The Cluster Network1 Development Programme supports GP … GP Cluster... · 2017-06-12 · DR AFT...
23
DR 2016 Version 0a 1 Cluster Network Action Plan 2016-17 (Third year of the Cluster Network Development Programme) Anglesey Cluster The Cluster Network 1 Development Programme supports GP Practices to work to collaborate to: • Understand local health needs and priorities. • Develop an agreed Cluster Network Action Plan linked to elements of the individual Practice Development Plans. • Work with partners to improve the coordination of care and the integration of health and social care. • Work with local communities and networks to reduce health inequalities. The Action Plan should be a simple, dynamic document and in line with CND 002W guidance. The Plan should include: - Objectives that can be delivered independently by the network to improve patient care and to ensure the sustainability and modernisation of services. Objectives for delivery through partnership working Issues for discussion with the Health Board For each objective there should be specific, measureable actions with a clear timescale for delivery. Cluster Action Plans should compliment individual Practice Development Plans, tackling issues that cannot be managed at an individual practice level or challenges that can be more effectively and efficiently delivered through collaborative action. 1 A GP cluster network is defined as a cluster or group of GP practices within the Local Health Board’s area of operation as previously designated for QOF QP purposes
Transcript of The Cluster Network1 Development Programme supports GP … GP Cluster... · 2017-06-12 · DR AFT...
DRAFT
2016 Version 0a 1
Cluster Network Action Plan 2016-17
(Third year of the Cluster Network Development Programme)
Anglesey Cluster
The Cluster Network1 Development Programme supports GP Practices to work to collaborate to:
• Understand local health needs and priorities.
• Develop an agreed Cluster Network Action Plan linked to elements of the individual Practice Development Plans.
• Work with partners to improve the coordination of care and the integration of health and social care.
• Work with local communities and networks to reduce health inequalities.
The Action Plan should be a simple, dynamic document and in line with CND 002W guidance.
The Plan should include: -
Objectives that can be delivered independently by the network to improve patient care and to ensure the sustainability and modernisation of
services.
Objectives for delivery through partnership working
Issues for discussion with the Health Board
For each objective there should be specific, measureable actions with a clear timescale for delivery.
Cluster Action Plans should compliment individual Practice Development Plans, tackling issues that cannot be managed at an individual
practice level or challenges that can be more effectively and efficiently delivered through collaborative action.
1
A GP cluster network is defined as a cluster or group of GP practices within the Local Health Board’s area of operation as previously designated
for QOF QP purposes
DRAFT
2016 Version 0a 2
To understand the needs of the population served by the Cluster Network
The Cluster Profile provides a summary of key issues. Local Public Health Teams can provide additional analysis and support. Consider
local rates of smoking, alcohol, healthy diet and exercise – what role do Cluster practices play and who are local partners. Is action
connected and effective? What practical tools could support the delivery of care? Health protection- consider levels of immunisation and
screening- is coverage consistent- is there potential to share good practice? Are there actions that could be delivered in collaboration-
e.g. Community First to support more effective engagement with local groups
No Objective For completion by: - Outcome for patients Progress to Date
1 To review the needs of the
population using available data
To ensure that services are
developed according to
local need
2 To identify additional
information requirements to
support service development
Improved support for
service development
3 To consider learning from
previous analyses to identify
any outstanding service
development needs
4 To develop a plan to contribute
to the reduction in prevalence
of smoking
Improved health outcomes
Improved quality of life
PLEASE NOTE THIS PIECE OF WORK WILL BE SUPPORTED BY PUBLIC HEALTH WALES AND YOUR LOCAL AREA TEAMS

DRAFT
2016 Version 0a 3
POPULATION NEED (Priority 1 – Smoking Cessation)
Priority 1 The issues Aims and objectives How will this be done? Named Lead
Time Scale
Smoking
cessation
22% of adults smoke on Anglesey (2013/14). Although this shows a reduction from 2012/13, it is still above the North Wales average of 20%. Smoking is linked to social class and accounts for a high proportion of the inequalities in health outcomes. North-West Anglesey has the highest level of deprivation and had the highest level of smoking-attributable admissions in BCU. Quitting smoking offers better improvement to healthy life expectancy than almost any other medical or social intervention. NICE guidance is that 5% of adult smokers should be treated every year. This is now a Health Board Tier 1 target, with 40% quit rate. Although we have reached the 5% target our recorded quit rates are well below 40% Variable referral rates and access to smoking cessation services on the island.
Implementation smoking cessation pathway in all Practices: GP Practices are asked to signpost to specialist smoking cessation service such as Stop Smoking Wales or Pharmacy Level 3 as this is the most effective support for a successful quit. Increase demand for specialist smoking cessation services
Offer timely and appropriate support for all adult smokers who wish to make a quit attempt Try and improve quit rates Ensure tailored interventions and equity of access and outcomes for specific groups, such as pregnant women, manual workers, people with mental health problems and socioeconomically disadvantaged communities
PHW are undertaking work to map smoking cessation services across the island starting in Holyhead first.The objective is to ensure an integrated smoking cessation service across community, secondary care, mental health, social care, and other local settings. The smoking cessation integration project commenced in Holyhead in January 2016. The outcomes from this Integrated Smoking Cessation Service project and progress across the island to be shared with the Cluster Smoking cessation advice pathway to be available and understood by all members of each practice team on the island
PHW
SM
Ongoing over next 12 months
9 months

