th EDITION OF DANCE FOR LIFE: A GREAT SUCCESS! · Proofreaders: Geneviève Beauregard Patricia...
12
JANUARY 2012 VOLUME 20, NUMBER 1 Le Groupe Jean-Coutu La Tête Chercheuse Le Ballet théâtral de Montréal THE 5 th EDITION OF DANCE FOR LIFE: A GREAT SUCCESS! The CHSQ presented the 5 th Edition of its benefit show Dance for Life last November 12, at the Gesù Theatre in the heart of Montreal's Quartier des spectacles. Over $25,000 was raised during this gala evening that brought together the principle CHSQ partners, medical personnel from Hemophilia Treatment Centres (HTC), a number of invited guests, some 40 highly talented dancers along with an audience that was thrilled with this wonderful show with actor Martin Laroche as Master of Ceremonies. The CHSQ wishes to thank its partners, volunteers and friends in the public who made this charitable event a great success. § - G.B. Nurses Claudine Amesse (CHU Sainte- Justine), Catherine Sabourin (Montreal Children's Hospital) and Catherine Thibeault (CHU Sainte-Justine). Actor Martin Laroche, Master of Ceremonies for the evening, with Geneviève Beauregard, CHSQ Program Coordinator and instigator of the Dance for Life benefit show. < CHSQ Executive Director, Charles Vanasse, with Louise Couture, Pfizer representative, and Renaud Laporte, representative from Octapharma. CHSQ President, François Laroche, accompanied by former presidents of the organisation: David Page, Patricia Stewart, Mylene D'Fana and Marcel Lafrance. Dancer Alexander Ocampo. < The Suite 19 dance company.
Transcript of th EDITION OF DANCE FOR LIFE: A GREAT SUCCESS! · Proofreaders: Geneviève Beauregard Patricia...

JANUARY 2012VOLUME 20, NUMBER 1
Le Groupe Jean-Coutu
La Tête Chercheuse
Le Ballet théâtralde Montréal
THE 5th EDITION OF DANCE FOR LIFE: A GREAT SUCCESS!
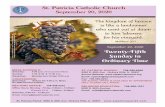
The CHSQ presented the 5th Edition ofits benefit show Dance for Life lastNovember 12, at the Gesù Theatre in theheart of Montreal's Quartier desspectacles.Over $25,000 was raised during this galaevening that brought together theprinciple CHSQ partners, medicalpersonnel from Hemophilia TreatmentCentres (HTC), a number of invited guests,some 40 highly talented dancers alongwith an audience that was thrilled withthis wonderful show with actor MartinLaroche as Master of Ceremonies.The CHSQ wishes to thank its partners,volunteers and friends in the public whomade this charitable event a greatsuccess. § - G.B.
Nurses Claudine Amesse (CHU Sainte-Justine), Catherine Sabourin (MontrealChildren's Hospital) and Catherine Thibeault(CHU Sainte-Justine).
Actor Martin Laroche, Master ofCeremonies for the evening, withGeneviève Beauregard, CHSQ ProgramCoordinator and instigator of the Dancefor Life benefit show.
< CHSQExecutiveDirector,CharlesVanasse, withLouise Couture,Pfizerrepresentative,and RenaudLaporte,representativefromOctapharma.
CHSQ President, François Laroche, accompanied by formerpresidents of the organisation: David Page, Patricia Stewart,Mylene D'Fana and Marcel Lafrance.
Dancer Alexander Ocampo.
< The Suite 19dance company.

2
A WORD FROM THE EDITOR
The year 2012 marks the20th anniversary of the creation ofthe CHSQ newsletter that you'represently reading: L'Écho du facteur.It was in October 1993 that the firstedition of L'Écho du facteur waspublished. The CHSQ ProgramCommittee, whose chair wasPascale Vallée, wanted thecommunity to be able to count ona quarterly information tool thatwould allow us to keep in touchwith members and make them feelpart of the organisation. With thisin mind, I was asked to becomeeditor in chief...and I still am 20years later!The CHSQ had had no officialnewsletter since the publication ofLe Facteur/In Another Vein hadceased in the late 1980s. "Olderpeople" will no doubt rememberthis eight-page newsletter,published in both official languages,whose editor-in-chief was Jean-Pierre Roy.In the meantime, to sendinformation to its members, theCHSQ simply photocopied sheetsof paper that it included in itsmailings under the title: Chapternews.
The first volume included an eight-page French version as well as anEnglish version. For the past 15years, the two versions each have12 pages. The layout, done by a staffperson for the first two years, wassimple enough, but has been refinedthanks to technological advancesover the years. In fact, its an ongoingchallenge to keep the newsletterattractive and pleasant to read,while meeting our members' needfor information.As usual, I'd like to invite you all,but especially during this20th anniversary year of ournewsletter, to send us yourimpressions of L'Écho du facteur, totell us about any articles thatparticularly touched you or caughtyour attention, or to send us anycomments that could help usimprove the content or look of ournewsletter. It's important that thenewsletter properly reflects yourneeds and preoccupations since it'sspecifically for you.Thanks for your loyalty in readingus; we're on our way towardsanother twenty years!Finally, I'd like to take theopportunity with this first editionfor the year 2012 to wish you allhealth, happiness and success. §
SUMMARY
EDITORIALSTAFFEditor:François LarocheContributors:Geneviève BeauregardSébastien BédardAnna BizunoviczMylene D’FanaLisa-Marie MathieuClaude MeilleurCatherine SabourinPatricia StewartCharles VanasseProofreaders:Geneviève BeauregardPatricia StewartCharles VanassePage Layout:François LarocheTranslation:Patricia Stewart
The 5th Editionof Dance for Life:A great success! 1
A Word from the Editor 2
Editorial 3For you, with you!
CHSQ Activities 4 & 5Building the coming year 2012on solid ground!
