Christie Clem Frozen Shoulder Background
18
Christie Clem 1 Frozen Shoulder Background Frozen shoulder is a long lasting painful condition that results in decreased range of motion at the glenohumeral (GH) joint. 1,2 The condition was first described in the late 1800’s and referred to as scapulohumeral periarthritis. 3,4 In the 1930’s it was called frozen shoulder by Codman and in the 1940’s Neviaser referred to the condition as adhesive capsulitis. 3,5 Other names for the condition include stiff shoulder, the fifty year shoulder (in Asian countries), and contracture of the shoulder. 4 The variety of names can be contributed to the fact that frozen shoulder is still not well understood. As research attempts to explain the etiology and pathology of the condition the names for the condition have evolved. In 2011 the majority of the members of the American Shoulder and Elbow Surgeons agreed with the following standard definition for frozen shoulder: “a condition characterized by functional restriction of both active and passive shoulder motion for which radiographs of the glenohumeral joint are essentially unremarkable except for the possible presence of osteopenia or calcific tendonitis.” 6p.323 Epidemiology Frozen shoulder has a prevalence rate of 2-5% in the general population. 2,7 Women are more affected than men. Frozen shoulder most commonly occurs between the ages of 40 and 65 years 2,7,8 with the most common age being in the mid-fifties. 2 Individuals with type I diabetes have a 40% chance of developing frozen shoulder while approximately 29% of people with type II diabetes will develop the condition. 7 Other conditions that are associated with frozen shoulder include thyroid disorders, Parkinson disease, autoimmune conditions, and heart disease, 7 Dupuytrens contractures and breast cancer treatments. 9 Having frozen shoulder in one arm increases the risk of getting frozen shoulder in the other by 5-34%. 8
Transcript of Christie Clem Frozen Shoulder Background

ChristieClem
1
FrozenShoulder
Background
Frozenshoulderisalonglastingpainfulconditionthatresultsindecreasedrangeof
motionattheglenohumeral(GH)joint.1,2Theconditionwasfirstdescribedinthelate1800’s
andreferredtoasscapulohumeralperiarthritis.3,4Inthe1930’sitwascalledfrozenshoulder
byCodmanandinthe1940’sNeviaserreferredtotheconditionasadhesivecapsulitis.3,5
Othernamesfortheconditionincludestiffshoulder,thefiftyyearshoulder(inAsian
countries),andcontractureoftheshoulder.4Thevarietyofnamescanbecontributedtothe
factthatfrozenshoulderisstillnotwellunderstood.Asresearchattemptstoexplainthe
etiologyandpathologyoftheconditionthenamesfortheconditionhaveevolved.In2011
themajorityofthemembersoftheAmericanShoulderandElbowSurgeonsagreedwiththe
followingstandarddefinitionforfrozenshoulder:“aconditioncharacterizedbyfunctional
restrictionofbothactiveandpassiveshouldermotionforwhichradiographsofthe
glenohumeraljointareessentiallyunremarkableexceptforthepossiblepresenceof
osteopeniaorcalcifictendonitis.”6p.323
Epidemiology
Frozenshoulderhasaprevalencerateof2-5%inthegeneralpopulation.2,7Women
aremoreaffectedthanmen.Frozenshouldermostcommonlyoccursbetweentheagesof40
and65years2,7,8withthemostcommonagebeinginthemid-fifties.2IndividualswithtypeI
diabeteshavea40%chanceofdevelopingfrozenshoulderwhileapproximately29%of
peoplewithtypeIIdiabeteswilldevelopthecondition.7Otherconditionsthatareassociated
withfrozenshoulderincludethyroiddisorders,Parkinsondisease,autoimmuneconditions,
andheartdisease,7Dupuytrenscontracturesandbreastcancertreatments.9Havingfrozen
shoulderinonearmincreasestheriskofgettingfrozenshoulderintheotherby5-34%.8

ChristieClem
2
Anatomy
Theglenohumeraljointisaball-and-socketsynovialjointthatissurroundedbythe
GHcapsuleandligaments.Whenthearmisrelaxedattheside,theGHcapsuleistightonthe
superioraspectandloosebothanteriorlyandinferiorly.10Thislaxityallowsforfull
abductionandexternalrotationofthehumerus.TheGHcapsuleisstrengthenedbyboththe
GHligaments(superior,middle,andinferior)andthecoracohumeral(CH)ligament.The
threeGHligamentsarethickenedareasofthatcapsule.ThesuperiorGHLextendsfromthe
superiorglenoidlabrumtotheneckofthehumerusdeeptotheCHligament.10Themiddle
GHLoriginatesonthesuperioranterioraspectofthelabrum,inferiortotheSGHL,and
attachesontheproximalhumerusinferiortotheSGHLattachment.TheinferiorGHLis
madeupofanaxillarypouchthatispositionedbetweenanteriorandposteriorbands.10The
CHligamentoriginatesonthecoracoidprocessandjoinswiththeanterioraspectoftheGH
capsulebeforeinsertingonthelesserandgreatertuberositiesofthehumerus.Becausethe
CHligamentattachestobothtuberosities,itcrossesthebicipitalgrooveandkeepsthelong
headofthebicepstendoninplace.11Thetriangularareabetweenthecoracoidprocess,the
anterioraspectofthesupraspinatustendon,andthesuperioredgeofthesubscapularis
tendonisknownastherotatorinterval.11Therotatorintervalcapsuleisacombinationof
theGHcapsule,theCHligament,andtheSGHL.11(seeFigure1inAppendix)
Pathology
Thecauseandpathologyoffrozenshoulderisstillnotwellunderstood,but
informationhasbeengainedthroughbiopsiesthathavetakenplaceduringsurgical
interventions.Onepossibilityisthatfrozenshoulderbeginsasaninflammatoryresponse
thatisthenfollowedbycapsularfibrosis.2,12Becauseindividualshavepainbeforetheybegin
showingadecreaseinrangeofmotion,itisthoughtthattheinflammatoryprocesshappens

