
The impact of local treatment of the prostate in patients with...
57
FACULTY OF MEDICINE AND HEALTH SCIENCES Academic Year 2015 - 2016 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. Miet VANDEMAELE Promotor: Prof. Dr. P. Ost Dissertation presented in the 2 nd Master year in the programme of Master of Medicine in Medicine
Transcript of The impact of local treatment of the prostate in patients with...

FACULTY OF MEDICINE AND HEALTH SCIENCES
Academic Year 2015 - 2016
The impact of local treatment of the prostate in patients with newly diagnosed metastatic
prostate cancer.
Miet VANDEMAELE
Promotor: Prof. Dr. P. Ost
Dissertation presented in the 2nd Master year in the programme of
Master of Medicine in Medicine

FACULTY OF MEDICINE AND HEALTH SCIENCES
Academic Year 2015 - 2016
The impact of local treatment of the prostate in patients with newly diagnosed metastatic
prostate cancer.
Miet VANDEMAELE
Promotor: Prof. Dr. P. Ost
Dissertation presented in the 2nd Master year in the programme of
Master of Medicine in Medicine


“The author and the promotor give the permission to use this thesis for consultation and to copy parts
of it for personal use. Every other use is subject to the copyright laws, more specifically the source must
be extensively specified when using results from this thesis.”
Date
11/04/2016
Miet Vandemaele Prof. Dr. Piet Ost


The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 5
I. Acknowledgements
This thesis has been a long process and a challenge in many ways, and I would like to express
my gratitude for the people who helped make this dissertation possible.
First of all, I would like to thank my promotor, prof. Dr. Piet Ost, for his supervision. His
constructive feedback made the writing of this thesis possible, and transformed it into a valuable
learning process.
A special thanks goes out to my family and friends, for reading and rereading this thesis many
times. Their encouragements supported me throughout the entire process of this thesis and their
input has been a great help.

p. 6 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 7
II. Abstract
1. Abstract
Goal of this thesis: The evolutions in screening tactics and treatment have had a positive impact
for men diagnosed with metastatic prostate cancer. However, survival rates are still dramatic.
This thesis takes a critical look at the arguments and current evidence to investigate if local
treatment of the prostate improves the survival rate or clinical outcomes of patients with newly
diagnosed metastatic prostate cancer.
Methods: A literature research was performed in Ovid. 4511 articles were found with a search
strategy including men with newly diagnosed mPCa, undergoing local treatment (whether or
not combined with systemic treatment), compared to systemic treatment alone, with outcomes
including overall survival rate (OS), disease specific survival rate (DSS), progression free (or
failure free) survival rate, toxicity, and biochemical response. 63 articles remained after
reviewing title and abstract, and were assessed by full text, to ultimately select 9 studies. These
studies were assessed for quality with a ‘modified Delphi technique’, leaving only two studies
that met the threshold: a retrospective cohort study by Culp et al. investigating radiotherapy and
radical prostatectomy, and a case-control study by Heidenreich et al. looking at radical
prostatectomy.
Results: Both studies indicate an OS benefit for metastatic prostate cancer patients treated with
radiotherapy (RT) or radical prostatectomy (RP), compared to systemic therapy alone. Culp et
al. showed an prolonged DSS rate for RP and RT independently, Heidenreich et al. confirmed
this for RP. The absolute DSS found by Heidenreich et al. was not significantly better than in
the control group. Culp et al. performed subgroup analysis for age, PSA level and M stage, with
results following the trend of the previous outcomes. They also identified factors independently
associated with worse survival rates: age ≥ 70 yr, cT4 disease, PSA ≥ 20 ng/ml, high-grade
disease, and pelvic lymphadenopathy.
Conclusion: Adding surgery or radiotherapy to systemic treatment in mPCa patients seems a
promising approach. There is a profit in both overall survival and disease specific survival for
local treatments added to systemic therapy, compared to systemic therapy alone. It was not
possible to distinguish which local therapy is the most beneficial, or to identify what patients

p. 8 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
could profit most. Furthermore, because of the lack of comparative or randomised trials and the
many limitations in the included studies, adding local treatment cannot be recommended at this
time as a new standard of care. There are several prospective trials in the near future that could
provide more conclusive evidence, and make more validated recommendations.
2. Nederlandstalig abstract
Doel van deze thesis: De voorbije jaren is de prognose voor mannen met gemetastaseerde
prostaat kanker positief geëvolueerd. Vooral een betere screening en nieuwe therapieën hebben
hieraan bijgedragen. Toch zijn de overlevingskansen nog steeds bedroevend. In deze thesis
wordt een overzicht gegeven van de argumenten en evidentie in de bestaande literatuur die de
lokale behandeling van de prostaattumor ondersteunen, om uit te wijzen of er een verbeterde
overleving of klinische uitkomst is in patiënten met primair gemetastaseerde prostaatkanker.
Methode: Op basis van een zoekstrategie werd literatuur geselecteerd in Ovid. Inclusiecriteria
waren patiënten met nieuw gediagnosticeerde prostaat kanker, behandeld met lokale therapie,
al dan niet gecombineerd met systemische behandeling, met als controlegroep enkel
systemische therapie. De beoogde uitkomsten waren totale overleving (overall survival OS),
ziektespecifieke overleving (disease specific survival DSS), overleving zonder recidiveren
(failure free survival FFS), toxiciteit en biochemische respons. 63 artikels werden weerhouden
na selectie op titel en abstract. Hiervan werden 9 studies geselecteerd na lezen van de volledige
tekst: deze werden beoordeeld op kwaliteit door middel van een ‘modified Delphi technique’.
Twee studies werden uiteindelijk weerhouden: een retrospectieve cohort studie door Culp et al.
die zowel radiotherapie als een chirurgische aanpak onderzocht, en een case-control studie door
Heidenreich et al. die enkel prostatectomie bekeek.
Resultaten: In beide studies was er een OS voordeel bij behandeling met radiotherapie (RT) of
radicale prostatectomie (RP), in vergelijking met enkel een systemische aanpak. Culp et al.
toonden een betere DSS rate aan voor zowel RT als RP, Heidenreich et al. bevestigden dit voor
RP. De absolute DSS die Heidenreich et al. waarnamen, was niet significant beter voor de
geopereerde patiënten, in vergelijking met de controle groep. Culp et al. voerden een analyse
uit op subgroepen gebaseerd op leeftijd, PSA level, en M stagering: de resultaten waren
gelijkaardig aan die van de volledige groep. De auteurs vonden ook enkele factoren die

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 9
onafhankelijk geassocieerd zijn met een slechtere overlevingskans: leeftijd ≥ 70 jaar, cT4
ziekte, PSA ≥ 20 ng/ml, hooggradige maligniteit, en aangetaste lymfeklieren in het bekken.
Conclusie: Lokale therapie onder de vorm van radiotherapie of chirurgie lijkt een meerwaarde
te zijn in patiënten met primair gemetastaseerde PCa. Er is een voordeel in totale overleving en
ziektespecifieke overleving in vergelijking met patiënten die enkel systemisch behandeld
worden. Het is niet mogelijk om op basis van deze thesis een besluit te maken over de meest
voordelige lokale therapie, of over de eigenschappen die een patiënt meest geschikt maken voor
deze aanpak. Door het gebrek aan gerandomiseerde en prospectieve onderzoeken, en de
verschillende tekortkomingen in de huidige evidentie, kan op dit moment de toevoeging van
lokale behandeling niet aanbevolen worden als nieuwe standaardtherapie. Er zijn momenteel
verscheidene prospectieve trials gepland, die binnen afzienbare tijd voor sterkere bewijzen
kunnen zorgen, en meer onderbouwde adviezen zullen formuleren.

p. 10 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 11
III. Contents
I. Acknowledgements ......................................................................................................................... 5
II. Abstract ........................................................................................................................................... 7
1. Abstract ........................................................................................................................................... 7
2. Nederlandstalig abstract .................................................................................................................. 8
III. Contents ..................................................................................................................................... 11
IV. Abbreviations ............................................................................................................................ 13
V. Introduction ................................................................................................................................... 14
1. Epidemiology and incidence of prostate cancer ............................................................................ 14
2. Outcome and survival of PCa ........................................................................................................ 14
3. Metastatic prostate cancer ............................................................................................................. 15
3.1. Epidemiology and incidence ................................................................................................. 15
3.2. Survival and outcome ............................................................................................................ 16
3.3. Treatment of metastatic prostate cancer ................................................................................ 18
3.4. The use of local therapy in PCa ............................................................................................ 19
a. Delaying Local progression .................................................................................................. 20
b. Preventing further metastasis and inhibiting growth of existing metastases and progression
of the disease ................................................................................................................................. 20
c. Benefit for local treatment in PCa and other malignancies ................................................... 21
d. Improved response to systemic therapy ................................................................................ 22
4. Local treatment in metastatic PCa ................................................................................................. 22
VI. Materials and methods .............................................................................................................. 23
1. Research question and PICO ......................................................................................................... 23
2. Article selection............................................................................................................................. 23
3. Qualitative synthesis ..................................................................................................................... 25
VII. Results ....................................................................................................................................... 27
1. Study description ........................................................................................................................... 27
2. Outcomes ....................................................................................................................................... 27
2.1. Overall survival ..................................................................................................................... 28
a. Survival rates ......................................................................................................................... 28
b. Subset analysis by Culp et al. ................................................................................................ 29
2.2. PCa-specific survival............................................................................................................. 30
a. Survival rates ......................................................................................................................... 30
b. Subset analysis by Culp et al. ................................................................................................ 31
2.3. FFS in Heidenreich et al. ....................................................................................................... 32
VIII. Discussion ................................................................................................................................. 33
p. 12 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
1. Diversity of patients and selection bias ......................................................................................... 33
1.1. Selection criteria .................................................................................................................... 33
1.2. Number of included patients.................................................................................................. 34
2. Data collection ............................................................................................................................... 35
3. Identification of patients ................................................................................................................ 35
4. Outcomes ....................................................................................................................................... 37
5. Other Literature ............................................................................................................................. 38
6. Future studies ................................................................................................................................. 40
7. Limitations of this thesis................................................................................................................ 40
IX. Conclusion ................................................................................................................................. 43
X. Bibliography .................................................................................................................................. 44
XI. Appendix ...................................................................................................................................... i
1. Distribution of mPCa ........................................................................................................................ i
2. Description of the 9 selected studies selected by literature search ................................................. iii
3. Patient characteristics Heidenreich et al. ........................................................................................ iv
4. Patient characteristics Culp et al. ..................................................................................................... v
5. Subset analysis by Culp et al. ......................................................................................................... vi
6. Future studies ................................................................................................................................ viii