Rare Bleeding Disorders’Corner 6 & 7Living with severefactor XIII deficiency
Hemophilia TreatmentCentres’ Corner 8 & 9Pain control in hemophilia
Parents’ Corner 9The story of little Jaëlle
Inhibitors’ Corner 10A suggested reading
The WFH 7th GlobalForum 11 & 12On the safety and supplyof treatment productsfor bleeding disorders
In a Word 12
byFrançois Laroche
The opinions expressed in the various columns are those of the authors and do notnecessarily represent the viewpoint of the CHSQ.To let us know your comments or to give your opinion on any related topics,send your text to the following address:L'Écho du facteur, CHSQ, 1102-2120, Sherbrooke Street EastMontreal, Quebec H2K 1C3Telephone: 514-848-0666 or 1-877-870-0666Fax: 514-904-2253or by e-mail to the followingaddress: [email protected]: www.hemophilia.ca
• L’Écho du facteur is a newsletter producedby the Quebec Chapter of the CanadianHemophilia Society and is distributed threetimes a year to its members.Circulation: 250 in French, 100 in EnglishLegal deposit: Bibliothèque nationale duQuébec, 2012.

3
EDITORIAL
The CHSQ is a reliable sourceof documents and informationVia its website and its telephoneinformation service, CHSQ can leadyou to the right information andresources concerning any questionabout how to deal with your disease.CHSQ also offers you our newsletter,L'Écho du facteur, as well as periodicinfo-letters that give you informationabout our activities and a variety oftopics that may be of interest to you.
The CHSQ is a partner that caresabout making your life aspleasant as possibleActivities are for all, either simplyfor pleasure or educational, and aredefinitely an opportunity to meeteach other: annual CHSQ familyweekend (for the whole family), mini-camp for children with inhibitors,the 41st annual CHSQ Summer Camp(5 to 15 year-olds), youth activities(14 to 25 year-olds), father-sonactivities, volunteer appreciationactivities, etc. This program ofactivities is spread out over the yearin order to increase your chances tomeet and share.
The CHSQ is a good resourcefor those who have questionsPsychological support with a healthprofessional, help for adolescents intheir career choice, collegial anduniversity scholarships and bursaries,direct financial aide, specificinformation workshops for variousbleeding disorders, informationmeetings for carriers mothers,mentorships and meetings for newlydiagnosed families, etc. Ourorganisation is constantly workingto help support people living with arare bleeding disorder who, at times,require a bit of support or comfort.
The CHSQ is on the front lineto protect your rights and theblood supplyOur organisation delegatesrepresentatives chosen from our
The Canadian HemophiliaSociety-Quebec Chapter (CHSQ)is a public health non-governmentorganisation (NGO) that plays anintegral role in accompanying andsupporting some 60,000Quebecers living with a hereditarybleeding disorder, as well as thoseinfected with HIV and hepatitis Cduring the contaminated bloodscandal. Assistance, support andpublic awareness are at the heartof our organisation's mission. Thismission becomes reality throughthe participation of people inactivities that the CHSQ offers. Thegoal of these activities is to meetthe needs expressed by CHSQmembers and to allow them togather and share with othersaffected by these diseases.
The CHSQ offers people living withan inherited bleeding disorder, aswell as their families and relatives,made-to-measure activities thatpromote improved knowledge andbetter management of theirconditions. The activities we offerare developed by a team ofprofessionals accompanied bymany volunteers whose sole desireis to improve their quality of lifeas well as that of their peers. It'sin this spirit of cooperation andfraternity that I'd like to invite you,as the Executive Director of CHSQ,to join our organisation andparticipate, along with all membersand volunteers, in the variousactivities proposed for you duringthe coming year, 2012.
members to sit on the boards ofcommittees related to themanagement of the blood systemin Quebec and Canada. Others aredesigned to ensure constantvigilance in defence of the rightsof people living with a bleedingdisorder. And finally, our membershave the opportunity to participatein international exchanges thatoccur during twinning programscreated by the World Federation ofHemophilia (WFH) or duringinternational congresses devotedto bleeding disorders.
The CHSQ brings hope tothose living with a rarebleeding disorderThrough its public awarenessactivities about bleeding disordersand von Willebrand disease,amongst others, the CHSQeducates the public and health careprofessionals about the specificsof these diseases. In order toaccomplish this, the CHSQorganizes public meetings withtargeted groups and ensures acontinuous presence on the socialnetwork. The CHSQ also instigatesvarious public relation activitiesand fundraising campaigns thatallow our organisation to be seenand to promote the importancethat must be given to research onbleeding disorders. The benefitshow Dance for Life is at the heartof this awareness and fundingwork.
This is a brief overview of ourprogramming activities for 2012.The complete program (descriptionof the activities, dates, locations,registration, useful references, etc.)will be published in a documentand distributed in February to allreaders of L'Écho du facteur andwill also be available at alltreatment centres.
All that's left is for you to registerand participate!I wish you all a great year in 2012. §
For you, with you!
byCharles VanasseExecutive Director

4
Review of the final 2011activities
Mini-camp for children livingwith inhibitorsThe CHSQ organized its first mini-camp for children with inhibitorslast October. A real challenge since,for the first time, the kids wereseparated from their parents for afull three days. With a teamcomprised of two nurses, our campdirector and volunteer, as well asthe program coordinator, sevenwell-supervised youngsters got achance to spend a weekendamongst themselves, withoutparents. A unique experience forthese youngsters who were able todevelop their sense of autonomyeven more.The mini-camp was held in abucolic setting in the EasternTownships, in an inn located at thefoot of Mount Orford. As soon asthe young campers arrived, theircomplicity began...greetings, smiles,the joy of being together, it was allvery magical!During the weekend, the campersworked on creating a short videoin "stop motion", an activity thatwas highly appreciated. They all gotto swim in the pool, and a filmshown on a giant screen and hotpopcorn awaited them in theevening. Mornings were spentlearning self-infusion, which was
CHSQ ACTIVITIES
A new wind is blowing throughour organisation and it's on a solidbase, already achieved over theyears, that the CHSQ will continueto build its future. As for me, Icouldn't be more motivated tocontinue my work at the heart ofthis great organisation.The year 2011 allowed us toimprove many of our activities andstrengthen the basics for some newprojects. As far as I'm concerned,2011 was a year filled with emotionand it was great to spend time withyou during our activities where youalways participated in largenumbers. I'd like to share thesuccess of our 2011 projects withyou. Bravo and thanks!I'd also like to take advantage ofthis opportunity to wish all of you,dear readers, a wonderful 2012! Apromising new year during whichthe CHSQ is planning a program ofactivities to meet your needs!