ChristieClem
3
beforethefibrosis.Histologicalstudieshavefoundbothinflammatorycellsandan
abundanceofproliferatingfibroblasts.12Studieshavealsoidentifiedthegrowthofnew
bloodvesselsandnerveswithintheGHcapsuleandsupportingligamentswhichcanhelp
explainthehighlevelsofpainthatisexperiencedbythosewithfrozenshoulder.8,12The
structuresoftherotatorintervalincludingtheGHcapsule,CHligament,andSGHligament
havebeenfoundtohavesignificantfibrosisandcontractureandbetheprimaryareaof
changeinindividualswithfrozenshoulder.8,12Inadditiontodecreasingthelaxityofthe
rotatorinterval,theoverallGHcapsuleundergoesfibroticchangesthatreducetheoverall
volumeofthejoint.8ThestructuresoftherotatorintervalincludingtheCHligamentresist
externalrotation(ER)whenthearmisattheside;asthehumerusisabducted,thelaxityin
theIGHligamentdisappearsandtheIGHligamentpreventsthehumeralheadfrom
translatingtoofarintheinferiordirection.10Asthecapsulebecomesfibroticand
contracturesform,normalexternalrotationandabductionbecomeslimited.
Classification
Aclearlydefinedclassificationsystemforfrozenshoulderhasnotbeenconsistently
usedthroughouttheliterature.In2011thefollowingclassificationsystemwasproposedby
Zuckermaninanefforttomakeclinicaldiagnosesmoreconsistentandincreasetheabilityto
compareresearchstudies.6Individualswhohavealimitationinbothactiveandpassive
rangeofmotionoftheGHjointwhenx-raysshownothingotherthanpossiblyosteopeniaor
calcifictendonitis,willbediagnosedwitheitherprimaryorsecondaryfrozenshoulder.
Primaryfrozenshoulderisalsoreferredtoasidiopathicandthereisnoknowncauseor
relatedcondition.Iftheetiologyoranassociatedconditioncanbeidentified,thepersonis
classifiedwithsecondaryfrozenshoulder.6Secondaryisdividedfurtherintothreegroups:
systemic,extrinsic,andintrinsic.6,8Secondarysystemicincludesindividualswithdiabetes,

ChristieClem
4
thyroidconditions,autoimmuneconditionsoranyothersystemicconditionthathasbeen
associatedwithfrozenshoulder.Secondaryextrinsicincludespathologiesthatarenot
directlyrelatedtotheshouldersuchasbutnotlimitedtostroke,heartdisease,distalarm
fracture,andbreastcancertreatment.Secondaryintrinsicfrozenshoulderiscausedbya
pathologywithintheshoulderitself(ex:rotatorcuffinjury,upperarmfracture,damaged
labrum,acromioclavicularinjury,bicepstendinopathy).6,8
Stages
Frozenshoulderistypicallythoughttoprogressthroughthreestages(freezing,
frozen,andthawing),2,5butothersdescribeitashavingfourphases(Table1inAppendix).8,9
Thereisnoclearbeginningandendtoeachphase,butinsteadtheyrepresenttheclinical
andhistologicalprogressionthathasbeenseen.Hereitwillbedescribedasfourstages.
Stage1beginswithagradualonsetofpainattheendrangesofGHmotion,achingpain
duringrest,andmoreintensepainwithmovement.8,9Peopleareoftenunabletosleeponthe
affectedsideandnightpainiscommon.Duringstage1motionisrestrictedbypain,but
whenunderanesthesiafullrangeofmotionispossible.Contracturesarenotpresentatthis
time,butthereisaninflammatorysynovialreaction.9Stage2isalsocalledthe“painful”or
“freezing”stage;theintensityofpainoftenincreasesandmotionbecomesmorelimitedinall
directions.9Fullrangeofmotionisnotpossibleunderanesthesiaduetoaclearreductionin
theaxillarypouch.9Stage3iscommonlycalledthe“frozen”stage.Thepainisoftenless
commonandlesssevere,butstiffnessorlackofmotiondominates.9Duringthistimethereis
adecreaseinthesynovialinflammationandthenumberofbloodvesselsinthearea,buta
continuedincreaseinthecapsularfibrosis.Afulllossoftheaxillarypouchhasbeenfound
whichgoesalongwiththefindingsthatthereisnoimprovementintherangeofmotion
whentheindividualisunderanesthesia.8,9Stage4isreferredtoasthe“thawing”orchronic

ChristieClem
5
stage.Thereislittle,ifany,pain,butlargerangeofmotionlossesarestillpresent.8,9
Graduallymotionwillimprovealthoughthereisnotspecificconsensusonhowmuchmotion
willreturnorhowlongitwilltake.Frozenshoulderhasbeensaidtoresolvein12to18
months,butlong-termstudiesshowitmaytakeseveralyearsandthatfullresolutionisnota
given.8Asurveyofover200patientsfoundthat59%hada“nearnormalshoulder”52
monthsaftersymptomsbeganaccordingtotheOxfordShoulderScale(OSS),35%had
mild/moderatesymptomsand6%hadseveresymptoms,butatthreeyears56%reported
mild/moderatesymptoms.13Anotherlong-termstudyfound45%ofpatientshadpainor
rangeofmotionrestrictionswhenevaluated40-48monthsafteronset.14Lessthanhalfof
the40%thathadalimitedrangeofmotion,realizedtheirmotionwasrestricted.14This
supportsthatthemajorityofindividualsthatexperiencefrozenshoulderwillhavenormal
functionalmobilitythreetofouryearsafteronset.Althoughtherangeofmotioninmost
directionswassignificantlylessthanthatofcontrolsmatchedforageandsex.14
Diagnostics
Clinicaldiagnosisoffrozenshoulderisbasedonthepatient’shistoryandphysical
exam.2,7,8Theindividualwillpresentwithagradualonsetofpaininaunilateralshoulder
thatoftenoccursatnightandissevereenoughtopreventlyingontheinvolvedsideor
wakesthemduringsleep.Theendrangesofmotionarealsopainful.8Adefinitionthathas
beenusedinmanystudiesis“ROMlossgreaterthan25%inatleasttwoplanesandpassive
externalrotationlossthatisgreaterthan50%oftheuninvolvedshoulderorlessthan30
degreesofexternalrotation.”8Reductioninexternalrotation,abduction,forwardflexion,
andinternalrotationarethemostcommon.7Nospecificcapsularpatternhasbeen
identified.ExternalrotationismorelimitedwhentheGHjointisat0degreesofabduction
ascomparedto90degreesofabductionwhileinternalrotationistheopposite(more

