 175 51 ThXII
23 years after MUA 145 152 43 LI
Contralateral shoulder 23 years after MUA and p-value between affected and unaffected shoulder
147
p=0.440
152
p=0.882
47
p=0.115
LII
p=0.135
5.3. Outcome of postoperative frozen shoulder after open rotator cuff repair
Incidence of postoperative frozen shoulder was 20%. Healing after surgery was delayed by 3-6
months, but resolution occurred a mean 6.3 months postoperatively. External rotation resolved first,
corresponding to that of the controls at 3 months. Flexion and abduction corresponded to that of the
controls at 1 year after surgery. The mean summarized ROM (flexion + abduction + external
rotation) reached 93% of the controls` ROM by 6 months and 100% by one year. Range of motion
improved to the contralateral level as did pain, strength, and function. Factors associated with
postoperative frozen shoulder were higher age at surgery and good condition of the biceps tendon.
46
5.4. Does timing of MUA for frozen shoulder associate with results?
Timing of MUA was statistically associated with the long-term outcome of frozen shoulder.
Preoperatively, no difference appeared between the groups in flexion or abduction. At follow-up,
abduction (177 vs. 167 ) and external rotation (61 vs. 51 ) were statistically significantly better in
Group A. Forward flexion was also better in Group A, but not significantly (162 vs. 156). The final
ROM of the once-frozen shoulder was similar to that of the contralateral, unaffected shoulder
(p=0.528-0.926). Regarding function, Simple Shoulder Test scores were better in Group A (11.3 vs.
9.5), at statistical significance: p=0.002. Constant Score was also better, but not significantly (87 vs.
83).
Regarding pain, patients manipulated between 6 and 9 months from onset of symptoms reported
significantly less pain at rest and night than did other patients. They had less pain also during
exertion, but not significantly. Subjectively, patients in Group A were more satisfied with their
results: 91% of Group A were satisfied or very satisfied, in Group B 72% (p=0.076). All the
patients who were either dissatisfied or very dissatisfied were from Group B (their frozen shoulders
had been manipulated at 3, 5, 12, and 19 months after the beginning of symptoms). Sick-leave after
the manipulation was similar and averaged 1.3 months (range, 0-7months). In Group A, 84% felt
that their symptoms improved after manipulation, in Group B 75% (p=0.084). During the year
before the follow-up, nine patients (16%) had suffered shoulder complaints in daily living activities,
with a tendency toward a significant difference between groups (one patient, 4%, in Group A, and
eight , 20%, in Group B (p=0.068). At follow-up, glenohumeral motion was somewhat restricted in
nine patients and severely restricted in one patient from Group B. Group A had only one patient
with a little restriction in the glenohumeral joint (p=0.054). Of the 57 patients, 26 continued to
work, and 28 (49%) had retired, none due to any shoulder disorder. Under the same circumstances,
95% of the patients in Group A and 75% in Group B would have chosen the manipulation again.
Five re-manipulations took place in each group with no evident significance, not even when
calculated between patients manipulated before 6 months versus all the others (p=0.259). When
evaluating a subgroup of patients manipulated later than 12 months after symptom onset, the results
were more clearly inferior compared to results for those manipulated between 6 and 9 months.
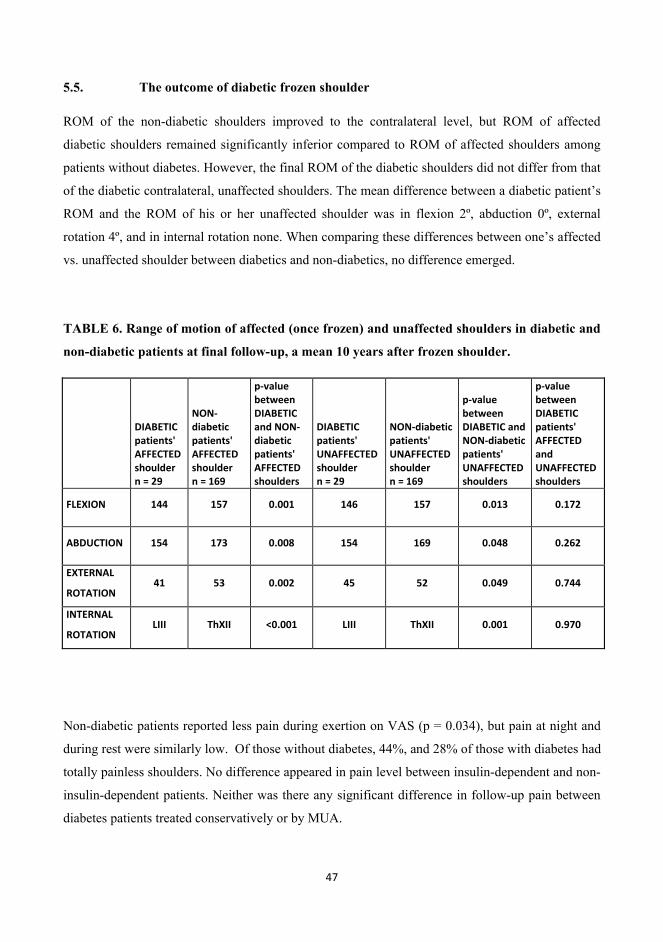
47
5.5. The outcome of diabetic frozen shoulder
ROM of the non-diabetic shoulders improved to the contralateral level, but ROM of affected
diabetic shoulders remained significantly inferior compared to ROM of affected shoulders among
patients without diabetes. However, the final ROM of the diabetic shoulders did not differ from that
of the diabetic contralateral, unaffected shoulders. The mean difference between a diabetic patient’s
ROM and the ROM of his or her unaffected shoulder was in flexion 2º, abduction 0º, external
rotation 4º, and in internal rotation none. When comparing these differences between one’s affected
vs. unaffected shoulder between diabetics and non-diabetics, no difference emerged.
TABLE 6. Range of motion of affected (once frozen) and unaffected shoulders in diabetic and
non-diabetic patients at final follow-up, a mean 10 years after frozen shoulder.
DIABETIC patients' AFFECTED shoulder n = 29
NON-diabetic patients' AFFECTED shoulder n = 169
p-value between DIABETIC and NON-diabetic patients' AFFECTED shoulders
DIABETIC patients' UNAFFECTED shoulder n = 29
NON-diabetic patients' UNAFFECTED shoulder n = 169
p-value between DIABETIC and NON-diabetic patients' UNAFFECTED shoulders
p-value between DIABETIC patients' AFFECTED and UNAFFECTED shoulders
FLEXION 144 157 0.001 146 157 0.013 0.172
ABDUCTION 154 173 0.008 154 169 0.048 0.262
EXTERNAL
ROTATION 41 53 0.002 45 52 0.049 0.744
INTERNAL
ROTATION LIII ThXII <0.001 LIII ThXII 0.001 0.970
Non-diabetic patients reported less pain during exertion on VAS (p = 0.034), but pain at night and
during rest were similarly low. Of those without diabetes, 44%, and 28% of those with diabetes had
totally painless shoulders. No difference appeared in pain level between insulin-dependent and non-
insulin-dependent patients. Neither was there any significant difference in follow-up pain between
diabetes patients treated conservatively or by MUA.

48
Constant-Murley Score and Simple Shoulder Test figures were better in non-diabetes patients than
in diabetes patients, 82 vs. 76 (p=0.055), and 11 vs. 9, (p=0.005). There was no difference in
functional scores between insulin-dependent and non-insulin-dependent patients.
Insulin-dependent diabetes patients had inferior internal rotation and a tendency towards inferior
external rotation compared to non-insulin dependent diabetes patients during frozen shoulder but
not statistically significantly. Those insulin-dependent patients had inferior external rotation to other
diabetics also at follow-up (p=0.035). Otherwise, their outcome was similar with non-insulin
dependent diabetics.
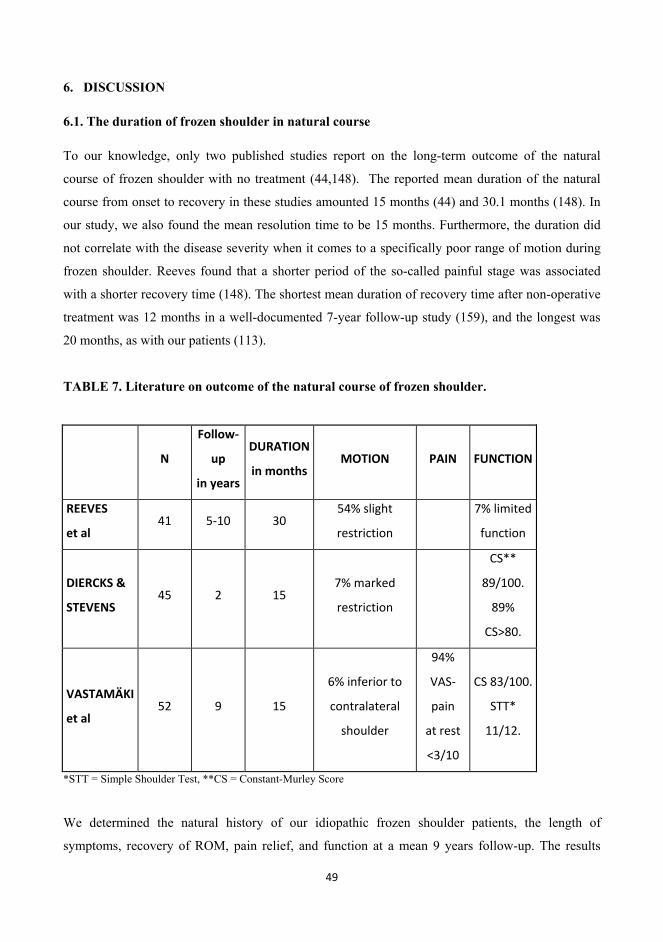
49
6. DISCUSSION
6.1. The duration of frozen shoulder in natural course
To our knowledge, only two published studies report on the long-term outcome of the natural
course of frozen shoulder with no treatment (44,148). The reported mean duration of the natural
course from onset to recovery in these studies amounted 15 months (44) and 30.1 months (148). In
our study, we also found the mean resolution time to be 15 months. Furthermore, the duration did
not correlate with the disease severity when it comes to a specifically poor range of motion during
frozen shoulder. Reeves found that a shorter period of the so-called painful stage was associated
with a shorter recovery time (148). The shortest mean duration of recovery time after non-operative
treatment was 12 months in a well-documented 7-year follow-up study (159), and the longest was
20 months, as with our patients (113).