byGeneviève BeauregardProgramCoordinator
Of course, before everyone managedto fall asleep, there was a lot oflaughter and whispering, despite afew comments from the monitorsfor them to close their eyes andsleep.During the weekend, parents stayedin a second inn located a few metersfrom the place where the youngsterswere. They could take advantage ofthis well-earned respite as well astake part in a workshop offered byClaude Meilleur, nurse coordinatorfrom the Quebec Centre forCoagulation Inhibitors.Finally, when it came time to leave,one youngster was thespokesperson for the group ofcampers and told us how much heand the others adored theirexperience. The only glitch,according to them: the mini-campwas too short! "We need at leastfour or five days!", they allproclaimed as one. The mini-campfor children affected by inhibitors,an experience that each one of themhopes to relive!I'd like to thank Claude Meilleur andher colleague, Amélie Laroche-Provencher, nurse coordinator fromthe HTC in Sherbrooke, who tookthe time to come in order to give usa precious helping hand. Thanksalso to Maxime Lacasse Germainwho worked as director of our mini-camp and Yanick Massicote whokept the children busy during theweekend. And, of course, a heartfeltthanks to our financial partners whomade this activity possible. Thanksgo to all of you!
Appreciation evening for CHSQvolunteers and employeesThe CHSQ recognized and thankedits numerous volunteers during anannual appreciation evening thattook place at the Auberge Handfieldin Saint-Marc-sur-le-Richelieu lastDecember 4. The CHSQ took thisopportunity to thank the manyvolunteers who actively participatein the realisation of our variousprojects.It goes without saying that in anorganisation such as ours, theirinvolvement is essential for thesuccess of our activities.
very beneficialfor all of them.They were soproud to learnand succeed.Personally, Ithink the mostbeautifulmoments werewhen it wastime for bed.The youngstersshared a largecommon roomand it was funto see them alltogether,wishing eachother goodnight andsweet dreams.
Building the coming year 2012 on solid ground!
Participants in the mini-camp for youngsters living with inhibitors gatheredat the Auberge Orford, in the Eastern Townships

5
The revellers were served a copiousmeal, and games and a giftexchange were part of this lovelyevening. Once again, thanks to allthose who are always available togive us a much appreciated helpinghand!
The CHSQ Bowl-a-thonsThis fundraising event is, withoutdoubt, a favourite with many sinceit brings out hundreds of volunteersand participants across Quebec.During 2011, five Bowl-a-thonswere organized in as many regionsthanks to the initiative of localvolunteer committees. Bowl-a-thons were organized in Montreal,on Montreal's South Shore, inContrecoeur and Sorel-Tracy. Thefinal one took place October 30, inSaint-Georges-de-Beauce andbrought out over 80 participants,some in costume on this Halloweeneve. An enjoyable activity forparticipants who won a number ofdoor prizes. Bravo!The five Bowl-a-thons allowed usto raise a total of $20,000, thanksto the financial support of CHSQpartners as well as local sponsorswho all showed a lot of interest in
David Pouliot and Marius Foltea(Montreal), Sylvie Bouchard(Contrecoeur) along with IsabelleBlette and Patrick Raymond (Sorel-Tracy). Thanks to all of you for youravailability and your talents asorganizers. A great team!It's time to start preparing the nextBowl-a-thons for the year 2012. Bymultiplying the number of regionsthat participate, we can make evenmore people aware of the cause ofhemophilia and other bleedingdisorders. It's easy to organize thisactivity and the CHSQ willaccompany you throughout theprocess. If you'd also like tocollaborate on this financialinitiative and organize a Bowl-a-thon in your area, contactGeneviève Beauregard at the CHSQoffice (514 848-0666 local 21) rightaway, so that we can tell you howthe process works. Thanks!
A brief overview of upcoming2012 activities at the CHSQCHSQ 2012 annual familyweekendA place for the whole family to gettogether! The CHSQ 2012 annual
offers a family weekend for allfamilies affected by hemophilia oranother rare bleeding disorder aswell as people infected with HIVand/or hepatitis C from acontaminated blood product. Thisannual weekend is offered tofamilies to allow those who so wishto meet and discuss with otherfamilies who are CHSQ members.The program for the CHSQ weekendincludes information workshops,meetings and discussions as well asgames and outdoor activities. TheCHSQ also takes advantage of thisgathering to hold the annual generalmeeting with its members. Toparticipate in this activity, simplycomplete the registration form andreturn it to the CHSQ office (theregistration form is available on theCHSQ website). Check your emailsand visit our website regularly tofind out more about this activity orsimply contact GenevièveBeauregard at 514-848-0666,local 21.
Women's weekendThe weekend reserved for womenliving with a bleeding disorder willtake place in Winter of 2012. Thisactivity will provide mothers whoare carriers as well as those affectedby a bleeding disorder a break anda chance to meet and discuss whatthey experience, in the company ofhealth care professionals and otherwomen with the samepreoccupations.The CHSQ is finalizing preparationsfor this activity. We'll send you thefinal information as well as theregistration form in the first fewweeks of 2012.
Help wanted
Assistant-counsellors for theCHSQ summer campThe CHSQ is looking for youngpeople aged 16 and up who'd liketo live an extraordinary summerexperience by participating in theCHSQ annual summer camp as anassistant-counsellor. If this challengeinterests you, contact GenevièveBeauregard right away at the CHSQoffice (514-848-0666, local 21 or1-877-870-0666, local 21) in orderto submit your candidature.A complete training session is givento assistant-counsellors before campoccurs. §
CHSQ ACTIVITIES (cont’d)our cause. Thankyou! This activitywouldn't havebeen as successfulif we hadn't beenable to count onthe initiatives ofthe followingpeople: Lisa-MarieMathieu (Beauce),Karine Perrier(Montreal SouthShore), MaximeLacasse Germain,The CHSQ volunteer and staff recognition evening.
weekend will beheld March 16,17and 18 at thevacation centre LaJouvence in themountains andforests of theAppalachians nearMount Orford inthe EasternTownships.This key activity forour organisation
< Lisa-Marie Mathieu wasvery happy with the resultsof the Bowl-a-thon inSaint-Georges-de-Beauce.

