
Thank you for joining us today! · If you wish to download today’s presentation it is ... (CNSs)...
66
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. If you wish to download today’s presentation it is is available at www.chsrf.ca/researcheroncall .
Transcript of Thank you for joining us today! · If you wish to download today’s presentation it is ... (CNSs)...
Thank you for joining us today!
Please dial 1.800.732.6179 now to connect to the audio for this webinar.
To show/hide the control panel click the double arrows.
If you wish to download today’s presentation it is is available at www.chsrf.ca/researcheroncall.
Integrating Advanced P ti N (APN )Practice Nurses (APNs)
Dr. Alba DiCenso, McMaster UniversityLinda Sawchenko, Interior Health
Dr. Sophie Nadeau, McGill UniversityG N d C l P l i Fl Cli iGrace Neustaedter, Calgary Pelvic Floor Clinic
Wednesday March 17th 2010Wednesday, March 17th, 201012:00 – 1:30pm EDT
2

Objectives
• To distinguish the 3 types of APNs in CanadaT tli th f ilit t d h ll t th i f ll • To outline the facilitators and challenges to their full integration into the Canadian healthcare systemT l f f l i i f h • To present examples of successful integration of these roles
3
Advanced Practice Nurse
• Registered nurse• Graduate nursing degreeGraduate nursing degree• Expert clinician with advanced clinical
decision-making skills and a high level of g gautonomy
• Expanded scope of practice• Formal credentialing process
4
APN Competencies
• Clinical• EducationEducation• Research• LeadershipLeadership• Consultation & Collaboration
5

Types of Advanced Practice Nurses in CanadaCanada
• Primary Health Care Nurse Practitioners (PHCNPs)(also known as family or all ages NPs)(also known as family or all-ages NPs)
• Acute Care Nurse Practitioners (ACNPs)( l k i lt NP d lt di t i (also known as specialty NPs, adult, pediatric or
neonatal NPs)
• Clinical Nurse Specialists (CNSs)
6
Nurse Practitioners
• involved in health promotion, disease prevention & acute and chronic illness management
• diagnose• order and interpret diagnostic testsg• prescribe pharmaceuticals • perform specific procedures within their legislated p p p g
scope of practice
7

Clinical Nurse Specialistst ib t t d l t f i k l d d • contribute to development of nursing knowledge and
evidence-based practice and facilitate system change
• address complex health care issues for patients, families, other disciplines, administrators, and policy makers
• specialize in specific area of practice that may be defined in terms of a population, a setting, a disease or medical in terms of a population, a setting, a disease or medical subspecialty, type of care, or type of problem
8

9
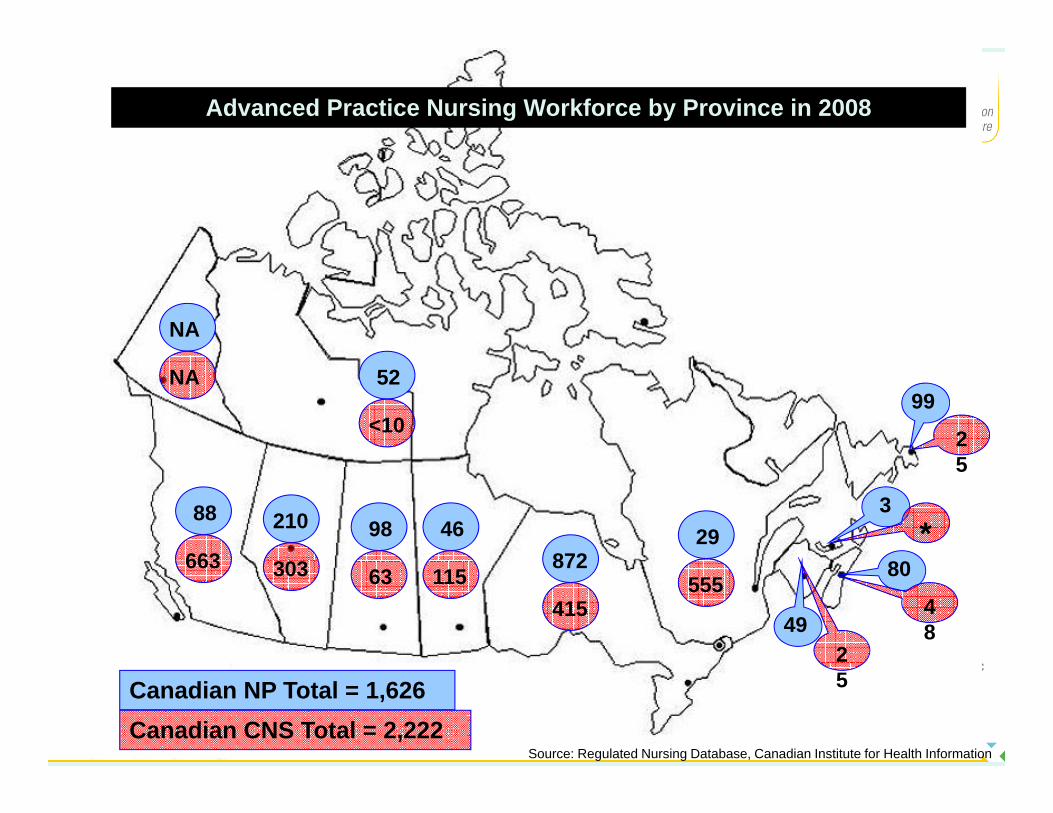
Advanced Practice Nursing Workforce by Province in 2008
NA
9952
25
<10
NA
346
8898210
872*
5
29663 80872
249
48
555415
11563303663
Canadian NP Total = 1,626
Source: Regulated Nursing Database, Canadian Institute for Health InformationCanadian CNS Total = 2,222
5