ChristieClem
6
restrictedat90degreesabduction).15Rangeofmotionrestrictionsshouldhavebeenpresent
foratleastonemonth,8butseveralstudieshaveusedaminimumthreemonthdurationas
partofthediagnosticcriteria.15Functionalmobilitywillbelimitedduetothepainand
decreasedrangeofmotion;placingahandinabackpocketandreachingoverheadorbehind
theneckcanbedifficultorimpossibletoperform.2,8
Otherpathologiesmustberuledout,especiallyduringstage1ofthefrozenshoulder
whenthereisnotyetapassiverangeofmotionrestriction.Theisometricstrengthofthe
rotatorcuffistypicallynormal,8,16althoughpainrelatedweaknessmaybepresentwhen
neartheendrangesofmotion.Specialteststhatrequirethepatienttoactivelyorpassively
movetoendrangescanproducefalsepositiveresults.Amainsignoffrozenshoulderwillbe
thefirmor“tethered”endfeelofthepassiverangeofmotion.16
Imagingstudiescanbeusedtoruleoutunderlyingpathologiessuchasosteoarthritis
androtatorcufftendinopathies,butarenotthereferencestandardwhendiagnosingfrozen
shoulder.Radiographsshouldbenormalexceptforpossibleosteopeniaorcalcific
tendonitis.6,8MRI’sarenotnecessary,butcanhelpwithdifferentialdiagnosis.MRIfindings
consistentwithfrozenshoulderincludeCHligamentandrotatorintervalthickening,2,3,8
reducedaxillarypouch,8andsynovitis-likeabnormalitiesaroundthelongheadofthebiceps
tendon.3
Interventions
Frozenshoulderisconsideredaself-limitingconditionwithavarietyofinterventions
thatcanbeutilized.Researchhasnotfoundadefinitivetreatmentapproach,butmultiple
treatmentshaveshownbenefits.Becauseindividualsrecoveratdifferentratesandsome
havesymptomsthatarestillpresentlong-term,8,13,14patienteducationisvital.Information
regardingthenaturalprogressionofthecondition,8,17theimportanceofdoingadailyhome

ChristieClem
7
exerciseprogram,8,17andtheneedtomatchtheintensityofexercisestotheirritability
level17shouldbeprovided.Commonconservativeinterventionsincludecorticosteroid
injections,intra-articulardilation(distension)andphysicaltherapytreatmentssuchas
modalities,jointmobilizations,andstretching,andahomeexerciseprogram.More
aggressiveapproachesincludemanipulationoftheGHjointunderanesthesiaand
arthroscopicsurgicalrelease.
Oralmedications,acetaminophenandnon-steroidalanti-inflammatories,aretypically
usedearlyforpainrelief,butthereislittleresearchtosupporttheiruse.Asystematic
reviewforNSAIDsrelatedtomultipletypesofshoulderconditionsfoundastatistically
significantimprovementascomparedtoplacebo,butthestudiesusedhadsmallsample
sizesandpoorquality.18
Asystematicreview(SR)evaluatingtheeffectivenessofGHcorticosteroidinjections
foundtheinjectionsprovideshorttermreliefforfrozenshoulder.7Thesebenefitsareseen
duringstage1andstage2(freezing).19Statisticallyandclinicallymeaningfulimprovements
forpainandfunctionwereobservedat6-weeks,butnotlonger.Corticosteroidinjections
outcomesat12weeksweresimilartootherinterventionsandplacebo.7Injectionsresulted
inagreaterimprovementinoutcomemeasuresascomparedtophysicaltherapyaloneata
short-term6-weekfollowup.7Intra-articularinjectionsresultedingreaterimprovementsin
painandROMascomparedtoextra-articularinjections.7Corticosteroidinjectionsworkby
decreasingtheinflammatoryresponseanddecreasingpain,8soaccurateplacementofthe
medicationcouldbeimportantforthegreatestbenefitstoberealized.Physiciansaremore
accuratewithinjectionplacementwhenusingimage-guidedinjectiontechniquesas
comparedtoanatomicallandmarkinjectiontechniques(92-100%accuracyvs.26-79%
accuracy).7TheSRdidnotfindasignificantdifferencebetweentheinjectiontechniques,but

ChristieClem
8
image-guidedplacementmayresultinbetteroutcomesaccordingtosomeindividual
studies.2
Intra-articulardilationordistensioninvolvesinjectingtheGHjointcapsulewith
salineorasaline/corticosteroidcombination.Thesalineisinjectedintothecapsuleunder
pressure,inanefforttoexpandthecapsulesincetheoverallvolumeistypicallyreduced
withfrozenshoulder.8Asystematicreviewfoundshort-termimprovementsinpain,rangeof
motion,andoverallshoulderfunctionwhendistensionwasdonewithacombinationof
salineandcorticosteroid,butdistentionwithcorticosteroidshasnotbeenshowntobe
betterthanonlyacorticosteroidinjection.2
Modalitiescanimprovesymptomsoffrozenshoulder,buttheuseofmodalitieswith
otherinterventionsandthelowqualityevidencemakesitdifficulttostateifasingle
modalityiseffectivewhenusedaloneorbetterthananother.8,20AsystematicreviewbyPage
etal.wasonlyabletoidentifythatlow-levellasertherapy(LLLT)maybebetterthan
placeboaftersixdaysoftreatmentandLLLTplusexercisemaybebetterthanexercisealone
atfourweeksforpaincontrol.20AsystematicreviewbyJainfoundstrongevidencethatLLLT
improvespain,moderateevidencethatitimprovesfunction,andnoevidencethatitaffects
ROM.19Theadditionofdeepheat,shortwavediathermy,tostretchingmadesignificantgains
inROMascomparedtosuperficialheat/stretchingorstretchingalone.Thedeepheatalso
providedbenefitsinpainandfunction.19Nobenefitsinpain,ROM,orfunctionwerefound
withultrasoundinthesystematicreview,19butultrasoundwasfoundtoincreaseonlyROM
immediatelyposttreatmentandata3-monthfollow-upinstudybyDogruetal.8Thereisnot
strongevidencefortheuseofothermodalitiessuchasiceorelectricalstimulation,but
tryingtheseinterventionsmaybeappropriateforindividualswithhighlevelsofpain.