6
RARE BLEEDING DISORDERS’ CORNERLiving with severe factor XIII deficiency
a great deal of anxiety. Despite itall, my parents decided to haveanother child, my brother Nicolas,born 3 years after me, who didn'thave this disease.Throughout my childhood, I visitedthe emergency room about twicea year, mainly for hematomas, butalso for other types of bleeds thatoften appeared long after an injury.My early years were spent in a veryprotective environment where mymother took all possible means toensure my safety. My startingschool was difficult for her since,for the first time in his life, her littleSébastien wouldn't be under herprotection...so I needed a MedicAlert bracelet and I had to tell allmy friends and the people at schoolthat little Sébastien was a factorXIII hemophiliac and that if anaccident happened, they had to....My mother became so protectivethat she literally suffocated me.Aware of the effect of her actionson my development, she decidedto have my father manage my case,because it was too hard for her. Myfather preferred to see me happy,so I could do everything my friendsdid, or almost, “on condition that Ibe careful”.It was a liberation for me, and I wasallowed to play sports that eventhe hematologist didn't agree with.I was aware that I was more fragilethan the others and so I had toanticipate potential hits in order toavoid them. It's as if my father hadsigned a pact with me by saying:“You can play with your friends, aslong as you don't get hurt”.
It all began May 26, 1978 at4:40 p.m. when I was born at theChrist-Roi Hospital in Quebec City.The pregnancy, like the birth, wentwell. All the usual first testsindicated that I was in perfecthealth.However, on the morning ofMay 28, the first symptoms beganto appear: baby was pale, crying,had a drop in hemoglobin,jaundiced and the doctor felt amass on the right side of myabdomen. By afternoon, I wastransferred to CHUL and from thatmoment on began a long period ofworry and anxiety for my parents.In the following weeks, my statedidn't improve much. I had bleedsfrom the navel and the mass onmy right side continued to worrythe specialists. I had a number ofblood transfusions that wereinjected directly into my scalp.There was one doctor after anothertrying to find the source of all theseproblems. Theories changed fromday to day until, at the age of 3weeks, all the specialists werepersuaded that I should havesurgery to remove the mass thatmust be a tumour, according tothem. My parents suffered terribly,especially my mother, so much sothat she asked the priest to giveme extreme unction because, inher mind, a tumour meant death.She braced herself to lose the childthat had grown inside her.On June 21, the surgeon proceededto operate. In the recovery room,my parents found their son with ascar 20 cm long on his stomach. Itwasn't a tumour, but an intra-abdominal hemorrhage locatedbetween the liver and the right
kidney. The decision was clear —I suffered from 'a hemorrhagicsyndrome' whose etiologie escapedthe doctors.And yet, this theory had alreadybeen proposed before surgery, butall blood tests showed thatcoagulation was “normal”. Whatthis meant is that these tests couldmeasure the time for a clot to form,but in the case of a deficiency infactor XIII, the time to form a clotis normal. In the absence of factorXIII, the bleeding happens after theclot has formed because the fibrinchains that form the clot rapidlybreak down and bleeding follows.From this time on, my case wasconfined to a young hematologist,Dr. Louis Desjardins. He sent bloodsamples from both my parents andme to Dr. Jack Hirsh at McMasterand it was there that the finaldiagnosis was made. I sufferedfrom severe factor XIII deficiencysub unit A and my parents wereboth carriers.Dr. Desjardins explained to myparents that this was an extremelyrare disease, that little was knownabout it and that I was the first casehe'd seen in his life, which wasn'tvery reassuring for my parents(2011: 31 severe cases arediagnosed in Canada).Soon after, cryoprecipitate wasused to treat my bleeds and I wasdischarged from the hospital atabout 6 weeks of age. My parentsleft the hospital with manyunanswered questions, with noreference points, with little scientificinformation and, most of all, with
bySébastien Bédard
Sébastien, about three months old. The scar from surgery is highly visible (on left).

