The Future of Dentistry
32
North Texas Dentistry a business and lifestyle magazine for north texas dentists special issue SPOTLIGHT The Future of Mission Dentistry Shaping Smiles Science vs. the Tooth Fairy
-
Upload
lulu-stavinoha -
Category
Documents
-
view
225 -
download
4
description
A Special Issue of North Texas Dentistry highlighting thought leaders in the practice of dentistry and cutting edge products and technologies
Transcript of The Future of Dentistry

North Texas
Dentistrya business and lifestyle magazine for north texas dentists
special issue
SPOTLIGHTThe Future of Mission Dentistry
Shaping Smiles
Science vs. the Tooth Fairy

STRAUMANN® CARES® DIGITAL SOLUTIONS SEAMLESS CONNECTIONS
Pave your way to success. Covering a full product range from temporary restorations to esthetic crown and bridge restorations, Straumann® CARES® Digital Solutions is now featuring:
new generation scanner new CAD software new applications leading range of materials
Straumann® CARES® Digital Solutions brings modern digital dentistry to dental professionals as a complete system – reliable, precise, and dedicated to your needs.
Please contact us at 800/448 8168. More information on www.straumann-cares-digital-solutions.comSome products and indications may be pending regulatory approval and may not be available in your local region.
INTRA-ORAL SCAN
GUIDED SURGERY
CADCAM
STRAUMANN
STRAUMANN® CARESSEAMLESS CONNECTIONS
CARES® DIGITSEAMLESS CONNECTIONS
SOLUTIONSAL GIT TAL SEAMLESS CONNECTIONS
SOLUTIONS
muratS
ccuo sy tar wuoe yvaPe regdir bdn anwo crcitehtse
ew genpw aen
nna ® ESRA C ® s bnoitulol Staigi Dbaielr
s. sec t rcudorl plug a fnirevoCnnamaurt S,snoiatrotse ® ESRA C
r enncan soitarene w Cens noitcailpp gnag rnidael
y trtsitnel dtaigin dredos mgnirs bo yd tteacided dn, aesicer, pelb
itarotsey rraropmm teore fgnat rES® taew fs nos inoitulol Staigi D
erawtfoD sAw Cslairetaf me og
mos a cs alanoisseforl ptaneo dy t.sdeer nuoo y
os tno:gnirut
m –tesyte selpm
baielr
o yd tteacided dn, aesicer, pelb
.sdeer nuoo y
Please contact us at
Please contact us at 800/448 8168. y bas mnoitacidnd ins atcudore pmoS
mation onMore infor .swwww.straumann-cares-digital-solutions.comnl aavorppy arotalugeg rnidnee py b
.straumann-cares-digital-solutions.comacor luon y yoe ilbaliave at boy nad mn
.straumann-cares-digital-solutions.com.noigel ra

S
e
r
What do you think the future of dentistry
will hold?
I believe this is a very exciting time to be a part
of the field of dentistry. New research and
technologies are changing the way dentists
relate to and treat their patients. With the use
of soothing spa treatments and procedures
that can be performed without injections,
maybe someday soon people will no longer
“dread” the trip to the dentist.
Dentistry has strived to address the busy lives
of patients. With new technology you can get
a crown in one appointment and even an
implant. Implant procedures continue to be
improved and are becoming the norm in many
dental treatment plans. Digital dentistry has
changed the process of taking impressions and
milling crowns.
New systemic research is leading the way to
many intriguing findings. The harvesting of
stem cells found in the pulp of teeth is being
explored as an effective treatment in some
diseases. Some people believe that in the not
too distant future, scientists will be capable of
growing a tooth in the laboratory from stem
cells. Genetic testing of saliva is also being
used to evaluate patients and improve their
treatment. Continued research endorses the
connection between a healthy mouth and a
healthy body. As those in the practice of
dentistry know, the mouth mirrors the health
of the rest of the body.
Another look at the future of dentistry is a bit
overwhelming, the underserved population.
Our look at Mission Dentistry is very heart-
warming and informative. Help is needed in
our own backyard as well as in the four
corners of the world. Funding cuts to dental
health programs have been staggering and are
not likely to improve in the near future. Take
a look and consider what contributions you
can make to brighten this population’s future.
The Future of Dentistry has been inspired by
doctors, businesses and products who are on
the cutting edge of many of these topics.
These leaders have incorporated the latest
research and technology to improve the
practice of dentistry. Through a series of
Q&A’s and Custom Profiles you will find more
insight into The Future of Dentistry.
I hope you enjoy this Special Issue of North
Texas Dentistry! It has been a pleasure
working with the team that has made this
issue go from an idea to a publication!
Take care and keep smiling!
LuLu Stavinoha, RDH
Publisher
(214) 629-7110
from the publisher
Publisher | LuLu Stavinoha
Photographer | Ray Bryant, Bryant Studios
Contributing Writers | Tina Cauller, Marc Fowler,
Sloan Hildebrand, DDS
Although every effort is made to ensure the
accuracy of editorial materials published in North
Texas Dentistry, the publisher cannot be held respon-
sible for opinions expressed or facts supplied by its
contributing authors. Copyright 2011. All rights
reserved. Reproduction in part or in whole without
written permission is prohibited.
Advertise in North Texas DentistryFor more information on advertising in North Texas
Dentistry, call LuLu Stavinoha at (214) 629-7110 or
email: [email protected]. Send press
releases and all other information related to this
publication to:
North Texas Dentistry
P.O. Box 12623
Dallas, Texas 75225
North Texas
Dentistry
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 3

NORTH TEXAS DENTISTRY | www.northtexasdentistry.com4
10
18
SEDATION RESOURCEKeeping Sedation Simple
DR. DENNIS M. ABBOTTDental Oncology Specialists of North Texas
STEVE BILTCEO, Smile Brands, Inc.
STEVEN LUGERBeaird Harris Wealth Management, Inc.
BLAKE EATONFounder, 3i Outsourcing Solutions, Inc.
22
26
31
17
12
20
24
PROFILES
DR. STEPHEN BASS & DR. ELLEN HALLDental Implant &Periodontal Partners
DR. DOUGLASDINGWERTH & DR. MAXWELL FINN Oral Surgery Associates of North Texas
DR. EDUARDO TANUR & DR. RUBEN OVADIAPeriodontal Associates
DR. J. HADLEY HALL Co-Developer, SockIt!
DR. HAROON ISMAILIPark Forest Oral & Maxillofacial
Surgery
The Future of Dentistry
25
31

6
13
16
27
SHAPING SMILES
Making dentistry digital
with CAD/CAM
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 3
special issue
18
28
27
16
13
FEATURES
North Texas
Dentistry
28
EMERGING TECHNOLOGIES in DENTISTRY ENHANCE PATIENT CARE
A look at new technologies and techniques to improve the practice of dentistry
THE FUTURE of MISSION DENTISTRYin UNDERSERVED COMMUNITIESExamining portable equipment options and volunteer opportunities at home and around the world
THE FUTURE of DENTAL MARKETINGA properly implemented online marketing campaign is the most effective way to reach potential new patients
THE ROLE of SALIVARY DIAGNOSTICSin TODAY’S PRACTICE
Salivary diagnostics presents a new scientific tools that affords dental practices the opportunity to provide lab-baseddata in educating patients and dental professionals
SCIENCE vs THE TOOTH FAIRYExciting new promise in baby teeth

At the start of the 20th century, around the time when Texas A&M
Health Science Center Baylor College of Dentistry in Dallas began as
State Dental College, most Americans expected to be toothless by age
45, and unfortunately they were.
Today people are living longer and are keeping their natural teeth,
thanks to advancements in dental equipment, materials and procedures
that are redefining oral health and dentistry. These advancements are
helping transform what was once the dreaded visit to the dentist into a
more comfortable, educational and stress-free experience.
As the new technologies replace or enhance traditional practices,
dental students expect to learn about these emerging trends and master
them. In turn, patients will benefit from more efficient and effective
delivery of oral health care.
Quick Crowns
In some offices, gone are the days of long waits to get dental crowns.
The traditional process of creating a crown means forming a mould of
the patient’s tooth and shipping it off to a lab that produces the crown
and sends it back to the dental office, a process that can take a few
weeks. With the newest technology, dentists can use a wand with a
laser sensor to get a 3D digital image of the patient’s teeth and mark
the spot for crown. The images can be manipulated to get the exact fit
for crown placement, and crowns can be manufactured within about 20
minutes. This eliminates the period of wearing temporary crowns, which
can be susceptible to fracture and can come off the teeth.
Implant Dentistry
In recent years, implant dentistry has advanced exponentially, making
it by far the fastest-growing segment in dentistry. Today’s implants are
far more predictable in the rate of success for placement and function-
ality. Dentists have discovered that implant technology works well in a
broader range of dental areas such as orthodontics and prosthetic care
for patients who have lost facial structure due to trauma or cancer. Lead-
ing a national effort by dental schools to prepare their graduates for the
increased demands in this area, HSC-Baylor College of Dentistry has
developed a comprehensive program for pre-doctoral students to gain
experience with dental implants.
More specifically, we are seeing a surge in mini implants, which are
relatively simple to place and cost less than traditional implants. These
implants are smaller in diameter than traditional implants and are de-
signed for patients with higher bone density. Unlike standard implants,
mini implants can be placed immediately. This means that in many
cases, the patient can walk out of the office on the day of surgery with
a lower denture which is not only stable, but can be used for chewing
immediately. Mini implants often can be placed in the lower jaw without
an incision in the gums.
Digital X-rays
Digital radiographs (x-rays) have grown in popularity in dental schools
as well as private dental offices and clinics. Although digital x-rays look
similar to film x-rays, there’s no film developing process and dentists
are able to optimize digital images to make better diagnoses. During
the last five years, the number of dentists using digital x-rays has
increased to the point that many patients are accustomed to seeing a
computer monitor next to the dental chair. The technology has become
so sophisticated that by using cone beam radiographs, dentists can get
a three-dimensional image of the patient’s mouth that outlines the
nerves and blood vessels and can even produce a surgical guide for
placing implants.
For patients who are unable to visit the dentist’s office, new portable
digital x-ray units allow dentists to more effectively treat patients in nurs-
ing homes, hospital rooms or other settings where patients may have
difficulty with mobility.
Healthy Mouth, Healthy Body
As dentists, we know the mouth is the window to the body and it
speaks volumes about the overall well being of patients.
EMERGING
TECHNOLOGIES
IN DENTISTRY
ENHANCE
PATIENT CARE
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com6

