THE COST-EFFECTIVENESS ANALYSIS FOR USE … as infertility, threatened miscarriage / habitual...
13
Faculty of Applied Mathematics and Control Processes, St. Petersburg State University 3 First Pavlov State Medical University of St. Petersburg 1 Faculty of Medicine, St. Petersburg State University 2 THE COST-EFFECTIVENESS ANALYSIS FOR USE OF DYDROGESTERONE IN PREMENSTRUAL SYNDROME Kolbin A. 1,2 , Vilyum I. 1 , Kurylev A. 1 , Balykina Yu. 3 , Proskurin M. 3 The study was conducted by support from Abbo5 Laboratories.
Transcript of THE COST-EFFECTIVENESS ANALYSIS FOR USE … as infertility, threatened miscarriage / habitual...

Faculty of Applied Mathematics and Control Processes, St. Petersburg State University 3
First Pavlov State Medical University of St. Petersburg1
Faculty of Medicine, St. Petersburg State University 2
THE COST-EFFECTIVENESS ANALYSIS FOR USE OF DYDROGESTERONE IN
PREMENSTRUAL SYNDROME
Kolbin A.1,2, Vilyum I.1, Kurylev A.1, Balykina Yu.3, Proskurin M.3
The study was conducted by support from Abbo5 Laboratories.
BACKGROUND
§ Premenstrual Syndrome (PMS) - a cyclical symptom that occurs during the premenstrual period and is characterized by somatic, neuropsychiatric, vegetative-vascular, metabolic and endocrine disorders.
§ Progesterone is a well-known drug for treatment of clinical symptoms of PMS.
§ In Russia the following drugs are used: micronized progesterone (Utrogestan®, oral and intravaginal administration); dydrogesterone (Duphaston®, oral); micronized progesterone (Krayon®, intravaginal).
§ These drugs are currently used for various gynecological indications, such as infertility, threatened miscarriage / habitual miscarriage, amenorrhea, dysfunctional uterine bleeding, dysmenorrhea, premenstrual syndrome, endometriosis and endometrial hyperplasia.

OBJECTIVES
The primary objective of the study is to analyze pharmaco-economic expediency of administration dydrogesterone (Duphaston®) for premenstrual syndrome (PMS) treatment in comparison with oral micronized progesterone (Utrogestan®).

For the calculation of the efficacy were used data of clinical trials (n = 3)
Author (year) Study (N of patients), age Wyatt K., et al.
(2001) Systematic review (n=909), 20-40
Dennerstein L., et al. (1985)
A double blind crossover trial (n=23), 18-45
Haspels A.A., et al (1981)
A double-blind, placebo-controlled, multi-center study
(n=130), 18 -40
MATERIALS

METHODS • The mathema9cal modeling with dydrogesterone or oral micronized
progesterone was applied in the study. • The model was constructed as follows: in each branch of the decision tree cost
and efficacy were analyzed for a group of 100 pa9ents (female aged 18 -‐ 45 years) and per pa9ent.
• Modeling dura9on was 3 months (therapy during three cycles). • The incremental cost-‐effec9veness ra9o (ICER) were counted. • Results were evaluated as to the cost-‐effec9veness threshold. • Efficacy was es9mated on the basis of clinical trials. • Calcula9on of cost included: the cost of treatment course with selected drugs;
the cost of gynecologist’s consulta9ons and diagnosis; the cost of inefficient therapy – costs of addi9onal diagnos9c examina9on.
• The comprehensive sensi9vity analysis was performed.

Female with premenstrual
syndrome
Administration of dydrogesterone (Duphaston®)
Administration of micronized progesteron
(Utrogestan®)
Effectiveness – symptoms were cured
Symptoms were not cured, further search for causes
of the disease
Symptoms were not cured, further search for causes
of the disease
DECISION TREE
Effectiveness – symptoms were cured

Results
• The cost of the total course of therapy with dydrogesterone was more
expensive in comparison with micronized progesterone – 123.67$
against 121.47$.
• Strategy of administration of dydrogesterone showed more efficacy
(73%) in comparison with oral micronized progesteron (65%) - 8%
increase of effectiveness.
• CERs for dydrogesterone and micronized progesterone were 169.41
and 186.87 respectively.
• The ICER for dydrogesterone amounts to 27.55$ per patient.
• The sensitivity analysis confirmed conclusions of the main scenario.