7
Looking back, I realize that I wasfairly lucky: I only visited the ER afew times for injuries that didn'tleave any serious consequences.As a child, only physical painaffected me. With the arrival ofadolescence, this suffering wastransformed little by little intopsychological pain.In November 1991, having had ablow to my thigh, I had anintramuscular bleed that requireda few days of hospitalisation.During this stay, I was infused withplasma to cure the bleed and, inthe wake of the contaminatedblood scandal, the hematologistannounced the need to be testedfor HIV and hepatitis viruses, sinceI had been exposed to these viruseswhen I'd received a number ofblood products. My mother thenasked the hematologist what thechances were. I remember the lookon his face. He lowered his eyesand, looking at the ground said,“He's been exposed, I don't know.”At that precise moment, I can tellyou that the psychological sufferingwas horrible and waiting for theresults was interminable and veryfrightening.About two months went by beforeI was called to meet thehematologist in his office. He finallyannounced that I hadn't beencontaminated with HIV nor anyhepatitis virus and the fact that
I had opted not to haveprophylactic treatment hadprobably contributed to the results.This was a second liberation. WhenI look back, I compare this sufferingto that which my parents hadexperienced at my birth waitingfor the diagnosis.A while after this event, during thecontaminated blood scandal thatexploded in the media, peopleoften associated hemophilia withAIDS. At school, some classmateswho remembered that I hadhemophilia wrote “AIDS” in myagenda or on my locker and someasked me if I had AIDS. I washelpless and defenceless whenfaced with all this. It was a verysad time in my life where I tried toimagine what kind of life I wouldhave as an adult...a spouse, work,health...At this precise moment, I wouldlike to have known or metsomeone suffering with the samedisease as me. I was completelylost. I can sum up this period inone word: ISOLATION. From thenon, knowing human nature, thisdisease was going to become mysecret, no one would ever know...In 1995, I was transferred to theHemophilia Treatment Centre inSaint-Sacrement Hospital. Rightfrom my first meeting withDr. Jobin, prophylactic treatmentwas started with factor XIII
concentrates (Fibrogammin P®) inorder to prevent spontaneousintracranial hemorrhages, whichare the main risk for peoplesuffering with severe factor XIIIdeficiency. He explained that aninjection of 1000 units every 4weeks would be sufficient since thehalf-life of factor XIII is extremelylong. This new treatment eliminatedalmost all the physical symptomsof my disease. I kind of fell into acertain denial, sometimes evenforgetting about the disease.After that, I completed my studies,met my present wife and foundeda lovely little family. My two childrendon't have the disease, but they arecarriers. Today, I have a life that I'dqualify as normal and happy.In 2008, I was introduced to theextended family of the CanadianHemophilia Society during aworkshop for people suffering withrare bleeding disorders. Thismeeting has changed my life byallowing me to come out of myisolation, which has helped me healmany old wounds from the past andto finally accept my disease. For thefirst time in my life, through theCHSQ, I've met another personliving with the same bleedingdisorder as me, a young girl inQuebec.Since then, I've gotten involved inthis great organisation in order tohelp people break their isolation. §
RARE BLEEDING DISORDERS’ CORNER (cont’d)
IN MEMORIAMThe CHSQ was saddened to learnof the passing of Denis Durocherwho died on November 26th, at theage of 71.Denis served as treasurer on ourBoard of Directors for twoconsecutive mandates, from 2007to 2011. His availability and theskills that he brought to the serviceof the CHSQ during those four yearsas treasurer were greatlyappreciated. But even more thanthis, Denis Durocher, a member of
the organisation for over 20 years,was highly involved in a numberof activities (programs andfundraising) over the years, alongwith his wife, Céline Durocher.The CHSQ is grateful for all hishelp over the years.The CHSQ wishes to express itssincere condolences to Denis' wife,Céline Leclerc, to his son Gaétan(Vivian Fortier), his daughterGuylaine (Serge Aubin), hisgranddaughter Sabrina, his
grandson Edgar, and to all hisbrothers, sisters, in-laws, familyand friends.Denis graciously requested thatpeople show their sympathy bymaking a donation to the CHSQ. §
- F.L.

8
have been on prophylaxis since infancy canhope for a life without chronic joint pain.
How is pain measured?Since pain is a subjective and invisibleexperience, there is no machine to give aunit of measurement. With acute pain,changes in other vital signs can be noticed:increase in heart rate, respiration and bloodpressure. However, these changes are notnecessarily always present with pain.Communication with your medical team isthe key. Health professionals use pain scalesin order to measure pain level:• Numeric Rating Scale: You must choosea number from 0 to 10 to indicate howstrong your pain is right now. 0 being nopain at all and 10 being the worst amountof pain you've ever had or you could everimagine.• Visual Analog Scale: You are askedto put a mark on a line to showhow strong your pain is right now."No pain at all _________________ The worstpain imaginable"• Category Scale: You must choose a wordthat best describes how your pain feels rightnow. Mild-Discomforting-Distressing-Horrible-Excruciating• Faces Scale: Used by professionals forpain assessment before the age of 3-5 yearsold. Facial expressions are used as a wayto quantify pain.Describing your pain is important: is itburning, throbbing, feels like pins andneedles, etc. What makes it worse, whatmakes is better, does it go down with theinfusion of factor? It is also very importantthat the limitations that pain imposes onnormal activities such as work and sleepbe communicated to your healthprofessional. Pain control will have as agoal the return to your activities of dailyliving with little or no pain.In young children, pain assessment will bedone by observing the child for thefollowing: anxiety, agitation, restlessness,crying and inconsolability. Less intense paincan be manifested by withdrawal anddecreased activity. Parents must reportchange of behaviour to the health carepersonnel. Even if the pain is mild, it shouldbe managed.
What pain medications are best?The choice of pain medication and itsdosage will vary depending on the type andintensity of the pain. The prescribing doctorwill choose a medication and dosage thatwill give the best pain control with the leastside effects as possible. Again, there is norecipe and no one's pain fits the samemould.• Acetaminophen (Tylenol®, Tempra®):This common over-the-counter medicationcan be safely used in mild cases of pain. Itcan be taken every 4-6 hours with amaximum of 5 doses per day. Individualswith compromised liver function shoulddiscuss acetaminophen use with their liverspecialist.
For individuals living with hemophiliaand other bleeding disorders, pain relatedto the disease is a negative experience thatneeds attention. Referred as the fifth vitalsign, pain needs to be evaluated andtreated by your hemophilia health careprofessionals. Here is a brief introductionto pain evaluation and management. Thisinformation has been taken from the CHSpublication Pain the Fifth Vital Sign: AResource on Managing Pain for People withBleeding Disorders. Should you wish tolearn more about pain, I encourage you torequest a copy of this book at your nextHTC visit.
What is pain?According to the International Associationfor the Study of Pain, pain is "an unpleasantsensory and emotional experienceassociated with actual or potential tissuedamage, or described in terms of suchdamage". Pain is subjective, meaning thatindividuals will experience pain differently.Therefore, pain needs to be assessed in anapproach of individualizing the treatmentplan. Nobody's pain fits in the same mould.