Researchers continue to look at the
association between cavities, periodontal
(gum) disease and heart disease.
According to the American Academy of
Periodontology, people with periodontal
disease are twice as likely to suffer from
coronary artery disease. The American
Heart Association also concludes that
poor oral health could increase your
chances of developing heart disease.
Other conditions that are related to poor
oral health and poor oral hygiene are
stroke, preterm and low birth weight
babies.
There also are some diseases that are
associated with an increased risk of in-
fections. Diabetes, for one, increases the
risks of gingival and periodontal inflam-
mation and infections. Or your dentist
may tell you that osteoporosis, a disease
that causes the bones to become less
dense over time as the body loses cal-
cium, could be at the root of tooth loss.
Access to Care
Although Americans in general are experiencing better oral health
care, some populations, including the poor, minorities, institutionalized,
elderly and other groups do not have adequate access to dental care.
As the largest provider of oral health care in North Texas, we are well
aware of the need for more access to care. Last year, the college re-
ceived more than 96,000 patient visits, and more than 170,000 people
were served through our community-based care, screening and educa-
tion programs. With more resources, we could have served tens of thou-
sands more.
One way we are addressing the access to care issue is through our
Bridge to Dentistry dental pipeline programs, which seek to introduce
the dental profession to young people from disadvantaged backgrounds
and/or underserved communities. Research has shown that many of
these students who choose to pursue dentistry as
a profession will incorporate service to the under-
served as practicing dentists.
Improved Preventative Therapies
Although not a new technique, fluoride varnish
has improved as a caries (cavity) prevention ther-
apy. It may be applied to the enamel, dentin or
surface layer of the tooth root to remineralize the
tooth, treat hypersensitivity and make teeth more
decay resistant. The new varnishes also have bet-
ter flavor, an added bonus for the patient. The use
of glass ionomers — a composite-type filling ma-
terial that continually releases fluoride — is
another method of strengthening patients’ teeth. Patients using fluoride-
based toothpaste continue to receive the benefits of this composite fill-
ing as use of fluoride toothpaste will recharge the ionomer.
However, with all the new advancements in dentistry, some things
never change — dental professionals still focus on prevention as key
to maintaining a healthy mouth. Our message of practicing good daily
oral hygiene with toothbrushing and flossing, eating a proper diet and
seeing your dentist on a regular basis, still rings true. n
Founded in 1905, Baylor College of Dentistry in Dallas is a college of
the Texas A&M Health Science Center. HSC-BCD is a nationally rec-
ognized center for oral health sciences education, research, specialized
patient care and continuing dental education. The HSC serves the state
as a distributed, statewide health science center that is present in com-
munities throughout Texas.
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 7

What do you think is the mostsurprising development on thehorizon in the dental field?
Dr. Abbott: Attention to overall wellness and the inclusion of oral
concerns in the concept of total health will increase in the next decade.
From a more prominent role in the care of cancer and transplant patients
to an emphasis on oral health for patients concerned with an overall
healthy lifestyle, aspects of dentistry will blend with medicine, nutrition,
and fitness in an increased focus on oral healthcare. I believe that within
the future of dentistry lies a place where the marked delineation between
dentistry and medicine is more blended into oral medicine; where the
focus is on the removal of harmful bacteria, be it from hard or soft tissue,
and the systemic benefits are realized by the patient. As advances in
bioengineering, gene therapy, and nano-technology are applied to the
realm of dentistry, tomorrow's dentist will practice in a world with new
materials, new drugs and new procedures.
Dr. Dennis M. Abbott CURRENT ROLEFounder and CEO, Dental Oncology Professionals of North Texas
www.dopnt.com
Private Practice
www.abbottdds.com
EDUCATION AND TRAININGBA, Biology - Rice University, Houston, TX, 1990
DDS - Baylor College of Dentistry, Dallas, TX, 1994
Postdoctoral studies in Oral Biology and Oral Medicine,
School of Dental Medicine, State University of New York
at Buffalo, Buffalo, NY, 1994-1997
PROFESSIONAL AFFILIATIONSMember, American Dental Association
Member, Texas Dental Association
Member, Dallas County Dental Society
Member, American Academy of Oral Medicine
Member (pending), Oral Cancer Foundation
Dental Oncology Professionals of North Texas(972) 226-6947
www.dopnt.com
Q:
&AQDr. Dennis M. AbbottDental Oncology Professionals of North Texas
Ph
oto
by: S
usa
n C
ole
ma
n, T
rue
Ble
ssin
gs P
ho
tog
rap
hy
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com8
What is the first thing that needs tohappen to improve dental care inAmerica?
Dr. Abbott: Unfortunately, dental care is often dictated by the patient's
ability or inability to pay for services. Too many times, a patient will delay
necessary treatment because insurance will not cover the expense or
the yearly maximum has already been met. Although I don’t have the
solution to the problem, until patients can pay for necessary treatments
and not be limited by insurance companies willingness to pay claims,
necessary treatments will go unrendered.
What new development in dentistryexcites you the most for it's potentialeffect on patient care and why?
Dr. Abbott: Dental oncology is one of the most exciting area of dentistry
that I see on the horizon. Dentists are in a unique position to care for
the variety of oral health needs of patients battling all kinds of cancer.
Modern treatments for cancer such as chemotherapy and radiation
therapy can be detrimental to the oral health of the patient, often
increasing the risk of pain and infection. Severe mucositis and
xerostomia can plague patients, reducing their quality of life and
compromising planned cancer treatments at a time when continued care
is essential. Dentists who enjoy complex treatment planning and caring
for medically compromised patients can be a valuable member of the
patient's oncology care team while dentists focused on prosthodontics
can restore oral maxillofacial defects that are often realized in patients
with head and neck cancers.
What do you think will be thebiggest change in dentistry in thenext 10 years?
Dr. Abbott: I hope the next ten years of dentistry see an increased
emphasis placed on the, as of yet, underserved population of patients
battling cancer. So much of medicine is focused not only on cancer
treatments but also cancer research and long-term care for cancer
survivors. We, as dentists, have so much that we can do to eliminate
pain, reduce the risk of infection and improve the quality of life for these
patients, that I hope the next ten years – and ten years beyond that –
see an increase in the number of dental professionals dedicated to
caring for the unique dental and oral health needs of individuals
battling cancer.
Why are you so passionate aboutdentistry?
Dr. Abbott: I truly believe that we, as dentists, help people.
Although a dental office is the last place most patients want to be,
I believe we are part of a noble profession that cares about the
well-being of our patients and does everything we can to improve their
lives. Knowing that what I do makes a difference in the lives of the people
I treat makes me still passionate about dentistry.
Do you have a personal motto thatyou live by?
Dr. Abbott: “Therefore, since we are surrounded by such a great cloud
of witnesses, let us throw off everything that hinders and the sin that so
easily entangles, and let us run with perseverance the race marked out
for us.” – Hebrews 12:1
What or who inspired you to pursuea career in dentistry?
Dr. Abbott: Three classes I took at Rice as an under-
graduate inspired me to pursue dentistry: microbiology, immunology, and
a course on cancer.
What aspect of modern clinical care, in your opinion, has made
the greatest difference in the lives of themost people?
Dr. Abbott: Hands down...local anesthetics!
In general, do you think patientstoday are better informed about
dentistry that in earlier times and why or why not?
Dr. Abbott: Yes... and no. There is no doubt that patients have more
access to more information that ever before. Unfortunately, the infor-
mation that they get as “Internet-trained dentists” is not always correct.
I sometimes find myself spending more time explaining “why not” than
“why”. But that, too, is part of my job.
What message about dental health doyou most wish to communicate toyour patients?
Dr. Abbott: Dental plaque and calculus are comprised of bacteria. It is
not OK to walk around with 20 years of deposits on the teeth, even if it
doesn't hurt. Inattention to dental health is a compromise to your
systemic health.
What is the key to being successful?
Dr. Abbott: Dream big. Work hard.
What motivates you each day?
Dr. Abbott: My patients depend on me. My staff supports
me. My sons inspire me. My wife loves me. This gets me
through the day.
Q:
Q:
Q:
Q:
Q:
Q:
Q:
Q:
Q:
Q:
Q:
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 9

Sedation Resource brings a fresh and innovative approach to the
sedation market. With headquarters in East Texas, Sedation Resource
provides superior service to its customers and seeks to foster an envi-
ronment of integrity and education by participating in sedation courses
across the nation. Collaborating with the ADSA, AAPD, AAOMS,
ADA and others, Sedation Resource has built relationships with some
of the top minds in the industry in order to stay current on advancements
within dentistry.
“Our goal is to focus on the importance of education over salesman-
ship, which isn’t always easy for a small, family owned company”
explains founder, Rose Dodson, “We believe if we remain honest and
ethical, helping our customers advance their knowledge of necessary
products, fiscal responsibilities will take care of themselves.”
State regulations vary for sedation dentistry. In the spirit of “education
over salesmanship,” Sedation Resource staff members are continually
updated on guidelines, and work hands-on with products and equipment
to ensure that every customer receives professional service, along with
the most effective and relevant products for their state requirements and
office needs. Depending on the size of the practice, or a particular situ-
ation, it may not be necessary for a dentist to buy a certain product. “I’m
not going to sell one product over another because it will produce a
larger profit for my company,” explains Rose.
“My staff is there to ensure that every customer
is cared for. Whether it is a large purchase or a
simple walk through the initial stages of sedation
set-up.”
In 2003, the inception of Sedation Resource
came from the frustration of doctors not know-
ing where to find products that were being
implemented into state regulations for certain
monitoring and emergency equipment. As an
independent sales representative for Welch Allyn
monitors and AEDs, part of Rose’s job was to
attend Continuing Education courses to generate
sales and leads. It became apparent that a single
source was needed to provide these items that
were not readily available. Starting as a few
products to simply help, Sedation Resource has
developed a company culture of helping by
assisting CE courses in various ways, and
providing flexible jobs in the local community.
One of the most successful products that
Sedation Resource distributes is the Sedation
Stethoscope. After explaining the culture of
Sedation Resource and their desire to help the
sedation community to Dr. Mort Rosenberg at a sedation course,
Dr. Rosenberg described the need for a precordial stethoscope that
could be operated wirelessly. Over the next couple of years, Rose, and
her husband, Fred, developed this item and in 2007 debuted their first
amplified precordial stethoscope with Bluetooth – the Sedation Stetho-
scope. This piece of equipment has become an essential monitoring
device in dental practices around the globe and an invaluable tool in
teaching institutions across the nation. “We’re excited to use Bluetooth
to allow the clinician freedom from the tether associated with the tradi-
tional precordial. It brings dentistry back to the foundational principles of
real time monitoring, while allowing the convenience to move around the
room,” explains Dr. Robert Bosack (www.dentalanesthesiaonline.com).
Sedation Resource is continually expanding its knowledge base and
acquiring more experience in order to assist dental professionals, stu-
dents and residents in any way possible. Whether it is a specific piece
of equipment or a crash course on the latest state regulations, Sedation
Resource strives to provide everything needed with genuine customer
service and integrity. It doesn’t take many words for Dr. Ken Reed, co-
course director with Dr. Stanley Malamed (www.learnivsedation.com), to
sum up Sedation Resource, “They simply have the supplies and equip-
ment that dentists doing sedation need. The prices are fair and service
is outstanding.”
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com10
Photo Courtesy of Solis Surgery Arts Center www.advancedanesthesia.org
Sedation Resource
Sedation ResourceIs Keeping Sedation Simple