DRAFT
2016 Version 0a 4
POPULATION NEED (Priority 2 to be chosen by Cluster)
Priority 2 The issues Aims and objectives How will this be done? Named Lead
Time Scale
Obesity
29% of boys and 23% of girls aged 4-5 are overweight or obese in Anglesey, which is slightly over the BCUHB average. 57% (2012/13) adults on Anglesey are either overweight or clinically obese. 23% of adults are clinically obese and this figure has risen from 21% the previous year. Increasingly significant public health challenge
To ensure that there is a clear locality pathway to support individuals trying to lose weight Provide education for primary care staff
• All primary care professionals should be
aware of the ’10 steps’ advice
• Map organizations on the island already providing weight loss support
• Development of Childhood Obesity
Framework on the island
PHW
PHW
PHW
3 months
12 months
6 months
DRAFT
2016 Version 0a 5
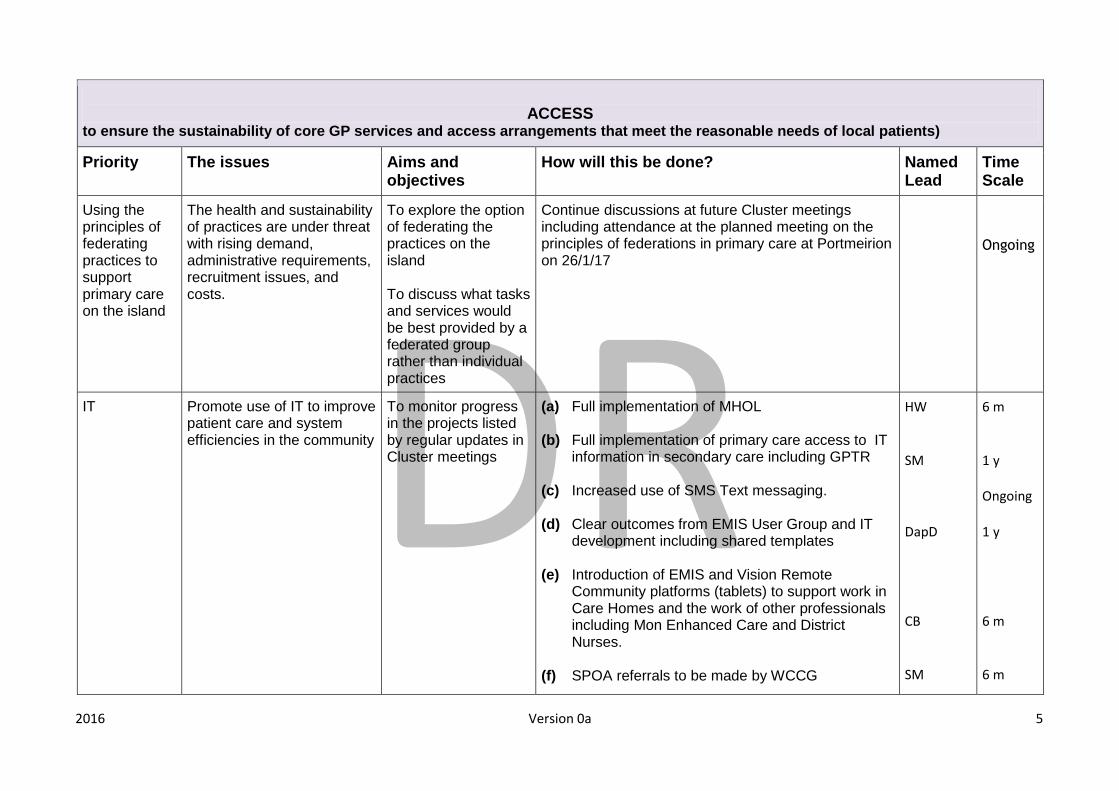
ACCESS
to ensure the sustainability of core GP services and access arrangements that meet the reasonable needs of local patients)
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Using the principles of federating practices to support primary care on the island
The health and sustainability of practices are under threat with rising demand, administrative requirements, recruitment issues, and costs.
To explore the option of federating the practices on the island To discuss what tasks and services would be best provided by a federated group rather than individual practices
Continue discussions at future Cluster meetings including attendance at the planned meeting on the principles of federations in primary care at Portmeirion on 26/1/17
Ongoing
IT Promote use of IT to improve patient care and system efficiencies in the community
To monitor progress in the projects listed by regular updates in Cluster meetings
(a) Full implementation of MHOL (b) Full implementation of primary care access to IT
information in secondary care including GPTR (c) Increased use of SMS Text messaging. (d) Clear outcomes from EMIS User Group and IT
development including shared templates (e) Introduction of EMIS and Vision Remote
Community platforms (tablets) to support work in Care Homes and the work of other professionals including Mon Enhanced Care and District Nurses.
(f) SPOA referrals to be made by WCCG
HW SM DapD CB SM
6 m 1 y Ongoing 1 y 6 m 6 m
DRAFT
2016 Version 0a 6
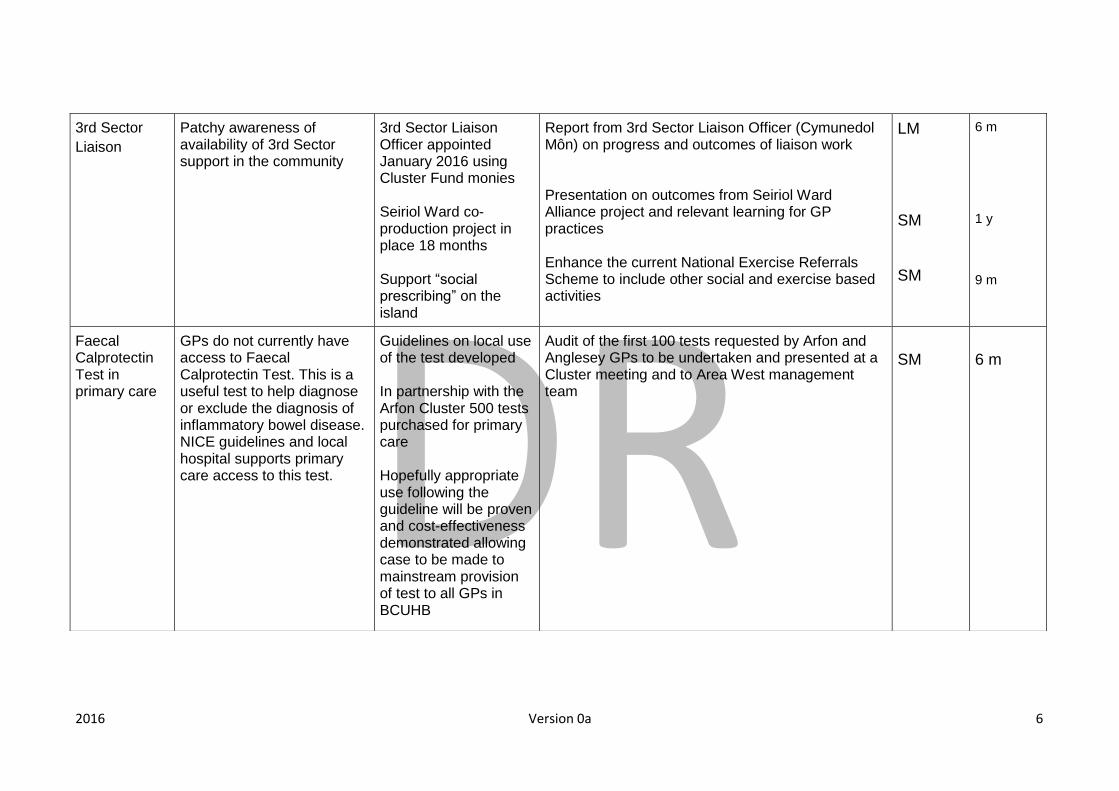
3rd Sector
Liaison
Patchy awareness of availability of 3rd Sector support in the community
3rd Sector Liaison Officer appointed January 2016 using Cluster Fund monies Seiriol Ward co-production project in place 18 months Support “social prescribing” on the island
Report from 3rd Sector Liaison Officer (Cymunedol Môn) on progress and outcomes of liaison work Presentation on outcomes from Seiriol Ward Alliance project and relevant learning for GP practices Enhance the current National Exercise Referrals Scheme to include other social and exercise based activities
LM SM SM
6 m 1 y 9 m
Faecal Calprotectin Test in primary care
GPs do not currently have access to Faecal Calprotectin Test. This is a useful test to help diagnose or exclude the diagnosis of inflammatory bowel disease. NICE guidelines and local hospital supports primary care access to this test.
Guidelines on local use of the test developed In partnership with the Arfon Cluster 500 tests purchased for primary care Hopefully appropriate use following the guideline will be proven and cost-effectiveness demonstrated allowing case to be made to mainstream provision of test to all GPs in BCUHB
Audit of the first 100 tests requested by Arfon and Anglesey GPs to be undertaken and presented at a Cluster meeting and to Area West management team
SM
6 m