What causes pain in hemophilia?Pain in hemophilia can be sorted into twocategories: acute and chronic.Acute means "something new is causingthis". A new joint or muscle bleed is causingdamage to the body and pain is the body'sway of telling you something is wrong.The blood has accumulated in the jointspace or between the muscle fibres andthe pressure and inflammatory reaction ofthe body are why pain is experienced. Paincan often be the first sign of a bleed. Paincontrol, with the infusions of adequateamount of factor and rest, will be used fora limited period of time as this type of painwill stop when the bleed is resolved.Chronic pain in haemophilia is pain thatpersists in the joint well after bleeding hassubsided. With repeated bleeds in the samejoint, destruction of the cartilage tissueand chronic inflammation creates asituation where pain can be felt daily andinterfere with activities. This is calledhemophiliac arthropathy. Quality of lifecan be greatly affected. Quick treatmentof bleeds with factor infusions is the wayto avoid joint damage and the ensuingchronic pain. Those who have severebleeding disorders will benefit fromprophylaxis and many young people who
HEMOPHILIA TREATMENT CENTRES’ CORNERPain control in hemophilia
• Celecoxib (Celebrex®):A Non-Steroidal Anti-Inflammatory (NSAID)that won't cause further bleeding risk inpeople with bleeding disorders as it doesn'taffect platelet function like other NSAID's. This seems to be the drug of choice for themanagement of chronic pain due tohemophiliac arthropathy. It can be takenonce daily or can be split into two dosesgiven in the morning and in the evening.Risks include gastrointestinal bleeding.• Opioids (Codeine, Morphine,Hydromorphone and others):A class of medication that relieves pain byacting directly on the central nervoussystem. This can be adequately used totreat chronic and acute pain. Many formsexist and different opioids will be used indifferent pain experiences. Side effectsinclude nausea and vomiting, sleepiness,constipation, itchiness, tolerance anddepression. These side effects can be scarybut a careful selection of the medicine andits dosage, with ongoing communicationwith your doctor, can make pain controlwith opioids a positive experience. Thereis a fear of addiction to opioids since thereis a known side effect of euphoria, however,many studies have proven that whenopioids are used as prescribed in a situationof pain, the chance of addiction is very low.If pain persists despite taking the medicationas prescribed, call your doctor. Short-termuse of opioids for an acute bleed or aftersurgery is very unlikely to lead to addiction.
What medications should beavoided?People with bleeding disorders must nottake Aspirin® as it "thins the blood" bysignificantly affecting platelet function.Usage of NSAID's such as Ibuprofen (Advil®,Motrin®) and Naproxen (Anaprox®, Aleve®)are also to be avoided.
How can physio help?Your physiotherapist is your joint expert.He or she will be involved in the assessmentof your joint and in the treatment plan tocontrol pain. The treatment plan will, again,depend on each individual case and willdiffer with the type of pain (chronic vsacute). An exercise and fitness programcan also help control pain and potentiallyprevent some pain.• Muscle Strength: stronger muscles willbetter support and protect your joint.• Range of Motion: better mobility willbring better alignment of the joint andreduce stiffness.• Flexibility: joint and muscle contracturescan cause pain that will decrease withstretching exercises.• Coordination and balance: improvementof these skills will help you respond quicklyto sudden movement and therefore avoidmore bleeding.• Weight Loss: cardio-vascular exercisescan make you lose weight that will translateinto less stress on your lower-body joints.
byCatherine SabourinNurse CoordinatorHemophiliaTreatment CentreMUHC MontrealChildren’s Hospital

9
PARENTS’ CORNER
The holiday season is already over andwe got to see the smiles and joy on ourlittle ones' faces when they opened theirgifts. In my case, it's a happy time, yes, butalso synonymous with difficult momentsthat happened eight years ago.It was actually two days before Christmas,in 2003, that our son was tested to verifythe factor VIII levels in his blood. A fewdays beforehand, we'd found numerousbruises on his body, a sign that there wassomething wrong. In fact, on January 4,2004, we got the diagnosis: our son hadsevere hemophilia A.I'm reminded of this time because, duringthe last check-up with our children, I gotto meet a family from Sept-Îles in thewaiting room and their story brought backDylan's diagnosis. While talking with thembetween two appointments, I learned thatJaëlle, the pretty little princess calmly sittingin her carriage, was also part of theextended hemophilia family and, despiteher young age, had already lived througha number of difficulties.I'll let her mother, Isabelle, tell their story...
***
Jaëlle was only 4 days old when I noticedthat she was bleeding from her navel, butI was told it was normal. When I got uptwo days later, I was terrified: her diaperwas filled with blood and there was a largemass of blood around her navel.Then, four days later, we were dischargedafter lunch. The afternoon went well.Around 4 p.m. on the same day, it startedbleeding again! What a panic! We returnedto the emergency room at the hospital and
After that, we went to the hospital every twoweeks for blood tests and her factor XIII levelwas established at 8%. She was declared amild hemophiliac!From 10 days of age to 15 and a half months,all was well. She had started walking. Thenightmare returned on October 22, 2008.That morning, we got up, got ready to go towork; the daily routine. I put Jaëlle on thefloor to get myself ready and, instead ofsticking to me like glue as she usually did,she stayed curled up where she was. WhenI tried to dress her, I couldn't lift her left arm.I fed her breakfast and her left hand wouldn'topen. I said to my husband, “Come on, we'regoing to the hospital. Something's not right!”.While we were waiting to see a doctor, herstate deteriorated: she had facial spasms andher left leg was weakening. At first, thedoctors thought it was epilepsy. She had anelectro-encephalogram and they realizedthat something was wrong. Then they didan emergency scan (tomodensiometer) andtold us that the little one was having aspontaneous cerebral hemorrhage and thatit had led to paralysis! OUF! What a shock!She was transferred to emergency at theCHUL - Mother-Child Centre in Quebec Citywhere we stayed for a week.That's where our little princess wasdiagnosed with severe factor XIII deficiency.Since then, she gets two vials ofFibrogammin P® every three weeks and shehas blood tests after every fourth treatment.What's more, she's developed inhibitors. Buttoday, she's 4 1/2 years old, she's doing welland responding well to treatment. A realchampion.
***
I want to thank Isabelle for generouslyagreeing to share this difficult period in theirlives with us. As I mentioned, I got to meetthem and I can assure you Jaëlle ismagnificent! A pretty little princess who hasalready been through so much! Accordingto Isabelle, Jaëlle is doing well and, with hertreatment, can live like any four and halfyear-old girl.Following this very touching text, I'll end bywishing you all a happy 2012. May you enjoyhealth and may your dearest wishes cometrue! §
byLisa-Marie Mathieu
The story of little Jaëlle
LittleJaëllein hermotherIsabelle'sarmsalongwith herfather,Martin.
that was very hard:the little one'shemoglobin was at58 and she had tohave a bloodtransfusion. I thankGod it didn'thappen during thenight.After that, shestopped bleeding.The pediatricianchecked with thehematologists inQuebec to confirmwhat he thought:Jaëlle had factor XIIIdeficiency.