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 13
IV. Abbreviations
PCa Prostate cancer
mPCa Metastatic prostate cancer
PSA Prostate-specific antigen
SEER study The Surveillance, Epidemiology and End
Results study
TNM Classification of Malignant Tumours:
- T describes the size of the original
(primary) tumour and whether it has
invaded nearby tissue
- N describes nearby (regional) lymph
nodes that are involved
- M describes distant metastasis
RT Radiotherapy
BT Brachytherapy *
RP Radical prostatectomy
NSR No surgery or radiotherapy (control group)
OS Overall survival
DSS Disease specific survival (PCa specific
survival): the time from start to treatment to
disease progression or disease related death
ADT Androgen deprivation therapy
SHR Subhazard ratio
LT Local treatment
* Culp et al. only mention brachytherapy (BT), but different forms of radiotherapy are
included in the study. The term BT is used in Results to be consistent with the original study.
p. 14 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
V. Introduction
1. Epidemiology and incidence of prostate cancer
In 2010, prostate cancer (PCa) was the highest 5-year prevalent cancer in Belgian men with
363.9/100,000 person years (adjusted to the world standard population), or 43,984 cases. [1, 2]
Prostate cancer is typically found in elderly men: more than 50% of the Belgian PCa patients
were 70 years or older in 2010. Despite this general elderly patient population, men older than
80 years have a significantly lower risk of diagnosis, and this number is dropping even further
since the latest recommendations against PCa screening. The risk of dying of PCa however,
keeps rising with age. [1-4]
Presently, most PCa are diagnosed by prostate biopsies after an abnormal PSA-test in
asymptomatic men. [3] The increased use of PSA-testing influenced not only the number of
PCa diagnoses, but also caused a stage migration and a relatively younger patient population.
The SEER (Surveillance, Epidemiology and End Results) study of the US National Cancer
Institute reports an increasing number of diagnosis of organ-confined PCa, but this evolution is
changing since the new screening recommendations. Decreased screening causes a reduction in
diagnosis of intermediate and high risk PCa, and a small increase in non-localized PCa. These
results give cause for concern that in future years the diagnosis of advanced disease may rise
again. [3-6]
2. Outcome and survival of PCa
The prognosis and survival of PCa patients has improved immensely during the last decade due
to earlier diagnosis and new therapies. Overdiagnosis and the detection of clinically
insignificant PCa have also contributed to the better outcomes. At present, the 5-year relative
survival rate for men with local and regional prostate cancer is 100%. [3, 5, 7, 8]
Prostate cancer has a remarkably high incidence-to-mortality ratio, meaning a large part of men
diagnosed with PCa will die of other, unrelated, causes. This is very clearly to see in the Belgian
PCa cases from 2004 to 2008: the 5-year observed survival rate is 77.6% and the 5-year relative
survival rate is 95.3%. Despite this optimistic ratio, PCa mortality is still considerable because

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 15
of its frequent occurrence: 9.3% of all cancer deaths in Belgian men in 2008 were caused by
PCa. [6, 9]
3. Metastatic prostate cancer
3.1. Epidemiology and incidence
Presently, about 4% of prostate cancer patients already have metastases at the moment of
diagnosis. The evolution in incidence is not exactly the same as for PCa in general. The SEER
program in the USA observed a decrease in stage IV PCa with distant metastasis at diagnosis:
incidence fell from 18.4 per 100,000 in 1988 to 6.7 per 100,000 in 2003, an average reduction
of 8.0% per year (Figure 1). As mentioned before: this evolution mostly is explained by
screening tactics and PSA-testing: diagnoses are made at an earlier stage. Again, this decline in
stage is combined with a younger age at moment of diagnosis. The proportion of men aged 60
or less at diagnosis rose from 8.5% in 1988 to over 15% in 2003. A distribution of mPCa for
age and other variables can be found in the Addendum (Addendum Table 1 and Addendum
Table 2). This evolution is less pronounced than the age shift in PCa in general, but still
significant. But there is reason for caution: as mentioned before, the new PCa screening tactics
may turn this evolution around. [4, 5, 8, 10]
Figure 1: Incidence of PCa, metastatic at first presentation (USA, 1975–2012) [10]

p. 16 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
3.2. Survival and outcome
The SEER study in the USA registered a 25.0% survival for patients diagnosed with distant
metastasis in 1988, rising to 27.0% in 2001. A part of this improvement in survival is due to the
earlier detection and less advanced state, even in metastatic disease. But this small rise in
survival rate is hardly significant, especially when compared to the enormous progression for
prostate cancer in general. [5, 7, 8]
The age-adjusted survival rates in Belgium for 2004-2008 for different stages of PCa show how
both age and stage are important for prognosis: for stage I and II, all age groups have a 5-year
relative survival rate of practically 100%. [6] In stage III there is a difference in the different
age groups: patients between 15-74 years have a 5-year relative survival of almost 100%,
patients older than 75 have a rate of only 89.4%. [6]
Figure 2: PCa relative survival by stage (Belgium, 2004-2008) [6]
This difference only grows bigger in stage IV: the prognosis is poor for all age groups, but the
oldest patients have the most unfavourable predictions. Patients between 15 and 59 years have
a 5-year survival rate of 63.3%, between 60-74 years the rate decreases to 58.6%, and for
patients older than 75 years the rate has dropped to 40.4%. [6] The relative survival by age
group and stage for Belgian men in 2004-2008 can be seen in Figure 2 and Table 1, by Schutter
et al.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 17
Table 1: PCa, relative survival by age group (Belgium, 2004-2008) [6]
Even with the most up-to-date therapies, survival rates are depressing for men diagnosed with
mPCa. Several studies recently investigated the progress of survival with the current standard
of care.
The SWOG-phase 3 trials (performed by the South West Oncology Group) confirm these
improved survival trends again in men with newly diagnosed M1 metastatic prostate cancer.
The overall survival of patients receiving similar ADT (Androgen Deprivation Therapy) was
compared before and after PSA testing became standard screening. After adjusting for other
risk factors it was found that overall survival improved significantly for all groups of men. It is
possible that the latest screening recommendations undo this survival profit. [4, 5]
An important insight on survival outcomes and prognostic factors for men with newly
diagnosed M1 disease, treated with standard-of-care therapy, can be found in the control arm
of the STAMPEDE trial. This ‘Systemic Therapy in Advancing or Metastatic Cancer:
Evaluation of Drug Efficacy: A Multi-Stage Multi-Arm Randomised Controlled Trial’
randomised and followed a cohort of PCa patients, of which 917 were newly diagnosed
metastatic patients. Outcome for this group was, as expected, not very good. Median FFS (FFS:
Failure Free survival: the time from start to treatment to disease progression or disease related
death) for the entire group was 11.2 months, median OS was 42.1 month (OS: Overall Survival:
the time from start of treatment to any cause of death). Two year estimate for FFS was 29%,
for overall survival 72%.
Several factors independently influenced these outcome rates: primary tumour stage, initial
Gleason sum score category, metastases grouping, age group, and WHO performance status are
associated with both OS and FFS. A lower two-year survival was observed in patients with
bone metastases and soft tissue metastases at the same time. A worsened FFS was seen in
patients with higher PSA level before starting ADT and in patients with higher primary tumour
stage. [7]

p. 18 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
A significant evolution for survival of mPCa patients was adding chemotherapy to ADT.
Several RCT’s (CHAARTED, GETUG-15, STAMPEDE) showed that the addition of
docetaxel improved both failure-free and overall survival. The addition of docetaxel is now
recommended as the standard of care in men with newly diagnosed mPCa. [11]
The STAMPEDE and other randomised trials confirm the conclusions of other research and
studies. Survival of newly diagnosed prostate cancer has improved somewhat over the years,
mostly due to PSA screening and new treatments, but outcomes are still depressing. [5, 7, 8]
3.3. Treatment of metastatic prostate cancer
The most recent guidelines on the treatment of mPCa by the European Association of Urology
state that luteinising hormone-releasing hormone (LHRH) agonists are the standard of care in
mPCa. They provide reversible androgen deprivation and can be used in intermittent therapy.
[12] Recently, adding docetaxel to ADT is recommended as the new standard of care for mPCa
patients. [11]
Other options are less frequently used, or only for specific indications (Table 2).
LHRH antagonists decrease testosterone levels without any testosterone surge, and they may
have an oncologic benefit compared with LHRH analogues. This has yet to be confirmed in
prospective trials. Anti-androgen monotherapy may be an option in locally advanced or M0
patients, but not in mPCa. Maximum androgen blockade with anti-androgens has a small
advantage over LHRH monotherapy for survival, but causes significant impairment of quality
of life. Intermittent androgen deprivation has equal oncologic efficacy when compared with
continuous ADT, in well-selected populations. For mPCa, there is no significant survival
advantage for early ADT compared with delayed ADT. [12]
Additional local treatments in mPCa are at present only used for relapsing mPCa, symptomatic
relief or palliative treatment. [12]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 19
Table 2: indications for hormonal therapy in mPCa [12]
3.4. The use of local therapy in PCa
Local therapy of the prostate has long proven its worth in treatment of non-metastatic tumours.
From the moment the cancer expands beyond the prostate capsule, systemic treatment becomes
the standard of care. Local treatments are then only offered to reduce local symptoms and to
assist palliative care. [13] However, systemic treatment alone is often not sufficient. Many
patients with mPCa ultimately develop resistance to hormonal therapy, and will need alternative
or additional treatment. [14]
In many other metastatic cancers, studies have shown a positive influence of local treatment,
either radiotherapy or surgery, on survival rates, but its benefit in mPCa remains uncertain. [13-
15]. There are several possible theories why adding local therapy could improve survival rates:
delaying local progression, removal of a persistent source of possible metastasis, and an
improved response to systemic treatment through debulking and decreasing tumour burden. So
far, none of these theories are supported by extensive evidence. [14, 16]

p. 20 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
a. Delaying Local progression
Local progression can cause serious morbidity with a strong impact on the quality of life of the
patient: ureteral and bladder outlet obstruction, perineal or bony pain, … [16, 17] Adding
prostatectomy or radiotherapy to ADT in N+ patients delays local progression compared to
ADT alone. [16] The profits of local therapy are very clear, but there is no evidence so far for
metastatic PCa. It is possible that surgery or radiation therapy in mPCa could have a positive
impact on survival rates by delaying local progression, instead of only relieving symptoms, as
it already does for N+ or locally confined PCa.
b. Preventing further metastasis and inhibiting growth of existing
metastases and progression of the disease
There are many studies describing the relationship between the primary tumour and its
metastases. Some argue that metastases are a result of progression of locoregional lymphatic
disease, and thus require early detection and cure. Others propose that cancer is a systemic
disease; local therapies are not as important as systemic therapy. [13-15, 18] Although none of
these hypotheses have been proven with RCT’s, they are more or less accepted and used to
explain the effect of local therapies in some malignancies.
A first reason for local therapy, is the assumption that the primary tumour and its metastases
are communicating systems, in a complex network with several molecular pathways. An
uncontrolled local tumour probably promotes the growth of its metastases, as well as creating
new ones. It should also be considered that the primary PCa can synthesise testosterone from
weak adrenal androgens, and be a source of intraprostatic androgen even after ADT. Therefore
attacking the primary tumour with local therapy, can have an effect on the linked metastases.
[13, 14]
The ‘tumour seeding’ theory states that the primary tumour is responsible for priming an
environment for metastatic growth. Consequently, metastasis can be prevented with local
therapy of the primary tumour. There could be no preparation of distant tissue for metastatic
cell arrival, and the amount of possible metastases could be reduced with local control of the
primary source. The continuous cycle of metastases becoming metastatic tumours themselves
might be avoided as well. [14, 15, 19, 20]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 21
Another claim for additional local therapy is the abscopal effect: the phenomenon of regression
of distant disease after the primary tumour is treated locally. This effect is mostly attributed to
the activation of anti-tumour immunity, with a positive systemic effect. The local inflammation
caused by radiotherapy starts a cascade of immune reactions, leading to a targeted T-cell
response against both tumour and metastases. This immune response is empowered by
hormonal therapy. ADT has an effect on the gene expression in tumour cells, changing the
cellular and membrane environment. This modifies tolerance and enables the immune system
to recognise the tumour cells, an effect that is in its turn strengthened by local radiotherapy, and
leads to tumour cell death. [19]
c. Benefit for local treatment in PCa and other malignancies
There is plenty of evidence for the benefit of local treatment in other forms of PCa and other
tumours. Local control of the tumour has improved survival in patients with metastatic colon
cancer, renal cell carcinoma, glioblastoma, ovarian cancer. Decreasing the primary tumour
burden also has an effect of increasing response to systemic chemotherapy in breast cancer,
colon cancer, and ovarian cancer. Many studies suggest that metastatic PCa may react in a
similar way. [14, 16]
There are several studies confirming a positive impact of adding a local therapy to systemic
treatment in patients with locally advanced or lymph node positive PCa. Many studies and
reviews show a long lasting survival benefit in favour of the N+M0 patients receiving a local
treatment to the primary tumour, compared to those treated systemically only. At present, there
are three large prospective randomized phase III trials suggesting that, in patients with locally
advanced tumours with high risk of occult micrometastases, the 10-year outcome can be
improved by adding radiotherapy to androgen deprivation (D’Angelillo et al., 2015; Mottet et
al., 2012; Warde et al. 2011). [19]
The results for additional local therapy in similar metastatic malignancies or mPCa are
promising. Further research for the benefits of local therapy in metastatic prostate cancer is
certainly appropriate, based on this matching evidence in other fields.
p. 22 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
d. Improved response to systemic therapy
Metastatic PCa appears to increase in heterogeneity as it progresses. The result is variable
androgen responsiveness, resistance to chemotherapy, proliferation, risk of metastasis…
Studies in N+ suggest that local treatment could eliminate some of this heterogeneity, and thus
improve the success of systemic therapy. It seems logical that this argument can be used for
M+ prostate cancer as well. [16] As mentioned before, the abscopal effect depends on an
improved response to systemic therapy as well. ADT and radiotherapy empower each other,
resulting in a more effective remedy. [19]
4. Local treatment in metastatic PCa
The last decades have meant an enormous progress for the treatment of prostate cancer, but
metastatic PCa still has dramatic survival rates. Even the newest recommendations for therapy
promise only small profit in survival rates. Survival and incidence rates show that in this group
of relatively young and otherwise healthy men, there is still a lot of potential health to gain.
Other options need to be explored, and additional local treatment is supported by many
arguments. However, these claims presented in literature are all theoretical, backed by evidence
in other malignancies or experiences in non-metastatic PCa.
The goal of this literature review is to summarise and critically review the existing data, and to
determine if there is conclusive evidence for a survival benefit for local treatment combined
with systemic treatment in newly diagnosed metastatic prostate cancer patients, compared to
systemic treatment alone.
The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 23
VI. Materials and methods
1. Research question and PICO
The research question for this thesis is: “Does local treatment of the prostate improve the
survival rate or clinical outcomes of patients with primary metastatic prostate cancer.” This
question was framed in terms of population, interventions, controls, and outcome (PICO). The
result is as follows:
Patient: men with newly diagnosed metastatic (Tx, Nx, M+) prostate cancer (not metastatic
recurrence).
Intervention: Local treatment of the primary prostate cancer, whether or not combined with
systemic therapy. This local treatment includes, but is not restricted to: radiotherapy, radical
prostatectomy, and/or combinations.
Controls: treatment with systemic therapy alone, at present the standard-of-care for men with
newly diagnosed metastatic prostate cancer.
Outcome: Overall survival rate, progression free (or failure free) survival rate, toxicity,
biochemical response.
For each term, a selection of appropriate Mesh descriptors were selected, as well as relevant
text words to include suitable articles.
2. Article selection
Potential articles were then selected in the Ovid database, with Ovid MEDLINE, Ovid
MEDLINE in-process & other non-indexed citations and Ovid MEDLINE Daily Update as
selected resources. No limitations were set for publication language or publication year.
Using the search strategy: “(exp prostatic neoplasms/ or prostat* cancer.tw.) and (Neoplasms
metastasis/ or metast*.tw.) and (Local treatment.tw. or local therapy.tw. or Exp radiotherapy/
or radio?therapy.tw. or radiation therapy.tw. or exp prostatectomy/ or radical
prostatectomy.tw.)”, 4511 articles were found on 12/06/2015.

p. 24 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
Other sources added 13 articles. The last articles were added on 6/02/2016. Additional studies
were identified through related citations and bibliographies of relevant articles, adding 2 new
articles. After removing 112 duplicates, title and abstract were reviewed for relevance to the
research question. The remaining articles (63) were assessed by full text. Studies were excluded
if they did not meet the PICO framework. Because of the small amount of research on this
subject, all types of studies (such as randomized controlled trials, cohort, case series etc.) were
included. Other sorts of publication types, such as reviews, commentaries, editorials, were
excluded. Articles without available full text were excluded as well. 9 studies were selected
based on full text.
The selection process can be seen in the PRISMA diagram below (Figure 3).
Figure 3: PRISMA Diagram for literature selection

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 25
3. Qualitative synthesis
Potential studies were identified from the selected articles, as described in the PRISMA
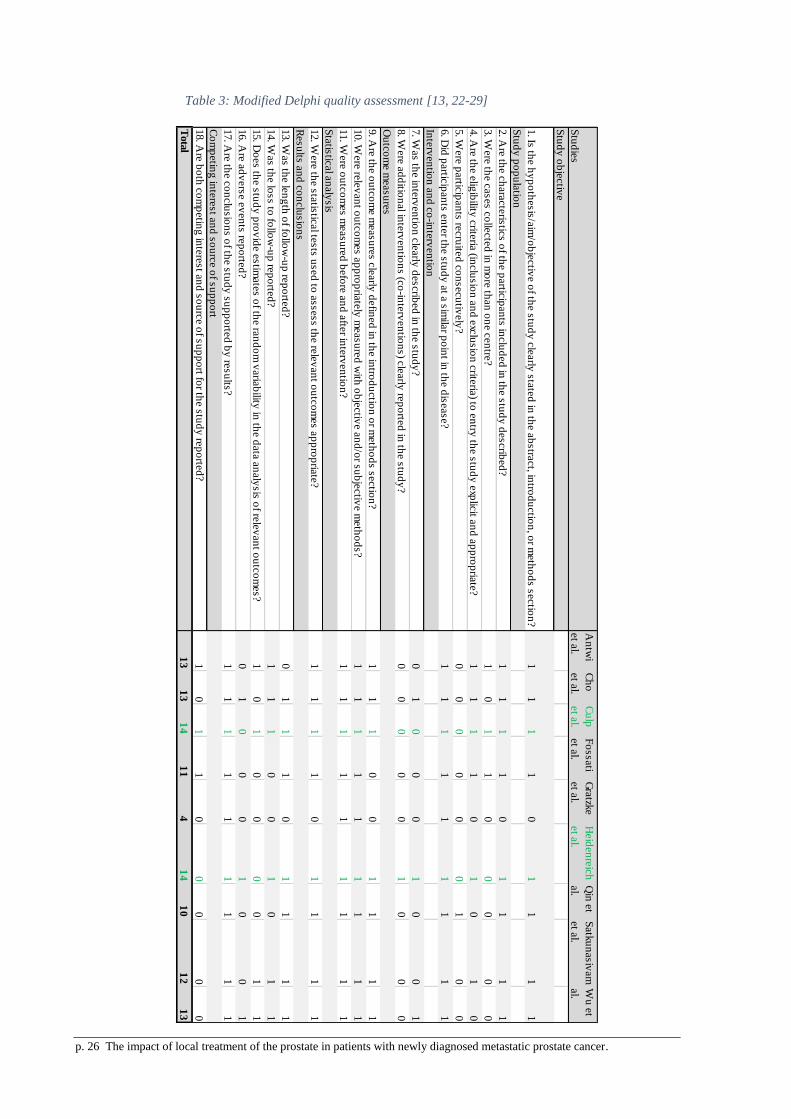
diagram. The 9 selected studies were assessed for quality with the “quality appraisal tool for
studies using a modified Delphi technique”, including assessment of study objectives,
interventions, outcome measures, statistical analysis, and more. The assessment tool uses
indicators of the overall quality and identifies the risk of bias, with items such as ‘selection of
consecutive cases’, ‘key outcomes measured before and after the intervention’, and
‘information provided on the loss to follow-up’. This ‘modified Delphi’ was the most
appropriate assessment tool, considering the variability of study designs.
A study with 14 or more positive responses is considered to be of acceptable quality. [21] Only
2 studies met this threshold: a retrospective cohort study by Culp et al. and a case-control study
by Heidenreich et al.
A brief description and the complete quality assessment for all 9 studies can be found
respectively in Addendum Table 3 and Table 3.
p. 26 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
Stu
die
s
An
twi
et a
l.
Ch
o
et a
l.
Cu
lp
et a
l.
Fo
ssati
et a
l.
Gra
tzke
et a
l.
Heid
en
reic
h
et a
l.
Qin
et
al.
Satk
un
asiv
am
et a
l.
Wu
et
al.
Stu
dy
ob
jectiv
e
1. Is
the h
yp
oth
esis
/aim
/ob
jectiv
e o
f the s
tud
y c
learly
sta
ted
in th
e a
bstra
ct, in
trod
uctio
n, o
r meth
od
s s
ectio
n?
11
11
01
11
1
Stu
dy
po
pu
latio
n
2. A
re th
e c
hara
cte
ristic
s o
f the p
artic
ipan
ts in
clu
ded
in th
e s
tud
y d
escrib
ed
?1
11
10
11
11
3. W
ere
the c
ases c
olle
cte
d in
mo
re th
an
on
e c
en
tre?
10
11
00
00
0
4. A
re th
e e
ligib
ility c
riteria
(inclu
sio
n a
nd
exc
lusio
n c
riteria
) to e
ntry
the s
tud
y e
xplic
it an
d a
pp
rop
riate
?1
11
10
10
10
5. W
ere
partic
ipan
ts re
cru
ited
co
nsecu
tively
?0
00
00
01
00
6. D
id p
artic
ipan
ts e
nte
r the s
tud
y a
t a s
imila
r po
int in
the d
isease?
11
11
11
11
1
Inte
rven
tion
an
d c
o-in
terv
en
tion
7. W
as th
e in
terv
en
tion
cle
arly
describ
ed
in th
e s
tud
y?
01
00
01
00
1
8. W
ere
ad
ditio
nal in
terv
en
tion
s (c
o-in
terv
en
tion
s) c
learly
rep
orte
d in
the s
tud
y?
00
00
01
00
0
Ou
tco
me m
easu
res
9. A
re th
e o
utc
om
e m
easu
res c
learly
defin
ed
in th
e in
trod
uctio
n o
r meth
od
s s
ectio
n?
11
10
01
11
1
10. W
ere
rele
van
t ou
tco
mes a
pp
rop
riate
ly m
easu
red
with
ob
jectiv
e a
nd
/or s
ub
jectiv
e m
eth
od
s?
11
11
11
11
1
11. W
ere
ou
tco
mes m
easu
red
befo
re a
nd
afte
r inte
rven
tion
?1
11
11
11
11
Sta
tistic
al a
naly
sis
12. W
ere
the s
tatis
tical te
sts
used
to a
ssess th
e re
lev
an
t ou
tco
mes a
pp
rop
riate
?1
11
10
11
11
Resu
lts a
nd
co
nclu
sio
ns
13. W
as th
e le
ng
th o
f follo
w-u
p re
po
rted
?0
11
10
11
11
14. W
as th
e lo
ss to
follo
w-u
p re
po
rted
?1
11
00
10
11
15. D
oes th
e s
tud
y p
rov
ide e
stim
ate
s o
f the ra
nd
om
varia
bility
in th
e d
ata
an
aly
sis
of re
lev
an
t ou
tco
mes?
10
10
00
01
1
16. A
re a
dv
ers
e e
ven
ts re
po
rted
?0
10
00
10
01
17. A
re th
e c
on
clu
sio
ns o
f the s
tud
y s
up
po
rted
by
resu
lts?
11
11
11
11
1
Co
mp
etin
g in
tere
st a
nd
so
urc
e o
f su
pp
ort
18. A
re b
oth
co
mp
etin
g in
tere
st a
nd
so
urc
e o
f su
pp
ort fo
r the s
tud
y re
po
rted
?1
01
10
00
00
Tota
l1
31
31
41
14
14
10
12
13
Table 3: Modified Delphi quality assessment [13, 22-29]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 27
VII. Results
1. Study description
The study selection process is outlined in the PRISMA diagram (Figure 3). Nine studies were
found through a literature search: 4 retrospective case series, 3 retrospective cohort studies, 1
case-control study and 1 prospective, controlled, non-randomized study. There was significant
variation in inclusion criteria, in additional local therapies in the intervention groups, and in
reporting of outcomes. (summary in Addendum Table 3). [13, 22-29]
Two studies were selected after quality assessment: Culp et al. (a retrospective cohort study),
and Heidenreich et al. (a case-control study) were considered to be of sufficient quality. Culp
et al. describe 8185 patients selected from the SEER database, consisting of population-based
cancer registries, between 2004-2010. Both radical prostatectomy (RP) and radiotherapy (RT)
are included. In the study only brachytherapy (BT) is mentioned, but different forms of
radiotherapy are included (the term BT will be used in Results to be consistent with the original
study). Heidenreich et al. selected two groups of patients: 23 patients with low volume
metastatic disease who were treated with RP, and a control group of 38 men initially treated
with ADT only. The patient characteristics of both studies can be found in the Addendum:
Addendum Table 4 and Addendum Table 5.
2. Outcomes
Outcomes in the selected studies are similar: OS (overall survival) and PCa-specific survival
(further referred to as disease specific survival [DSS], to be consistent with the original study)
are registered in both. Culp et al. also determined ‘factors associated independently with cause-
specific mortality’, Heidenreich et al. added FFS (failure free survival). The latter also reported
on complications of surgery and functional outcomes, describing feasibility of RP, that are not
relevant for this study: these results will not be described further. Other outcomes like toxicity
of radiotherapy or biochemical response were not registered in these studies.

p. 28 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
2.1. Overall survival
a. Survival rates
Culp et al. reported 5-yr OS rates with a median follow-up of 16 months. The 5-yr OS was
significantly higher in patients who had local treatment: RP (67.4%; 95% confidence interval
[CI], 58.7–74.7) or BT (52.6%; 95% CI, 39.8–63.9) compared with NSR (no surgery or
radiotherapy) patients (22.5%; 95% CI, 21.1–23.9) ( p < 0.001). This result is confirmed in a
multivariable competing risks regression, showing adjusted subhazard ratios for RP, BT and
NSR. With non-local treatment as the reference group, radical prostatectomy and brachytherapy
have an adjusted SHR (subhazard ratio) of 0.38 (95 %CI: 0.27-0.53, p<0.001) and 0.68 (95%
CI: 0.49-0.93, p=0.018), respectively. (Table 4). Non-PCa caused deaths were seen in 15.7%
of the patients (1284 in total), but there was no significant difference among the various groups.
[22]
A second analysis was performed, excluding patients who died within 12 months from
diagnosis. This analysis was performed to reduce bias by excluding patients who might benefit
least from local therapy: patients with progressive disease, significant comorbidity, or history
of other primary malignancies. Results were similar to those for all patients: at a median follow-
up of 27 months (IQR: 18–42), 5-yr OS was still higher in patients undergoing RP (76.5%; 95%
CI, 67.0–83.7) or BT (58.2%; 95% CI, 44.5–69.7), compared with NSR patients (30.6%; 95%
CI, 28.9–32.4) ( p < 0.001). (Table 4) [22]
Heidenreich et al. compared radical prostatectomy with a control group of ADT. The local
treatment group had an overall survival rate of 91.3%, with a median follow-up of 40.6 months.
The control group was followed for a median time of 44.0 months, with an OS of 78.9%. The
p-value for comparing these groups was 0.048 (Table 5).

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 29
Table 4: Results from Culp et al.
5yr-OS, % adjusted SHR DSS 5 yr-probability (%)
all patients NSR 22.5; 95% [CI], 21.1–23.9 reference group 48.7
RP 67.4; 95% [CI], 58.7–74.7 0.38; 95 %[CI] 0.27-0.53 75.8
BT 52.6; 95% [CI], 39.8–63.9 0.68; 95%[CI] 0.49-0.93 61.3
2nd analysis NSR 30.6; 95% [CI], 28.9–32.4 reference group 46.9
RP 76.5; 95% [CI], 67.0–83.7 0.37; 95% [CI] 0.26–0.54 75.1
BT 58.2; 95% [CI], 44.5–69.7 0.57; 95% [CI] 0.37–0.87 64.5
p<0,001
p<0,05
p not significant/ no p-value
b. Subset analysis by Culp et al.
Culp et al. performed subset analysis to find out if overall survival is different among groups
based on age (<70 yr or ≥70 yr old) or PSA (<20 or ≥ 20 ng/ml).
For both age groups, OS rates were significantly higher for local treatment compared to the
NSR controls. In men <70 yr, 5-yr OS was 71.2% (95% CI, 61.6–78.9) for the RP group, 57.4%
(95% CI, 22.6–66.6) for the BT group, compared with 28.9% (95% CI, 26.6–31.3) for the
controls (p<0.001). In men ≥70 yr, 5-yr OS was 50.3% (95% CI, 30.1–67.5) for the RP group,
48.5% (95% CI, 30.0–64.7) for the BT group, compared with 18.1% (95% CI, 16.5–19.8) for
the controls (p<0.001). (Addendum Table 6 and Addendum Table 7)
In the subset analysis for PSA, OS rates were significantly higher in patients with additional
local treatment in both subgroups (<20 or ≥20ng/ml), compared to no local treatment. In men
with PSA <20 ng/ml, treatment with RP had a 5-yr OS rate of 77.1% (95% CI, 66.1-85.0), BT
had 71.2% (95% CI, 46.8–85.9), compared to 33.7% (95% CI, 30.4–37.1) for NSR (p<0.001).
The subgroup with PSA ≥20ng/ml, had 5-yr OS rate of 55.7% (95% CI, 37.1-70.9) for RP,
37.3% (95% CI, 21.4-53.2) for BT, compared to 19.8% (95% CI, 18.2-42.3) for NSR (p<0.001
and <0.05, respectively). (Addendum Table 6 and Addendum Table 7)
Another analysis was performed to determine if the outcomes of the different treatment are
influenced by the extent of metastatic disease, based on AJCC M stage (M1a-c). Although these
results reflect the trend of the previous outcomes, many were not significant. Patients treated
with RP had a significantly higher OS in M1b and M1c disease, compared to NSR patients. RP
in M1b had 5-yr OS rates of 70.1 % (95% CI, 58.1-79.2) compared to 22.9% (95% CI, 21.2-

p. 30 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
24.6) in controls (p<0.001). RP in M1c had 60.7% (95% CI, 42.7-74.6) OS rates, compared to
18.6% (95% CI, 16.1-21.2) in controls (p<0.001). (Addendum Table 6 and Addendum Table
7)
In patients treated with BT, OS was significantly higher regardless of M stage. In M1a patients,
5-yr OS rates were 54.7% (95% CI, 8.6–86.2) for BT, compared to 35.1% (95% CI, 28.0–42.3)
for controls (p = 0.014). In M1b, 5-yr OS rates were 55.0% (95% CI, 31.1-64.5) for BT,
compared to 22.9% (95% CI, 21.2-24.6) for controls (p <0.001). In M1c, 5-yr OS rates were
53.4% (95% CI, 34.4-69.2) for BT, compared to 18.6% (95% CI, 16.1-21.2) for controls
(p<0.001). (Addendum Table 6 and Addendum Table 7)
The study tried to identify factors independently associated with lower survival rates in patients
with local treatments. These factors included age ≥ 70 yr, cT4 disease, PSA ≥ 20 ng/ml, high-
grade disease, and pelvic lymphadenopathy. Patients with none or only one of these factors (n
= 181 [48.4%]) had the highest OS (77.3%; 95% CI, 67.4–84.5) probability. Patients with two
factors (n = 116 [31.0%]) had a lower 5-yr OS (53.1%; 95% CI, 38.9–65.4), but this survival
rate is still better than for patients without local treatment. (Addendum Table 6 and Addendum
Table 7)
2.2. PCa-specific survival
a. Survival rates
In Culp et al. both RP or BT were each independently associated with improved DSS, with
predicted 5-yr DSS probabilities of 75.8% for RP and 61.3%, for BT, compared with 48.7% for
NSR patients. There was no significant difference in DSS between RP and BT. [22] The second
analysis on DSS, excluding patients who died within 12 months from diagnosis, showed similar
results: treatment with RP (subhazard ratio [SHR]: 0.37; 95% CI, 0.26–0.54; p < 0.001) or BT
(SHR: 0.57; 95% CI, 0.37–0.87; p = 0.01) was still each independently associated with
decreased DSS compared with NSR patients, with 5-yr DSS probabilities of 75.1%, 64.5%, and
46.9%, respectively. [22] (Table 4)
Heidenreich et al. found that the median DSS in the radical prostatectomy group was 47 (range
9-71) months, and 40.5 (19-75) months in the control group. An extra analysis on the control
group was performed with only the patients with a PSA < 1.0ng/ml after 6 months of ADT: this
adapted group had a median DSS of 44.3 (21-75) months. The p-value for comparing DSS was
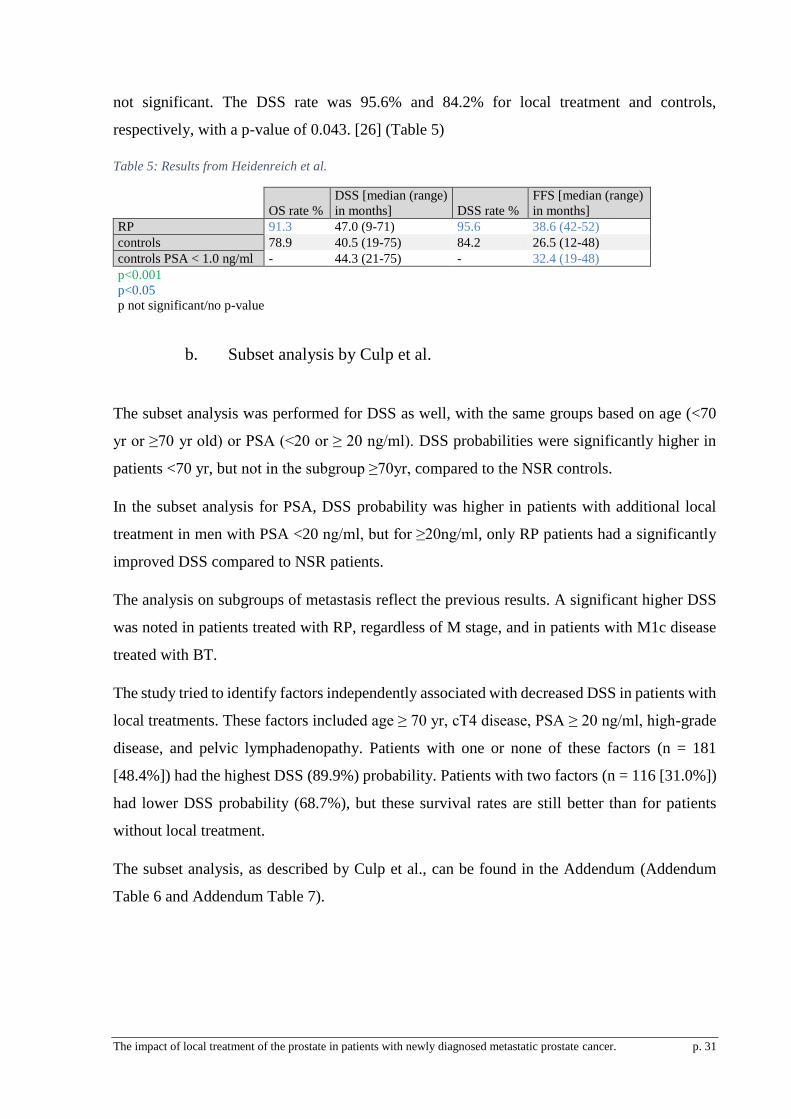
The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 31
not significant. The DSS rate was 95.6% and 84.2% for local treatment and controls,
respectively, with a p-value of 0.043. [26] (Table 5)
Table 5: Results from Heidenreich et al.
OS rate %
DSS [median (range)
in months] DSS rate %
FFS [median (range)
in months]
RP 91.3 47.0 (9-71) 95.6 38.6 (42-52)
controls 78.9 40.5 (19-75) 84.2 26.5 (12-48)
controls PSA < 1.0 ng/ml - 44.3 (21-75) - 32.4 (19-48)
p<0.001
p<0.05
p not significant/no p-value
b. Subset analysis by Culp et al.
The subset analysis was performed for DSS as well, with the same groups based on age (<70
yr or ≥70 yr old) or PSA (<20 or ≥ 20 ng/ml). DSS probabilities were significantly higher in
patients <70 yr, but not in the subgroup ≥70yr, compared to the NSR controls.
In the subset analysis for PSA, DSS probability was higher in patients with additional local
treatment in men with PSA <20 ng/ml, but for ≥20ng/ml, only RP patients had a significantly
improved DSS compared to NSR patients.
The analysis on subgroups of metastasis reflect the previous results. A significant higher DSS
was noted in patients treated with RP, regardless of M stage, and in patients with M1c disease
treated with BT.
The study tried to identify factors independently associated with decreased DSS in patients with
local treatments. These factors included age ≥ 70 yr, cT4 disease, PSA ≥ 20 ng/ml, high-grade
disease, and pelvic lymphadenopathy. Patients with one or none of these factors (n = 181
[48.4%]) had the highest DSS (89.9%) probability. Patients with two factors (n = 116 [31.0%])
had lower DSS probability (68.7%), but these survival rates are still better than for patients
without local treatment.
The subset analysis, as described by Culp et al., can be found in the Addendum (Addendum
Table 6 and Addendum Table 7).

p. 32 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
2.3. FFS in Heidenreich et al.
Heidenreich et al. reported the median months of clinical progression free survival (further
referred to as Failure Free Survival or FFS). Biochemical progression or failure was defined as
a PSA increase to 0.2 ng/ml validated by two consecutive increases at two-week intervals, if
PSA decreased to undetectable serum levels postoperatively. If the postoperative PSA was still
detectable, biochemical progression was defined by two consecutive increases above the first
postoperative PSA, one week apart, resulting in 2.50% increases over the nadir. [26]
The RP group had a median FFS of 38.6 months (range 42-52), the control group had a median
FFS of 26.5 (12-48) months, and the adapted control group (cf. supra) had a median FFS of
32.4 (19-48) months. In the group treated with surgery, all patients had a serum testosterone of
<50ng/dl. In the control group, mean time between start of ADT and symptomatic progression
was 23 months (range 6-52). [26]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 33
VIII. Discussion
Both studies are analogous in their outcomes, as described earlier in ‘Results’. Although these
studies have been assessed for quality, they still have limitations and flaws that should be looked
into before interpreting the results.
1. Diversity of patients and selection bias
1.1. Selection criteria
Methodology and inclusion criteria are significantly different in both studies.
Heidenreich et al. selected 23 patients for their intervention group, with biopsy proven PCa and
low volume metastatic disease who underwent RP. These men were eligible for surgery if they
met 6 inclusion criteria, concerning limited metastatic disease (osseous, lymphatic, visceral)
and possibility of resecting the tumour. The patients received flare-up prophylaxis with
bicalutamide and ADT with LHRH-analogues for at least 6 months. Men with a PSA decrease
to less than 1.0 ng/ml, remission or stable disease of osseous metastases and without the
development of new lymph node or visceral metastases, were considered candidates for surgery.
The control group was 38 men initially treated with androgen deprivation therapy only, and
followed until progression, development of castration resistant PCa or death. There is no
mention of other selection criteria for the control group. [26] The contrast in selection criteria
for both groups could cause serious bias. Although the intervention group was matched for
biological, clinical and oncologic parameters with the control group, it is very likely that
patients were overselected for local treatment.
Culp et al. identified cases from the SEER database between 2004 and 2010. Patients were
selected by age ≥ 35 years. At time of diagnosis, they had to be documented stage IV (M1a-c)
PCa, based on the American Joint Committee on Cancer (AJCC) Cancer Staging Manual (sixth
edition) with either radiographic or pathologic confirmation of metastatic disease through the
Collaborative Staging System. Groups were based on no surgery or radiation therapy (NSR) or
definitive local therapy to the prostate: either radical prostatectomy (surgery site codes 50 or
70) or brachytherapy (radiation-specific codes 2, 3, or 4: respectively meaning radioactive
implants, radioisotopes, and beam radiation combined with 2 or 3). Within the local treatment
group, men were not excluded if they received adjuvant external-beam radiation therapy.

p. 34 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
Relevant data (PSA, age, disease grade, marital status, race, …) was registered at time of
diagnosis, using the SEER coding guidelines. The limitations in selection criteria and data
analysis caused by this SEER coding are mentioned further. [22].
1.2. Number of included patients
In both studies, the number of patients with local treatment is (relatively or absolutely) low
(patient characteristics can be found in Addendum Table 4 and Addendum Table 5). Culp et al.
included a total of 8185 patients, but only 374 of them received additional local treatment: 4.6%
of the selected patients. The reason for adding local treatment was not registered. It is likely
that patients received extra treatment because of better underlying health, and being capable of
tolerating the extra burden. Another possibility is that patients with worse prognosis were
singled out for extra treatment, in the hopes to prolong their survival. Although both groups are
significantly similar in clinical and oncological parameters, selection bias in this study is likely
and could influence the results. [30]
Heidenreich et al. compared two groups, selected in a single institution: 23 patients were treated
with radical prostatectomy, and a control group of 38 patients initially received ADT only. The
intervention group and the control group were matched for biological, clinical and oncologic
data: as shown in Addendum Table 4, almost all p-values for comparing the groups are not
significant, meaning they are significantly similar for (almost) all parameters. However, both
groups have a low number of patients: the chance of statistical error in comparing these groups
is realistic. The diversity in the groups may not be statistically significant because of the lack
of power, but it may influence the outcomes of the study. Furthermore, the low number of
patients in itself and the single-institute selection could bias the results. This should be a point
of attention for future prospective studies: recruiting a sufficient number of patients in several
medical institutions will be necessary to avoid sampling bias. Statistical power should be
ensured by larger numbers as well.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 35
2. Data collection
Culp et al. selected patients from the SEER database, using the SEER coding guideline to
identify suitable patients. Because of this coding, there was no detailed description of the used
interventions possible for selecting patients or analysis of interventions. There is no
specification of used techniques, or of dosage and timing of the therapies. This may have caused
a heterogeneity in the intervention group, influencing the outcomes.
Many relevant variables are not included or coded in the SEER database, and thus not reported
or analysed in this study. These variables are the already mentioned details of therapy, but also
additional interventions, patient performance status, site-specific EBRT codes and comorbidity
or adverse events. [22] These coding guidelines are a serious limitation for this retrospective
study. It’s difficult to define what the best local therapy is, or what patient might benefit most,
without these missing variables. It is also not possible to identify possible confounders that
could influence the results of the study, because of this limited SEER coding.
Data collection in both studies was also limited because of the relative short time of follow-up.
Culp et al. had a median follow-up of 16 months, Heidenreich et al. 40.6 and 44.0 months for
the intervention group and control group respectively. These short periods make it impossible
to evaluate long term outcomes or adversary events. It should also be noted that Heidenreich et
al. make no mention of the period of time for the survival rates: it is unclear if these rates are
calculated for median follow-up time or for the usual 1 or 5 year interval.
3. Identification of patients
Culp et al. performed a subset analysis, trying to mark out patients with better prospects
(Addendum Table 6 and Addendum Table 7). Subgroups were made based on age (<70 yr or
≥70 yr old), PSA (<20 or ≥ 20 ng/ml) or extent of metastatic disease (M1a-c). Several features
were found to be independently associated with decreased DSS, as described in Results: age ≥
70 yr, cT4 disease, PSA ≥ 20 ng/ml, high-grade disease, and pelvic lymphadenopathy. There is
an extra argument for the influence of T and N state: patients with advanced disease have more
potential of ‘leaving disease behind’ after local treatment. The positive effects of RP might be
undone. [22]

p. 36 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
The identification of patients with mPCa who would benefit the most from definitive local
treatment, is also the subject of many research papers.
The factors associated with DSS as described by Culp et al. are very similar to those researched
in the STAMPEDE trials: primary tumour stage, initial Gleason sum score category, metastases
grouping, age group, and WHO performance status. As described in the introduction, these
features are found to have an influence on the survival outcomes and prognosis in newly
diagnosed mPCa patients. Unfavourable scores on these factors predict worse outcomes for
patients, compared to patients without these negative predictors. [7, 22]
The SWOG 8894 trial tried to identify the patients, treated with ADT, with the best long-term
survival odds. The authors suggest that this long-surviving subgroup in mPCa may benefit the
most from additional local treatment of the prostate. Of the patients with mPCa enrolled in the
SWOG 8894 trial, 7% was still alive after 15 years, despite their pessimistic initial presentation.
Several predictors of long-term success for local treatment are suggested: performance status,
diploid tumour, Gleason score, number of nodes involved, seminal vesicle invasion, and the
number of metastatic lesions. [16]
The factors found by Culp et al., associated with improved DSS in patients treated with local
therapy, seem similar to factors associated with overall condition and survival rates in mPCa
patients. The improved DSS in patients treated with local therapy could be (partially) explained
by these independent factors. It is suggested by some articles that only patients with good
overall condition or positive predictors could benefit most from additional therapy. However,
it is not unreasonable that patients with fast progressive mPCa could benefit from local therapy
as well, especially when they quickly evolve to castration-resistant mPCa.
To sum up, mPCa patients are a heterogeneous group with varying survival rates, influenced
by many independent factors. There is a lot of literature to support the suggestions made by
Culp et al. about what patient characteristics can influence the outcomes. It is important that
future prospective studies look carefully at these characteristics, to confirm their impact, and to
make precise recommendations on what patients could benefit the most from additional local
therapy. [7, 19, 22, 26]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 37
4. Outcomes
The local treatments looked at in this thesis are radical prostatectomy and radiotherapy. Both
Culp et al. and Heidenreich et al. researched the effects of prostatectomy, radiotherapy was
researched by Culp et al. only. As mentioned before, the term brachytherapy is used in the
study, but in fact different forms of radiotherapy were included. Heidenreich et al. only looked
into surgery and made no comparison with radiotherapy.
Both Heidenreich et al. and Culp et al. indicate an overall survival benefit for metastatic prostate
cancer patients treated with radiotherapy or radical prostatectomy, compared to systemic
therapy alone. They agree on a significant advantage for patients treated with RP compared
with no local treatment. Culp et al. studied radiotherapy as well, and found here too an OS
benefit compared to the controls without local treatment.
Both studies also compared DSS for local therapy and systemic treatment. Culp et al. showed
a prolonged DSS for RP and BT independently, but Heidenreich et al. found no significant
improvement in DSS for RP. The DSS rate however, found by Heidenreich et al., was
significantly better for the group treated with radical prostatectomy.
Heidenreich et al. looked also at FFS for RP. Patients treated with RP had a longer median time
before PSA elevation, compared to both the control group and the adapted control group. The
ranges of FFS of all three groups overlap each other, indicating that these results may not be
significantly different. There are several possible explanations for this overlap, but the small
number of patients is the most likely.
The possible differences between RP and BT have not been explored by Culp et al. Both
treatments were associated independently with increased OS and DSS, but they were only
compared with the controls, treated with systemic therapy. Comparing the outcomes for the
local treatments in this study is useless: patients were recruited from the SEER database, and
grouped by additional local treatment or no additional local treatment. The reason for additional
local treatment is unknown: it is very likely that the groups are significantly different in
characteristics and prognosis, thus influencing outcomes. The different local treatment groups
should be matched for clinical and oncological characteristics to look at possible differences in
survival.

p. 38 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
The results of the studies are consistent with many literature reviews: adding local therapy
seems beneficial for mPCa patients. Of course, there are many limitations to consider: the
results of the studies may be significant, but they are not absolute. However, the consensus in
results in this thesis and the support of many other (not-selected) studies and literature reviews,
are more than enough reason to authorize further research and trials for additional local therapy
in men with mPCa.
5. Other Literature
Various systemic reviews were published recently to evaluate evidence on local treatments for
metastatic PCa: a short overview.
Arcangeli et al. (2016) reviewed 6 retrospective studies providing analysis of survival of
patients with locally advanced or metastatic PCa according to the treatment received. This
publication is limited by the heterogeneity and the shortage of published data, and presented
rather an overview of present knowledge than a systematic review. The conclusion of this
publication shows there is strong support for the benefit of local treatment in PCa, but this needs
to be validated by future studies. [19]
Aoun et al. (2014) provide an overview of the currently available literature about local control
of primary tumour and oligometastases in metastatic prostate cancer and salvage lymph node
dissection of clinical lymph node relapse after curative treatment of prostate cancer. The
conclusion of this comprehensive review is that local control of the primary tumour is still
experimental, but there is growing evidence of genetic and molecular research to support the
hypothesis. [14]
Bayne et al. performed a literature review in 2015 regarding the treatment of the primary tumour
in metastatic patients. Since they found no RCT comparing the combination of local therapy
and systemic therapy to systemic therapy alone, they analysed prospective studies of men with
locally advanced PCa and retrospective studies of occult node-positive PCa with additional
local treatment. The review concludes that treatment of the primary tumour in PCa is being
increasingly explored, with preclinical, translational and retrospective evidence to support
additional local treatment. There are some upcoming studies described to evaluate this new

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 39
approach and identify the metastatic patients most likely to benefit from additional local
treatment. [15]
Another literature review was performed by Ghadjar et al. in 2014. Screening population-based
data and retrospective series presented arguments to suggest that the use of local treatment of
the prostate in patients with primary metastatic prostate cancer may improve cancer-specific
survival and overall survival compared with treating these patients with androgen deprivation
therapy alone.
All these studies suggest several reasons why local treatment should be investigated further,
and many theories to prove why it could work. Most of them state some evidence as well for
survival benefits in patients treated with local therapy, but the results should be looked at
critically. Nearly all of these reviews are making conclusions out of the same group of studies:
retrospective case series or cohort studies selected out of population-wide databases (e.g. the
SEER database) are the most common source of input. Because of the limited amount of
existing data, few articles exclude studies based on quality assessments, to ensure a more
complete overview of the current evidence. This thesis only accepted two studies after quality
assessment, and still there are many limitations to consider. Despite the general consensus that
additional local therapy in mPCa patients is very likely to be beneficial, evidence is still very
poor. This thesis does not provide stronger evidence, but it gives a more critical look on existing
information and the current conclusions.

p. 40 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
6. Future studies
There are many theories that support adding local therapy in mPCa, and the evidence in
literature is growing steadily. It is no surprise that many upcoming studies are trying to prove
the benefits of additional radiotherapy, prostatectomy, or both, for mPCa patients. A short
overview is presented in Addendum Table 8.
7. Limitations of this thesis
As described in the methodology, only one database was used for literature research: the Ovid
database. The literature search was not repeated. Even though a large number of articles was
found, the use of a single source could have limited the amount and variety of studies.
Another limitation is the small number of selected studies: only two articles are included in
results of this literature research. Although 9 articles were found through the literature research,
only two of them met the threshold score of the quality assessment (Table 3). Of the 9 articles,
many are deficient in the same categories: recruitment in more than one centre, consecutive
recruitment of participants, clearly describing the intervention, reporting of co-interventions,
reporting of adverse events, reporting of both competing interests and source of support.
Some of these deficiencies can be explained by the retrospective design: not all relevant data
was registered at the time the patient was actually treated, causing lacking information. Three
of the studies used the SEER database, and are limited in description of the intervention,
reporting of adverse events, and reporting of all co-intervention. A detailed description of other
SEER limitations is mentioned earlier for Culp et al. The retrospective and observational design
explains the flaws in recruitment: patients are recruited from existing databases, instead of
consecutively.
The quality of the studies themselves is important as well. Although both studies used were
included after a quality assessment, they have some limitations that could influence their results.
These limitations are described above, and should be regarded carefully before making any
recommendations based on the outcomes of this thesis. Both of the studies used in this thesis
are retrospective: Heidenreich et al. published a cohort study, Culp et al. a case-control study.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 41
The level of evidence for these types of research, according to the Oxford Center for Evidence
Based Medicine, is IIb and IIIb, respectively.
To rate the quality of evidence of this thesis, the GRADE (Grading of Recommendations
Assessment, Development, and Evaluation) system was chosen and can be found in Table 6.
[31] The quality of evidence starts out as ‘low’, because of the observational study design. The
assessment is equal for OS and DSS, FFS is only described by Culp et al., and has a slightly
different score.
Table 6: GRADE analysis
GRADE Quality assesment
Quality
Importance
of outcome
no. of
studies Study design
Risk of
bias imprecision inconsistency indirectness
other
considerations
OS
2 observational
very
serious serious not serious serious none
●○○○
very low critical
DSS
2 observational
very
serious serious not serious serious none
●○○○
very low critical
FFS
1 observational
very
serious not serious not serious serious none
●○○○
very low critical
For all outcomes, there were sufficient reasons to lower the GRADE assessment to ‘very low’.
As described before, the risk of bias is very serious in both studies: it’s likely there is a bias in
selecting patients, and several limitations in data collection are reported. The down-rating for
imprecision is explained because of the low numbers in the intervention group and the lack of
confidence interval in the results of Heidenreich et al. This is less of a problem for FFS: this
outcome is only studied by Culp et al. Inconsistency gives little reason for concern: both of the
studies have similar results. The indirectness is serious: applicability of the results is difficult.
The sampled patients used by Heidenreich et al. are not representative for the population, and
Culp et al. do not describe details of the local therapies used in the intervention group. However,
combined with the hard outcomes and the direct comparisons between intervention and
controls, indirectness should only decrease by one level.
Together, all these flaws lower the level of evidence even more: from ‘low’ to ‘very low’. This
implies that the true effect of local therapy in mPCa is likely to be substantially different from
the results presented in this thesis.
Using the GRADE approach, a recommendation for the acquired evidence can be made for
local treatment in mPCa. Only Heidenreich et al. reported on feasibility of radical

p. 42 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
prostatectomy, Culp et al. registered no adverse events, so the desirable effects (or lack of it)
are most taken into account. All 3 outcomes (OSS, DSS, FFS) are significantly better in the
intervention groups with local treatment, compared to systemic therapy alone. However,
considering the many limitations in the studies, local therapy in men with newly diagnosed
mPCa can only be conditionally recommended. Other or better studied alternatives should be
considered as well.
The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 43
IX. Conclusion
Adding surgery or radiotherapy to systemic treatment in mPCa patients seems a promising
approach. There is a profit in both overall survival and disease specific survival for local
treatments added to systemic therapy, compared to systemic therapy alone.
Based on the selected articles, it was not possible to distinguish which local therapy is the most
beneficial, or to identify what patients could profit most. Furthermore, because of the lack of
comparative or randomised trials and the many limitations in the studies that were used, adding
local treatment cannot be recommended at this time as a new standard of care. This is confirmed
by a GRADE analysis and strength of recommendation.
There are many arguments in literature to endorse the research for additional local therapy in
mPCa. Several randomised prospective trials in the near future should provide more conclusive
evidence on the benefits of these treatments. These trials should pay careful attention to
specifications of the local therapies used and the identification of patients who could benefit
the most. It is to be expected that new recommendations will follow soon.

p. 44 The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer.
X. Bibliography
1. Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, et al. EAU
guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-
update 2013. Eur Urol. 2014;65(1):124-37.
2. Henau K, Damme NV, Calay F, Slabbaert M, Thibaut L, Francart J, et al. Cancer incidence in
Belgium 2010. Brussels: Belgian Cancer registry, 2013 D/2013/11.846/1
3. Brawley OW. Prostate cancer epidemiology in the United States. World Journal of
Urology.30(2):195-200.
4. Barocas DA, Mallin K, Graves AJ, Penson DF, Palis B, Winchester DP, et al. Effect of the
USPSTF Grade D Recommendation against Screening for Prostate Cancer on Incident Prostate Cancer
Diagnoses in the United States. The Journal of urology. 2015;194(6):1587-93.
5. Tangen CM, Hussain MH, Higano CS, Eisenberger MA, Small EJ, Wilding G, et al. Improved
overall survival trends of men with newly diagnosed M1 prostate cancer: a SWOG phase III trial
experience (S8494, S8894 and S9346). The Journal of urology. 2012;188(4):1164-9.
6. Schutter HD, Adam M, Giusti F, Schillemans V, Gendt CD, Jegou D, et al. Cancer Survival in
Belgium. Belgian Cancer Registry, 2012 D/2012/11.846/1.
7. James ND, Spears MR, Clarke NW, Dearnaley DP, De Bono JS, Gale J, et al. Survival with
Newly Diagnosed Metastatic Prostate Cancer in the "Docetaxel Era": Data from 917 Patients in the
Control Arm of the STAMPEDE Trial (MRC PR08, CRUK/06/019). Eur Urol. 2015;67(6):1028-38.
8. Cetin K, Beebe-Dimmer JL, Fryzek JP, Markus R, Carducci MA. Recent time trends in the
epidemiology of stage IV prostate cancer in the United States: analysis of data from the Surveillance,
Epidemiology, and End Results Program. Urology.75(6):1396-404.
9. Penson DF, Rossignol M, Sartor AO, Scardino PT, Abenhaim LL. Prostate cancer:
epidemiology and health-related quality of life. Urology.72(6 Suppl):S3-11.
10. Welch HG, Gorski DH, Albertsen PC. Trends in Metastatic Breast and Prostate Cancer —
Lessons in Cancer Dynamics. New England Journal of Medicine. 2015;373(18):1685-7.
11. Vale CL, Burdett S, Rydzewska LHM, Albiges L, Clarke NW, Fisher D, et al. Addition of
docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-
sensitive prostate cancer: a systematic review and meta-analyses of aggregate data. The Lancet
Oncology. 2016;17(2):243-56.
12. Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, et al. EAU
guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant
prostate cancer. European Urology.65(2):467-79.
13. Antwi S, Everson TM. Prognostic impact of definitive local therapy of the primary tumor in
men with metastatic prostate cancer at diagnosis: A population-based, propensity score analysis.
Cancer Epidemiology.38(4):435-41.
14. Aoun F, Peltier A, van Velthoven R. A comprehensive review of contemporary role of local
treatment of the primary tumor and/or the metastases in metastatic prostate cancer. BioMed Research
International.2014:501213.
15. Bayne CE, Williams SB, Cooperberg MR, Gleave ME, Graefen M, Montorsi F, et al.
Treatment of the Primary Tumor in Metastatic Prostate Cancer: Current Concepts and Future
Perspectives. Eur Urol. 2015.
16. Canby-Hagino ED, Swanson GP, Crawford ED, Basler JW, Hernandez J, Thompson IM.
Local and systemic therapy for patients with metastatic prostate cancer: should the primary tumor be
treated? Current Urology Reports.6(3):183-9.
17. Bott SR, Birtle AJ, Taylor CJ, Kirby RS. Prostate cancer management: 2. An update on locally
advanced and metastatic disease. Postgraduate Medical Journal.79(937):643-5.
18. Conde Moreno AJ, Ferrer Albiach C, Muelas Soria R, Gonzalez Vidal V, Garcia Gomez R,
Albert Antequera M. Oligometastases in prostate cancer: restaging stage IV cancers and new
radiotherapy options. Radiation Oncology.9:258.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 45
19. Arcangeli S, Zilli T, de Bari B, Alongi F. “Hit the primary”: A paradigm shift in the treatment
of metastatic prostate cancer? Critical Reviews in Oncology-Hematology. 2016(97):231-7.
20. Ghadjar P, Briganti A, De Visschere PJ, Futterer JJ, Giannarini G, Isbarn H, et al. The
oncologic role of local treatment in primary metastatic prostate cancer. World Journal of
Urology.33(6):755-61.
21. Moga C, Guo B, Schopflocher D, Harstall C. Development of a quality appraisal tool for case
series studies using a modified Delphi technique. Institute of Health Economics. Alberta Canada.
2012.
22. Culp SH, Schellhammer PF, Williams MB. Might men diagnosed with metastatic prostate
cancer benefit from definitive treatment of the primary tumor? A SEER-based study. European
Urology.65(6):1058-66.
23. Cho Y, Chang JS, Rha KH, Hong SJ, Choi YD, Ham WS, et al. Does Radiotherapy for the
Primary Tumor Benefit Prostate Cancer Patients with Distant Metastasis at Initial Diagnosis? PLoS
ONE [Electronic Resource]. 2016;11((1)):e0147191.
24. Fossati N, Trinh QD, Sammon J, Sood A, Larcher A, Sun M, et al. Identifying optimal
candidates for local treatment of the primary tumor among patients diagnosed with metastatic prostate
cancer: a SEER-based study. European Urology.67(1):3-6.
25. Gratzke C, Engel J, Stief CG. Role of radical prostatectomy in clinically non-organ-confined
prostate cancer. Current Urology Reports.15(11):455.
26. Heidenreich A, Pfister D, Porres D. Cytoreductive radical prostatectomy in patients with
prostate cancer and low volume skeletal metastases: results of a feasibility and case-control study.
Journal of Urology.193(3):832-8.
27. Qin XJ, Ma CG, Ye DW, Yao XD, Zhang SL, Dai B, et al. Tumor cytoreduction results in
better response to androgen ablation--a preliminary report of palliative transurethral resection of the
prostate in metastatic hormone sensitive prostate cancer. Urologic Oncology.30(2):145-9.
28. Satkunasivam R, Kim AE, Desai M, Nguyen MM, Quinn DI, Ballas L, et al. Radical
Prostatectomy or External Beam Radiation Therapy vs No Local Therapy for Survival Benefit in
Metastatic Prostate Cancer: A SEER-Medicare Analysis The Journal of urology.194(2):378-85.
29. Wu RY, Wang GM, Xu L, Zhang BH, Xu YQ, Zeng ZC, et al. The feasibility and safety of
high-intensity focused ultrasound combined with low-dose external beam radiotherapy as
supplemental therapy for advanced prostate cancer following hormonal therapy. Asian Journal of
Andrology.13(3):499-504.
30. Giordano SH, Kuo Y-F, Duan Z, Hortobagyi GN, Freeman J, Goodwin JS. Limits of
observational data in determining outcomes from cancer therapy. Cancer. 2008;112(11):2456-66.
31. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1.
Introduction—GRADE evidence profiles and summary of findings tables. Journal of Clinical
Epidemiology. 2011;64(4):383-94.

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. p. 46

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum p. i
XI. Addendum
1. Distribution of mPCa
Addendum Table 1: mPCa distribution pt. 1 [8]

p. ii The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum
Addendum Table 2: mPCa distribution pt. 2 [8]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum p. iii
2. Description of the 9 selected studies selected by literature search
Stud
yty
pe o
f stu
dy
Dat
a so
urce
(stu
dy
inte
rval
)
No.
Of
patie
nts
incl
usio
n cr
iteria
type
of l
ocal
ther
apy
adde
d to
stan
dard
of c
are
treat
men
t in
cont
rol
arm
Med
ian
follo
w-u
p
time
Out
com
e
Ant
wi e
t al.
retro
spec
tive
coho
rt
stud
ySE
ER d
ata(
2004
-201
0)78
58
≥35y
rs, d
ocum
ente
d st
age
IV (M
1a-c
), p
atho
logi
cal o
r rad
iolo
gica
l
conf
irmat
ion
of m
etas
tasi
s, P
ca is
the
first
and
onl
y pr
imar
y tu
mou
r.RP
or b
rach
ythe
rapy
stan
dard
of c
are
Not
repo
rted
OS,
DSS
Cho
et a
l.
retro
spec
tive
case
serie
sYo
nsei
Can
cer c
ente
r14
0
dist
ant m
etas
tasi
s (M
1) a
t ini
tial d
iagn
osis
or w
ithin
1 m
onth
from
initi
al d
iagn
osis
, with
out o
ther
prim
ary
mal
igna
ncie
s, n
o RP
bef
ore
befo
re R
TRT
stan
dard
of c
are
34,0
mon
ths
(1,7
-
108,
8mo)
OS,
FFS
, tox
icity
Culp
et a
l.
retro
spec
tive
coho
rt
stud
ySE
ER d
ata
(200
4-20
10)
8185
≥35y
rs, d
ocum
ente
d st
age
IV (M
1a-c
), ra
diog
raph
ic o
r pat
holo
gica
l
conf
irmat
ion
of m
etas
tatic
dis
ease
RP o
r bra
chyt
hera
pyno
sur
gery
or R
T16
mon
ths
OS,
DSS
, cau
se-
spec
ific
mor
talit
y
Foss
ati e
t al.
retro
spec
tive
case
serie
sSE
ER d
ata
(200
4-20
11)
8197
age
35-9
0 yr
, mPC
a (M
1a-c
), ex
clus
ion
of u
nkno
wn
PSA
or G
leas
on
scor
e, e
xclu
sion
of o
nly
EBRT
RP a
nd p
elvi
c ly
mph
nod
e
diss
ectio
n or
bra
chyt
hera
pyO
bser
vatio
n or
AD
T
36 m
onth
s in
LT,
31
mon
ths
for N
LTD
SS a
fter 3
yea
rs
Grat
zke
et a
l.
retro
spec
tive
case
serie
s
Mun
ich
Canc
er C
ente
r
(199
8-20
10)
1538
new
ly d
iagn
osed
M+
Pca
RP
stan
dard
of c
are
with
out R
PN
ot re
porte
dO
S
Hei
denr
eich
et a
l.
retro
spec
tive
case
-
cont
rol s
tudy
Dep
artm
ent o
f Uro
logy
,
Uni
vers
ity A
ache
n
23 +
38
(con
trols
)
6 cr
iteria
for c
ytor
educ
tive
RP;
biop
sy p
rove
n PC
a, m
inim
al o
sseo
us
met
asta
ses
(3 o
r few
er h
ot s
pots
on
bone
sca
n), N
0, P
SA d
ecre
ase
to
≤1.0
1.0
ng/
ml a
fter n
eoad
juva
nt a
ndro
gen
depr
ivat
ion
ther
apy
cyto
redu
ctiv
e RP
stan
dard
of c
are
with
out l
ocal
ther
apy
OS,
DSS
, FFS
Qin
et a
l.
retro
spec
tive
case
serie
s
Fuda
n U
nive
rsity
Sha
ngha
i
Canc
er C
entre
(200
6-20
07)
146
new
ly d
iagn
osed
M+
Pca
TURP
AD
T +
anti-
andr
ogen
15 m
onth
sO
S, D
SS, F
FS
Satk
unas
ivam
et a
l.
retro
spec
tive
coho
rt
stud
ySE
ER d
ata
(200
4-20
09)
4069
≥66
yrs,
mPC
a
RP, c
onfo
rmal
RT,
Inte
nsity
Mod
ulat
ed R
adia
tion
ther
apy
stan
dard
of c
are
with
out l
ocal
ther
apy
20 m
onth
sO
S, D
SS
Wu
et a
l.
pros
pect
ive,
cont
rolle
d an
d no
n-
rand
omize
d st
udy
Zhon
gsha
n H
ospi
tal o
f
Fuda
n U
nive
rsity
120
first
-tim
e pa
tient
s w
ith lo
cally
adv
ance
d (T
3-4,
N0-
1, M
0) o
r
met
asta
tic (M
+) P
ca
HIF
U, L
ow-d
ose
exte
rnal
beam
RT,
con
vent
iona
l-dos
e
exte
rnal
bea
m R
T
stan
dard
of c
are
with
out l
ocal
ther
apy
14,1
- 55
,1 m
onth
s O
S, D
SS, t
oxic
ity
Addendum Table 3: studies selected by full text assessment [13, 22-29]

p. iv The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum
3. Patient characteristics Heidenreich et al.
Addendum Table 4: patient characteristics by Heidenreich et al. [26]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum p. v
4. Patient characteristics Culp et al.
Addendum Table 5: patient characteristics by Culp et al. [22]

p. vi The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum
5. Subset analysis by Culp et al.
Addendum Table 6: Subset analysis by Culp et al. pt 1 [22]

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum p. vii
Addendum Table 7: Subset analysis by Culp et al. pt 2 [22]
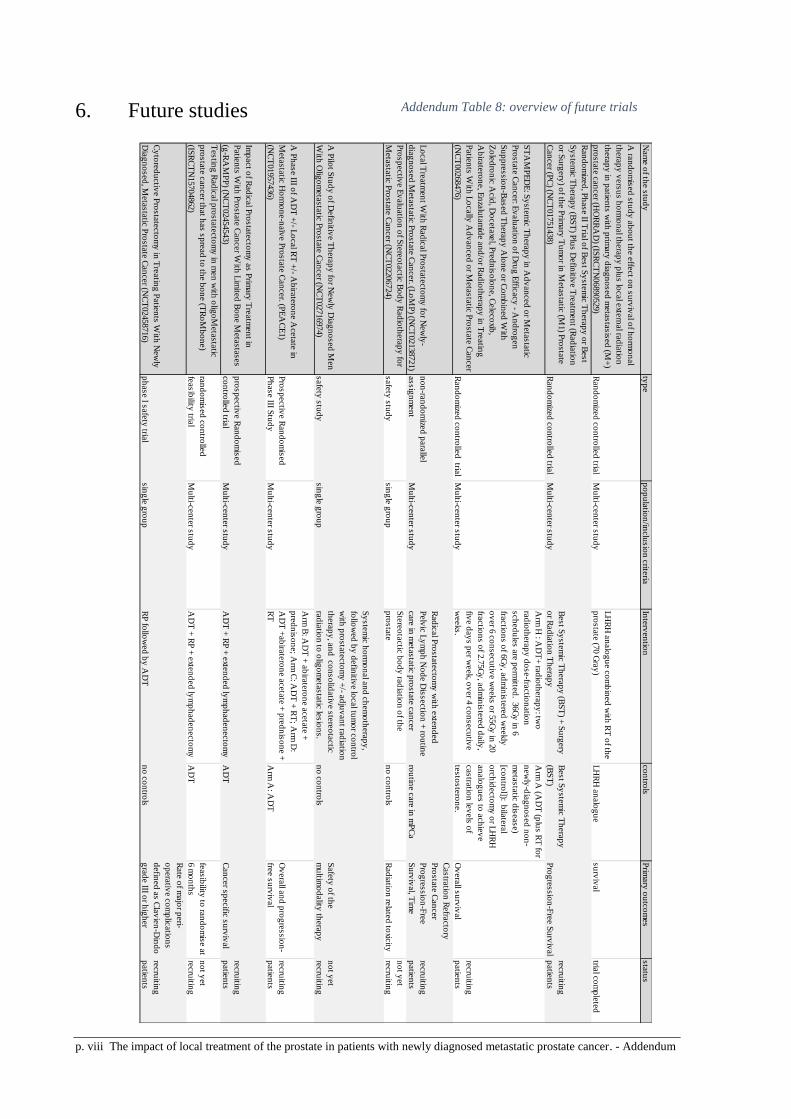
p. viii The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum
6. Future studies
Nam
e o
f the s
tud
y
typ
ep
op
ula
tion
/inclu
sio
n c
riteria
Inte
rven
tion
co
ntro
lsP
rimary
ou
tco
mes
sta
tus
A ra
nd
om
ised
stu
dy
ab
ou
t the e
ffect o
n s
urv
ival o
f ho
rmo
nal
thera
py
vers
us h
orm
on
al th
era
py
plu
s lo
cal e
xtern
al ra
dia
tion
thera
py
in p
atie
nts
with
prim
ary
dia
gn
osed
meta
sta
sis
ed
(M+
)
pro
sta
te c
an
cer (H
OR
RA
D) (IS
RC
TN
06890529)
Ran
do
mize
d c
on
trolle
d tria
lM
ulti-c
en
ter s
tud
y
LH
RH
an
alo
gu
e c
om
bin
ed
with
RT
of th
e
pro
sta
te (7
0 G
ray
)L
HR
H a
nalo
gu
esu
rviv
al
trial c
om
ple
ted
Ran
do
mize
d, P
hase II T
rial o
f Best S
yste
mic
Th
era
py
or B
est
Sy
ste
mic
Th
era
py
(BS
T) P
lus D
efin
itive T
reatm
en
t (Rad
iatio
n
or S
urg
ery
) of th
e P
rimary
Tu
mo
r in M
eta
sta
tic (M
1) P
rosta
te
Can
cer (P
C) (N
CT
01751438)
Ran
do
mize
d c
on
trolle
d tria
lM
ulti-c
en
ter s
tud
y
Best S
yste
mic
Th
era
py
(BS
T) +
Su
rgery
or R
ad
iatio
n T
hera
py
Best S
yste
mic
Th
era
py
(BS
T)
Pro
gre
ssio
n-F
ree S
urv
ival
recru
iting
patie
nts
ST
AM
PE
DE
: Sy
ste
mic
Th
era
py
in A
dv
an
ced
or M
eta
sta
tic
Pro
sta
te C
an
cer: E
valu
atio
n o
f Dru
g E
fficacy
- An
dro
gen
Su
pp
ressio
n-B
ased
Th
era
py
Alo
ne o
r Co
mb
ined
With
Zo
led
ron
ic A
cid
, Do
ceta
xel, P
red
nis
olo
ne, C
ele
co
xib,
Ab
irate
ron
e, E
nza
luta
mid
e a
nd
/or R
ad
ioth
era
py
in T
reatin
g
Patie
nts
With
Lo
cally
Ad
van
ced
or M
eta
sta
tic P
rosta
te C
an
cer
(NC
T00268476)
Ran
do
mize
d c
on
trolle
d tria
lM
ulti-c
en
ter s
tud
y
Arm
H : A
DT
+ ra
dio
thera
py
: two
rad
ioth
era
py
do
se-fra
ctio
natio
n
sch
ed
ule
s a
re p
erm
itted
. 36G
y in
6
fractio
ns o
f 6G
y, a
dm
inis
tere
d w
eekly
ov
er 6
co
nsecu
tive w
eeks o
r 55G
y in
20
fractio
ns o
f 2.7
5G
y, a
dm
inis
tere
d d
aily
,
five d
ay
s p
er w
eek, o
ver 4
co
nsecu
tive
weeks.
Arm
A (A
DT
(plu
s R
T fo
r
new
ly-d
iag
no
sed
no
n-
meta
sta
tic d
isease)
[co
ntro
l]): bila
tera
l
orc
hid
ecto
my
or L
HR
H
an
alo
gu
es to
ach
iev
e
castra
tion
lev
els
of
testo
ste
ron
e.
Ov
era
ll su
rviv
al
recru
iting
patie
nts
Lo
cal T
reatm
en
t With
Rad
ical P
rosta
tecto
my
for N
ew
ly-
dia
gn
osed
Meta
sta
tic P
rosta
te C
an
cer. (L
oM
P) (N
CT
02138721)
no
n-ra
nd
om
ized
para
llel
assig
nm
en
tM
ulti-c
en
ter s
tud
y
Rad
ical P
rosta
tecto
my
with
exte
nd
ed
Pelv
ic L
ym
ph
No
de D
issectio
n +
rou
tine
care
in m
eta
sta
tic p
rosta
te c
an
cer
rou
tine c
are
in m
PC
a
Castra
tion
Refra
cto
ry
Pro
sta
te C
an
cer
Pro
gre
ssio
n-F
ree
Su
rviv
al, T
ime
recru
iting
patie
nts
Pro
sp
ectiv
e E
valu
atio
n o
f Ste
reo
tactic
Bo
dy
Rad
ioth
era
py
for
Meta
sta
tic P
rosta
te C
an
cer (N
CT
02206724)
safe
ty s
tud
ysin
gle
gro
up
Ste
reo
tactic
bo
dy
rad
iatio
n o
f the
pro
sta
ten
o c
on
trols
Rad
iatio
n re
late
d to
xicity
no
t yet
recru
iting
A P
ilot S
tud
y o
f Defin
itive T
hera
py
for N
ew
ly D
iag
no
sed
Men
With
Olig
om
eta
sta
tic P
rosta
te C
an
cer (N
CT
02716974)
safe
ty s
tud
ysin
gle
gro
up
Sy
ste
mic
ho
rmo
nal a
nd
ch
em
oth
era
py
,
follo
wed
by
defin
itive lo
cal tu
mo
r co
ntro
l
with
pro
sta
tecto
my
+/- a
dju
van
t rad
iatio
n
thera
py
, an
d c
on
so
lidativ
e s
tere
ota
ctic
rad
iatio
n to
olig
om
eta
sta
tic le
sio
ns.
no
co
ntro
ls
Safe
ty o
f the
mu
ltimo
dality
thera
py
no
t yet
recru
iting
A P
hase III o
f AD
T +
/- Lo
cal R
T +
/- Ab
irate
ron
e A
ceta
te in
Meta
sta
tic H
orm
on
e-n
aïv
e P
rosta
te C
an
cer. (P
EA
CE
1)
(NC
T01957436)
Pro
sp
ectiv
e R
an
do
mis
ed
Ph
ase III S
tud
yM
ulti-c
en
ter s
tud
y
Arm
B: A
DT
+ a
bira
tero
ne a
ceta
te +
pre
dn
iso
ne; A
rm C
: AD
T +
RT
; Arm
D:
AD
T +
ab
irate
ron
e a
ceta
te +
pre
dn
iso
ne +
RT
A
rm A
: AD
T
Ov
era
ll an
d p
rog
ressio
n-
free s
urv
ival
recru
iting
patie
nts
Imp
act o
f Rad
ical P
rosta
tecto
my
as P
rimary
Tre
atm
en
t in
Patie
nts
With
Pro
sta
te C
an
cer W
ith L
imite
d B
on
e M
eta
sta
ses
(g-R
AM
PP
) (NC
T02454543)
pro
sp
ectiv
e R
an
do
mis
ed
co
ntro
lled
trial
Mu
lti-cen
ter s
tud
yA
DT
+ R
P +
exte
nd
ed
lym
ph
ad
en
ecto
my
AD
TC
an
cer s
pecific
su
rviv
al
recru
iting
patie
nts
Testin
g R
ad
ical p
rosta
tecto
my
in m
en
with
olig
oM
eta
sta
tic
pro
sta
te c
an
cer th
at h
as s
pre
ad
to th
e b
on
e (T
Ro
Mb
on
e)
(ISR
CT
N15704862)
ran
do
mis
ed
co
ntro
lled
feasib
ility tria
lM
ulti-c
en
ter s
tud
yA
DT
+ R
P +
exte
nd
ed
lym
ph
ad
en
ecto
my
AD
T
feasib
ility to
ran
do
mis
e a
t
6 m
on
ths
no
t yet
recru
iting
Cy
tore
du
ctiv
e P
rosta
tecto
my
in T
reatin
g P
atie
nts
With
New
ly
Dia
gn
osed
, Meta
sta
tic P
rosta
te C
an
cer (N
CT
02458716)
ph
ase I s
afe
ty tria
lsin
gle
gro
up
RP
follo
wed
by
AD
Tn
o c
on
trols
Rate
of m
ajo
r peri-
op
era
tive c
om
plic
atio
ns
defin
ed
as C
lav
ien
-Din
do
gra
de III o
r hig
her
recru
iting
patie
nts
Addendum Table 8: overview of future trials

The impact of local treatment of the prostate in patients with newly diagnosed metastatic prostate cancer. - Addendum p. ix


