TABLE 7. Literature on outcome of the natural course of frozen shoulder.
N
Follow-
up
in years
DURATION
in monthsMOTION PAIN FUNCTION
REEVES
et al 41 5-10 30
54% slight
restriction
7% limited
function
DIERCKS &
STEVENS 45 2 15
7% marked
restriction
CS**
89/100.
89%
CS>80.
VASTAMÄKI
et al 52 9 15
6% inferior to
contralateral
shoulder
94%
VAS-
pain
at rest
<3/10
CS 83/100.
STT*
11/12.
*STT = Simple Shoulder Test, **CS = Constant-Murley Score
We determined the natural history of our idiopathic frozen shoulder patients, the length of
symptoms, recovery of ROM, pain relief, and function at a mean 9 years follow-up. The results
50
were similar to those reported by Diercks et al (44), but better than those reported by Reeves et al
(148), their patients took twice as long to recover from their frozen shoulder. This difference was
unexplainable. Diercks stated that supervised neglect for patients with FS yields better outcomes
than does intensive physical therapy and passive stretching. Our study yielded similar outcome
results: Patients in the present natural course, or untreated group had better pain relief, ROM, and
function than did those with the present non-operative, meaning conservative treatment, such as
physiotherapy group. The present study and the literature show most patients with idiopathic FS as
experiencing resolution without any treatment. We believe it is important to be able to tell a patient
with some confidence that an idiopathic frozen shoulder generally recovers well without any
restriction of motion or pain.
6.2. Long-term range of motion and function after frozen shoulder
Of Reeves’ frozen shoulder patients, 39% had a full recovery in the natural course, and 54% had a
clinically detectable limitation with no effect on their normal functional activities. This amounts to
93% with no effect on patients’ daily function. Of our 51 natural-course patients, a similar 94%
eventually had ROM as good as on the contralateral side. Binder et al reported that 12% of patients
after non-operative treatment had severe restriction, and 28% had mild restriction at 4 years (9).
Shaffer et al reported that 30% had measurable restriction at 7 years (159). However, even better
results after non-operative treatment have occurred (46). After non-operative treatment, 92% of the
patients in the present study achieved ROM similar to that of the contralateral shoulder, suggesting
that the recovery of ROM after non-operative treatment for an idiopathic frozen shoulder is better
than reported earlier. The patients with a specifically poor range of motion during frozen shoulder
had as good ROM in long-term follow-up as did others, except for the external rotation that was
inferior in these patients (40.4 vs 52.7 ). Also, our patients with a poorer final Constant Score did
not have specifically poor ROM during frozen shoulder.
Numerous retrospective studies suggest that the duration of symptoms of idiopathic frozen shoulder
may be reduced by manipulation under anesthesia (45,52,81,109,127,127,143,146,
174,175,190,195,196). However, the very long-term clinical outcome after MUA is unknown, with
only one questionnaire survey available (49). In 1992, a substantial increase in ROM and
appropriate pain relief were evident in 26 patients following a mean 7 years after MUA for
spontaneous frozen shoulder (185,186). ROM also improved to normal in a retrospective study with
51
32 patients on average 13 weeks after MUA, and lasted for at least 5 years (143). Improvement in
ROM lasted at least 3.5 years in one retrospective study of 246 patients (175) and 5 years in another
study with 145 patients (52). For 18 patients, 15 years after MUA, forward flexion estimated by the
patients reached 180° and external rotation reached 90° in almost all shoulders. This was, however,
a questionnaire study (49). The patients were a mean 66 years old at the time of the survey. A
healthy population very seldom attains such a perfect ROM at that age, and patients tend to
overestimate ROM in questionnaires.
The results of Farrell (49) resemble those of our Study II. Here, ROM had recovered to normal at
the 7-year evaluation but had deteriorated by 6% to 16% during the next 16 years, however,
reaching the contralateral level. Such deterioration could be explained by the patients’ aging.
Thomas et al (175) report that 3.5 years after MUA, the Oxford Shoulder Score (OSS) improved
from a mean of 27 to 44. Flannery et al report that 5 years after MUA, the OSS improved from a
median of 12 to 40 (52). In Farrell’s questionnaire survey with a follow-up time of 15 years, the
SST averaged 9.5 of 12 and the American Shoulder and Elbow Surgeons score 80 of 100 (49). Our
present Study II showed that, of 15 patients, 12 reached the age- and sex-adjusted normal Constant-
Murley score, and the SST averaged 10 of 12. Diercks considered 80 points out of 100 to indicate a
normally functioning shoulder (44).
The full range of motion of the shoulder joint does not remain the same throughout life, but
deteriorates with age (7). In addition, “although shoulder abduction is reported to be 180 degrees,
biomechanical studies show that it is rarely greater than 170 degrees” (110). In Study II, ROM also
deteriorated between 7 and 23 years after manipulation. However, MUA leads to full improvement
of ROM and leaves no pain in 90% of cases also in the long run. For patients with excessively
severe pain and stiffness not responding to non-operative treatment in 6 months and being unable
to work, MUA can be considered as one treatment option; however, with respect to the RCT
studies, only in selective, rare cases.
Concerning the long-term ROM of diabetic frozen shoulder, the primary outcome of this study is
that the ROM of diabetes patients’ once frozen shoulder does reach the same level as that of their
unaffected contralateral shoulder. During frozen shoulder, diabetes patients’ ROM was similar to
non-diabetes patients’ ROM. Nor did Cinar (30) find any significant differences in preoperative
functional scores between diabetic and non-diabetic frozen shoulder patients. Follow-up ROM of
diabetic patients was inferior to ROM of non-diabetic patients in all directions. Griggs (63) also
52
reported that diabetes in frozen shoulder patients is associated with worse outcome of ROM. The
results of arthroscopic capsular release for frozen shoulder in diabetic patients are also less good
concerning ROM (30). Diabetic patients had inferior results also after open surgical release (130).
However, in Study V, at follow-up, the ROM of the diabetes patients’ once frozen shoulder did
reach the same level as that of their non-affected shoulder. According to the present study, frozen
shoulder does not make diabetes patients` shoulder ROM inferior to their own other, non-affected
shoulder. The other studies lack comparison of ROM to their own contralateral level.
Concerning function in patients with diabetes, Constant-Murley Score results were in accordance
with our hypothesis. However, diabetes patients self-evaluated their function as inferior to that of
non-diabetes patients in the Simple Shoulder Test. Cinar (30) reported the CM score in those with
diabetes as 82 versus 94 in the others(p<0.05) Omari (130) an ASES (American Shoulder and
Elbow Score) score 61 vs. 75, and Jenkins (81) an Oxford Shoulder Score 42 vs. 45 (p<0.001).
Callinan et al. (27) found that diabetes patients’ gain in flexion 6 weeks after hydroplasty was 7.5
degrees inferior to that of those without diabetes. However, in their study, all without diabetes also
received intra-articular corticosteroids, but some with diabetes and concerned about glucose control
received no corticosteroid. It is thus difficult to compare results, considering the differing treatment
protocols.
6.3. Pain after frozen shoulder
We found no published studies regarding pain in an untreated frozen shoulder. Diercks et al stated
that 89% of their patients had normal or near-normal painless shoulder function, but they used only
the Constant-Murley questionnaire and not a VAS (44). In the present study, 94% of the patients
reported pain at rest as less than 3/10 on a VAS, showing good recovery. The threshold level of 3
on the Visual Analogue Scale was chosen because patients who report pain level 3/10 on VAS are
interpreted to have minimal pain and low irritability of the shoulder (84). Concerning non-operative
treatment, 43% of patients were reported to have persistent pain at 3 years (165), 35% mild pain at 7
years (159), and 27% mild or moderate pain at 1.8 years (63). With the non-operatively treated
patients in the present study, pain at rest was less than 3/10 in 91%.
Bulgen followed patients for only 8 months. He found, in a prospective and randomized study (20),
that the decrease in pain was at its greatest by the fourth week of treatment. After that time, pain
53
continued to slowly decrease. He suggested that local steroid injection should be the first treatment
of choice, and that treatment should be given during the first month.
Concerning pain after MUA, “Pain diminished from a mean VAS score of 7.6 to 1.5 in 31 patients
at 14 months’ follow-up after MUA (75) and from a median VAS score of 8 to 1 for 146 patients at
a mean 5-year clinical follow-up (52). In a 15-year long-term questionnaire review of 18 patients,
only two experienced transitional pain in the manipulated shoulder (49). In this Study II, pain also
was minimal after 23 years, except for two arthritic shoulders.
Concerning pain after diabetic frozen shoulder, we found the outcome similar to that of non-
diabetic individuals at rest and during the night, but worse during exertion. In the literature, pain
occurred in 26% of those with diabetes, but in none of those without diabetes (30), and after open
surgical release VAS pain averaged a respective 4.3 and 1.1 (130). Several researchers describe
how frozen shoulder causes pain both at rest and during exertion, but especially during the night
time (68,109,163). For this reason, we wanted to evaluate the pain on the VAS scale in three
different ways: pain at rest, pain during exertion/activity, and pain during the night time.
We found two fractures of the glenoid rim (13%). This is a rather high complication rate.
Complications related to MUA are unusual, but they do exist (121,131). Magnusson reported one
glenoid fracture during manipulation under anesthesia for adhesive capsulitis (105). However, no
difference was detected in our two patients’ final follow-up pain, ROM, or function, when
compared to others. Nor did their range of motion differ at discharge, a few days after the
manipulation.
6.4. Outcome of postoperative stiff shoulder after open rotator cuff repair
Rotator-cuff repair (RCR) is a common orthopedic procedure (1,11,12,57,58,89-
91,160,183,184,200). Postoperative stiff shoulder after RCR is a common complication
(54,55,72,173,188,191,199), resolving normally in 6 months. In 2004, Simon Bell from Australia
stated that after open RCR incidence of postoperative stiffness was 25% (9th International
Conference for Shoulder and Elbow Surgery, Washington, DC), but he never published his results.