And remember that exercise releasesendorphins which are the body's feel-good chemicals known to decrease pain!
Are there surgical options formy pain?In some cases of advanced arthropathy,orthopaedic surgery will diminish pain. Joint replacement surgery will restorejoint function and greatly diminish pain.Other surgical procedures to the jointcan also significantly decrease pain.Synovectomy, the removal of synovialtissue, either surgically or by injectionof a radioactive isotope, can diminishthe pain of synovitis or repeated bleedsin a target joint. Surgical options canfirst be discussed with yourphysiotherapist.
What can the social worker add?Pain can disrupt your personal andprofessional life. The social worker atyour HTC can assist you in thosecomplications. For example, the socialworker will ensure that you receive allmonetary assistance that you are eligiblefor and support you in communicatingyour needs with a school or employer.
And what about my nurse?The hemophilia nurse's role in themanagement of your pain is to ensurethat you receive all the attention andcare that is needed. The nurse willinitiate the pain assessment and sharethe information with the other membersof the team, encouraging you to beproactive in achieving pain control.Bleed diaries will be reviewed by yournurse to look for adequate usage offactor for bleeds and bleeding patterns.The nurse will discuss her findings withthe hematologist and physiotherapist inorder to achieve as little bleeding, andpain, as possible.
What to do when I feel that mypain is being ignored?Speak and be heard. Often, you will findthat your health professional has simplyneglected to discuss the issue with youand will be happy to work with you toachieve pain control. If after discussingthe details of your pain you find yourselfin a situation where you don't agreewith the pain management plan, calmlyexpress your feelings. If all else fails,request a referral for a second opinion.
The vision of the Canadian HemophiliaSociety is a world free of the pain andsuffering of inherited bleeding disorders.Until a cure is found, pain willunfortunately continue to beexperienced. Thanks to the success ofprophylaxis, chronic pain is largelyavoided by the younger generation ofseverely affected people with bleedingdisorders. Those suffering fromarthropathy deserve individualized painmanagement treatment plans. §
HTCs’ CORNER(cont’d)

10
Hello everyone,
I'd like to give you a brief resumeof a chapter that recently appearedthis year in Current and FutureIssues in Hemophilia Care entitledPhysiotherapy Evaluation andIntervention in AcuteHemarthrosis: Challenging theParadigm.
This interesting chapter was, infact, written in part by one of ourcolleagues who is a physiotherapistat CHU Sainte-Justine, Mr. NichanZourikian.
We all know that physiotherapistshave an important role to play inthe prevention of joint bleeds(hemarthrosis) and in joint recoveryfollowing a bleed. The importanceof evaluation and re-evaluation inorder to modify treatment for apatient are major keys to thesuccess of the treatment.
In order tooffer qualitycare andservices,Mr. Zourikianand hiscolleague,Ms AngelaForsyth,questionedpresentmethods usedby teams athemophiliatreatmentcentres (HTC).During thisprocess, thefirst point thatbecameevident tothem was thenecessity ofverifying andvalidating
information gathered from literaryresearch but also by developingresearch in their own field.
In this article, they were taken withtwo specific recommendations: theuse of ice and rest in hemophiliapatients having a joint bleed. Whilethe initial treatment for ahemarthrosis in hemophiliapatients is the administration of themissing coagulation product,certain actions must occur at thesame time, these being Rest, theapplication of Ice, Compression andElevation of the affected member(RICE).
The main objective of ourprofessionals was to stimulatereflexion, based on conclusiveevidence and data surroundingcurrent recommendations on theuse of ice and rest during the acutestage of a hemarthrosis inhemophiliacs. In fact, do theserecommendations, borrowed fromtreatment administered to athletesor the general public, really meetthe needs of hemophiliacs?
For example, studies suggest thatcold prolongs bleeding time andlowers platelet aggregation, whichcompromises coagulation. Thiscould actually prolong post-injurybleeding in the joint.
Scientific literature shows that theaccumulation of blood in joints hasnegative effects on the cartilageand synovium.
Our colleagues concluded withrecommending the use of acompression bandage andelevation of the injured area tocontrol and lessen swelling,especially in situations followinginjury where coagulation factor hasnot yet been infused. If the painpersists, the use of a TENS(transcutaneous neurostimulator)or anti-inflammatory medicationprescribed by a doctor may help.
Following this, the physiotherapistsdealt with the second variablewhich is Rest versus a quick returnto walking, running or any otherphysical activity.
Studies suggest
that cold
prolongs
bleeding time
and lowers
platelet
aggregation,
which
compromises
coagulation.
This could
actually prolong
post-injury
bleeding in the
joint.
INHIBITORS’ CORNERA suggested reading
byClaude Meilleur, Pivot NurseQuebec Reference Centre for Patientswith [email protected]
They concluded that prolonged restcan cause, amongst other things,muscular atrophy and thecontraction of muscles. However, aprecocious return to daily activitiescan provoke a new bleed in a joint.The acceleratedreturn tomovement in ahemophiliapatient can alsoprovoke chronicsynovitis, atarget joint,damage to thecartilage, a newbleed and,eventually,hemophilicarthropathy.
It is thereforevery importantfor thephysiotherapistto establishproperevaluation of thehemarthrosisand joint health,as well as doinga follow-up of itsevolution until itis resolved. Thisis to maintain an adequate balancebetween rest and resumption ofactivity, while trying to diminishrepeat hemarthrosis or thepersistence of chronic synovectomy.This is a challenge is for both thephysiotherapist and the patient.
The suggestions the twophysiotherapists offer are to:1) follow the evolution and healthof the joint post-hemarthrosis ona regular and systematic basis2) analyse, modify and closelysupervise post-hemarthroticactivity in order to prevent micro-traumatisms to the joint,inflammation and hypertrophy ofthe synovial tissue.