Decision Support Synthesis
To conduct a review of the literature and stakeholder interviews to:interviews to:
• Identify and describe distinguishing characteristics of CNS and NP role definitions and competenciesCNS and NP role definitions and competencies
• Identify key barriers and facilitators for effective development and utilization of CNS and NP rolesdevelopment and utilization of CNS and NP roles
11

Decision Support Synthesis
Scoping Review of Literature • 468 papers (all Canadian papers of any type or date 468 papers (all Canadian papers of any type or date
and international review papers 2003-2008)
Key Stakeholder Interviews (81) • APNs, government policymakers, nurse administrators,
regulators educators physicians other health care regulators, educators, physicians, other health care team members
12

Effectiveness of APNs
Numerous randomized controlled trials (RCTs) and systematic reviews have shown that APNs are effective, safe practitioners who can positively influence patient safe practitioners who can positively influence patient, provider and health system outcomes:
ACNPs: 18 RCTs (11 since 2000)PHCNPs: 28 RCTs (18 since 2000)CNSs: 32 RCTs (20 since 2000)CNSs: 32 RCTs (20 since 2000)
13
General Key Facilitators
• Systematic patient-focused planning to guide role development including early stakeholder involvement
• Clearly defined APN roles• Public and health provider awarenessp
14

PHCNPs – Facilitators and ChallengesFacilitators:
• Government legislation and regulation• Government funding for NP positions• Emphasis on interprofessional collaboration facilitated by a Emphasis on interprofessional collaboration facilitated by a
shift away from FFS physician reimbursement model
Challenges:Challenges:• Working out relationship between two autonomous clinicians
(NPs and GPs) with substantial overlap in scope of practice• Inconsistencies in educational preparation across Canada• Inconsistencies in educational preparation across Canada
15
ACNPs – Facilitators and ChallengesFacilitators:
• Support from medical & nursing administrators within hospitals• Support from physician colleagues who appreciate help with
heavy patient care demandsy p
Challenges:Diffi lt i l ti li i l di i f th l• Difficulty implementing non-clinical dimensions of the role
• Limitations to scope of practice due to hospital restrictions on NPs’ autonomous ordering and prescribingI i t t t t• Inconsistent team acceptance
• Funding of role
16

CNSs – Facilitators and ChallengesFacilitators: Facilitators:
• Support of health administrators• Increased emphasis on promoting evidence-based practice
Challenges:• Lack of a common vision and understanding of the CNS roleLack of a common vision and understanding of the CNS role• Limited access to CNS-specific graduate education
programs• Lack of title protection or credentialing• Lack of title protection or credentialing
17
N P titi /G l P titiNurse Practitioner/General Practitioner(NP/GP)( )
Primary Health Care Model
Linda Sawchenko, RN, MSHA Regional Practice Leader Interior HealthRegional Practice Leader, Interior Health
18
Interior Health/BC Context• Legislation enacted in 2005 allowing for the introduction of NPs in
British Columbia • Provincial co-ordination including CNOs VPs Medicine Ministry & Provincial co ordination including CNOs, VPs Medicine, Ministry &
College of Registered Nurses BC• Common title, wage scale & scope of practice document
B d NP f ti i l di di i ibi f l• Broad NP scope of practice including diagnosis, prescribing, referral• Dedicated funding to health authorities; however, majority of primary
care provided in fee-for-service (FFS) GP offices
19

Interior Health, British Columbia17 NPs in Rural and Urban Settings17 NPs in Rural and Urban Settings
20
5 Years Later - NP Progress in IH
• 17 family NPs employed in Interior Health1 t NP i th i • 1 acute care NP in thoracic surgery
• 4 NPs in FFS GP PHC Model• 100% retention rate since 2005• Key factor: Community of Practice supportKey factor: Community of Practice support
21
Early Success of NP/GP Collaboration –E d b PHCEnderby PHC
• Ministry of Health Best P ti Practices Innovation AwardAward
22
NP/GP FFS PHC Model• Early success achieved in funded PHC sites• Need identified to build partnerships with FFS physicians and a
call for proposals was sent out to community physicians • Model has health authority funded NPs situated in FFS GP
ffi tioffice practices• NPs provide health care services from a holistic nursing
perspective diagnose and treat acute and chronic illnesses perspective, diagnose and treat acute and chronic illnesses, including prescribing medications
23

NP/GP FFS PHC ModelQualitative Evaluation Findings 2008g
Patient and Physician Satisfaction“Having an NP has increased my access to health care.” (patient)“The GP and NP seem to be in tune with one another – they consult one another to make decisions and they listen to each other and one another to make decisions and they listen to each other and communicate well.” (patient)“This model makes primary health care easier and more p ysustainable.” (physician)
24

Reduced ED Visits/Acute Care AdmissionsAdmissions
“The NP is instrumental in keeping patients out of the hospital and The NP is instrumental in keeping patients out of the hospital and Emergency. I know that because I am no longer driving up to the hospital everyday to see patients – I can go for three weeks without a patient in acute care.” (physician)
25

Patient-Focused Care
“The NP and physician work together with me, I o toget e t e,feel I have more personal control over my care plan and feel like I care plan and feel like I am part of the decision making process.” (patient)
26

Improved Achievement of Chronic Disease Management TargetsDisease Management Targets
“The collaborative approach to • “The collaborative approach to health care has improved results related to the management of chronic diseases, such as diabetes, and their related complications.” (physician)complications. (physician)
27
Priorities/Next Steps
• Celebrate and publish the success of this model• Ongoing knowledge exchange activitiesOngoing knowledge exchange activities• Conduct quantitative research on outcomes related to the
NP/GP FFS PHC model• Expand the model to other communities• Continue to support the NP Community of Practice
28
29
Quebec Neonatal Nurse Practitioners: History and Challenges
Sophie Nadeau, MD, FRCPCMedical Director, McGill University Health Centre NNP Program
Medical Coordinator, NNP Graduate Program
30
Montreal Children’s Hospital
• Early 1990’s: Shortage of residents• 94-96: “Home-made” training program• 97-98: Pilot project accepted by the Collège des
Médecins du Québec• 99-00: MSc Nurs @ Stony Brook U
31

Quebec Government• Bill 90: Nurse practitioners as a distinct profession (2002):
allowed them to– Prescribe diagnostic testsPrescribe diagnostic tests– Perform diagnostic tests that are invasive or place the patient at
risk– Prescribe medications and other substancesPrescribe medications and other substances– Prescribe medical treatments– Perform medical treatments that are invasive or place the patient
at riskat risk
32

Ordre des Infirmiers et Infirmières du Québec-Collège des Médecins du Québec
• OIIQ– Exams and certification
Continuous education– Continuous education
• CMQ– « Règles de soins »: practice boundaries
• Labs• Meds• Techniques
33

McGill University
• MSc Nursing at McGill (NNP stream)Developed in 2002 2003– Developed in 2002-2003
– First students in 2004F ll dit ti i 2008• Full accreditation in 2008
34

Unique Contributions of NNPs• Provision of holistic care to infants and families• Provision of holistic care to infants and families• Co-ordination of care for infants requiring multiple
servicesservices• Facilitation of family communication and support• Provision of interdisciplinary educational opportunitiesp y pp• Education of nurses, nursing students and NNP
students• Education and support of pediatric residents
35
MUHC NNP Role70% li i l ti• 70% clinical time:– Antenatal consultations– Attendance at high-risk deliveries– Attendance at high-risk deliveries– Admission and stabilization of critically ill infants– Completion of history and physical exams– Formulation of clinical impressions – Development, implementation, and evaluation of treatment plans
Discharge planning– Discharge planning– Transport calls
36
MUHC NNP Role• 30% non-clinical time:
– Research– Teaching/education– Administration– Quality improvement/Quality assurance
37

Évaluation de l’implantation du pprogramme d’intéressement au titre d’infirmière praticienne spécialiséed infirmière praticienne spécialisée
Ministère de la Santé et de Services sociaux du QuébecMars 2007
38

Challenges• Integration of the NNP role in the clinical setting
(multidisciplinary)I t t ti f th l i b t i d – Interpretation of the role: in between nursing and medicineCompetition for type of patients procedures etc (RTs – Competition for type of patients, procedures, etc. (RTs, residents)
– Administrative structure of the role: nursing director +/-d s a e s uc u e o e o e u s g d ec o /medical director: lines of communication
39

Challenges• Recruitment of new students/candidates
– Minimal requirements: bachelor degree and 2 years of experience
– “Heavy” Master’s degree training programBursaries during training: not enough to survive– Bursaries during training: not enough to survive
– Level of responsibilities: too elevated– Salary: too lowSalary: too low– No jobs available post-training (no money for recruitment)
40

Challenges• Retention of NNPs
– Heavy workload/not enough colleaguesy g g– Non-clinical time: almost impossible!– Salary: too low for the level of responsibilitiesy p– Unionized position: why?
41

Challenges• Perpetuation of the NNP role
– Lack of students (1-2/year)( y )– Lack of training resources: teachers (both NNPs and
MDs), clinical teaching sites– McGill (anglophone institution)
42

Facilitators: What Can We Improve? (Retention)( )
• Increased role satisfaction– Role diversity, feelings of accomplishment, working in a
challenging environment, cohesive atmosphere• Role expansion
Research teaching education presentation at conferences – Research, teaching, education, presentation at conferences, publications
• Successful transition of NNP studentsSuccessful transition of NNP students• Sufficient compensation ($$$$)
43

Quebec = 7 « Active » NNPs• McGill University (MUHC + JGH)
– MUHC: 4 (+1) NNPsJGH: 0 NNP– JGH: 0 NNP
• Université de Montréal (HSJ + HMR)– HSJ: 3 (+1) NNPs( )– HMR: 0 NNP
• Université de Sherbrooke (CHUS): 0 NNPU i ité L l (CHUL) 0 NNP• Université Laval (CHUL): 0 NNP
44

Clinical Nurse Specialist
Grace Neustaedter, RN, MN, NCACNS Pelvic Floor ClinicCNS, Pelvic Floor Clinic
Calgary, Alberta
45
Objectives
• Identify key practice components of a CNS role• Review background of the CNS role in Canadag• Clarify differences between CNS and NP roles• Review role of CNS in acute care settingsg• Review role of CNS in the Pelvic Floor Clinic in Calgary
46

CNS Role Practice Components (CNA) 1. Direct nursing care – in specialty area2. Clinical consultant – to nurses and other healthcare
professionalsprofessionals3. Educator – to healthcare professionals, students, clients, families,
communitiesf f4. Researcher – developer of research projects, evaluator of care
and program delivery, user of research in program development5. Leader – develops standards, policies, programs of care to meet p , p , p g
needs of specialty population
47
Background of CNS Role in Canada
• CNS emerged in 1970’s as client care grew more complex• Fiscal cutbacks in 80’s and 90’s eliminated many of these Fiscal cutbacks in 80 s and 90 s eliminated many of these
positions• Regaining prominence as concerns build over quality and g g p q y
safety of patient care
48

Differences Between CNS and NP Roles
• Both roles work with multidisciplinary teamsNP f di t ti t h i i h lth ti d th • NP focus - direct patient care emphasizing health promotion and the treatment and management of health conditions; focus is on individual client level
• CNS focus - expert nursing care for specialized client populations; emphasis on development of clinical guidelines and protocols; focus on facilitating system changeon facilitating system change
49
CNS in Practice• Specialty area – in any acute care settingp y y g• Program development – to address needs of their population (e.g.,
education for children with newly diagnosed chronic conditions to stabilize, treat, support families, avoid admission to acute care), , pp , )
• Development of guidelines and policies (e.g., wound care, suctioning, discharge planning – evidence-based guidelines that affect system of care rather than individuals only)care rather than individuals only)
• Working with staff nurses by providing education and support • Research – regularly reviewing current literature and applying to the
setting or population; involved in research activities in own settingsetting or population; involved in research activities in own setting• Consultant – to other organizations or bodies
50
Pelvic Floor Clinic
• 7 nurses, plus CNS• 3 urogynecologists, 2 fellows• Family doctor• 3 physiotherapists• Support staff
51
Development of CNS Role in Clinic
• 1998 – 2 nurses working with 2 physicians(one providing physician support (Grace); one doing (one providing physician support (Grace); one doing urodynamic testing for patients)
• 2000 – Grace began fitting and following patients requiring g g g gpessaries throughout Calgary region (nurse-led clinic)
• Completed Nurse Continence Advisor course (McMaster Uni ersit ) and MN (U of Calgar )University) and MN (U of Calgary)
52
CNS Role in Pelvic Floor Clinic• Formal clinic began in 2002 with fundingg g• Patient Education Workshop introduced by Grace in 2002• Initial assessment clinics by RNs began (in addition to pessary clinics)• Expansion of staff in clinic (more nurses physiotherapists and family • Expansion of staff in clinic (more nurses, physiotherapists and family
doctors); created training and learning modules used to train new staff• More outside requests for workshops, inservices, presentations to
nursing groups (e g UNC) community groups (physician groups) nursing groups (e.g., UNC), community groups (physician groups), seniors groups (LTC homes), pharmacists, public settings, medical resident groups
• Development of clinic processes, protocols and educational resources Development of clinic processes, protocols and educational resources (teaching handouts, brochures, public education)
53
Clinic Progression• More awareness in Calgary, southern Alberta, BC and Saskatchewan• Longer waiting lists (6+ months)
2008 i tt t t h t it li t d b fit ll ti t ll • 2008 – in attempt to shorten wait lists and benefit all patients equally, began teaching 2 workshops per week to most new patients as a required first appointment
• Positive feedback, reduction of wait times, creation of increased availability of appropriate appointments, reduction of unnecessary appointmentspp
54
CNS Role in Pelvic Floor Clinic1. Direct nursing care – 2 days per week of patient clinics, providing
clinical support for other team members as required2 Teaching clinic patients through workshops within Southern Alberta and 2. Teaching clinic patients through workshops within Southern Alberta and
now internationally (using telehealth), teaching other RNs to teach classes
3. (Education and) consultation to family doctors, Ob/Gyn residents, university nursing students, enterostomal therapy students, NCA students, public health nurses, the public, pharmacists, physiotherapists students, public health nurses, the public, pharmacists, physiotherapists (locally, nationally, internationally)
55
CNS Role in Pelvic Floor Clinic4. Nursing Research – publication of research project on readiness
for urodynamic testing forthcoming; currently 3 other nursing research studies being developed; regularly reviewing and research studies being developed; regularly reviewing and implementing current research in clinic
5. Leadership – developing nursing standards for care; reviewing p p g g gand revising clinic processes; improving programs within the clinic and outside by providing consultation
56

Summary
• CNS role – both formal education and experience• Using scientific research, methods, and knowledge to develop
standards and policies• Expert in clinical practice, passes on expertise to other clinicians and to
patientspatients• Role expands and develops to meet the needs within the specialty area• Personal challenge – to get it all done!!
57

CHSRF RoundtableApril 2009April 2009
Representatives:• Policy makers, nursing and medical professional leaders,
regulators, administrators, practitioners, educators
Mandate:• To develop recommendations for policy, practice &
research
58

Recommendations
• Create a vision statement that clearly articulates the value-added role of APNs across settings.
• Establish a pan-Canadian multidisciplinary task force p p yinvolving key stakeholder groups to facilitate the implementation of APN roles.
59
Recommendations
• Consider advanced practice nursing as part of health human resources planning based strategically on population healthcare needs.
• Standardize APN regulatory and educational standards, requirements and processes across the
tcountry.
60

Recommendations
• Include components that address inter-professionalism in undergraduate and post-graduate health professional training programs.
• Develop a communications strategy to disseminate to a wide readership the positive contributions of
d d ti iadvanced practice nursing.
61
Recommendations
• Protect funding support for APN positions and education to ensure stability and sustainability.
• Conduct further research on: • the ‘value-added’ of APN roles• their impact on healthcare costs• the CNS role
62

Next Steps
• Dissemination of APN Decision Support Synthesis and recommendations
• Implementation of recommendationsImplementation of recommendations
63

Dissemination• Special report on CHSRF websitep p• Special issue of Canadian Journal of Nursing Leadership,
Spring 2010 (10 papers)• CHSRF Mythbuster• Organization for Economic Co-operation and Development
(OECD)• ICN INP/APNN Conference in Australia Sept 2010
J i f C di J l f N i R h • June issue of Canadian Journal of Nursing Research on APNs
64

How to ask a question…
- To ask your question verbally, please enter *1 on your telephoneplease enter 1 on your telephone.
- To submit your question in writing please use the “Questions” box on the control panel.

Thank you!F i f ti thi f t For more information on this or future
sessions please visit pwww.chsrf.ca/researcheroncall


