In other studies, incidence was 3% after open RCR (106), and 16% after open revision surgery (8).
In our Study III, the incidence was 20%. The reason for differing incidences may be the fact that in
54
Study III, diagnosis of postoperative stiffness occurred at an earlier stage, just 6 weeks after surgery
and after 2 to 5 days of physiotherapy. In a similar population of 209 patients after open RCR (177),
when the inclusion criterion fell into the lower quartile of passive ROM, stiffness incidence at 6
weeks after surgery was 17%. Postoperative stiffness of the shoulder joint shoulder tends to recover
within 6 months. When evaluating postoperative stiffness at 3 or 6 months after RCR, incidence
should be even lower. In a review of 500 rotator cuff repairs, when evaluated at 9 months, 4% had
significant arthrofibrosis after RCR (106) and 5% after arthroscopic RCR (76).
Duration of symptoms of postoperative stiff shoulder is not reported precisely. Brislin et al (14) did
state that their patients’ postoperative stiffness after arthroscopic RCR resolved with almost no
deficit of ROM at all (<10% passive loss in any plane) in a mean 5 months after the operation, in 14
of 23 patients. The other 39% still had significant lack of passive ROM at 5 months (14). In Study
III, postoperative stiffness lasted approximately 6 months and had resolved before one year. Thus
the length of the symptoms was shorter than for idiopathic frozen shoulder.
Motion usually improves steadily between 6 weeks and 76 weeks postoperatively, reaching nearly
complete recovery (177). In Study III, ROM began to improve on average at 3 months and had
improved to almost normal (93% of ROM in the control group) on average by 6 months without
any treatment other than physiotherapy. External rotation resolved first, in 3 months, as occurred
also in Cho`s study of 15 patients with arthroscopic RCR of preoperatively stiff shoulders (29).
Pain caused by postoperative stiffness after RCR has received any mention only rarely. Pain scores
improved from 5.6 to 2.0 among patients with stiff shoulders (p = 0.590) and from 5.1 to 1.7 among
ones free of stiffness (p = 0.820). With Trenerry’s patients, some of them already experiencing
preoperative stiffness, pain subsided by 24 weeks (177). In Study III, pain resolved well.
Flatow (137) found no statistically significant difference between mean 1-year ASES scores among
stiff-shoulder patients and ones without stiffness, as well as Constant-Murley scores of 77 and 74.
For the present population, Constant-Murley scores for postoperative frozen shoulders for 56%
averaged 78, being 80. Thus, postoperative stiff shoulder does not seem to affect shoulder
function in the long term.
After rotator-cuff repair, postoperative stiff shoulder is an important complication that should
receive more recognition. However, it resolves without any surgery within 6-12 months quite well.
Its etiology still remains unknown. Warner & Holovacs, in their chapter on acquired shoulder
stiffness, conclude that “It is not clear whether the cause of posttraumatic or postsurgical capsulitis
55
is different from that of idiopathic adhesive capsulitis or whether some patients simply develop
adhesive capsulitis in the context of trauma or surgery” (201). Our study showed that postoperative
frozen shoulder was associated with a sound biceps tendon. This strengthens Mansat et al.’s finding
of the more tissue is present, the greater risk for postoperative frozen shoulder.
6.5. Does timing of MUA for frozen shoulder associate with outcome?
To our knowledge, only four published papers handle the effect of timing of manipulation under
anesthesia (50,52,136,175). These four present very conflicting results on the effect of timing on the
outcome. Flannery (52) examined 145 patients with a mean follow-up time of 5 years and found
that MUA that was performed less than 9 months from the beginning of symptoms yielded better
results (Oxford shoulder Scores) than did MUA after 9 months. Mobility and VAS pain were also
better than among those manipulated after 9 months. Kelly (50) reported that the modified Neer
questionnaire scores of patients manipulated during 6 months after onset of symptoms did not differ
from scores of the others. Kelly stated that manipulation can thus be considered a viable treatment
in the early stages of frozen shoulder. Pap (136) found that the patients manipulated at a mean 8.4
months from the beginning of symptoms had a better outcome than did those manipulated at a mean
5.7 months. He recommended manipulation at stage III, and at stage II only if the pain is already
decreasing and limitation in ROM is the main symptom. Thomas (175), in his questionnaire survey,
found no correlation between timing and the results.
We can add some weight to Flannery`s conclusion that MUA before 9 months results in a better
outcome. However, clinical significance cannot be considered as remarkable as statistical
significance.
Flannery (52) also reported that patients who were manipulated less than 9 months after symptom
onset had better ROM in all directions, but only their gain in external rotation reached statistical
significance, 77° vs. 72°, p=0.049. Based on the long clinical experience of those senior in our
study group, we earlier believed that early manipulation, MUA performed before 6 months from
onset of symptoms, may lead to a relapse. This was not shown in the Study IV. Nowadays, we
prefer intra-articular corticosteroid injections at the earlier stages of the disease during the
inflammation period.
56
Summarizing the results of Study IV and Colville`s (52) findings, we all found that MUA before 9
months yielded significantly better results than did treatments with MUA after 9 months. In
addition, Study IV showed that MUA between 6 and 9 months yielded better ROM in abduction
and external rotation. Clinically the difference was, 10 for both. On the other hand, Thomas’s
survey found no differences concerning timing of MUA (175). One reason may be differing
inclusion criteria. Thomas included patients with good preoperative flexion and abduction as great
as 170° and external rotation up to 70°. We find it challenging to make a definite diagnosis of
frozen shoulder along with such a good range of motion. Moreover, no questionnaire survey is as
accurate as a clinical examination. Colville’s (52) study included no figures on results for patients
manipulated between 6 and 9 months, which perhaps would have strengthened his findings. Today,
we rarely manipulate, but if needed, preferably between 6 and 9 months after symptom onset.
Concerning pain, we found no articles showing influence of timing. Flannery (52) used VAS pain
intensity score, but the results did not show any effect of timing. However, our results showed
significant influence, VAS pain at rest was 0.2 vs. 1.2, p=0.039 and at night 0.6 vs. 2.0, p=0.049,
but the difference in pain with exertion 0.7 vs. 2.5, p=0.114 was not significant. Minimal clinically
important difference (MCID) in the visual analogue scale is 1.2 to 1.4 cm (56,171) and 3.0 cm after
adequate pain control (92), meaning that our results may not be clinically veryrelevant. The
minimum clinically significant difference in Visual Analogue Scale pain score does not differ with
severity of pain (85).
When it comes to function, Flannery et al. (52) showed that MUA before 9 months yielded a
significantly better Oxford Shoulder Score than did MUA after 9 months, 13 vs. 16, (p=0.0024).
Study IV had similar results: patients manipulated between 6 and 9 months had a significantly
better Simple Shoulder Test scores than did other patients (p=0.002). However, some feel that a
two-point difference on the Simple Shoulder Test is clinically significant (172). In the present
study, the difference was only 1.8 points, not 2.0 (9.5 vs 11.3). It is also difficult to compare earlier
results, because treatment methods vary. In Flannery’s study (52), an intra-articular steroid injection
was added to MUA; Study IV involved no intra-articular steroid injections.
In consideration of manipulation, a favorable option seems to be to avoid performing it too early or
too late; if done late, more than 9 months after symptom onset, the results deteriorate. In
randomized controlled trials, MUA has not been more favorable than other treatments (86,145). For
instance, Quraishi et al. (145), in their RCT, found that hydrodilatation led to significantly better
results than MUA at 6 months. VAS was 2.7 in that MUA group and 1.7 in the hydrodilatation
57
group, p<0.0001). CS was 59.5 for MUA and 65.9 for the hydrodilatation group, p=0.02. Adolfsson
and his group stated that the minimal important change in Constant-Murley score is 17 for patients
with subacromial pain (73). ROM was similar between the groups.
On the other hand, many researchers defend MUA as the treatment of choice. If supervised neglect
or non-operative treatment has not helped sufficiently, and limitation of shoulder motion is too
burdensome, manipulation can be considered in rare, selective cases, preferably after 6 months but
before 9 months after symptom onset.
6.6. Limitations of the study
The current study has several limitations. First, we used the Constant-Murley Score (Studies I-V),
popular in Europe for functional assessment of the shoulder. Today, the relevance of the Constant-
Murley score is disputed, and for frozen shoulder it may not be the best choice, especially with
muscle strength included (132). The strength of a normal shoulder often differs by gender and
deteriorates with age (83). Thus, the Constant-Murley Score may also decrease in absolute value
while still reflecting a normal score.
Second, due to the retrospective nature of this study, we did not obtain Constant-Murley Scores or
Simple Shoulder Test scores at the time the patients were initially seen (Studies I-V). Although we
place great value on longitudinal assessment of outcome measures, only ROM and strength
measurements were available. We excluded patients whose medical records inadequately provided
ROM, and included only those with appropriate records.
Third, it is difficult to estimate the influence of MUA (II, IV), because the natural course of frozen
shoulder is mostly beneficial. Our indications for manipulation were therefore stringent. Fourth, the
patient population for Study II was small. We could reach only 15 of the original patients, 4 were
dead, and some others were too old to attend the last follow-up evaluation because of the very long-
term follow-up time. Fifth, active internal rotation of the arm behind the back was assessed by the
method we have used for decades, by determining the vertebral level reached by the dorsum of the
hand. Recent authors (66) have questioned the accuracy of this method and suggest their measuring-
tape method, the distance between the C7 spinous process and the point reached.
58
Sixth is a possible selection bias (I, II, III, V) because our hospital is a third-level referral hospital,
meaning perhaps with more difficult cases, but we also have many private patients coming directly
to our hospital. Seventh, the arm was immobilized in an abduction splint for a mean 5 weeks in
most cases (Study III). Today, most shoulder surgeons do not use a splint, and even using a sling,
they mobilize the arm early. We found, however, no correlation between incidence of postoperative
stiff shoulder and use of the abduction splint. As a matter of fact, abduction splints were used more
often and longer for our control patients (80% vs. 93%, mean 4 vs. 5 weeks).
Eighth, concerning preoperative ROM in Study IV, we obtained exact figures for flexion and
abduction, but external and internal rotation was mostly listed only as “severely restricted.” We
excluded patients whose ROM was inadequately documented in their medical records, and included
only patients with appropriate records for flexion and abduction. Ninth, a possible selection bias
may arise from the number of drop-outs. We were able to include in the study 234 patients. The
participation rates were 67% (I), 58% (II), 67% (III), and 71% (IV).This may be considered
acceptable with regards to the very long follow-up times and the fact that the patients live all over
Finland. However, the purpose of this academic dissertation was to study the very long-term
outcome of frozen shoulder, and this large retrospective material gave us the possibility.
6.7. Strengths of the study
First, all the patients are examined clinically. We believe that clinical examination is crucial when it
comes to exploring such important factors involving the shoulder joint as movement and range of
motion. As Hazleman (70) and also Bulgen (20) have previously found, patients often may claim
that they have regained full movement, but when tested objectively, that has not been so. Thus,
objective, clinical examination of the range of motion is very important.
Second, the follow-up time was long, several years (III, IV) or, even decades (I, II, V). One paper
presents the longest clinically examined series on outcome of frozen shoulder after manipulation
under anaesthesia (II).
Third, we have had strict inclusion criteria. All the patients were examined at first consultation by
an orthopedic surgeon experienced in shoulder surgery. Thus, we believe that diagnosis has been
appropriate from the beginning. Only patients with appropriate status recordings, measured degrees
of flexion, abduction, and external rotation (I, II, III, V) or that of flexion and abduction with
severely decreased rotations (IV) were included.
59
Fourth, some studies included in this thesis work are exceptional concerning the large population.
One article presents, to our knowledge, the largest-ever clinically examined series published on the
true natural course of frozen shoulder (I), another, the largest clinically examined series published
on the outcome of postoperative stiff shoulder (III).
This study covers both idiopathic/primary and secondary frozen shoulder, whether secondary means
post-surgical or systemic, such as those with diabetes.
6.8. Recommendations for future research
The fact that populations are aging, and the number of patients with diabetes is increasing in every
country (Diabetes Atlas, IDF), also makes frozen shoulder an epidemiologically increasing
condition. It causes intense pain, deteriorated function, and inability to work. In addition, its true
etiology still remains somewhat of an enigma, making it an important focus for research. Further
studies are vital, and we recommend prospective, randomized controlled trials in which different
treatment methods are judged against the natural course of frozen shoulder, and both efficacy,
effectiveness, and cost effectiveness are considered. Considering the intense pain that also may
produce mental stress often with inability to work, one interesting possibility concerning
physiotherapy might be some kind of group therapy with peer support.
60
7. MAIN FINDINGS
Idiopathic frozen shoulder generally recovered well throughout its natural course without pain or
restriction of motion. The worst frozen shoulder cases with the poorest range of motion during the
condition also recovered as well as the others except for external rotation. Diabetic frozen shoulder
also recovered to the contralateral level concerning range of motion.
The outcome of MUA for frozen shoulder was generally good with long-term follow-up. Timing
had some association with outcome of manipulation of the idiopathic frozen shoulder. Concerning
postoperative stiff shoulder after open rotator cuff repair, this was a common finding with an
incidence of 20%. It generally resolved in 6 months.
8. CONCLUSIONS
Codman originally described a self-limiting natural history of frozen shoulder that lasts less than 2
years. In this project, we were able to confirm Codman`s view (I). We recommend supervised
neglect with, throughout, patient information and an explanation of the condition and what can be
expected. Systematic status records should be kept, from which both the clinician and the patient
can monitor recovery.
The natural course of frozen shoulder, though benign, often includes a long period of pain and
deteriorated function and inability to work. These are the main reasons for interventions other than
supervised neglect. At the beginning of the condition, during the inflammatory phase, an intra-
articular corticosteroid injection can be considered. Concerning physical therapies, during the first
stages, we recommend concentrating on reducing the pain, and only after that, regaining the ROM.
Although retrospective series show good results of MUA, RCTs do state that MUA does not add
benefit. If supervised neglect or conservative treatment is insufficient, manipulation under
anesthesia should only be considered in rare, selective cases. In conclusion, the long-term outcome
of frozen shoulder is good.
61
ACKNOWLEDGEMENTS
Research for this study was carried out in collaboration between Orton Orthopaedic Hospital, Orton Research Institute, Orton Foundation in Helsinki, and the University of Helsinki, Finland. The patients for study IV were treated and examined at Rauma Hospital, Rauma, Finland. This work was financially supported by the Helsinki University Hospital Research Fund (EVO), the Finnish Society for Surgery of the Hand, and The Finnish Medical Foundation. I express my appreciation to all the patients who participated in this study.
I truly respect the important work the Orton Research Institute does, as well as Orton’s dedaces-long encouragement for young doctors to do scientific research. I owe my deepest gratitude to my supervisor, Docent Martti Vastamäki. His encouragement and guidance were essential for completion of this work.
My sincere thanks to co-author Leena Ristolainen, PT, DSc, for her collaboration, statistical advice and the crucial help in literature search. My warm thanks go also to co-author Jyrki Kettunen for statistical advice and guidance, to co-author Lassi Varjonen, M.D., who provided me with his extensive material of manipulated frozen shoulders at Rauma Hospital for Study V, and Professor Pertti Aarnio for his support in utilizing that material.
I would like to extend my warmest thanks to research nurses Ella Haaranen at Orton Hospital for her help with the enormous amount of office work and practical matters related to this study, and Ulla Hohtari-Kivimäki at Rauma Hospital. What would we do without research nurses!
I wish to express my gratitude to the official reviewers of this thesis, Docent Ville Äärimaa and Docent Janne Lehtinen for their constructive criticism and valuable advice during the final preparation of this work.
I owe my deepest gratitude to Carol Norris, PhD, for her quick and superb language revision work during our many years of cooperation. This lady’s energy, capability and expertise are admirable.
I am grateful to Katri Laimi, MD, PhD, for helping me to see something that was already there; to discover the common thread of my thesis. I would like to thank Professor Hannu Aro for his encouraging words and the crucial six words that really inspired me to start the final process in finishing this long project.
My thanks to Docent Veli-Matti Tiainen and all the other gentlemen at the Orton Research Institute for many interesting discussions and cheerful lunch breaks during long, long days (and years) of research. I would also like to thank Professor Jouko Miettunen from the University of Oulu for a great deal of valuable advice concerning reviews along the years.
I would like to thank shoulder surgeons Wayne (Buz) Burkhead, MD, for all his kind supervising at the shoulder unit of the Carrell Clinic in Dallas, USA, and Sumant Krishnan, MD for his useful advice in surgery and for encouraging me to “accept the challenge”.
You don’t become a surgeon overnight. I would like to thank all the colleagues who have guided and taught me during the years of specialization in Helsinki University Hospital, Oulu University Hospital, Orton Orthopaedic Hospital, Forssa Hospital, Jorvi Hospital and Turunmaa Hospital.
I highly appreciate a working environment which encourages open consultation, discussion and co-operation. For this, I would like to express my gratitude to all my colleagues at , Turku University Hospital (TYKS), especially the great orthopedic surgeons Kari Isotalo, Mika Junnila, Jani
62
Knifsund, Kaisa Lehtimäki, Petri Paakki, Katri Pernaa, Niko Strandberg and Stefan Suvitie, plastic surgeon Tarja Niemi and radiologists Kimmo Mattila and Jussi Kankare, just to mention a few.
I would like to warmly thank the hand surgical team in TYKS. I truly feel that I have found my ideal field, and I have the pleasure to work with the greatest team ever, with skillful professional nurses such as Jaana Aaltonen, Jonna Andsten-Lehtonen, Pauliina Kaukovalta, Heidi Pehkonen, Mari Kallio, Anu Jalonen, Teija Rantala, Elina Oikarinen, Outi Harri and hand therapists Katariina Kallanranta, Mimmi Evijärvi and Kristiina Ahti. It is an honor to work with great hand surgeons Hanna-Stiina Taskinen, whose skills as our boss I truly admire, Nina Tamminen, Merlin Mäesalu and Tero Kotkansalo.. Especially I would like to thank Tero, with whom I have had a chance for many interesting and instructive consultations, discussions and many lighthearted debriefings on long Tuesday afternoons. I would like to thank all my friends in music, poker and other hobbies. During these past years, I have especially received support and encouragement from a few wonderful ladies, with whom I have had the honor of being close friends for many years: Sanna Valliaro, Susanna Lappalainen, and Christine Shaaban, thank you for everything!
Work and research means a great deal to me. But family is everything. This thesis is dedicated to my daughter Victoria, the light of my life, and my parents, Anita and Martti. I would also like to thank my big sisters Liisa Hakaste and Pirjo Vastamäki. My warmest thanks go to my dear older brothers Erkki Paatonen and Olli Paatonen, who have supported me all these years, and who still are (and will probably always be) my idols. And Erkki, thank you for bringing my head down from the clouds, yes, tens of times, and thank you for positively kicking me in the butt with this whole thesis project! I love you!
I owe my deepest gratitude to my dear mother Anita, for all her support, encouragement, upbringing, help, love, babysitting and caring. Without you, this would have never happened.
And, dear dad, I truly respect the energy for both scientific and clinical work that is still showing strong in your everyday life. Thank you for trusting that my scientific awakening would come someday. It came, and oh, boy, has it felt good to do research ever since!
The past year has not been easy. Who would have guessed! But here I am, alive and kicking, with the brand new thesis in my hand. Strong people take the step forward. Thank you friends and family, I can’t wait to spend more time with you! Towards next challenges in research and life!
In Kaarina, in April 2015,
Heidi Vastamäki
63
REFERENCES
1. Adamson G, Tibone J. Ten-year assessment of primary rotator cuff repairs. J Shoulder Elbow Surg. 1993;2:57-63.
2. Allander E, Björnsson OJ, Olafsson O, Sigfusson N, Thorsteinsson J. Normal Range of Joint Movements in Shoulder, Hip, Wrist and Thumb with Special Reference to Side: a Comparison between Two Populations. Int J Epidemiol. 1974;3:253-261.