In conclusion, I invite you to readthis chapter that further describesthe ins and outs of the results whichthe physiotherapists arrived at. §
The
accelerated
return to
movement in
a hemophilia
patient can
also provoke
chronic
synovitis,
a target joint,
damage to the
cartilage,
a new bleed
and,
eventually,
hemophilic
arthropathy.

11
THE WFH 7th GLOBAL FORUMOn the safety and supply of treatment products for bleeding disorders
The 7th Global Forum on theSafety and Supply of TreatmentProducts for Bleeding Disorderstook place in MontrealSeptember 22-23, 2011. Thisconference, organized by theWorld Federation of Hemophilia(WFH), brought together almost180 participants includinghemostasis specialists,researchers, suppliers, regulatorsand product manufacturers, aswell as people living withbleeding disorders.Here are impressions from CHSQdelegates who attended theForum.
- F.L.
•••
The Forum focussed on threethemes : 1) perspectives on risk,2) achieving a safe and affordableblood supply and 3) noveltechnologies.
1) Perspectives on risk —including donor screening, viraltesting and new infectiousagents.
A report and future steps from aninternational consensus conferenceon risk-based decision making forblood safety was presented by theCBS. The WFH presented on theMSM issue (men having sex withmen) and donor deferral, while theDirector of Public Policy from theGay Men's Health CrisisAssociation advocated to revisethe Blood Donations Policies forMSM.
Also, data from a multicenterefficacy study of HIV, HCV and HBVblood screening scenarios waspresented.
After the four Perspectives on riskwere presented, a survey done withthe participants concluded thatdonor deferral is still needed asdonor deferrals are not judgementsabout the individual donor, but
rather are a method to reduce therisk from known, unknown,undetectable or emergingpathogens.
2) Achieving a safe and affordableblood supply —including innovative globalprojects to improve supply,changing trends in nationaltenders and bio-similar (follow-on biologics) policies.
An assessment of hemophilia andhealth technology, an update oninhibitors and clinical trial issueswere also presented by experts inthese fields.
3) Novel technologies —including updates on genetransfer studies, longer lastingproducts and other innovativeproduct developments.
There was an update on clinicalexperience using cryoprecipitate.Manufacturers presented theirupdates on pioneering designs forrecombinant coagulation factors,treatment options, research,efficacy and safety.
This was the second Global ForumI attended and, like every WFHconference, it was two intense daysof shared information. Once again,the information learned is that eventhough we might be close to genetherapy, for now our main focushas to stay on the safety and supplyof our products.
If you're interested in reading thepresentations mentioned above,they can be found on the WFHwebsite (www.wfh.org) underEvents.
Mylene D’Fana
•••
The conference touched upon afew subjects which are equallyimportant in today's hemophiliaworld. These subjects are importantnot only for hemophiliacs as clientsbut as well to the medicalcommunity and to suppliers ofthese products.
The whole machinery and peoplewho are involved in this domainmust carefully approach thesituation which is stable but stillcrucial. Decisions made based onpolitics could not be the best choiceand we don't want history to berepeated. What do I mean by this?I will briefly explain in my article.
Acceptance of blood donations frommen having sex with other men(MSM), with all respect to people'sorientation and without prejudice,should be evaluated based onscience, history and current spreadrate of infectious diseases withinthis community. The MSMcommunity is very fragile and doesnot want to be rejected with theirnoble gesture, which is really nobleas long as the donated blood is notonly free from HIV and hepatitiscontamination, but also from otherundetected viruses as well, whichthis group of people is more likelyto be prone.
It was also mentioned that menhaving sex with other men is not aproblem. Only unprotected sex isproblematic, but how far can wego with trust and not repeatmistakes from the 80s and 90s withthe blood scandal.
Selection criteria for donors at riskoutside of MSM community shouldalso be re-evaluated so as toincrease restrictions to ensure asafe and secure blood supply.
The cost of prophylaxis is high, butother factors should be taken underconsideration like the number ofbleeds in joints and the impact ofthese bleeds on the quality of lifeof not only the hemophiliac but ofhis family, etc.
Another important topic was oninhibitors. The world communitysees benefits in centralizing dataon patients with inhibitors, so as totransfer knowledge to specialistsaround the world. Patients whoswitch from plasma to recombinantfactor and from one recombinant
cont’d on page 12 : Global Forum >

proposed, but there was no solidevidence of positive response.There was a brief mention aboutbiosimilar products and theimportance of safety over efficacy.Biosimilars will be brought to themarket, but it is not known whenas they have not received approvalfrom the FDA yet.On a final note, it is important tohave a uniform method to labelproducts so as to have a standardway to communicate informationon products to patients and to themedical community.Closing remarks from the WFHPresident Mark Skinner concludedThe Seventh Global Forum. §
Anna Bizunowicz
CHSQ Appointment
The CHSQ Executive Director,Charles Vanasse, is pleased toannounce the appointment ofChristella Biha to the position ofadministrative assistant. Mrs. Bihawill take over from Suheir Maariwho is on maternity leave.Christella Biha has a richexperience in management withcommunity organisations,including the United Nations,having worked on a developmentprogram for Mauritania. Christellawas trained in accounting inCanada, and has a certificate inBusiness Administration fromSenegal.Christella Biha will ensure thesmooth running of our accountsand will participate in themanagement of our variousprojects. You can reach her bycalling 514 848-0666, local 24,or by writing to her at:[email protected] is in the office onTuesdays and Wednesdays. §
- C.V.
IN A WORD
to another do not show evidencethat they develop inhibitors.Nevertheless, it is a good idea tomonitor patients who switch fromone product to another.
It isimportantnot totransfer apatient fromone productto another incase ofillness. It isnotimportanthow manytreatmentsthe patienttakes but thebrand.Vaccinationto strengthenthe immunesystem was
GLOBAL FORUM (cont’d)
The world
community sees
benefits in
centralizing
data on patients
with inhibitors,
so as to transfer
knowledge to
specialists
around the
world.
HappyNew Year
2012!
The publication of this newsletter has been madepossible thanks to the financial contribution of
these pharmaceutical companies: