
TEVAR is Superior to Open Repair for Blunt Aortic Injury Royce Calhoun, MD, Stephanie Mayberg, PA-C,...
12
TEVAR is Superior to Open Repair for Blunt Aortic Injury Royce Calhoun, MD, Stephanie Mayberg, PA- C, Bill Pevec, MD, Danh Nguyen, PhD^, Lisa Mu^ J. Nilas Young, MD John Laird, MD o Division of Cardiothoracic Surgery o Division of Cardiology ^Department of Biostatistics University of California Davis Medical Center
-
Upload
susan-phillips -
Category
Documents
-
view
216 -
download
0
Transcript of TEVAR is Superior to Open Repair for Blunt Aortic Injury Royce Calhoun, MD, Stephanie Mayberg, PA-C,...

TEVAR is Superior to Open Repair for Blunt Aortic Injury
TEVAR is Superior to Open Repair for Blunt Aortic Injury
Royce Calhoun, MD, Stephanie Mayberg, PA-C, Bill Pevec, MD, Danh Nguyen, PhD^, Lisa Mu^
J. Nilas Young, MD John Laird, MDo
Division of Cardiothoracic SurgeryoDivision of Cardiology
^Department of BiostatisticsUniversity of California Davis Medical Center
Royce Calhoun, MD, Stephanie Mayberg, PA-C, Bill Pevec, MD, Danh Nguyen, PhD^, Lisa Mu^
J. Nilas Young, MD John Laird, MDo
Division of Cardiothoracic SurgeryoDivision of Cardiology
^Department of BiostatisticsUniversity of California Davis Medical Center

Blunt Aortic InjuryBlunt Aortic Injury
• 75% patients die at scene of accident
• 5% are unstable and die shortly after accident
• 25% of remainder die of other injuries
• Traditional approach to repair has been emergent open repair- Paraplegia 2-19%, Mortality 15-35%
• Current trend is appropriately timed urgent repair with an evolving endovascular role - Paraplegia 0%, Mortality 0-17%
• 75% patients die at scene of accident
• 5% are unstable and die shortly after accident
• 25% of remainder die of other injuries
• Traditional approach to repair has been emergent open repair- Paraplegia 2-19%, Mortality 15-35%
• Current trend is appropriately timed urgent repair with an evolving endovascular role - Paraplegia 0%, Mortality 0-17%

MethodsMethods
• Comparison of open repair vs. stent for TTAT
• 1999 to 2011
• First thoracic aortic stent was October 2005
• Exclusively stent repair for last 4 years
• Comparison of open repair vs. stent for TTAT
• 1999 to 2011
• First thoracic aortic stent was October 2005
• Exclusively stent repair for last 4 years

ApproachApproach
• Open
- n=35
- Thoracotomy, L groin 30
- Partial bypass 24
- Full bypass 7
- DHCA 4
- Thoracotomy, Gott shunt 1
• Open
- n=35
- Thoracotomy, L groin 30
- Partial bypass 24
- Full bypass 7
- DHCA 4
- Thoracotomy, Gott shunt 1
• Endograft
- n=40
- Femoral (cut down) 33
- Iliac (RP with graft) 2
- Infrarenal Aorta (4 RP, 1 Lap) 5
• Endograft
- n=40
- Femoral (cut down) 33
- Iliac (RP with graft) 2
- Infrarenal Aorta (4 RP, 1 Lap) 5

Stent Graft ResultsStent Graft Results
• Stents Used- 7 TAG - 1 C-TAG- 17 Excluder Cuffs - 4 AneuRx Cuffs - 2 Talent - 9 TX2
• 36/40 immediate technical success
• 39/40technical success after re-interventions
• Complete coverage of traumatic tear with no stent migration or endoleaks at most recent follow-up
• Stents Used- 7 TAG - 1 C-TAG- 17 Excluder Cuffs - 4 AneuRx Cuffs - 2 Talent - 9 TX2
• 36/40 immediate technical success
• 39/40technical success after re-interventions
• Complete coverage of traumatic tear with no stent migration or endoleaks at most recent follow-up