3. Andersen NH, Söjbjerg JO, Johannsen HV, Sneppen O. Frozen shoulder: Arhtroscopy and manipulation under general anesthesia and early passive motion. J Shoulder Elbow Surg. 1998;7:218-222.
4. Arkkila PE, Kantola IM, Viikari JS, Ronnemaa T. Shoulder capsulitis in type I and type II diabetic patients: association with diabetic complications and related diseases. Ann Rheum Dis 1996;55:907-914.
5. Arroll B, Goodyear-Smith F. Corticosteroid injections for painful shoulder: a meta-analysis. Br J General Practice 2005;55:224–228.
6. Arslan S, Celiker R. Comparison of the efficacy of local corticosteroid injection and physical therapy for the treatment of adhesive capsulitis. Rheumatol Int. 2001;21:20-23.
7. Barnes CJ, Van Steyn SJ, Fischer RA, The effects of age, sex, and shoulder dominance on range of motion of the shoulder. J Shoulder Elbow Surg. 2001;10:242–246-
8. Bigliani LU, Cordasco FA, McIlveen S, Musso ES. Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am. 1992;74:1505-1515.
9. Binder AI, Bulgen DY, Hazleman BL, Roberts S. Frozen shoulder: a long-term prospective study. Ann Rheum Dis. 1984;43:361–364.
10. Binder A, Hazleman BL, Parr G, Roberts S. A controlled study of oral prednisolone in frozen shoulder. Br J Rheumatol 1986;25:288-292.
11. Björnsson HC, Norlin R, Johansson K, Adolfsson LE. The influence of age, delay of repair, and tendon involvement in acute rotator cuff tears: structural and clinical outcomes after repair of 42 shoulders. Acta Orthop. 2011;82:187-192. doi: 10.3109/17453674.2011.566144. Epub 2011 Mar 24
12. Borgmästars N, Paavola M, Remes V, Lohman M, Vastamäki M. Pain relief, motion, and function after rotator cuff repair or reconstruction may not persist after 16 years. Clin Orthop Relat Res. 2010;468:2678-2689 .
13. Bridgman JF. Periarthritis of the shoulder and diabetes mellitus. Ann Rheum Dis 1972;31:69-71.
64
14. Brislin KJ, Field LD, Savoie FH III. Complications after arthroscopic rotator cuff repair. Arthroscopy 2007;23:124-128.
15. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev 2003; Issue 1, Art. No. CD004016.
16. Buchbinder R, Green S, Forbes A, Hall S, Lawler G. Arthrographic joint distension with saline and steroid improves function and reduces pain in patients with painful stiff shoulder: results of a randomised, double blind, placebo controlled trial. Ann Rheum Dis. 2004;63:302–309.
17. Buchbinder R, Hoving JL, Green S, Hall S, Forbes A, Nash P. Short course prednisolone for adhesive capsulitis (frozen shoulder or stiff painful shoulder): a randomized, double blind, placebo controlled trial. Ann Rheum Dis 2004;63:1460-1469.
18. Buchbinder R, Green S, Youd JM, Johnston Renea V. Oral steroids for adhesive capsulitis. Cochrane Database Syst Rev 2006; Issue 4, Art. No. CD006189.
19. Bulgen DY, Hazleman BL, Voak D. HLA-B27 and frozen shoulder. The Lancet 1976; 307:1042–1044.
20. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an evaluation of three treatment regimens. Ann Rheum Dis. 1984;43:353–360.
21. Bunker TD. Time for a new name for 'frozen shoulder. Br Med J (Clin Res Ed). 1985;290: 1233–1234.
22. Bunker TD. Frozen shoulder: unravelling the enigma. Ann R Coll Surg Engl 1997;79:210–213.
23. Bunker TD. Time for a new name for frozen shoulder – contracture of the shoulder. Shoulder Elbow 2009;1:4–9.
24. Bunker TD, Anthony PP. The pathology of frozen shoulder. A Dupuytren-like disease. J Bone Joint Surg Br 1995;77:677-683.
25. Bunker TD, Reilly J, Baird KS, Hamblen DL. Expression of growth factors, cytokines and matrix metalloproteinases in frozen shoulder. J Bone Joint Surg Br. 2000;82:768-773.
26. Burkitt HG, Young B, Heath JW. Wheater’s Functional Histology. A Text and Color Atlas. Third edition. 1999.
27. Callinan N, McPherson S, Cleaveland S, Gardiner Voss D, Rainville D, Tokar N. Effectiveness of Hydroplasty and Therapeutic Exercise for Treatment of Frozen Shoulder. J Hand Therapy 2003, 16:219–224.
28. Cameron RI, McMillan J, Kelly IG. Recurrence of a "primary frozen shoulder": a case report. J Shoulder Elbow Surg, 2000;9: 65-67.
65
29. Cho N, Rhee Y. Functional outcome of arthroscopic repair with concominant manipulation in rotator cuff tears with stiff shoulder. Am J Sports Med. 2008;36:1323-1329. doi: 10.1177/0363546508314402. Epub 2008 Jun 6.
30. Cinar M, Akpmar S, Derincek A, Circi E , Uysal M. Comparison of arthroscopic capsular release in diabetic and idiopathic frozen shoulder patients. Arch Orthop Trauma Surg 2010;130:401-406.
31. Clarke GR. Measurement in shoulder problems. Rheumatol Rehabil. 1976;15:191-193.
32. Codman EA. On stiff and painful shoulders: the anatomy of the subdeltoid bursa and its clinical importance: subdeltoid bursitis. Boston Med Surg J, 1906;154: 613-620.
33. Codman EA. The pathology and treatment of lesions in and about the shoulder joint. Int Doctor. 1926;4:121-131.
34. Codman EA. The Shoulder. Boston, MA. Thomas Todd Co. 1934:216–224.
35. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–164.
36. Dawson J, Shepperd S, Carr A. An overview of factors relevant to undertaking research and reviews on the effectiveness of treatment for frozen shoulder. Shoulder Elbow 2010;2:232–237.
37. De Carli A, Vadalà A, Perugia D, Frate L, Iorio C, Fabbri M, Ferretti A. Shoulder adhesive capsulitis: manipulation and arthroscopic arthrolysis or intra-articular steroid injections? Int Orthop. 2012;36:101-106. doi: 10.1007/s00264-011-1330-7. Epub 2011 Aug 11.
38. Degreef I, Debeer P. Post-vaccination frozen shoulder syndrome. Report of 3 cases. Acta Chir Belg. 2012;112:447-449.
39. Dehghan A, Pishgooei N, Salami MA, Zarch SM, Nafisi-Moghadam R, Rahimpour S, Soleimani H, Owlia MB. Comparison between NSAID and intra-articular corticosteroid injection in frozen shoulder of diabetic patients; a randomized clinical trial. Exp Clin Endocrinol Diabetes. 2013;121:75-79. doi: 10.1055/s-0032-1333278. Epub 2013 Feb 20.
40. De Jong BA, Dahmen R, Hogeweg JA, Marti RK. Intra-articular triamcinolone acetonide injection in patients with capsulitis of the shoulder: a comparative study of two dose regimens. Clin Rehabil. 1998;12:211–215.
41. DePalma AF. Loss of scapulohumeral motion (frozen shoulder). Ann Surg, 1952;135:193-204.
42. Desplats H. De l'atrophie musculaire dans la peri-arthrite scapulo humerale.(French). Gazette Hebdomadaire Med Chir. 1878;24:371.
43. Dias R, Cutts S, Massoud S. Frozen shoulder. BMJ 2005;331:1453–1456.
66
44. Diercks RL, Stevens M. Gentle thawing of the frozen shoulder: a prospective study of supervised neglect versus intensive physical therapy in seventy-seven patients with frozen shoulder syndrome followed up for two years. J Shoulder Elbow Surg. 2004;13:499–502.
45. Dodenhoff RM, Levy O, Wilson A, Copeland SA. Manipulation under anesthesia for primary frozen shoulder: effect on early recovery and return to activity. J Shoulder Elbow Surg. 2000;9:23–26.
46. Dogru H, Basaran S, Sarpel T. Effectiveness of therapeutic ultrasound in adhesive capsulitis. Joint Bone Spine 2008;75:445–450.
47. Dudkiewicz I, Oran A, Salal M, Palti R, Pritsch M. Idiopathic adhesive capsulitis: long-term results of conservative treatment. Israel Med Assoc J. 2004;6:524–526.
48. Duplay S. De la peri-arthrite scapulo-humerale et des raideurs de l’epaule qui en sont la consequence. Arch Gen Med 1872;20:513-542.
49. Farrell CM, Sperling JW, Cofield RH. Manipulation for frozen shoulder: long-term results. J Shoulder Elbow Surg. 2005;14:480–484.
50. Fazzi UG, Kelly IG. Is there a continued role for closed manipulation in adhesive capsulitis of the shoulder -when should it be used? J Shoulder Elbow Surg, 1999;8:554.
51. Favejee MM, Huisstede BM, Koes BW. Frozen shoulder: the effectiveness of conservative and surgical interventions-systematic review. Br J Sports Med. 2011;45:49-56.
52. Flannery O, Mullett H, Colville J. Adhesive shoulder capsulitis: does the timing of manipulation influence outcome? Acta Orthop Belg. 2007;73:21-25.
53. Fox A, Board TN, Srinivasan MS. Improvement in shoulder function following manipulation for adhesive capsulitis: how long does it last? J Bone Joint Surg Br. 2006;88 (Suppl I):138-139.
54. Franceschi F, Papalia R, Palumbo A, Vasta S, Maffulli N, Denaro V. Management of postoperative shoulder stiffness. Sports Med Arthrosc Rev. 2011;19:420-427.
55. Galatz LM, Griggs S, Cameron BD, Iannotti JP. Prospective longitudinal analysis of postoperative shoulder function: a ten-year follow-up study of full-thickness rotator cuff tears. J Bone Joint Surg Am. 2001;83:1052-1056.
56. Gallagher EJ, Liebman M, Bijur PE. Prospective validation of clinically important changes in pain severity measured on a visual analog scale. Ann Emerg Med. 2001;38:633-638.
57. Gazielly DF, Gleyze P, Montagnon C. Functional and anatomical results after rotator cuff repair. Clin Orthop Relat Res. 1994;304:43-53.
58. Goutallier D, Postel JM, Radier C, Bernageau J, Zilber S. Long-term functional and structural outcome in patients with intact repairs 1 year after open transosseous rotator cuff repair. J Shoulder Elbow Surg. 2009;18:521-528.
67
59. Green S, Buchbinder R, Glazier R, Forbes A. Systematic review of randomised controlled trials of interventions for painful shoulder: selection criteria, outcome assessment, and efficacy. BMJ 1998;316:354–360.
60. Green A, Griggs S, Ahn A. Idiopathic adhesive capsulitis: a prospective outcome study. Orthop Trans. 1998-1999;22:59.
61. Grey RG. The natural history of "Idiopathic" frozen shoulder. J Bone Joint Surg. 1978; 60-A: 564.
62. Griesser MJ, Harris JD, Campbell JE, Jones GL Adhesive capsulitis of the shoulder: a systematic review of the effectiveness of intra-articular corticosteroid injections. J Bone Joint Surg Am. 2011;93:1727-1733.
63. Griggs SM, Ahn A, Green A. Idiopathic adhesive capsulitis: a prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am. 2000;82:1398–1407.
64. Haggart GE, Digman RJ, Sullivan TS. Management of the frozen shoulder. JAMA. 1956;161: 1219-1222.
65. Hamdan TA, Al-Essa KA. Manipulation under anaesthesia for the treatment of frozen shoulder. Int Orthop 2003;27:107-109.
66. Han SH, Oh KS, Han KJ, Jo J, Lee DH. Accuracy of measuring tape and vertebral-level methods to determine shoulder internal rotation. Clin Orthop Relat Res. 2012;470:562–566.
67. Hanchard N, Goodchild L, Thompson J, O’Brien T, Davison D, Richardson C, et al. Evidencebased clinical guidelines for the diagnosis, assessment and physiotherapy management of contracted (frozen) shoulder. London: Chartered Society of Physiotherapy; 2011. URL: www.csp.org.uk/skipp. Accessed 11 March 2011.
68. Hand GCR, Athanasou NA, Matthews T, Carr AJ. The pathology of frozen shoulder. J Bone Joint Surg Br. 2007;89:928–932.
69. Hand C, Clipsham K, Rees JL, Carr AJ. Long-term outcome of frozen shoulder. J Shoulder Elbow Surg. 2008;17:231–236.
70. Hazleman BL. The painful stiff shoulder. Rheumatology 1972;11:413-421.
71. Hill JJ Jr et al. Manipulation in the treatment of frozen shoulder. Orthopedics. 1988;11:1255-1260.
72. Holloway GB, Schenk T, Williams GR, Ramsey ML, Iannotti JP. Arthroscopic capsular release for the treatment of refractory postoperative or post-fracture shoulder stiffness. J Bone Joint Surg Am. 2001;83:1682-1687.
73. Holmgren T, Oberg B, Adolfsson L, Björnsson Hallgren H, Johansson K. Minimal important changes in the Constant-Murley score in patients with subacromial pain. J Shoulder Elbow Surg. 2014;23:1083-1090. doi: 10.1016/j.jse.2014.01.014. Epub 2014 Apr 13
68
74. Hsieh LF, Hsu WC, Lin YJ, Chang HL, Chen CC, Huang V. Addition of intra-articular hyaluronate injection to physical therapy program produces no extra benefits in patients with adhesive capsulitis of the shoulder: a randomized controlled trial. Arch Phys Med Rehabil. 2012 ;93:957-964. doi: 10.1016/j.apmr.2012.01.021. Epub 2012 Apr 13.
75. Hsu JE, Anakwenze OA, Warrender WJ, Abboud JA. Current review of adhesive capsulitis. J Shoulder Elbow Surg. 2011;20:502–514.
76. Huberty D, Schoolfield J, Brady P, Vadala A, Arrigoni P, Burkhart S. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy 2009;25;880-890.
77. Ibrahim T, Rahbi H, Beiri A, Taylor GJS. Manipulation under anaesthesia for adhesive capsulitis of the shoulder following distension arthrogram. J Bone Joint Surg Br. 2006;88 (Suppl I):138.
78. Jacobs LG, Smith MG, Khan SA, Smith K, Joshi M. Manipulation or intra-articular steroids in the management of adhesive capsulitis of the shoulder? A prospective randomized trial. J Shoulder Elbow Surg. 2009;18:348–353.
79. James M, Stokes EA, Thomas E, Dziedzuc K, Hay EM. A cost consequences analysis of local corticosteroid injection and physiotherapy for the treatment of new episodes of unilateral shoulder pain in primary care. Rheumatology 2005;44:1447-1451.
80. Janda DH, Hawkins RJ, Milch Y, Colo V. Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: a clinical note. J Shoulder Elbow Surg. 1993;2:36-38.
81. Jenkins EF, Thomas WJ, Corcoran JP, Kirubanandan R, Beynon CR, Sayers AE, Woods DA. The outcome of manipulation under general anesthesia for the management of frozen shoulder in patients with diabetes mellitus. J Shoulder Elbow Surg. 2012;21:1492-1498.
82. Jia X, Petersen S, Khosravi A, Almareddi V, Pnnirselvam V, McFarland E. Examination of the shoulder: the Past, the Present, and the Future. J Bone Joint Surg Am. 2009;91:10-18.
83. Katolik LI, Romeo AA, Cole BJ, Verma NN, Hayden JK, Bach BR. Normalization of the Constant score. J Shoulder Elbow Surg. 2005;14:279-285.
84. Kelley MJ, Shaffer MA, Kuhn JE, Michener LA, Seitz AL, et al. Shoulder Pain and Mobility Deficits: Adhesive Capsulitis. Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2013;43:A1-A31. doi:10.2519/jospt.2013.0302
85. Kelly A-M. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J. 2001;18:205-207 doi:10.1136/emj.18.3.205.
86. Kivimäki J, Pohjolainen T, Malmivaara A, Kannisto M, Guillaume J, Seitsalo S, Nissinen M. Manipulation under anesthesia with home exercises versus home exercises alone in the treatment of frozen shoulder: a randomized, controlled trial with 125 patients. J Shoulder Elbow Surg. 2007;16:722-726.
69
87. Krishnan SG, Hawkins RJ, Warren RF. The shoulder and the overhead athlete. Lippincott Williams & Wilkins, 2004.
88. Klapp R. Die operative Erweiterung der Schultergelenkkapsel. Eine Methode zur blutigen Mobilizierung von Schultersteifigkeiten.(German). Zbl Chir. 1916;43:137.
89. Kukkonen J, Joukainen A, Itälä A, Äärimaa V. Operatively treated traumatic versus non-traumatic rotator cuff ruptures: a registry study. Ups J Med Sci. 2013;118:29-34. doi: 10.3109/03009734.2012.715597. Epub 2012 Nov 20
90. Kukkonen J, Joukainen A, Lehtinen J, Aärimaa V. The effect of glenohumeral osteoarthritis on the outcome of isolated operatively treated supraspinatus tears. J Orthop Sci. 2013;18:405-099. doi: 10.1007/s00776-013-0369-2. Epub 2013 Mar 20.
91. Kukkonen J, Kauko T, Virolainen P, Äärimaa V. The effect of tear size on the treatment outcome of operatively treated rotator cuff tears. Knee Surg Sports Traumatol Arthrosc. 2015;23:567-572. doi: 10.1007/s00167-013-2647-0. Epub 2013 Aug 31
92. Lee JS, Hobden E, Stiell IG, Wells GA. Clinically important change in the visual analog scale after adequate pain control. Acad Emerg Med. 2003;10:1128-1130.
93. Lee HJ, Lim KB, Kim DY, Lee KT. Randomized controlled trial for efficacy of intra-articular injection for adhesive capsulitis: ultrasonography-guided versus blind technique. Arch Phys Med Rehabil. 2009 Dec;90(12):1997-2002. doi: 10.1016/j.apmr.2009.07.025.
94. Leung MSF, Cheing GLY. Effects of deep and superficial heating in the management of Frozen shoulder. J Rehabil Med 2008; 40:145–150
95. Lim TK, Koh KH, Shon MS, Lee SW, Park YE, Yoo JC. Intra-articular injection of hyaluronate versus corticosteroid in adhesive capsulitis. Orthopedics. 2014 Oct;37(10):e860-5. doi: 10.3928/01477447-20140924-51.
96. Linsell L, Dawson J, Zondervan K, Rose P, Randall T, Fitzpatrick R et al. Prevalence and incidence of adults consulting for shoulder conditions in UK primary care; patterns of diagnosis and referral. Rheumatology 2006;45:215–221.
97. Lippmann RK. Frozen shoulder, periarthritis, bicipital tenosynovitis, Arch Surg, 1943;47:283-296.
98. Lippmann RK. The frozen shoulder. Surg Clin North Am. 1951;31:367.
99. Loew M, Heichel TO, Lehner B. Intraarticular lesions in primary frozen shoulder after manipulation under general anesthesia. J Shoulder Elbow Surg. 2005;14:16–21.
100. Lorbach O, Anagnostakos K, Scherf C, Seil R, Kohn D, Pape D. Nonoperative management of adhesive capsulitis of the shoulder: oral cortisone application versus intra-articular cortisone injections. J Shoulder Elbow Surg. 2010;19:172-179.
70
101. Lundberg BJ. Arthrography and manipulation in rigidity of the shoulder joint. Acta Orthop Scand. 1965;36:35-44.
102. Lundberg BJ. The frozen shoulder. Acta Orthop Scand 1969;119:1-59.
103. Ma SY, Je HD, Jeong JH, Kim HY, Kim HD. Effects of whole-body cryotherapy in the management of adhesive capsulitis of the shoulder. Arch Phys Med Rehabil. 2013 Jan;94(1):9-16. doi: 10.1016/j.apmr.2012.07.013. Epub 2012 Jul 28.
104. Magnusson R Periarthritis humero-scapularis. J Bone Joint Surg. 1963;45-B:207.
105. Magnusson RA, Taylor DC. Glenoid fracture during manipulation under anesthesia for adhesive capsulitis: a case report. J Shoulder Elbow Surg. 2011;20:e23–e26.
106. Mansat P, Cofield R, Kerssten T, Rowland C. Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
107. Manske RC, Prohaska D. Clinical commentary and literature review: diagnosis, conservative and surgical management of adhesive capsulitis. Shoulder Elbow 2010;2:238–254.
108. Massoud SN, Pearse EO, Levy O, Copeland SA. Operative management of the frozen shoulder in patients with diabetes. J Shoulder Elbow Surg. 2002;11:609–613.
109. Maund E, Craig D, Suekarran S, Neilson A, Wright K, Brealey S, Dennis L, Goodchild L, Hanchard N, Rangan A, Richardson G, Robertson J, McDaid C. Management of frozen shoulder: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2012;16:1-264.
110. McFarland EG. Examination of the Shoulder: The Complete Guide. Thieme, 2006.
111. McLaughlin HL. The frozen shoulder. J Bone Joint Surg. 1958;40-A:960.
112. McLaughlin HL. The "frozen shoulder". Clin Orthop. 1961;20:126-131.
113. Melzer C, Wallny T, Wirth CJ, Hoffmann S. Frozen shoulder: treatment and results. Arch Orthop Trauma Surg. 1995;114:87–91.
114. Meulengracht E, Schwartz M. The course and prognosis of periarthritis humeroscapularis with special regard to cases with general symptoms. Acta Med Scand. 1952;118:350–360.
115. Miller M, Wirth M, Rockwood C Jr. Thawing the frozen shoulder: the ‘‘patient’’ patient. Orthopedics. 1996;19:849–853.
116. Moren-Hybbinette I, Moritz U, Schersten B. The clinical picture of the painful diabetic shoulder – natural history, social consequences and analysis of concomitant hand syndrome. Acta Med Scand 1987;221:73-82.
117. Nagy MT, MacFarlane RJ, Khan Y, Waseem M. The Frozen Shoulder: Myths and Realities. Open Orthop J. 2013;7 Suppl 3:352–355. doi: 10.2174/1874325001307010352
71
118. Namdari S, Green A. Range of motion limitation after rotator cuff repair. J Shoulder Elbow Surg. 2010;19:290-296.
119. Neviaser JS. Adhessive capsulitis of the shoulder. J Bone Joint Surg. 1945;27: 211-222.
120. Neviaser JS. Adhesive capsulitis and the stiff and painful shoulder. Orthop Clin North Am. 1980;11:327-331.
121. Neviaser AS, Hannafin JA. Adhesive capsulitis: a review of current treatment. Am J Sports Med. 2010;38:2346–2356.
122. Neviaser R, Neviaser TJ. The frozen shoulder diagnosis and management. Clin Orthop. 1987;223:59-64.
123. Neviaser AS, Neviaser RJ. Adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2011;19: 536-542.
124. New Zealand Guidelines Group. The diagnosis and management of soft tissue shoulder injuries and related disorders. Wellington: New Zealand Guidelines Group; 2004. URL: www.nzgg.org.nz. Accessed 9 March 2009.
125. Ng CY, Amin AK, Narborough S, McMullan L, Cook R, Brenkel IJ. Manipulation under anaesthesia and early physiotherapy facilitate recovery of patients with frozen shoulder syndrome. Scott Med J. 2009;54:29–31.
126. Nicholson GG. The effects of passive joint mobilization on pain and hypomobility associated with adhesive capsulitis of the shoulder. See comment in PubMed Commons belowJ Orthop Sports Phys Ther. 1985;6:238-246.
127. Ogilvie-Harris DJ, Biggs DJ, Fitsialos DP, MacKay M. The resistant frozen shoulder: manipulation versus arthroscopic release. Clin Orthop Relat Res. 1995;319:238–248.
128. Oh JH, Oh CH, Choi JA, Kim SH, Kim JH, Yoon JP. Comparison of glenohumeral and subacromial steroid injection in primary frozen shoulder: a prospective, randomized short-term comparison study. J Shoulder Elbow Surg. 2011;20:1034-1040.
129. Ohta S, Komai O, Hanakawa H. Comparative study of the clinical efficacy of the selective cyclooxygenase-2 inhibitor celecoxib compared with loxoprofen in patients with frozen shoulder. Mod Rheumatol. 2014;24:144-149. doi: 10.3109/14397595.2013.852857.
130. Omari A, Bunker TD. Open surgical release for frozen shoulder: surgical findings and results of the release. J Shoulder Elbow Surg 2001;10:353-357.
131. Othman A, Taylor G. Manipulation under anaesthesia for frozen shoulder. Int Orthop. 2002;26:268–270.
132. Othman A, Taylor G. Is the Constant scale reliable in assessing patients with frozen shoulder? 60 shoulders scored 3 years after manipulation under anaesthesia. Acta Orthop Scand. 2004;75:114-116.
72
133. Painter CF. Subdeltoid bursitis. Boston Med Surg J. 1907;156:345-349.
134. Pal B, Anderson J, Dick WC, Griffiths D. Limitation of joint mobility and shoulder capsulitis in insulin- and non-insulin-dependent diabetes mellitus. Br J Rheumatol. 1986;25:147-151.
135. Park KD, Nam HS, Lee JK, Kim YJ, Park Y. Treatment effects of ultrasound-guided capsular distension with hyaluronic acid in adhesive capsulitis of the shoulder. Arch Phys Med Rehabil. 2013 Feb;94(2):264-70. doi: 10.1016/j.apmr.2012.10.002. Epub 2012 Oct 12.
136. Pap G, Liebau C, Meyer M, Merk H. Ergebnisse der Narkosemobilisation bei Adhasiver Kapsulitis in Abhangigkeit vom Stadium der Erkrankung. [Results of mobilization under anesthesia in adhesive capsulitis in relation to stage of the disease] (German). Z Orthop Ihre Grenzgeb. 1998;136:13-17.
137. Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010;19:1034-1039.
138. Paul A, Rajkumar JS, Peter S, Lambert L. Effectiveness of sustained stretching of the inferior capsule in the management of a frozen shoulder. Clin Orthop Relat Res. 2014 Jul;472(7):2262-8. doi: 10.1007/s11999-014-3581-2. Epub 2014 Mar 25.
139. Platzer W. Color Atlas of Human Anatomy, Vol I-Locomotor System, 6th Ed 2008, Thieme E-book Library
140. Pollock RG, Duralde XA, Flatow EL, Bigliani LU. The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop Relat Res. 1994;304:30-36.
141. Pomeranz SJ1, Modi N. Adhesive capsulitis. J Surg Orthop Adv. 2014;23:119-121.
142. Puttman JJ. The treatment of a form painful periarthritis of the shoulder. Boston Med Surg. 1882;107:536.
143. Quigley TB. Checkrein shoulder; type of "frozen shoulder"; diagnosis and treatment by manipulation and ACTH or cortisone. N Engl J Med. 1954;250:188-192.
144. Quigley TB. Use of corticosteroid in treatment of painful and stiff shoulder. Clin Orthop Relat Res. 1957;10:182-189.
145. Quraishi NA, Johnston P, Bayer J, Crowe M, Chakrabarti AJ. Thawing the frozen shoulder: a randomised trial comparing manipulation under anaesthesia with hydrodilatation. J Bone Joint Surg Br. 2007;89:1197–1200.
146. Ramesh R, Smith S, Bunker T. Long term follow up after manipulation for frozen shoulder: is this as benign a disease as thought? J Orthop Med. 2003;25:46–48.
147. Raykha CN, Crawford JD, Burry AF, Drosdowech DS, Faber KJ, Gan BS, O'Gorman DB. IGF2 expression and -catenin levels are increased in Frozen Shoulder Syndrome. Clin Invest Med. 2014;37:E262-7.
73
148. Reeves B. The natural history of the frozen shoulder syndrome. Scand J Rheum. 1975;4:193–196.
149. Reichmister JP, Friedman SL. Long-term functional results after manipulation of the frozen shoulder. Md Med J. 1999;48:7–11.
150. Richards DP, Glogau AI, Schwartz M, Harn J. Relation between adhesive capsulitis and acromial morphology. Arthroscopy. 2004;20:614-619.
151. Rill BK, Fleckenstein CM, Levy MS, Nagesh V, Hasan SS. Predictors of outcome after non-operative and operative treatment of adhesive capsulitis. Am J Sports Med. 2011;39:567-74. doi:10.1177/0363546510385403
152. Rizk TE, Pinals RS, Talaiver AS. Corticosteroid injections in adhesive capsulitis: investigation of their value and site. Arch Phys Med Rehabil. 1991;72:20–22.
153. Roh YH, Yi SR, Noh JH, Lee SY, Oh JH, Gong HS, Baek GH. Intra-articular corticosteroid injection in diabetic patients with adhesive capsulitis: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2012;20:1947-1952. Epub 2011 Nov 24.
154. Rookmoneea M, Dennis L, Brealey S, Rangan A, White B, McDaid C, et al. The effectiveness of interventions in the management of patients with primary frozen shoulder. J Bone Joint Surg Br. 2010;92:1267–1272.
155. Rosenbloom AL, Silverstein JH. Connective tissue and joint disease in diabetes mellitus. Endocrinol Metab Clin North Am. 1996;25:473-483.
156. Russell S, Jariwala A2, Conlon R1, Selfe J3, Richards J3, Walton M4. A blinded, randomized, controlled trial assessing conservative management strategies for frozen shoulder. J Shoulder Elbow Surg. 2014;23:500-507. doi: 10.1016/j.jse.2013.12.026.
157. Segmüller HE, Taylor DE, Hogan CS, Saies AD, Hayes MG. Arthroscopic treatment of adhesive capsulitis. J Shoulder Elbow Surg. 1995;4:403–408.
158. Severud EI, Ruotolo C, Abbott DD, Nottage WM. All-arthroscopic versus mini-open rotator cuff repair: A long-term retrospective outcome comparison. Arthroscopy 2003;19:234-238.
159. Shaffer B, Tibone J, Kerlan R. Frozen shoulder: a long-term follow-up. J Bone Joint Surg Am. 1992;74:738–746.
160. Shah N, Lewis M. Shoulder adhesive capsulitis: systematic review of randomised trials using multiple corticosteroid injections. Br J Gen Pract. 2007;57:662–667.
161. Sharma S. Management of frozen shoulder - conservative vs surgical? Ann R Coll Surg. 2011; 93:343-344; discussion 345-346.
162. Sharma RK, Bajekal R, Bhan S. Frozen shoulder syndrome. A comparison of hydraulic distension and manipulation. Int Orthop. 1993;17:275-278.
74
163. Sheridan MA, Hannafin JA. Upper extremity: emphasis on frozen shoulder. Orthop Clin North Am. 2006;37:531-539.
164. Shin SJ, Lee SY. Efficacies of corticosteroid injection at different sites of the shoulder for the treatment of adhesive capsulitis. J Shoulder Elbow Surg. 2013 Apr;22(4):521-7. doi: 10.1016/j.jse.2012.06.015. Epub 2012 Sep 21.
165. Simmonds FA. Shoulder pain: with particular reference to the ‘‘frozen’’ shoulder. J Bone Joint Surg Br. 1949;31:426–432.
166. Simple Shoulder Test. February 10, 2005. Available at: http://www.orthop.washington.edu/?q=patient-care/articles/shoulder/simple-shoulder-test. Accessed August 3, 2012.
167. Sivardeen KAZ, Green M, Massoud SNF, Learmonth DJA. Frozen shoulder - manipulation under anaesthesia or manipulation under anaesthesia and arthroscopic capsular release. Which is the better treatment modality? J Bone Joint Surg Br. 2008;90(Suppl II):350.
168. Smith SP1, Devaraj VS, Bunker TD. The association between frozen shoulder and Dupuytren's disease. J Shoulder Elbow Surg. 2001;10:149-151.
169. Stergioulas A. Low-power laser treatment in patients with frozen shoulder: preliminary results. Photomed Laser Surg. 2008;26:99–105.
170. Tamai K, Akutsu M, Yano Y. Primary frozen shoulder: brief review of pathology and imaging abnormalities. J Orthop Sci. 2014;19:1-5.
171. Tashjian RZ, Powell AP. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease. J Shoulder Elbow Surg. 2009;18:927-32. DOI: 10.1016/j.jse.2009.03.021
172. Tashjian RZ1, Deloach J, Green A, Porucznik CA, Powell AP. Minimal clinically important differences in ASES and simple shoulder test scores after nonoperative treatment of rotator cuff disease. J Bone Joint Surg Am. 2010;92:296-303. doi: 10.2106/JBJS.H.01296.
173. Tauro J. Stiffness and rotator cuff tears: Incidence, arthroscopic findings, and treatment results. Arthroscopy 2006;22:581-586.
174. Thomas D, Williams RA, Smith DS. The frozen shoulder: a review of manipulative treatment. Rheumatol Rehabil. 1980;19: 173-179.
175. Thomas WJ, Jenkins EF, Owen JM, Sangster MJ, Kirubanandan R, Beynon C, Woods DA. Treatment of frozen shoulder by manipulation under anaesthetic and injection: does the timing of treatment affect the outcome? J Bone Joint Surg Br. 2011;93:1377–1381.
176. Tighe CB, Oakley WS Jr. The prevalence of a diabetic condition and adhesive capsulitis of the shoulder. South Med J. 2008;101:591-595. doi:10.1097/SMJ.0b013e3181705d39
75
177. Trenerry K, Walton JR, Murrell GA. Prevention of shoulder stiffness after rotator cuff repair. Clin Orthop Relat Res. 2005;430:94-99.
178. Tveita EK, Tariq R, Sesseng S, Juel NG, Bautz-Holter E. Hydrodilatation, corticosteroids and adhesive capsulitis: a randomized controlled trial. BMC Musculoskelet Disord. 2008;9:53.
179. Zuckerman JD, Cuomo F, and Rokito S. Definition and classification of frozen shoulder: a consensus approach. J Shoulder Elbow Surg. 1994;3:S72.
180. Zuckerman J, Rokito A. Frozen shoulder: a consensus definition. J Shoulder Elbow Surg. 2011;20:322–325.
181. van den Hout WB, Vermeulen HM, Rozing PM, Vliet Vlieland TPM. Impact of adhesive capsulitis and economic evaluation of high-grade and low-grade mobilisation techniques. Austral J Physiother. 2005;51:141–149.
182. van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54:959–964.
183. Vastamäki M. Rupture of the Rotator Cuff: Operative Repair. An Analysis of 128 Consecutive Cases [thesis]. Proceedings of the Orthopaedic Hospital of the Invalid Foundation. Supplement 1, pp. 1-112, Helsinki 1983. (ISBN 951-99469-1).
184. Vastamäki M. Factors influencing the operative results of rotator cuff rupture. Int Orthop. 1986;10:177-181.
185. Vastamaäki M. [Long-term results of the manipulated frozen shoulder] [in Finnish]. Suomen Ortopedia ja Traumatologia 1992;15:389–390.
186. Vastamaki M. Outcome of the manipulated frozen shoulder. J Shoulder Elbow Surg. 1994;3: S26.
187. Vastamaki M. Long-term outcome of the manipulated spontaneous frozen shoulder. In: Surgery of the Shoulder, Eds: Vastamaki M, Jalovaara P, Elsevier, Amsterdam: 265-268, 1995.
188. Vastamäki H, Vastamäki M. Rotator cuff-korjauksen jälkeinen jäätynyt olkanivel – pitkäaikaisseuranta 73 potilaalla. (in Finnish) Suomen Ortopedia ja Traumatologia 2007;30:256-257.
189. Vastamäki H, Varjonen L, Vastamäki M. [Good results after manipulation under anaesthesia for idiopathic frozen shoulder] [in Finnish]. Suomen Ortopedia ja Traumtologia 2007;30:258-261.
190. Vermeulen HM, Rozing PM, Obermann WR, leCessie S, Vliet Vlieland TPM. Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: Randomized controlled trial. Physical Therapy 2006;86:355-368.
191. Vezeridis PS, Goel DP, Shah AA, Sung S-Y, Warner JJP. Postarthroscopic arthrofibrosis of the shoulder. Sports Med Arthrosc Rev. 2010;18:198-206.
76
192. Walker-Bone K, Palmer KT, Reading I, Coggon D, Cooper C. Prevalence and impact of musculoskeletal disorders of the upper limb in the general population. Arthritis Care Res. 2004;51:642–651.
193. Walther M, Blanke F, von Wehren L, Majewski M. Frozen shoulder - comparison of different surgical treatment options. Acta Orthop Belg. 2014;80,172-177.
194. Wang JP, Huang TF, Hung SC, Ma HL, Wu JG, Chen TH. Comparison of idiopathic, post-trauma and post-surgery frozen shoulder after manipulation under anesthesia. Int Orthop. 2007;31:333–337.
195. Wang JP, Huang TF, Ma HL, Hung SC, Chen TH, Liu CL. Manipulation under anaesthesia for frozen shoulder in patients with and without non-insulin dependent diabetes mellitus. Int Orthop. 2010;34:1227–1232.
196. Warner JJ. Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg. 1997;5:130-140.
197. Warner JJ, Allen A, Marks PH, Wong P. Arthroscopic release for chronic, refractory adhesive capsulitis of the shoulder. J Bone Joint Surg Am. 1996;78:1808-1816
198. Warner JJ, Allen AA, Marks PH, Wong P. Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg. 1997;79-A:1151-1158.
199. Warner JJ, Greis PE. The treatment of stiffness of the shoulder after repair of the rotator cuff. J Bone Joint Surg Am. 1997;79-A,8:1260-1269.
200. Warner JJ, Tétreault P, Lehtinen J, Zurakowski D. Arthroscopic versus mini-open rotator cuff repair: a cohort comparison study. Arthroscopy 2005;21:328-332.
201. Warner JJ, Iannotti JP, Flatow LI. Complex and Revision Problems in Shoulder Surgery. Loppincott-Williams et Wilkins, 2008
202. Watson L, Dalziel R, Story I. Frozen shoulder: a 12-month clinical outcome trial. J Shoulder Elbow Surg. 2000;9:16-22.
203. Weber M, Prim J, Bugglin R, Michel BA, Gerber H. Long-term follow up to patients with frozen shoulder after mobilization under anesthesia. Clin Rheumatol. 1995;14:686-691.
204. Webster's Encyclopedic Unabridged Dictionary of the English Language. 1996. ISBN-13: 978-0517150269
205. Weiss JJ, Ting YM. Arthrography assisted intra-articular injection of steroids in treatment of adhesive capsulitis. Arch Phys Med Rehabil. 1978;59:285-287.
206. Wiley AM. Arthroscopic appearance of frozen shoulder. Arthroscopy 1991;7:138–143.
207. Williams NE, Seifert MH, Cuddigan JHP, Wise RA. Treatment of capsulitis of the shoulder. Rheumatology 1975;14:236.
77
208. Wolf JM, Green A. Influence of comorbidity on self-assessment instrument scores of patients with idiopathic adhesive capsulitis. J Bone Joint Surg Am. 2002;84-A:1167-1173.
209. Yang JL, Jan MH, Chang CW, Lin JJ. Effectiveness of the end-range mobilization and scapular mobilization approach in a subgroup of subjects with frozen shoulder syndrome: a randomized control trial. Man Ther. 2012;17:47-52. doi: 10.1016/j.math.2011.08.006. Epub 2011 Sep 25.
210. Yoon SH, Lee HY, Lee HJ, Kwack KS. Optimal dose of intra-articular corticosteroids for adhesive capsulitis: a randomized, triple-blind, placebo-controlled trial. Am J Sports Med. 2013 ;41:1133-1139. doi: 10.1177/0363546513480475. Epub 2013 Mar 18.