How is Sedation Resourcecontributing to the future of dentistry?
As the demand for technology increases, Sedation Resource is
constantly updating its product line in an effort to stay current with the
market trends and offerings. The development of a Bluetooth® wireless
precordial stethoscope is one of the ways Sedation Resource is
encouraging progress in the sedation dentistry market. Regardless of
technology, the doctor is still the most important monitor in the room and
the type of equipment chosen should extend his or her senses. The
Sedation Stethoscope by Sedation Resource allows the doctor to move
about freely and still have early warning of potential airway difficulties.
What is the Sedation Stethoscope?
The Sedation Stethoscope is an amplified Bluetooth® wireless stetho-
scope used to monitor ventilation. The Piezo version of the Sedation
Stethoscope has the microphone built into the chest piece, which
reduces ambient noise and produces diagnostic quality sound. With the
Sedation Stethoscope Classic, the microphone is built into the line, which
allows the ability to interchange various sizes of Wenger chest pieces
or use an esophageal probe. With either type of the Sedation Stetho-
scope, you can obtain the mobility you want with the continuous
monitoring you need.
How is the Sedation Stethoscopedifferent than a traditionalprecordial/pretracheal stethoscope?
The Sedation Stethoscope provides amplified auscultation with the
mobility of a wireless headset or speaker. Bluetooth® technology
removes the tether previously associated with a traditional precordial
stethoscope. The range of sound is approximately 30 feet which allows
the clinician to move about the procedure room while continuously
monitoring the patient. Foundational monitoring of ventilation is listening
to breath sounds. Bluetooth® technology and the amplification of the
Sedation Stethoscope is allowing doctors to return to the standard
principal of listening to the airway for those subtle clues that tell when a
patient is about to obstruct, enabling early intervention and prevention
of respiratory distress.
How is the Sedation Stethoscopeadvancing hands on education?
When listening to your patients breathing, it is not necessary to watch a
waveform or wait for an alarm to realize your patient is having respiratory
difficulty. Because of this, the Sedation Stethoscope has become an
invaluable tool in many teaching institutions across the country. The
instructor can monitor respiration alongside the student, helping to ensure
the patient’s airway patency and increasing instructional opportunities.
What else does Sedation Resourceprovide for dentists?
Sedation Resource carries an extensive line of sedation equipment and
supplies, as well as everything needed for an emergency in the dental
office. From syringes to vital signs monitors, AEDs to emergency drugs –
Sedation Resource has the products you need to keep sedation simple,
safe, and effective.
What is your Customer Service Policy?
Our company policy is simple – we will do our job, get your order out in
a timely manner and provide excellent customer service. If you have
questions, we will answer them or point you in the right direction to find
a solution. Please feel free to give us a call for more information at
(800) 753-6376 or visit us at www.sedationresource.com.
Q:
Q:
Q:
Q:
Q:
Q:
Sedation StethoscopeModern Technology for Sedation Dentistry
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 11

What new develop-ment in Periodonticsexcites you the most
for its potential effect onpatient care and why?
Dr. Bass: Though lasers in dentistry have
been available for many years, a relatively new
FDA approved technology for treatment of peri-
odontal disease is showing impressive results.
We recently incorporated the Millennium Dental
Technologies PerioLase® MVP-7 laser to per-
form the patented Laser Assisted New
Attachment Procedure (LANAP™). This tech-
nique utilizes a specific laser wavelength and
proprietary laser settings to provide the neces-
sary energy to treat the periodontal disease
without compromising healthy tissues. After
approximately one year follow-up, patients
treated in our office have demonstrated results
that are comparable to traditional osseous sur-
gery, including bone grafting. One of the chief
advantages of this technique is that no incision
and no suturing are required. This is much
more appealing to patients who need periodon-
tal treatment. It also is more cost effective
because bone graft material is not required.
It is important to note that the technique tends
to provide better results if the patient has not
undergone soft tissue management prior to
treatment, because the laser energy is more
effective in inflamed tissue, rather than in
patients previously treated with non-surgical
techniques.
Many of my patientshave gingival reces-
sion and dentin hypersensiti-vity. Can the periodontistaddress this problem?
Dr. Hall: Gingival grafting can cover exposed
root surfaces and increase the zone of kera-
tinized gingiva. Covering these root surfaces
can eliminate dentin hypersensitivity and
improve the overall health and appearance
of the tissues. In addition, old composite
restorations can be removed and grafted over
to improve the esthetics and in some cases
cover the exposed crown margins.
What enhancementsare coming in dental implant technologies?
Dr. Bass: The next development in dental
implant technology that will become routine in
our offices will be the use of CT imaging and
planning the implant placement on the com-
puter. This will allow placement in a position
that will require the least bone manipulation
and also will allow for fabrication of custom
abutments that will enhance the soft tissue
management of the implant restoration.
Though these technologies have existed, the
costs associated with fabrication of the com-
puter guided surgical guides as well as the
custom abutments are now more in line with
that of a stock abutment.
What can a restorative dentist do to maximize the
cosmetic result and achievePerio-Restorative harmony?
Dr. Hall: It is important for clinicians to con-
sider the perio/restorative connection in their
smile design. The amount of gingival display
and gingival symmetry should be considered
in order to optimize anterior esthetics. The
perio-restorative team needs to have an
understanding of the epithelial attachment,
biological width and supra-crestal fibers and
how to manage them to provide patients with
beautiful restorations. Crown lengthening or
gingivectomy surgical procedures should be in
the treatment plan to improve the restorative
outcome and create balance and perio-
restorative harmony.
Q:
Q:
Q:
Dr. Stephen Bass & Dr. Ellen HallDental Implant & Periodontal Partners, LLP
Dr. Stephen Bass CREDENTIALSDiplomate of the American Board of Periodontology
Fellow of the Institute for Advanced Laser Dentistry
EDUCATIONBS, Biology - Southwestern University, Georgetown, 1985
DDS - UTHSC, San Antonio, 1990
MS / Periodontal Certificate - UTHSC, San Antonio, 1993
PROFESSIONAL AFFILIATIONSDallas County Dental Society
Texas Dental Association
American Dental Association
Texas Society of Periodontists, President, 2003
Southwest Society of Periodontists, President, 2011-2012
American Academy of Periodontists
Dr. Ellen HallCREDENTIALSDiplomate of the American Board of Periodontology
EDUCATIONBS, Zoology - Texas A&M University, College Station, 1991
DDS - UTHSC, San Antonio, 1995
MS / Periodontal Certificate - UTHSC, San Antonio, 1998
PROFESSIONAL AFFILIATIONSDallas County Dental Society
Texas Dental Association
American Dental Association
Texas Society of Periodontists
Southwest Society of Periodontists
American Academy of Periodontists
Dental Implant & Periodontal Partners, LLP
(972) 612-2040
www.implantperioteam.com
Q:
&AQ
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com12

When asked to brainstorm the future of volunteer dentistry,
I sought out several individuals that I believe are at the
forefront of breaking the trail in this growing movement,
I was blown away at the paralleling desire and commitment of individu-
als and organizations around the world that continue to reach out to un-
derserved communities locally and abroad. Being that there are
underserved pockets right here in the Dallas area as well as around the
globe, I found that the needs of these organizations and sectors of pop-
ulation are vastly different dependent on their geographical location
alone. The common thread is the need for dental help alongside the
yearning for knowledge and advancement in equipment in order to
serve within these different locations. There is an ancient Chinese
proverb that says “Give a man a fish and feed him for a day, teach a
man to fish and feed him for a lifetime”.
Both aspects of the Chinese proverb are valid. The first addresses
relief efforts and the second addresses community development. Often
times the two overlap in that when disaster strikes, it seems that the un-
developed and underdeveloped communities suffer the greatest losses.
Many organizations that I have worked alongside globally are passion-
ately involved in both the relief and development efforts. Efforts most
impactful are interwoven with the message of hope and education for
these people that are seemingly less fortunate. Whether these individ-
uals are truly less fortunate remains a mystery to me in many facets of
our lives.
I believe the most important skill that can be taught to individuals
when serving overseas or within our underserved communities locally
is simply education in the areas of oral hygiene and preventative dental
health. The future of missions and care for others can be exponential
in terms of impact when children are taught the value of oral healthcare
and this lesson can be passed down from generation to generation.
Follow up care is also imperative to ensure that this message is cor-
rectly passed on within families and that care to subsequent generations
is allocated appropriately.
According to UNICEF, two out of three people globally live on less
than $2 per day and have inadequate access to clean water. Ongoing
wars, corruption, natural disasters, climate change, and increased costs
for both food and energy ensure that these miserable statistics will not
improve any time soon. The need for help in the developing world is lit-
erally limitless. For most of these people the possibility of dental care is
nonexistent due to financial constraints or geographic isolation. Thus,
the future for missionary dentistry is unlimited.
With the continual advancement of technology as well as the drive
for more comprehensive treatment within these developing communities
several key products have become available to better serve in remote
locations and more comprehensively treat those in need. Villages de-
void of electricity still require the basic elements and instruments to per-
form exodontias of hopeless or infected teeth, basic oral hygiene care
THE FUTURE OF
Mission DentistryIN UNDERSERVED COMMUNITIES
by Sloan Hildebrand, DDS
Dr. Sloan Hildebrand attending a traditional Maasai wedding ceremony alongside the Mara River, Kenya.
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 13
and fluoride treatment. Areas where a clinic
has previously been established or there is
some semblance of rudimentary clinical sup-
plies are more equipped to serve patients with
restorative, cosmetic, surgical or a basic den-
tal prophylaxis.
These remote areas of the earth require
portable dental equipment, which is available
from over twenty manufacturers and distribu-
tors. There are many parameters to consider
before purchasing portable dental equipment
for a mission such as; the source of electric,
your parameters of service, the country where
the equipment will be used, and availability of
a compressor for air pressure in some in-
stances. Even the altitude where the team
sets up to work can be a concern for your
equipment’s performance.
When it comes to portable dental units and
handpieces, one company truly stands out.
Bell Dental Products, www.belldental.com is
an innovative company developing dental
products utilizing proprietary state-of-the-art
core technologies. The company designs, de-
velops, and manufactures precision dental
equipment based on electric motor technol-
ogy. It was founded on a heritage of product
development and program management in the
aerospace, medical, and dental industries.
These products listed below are used exclu-
sively by the U.S. Army, U.S Navy and U.S
Marine Corps in the most remote corners of
the earth.
The PortaBELL™ Portable Dental Oper-
atory includes fiber optic electric motor and
hand pieces, high speed and slow speed hand
pieces, HVE, saliva ejector, air/water syringe,
over patient delivery for convenience,
reduced fatigue and standard hospital grade
duplex outlet. The PortaBELL™ is a totally
self-contained portable dental operatory that
has been designed and manufactured specif-
ically for the demanding environment of the
field dentist. The downside of such a unit is
that the unit alone weighs 60 lbs. (27.2kg) and
the unit including the shipping container
weighs 130 lbs. (46.8kg). The cost is approxi-
mately $20,000 and therefore a hindrance to
some smaller dental mission organizations.
This unit is fully operational at 10,000 ft.
(3,000m), with a torque speed of 40,000 rpm
and fiber optic illumination of 70,000 LUX.
A smaller, more affordable unit that is
portable and completely self-contained, the
TravelBELL™ is a light, six-pound, versatile
field dental system with capabilities you’d ex-
pect from your office. The TravelBELL™ goes
anywhere, anytime in a rugged, compact brief-
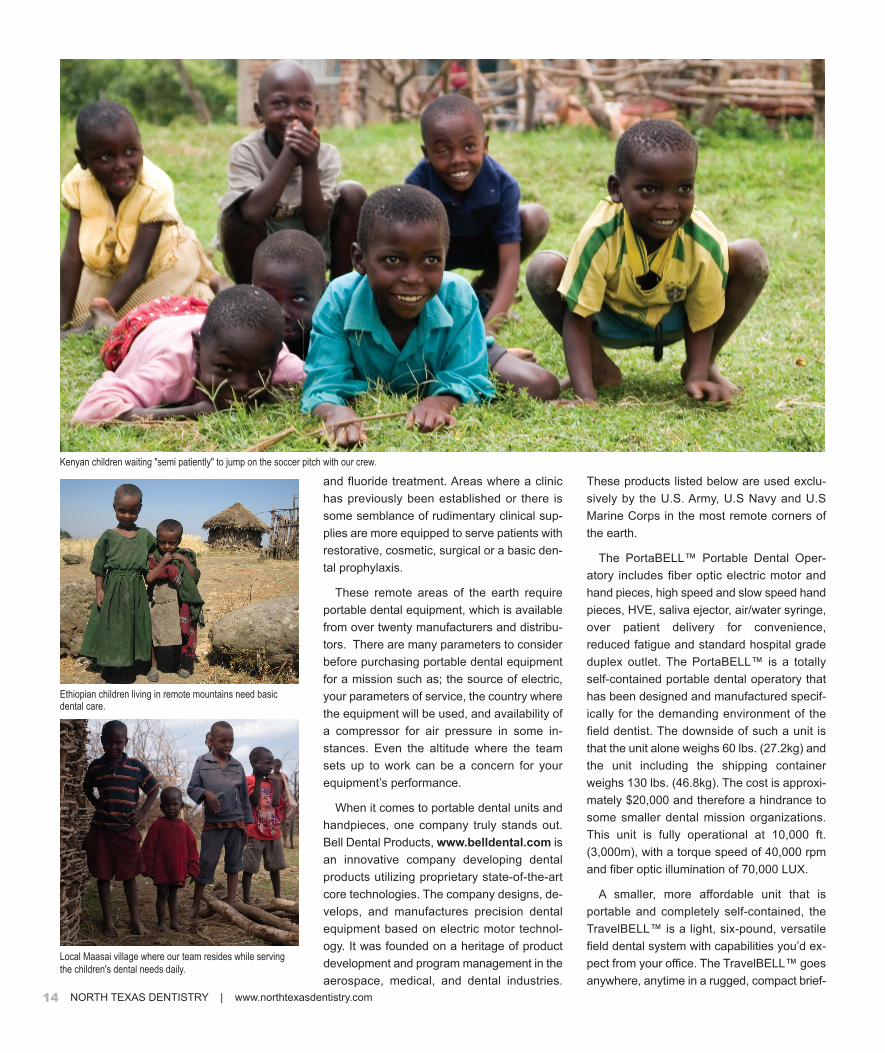
Ethiopian children living in remote mountains need basicdental care.
Local Maasai village where our team resides while serving
the children's dental needs daily.
Kenyan children waiting "semi patiently" to jump on the soccer pitch with our crew.
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com14

case. With the optional solar panels, you will
never need to be leashed to a wall plug.
A fully charged battery will last approximately
eight hours with a recharge life of 1,000 times.
The TravelBELL™ is an ultra-lightweight, full
featured battery powered field dental system
that is engineered for high-performance den-
tistry anywhere you can go. The E-type motor
will accept any standard E-type nose cone
providing a broad range of capability and flex-
ibility, from 200 to 150,000 rpm. The purchase
price is $3,295 and it has been used all over
the world in remote places from the jungles
of the Amazon basin to the high peaks of the
Himalayas.
With the availability of portable dental radi-
ography, including the new “Nomad” x-ray unit
from Aribex, volunteers now have the oppor-
tunity to bring more precise and diagnostic
dental services to isolated areas. The com-
pact design of these units and low weight, 5.5
pounds, allows a team to check them as reg-
ular luggage for international travel. Most com-
plete radiograph units retail for approximately
$7,495. These products present marvelous
opportunities for service organizations to fund
raise for a specific purpose and see the ben-
efits of their donations.
For those interested in donating
their dental skills, many organiza-
tions are available to partner along-
side providing a wide variety of
experiences. Given that caries is still
the most pervasive dental problem,
volunteers can provide care in multi-
ple venues, ranging from restorative
treatment in traditional clinics, to
extractions in isolated villages.
Organizations such as World Dental
Relief (www.worlddentalrelief.com)
provide critically needed supplies
and instruments donated by major
dental retailers, manufacturers, and
wholesalers to their mission ware-
houses. World Dental Relief sup-
plies over 400 teams a year with the
necessary equipment to more than
80 countries globally. Individuals
can both rent equipment from this
organization as well as go to their
website to learn of upcoming volun-
teer opportunities in their community
and worldwide.
You do not have to be a trained dental
professional to make a lasting impact on the
lives of others. No matter what facet you
choose to serve in, I can assure you that the
need is always great, your services will always
be appreciated and most certainly your life will
be changed eternally. You can also check
out www.dentalmissiontrips.com or visit
www.drsloanhildebrand.com to keep abreast
of opportunities to serve locally or globally for
any length of time and in virtually any capacity.
Dr. Sloan Hildebrand is honored to serve his
dental family with the utmost excellence. His
team provides complete dental health care,
specializing in prosthodontics, full mouth recon-
structions, implant supported prostheses and
elderly care. Dr. Hildebrand has been blessed
to travel literally around the world to share his
God-given talents to those less fortunate in
dental care, education or simply being geo-
graphically isolated. Whether he is serving in
the high Himalayas of Nepal, the jungles of
Cambodia, the plains of Africa, the under-
served communities of Dallas or a remote
island in the south Pacific, he feels the need is
global and the need is now. n
Maasai women wait to be seen at the clinic in
the African plains with Dr. Hildebrand.
Dr. Hildebrand and his team set up a makeshift dental clinic
under the "big tree" out in the Maasai Mara plains, Kenya
with anesthesia, sterilization, forceps, medicine, shade and
a chair. Villagers will walk for miles to be treated.
Watch www.drsloanhildebrand.com to
see where Dr. Hildebrand is serving next as
well as to become informed as to where you
can help serve others in a variety of capacities
locally or globally this year!
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 15

When you position yourself well on the
major search engines like Google, Yahoo and
Bing, they can deliver highly targeted con-
sumers directly to your website.
While most dentists understand the impor-
tance of having a presence on the internet,
many still believe they simply need to have a
website. With online marketing, the “build it
and they will come” approach does not work.
You can have the most beautiful website in
town, but if consumers can’t find it, it’s nothing
more than an expensive brochure. Most con-
sumers (according to one popular study –
89%) never go past the first page of the
search engine results. That means if you
aren’t on the first page of Google, Yahoo, Bing
– then to those consumers, you don’t exist.
Keep in mind, this is only the term “dentist”
and doesn’t include all the possible variations
such as “cosmetic dentist”, “dental office”,
“dental implants”, etc.
Let’s assume you are a dentist in Flower
Mound. How many postcards would you have
to mail to put your marketing message in front
of 3,600 people who are currently looking for
a new dentist?
It is the dentists on the first page of
Google who are getting those searchers as
new patients.
Most consumers assume (often incorrectly)
that the dentists on the first page of Google
are the “best” dentists in town. We often hear
from dentists that a competitor with inferior
clinical skills to theirs has a much larger, more
successful practice than them. Upon investi-
gation we always find that dentist with the
inferior clinical skills has superior marketing.
The bottom line is – the best marketer
always wins.
The foundation of a successful online mar-
keting strategy is a properly optimized practice
website that ranks high in search engines,
presents a positive first impression and gives
a compelling reason why visitors should select
you as their new dentist.
Once your main website is ranking well and
converting visitors into new patients, you can
add additional strategies such as microsites,
Google Places optimization, patient reviews
and reputation management, online videos
and social media.
In future articles in North Texas Dentistry,
we’ll take a deep dive into each of these
strategies so you’ll have a better understand-
ing of what it will take to become the dominant
dentist in your market. n
Marc Fowler is President of Bullseye Media,
LLC, a McKinney, TX based digital marketing
agency that specializes in helping dentists
leverage the internet to grow their practices.
He can be reached at 214-592-9393 or by vis-
iting www.OnlineDentalMarketing.com.
Remember the days when you could place an ad in the yellow pages and sit
back and wait for the phone to start ringing? That doesn’t happen today.
For most consumers, the internet (particularly Google) has replaced the yellow
pages when searching for local products & services. There are several reasons
for this:
n Most people have instant access to the internet (PC, smart phones, iPad, etc.)
n Too many versions of the yellow pages, most are thrown out immediately
n Doing a Google search is much faster than looking for a phone book
A properly implemented online marketing campaign is the most effective way
to reach potential new patients at the exact moment they are actively searching
for the services you offer.
According to Google, the average
number of monthly searches conducted
over a 12-month period for some select
keyword phrases are:
The
Futureof Dental Marketing by Marc Fowler
Dentist Dallas..........14,800
Dentist Flower Mound.....3,600
Dentist McKinney.........4,400
Dentist Rockwall.........1,300
Dentist DFW..............8,100
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com16

What new develop-ment do you findexciting for its
potential to impact patienthealth ?
Dr. Finn: We hear a lot about stem cells and
their amazing potential for use in medical ther-
apies because they can be directed to
differentiate into almost any type of human
cells. Recently, researchers at NIH discovered
stem cells in extracted teeth with healthy
dental pulp. In one study, dental pulp stem
cells were differentiated into functional pancre-
atic cells that may be useful in treating Type I
diabetes. Now, with a new, affordable process
called StemSave™, the oral surgeon can pre-
serve valuable stem cells from a child, teen,
or adult when there is a wisdom tooth,
baby tooth, orthodontic or other tooth extrac-
tion planned.
Are there any newoptions foredentulous patients?
Dr. Finn: With All-on-4™, we can create a
restoration using just four implants to support
an immediately loaded full-arch provisional
prosthesis. All-on-4™ offers improved stability
because it uses tilted implants that increase
bone-to-implant contact and reduces the need
for vertical bone augmentation. This technique
can be performed using digital methods to
ensure accurate diagnostics and treatment
planning, and an individualized surgical
template that guides exact implant placement.
Are there newoptions for patientswho want dental
implants but haveinadequate bone?
Dr. Dingwerth: Yes. Bone Morphogenetic
Protein (BMP) is an isolated protein that is
found naturally in the human body and helps
stimulate new bone development. The bone
morphogenetic protein clinical trials were done
over 10 years ago by multiple oral and maxillo-
facial surgery institutes. This protein has been
approved by the FDA, and BMP is now used
mainly by orthopedic and oral surgeons to
regenerate and augment bone volume. BMP
can eliminate the need for bone harvesting
from a donor site so the recipient can avoid the
discomfort and possible complications associ-
ated with the graft harvest site. This bone
growth and regeneration, therefore, can assist
with placing implants in people who may lack
appropriate bone volume.
How has newtechnology changedorthodontictreatment options?
Dr. Dingwerth: A new option that has been
around for a few years is the Bollard mini plate.
The Bollard mini plate is used for skeletal
anchorage to help modify the growth pattern of
the patient’s jaws. The plates help coordinate
the development of these jaws during a
patient’s growth phase. Bollard plates do not
apply forces on the teeth during this growth
modification process, which can eliminate the
undesirable movement that can occur with the
teeth. These anchors can take the place of
many auxiliary orthodontic appliances. These
plates can help to improve patient compliance
due to their more aesthetic presentation since
they are located intraorally. These plates, in
conjunction with orthodontic treatment, can
limit or eliminate the need for potential
orthognathic surgery for patients who have
skeletal growth abnormalities.
Q:
Q:
Q:
Dr. Douglas Dingwerth & Dr. Maxwell FinnOral Surgery Associates of North Texas
Douglas J. Dingwerth, DMD MDCREDENTIALS
Diplomate, American Board of Oral & Maxillofacial Surgery
EDUCATIONDMD - Southern Illinois University (1995)
MD -Texas Tech University (1998)
Internship in General Surgery/Oral & Maxillofacial Surgery
Residency - Baylor University Medical Center, Dallas, TX
PROFESSIONAL AFFILIATIONSAmerican Association of Oral and Maxillofacial Surgeons,
Southwest Society of Oral and Maxillofacial Surgeons, Texas
Society of OMS, North Texas Society of OMS
Maxwell D. Finn, DDS MDCREDENTIALSDiplomate, American Board of Oral and Maxillofacial Surgery
EDUCATIONDDS - Baylor College of Dentistry (1991)
MD -Texas Tech University (1995)
Internship in Oral & Maxillofacial Surgery/General Surgery
Residency, Oral & Maxillofacial Surgery - Baylor University
Medical Center Dallas, Dallas, TX
PROFESSIONAL AFFILIATIONSAmerican Association of Oral and Maxillofacial Surgeons,
Southwest Society of Oral and Maxillofacial Surgeons, Texas
Society of OMS, North Texas Society of OMS, American
College of Dentists
Oral Surgery Associates of North Texas
(214) 363-6040
www.northtexasoral surgery.com
Q:
&AQ
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 17
Ph
oto
by R
ay B
rya
nt, B
rya
nt S
tud
ios
Ph
oto
by R
ay B
rya
nt, B
rya
nt S
tud
ios

Back in the days before CAD/CAM
technology, most all manmade prod-
ucts began with ink and paper. The initial
concept flowed through the hand of a skilled
draftsman who painstakingly rendered succes-
sive iterations until ultimately arriving at a final
design, which was given in blueprint form to the man-
ufacturer. In the 1960s and 70s, demand by the military as
well as the aircraft and auto industries for a more efficient way
to model industrial products busied brilliant minds at MIT and other
thinktanks.
Early versions of computer aided design software relied on massive
mainframe computers that filled entire floors, required their own A/C
systems, and munched miles of information punched into paper tape.
Over three decades, the growth of CAD/CAM technology closely paral-
leled the development of the digital computer as computers evolved
from clunky multi-million dollar monstrosities into affordable desktop
necessities. Each step forward made CAD/CAM solutions smaller,
cheaper, faster and vastly more powerful, and pushed industry through
the looking glass into a world that was once unfathomable. The impact
has rippled outward to every corner of product design.
The computer scientists who breathed life into those early applications
probably didn’t have time to imagine that their work would revolutionize
manufacturing so completely that it would affect everything from aero-
space to zippers, including the way dentists restore a patient’s smile.
CAD/CAM Restorations
Even a minute discrepancy in fit between the tooth preparation and
the crown can result in an increased chance of infection and shifting,
so precision is critical.
To address the need
for optimum precision,
CAD/CAM technology
was first introduced in
restorative dentistry by Fran-
cois Duret in 1971. Since the first
CAD/CAM restoration was created
in the 1980s, dentists and laboratory
technicians have found that it helps them reli-
ably and efficiently fabricate all-ceramic crowns and
bridges with great precision.
CAD/CAM has also dramatically impacted the patient experience.
After the area is prepared, the dentist electronically captures an image
of the preparation. Alternatively, images can be obtained by scanning a
traditional model created from conventional impressions of the prepa-
ration. Newer systems are clinically and economically superior to
first-generation systems, so more dentists are now choosing to com-
pletely replace traditional impressions with optical impressions taken
with a digital scanner or camera. This can be a valuable marketing
device since it is especially attractive to patients who prefer to avoid the
sensory unpleasantness of the traditional impression process.
After the exact size and shape of the restoration required to fill the
defect is precisely specified using an on-screen cursor to draw the
design for the restoration on a three-dimensional image, the dentist
relays the digital information to a CAM milling apparatus, located either
in the office or in an off-site laboratory.
In about 20 minutes, the milling machine fabricates a ceramic restora-
tion, which conforms to the defect within 50 microns, from a solid block
of ceramic material that matches the surrounding teeth. When the
SHAPING
SMILESMaking Dentistry
Digital with
CAD/CAM
By Tina Cauller
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com18

restoration is complete, it is sectioned from the unmilled ceramic block
and tried in place in the patient’s mouth. Depending on the material cho-
sen, the restoration may be finished with stains and glazes to create a
highly natural look.
A final seat is accomplished in about an hour, and the restoration is
held in place by traditional bonding methods. Many experts believe that
there is less risk of sensitivity or subsequent root canals following
treatment since the leakage sometimes associated with a temporary
restoration is eliminated.
Since there is no dark metal substructure, the result is highly natural
and aesthetic. The restoration also does not block x-rays, so dentists
can monitor the area for decay without the interference created by gold
or porcelain-fused-to-metal crowns.
CAD/CAM and Dental Implants
In the early 1990s, CAD/CAM entered into the world of dental
implants, bringing an alternative to stock or cast implant
abutments and frameworks. CAD/CAM implant frame-
works are milled from a homogenous block of
material without waxing, investing, or casting so
inaccuracies are eliminated and production
costs are reduced. CAD/CAM also helps
meet the challenge to correct unfavorable
implant angulations and achieve a
proper emergence profile.
CAD/CAM technology has enabled
dentists to use special computer-
controlled milling equipment to
create completely customized
implant abutments and gain precise
control over the margin design,
emergence profile, angulation and
retention. Customized implant abut-
ments provide a better fit and can
offer greater durability since materials
such as titanium, alumina and zirco-
nium can be used. CAD/CAM ceramics
offer highly natural optical properties so
the result is predictable and esthetic.
In order to achieve the highest possible
level of accuracy during implant placement, den-
tists sometimes use stereolithography to
manufacture CAD/CAM surgical templates. In select
cases, dentists with chairside CAD/CAM technology can
place and complete the dental implant in a single visit, without
impressions, temporary restorations, or a return visit. This allows
the implant to be placed without a flap using minimally invasive sur-
gery, and the prosthesis can then be delivered with immediate
functional loading to the implants.
As with all new technologies, there are those who are reluctant to fully
embrace CAD/CAM technology. There is a learning curve required to
use CAD/CAM properly, and dentists make a significant capital invest-
ment to acquire CAD/CAM equipment. However, practitioners report
that by eliminating laboratory fees and second appointments, overall
restoration costs are actually reduced.
CAD/CAM dental technology is here to stay and growing numbers of
practitioners find that the advantages far outweigh the drawbacks. The
genie is unlikely to go back in the bottle and is probably the forerunner
of further technological marvels that will continue to advance dentistry
beyond the current bounds of our imagination. n
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 19

NORTH TEXAS DENTISTRY | www.northtexasdentistry.com20
What new develop-ment in dentistryexcites you the most
for its potential effect onpatient care and why?
Dr. Tanur: The advances that have been
made in Implant Dentistry and their success
rate. With the ongoing research and better
technology in this field we are able to increase
the scope of alternatives to replace missing
teeth and better serve our patients.
For a patient who has health issues andseverely compromised
teeth that will need to beextracted, is there analternative to wearingremovable dentures?
Dr. Ovadia: Today, dental implants are one of
the most common and successful types of
treatment for replacing teeth. If natural teeth
are compromised due to periodontal disease,
caries, fractures or other reasons, dental
implants may be a wonderful option.
When patientscomplain that adenture is unstable,
uncomfortable andawkward, is there analternative that provides a permanent solution?
Dr. Tanur: For the denture wearer, implants
can mean a life without pain or embarrass-
ment, and a return to healthy eating habits.
Implants that are placed strategically in the
jawbone are able to support a full arch fixed
prosthesis, and give the patient replacement
teeth that function and feel like natural,
healthy teeth.
Q:
Q:
Dr. Eduardo Tanur & Dr. Ruben Ovadia Periodontal Associates
Periodontal Associates8722 Greenville Ave. Suite #100
Dallas, TX, 75243
www.dallasimplant.com
Eduardo Tanur DDS MS
(214) 503-1000
Ruben Ovadia DDS MS
(214) 503-1000
Q:
&AQ
Photo by Ray Bryant, Bryant Studios

www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 21
What are dentalimplants?
Dr. Ovadia: Dental implants are
small screws made of titanium that a
specialized implant surgeon can place in the
area where teeth are missing. Implants can
be utilized to support a permanent fixed
prosthesis.
What makes apatient a good
candidate for dentalimplants?
Dr. Tanur: A thorough review of the person’s
medical history and a clinical examination with
radiographs will allow the implant surgeon to
determine if an individual is healthy enough
and has sufficient bone for implant placement.
How many implantsare required tostabilize a full arch
fixed prosthesis?
Dr. Ovadia: A minimum of four or more dental
implants is required to support a full permanent
prosthesis using the All-On-4 technique.
All-On-4 is a treatment concept designed to
replace missing teeth with a full dental bridge
supported by just four dental implants.
What are theadvantages with All-On-4?
Dr. Tanur: Since fewer implants are needed,
the All-On-4 is the most cost-effective perma-
nent prosthetic solution. There is less need for
bone grafting, and less overall treatment and
healing time. Typically, temporary provisional
teeth are placed the same day. All-On-4 is a
scientifically proven and extensively docu-
mented option.
What level of comfortcan a patient expectwith an implant-
supported prosthesis?
Dr. Ovadia: Recent studies have shown that
an implant-supported prosthesis increases
biting forces up to 10x within the first year and
can increase biting forces up to 300x over
three to five years. Patients can have a
prosthesis that feels, functions and looks like
natural teeth when they smile. They can chew,
speak, and smile with ease again.
How predictable istreatment withdental implants?
Dr. Tanur: Dental implants have been
available since 1975. Extensive research
worldwide for almost 40 years supports their
use. They are highly predictable and have a
97% success rate. Dental implants have
helped millions of people have the natural-
looking, fully functional smiles they deserve.
How long doimplants last?
Dr. Ovadia: With adequate hygiene and
regular maintenance, implants normally can be
expected to last a lifetime.
Do implants helpprevent further boneloss?
Dr. Tanur: Implants stimulate bone like natu-
ral teeth do. When bone is being stimulated, its
natural physiologic properties allow normal,
healthy remodeling and turnover to take place.
Without the presence of teeth or dental
implants, bone begins to resorb and collapse
because it loses volume and density, which
affects the profile, phonetics, esthetics
and function.
Q:
Q:
Q:
Q:
Q:
Dr. Eduardo TanurCREDENTIALSDiplomate of the American Board of Periodontology
Former Faculty Member, Baylor College of Dentistry
EDUCATIONDDS - University Technological of Mexico, Mexico City
Certificate and MS in Periodontics and Implant Dentistry,
Baylor College of Dentistry, Dallas TX
PROFESSIONAL AFFILIATIONSAmerican Academy of Periodontology
American Academy of Osseointegration
Southwest Society of Periodontics
American Dental Association
Dallas County Dental Association
Texas Dental Association
Alpha Omega Dental Fraternity
Hispanic Dental Association
Dr. Ruben OvadiaCREDENTIALSDiplomate of the American Board of Periodontology
EDUCATIONDDS - University Technological of Mexico, Mexico City
GPR - National Institute of Perinatology
Residency in Periodontics - Tufts University School of
Dental Medicine
MS - Tufts University School of Dental Medicine
PROFESSIONAL AFFILIATIONSAmerican Dental Association
American Academy of Periodontology
Hispanic Dental Association
Texas Dental Association
North Texas Hispanic Dental Association
Dallas County Dental Society
Alpha Omega Dental Fraternity
Q:
Q:
Q:

&A
As the head of the largest dentalsupport services company in the U.S.,what do you think is the biggestchallenge facing dentistry today?
Steve Bilt: Dentistry’s biggest challenge was and continues to be that a
significant majority of the country underutilizes dental care. This includes
people not in care at all and people who aren’t receiving full and
adequate care.
Between 45-50% of the population doesn’t go to the dentist regularly.
It might be that someone gets a diagnosis that a tooth could use an
inlay, but he waits. Then he gets a crown diagnosis but he still waits
because it doesn’t hurt. Then suddenly he needs a root canal or he
loses that tooth.
Underutilization can also mean people are not getting adequate peri-
odontal care and therefore suffer bone loss then ultimately tooth loss.
Or perhaps they are suffering from other illnesses, such as cardiovas-
cular disease, that can stem from poor oral health. Underutilization could
even mean not getting an oral cancer screening which will obviously
have catastrophic results.
What are the barriers to peopleseeking dental care and what doSmile Brands affiliated offices offerpatients to increase utilization ofdental care?
Steve Bilt: One barrier is that private practice dentists have to do it all.
They have to be CEOs, financiers, marketers, experts on real estate and
demographics, and more. Those activities distract a dentist from deliv-
ering the best dental care possible.
Smile Brands has developed a model that includes understanding a
market so we can help the dentist land in a location that’s going to be
best suited to him or her. We find and develop that location and provide
the financing to complete it. We develop marketing material to attract
patients and provide call center support. We also handle billing and
collections and offer patients financing – all of which frees the
practitioner to focus on dentistry.
Q
Steve BiltPresident & CEO
Smile Brands Inc.
Q:
Q:
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com22

What makes the Smile Brandsbusiness model attractive to dentists?
Steve Bilt: The first time you go into business you better be prepared to
take a few lumps. Some dentists start as an associate in a private
practice and work with a more experienced dentist to learn the business
aspects of running a practice. If the goal is to be in a private practice,
that model has worked well for many years.
Smile Brands has spent nearly 15 years and tens of millions of dollars
learning and improving the business support side of dentistry. It’s a
learning curve that some dentists want to climb themselves, but other
dentists say, “You know what? Smile Brands has developed a package
of support services that allows me to focus on dentistry. That means I
can serve a middle market that I probably couldn’t efficiently serve if I
were doing it all myself.”
Smile Brands lowers the risk of starting out in a dental practice so
providers can be more predictably successful. Why is that? Because
there are elements of risk in any business; to the extent we can take
away some of those variables, your chance of success improves. The
Smile Brands model works really, really well and it’s really predictable.
It allows doctors to focus on dentistry and oral hygiene and serve the
patients well, then we limit the risk on the downside because of the
support services we provide and what results, mathematically, is a much
higher chance the dentist will be successful.
In addition, Smile Brands provides forums for continuing education and
best practice sharing, and facilitates mentoring. Plus, affiliated practices
offer a career path because these locations have multiple job layers for
doctors to grow in their career.
What do you think the mostsignificant changes to dentistry will be over the next 5 – 10 years?
Steve Bilt: First, there are many of ways to think about change. There’s
the future of technology in the dental space and all the clinical innova-
tions that are on the way. But there are many people far more qualified
than I am to opine on those changes.
A different type of change is how the business of dentistry will change.
Historically, dentistry has been accessed through the sole practitioner
model and that’s a great model. But dentistry is a $120 billion space
today, a huge healthcare sector. Over the next 5 to 10 years, you’re
going to see more business models emerging to serve niche segments
of the market.
For an example of this, look at retail. There are retailers that focus
specifically on the high-end consumer and retailers that target the
discount consumer, and they don’t compete. You don’t hear debate in
the Nordstrom boardroom over how they’re going to reach the
Walmart customer, and conversely, Walmart isn’t wondering how they’re
going to capture the Nordstrom customer.
Today more dentists are supported by business organizations that allow
them to better define their niche and target the middle market without
competing, per se, with other dentists. The Smile Brands model is
specifically designed to support the needs of a middle market consumer
who is price sensitive or may need financing. We’ve designed our
support model to enable the dentist to effectively and profitably reach a
market that’s unserved or underserved.
This shift in how dentistry is provided could raise the number of people
in regular care from 50% to perhaps 90% someday. And that’s the dream
– to make sure patients are served, and that dentistry is accessible to
them so they can stay in regular dental care.
What does the future, or at least thenext decade, hold for Smile Brands?
Steve Bilt: First, it’s probably more informative to look back 5 to 10 years
at where we’ve come from. A decade ago, we were supporting 45
offices – today there are 350. Back then, we were just in three states on
the West Coast – now we’re all across the country. Plenty will change
around the technology in the offices – information systems; digital
radiography; impressions and milling; laser technology – it’ll be dramatic.
As our footprint grows, there will be more places for patients to access
regular care, plus have easier access to specialty services as these
become more fully integrated with the dental office teams.
There will also be inno vations to improve how the doctor and patient
interact. It’s hard to predict what those might be but it will likely involve
PDAs or smart phones with
access to patient records and
other useful information.
Over time, this advanced
communication will improve
both the patient’s under-
standing of their care and
their interactions with their
providers. Those are all
things that Smile Brands will
help facilitate and that will be
a very powerful experience.
Q:
Q:
Q:
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 23
Throughout my 40 years in the dental field (30 years as an oral
surgeon), I have been troubled by the fact that we create oral wounds
on a daily basis but have never had an effective means of taking care
of those wounds. For example, we routinely extract teeth and send
patients home with a gaping hole in the mouth. The wound is subject to
a hostile environment teeming with pathogens and exposed to various
noxious chemicals (food, drink, tobacco, etc.). Yet the treatment plan
generally consists of nothing more than a prescription for pain
medication. Ignoring wounds in other parts of the body would be
considered substandard, at the very least.
Dressings are routinely applied to external wounds to protect them
from further damage and contamination, and to allow optimal healing
to take place. In dentistry, however, wound dressings have not existed.
Some dentists apply topical antibiotics after surgical extractions, or have
their patients use antiseptic rinses. These therapies are of questionable
benefit and, because of toxicity to the cells of wound healing, can
adversely affect the healing process. I found it unacceptable that, in the
21st century, dentistry was so far behind medicine when it came to taking
care of wounds of the mouth.
I posed this problem to Dr. Bill McAnalley. Bill is a pharmacologist and
toxicologist with more than 30 years experience in the wound care
arena. He has been awarded 35 U.S. patents and hundreds of interna-
tional patents for technology associated with natural-source health
products. Bill and his team had already developed the world’s first
widely marketed hydrogel wound dressing for external wounds.
I knew that, with his vast knowledge and experience, he was the ideal
person to develop a suitable wound care product for the mouth. I was
pleasantly surprised and gratified that Bill immediately understood the
urgency of this problem. After studying the properties required for an
ideal oral wound dressing, we agreed that such a product should protect
oral wounds from contamination, provide pain relief, enhance healing
and, most importantly, be safe to swallow.
Exhaustive research led to Bill’s newest innovation – an oral hydrogel
wound dressing that consists of 100% all-natural food ingredients,
something that had never been done before. After extensive experimen-
tation, we learned to utilize the natural characteristics of the food
ingredients, blend those ingredients and optimize their potent and
synergistic effects. Upon approval by FDA for management of all oral
wounds, ulcers and lesions, SockIt! Oral Hydrogel Wound Dressing
was born!
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com24
Dr. J. Hadley Hall Co-Developer of SockIt!
CREDENTIALSDiplomate of the American Board of Oral and Maxillofacial Surgery
Board Certified in 1986
Licensed in Texas, Oklahoma and Colorado
Texas State Board of Dental Examiners 1995-1997
(President 1996)
EDUCATION AND TRAININGDDS - Baylor College of Dentistry (1973)
Residency in Oral and Maxillofacial Surgery,
Oklahoma Health Sciences Center, Oklahoma City, Oklahoma
PROFESSIONAL AFFILIATIONSAmerican Association of Oral and Maxillofacial Surgeons
American Dental Association
Texas Dental Association
Texas Society of Oral and Maxillofacial Surgeons
Southwest Society of Oral and Maxillofacial Surgeons
Twelfth District Dental Society
American Dental Society of Anesthesiology
Dr. J. Hadley HallCo-Developer of SockIt!

Dr. Haroon Ismaili
Park Forest Oral and Maxillofacial Surgery(817) 466-8080
www.pfoms.com
CREDENTIALSDiplomate of the American Board of Oral and Maxillofacial Surgeons
Fellow of the American College of Oral and maxillofacial Surgery
Fellow of the International Society of Oral and Maxillofacial Surgery
EDUCATION AND TRAININGDDS - New York University
Residency in Oral and Maxillofacial Surgery, Washington Hospital
Center, Washington DC
PROFESSIONAL AFFILIATIONSAmerican Association of Oral & Maxillofacial Surgeons
American College of Oral and Maxillofacial Surgeons
Southwest Society of Oral and Maxillofacial Surgeons
American Dental Association
International Society of Oral and Maxillofacial Surgeons
I was introduced to SockIt! by Dr. Hadley Hall shortly after I moved to
Texas. I was initially skeptical. First, I had not heard of it, and I try to
stay on top of current technology. Second, the idea of an oral wound
dressing does not automatically come to mind as far as oral surgery is
concerned. However, when you realize that just about any surgical
procedure, or treatment of a traumatic injury, anywhere else on the body
is accompanied by placement of a wound dressing, similar treatment
of oral wounds makes sense. Wound dressings perform several func-
tions. An important one is to protect wounds from further injury, whether
from trauma or from the environment, such as chemicals and
pathogens. Patients are pretty good at protecting oral wounds from
trauma. However, the mouth is a hostile environment for wounds when
one considers the chemicals introduced from food, drink, tobacco, etc.,
and the bacteria, fungi and viruses that are inhabitants. With SockIt! we
have a simple, effective means of treating oral wounds with the same
respect we give any other wound of the body.
In addition to general wound care, SockIt! is very effective in
managing pain. It starts to provide pain relief in less than a minute, and
does not cause numbness. It does not contain any drugs, and the
mechanism for pain relief is different from that of anesthetic agents.
SockIt! does prevent the influx of sodium ions, which is the first step in
the generation of the pain impulse, but it is not absorbed into the tissues,
and it does not paralyze neurons and produce local anesthesia. People
like that. They want pain relief, but they don’t generally like that numb
sensation. Patients also like the words “drug-free” and “all-natural.”
With SockIt! patients know they have a means to address discomfort
anytime they need to, without worrying about toxicity.
Patients stay comfortable and they heal nicely without complications.
From the practice standpoint, the significant reduction in post-op compli-
cations is huge. We are informed of a great deal of patients with very
good pain control upon follow-up and it certainly reduces the number
of post op patients on the schedule.
At Park Forest Oral and Maxillofacial Surgery, we keep up with the
latest in technology and innovation and use SockIt! for virtually every
procedure, from extractions (it is especially good for immediate denture
patients), to implants, to graft procedures, biopsies, etc.
SockIt! is a chargeable service and there is an insurance code for
reimbursement. In addition to the value of reduced post-operative
discomfort for our patients, it also allows for a modest income stream.
SockIt! is a very valuable addition to our practice*. We have a safe,
effective means to provide patients pain relief and wound care that
brings dentistry and oral surgery more into line with medicine as far as
patient care is concerned. Patients are happier which makes life in the
office much more pleasant. * Dr. Ismaili is not affiliated in any way with SockIt! gel or its manufacturers.
Dr. Haroon IsmailiPark Forest Oral and Maxillofacial Surgery
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 25

Steven M. Lugar, CFP®
Beaird Harris Wealth Management, Inc.
12221 Merit Drive, Suite 750, Dallas, TX 75251
(972) 503-1040
www.bhcocapital.com
Beaird Harris Wealth Management is an
independent, fee-only wealth management
firm in Dallas, Texas. We provide objective,
fee-only advice to financially established
individuals and families, trust funds, retirement
plans and non-profit organizations – with a
particular emphasis in the medical, dental and
healthcare industries.
Beaird Harris is dedicated to helping clients
maximize their assets, reduce their financial
stress and realize their personal and
financial goals.
What’s thedifference between a fee-only and a fee-based advisor?
Steve: In a word, huge! The vast majority of
dentists, and other professionals as well,
probably don’t appreciate the difference and
what it means to them. In short, in addition to
an asset-based percentage fee, a fee-based
advisor can also receive other compensation,
such as commissions, from selling financial
products and insurance policies. This addi-
tional compensation can create conflicts of
interest that are not easily discerned by a
client. Conversely, fee-only advisors accept no
compensation or commissions from the
products or services that they use to
implement the client’s financial plan.
When should a dentist consult a financial advisor?
Steve: Ideally, the day they graduate from
dental school. While the tendency may be to
defer that consultation for a few years until
they are somewhat established, that decision
can result in tens, or even hundreds of thou-
sands, of wasted dollars. The decisions that
are made in the early years of a career, i.e.,
whether to buy an existing practice or start
your own, evaluating what rate to pay down
debt vs. save for retirement, what kind of
retirement plan to establish, and determining
how much house to buy, are really important.
They have a material impact on lifetime
wealth accumulation.
After almost thirty years in the business, I can
say with conviction that the people who get
good advice early in their careers have a huge
jump on those who wait. There is simply
no way to overstate the importance of
avoiding mistakes that have negative reper-
cussions for many years to follow. Most
individuals find that they make better financial
decisions when they tap into the expertise,
experience and discipline provided by a fee-
only financial advisor.
What experience doyou have workingwith dentists specifically?
Steve: For more than fifteen years, Beaird
Harris has worked with dental practices of all
sizes and specialties. They include recent
graduates working as associates prior to their
“buy-in,” sole practitioners as they launch
their practice and large dental groups with mul-
tiple owners. We provide expertise and objec-
tive advice in the myriad of subjects that dental
school did not equip them to deal with. This in-
cludes making correct decisions in the areas
of life and disability insurance, business entity
structure, proper choice and design of their
company retirement plan, and tax-efficient
strategies for building a substantial net worth,
separate and apart from their dental practice.
Do you serve yourclients in a fiduciarycapacity?
Steve: Yes, and simply put, “fiduciary” is a legal
term meaning to put the clients’ interests ahead of
our own. However, in the financial services
industry, true fiduciaries are difficult to identify.
Most financial advisors adhere to the “suitability”
standard – meaning that they only have to
document why their investment advice was
“reasonably justified” for you. A financial advisor
operating under this standard could still win an in-
centive prize for selling you a particular “suitable”
investment. The line is blurred between function-
ing as a fiduciary and almost functioning in a fidu-
ciary capacity. Lesson learned? Don’t expect
financial gurus or salespeople to act in your best
interest. Ask your financial advisor to put in writing
whether he or she upholds the fiduciary standards.
How are you compensated?
Steve: Beaird Harris is a fee-only financial
planning and wealth management firm. This
independence allows us to remain totally
impartial and deliver objective fiduciary advice
to clients.
Q:
Q: Q:
Q: Q:
Steven M. Lugar, CFP®
Beaird Harris Wealth Management, Inc.
&AQ
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com26

The Role of
SalivaryDiagnosticsin Today’s Practice
Salivary diagnostics is moving today’s dental practices toward a
practice model of evidence-based dentistry, creating a balance
between the scientific and technically-based practice. Salivary
diagnostics presents a new scientific tool that affords dental practices
the opportunity to provide lab-based data in educating patients and
dental professionals alike.
There are numerous studies and articles authored on the oral-
systemic links and how the body is affected by the oral biofilm. Salivary
diagnostics provides the tool for acquiring more information on the oral
biofilm in the mouth at practice level.
When we perform salivary diagnostics we are testing the oral biofilm,
the bacteria present in the mouth. It is tested, typed and quantified. We
also have the ability to test the patients’ genetic predisposition for inflam-
mation. A patient is either positive or negative for the inflammation
marker. The inflammatory marker is linked to all critical diseases facing
the population today. These include, but are not limited to, heart
disease, stroke and diabetes. Performing these two tests answers
pieces of the puzzle in diagnosing the mouth that dentists and
hygienists have been unable to answer before.
Controlling the oral biofilm is the common denominator in dentistry
today. Clinically, when a practitioner is performing endodontics, peri-
odontics, decay removal or placing an implant, controlling or eradicating
the oral biofilm is one of the key steps in successful treatment. Prior to
the introduction of salivary diagnostics there has not been a way of
quantifying the oral biofilm in the mouth in a simple and concise way.
Dental professionals based a diagnosis on the effects of the damage
caused by the oral biofilm. We now have a way of preventing the
damage from the uncontrolled biofilm versus fixing the damage after
the damage has occurred.
When we speak of the oral biofilm what does this really mean? This
is the saliva in the mouth, but when we look deeper at the DNA of the
biofilm, it is made up of over 500 strains of bacteria; the majority of the
500 are harmless. Salivary diagnostics reveals the 13 strains of
bacteria that are known to be tissue and bone destructive in the mouth
and through research we know these same 13 are directly linked to
systemic issues in the body. Knowing the 13 infective types of bacteria
and whether or not it is of consequence on the body opens the window
in truly controlling the oral biofilm. With a quantifiable report, treatment
regimens become truly personalized based on a patient’s oral biofilm’s
bacteria types, bacteria concentrations and the patient’s genetic
predisposition to inflammation.
Quantifiable reports before and after treatment are of unquestionable
benefit. In medicine, it is standard of care to test a patient starting on a
cholesterol reducing drug, performing ongoing monitoring of how the
therapy is working with follow-up lab reports. Lab reports can answer
questions that at times would have been unanswerable in dentistry. We
have all had a mouth that looked CONTINUED ON PAGE 30 4
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 27

How much is a baby tooth worth — fifty cents?
A dollar? Ten dollars? Some researchers think a single
baby tooth could be priceless, providing you plan
ahead instead of giving it away to the tooth fairy.
When intellect, inspiration and serendipity converge, interesting things
can happen. Dr. Songtao Shi certainly has the first element of the
equation. He earned a D.D.S. and M.S. degree from Peking University
and a Ph.D. from USC. After serving on the faculty at Beijing Medical
University, Shi opened a private pediatric dentistry practice in Los
Angeles. He was eventually lured to the laboratories of the NIH, where
he quickly earned accolades in the scientific world for his brilliant work
in the area of stem cells taken from bone marrow. Then in 2003, along
came serendipity.
Shi’s little girl showed her dentist-scientist daddy a wiggly front tooth
and asked him for help. She needed to get it to the tooth fairy. He
obliged, and while cleaning the tooth off, he noticed a tiny bit of tissue
inside the tooth. That got Shi thinking. In 2000, he and another NIH
researcher had found mesenchymal stem cells (MSCs) in the dental
pulp of adult teeth. A few days later, when his daughter lost her other
front tooth at bedtime, Shi zipped off to his lab. Sure enough, his
inspiration had led him to an exciting discovery – there were young stem
cells in the tooth pulp left behind in the baby tooth!
A singularly special cell
Stem cells have a unique job. They are the only cells in our body that
can regenerate. A specific type of stem cell can differentiate into a
variety of specialized tissue types in order to regenerate organs, tissues,
and bones. Because stem cells are the building blocks of organ tissue,
the immune system and blood, scientists have pondered their healing
potential for decades. Stem cells from bone marrow were first used to
save the lives of cancer patients who need help regenerating blood and
immune cells after chemotherapy. Then, in the ‘80s, scientists began
looking at stem cells taken from umbilical cord blood, which offer a
number of advantages over bone marrow stem cells.
Youth, as it turns out, is particularly significant when it comes to a stem
cell. In fact, we age partly because the ravages of time outpace our
adult stem cells’ weakened ability to regenerate cells. Stem cells taken
from cord blood and teeth are vital and powerful, with only minimal
degradation from age. Cryopreserving stem cells protects them from
damage from aging, environmental factors, and viruses that occurs
naturally in our bodies as we grow older.
Cryopreserved stem cells are available right away as opposed to waiting
for cells from bone marrow, and collection is safe and painless. They
are very young but not taken from embryos, so they are not associated
with the same ethical controversy as embryonic stem cells. Because
Science vs. theTooth Fairy New Promise in Baby Teeth
By Tina Cauller
Songtao Shi, DDS, PhD, Associate Professor, Herman Ostrow School of Dentistry of USC (University of Southern California, Los Angeles, CA) in the laboratory.
Ph
oto
co
urt
esy o
f D
r. S
on
gta
o S
hi
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com28

the cells are autologous – taken from the patient’s own body – there is
less risk of complication and no need for immunosuppressive medica-
tions to prevent rejection.
After the discovery of stem cells in his daughter’s tooth, Songtao Shi
began collecting newly-lost baby teeth from her friends and any other
cooperative 7- and 8-year olds he could enlist. He named the cells
SHED (stem cells from human exfoliated deciduous teeth). He found
that they proliferated rapidly into clusters, much faster than stem cells
isolated from bone marrow or adult teeth.
Shi hypothesized that SHED are responsible for giving the order to
make bone around the permanent tooth as it comes in, and with the
proper cues, might be able to induce bone formation. He was right.
When he implanted SHED under the skin of mice, they triggered the
formation of bone. This was exciting – an earlier trial using stem cells
from adult wisdom teeth had been unsuccessful. Shi knew that the stem
cells in teeth share a common origin with neural tissue. With careful
direction, he managed to coax the SHED to form neural cells in the brain
and fat cells. Stem cells from adult teeth are much less potent
generators of neural cells and incapable of inducing fat cell formation.
Researchers believe that SHED may be able to restore cells damaged
by diseases like Parkinson’s or restore the cells that make dopamine
so nerve cells can function properly.
Tooth or fiction?
When it comes to therapies using stem cells, the future is here. It isn’t
science fiction and its promise, while still continuing to unfold, has
arrived. Whole bladders grown in the laboratory from a patient’s own
stem cells have been successfully implanted. Doctors have grown
patches to cover a hole or weakening in a blood vessel, as well as knee
cartilage and tendons. Stem cells are being used to grow cardiac tissue,
bone, insulin-producing pancreatic beta cells and other tissues. In some
cases, a biological or synthetic scaffold is required to direct the growth
of the cells into the desired form. Doctors recently replaced a British
teenager’s trachea with one grown from her own stem cells over a
donor scaffold. Dr. Jeremy Mao of Columbia University Medical Center
recently developed a growth factor-infused scaffold with the potential to
regenerate an anatomically correct tooth in just nine weeks from
implantation. Once the stem cells have colonized the scaffold, a tooth
can grow in the socket and then merge with the surrounding tissue.
Further research has proven that the tooth bud of the mandibular third
molar is an especially rich source of multipotent stem cells, which can
form enamel, dentin, blood vessels, dental pulp, neural tissues, muscle,
bone, organs, insulin-producing pancreatic cells, skin, cartilage, and
hepatocytes. Researchers are currently developing stem cell therapies
to treat a host of ailments including Type I diabetes, Parkinson’s,
Alzheimer’s, arthritis, cardiac disease, multiple sclerosis, spinal cord
injury and numerous others. Even some genetic conditions may be
treated using stem cells from a healthy sibling.
For dentistry, stem cell therapy could mean the ability to regrow natural
teeth. How far off is this? A whole tooth is complicated structure. Most
experts think that growing a whole tooth in a human mouth is a decade
or more in the offing. “We have a long way to go,” says Dr. Songtao
Shi. “A whole human tooth is no less complex an organ than a human
heart.” For now, Shi and his team at USC are working on growing a “bio
root” – a living tooth root – and he predicts that this milestone could be
just a year or two away. They have already grown a living root and
supporting periodontal ligaments in a pig sufficient to support a crown
restoration and hope to go to clinical trials in the near future.
“We are using the background information and experience from dental
implants and looking for ways to replace the artificial root substitute with
a functional bioimplant,” Shi notes. When asked about research goals
that are closer to realization, Shi shares his excitement about the team’s
proximity to success in treating periodontal disease. “At present, we can
treat periodontitis, but we lack an effective method to reverse the
damage done by disease. We are very close to being able to use cell
regeneration to grow new tissue to firmly support a tooth affected by
disease. This is a very promising development.”
Saving for the future
While NIH is prohibited by conflict of interest considerations from oper-
ating a stem cell bank, private companies are springing up to meet the
demand for this promising new area of medical technology. One
company at the forefront of this new technology is StemSave, an FDA-
registered company based In New York.
StemSave works with dentists to recover teeth at the optimal time,
before they become very loose, to assure the highest probability of stem
cell viability. (The pulp chamber of the deciduous tooth may be oblit-
erated by the erupting tooth by the time the tooth actually becomes
loose.) To participate, patients enroll at www.StemSave.com or by
calling 877-STEMSAVE. Prior to the planned procedure, the patient’s
dentist receives a patented kit that contains a vial with a special solution
to nourish and protect the cells during transport. When the tooth is
extracted, the dentist simply places the extracted tooth into the kit. The
kit is then sealed and sent to StemSave laboratories where the
specimen is processed. Once the presence and viability of the cells is
confirmed, the cells are cryopreserved. If the patient has a need for their
stem cells in the future, they contact StemSave directly to arrange
www.northtexasdentistry.com | NORTH TEXAS DENTISTRY 29

transport from storage. The StemSave process was carefully designed
to take less than a minute of a dentist’s time. The company maintains
the contractual relationship with the patient for cryopreservation so there
is no paperwork or payments for the dentist’s office to manage.
For parents who missed out on the chance to bank cord blood, harvest-
ing and preserving a child’s stem cells from baby teeth could be a
golden opportunity. Parents of older children may be relieved to know
that the opportunity to bank immature tooth-derived stem cells does not
end at the kindergarten door. Adolescents can bank dental stem cells
when bicuspid teeth are extracted in preparation for orthodontic treat-
ment, when a tooth is fractured, or after the extraction of wisdom teeth.
It is best to recover these teeth during the developmental stage,
between age 16 and 20, since this is when the stem cells are most
active in formation of the root. However, even third molars or permanent
teeth with healthy pulp that are extracted later in life can be a source of
viable stem cells.
Tooth wisdom
The value of tooth-derived stem cell banking is questioned by some
who argue that the future potential of the cells to provide useful therapy
is uncertain and speculative. Others argue that the companies are
preying on parents’ natural concerns for their child’s health, nudging
them toward excessive anxiety. There are concerns about what will
happen to the saved cells if the company goes under. Skeptics are
critical of the initial and annual costs of cryopreservation. Banking
companies have responded with assurances that their fees are fair and
worthwhile and that they have a plan in place for the continuity of their
services should the company fail.
Still, the NIH and HHS (Department of Health and Human Services) are
waving off these reservations. Both are putting a lot of eggs into the
basket of regenerative medicine, and these organizations are not known
to commit funds without good reason. Experts at both agencies are
banking on regenerative medicine to improve our quality of life and
reduce health care costs and have committed significant resources to
the field. The U.S. military’s Armed Forces Institute of Regenerative
Medicine is channeling hundreds of millions of dollars into efforts to
develop stem cell therapies to treat wounded soldiers.
While the practical payoff may be years away, research is advancing
our knowledge by leaps and bounds every day. Many informed and
thoughtful people who can afford to pay the fees for cryopreserving cells
from teeth are deciding that the potential benefit far outweighs the cost.
After all, how do you put a price on even the slightest possibility that
your child might someday be helped by investing in a simple, painless
procedure? Dentists are finding that the service is simple and
convenient. More important, they are finding that it is being enthusias-
tically received by patients who appreciate that their dentist is looking
out for them by offering an option that might someday save the life of
their child.
Of course, no one is looking to send the tooth fairy into quaint
obsolescence. Just hoping that she might become a lifesaving fairy
godmother for someone should the need arise. n
CONTINUED FROM PAGE 274 textbook perfect with slight
inflammation and bleeding only to have the patient return in six months
with bleeding and probe depths that were progressing and a noticeable
odor in the mouth.
Dentistry is revolutionized when biofilm pathogens are known and
quantified. Judicious care can be prescribed in treating and eradicating
the pathogens doing the damage when we use this powerful tool in
every day practice. A patient’s genetic risk assessment and biofilm test
all become part of the diagnostics equation along with x-rays and clinical
examination. Enabling practitioners to assess and know what a patient’s
inflammatory response and bacterial infection is as an adjunct to
prescribed therapy. By embracing the knowledge that saliva’s DNA
provides, dentists can prevent the oral cavity from being of any negative
consequence on the overall health of the body.
Today, patients are better educated in the care of their teeth and
gums, and have a better understanding of how this relates to their
body’s overall health. Patients are more ready than ever to embrace
and accept partnering with their doctors in their overall care, and fully
expect to keep their teeth for their lifetime. The integration of salivary
diagnostics into dentistry today will fuel the growth of the next century
of dentistry.
Creating a shift in the nature of today’s dental practice requires an
approach from many different angles. Currently, dentists are afforded
the opportunity to be at the forefront of integrating salivary diagnostics
into their practices and learn how this will grow and change the way
dentistry is practiced. Clinical research continues to give us the
empirical data needed as evidence grows on the oral-systemic links.
Indicators show there is a visionary shift in dentistry moving dental prac-
tices toward evidence-based dentistry utilizing salivary diagnostics.
Salivary diagnostics presents an adjunct for educating, motivating and
changing the way dentistry is practiced both today and in the future.
Salivary diagnostics, as with any new technique, product or service,
demands due diligence and proper training to employ the new tool and
interpret the results in order to utilize the product to its full potential and
benefit the patient and practices of today. Financially, this creates a
revenue stream much like the boost dental practices received from intra-
oral cameras. “A picture is worth a thousand words.” In the case of
salivary diagnostics, the picture is the lab report.
Go to www.mydentalgenetics.com for more information on
salivary diagnostics. n
ADVERTISER’S INDEX
Destiny Dental Laboratory ......................................................................page 7
Med+Tech Construction....................................................................back cover
Straumann..............................................................................inside front cover
NORTH TEXAS DENTISTRY | www.northtexasdentistry.com30