ChristieClem
9
Physicaltherapyexerciseandmobilizationsarehighlyrecommendedduringstage3
(frozen)andstage4(thawing)toassistwithpainreduction,regainingROM,andimproving
function.19Thephysicaltherapyinterventionshouldbebasedontheirritabilitylevelofthe
patient;astheirritability/paindecreasestheintensityoftheinterventioncanincreaseto
focusonregainingROM(Table2inAppendix).17Patientswithhighirritabilitywillperform
easy,short-durationROMexercisesforpainreductionandreceptorinput;ROMexercises
shouldbedone2-3timesadayforafewsecondsinalmostapain-freerange.17Pushinginto
thepainatthispointhasnotbeenfoundtobebeneficial.8,17Theintensityandholdtimeof
thestretchshouldincreaseasthepaindecreasesaswellasthefrequencyoftimes
performedduringtheday.AsystematicreviewonmanualtherapyandexercisebyPageet
al.determinedthatmanualtherapyandexercisemaynotdoaswellascorticosteroid
injectionsforshort-termresults.21AsystematicreviewbyFavejeeetal.identifiedthe
following:highgrademobilizationsimprovedGHmobilityanddecreaseddisabilitymore
thanlowgrademobilizations,posteriormobilizationsincreasedexternalrotationmorethan
mobilizationsintheanteriordirection,end-rangemobilizationsandmobilizationswith
movementweremorebeneficialthanmid-rangemobilizations,andmobilizationswith
movementwerebetterthanend-rangemobilizationsforscapulohumeralrhythm.22Overall,
physicaltherapyexerciseandmobilizationscanimproverangeofmotion.Allpatients
shouldperformaHEPthatconsistsofpassiveROMexercisesattheGHjoint:flexion,
extension,internalrotation,externalrotation,horizontaladduction,andabduction(Figure2
inAppendix).
Ifimprovementsdonotoccurwithconservativeinterventionsaftersixmonths17or
afteroneyear2referraltoaphysicianforconsiderationofamoreinvasiveprocedurecould
bethenextstep.Manipulationunderanesthesia(MUA)adequatelyincreasesthepatient’s

ChristieClem
10
ROM,butdoesnotallowthephysiciantheabilitytoisolatespecifictissues.2,17MUAinvolves
stabilizingthescapulawhilethehumerusisforcefullymovedpastend-rangeto“tear”the
capsule.Multiplestudieshavehadpositiveoutcomesin75-100%ofthesubjectsundergoing
MUA,17butthereistheriskoffracture,nerveinjury,muscleinjuries,andlabraltears.23
Arthroscopiccapsularreleaseallowsthephysiciantoselectspecificpartsofthecapsuleto
release.Arthroscopicreleasehasresultedinimprovedoutcomes:lesspain,improvedROM,
andbetterfunction.AsystematicreviewbyGrantetal.foundverylittledifferencesbetween
theresultsofMUAandarthroscopiccapsularrelease.23ThisSRfoundcapsularrelease
resultedinmoreabductionandexternalrotation,6degreesand8degreesrespectively,as
wellasaslightlyhigher,butnon-significantdifferenceinadisabilityoutcomemeasure.
SimilarcomplicationrateswerealsofoundbetweencapsularreleaseandMUA,0.5%and
0.4%respectively.23Manipulationisoftendoneimmediatelyfollowingthearthroscopic
capsularreleasetoregainfullmotion.ArthroscopiccapsularreleasecombinewithMUA
demonstratedROMimprovementsof~70degreesinflexion,~30degreesinexternal
rotation,andinternalrotationgainsmeasuredbyreachingtoL1insteadofL5inastudyof
50patientsthathadfailedoversixmonthsofconservativetreatment.24Patientsthathave
diabeteshaveoutcomesthataresignificantlybetterfollowingcapsularrelease,buttheir
improvementsaresignificantlylowerthanthosewithoutdiabetesandoftenhavelong-
lastinglimitations.25
OutcomeMeasures
TheDisabilityoftheArm,Shoulder,andHandScale(DASH)andtheShoulderPain
andDisabilityIndex(SPADI)aretwoofthemostcommonlystudiedshoulderoutcome
measures.8,26Becauseneitherhavebeenfoundtohavefloororceilingeffectsandbothhave
goodresponsiveness,theyarerecommendedintheoutpatientsetting.26TheSPADIismore

ChristieClem
11
responsivethantheDASHforpatientswithfrozenshoulder.8TheDASHisaself-report
questionnairewith30itemsthatarescoredonaonetofivescale.Therawscoreis
convertedtoa0-100scalewith0meaningnodisabilityand100fullydisabled.27The
minimaldetectablechange(MCD)isbetween6.6–12.2points(average10)with10.2points
asthechangeneededtobeclinicallymeaningful.8TheQuickDASHisashortened11-item
questionnairethatalsomeasuresphysicalfunctioninpatientswithanupperextremity
condition.TheQuickDASHhasbeenfoundtobevalid,reliable,andresponsive,butthe
originalDASHprovidesamorecomprehensivepicture.28TheSPADIisaself-report
questionnairethatassessespainanddisability.Fivequestionsareaboutpainand8
questionsaddressdisabilityforatotalof13totalitems.8TheMDCfortheSPADIis18points
whileachangebetween8and13isclinicallymeaningful.29,30SincepainandlimitedROMare
thetwoprimarycomplaintsoffrozenshoulder,bothoftheseshouldbeobjectively
measured,inadditionto,usinganoutcomemeasurefordisability.Thevisualanalogscale
canbeusedforoverallpain,butcanalsobeusedinconnectionwithspecificactivitiesthat
aredifficultsuchaspainduringsleep,reachingbehindtheback,orwhengettingdressed.
BothactiveandpassiveROMcanbemeasuredwithagoniometerinthefollowingplanesof
motion:flexion,abduction,internalandexternalrotationat90degreesofabduction(45
degreesif90isnotpossible),andexternalrotationat0degreesabduction.8
Conclusion
Frozenshoulderisconsideredaself-limitingconditionthatcausesdisabilitythrough
highlevelsofpainanddecreasedROM,buttheunderlyingcauseisnotwellunderstood.
2,8,9,12Someresearchersbelieffrozenshoulderbeginsasaninflammatoryprocesswhich
thentransitionstoafibroticconditionresultinginatightenedGHjointcapsulewithreduced
ROM.2,12,17TheCHligament,rotatorinterval,andaxillarypoucharethestructuresmost