DRAFT
2016 Version 0a 7
Wylfa and other commercial developments on the island population
A number of developments are being planned for Anglesey including Wylfa B nuclear power station, Land and Lakes tourist destination, and Lorry Terminal It is predicted that this could result in as many as 11000 workers and their families moving onto the island This will have an implication for provision of community care on the island including workforce and premises issues
To assure regular dialogue with developers, PHW, BCUHB/Area Team and other agencies to ensure community services supported with this predicted increase in population
Continue current series of meetings involving relevant GP practices, West Area Management Team, developers, LA, and other stakeholders.
WT Ongoing
48 hour Ambulatory ECG (AECG) Service in the community
Currently long waits for patients to have ambulatory ECG (AECG) investigations in secondary care
To enable GP Practices to have direct access to AECG recording for their patients
4 AECG machines leased from Cardionetics and put into several GP practices. Guidelines for use done. Self reporting software installed. Audit of use and outcomes to be undertaken at end of 12m use. Training session to be arranged with local cardiology specialist
SM SM
18/10/16 18/10/16

DRAFT
2016 Version 0a 8
WORKFORCE
Important Note: Each Practice has submitted practice specific plans to detail what will be done in order to meet any practice specific workforce needs e.g to cover a period of maternity leave, recruit to a specific vacancy. The table below refers to matters that can be taken forward at a Cluster level and/or require HB input.
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Recruitment in General Practice
Reduced availability of trained GPs to fill vacancies in practices. Potentially this could get worse over the next few years with expected GP retirements. Small pool of available GP locums. Increasing workload in primary care and fairly static GP numbers
To improve GP recruitment in BCUHB with particular reference to Anglesey
To attend RCGP Annual Conference in Harrogate and promote General Practice in North Wales on exhibition stand there List all practices willing to provide work experience to school children on the island
SM HW
8/10/16 1 month
DRAFT
2016 Version 0a 9
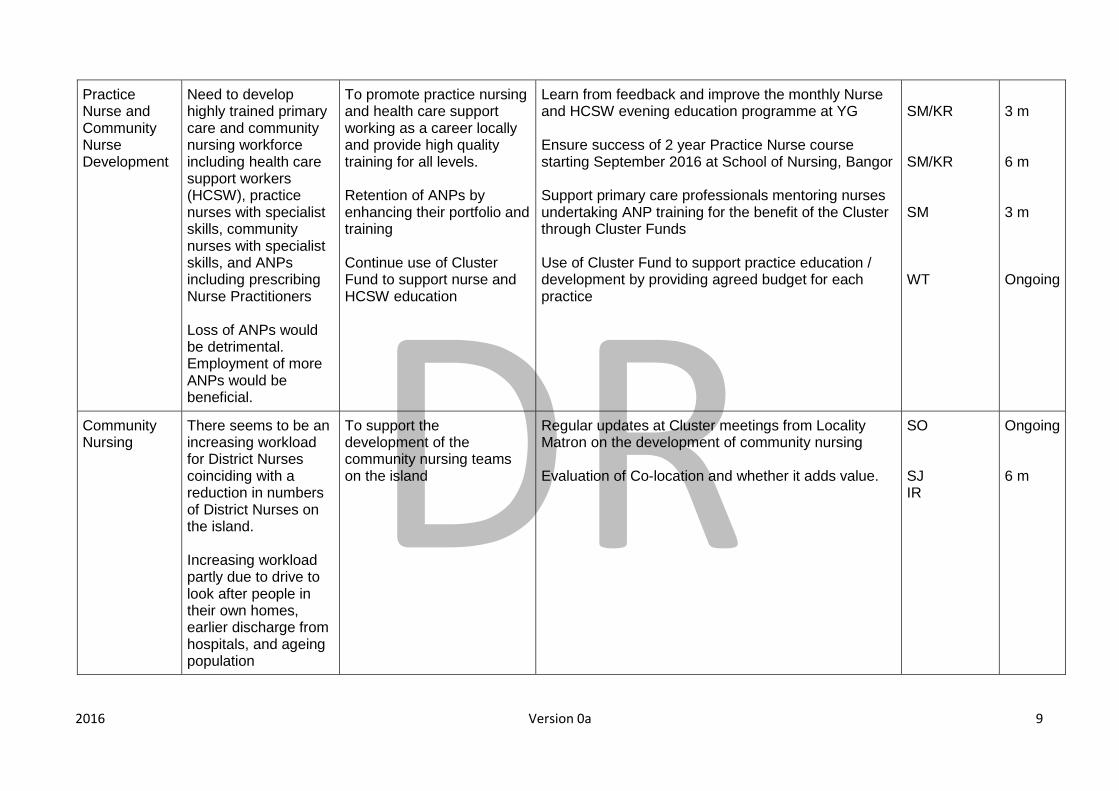
Practice Nurse and Community Nurse Development
Need to develop highly trained primary care and community nursing workforce including health care support workers (HCSW), practice nurses with specialist skills, community nurses with specialist skills, and ANPs including prescribing Nurse Practitioners Loss of ANPs would be detrimental. Employment of more ANPs would be beneficial.
To promote practice nursing and health care support working as a career locally and provide high quality training for all levels. Retention of ANPs by enhancing their portfolio and training Continue use of Cluster Fund to support nurse and HCSW education
Learn from feedback and improve the monthly Nurse and HCSW evening education programme at YG Ensure success of 2 year Practice Nurse course starting September 2016 at School of Nursing, Bangor Support primary care professionals mentoring nurses undertaking ANP training for the benefit of the Cluster through Cluster Funds Use of Cluster Fund to support practice education / development by providing agreed budget for each practice