CaseCase
• 17 YO male, ejected from car
• Intracranial bleed, multiple orthopedic injuries, splenic and liver lacerations
• Bilateral severe pulmonary contusions
• pO2 55 on 100% FIO2 with 20 PEEP
• Comminuted aortic tear
• 17 YO male, ejected from car
• Intracranial bleed, multiple orthopedic injuries, splenic and liver lacerations
• Bilateral severe pulmonary contusions
• pO2 55 on 100% FIO2 with 20 PEEP
• Comminuted aortic tear



ResultsResults
Endograft Open p
Patients 40 (33 male) 35 (30 male)
Age 39 42 0.52
ISS 43 42 0.67
Admit to OR (hrs)
57 22 <0.01
Procedure time (hrs)
3.5 5.9 <0.01
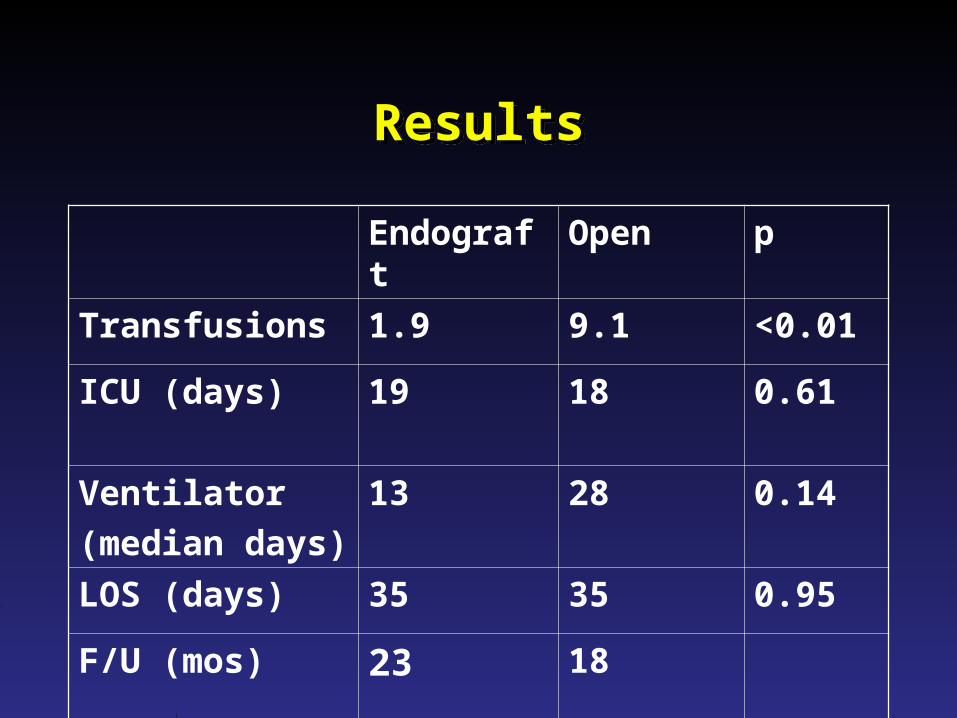
ResultsResults
Endograft Open p
Transfusions 1.9 9.1 <0.01
ICU (days) 19 18 0.61
Ventilator
(median days)
13 28 0.14
LOS (days) 35 35 0.95
F/U (mos) 23 18

Major Adverse EventsMajor Adverse Events
Endograft
n=40
Open
n=35
Death 3 7
Paraplegia 0 0
CVA 0 0
Renal Failure requiring dialysis
2 4
Subclavian Steal 2 0
Vascular Access 1 3
Re-intervention/re-op 6 5

ConclusionsConclusions• Endovascular stents for BAI can be
performed safely with excellent short and mid-term results
• Time from admission to intervention of BAI is increased in the stent group with no increased mortality
• Stents for BAI are associated with decreased OR times and intraoperative blood transfusions compared to open
• Endovascular stents for BAI can be performed safely with excellent short and mid-term results
• Time from admission to intervention of BAI is increased in the stent group with no increased mortality
• Stents for BAI are associated with decreased OR times and intraoperative blood transfusions compared to open


