ChristieClem
12
commonlyaffected3,8,11resultinginlossesofexternalrotation,abduction,andflexion.The
conditionprogressesthroughfourstages:1)earlypainwithfullROM,2)“freezing”or
“painful”,highlevelspain,limitedmotion,3)“frozen”,lesspain,increasedROMrestrictions,
4)“thawing”,littletonopain,largeROMdeficits,ROMbeginstoimprove.8,9Resolutionoften
occurswithinonetofouryears,butcompleteresolutionmayneveroccur.13,14Conservative
treatmentshouldbeattemptedforsixmonthsto1yearbeforesurgicalinterventionsare
explored.Patienteducationabouttheprogressionoftheconditionandtheimportanceofa
dailyHEPshouldbeprovided.Thereisnotevidencetosupportaspecificconservative
interventionasthebest,2,7,17,19,20,22butthepainirritabilitylevelofthepatientandthestage
oftheprogressionshouldbeconsideredwhendecidingatreatmentapproach.2,17Intra-
articularcorticosteroidinjectionsareeffectiveatreducingshort-termpainandshouldbe
usedduringtheearlystages.2,7,8Physicaltherapy(exercise,ROM,mobilizations,modalities)
isimportantforimprovingROMespeciallyduringthe“frozen”and“thawing”stages.9,17,19,22
MoreinvasivetreatmentoptionssuchasMUAandarthroscopiccapsularreleaseare
availableforpatientsthathavepersistentdisabilitywhenconservativemethodsfail.2,8,17,23
Resources
1. RoyA,AdahanT,TalaveraF,FoyeP.AdhesiveCapsulitisinPhysicalMedicineand
Rehabilitation.2014.http://emedicine.medscape.com/article/326828-overview.
AccessedNovember25,2015.
2. FieldsKB.OfficialreprintfromUpToDate®www.uptodate.com©2015UpToDate®.
2015:1-17.

ChristieClem
13
3. ZhaoW,ZhengX,LiuY,etal.AnMRIstudyofsymptomaticadhesivecapsulitis.PLoS
One.2012;7(10):e47277.doi:10.1371/journal.pone.0047277.
4. LewisJ.Frozenshouldercontracturesyndrome-Aetiology,diagnosisand
management.ManTher.2015;20(1):2-9.doi:10.1016/j.math.2014.07.006.
5. EljabuW,KlingerHM,vonKnochM.Prognosticfactorsandtherapeuticoptionsfor
treatmentoffrozenshoulder:asystematicreview.ArchOrthopTraumaSurg.October
2015.doi:10.1007/s00402-015-2341-4.
6. ZuckermanJD,RokitoA.Frozenshoulder:aconsensusdefinition.JShoulderElbow
Surg.2011;20(2):322-325.doi:10.1016/j.jse.2010.07.008.
7. SongA,HigginsLD,NewmanJ,JainNB.Glenohumeralcorticosteroidinjectionsin
adhesivecapsulitis:asystematicsearchandreview.PMR.2014;6(12):1143-1156.
doi:10.1016/j.pmrj.2014.06.015.
8. KelleyMJ,ShafferMa.,KuhnJE,etal.ShoulderPainandMobilityDeficits:Adhesive
Capsulitis.JOrthopSportPhysTher.2013;43(5):A1-A31.
doi:10.2519/jospt.2013.0302.
9. NeviaserAS,HannafinJA.AdhesiveCapsulitis:AReviewofCurrentTreatment.AmJ
SportsMed.2010;38(11):2346-2356.doi:10.1177/0363546509348048.
10. LudewigP,BorstadJ.TheShoulderComplex.In:JointStructureandFunction:A
ComprehensiveAnalysis.Vol5thed.;2011:247-250.
11. PetchprapaCN,BeltranLS,JazrawiLM,KwonYW,BabbJS,RechtMP.Therotator
interval:areviewofanatomy,function,andnormalandabnormalMRIappearance.
AJRAmJRoentgenol.2010;195(3):567-576.doi:10.2214/AJR.10.4406.
12. HandGCR,AthanasouNA,MatthewsT,CarrAJ.Thepathologyoffrozenshoulder.J
BoneJointSurgBr.2007;89(7):928-932.doi:10.1302/0301-620X.89B7.19097.

ChristieClem
14
13. HandC,ClipshamK,ReesJL,CarrAJ.Long-termoutcomeoffrozenshoulder.JShoulder
ElbowSurg.17(2):231-236.doi:10.1016/j.jse.2007.05.009.
14. BinderAI,BulgenDY,HazlemanBL,RobertsS.Frozenshoulder:along-term
prospectivestudy.AnnRheumDis.1984;43(3):361-364.
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1001345&tool=pmcentr
ez&rendertype=abstract.AccessedOctober29,2015.
15. RundquistPJ,AndersonDD,GuancheCA,LudewigPM.Shoulderkinematicsinsubjects
withfrozenshoulder.ArchPhysMedRehabil.2003;84(10):1473-1479.
http://www.ncbi.nlm.nih.gov/pubmed/14586914.AccessedNovember29,2015.
16. NeviaserAS,NeviaserRJ.Adhesivecapsulitisoftheshoulder.JAmAcadOrthopSurg.
2011;19(9):536-542.http://www.ncbi.nlm.nih.gov/pubmed/21885699.Accessed
October14,2015.
17. KelleyMJ,McClurePW,LegginBG.Frozenshoulder:evidenceandaproposedmodel
guidingrehabilitation.JOrthopSportsPhysTher.2009;39(2):135-148.
doi:10.2519/jospt.2009.2916.
18. EwaldA.AdhesiveCapsulitis:AReview.2011:417-422.
19. JainTK,SharmaNK.Theeffectivenessofphysiotherapeuticinterventionsintreatment
offrozenshoulder/adhesivecapsulitis:asystematicreview.JBackMusculoskelet
Rehabil.2014;27(3):247-273.doi:10.3233/BMR-130443.
20. PageMJ,GreenS,KramerS,JohnstonRV,McBainB,BuchbinderR.Electrotherapy
modalitiesforadhesivecapsulitis(frozenshoulder).CochranedatabaseSystRev.
2014;10:CD011324.doi:10.1002/14651858.CD011324.
21. PageMJ,GreenS,KramerS,etal.Manualtherapyandexerciseforadhesivecapsulitis
(frozenshoulder).CochranedatabaseSystRev.2014;8:CD011275.

ChristieClem
15
doi:10.1002/14651858.CD011275.
22. FavejeeMM,HuisstedeBMA,KoesBW.Frozenshoulder:theeffectivenessof
conservativeandsurgicalinterventions--systematicreview.BrJSportsMed.
2011;45(1):49-56.doi:10.1136/bjsm.2010.071431.
23. GrantJa.,SchroederN,MillerBS,CarpenterJE.Comparisonofmanipulationand
arthroscopiccapsularreleaseforadhesivecapsulitis:Asystematicreview.JShoulder
ElbSurg.2013;22(8):1135-1145.doi:10.1016/j.jse.2013.01.010.
24. TrsekD,CicakN,ZunacM,KlobucarH.Functionalresultsandpatientsatisfactionafter
arthroscopiccapsularreleaseofidiopathicandpost-traumaticstiffshoulder.Int
Orthop.2014;38(6):1205-1211.doi:10.1007/s00264-014-2283-4.
25. MehtaSS,SinghHP,PandeyR.Comparativeoutcomeofarthroscopicreleaseforfrozen
shoulderinpatientswithandwithoutdiabetes.BoneJointJ.2014;96-B(10):1355-
1358.doi:10.1302/0301-620X.96B10.34476.
26. BotSDM,TerweeCB,vanderWindtDAWM,BouterLM,DekkerJ,deVetHCW.
Clinimetricevaluationofshoulderdisabilityquestionnaires:asystematicreviewofthe
literature.AnnRheumDis.2004;63(4):335-341.
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1754942&tool=pmcentr
ez&rendertype=abstract.AccessedOctober27,2015.
27. SmileyJ,ToddA,CalabreseF,FaganA,GalvinP.RehabMeasures:Disabilitiesfothe
Arm,Shoulder,andHandQuestionnaire.2013.
28. TheQuickDASH.DASHOutcomeMeas.
29. RoyJ-S,MacDermidJC,WoodhouseLJ.Measuringshoulderfunction:asystematic
reviewoffourquestionnaires.ArthritisRheum.2009;61(5):623-632.
doi:10.1002/art.24396.

ChristieClem
16
30. RehabMeasures:ShoulderPainandDisabilityIndex.2015.
http://www.rehabmeasures.org/Lists/RehabMeasures/PrintView.aspx?ID=1207.
AccessedNovember30,2015.

ChristieClem
17
Appendix
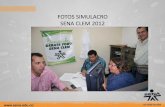
Figure1–RotatorIntervalAnatomy11–Petchprapaetal.2010
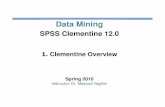
Table1–FourStagesAdhesiveCapsulitis9–Neviaser2010p.2347
568 AJR:195, September 2010
Petchprapa et al.
in only four of 63 (6%) shoulder dissections by Neer et al. [1].
The SGHL is a fold–focal thickening of the glenohumeral joint capsule (Fig. 4). It is variable in origin (supraglenoid tubercle, su-perior labrum, long head biceps tendon, mid-dle glenohumeral ligament, or some combina-tion) and may be absent in 3% of patients at arthroscopy [2]. The SGHL is anterior to and maintains a close relationship with the biceps tendon along its course. Before it inserts into a small depression above the lesser tuberosity (known as the fovea capitis of the humerus), it contributes to the biceps reflection pulley.
The long head of the biceps tendon may arise from the posterosuperior labrum, supraglenoid tubercle, or a combination of both [3]. The
tendon takes an oblique intraarticular course through the rotator interval and must make a 30° to 45° turn along the anterior surface of the humeral head before it exits the joint be-tween the lesser and greater tuberosities in the intertubercular groove. Anomalies of the bi-ceps brachii muscle are common, with 9–23% showing supernumerary heads [4]. More rare variants, particularly of the intraarticular por-tion of the long head of the biceps tendon, also have been reported in the literature [5].
The CHL and SGHL form a slinglike band surrounding the long head of the biceps tendon proximal to the bicipital groove (Fig. 5). This biceps reflection pulley plays an important role in the stability of the intraarticular biceps ten-don. When the arm is abducted and externally rotated, the pulley limits medial subluxation of the biceps tendon. Medially, the superior gle-nohumeral ligament lies anterior to the biceps tendon. Further laterally, the ligament folds into a cup-shaped structure that cradles the biceps tendon. At the opening of the bicipital groove, SGHL fibers are joined by medial fibers of the CHL to form the biceps reflection pulley [6]. The subscapularis and supraspinatus tendon insertions along the lesser and greater tuberos-ities, respectively, blend with those of the CHL and are thus intimately associated with the bi-ceps pulley [7, 8]. Injuries to any of these com-ponents of the sling are referred to as “pulley lesions” [9, 10].
ImagingImaging the components of the rotator in-
terval poses several challenges. The small
size of the structures requires high spa-tial resolution; this is optimized by the use of strong gradients, surface coils, and high-field-strength MR scanners that maximize the signal-to-noise ratio. Even after imag-ing parameters are optimized, evaluating the structures of the rotator interval can be difficult. Most often, the SGHL, CHL, and rotator interval capsule appear as interme-diate-weighted soft tissue filling the rotator interval and surrounding the biceps tendon. These normally coapted structures also can appear spuriously thickened when the shoul-der is internally rotated; in this position, the rotator interval structures are not taut. In-traarticular fluid, either a joint effusion or in-traarticular contrast material, separates the folds of tissue in this region and allows better structure delineation. It is for this reason that MR arthrography is recommended when ab-normality of the rotator interval is suspected [11], and this is our preference. Nonarthro-graphic images, however, do allow evalua-tion of the extraarticular portion of the CHL and the subcoracoid fat that surrounds it.
At our institution, MR arthrography is done after 10–12 mL of dilute (1:200 solu-tion) gadopentetate dimeglumine (Mag-nevist, Bayer HealthCare Pharmaceuticals) is injected into the joint and follows standard arthrography protocol: axial fat-saturated T1-weighted (TR/TE, 514/8.6), coronal oblique fat-saturated T1-weighted (754/8.6), sagittal oblique T1-weighted (450/9.4), coronal oblique fat-saturated T2-weighted (5,880/79), and abduction and external rotation
A
Fig. 1—Rotator interval.A–C, Illustrations in coronal (A) and sagittal (B) planes and corresponding sagittal MR proton density–weighted arthrogram (C) show boundaries of rotator interval, which are defined by coracoid process (COR) at its base, superiorly by anterior margin of supraspinatus tendon (SST) and inferiorly by superior margin of subscapularis tendon (SSC). Contents of rotator interval include long head of biceps tendon (BT), coracohumeral ligament (CHL), superior glenohumeral ligament (SGHL), and rotator interval capsule. Rotator interval capsule (RIC) is anterosuperior aspect of glenohumeral joint capsule, which merges with CHL and SGHL insertions medial and lateral to bicipital groove. CHL arises from base of coracoid process, traverses through subcoracoid fat, and inserts on anterior humerus. IST = infraspinatus tendon.
CB
Fig. 2—Photograph of anterior view of cadaver dissection shows stout coracohumeral ligament (CHL); it suspends shoulder joint from coracoid process. CHL arises from lateral base of coracoid process (CP) and broadly inserts on lesser and greater tuberosities where it becomes confluent with subscapularis tendon (black star), supraspinatus tendon (white star), and rotator interval capsule (asterisk).
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by U
niv
of N
C/A
CQ
Srv
s on
11/2
6/15
from
IP a
ddre
ss 1
52.2
.176
.242
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d
used to describe the idiopathic process of global capsularinflammation and fibrosis occurring in the absence of otherlesions. Secondary adhesive capsulitis has been used todescribe a constellation of conditions resulting in a stiffshoulder.41 Some of these conditions demonstrate isolatedareas of capsular contracture that are indistinguishablefrom idiopathic adhesive capsulitis but occur concurrentlywith other known injuries or diseases. Others have anextra-articular cause of shoulder stiffness without involve-ment of the joint capsule. Calcific tendinitis, rotator cuffinjury, biceps tendinitis, as well as glenohumeral or acro-mioclavicular arthritis, all can cause shoulder stiffness inthe absence of capsular limitation of motion. Distinguish-ing between primary or idiopathic disease and pain dueto other causes can be difficult and there is frequent over-lap. Yoo et al78 reported that 62% of patients with stage 2idiopathic adhesive capsulitis were found to have supraspi-natus lesions, most commonly partial-thickness tears, afterundergoing magnetic resonance imaging (MRI).
Subtle clues in the history and physical examinationallow discrimination of primary adhesive capsulitis fromthese other conditions. Treatment of so-called secondaryadhesive capsulitis should be directed toward the associatedcondition causing immobilization of the shoulder, and
outcomes differ based on that condition.30,50 Only the treat-ment of primary adhesive capsulitis will be discussed here.
Adhesive capsulitis progresses through 4 stagesdescribed by Neviaser and Neviaser49 based on the correla-tion of physical examination and arthroscopic examinationof affected joints. Hannafin et al28 demonstrated the histo-pathological progression of disease in capsular biopsiesfrom patients with Neviaser stages 1 to 3. Recognition ofthese stages is essential to applying appropriate treat-ment, communicating prognosis, and establishing theexpectations of both patient and physician (Table 1). Thearthroscopic and histopathological appearances of theshoulder capsule in the various stages of disease are dis-cussed below. These are not required to identify the stagesof disease. Diagnosis and staging of adhesive capsulitis aredetermined clinically based on symptoms and physicalexamination. Intra-articular anesthetic injection can beused to discriminate between the first 2 stages.
Stage 1 is characterized by a gradual onset of pain typ-ically referred to the deltoid insertion. It is usually achy atrest and sharper with movement. Pain at night is common,and patients frequently report an inability to sleep on theaffected side. Duration of symptoms is generally lessthan 3 months. Capsular pain on deep palpation or passive
TABLE 1Stages of Adhesive Capsulitis
Symptoms Signs Arthroscopic Appearance Biopsy
Stage 1
Pain referred todeltoid insertionPain at night
Capsular pain ondeep palpation
Empty end feel atextremes of motion
Full motion underanesthesia
Fibrinous synovialinflammatory reaction
No adhesions or capsularcontracture
Rare inflammatorycell infiltrate
Hypervascular,hypertrophic synovitis
Normal capsular tissue
Stage 2
Severe night painStiffness
Motion restricted inforward flexion,abduction, internal andexternal rotation
Some motion lossunder anesthesia
Christmas tree synovitisSome loss of axillary fold
Hypertrophic,hypervascular synovitis
Perivascular,subsynovial capsularscar
Stage 3
Profound stiffnessPain only at the end
range of motion
Significant loss of motionTethering at ends of motionNo improvement
under anesthesia
Complete loss ofaxillary fold
Minimal synovitis
Hypercellular,collagenous tissue witha thin synovial layer
Similar features toother fibrosingconditions
Stage 4
Profound stiffnessPain minimal
Significant motion lossGradual improvement
in motion
Fully mature adhesionsIdentification of intra-
articular structures difficult
Not reported
Vol. 38, No. 11, 2010 Adhesive Capsulitis 2347
at University of North Carolina at Chapel Hill on November 28, 2015ajs.sagepub.comDownloaded from

ChristieClem
18
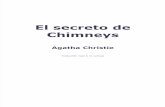
Table2–TreatmentStrategiesBasedonIrritabilityLevel17–Kelleyetal.p.140
Figure2–PassiveROMExercisesforHEP–Kelleyetal.p.140
140 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]in less pain and improved motion in pa-tients with frozen shoulder.99
The basic strategy in treating structuralstiffness is to apply appropriate tissuestress.74 It is helpful to think of the totalamount of stress being applied as the“dosage,” in much the same way that dos-age applies to medication. The primaryfactors that guide this process are painand ROM. Adjusting the dose of tissuestress results in the desired therapeuticchange (increased motion without in-creased pain). Three factors should beconsidered when calculating the dose, ortotal amount of stress delivered, to a tis-sue: intensity, frequency, and duration.The total end range time (TERT)34,66 is thetotal amount of time the joint is held ator near end-range position. TERT is cal-culated by multiplying the frequency andduration of the time spent at end rangedaily, and is a useful way of measuring thedose of tissue stress.34,66 Intensity remainsan important factor in tensile stress dosebut is typically limited by pain. Tradition-al ROM exercises are considered lowerforms of tensile stress, while the highesttensile stress doses are achieved by low-load prolonged stretching (LLPS), be-cause TERT is maximized. Therefore, thegoal with each patient is to determine thetherapeutic level of tensile stress.
Applying the correct tensile-stressdose is based upon the patient’s irritabil-ity classification ( ). In patients withhigh irritability, low-intensity and short-duration ROM exercises are performedto simply alter the joint receptors’ input,reduce pain, decrease muscle guarding,and increase motion.126
show commonly performed exercises forpatients with high irritability. Stretchesmay be held from 1 to 5 seconds at therelatively pain-free range, 2 to 3 times aday. A pulley may be used, depending onthe patient’s ability to tolerate the exer-cise. These exercises primarily influencedifferent regions of the synovial/CLCand have been used in supervised physi-cal therapy programs and an HEP in
(A) Forward flexion, (B) external rotation,(C) extension.
(A) Internal rotation, (B) horizontaladduction, (C) pulley for elevation.
Treatment StrategiesBased on Irritability Level
Modalities Heat/ice/electricalstimulation
Heat/ice/electricalstimulation
...
Activity modification Yes Yes ...
ROM/stretch Short-duration (1-5 s), pain-free, passive AAROM
Short-duration (5-15 s),passive, AAROM toAROM
End range/overpressure,increased-duration,cyclic loading
Manual techniques Low-grade mobilization Low- to high-grademobilization
High-grade mobilization/sustained hold
Strengthen ... ... Low- to high-resistance endranges
Functional activities ... Basic High demand
Patient education
Other Intra-articular steroidinjection
... ...
Abbreviations: AAROM, active assisted range of motion; AROM, active range of motion.
Jour
nal o
f Orth
opae
dic
& S
ports
Phy
sical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f Nor
th C
arol
ina/
Acq
Srv
cs o
n N
ovem
ber 2
9, 2
015.
For
per
sona
l use
onl
y. N
o ot
her u
ses w
ithou
t per
miss
ion.
C
opyr
ight
© 2
009
Jour
nal o
f Orth
opae
dic
& S
ports
Phy
sical
The
rapy
®. A
ll rig
hts r
eser
ved.
140 | february 2009 | volume 39 | number 2 | journal of orthopaedic & sports physical therapy
[ CLINICAL COMMENTARY ]in less pain and improved motion in pa-tients with frozen shoulder.99
The basic strategy in treating structuralstiffness is to apply appropriate tissuestress.74 It is helpful to think of the totalamount of stress being applied as the“dosage,” in much the same way that dos-age applies to medication. The primaryfactors that guide this process are painand ROM. Adjusting the dose of tissuestress results in the desired therapeuticchange (increased motion without in-creased pain). Three factors should beconsidered when calculating the dose, ortotal amount of stress delivered, to a tis-sue: intensity, frequency, and duration.The total end range time (TERT)34,66 is thetotal amount of time the joint is held ator near end-range position. TERT is cal-culated by multiplying the frequency andduration of the time spent at end rangedaily, and is a useful way of measuring thedose of tissue stress.34,66 Intensity remainsan important factor in tensile stress dosebut is typically limited by pain. Tradition-al ROM exercises are considered lowerforms of tensile stress, while the highesttensile stress doses are achieved by low-load prolonged stretching (LLPS), be-cause TERT is maximized. Therefore, thegoal with each patient is to determine thetherapeutic level of tensile stress.
Applying the correct tensile-stressdose is based upon the patient’s irritabil-ity classification ( ). In patients withhigh irritability, low-intensity and short-duration ROM exercises are performedto simply alter the joint receptors’ input,reduce pain, decrease muscle guarding,and increase motion.126
show commonly performed exercises forpatients with high irritability. Stretchesmay be held from 1 to 5 seconds at therelatively pain-free range, 2 to 3 times aday. A pulley may be used, depending onthe patient’s ability to tolerate the exer-cise. These exercises primarily influencedifferent regions of the synovial/CLCand have been used in supervised physi-cal therapy programs and an HEP in
(A) Forward flexion, (B) external rotation,(C) extension.
(A) Internal rotation, (B) horizontaladduction, (C) pulley for elevation.
Treatment StrategiesBased on Irritability Level
Modalities Heat/ice/electricalstimulation
Heat/ice/electricalstimulation
...
Activity modification Yes Yes ...
ROM/stretch Short-duration (1-5 s), pain-free, passive AAROM
Short-duration (5-15 s),passive, AAROM toAROM
End range/overpressure,increased-duration,cyclic loading
Manual techniques Low-grade mobilization Low- to high-grademobilization
High-grade mobilization/sustained hold
Strengthen ... ... Low- to high-resistance endranges
Functional activities ... Basic High demand
Patient education
Other Intra-articular steroidinjection
... ...
Abbreviations: AAROM, active assisted range of motion; AROM, active range of motion.
Jour
nal o
f Orth
opae
dic
& S
ports
Phy
sical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f Nor
th C
arol
ina/
Acq
Srv
cs o
n N
ovem
ber 2
9, 2
015.
For
per
sona
l use
onl
y. N
o ot
her u
ses w
ithou
t per
miss
ion.
C
opyr
ight
© 2
009
Jour
nal o
f Orth
opae
dic
& S
ports
Phy
sical
The
rapy
®. A
ll rig
hts r
eser
ved.