SM/KR SM/KR SM WT
3 m 6 m 3 m Ongoing
Community Nursing
There seems to be an increasing workload for District Nurses coinciding with a reduction in numbers of District Nurses on the island. Increasing workload partly due to drive to look after people in their own homes, earlier discharge from hospitals, and ageing population
To support the development of the community nursing teams on the island
Regular updates at Cluster meetings from Locality Matron on the development of community nursing Evaluation of Co-location and whether it adds value.
SO SJ IR
Ongoing 6 m
DRAFT
2016 Version 0a 10
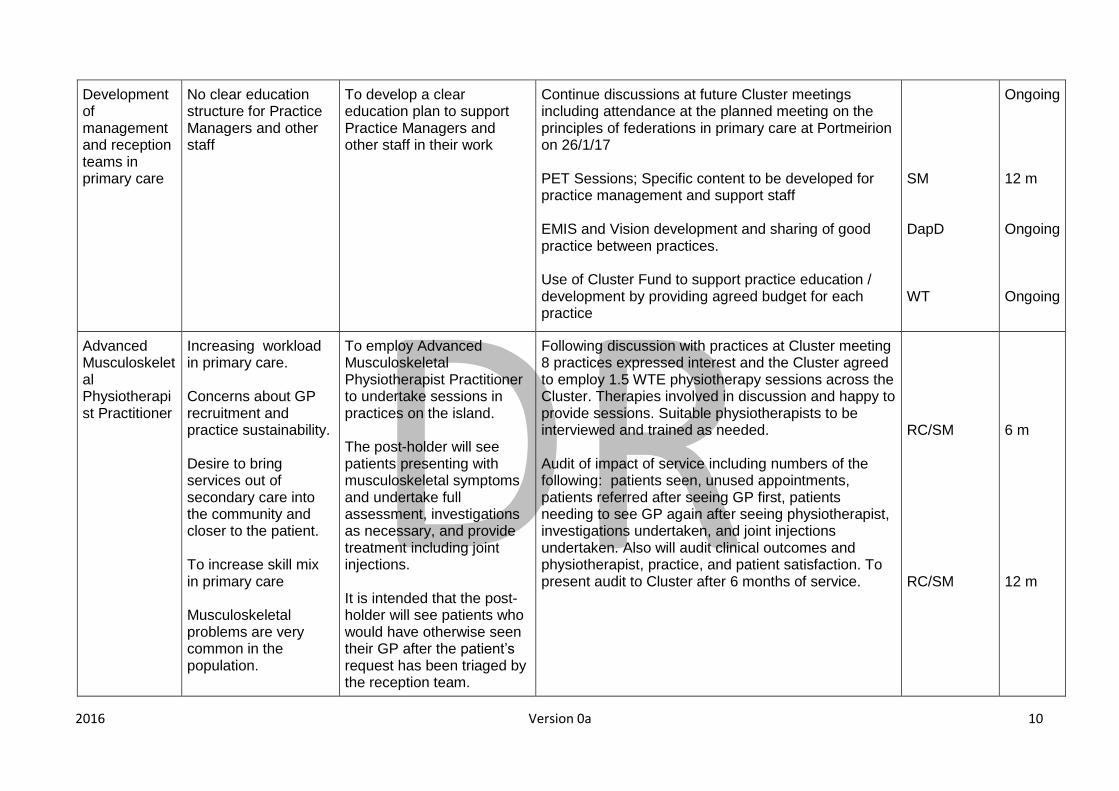
Development of management and reception teams in primary care
No clear education structure for Practice Managers and other staff
To develop a clear education plan to support Practice Managers and other staff in their work
Continue discussions at future Cluster meetings including attendance at the planned meeting on the principles of federations in primary care at Portmeirion on 26/1/17 PET Sessions; Specific content to be developed for practice management and support staff EMIS and Vision development and sharing of good practice between practices. Use of Cluster Fund to support practice education / development by providing agreed budget for each practice
SM DapD WT
Ongoing 12 m Ongoing Ongoing
Advanced Musculoskeletal Physiotherapist Practitioner
Increasing workload in primary care. Concerns about GP recruitment and practice sustainability. Desire to bring services out of secondary care into the community and closer to the patient. To increase skill mix in primary care Musculoskeletal problems are very common in the population.
To employ Advanced Musculoskeletal Physiotherapist Practitioner to undertake sessions in practices on the island. The post-holder will see patients presenting with musculoskeletal symptoms and undertake full assessment, investigations as necessary, and provide treatment including joint injections. It is intended that the post-holder will see patients who would have otherwise seen their GP after the patient’s request has been triaged by the reception team.
Following discussion with practices at Cluster meeting 8 practices expressed interest and the Cluster agreed to employ 1.5 WTE physiotherapy sessions across the Cluster. Therapies involved in discussion and happy to provide sessions. Suitable physiotherapists to be interviewed and trained as needed. Audit of impact of service including numbers of the following: patients seen, unused appointments, patients referred after seeing GP first, patients needing to see GP again after seeing physiotherapist, investigations undertaken, and joint injections undertaken. Also will audit clinical outcomes and physiotherapist, practice, and patient satisfaction. To present audit to Cluster after 6 months of service.
RC/SM RC/SM
6 m 12 m
DRAFT
2016 Version 0a 11
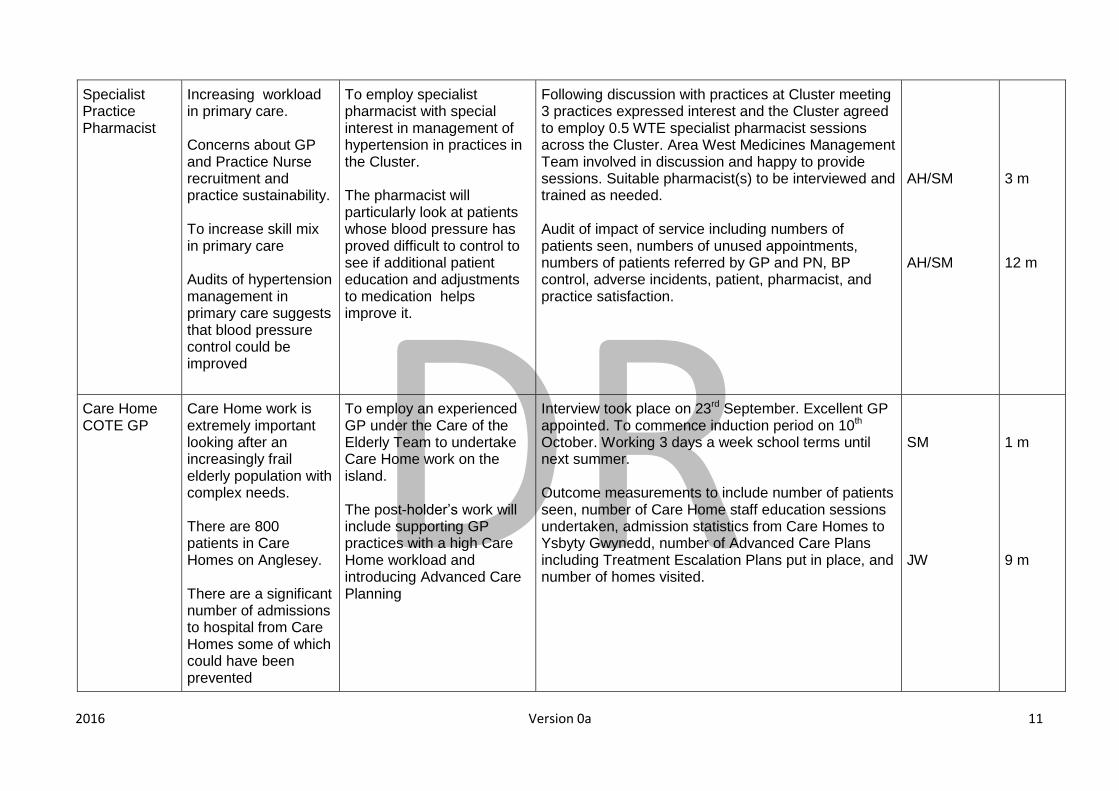
Specialist Practice Pharmacist
Increasing workload in primary care. Concerns about GP and Practice Nurse recruitment and practice sustainability. To increase skill mix in primary care Audits of hypertension management in primary care suggests that blood pressure control could be improved
To employ specialist pharmacist with special interest in management of hypertension in practices in the Cluster. The pharmacist will particularly look at patients whose blood pressure has proved difficult to control to see if additional patient education and adjustments to medication helps improve it.