123.67
121.47
Cost, $
Duphaston Utrogestan
Costs were calculated on the basis of Russian prices (grls.rosminzdrav.ru), 2013.
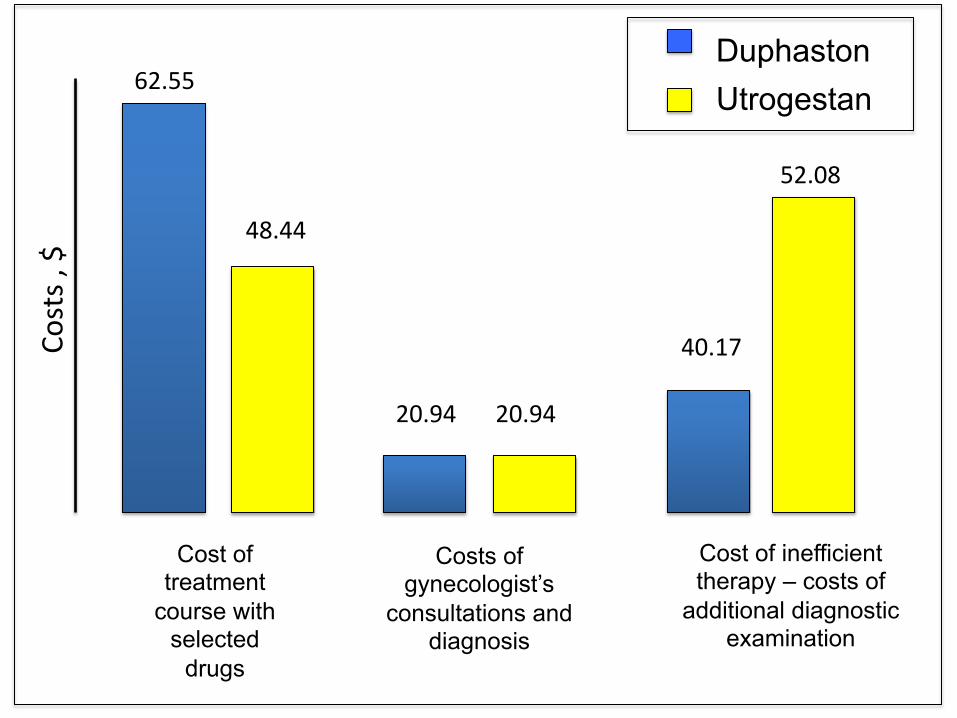
62.55 Co
sts , $ 48.44
52.08
40.17
20.94 20.94
Utrogestan Duphaston
Cost of treatment
course with selected
drugs
Costs of gynecologist’s
consultations and diagnosis
Cost of inefficient therapy – costs of
additional diagnostic examination

121
122
122
123
123
124
124
62,5% 65,0% 67,5% 70,0% 72,5% 75,0%
Cos
t, $
Efficacy, %
Дюфастон
Утрожестан
Duphaston
Utrogestan

Incremental Cost-Effectiveness Ratio
DRUGS Efficacy, Cost, $
CER Additional efficacy
Additional cost, $
ICER, $
Duphaston 0.73 123.67 169.41 0.08 2.2 27.55
Utrogestan 0.65 121.47 186.87
• The ICER for dydrogesterone amounts to 27.55$ per patient

CONCLUSION
The administration of dydrogesterone in PMS is economically
expedient from the point of view of the cost-effectiveness ratio.
In addition, an increase in effectiveness was noted for the use of
dydrogesterone.

1. Wyatt K. et al. Efficacy of progesterone and progestogens in management of premenstrual syndrome: systematic review. BMJ 2001;323:1–8
2. Haspels AA. A double-blind, placebo-controlled, multi-center study of the efficacy of dydrogesterone (Duphaston). In: The premenstrual syndrome (Eds:Van Keep PA and Utian WH), Lancaster England:MTP Press Limited, 1981, 81-92.
3. Martorano JT. Et al. Differentiating be-tween natural proges-terone and synthetic progestins: clinical implications for premenstrual syndrome and perimenopause management. ComprTher. 1998; 24(6&7):336–9.
4. Dennerstein L. et al. Progesterone and the premenstrual syndrome: a double blind crossover trial. Br Med J (Clin Res Ed). 1985 Jun 1; 290(6482): 1617–21.
5. O'Brien P.M. Helping women with premenstrual syndrome. BMJ. 1993 December 4; 307(6917): 1471–1475.
6. Magill PJ. Investigation of the efficacy of progesterone pessaries in the relief of symptoms of premenstrual syndrome. British Journal of General Practice 1995;45(400):589–93.
7. Vaneslow W, Dennerstein L, Greenwood KM, de Lignieres B. Effect of progesterone and its 5 alpha and 5 beta metabolites on symptoms of premenstrual syndrome according to route of administration. Journal of Psychosomatic Obstetrics and Gynaecology 1996;17(1):29–38.
List of References