Following discussion with practices at Cluster meeting 3 practices expressed interest and the Cluster agreed to employ 0.5 WTE specialist pharmacist sessions across the Cluster. Area West Medicines Management Team involved in discussion and happy to provide sessions. Suitable pharmacist(s) to be interviewed and trained as needed. Audit of impact of service including numbers of patients seen, numbers of unused appointments, numbers of patients referred by GP and PN, BP control, adverse incidents, patient, pharmacist, and practice satisfaction.
AH/SM AH/SM
3 m 12 m
Care Home COTE GP
Care Home work is extremely important looking after an increasingly frail elderly population with complex needs. There are 800 patients in Care Homes on Anglesey. There are a significant number of admissions to hospital from Care Homes some of which could have been prevented
To employ an experienced GP under the Care of the Elderly Team to undertake Care Home work on the island. The post-holder’s work will include supporting GP practices with a high Care Home workload and introducing Advanced Care Planning
Interview took place on 23rd September. Excellent GP appointed. To commence induction period on 10th October. Working 3 days a week school terms until next summer. Outcome measurements to include number of patients seen, number of Care Home staff education sessions undertaken, admission statistics from Care Homes to Ysbyty Gwynedd, number of Advanced Care Plans including Treatment Escalation Plans put in place, and number of homes visited.
SM JW
1 m 9 m
DRAFT
2016 Version 0a 12
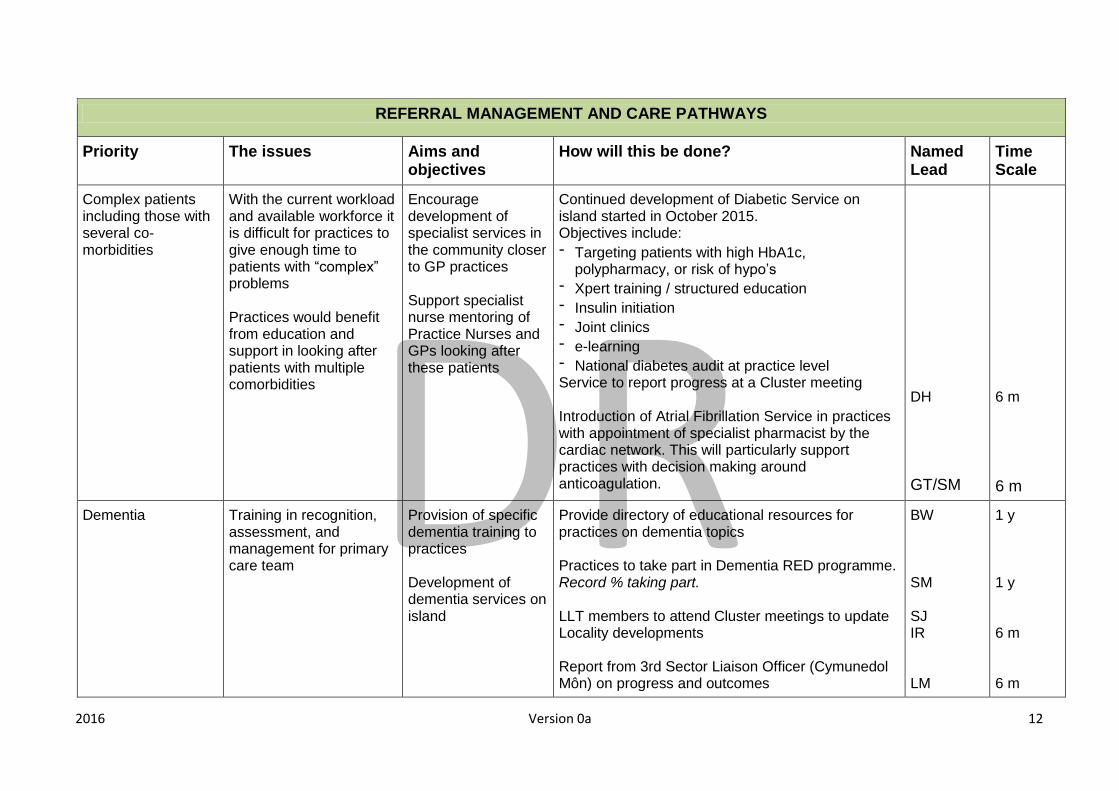
REFERRAL MANAGEMENT AND CARE PATHWAYS
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Complex patients including those with several co-morbidities
With the current workload and available workforce it is difficult for practices to give enough time to patients with “complex” problems Practices would benefit from education and support in looking after patients with multiple comorbidities
Encourage development of specialist services in the community closer to GP practices Support specialist nurse mentoring of Practice Nurses and GPs looking after these patients
Continued development of Diabetic Service on island started in October 2015. Objectives include: - Targeting patients with high HbA1c,
polypharmacy, or risk of hypo’s - Xpert training / structured education - Insulin initiation - Joint clinics - e-learning - National diabetes audit at practice level Service to report progress at a Cluster meeting Introduction of Atrial Fibrillation Service in practices with appointment of specialist pharmacist by the cardiac network. This will particularly support practices with decision making around anticoagulation.
DH
GT/SM
6 m
6 m
Dementia Training in recognition, assessment, and management for primary care team
Provision of specific dementia training to practices Development of dementia services on island
Provide directory of educational resources for practices on dementia topics Practices to take part in Dementia RED programme. Record % taking part. LLT members to attend Cluster meetings to update Locality developments Report from 3rd Sector Liaison Officer (Cymunedol Môn) on progress and outcomes
BW SM SJ IR LM
1 y 1 y 6 m 6 m

DRAFT
2016 Version 0a 13
Primary Care - Secondary Care interface
Improved communication and pathways between primary and secondary care very important on many levels including quality of care and patient safety
Continue primary care - secondary care meeting programme in Protected Education Time sessions Monthly Ynys Mon Medical Society Meetings programme to continue. Set up a Cluster working group looking at specific issues concerning the interface between primary and secondary care
SM SM SM
Ongoing Ongoing 6 m
Medical photography
It is helpful for the dermatology team to receive a photograph of skin lesions when a patient is referred as a USC referral
Practices have all been supplied with a camera and have been asked to attach a photograph when making a USC dermatology referral via WCCG
Audit use of camera and feedback from GPs and dermatology team
AM
6 m
Abnormal liver function tests investigation and management pathway
It became apparent at a Ynys Mon Medical Society meeting that primary care knowledge of the investigation and management of abnormal liver function tests is patchy
A pathway has been developed by the Benllech practice and circulated to all practices.
Monitor use of the pathway and make changes to it in response to feedback or new guidelines
SM
1 y

DRAFT
2016 Version 0a 14
UNSCHEDULED CARE (To provide high quality, consistent care for patients presenting with urgent care needs and to support the continuous development of services to improve patient experience, co-ordination of care ad effectiveness of risk management)
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Supporting provision of Near Patient Testing (NPT) in practices
Some tests can be used more effectively if result available without delay
To trial the use of a CRP NPT machine in primary care Quick access to CRP result will inform patient care including appropriate use of antibiotics
CRP NPT equipment provided in one GP surgery from November 2015 to see if it aids management decisions and allows better informed prescribing of antibiotics. Assessment of use has shown significant drop in antibiotic prescribing in that practice since then. Also noted that positive feedback from GPs and patients on the provision of the CRP NPT. To purchase additional CRP NPT equipment for 4 other practices on the island and record impact in the same way to see if antibiotic use reduced. In addition to introduce antibiotic audit to practices not using CRP NPT to see if audit process reduces antibiotic prescribing
AH SM
3 m 3 m
Suicide Prevention GPs and primary care teams feel uncertain as to how to assess suicide risk and support patients at risk. Significant public health issue Current lack of capacity in mental health services
Suicide Prevention Training took place on 22nd September. Reasonable attendance by Anglesey GPs.
Following the training on 22/9/16 the plan is to facilitate Suicide Awareness and Patient Support Plan software to be uploaded on to practice computer systems as clinical aid. It is hoped that the software will be available in January 2017.
SM
Jan/Feb 2017

DRAFT
2016 Version 0a 15
AKI Acute Kidney Injury is a significant cause of unscheduled admissions
To provide information to patients on how to avoid AKI
Circulate software to practices embedding issuing of AKI leaflet in computer system
DapD
6 m
Development of Enhanced Care Service / Mon Enhanced Care (MEC) I.V. Therapy provision Support of housebound patients with chronic disease such as COPD
Availability of nursing and social care support out of usual hours
Services to be developed more to provide more comprehensive 24 hour 7 day a week service Difficulty recruiting nursing professionals to take part in MEC Needs proper staffing and resourcing and further integration with district nursing teams
To support development of effective Enhanced Care Service (MEC) on the island To support provision of IV therapy in the community To support the development of user friendly referral documentation using appropriate e-referral system
Regular meetings with Locality Matron and MEC Team including COTE consultant to discuss issues. Support community nursing developments. Model Mon LLT members to attend Cluster meetings to update Locality developments including use of ICF monies Additional GP/COTE doctor has been in post now since July. This means that MEC now have much better doctor support than a year ago. Plans to expand role of MEC continue to be discussed in regular MEC meetings.
SM SJ IR SJ IR SM
Ongoing Ongoing Ongoing
Advanced Care Planning
Unfortunately some patients are admitted to hospital as an emergency when it isn’t in their best interest
To promote advanced care plans on the island particularly in Care Homes
Introduction of Treatment Escalation Plans (TEPs) in Care Homes across the island through education of GPs, use of ANPs, and support of COTE team including newly appointed GP/COTE Care Home doctor
SM
12 m
Flu immunisation programme
Flu immunisation is important in prevention of unscheduled admissions Uptake of flu vaccinations below BCUHB average on island
To promote flu immunisation on the island To clarify role of community pharmacists
Presentation and discussion at Cluster meeting by PHW. Learning also from other practices. Support from Medicines Management Team regarding role of community pharmacists.
PHW SM
Sept 2016 - ongoing

DRAFT
2016 Version 0a 16
TARGETING THE PREVENTION AND EARLY DETECTION OF CANCERS (Refer to National Priority Areas CND 006W)
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Referral of patients to other practices in the Locality for specific services
Some practices undertake specific procedures relevant to early detection of cancer that might be a useful referral option for other practices. Examples include sigmoidoscopy, dermatoscopy, minor surgery and indirect laryngoscopy.
Explore option of referrals from GP Practice to GP Practice for specific services
Discussion of federation model and sharing of services Attendance of practices at Federation Conference in Portmeirion on 26/1/17
SM 1 y
Early detection of
cancer and
appropriate USC
referrals
Early detection of cancer
is very important but often
difficult
To educate GPs and
other health
professionals in
locality on how to use
scoring systems such
as Qcancer
Clarify local referral,
investigation, and
management
pathways in different
specialities
Continue primary care - secondary care meeting programme in Protected Education Time sessions To continue monthly evening education meetings through the Ynys Mon Medical Society Clinicians to complete individual case reports for patients newly diagnosed with lung, digestive system and Ovarian cancers via the Significant Event Analyses Templates (SEA) 2015/16 To complete the exercise as laid out in requirements for cluster domain in QOF 2015/16. Results of this to be discussed at Cluster meeting
SM SM SM
Ongoing Ongoing March 2017

DRAFT
2016 Version 0a 17
IMPROVING THE DELIVERY OF END OF LIFE CARE (Refer to National Priority Areas CND 007W)
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
DNA CPR forms Advanced Decision Making
Confusion in relation to DNA CPR status within various settings – i.e. hospital , care homes and OOH - particularly when patient transferred Need to discuss end of life issues more with patients and their families
Everyone looking after a patient should be clear as to whether a DNACPR form is in place and when it was last discussed with the patient and family Promote Advanced Care Planning to our patients and families To support the Treatment Escalation Plan (TEP) pilot as a Cluster and support wider implementation
Continue palliative care input into Cluster meetings. Attending meeting in December. Introduction of Treatment Escalation Plans (TEPs) in Care Homes across the island through education of GPs, use of ANPs, and support of COTE team. Continue development of Palliative Care Templates with correct READ Codes etc on Practice Computer systems with support of EMIS Users group and Vision.
SM SM DapD
Ongoing 12 m 6 m
Palliative Care Education
Education for primary care professionals and Care Homes is important to improve palliative care in the community
Provide good quality education locally
Arrange palliative care educational sessions through discussions with palliative care team. PET educational meeting arranged for Tuesday 8th November and Wednesday 15th February.
SM

DRAFT
2016 Version 0a 18
MINIMISING THE HARMS OF POLYPHARMACY (Refer to National Priority Areas CND 008W)
Priority The issues Aims and objectives
How will this be done? Named Lead
Time Scale
Polypharmacy in the
frail elderly
Polypharmacy risks in the elderly.
To reduce risks in this patient group
“No-Tears” Reviews in Practices and sharing of lessons learnt.
SM
9 m

DRAFT
2016 Version 0a 19
PREMISES PLAN
Important Note: Each Practice has submitted practice specific plans to detail what will be done in order to meet any practice specific needs relating to premises. The table below refers to matters that can be taken forward at a Cluster level and/or require HB input.
Issue Why? What will be done at Cluster Level
How will this be done? (Practice; GP Cluster; Health Board) Named Lead
Time Scale
Capacity within current buildings including car parking
Not enough room for existing services Other agencies using rooms within the building Practices keen to house more members of the Patch MDT if only they had room Practices keen to develop services Difficult to increase training capacity on the island
Link budget for spatial development to commitment to training or development of specific services Liaise with Local Authority Liaise with BCUHB
Options suggested by clusters are:
1. New Primary Care building to be built on the Ysbyty Penrhos Stanley site to incorporate all 3 Holyhead Practices
2. New Primary Care building In Llangefni incorporating both practices.
3. Beaumaris Health Centre: Extension to provide more space for MDT working and new services. Alterations to Reception area to improve patient confidentiality.
4. Bodorgan, Llanfaelog, and Gaerwen: Working to full capacity and all 3 buildings would benefit from an extension.
5. Cemaes Surgery: Creation of additional room for HCA.
6. Coed Y Glyn: Funding for an extension if unable to proceed with new building in Llangefni (see 2. above)
7. Dwyran: Disabled access needs improving. Additional space / extension required for dispensing team.
8. Gwalchmai: Insufficient storage space for records: alternative storage options to be explored.
9. Llanfairpwll Health Centre: Significant lack of space both in building and in car park. HB owned building. Plenty of space to develop around the building. Significant extension needed to fully develop services and MDT working.
10. Star: Needs grant to improve disabled access
SM
WT
3 y

DRAFT
2016 Version 0a 20
MPIG Changes Potential closure of branch surgeries Loss of staff due to costs
Funding pressures in line with loss of MPIG Plans to close Transport problems for patient (in the event of branches closing)
Identify cost implications in relation to loss of MPIG.
Discussion with PCSU, BCUHB, GMC and WG through LMC EapI RK
Ongoing
Some practices are concerned regarding lack of confidentiality in their reception areas
Open plan reception areas causing concern
Sharing of
experiences of
different
reception area
design
Liaise with BCUHB regarding improvement grants (see premises plan above)
PMs group
1 y
Disabled Access Some practice buildings are not disabled compliant including facilities for deaf
Map problems
regarding
disabled
access
Discuss with BCUHB Estates Enquire regarding grants for specific equipment options to help patients with deafness access services
PMs group
3 y

DRAFT
2016 Version 0a 21
CLUSTER NETWORK ISSUES
Issue Why? What will be done?
How will this be done? (Practice; GP Cluster; Health Board) Named Lead
Time Scale

DRAFT
2016 Version 0a 22
LHB Issues
(in addition to any issues raised above requiring Health Board input)
Issue Why? What will be done?
How will this be done? (Practice; GP Cluster; Health Board) Named Lead
Time Scale
Paperwork Too much paperwork for primary care
Reduce unnecessary paperwork
PCSU/HB review of paperwork that Practices have to complete “Paper!” to be produced on how this can be addressed
PCSU PMs
3 y
Welsh Language What support is available for practices?
Review current support and identify unmet needs
Discussion between BCUHB, Cluster, LA, and 3rd Sector SM 3 y
Changing practice list sizes
Some practices feel under threat because of dropping list sizes, threatened closure branch surgeries and others are concerned regarding big influx of patients due to local developments such as Wylfa
Formation of clear strategy for the island regarding primary care provision and support of General Practice
Meetings between GP Practices and PCSU/BCUHB/Estates SM PMs WT
18 m
Information on BCUHB Intranet
Often difficult for primary care to access information on the BCUHB Intranet
Discussion between primary care and BCUHB on what needs to be developed
Issues to address include one clear point of access to all referral pathways SM 1 y

DRAFT
2016 Version 0a 23
LHB Issues
(in addition to any issues raised above requiring Health Board input)
Issue Why? What will be done?
How will this be done? (Practice; GP Cluster; Health Board) Named Lead
Time Scale
Specific Service Improvements in the community
There is documented concern about deterioration in provision of a number of services in the community affecting patient care
Discussion with BCUHB regarding concerns raised by GP Practices
Areas of concern include the following: Stroke Services in the community Physiotherapy Services in the community Speech Therapy Services Dementia Services particularly Day Care provision Mental Health Services particularly lack of substantive consultant psychiatry post on Anglesey Need for more Care of the Elderly specialist support in the community Better access to DAPHNE in the West Better access to dietetic services for patients with low BMI Pulmonary Rehabilitation Services Availability of equipment such as hip protectors
Ongoing
Continuing Health Care Funding
CHC Funding applications bureaucratic and time-consuming
Streamline application process? Leave responsibility in hands of Patch MDT? Nominal budgets for Cluster or Patch MDT?
Discussion at BCUHB level Steve 3 years